Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Differences in the Spirometry Parameters Between Indigenous and Non-Indigenous Patients with COPD: A Matched Control Study
Authors Sze DFL, Howarth TP ![]() , Lake CD, Ben Saad H
, Lake CD, Ben Saad H ![]() , Heraganahally SS
, Heraganahally SS ![]()
Received 10 February 2022
Accepted for publication 11 April 2022
Published 21 April 2022 Volume 2022:17 Pages 869—881
DOI https://doi.org/10.2147/COPD.S361839
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Dorothy FL Sze,1 Timothy P Howarth,2,3 Clair D Lake,4 Helmi Ben Saad,5,6 Subash S Heraganahally1,3,7
1Department of Respiratory and Sleep Medicine, Royal Darwin Hospital, Darwin, NT, Australia; 2College of Health and Human Sciences, Charles Darwin University, Darwin, NT, Australia; 3Darwin Respiratory and Sleep Health, Darwin Private Hospital, Darwin, NT, Australia; 4Pulmonary Function Laboratory, Royal Darwin Hospital, Darwin, NT, Australia; 5Laboratory of Physiology, Faculty of Medicine of Sousse, University of Sousse, Sousse, Tunisia; 6Research laboratory “Heart Failure, LR12SP09”, Farhat HACHED Hospital, Faculty of Medicine of Sousse, University of Sousse, Sousse, Tunisia; 7College of Medicine and Public Health, Flinders University, Adelaide, SA, Australia
Correspondence: Subash S Heraganahally, Department of Respiratory and Sleep Medicine, Royal Darwin Hospital, Darwin, NT, Australia, Tel +61-8-89228888, Fax +61-8-89206309, Email [email protected]; [email protected]
Background: Comparison of spirometry parameters between Indigenous and non-Indigenous patients with underlying chronic obstructive pulmonary disease (COPD) has been sparsely reported in the past. In this study, differences in the lung function parameters (LFPs), in particular spirometry values for forced vital capacity (FVC), forced expiratory volume in one second (FEV1) and FEV1/FVC ratio between Indigenous and non-Indigenous patients with COPD were assessed.
Methods: In this retrospective study, Indigenous and non-Indigenous patients with a diagnosis of COPD between 2012– 2020 according to spirometry criteria (ie; post-bronchodilator (BD) FEV1/FVC < 0.7) were included. A further analysis was undertaken to compare the differences in the spirometry parameters, including lower limit of normal (LLN) values matching for age, sex, height and smoking status between these two diverse ethnic populations.
Results: A total of 240/742 (32%) Indigenous and 873/4579 (19%) non-Indigenous patients were identified to fit the criteria for COPD. Indigenous patients were significantly younger (mean difference 9.9 years), with a greater proportion of females (50% vs 33%), underweight (20% vs 8%) and current smokers (47% vs 32%). Prior to matching, Indigenous patients’ post-BD percent predicted values for FVC, FEV1, and FEV1/FVC ratio were 17, 17%, and − 2 points lower (Hedges G measure of effect size large (0.91), large (0.87), and small (0.25), respectively). Among the matched cohort (111 Indigenous and non-Indigenous), Indigenous patients LFPs remained significantly lower, with a mean difference of 16%, 16%, and − 4, respectively (Hedges G large (0.94), large (0.92) and small (0.41), respectively). The differences persisted despite no significant differences in LLN values for these parameters.
Conclusion: Indigenous Australian patients with COPD display a significantly different demographic and clinical profile than non-Indigenous patients. LFPs were significantly lower, which may or may not equate to greater severity of disease in the absence of normative predictive lung function reference values specific to this population.
Keywords: chronic obstructive pulmonary disease, Global Initiative for Chronic Obstructive Lung Disease, First Nations, Indigenous, lung function test, spirometry
Plain Language Summary
Chronic Obstructive Pulmonary Disease (COPD) is more common among Indigenous Australians compared to non-Indigenous Australians, with a high morbidity and mortality associated. Previous studies have established generally lower lung function parameters in the Indigenous Australian population, however there is lack of published data showing how the lung function parameters would display in the presence of underlying COPD. In this study, we reported the differences in various lung function parameters between Indigenous and non-Indigenous patients who meet criteria for COPD diagnosis in the Top End of the Northern Territory of Australia. Our study showed that Indigenous patients with COPD are generally younger, with a higher proportion of females, and a lower body mass index. They also displayed significantly lower lung function values in comparison to their non-Indigenous counterparts, even after matching against age, sex, height and smoking status with both Forced Vital Capacity (FVC) and Forced Expiratory volume in one second (FEV1) approximately 16% lower. There was no significant difference in the lower limit of normal (LLN) values between the groups. Moreover, most Indigenous patients who demonstrate airflow obstruction, defined by a fixed FEV1/FVC ratio of <0.7, also demonstrated a FEV1/FVC ratio below LLN. The current approach to COPD diagnosis, treatment and management is based on recommendations drawn from non-Indigenous populations. There could be a role for correctional factors or use of LLN values when assessing the lung function in our Indigenous patients, so that health practitioners will be able to provide more appropriate care to this unique population.
Introduction
Chronic obstructive pulmonary disease (COPD) is a debilitating condition that is characterised by chronic airway inflammation, leading to obstruction of the airway and airflow limitation.1 In the Australian context, the prevalence of COPD is estimated to be around 7.5% for individuals aged 40 years and above. Amongst those aged 75 and above, the prevalence is increased to 30%.2 Clinical manifestations of COPD include shortness of breath, chronic cough and mucous production resulting in considerable impact on quality of life.1,3,4 Furthermore, COPD is noted to be the fifth leading cause of death in Australia.5 The risk factors for COPD include; genetic predisposition, tobacco smoking, and environmental or occupational exposure to dust, gas or fumes.1,3
The Australian Institute of Health and Welfare estimates that COPD is 2.3 times more prevalent among Australians of Aboriginal or Torres Strait Islanders descent (hereafter respectfully referred to as Indigenous Australians/patients), compared to non-Indigenous Australians.4 In the Northern Territory (NT) of Australia, approximately 30% of the population self-identify as Indigenous Australian, the highest proportion compared to all other Australian states and territories.6 Several recent studies from the Top End Health Service (TEHS) region of the NT of Australia have reported a significantly higher prevalence of chronic respiratory disorders among the Indigenous population, more specifically a high prevalence of COPD.7–11
Measurement of lung function tests including spirometry, static lung volumes using plethysmography and diffusing capacity for carbon monoxide (DLCO) aid in the clinical assessment and diagnosis of COPD.12 Spirometry, when appropriately performed, is a reproducible and objective measure of airway function and is essential in the diagnosis of COPD, and grading COPD airflow obstruction severity in terms of GOLD 1 to 4 (GOLD for Global Initiative for Chronic Obstructive Lung Disease).1 Lung function parameters (LFPs) measured on spirometry include: forced vital capacity (FVC), forced expiratory volume in one second (FEV1) and FEV1/FVC ratio.1,12 FEV1 and FVC are measured in litres (L), and subsequently calculated as a percentage of predicted values (% predicted) adjusted for age, sex, height, and race/ethnicity.13 According to the GOLD criteria, a diagnosis of COPD could be considered when post-bronchodilator (BD) spirometry results demonstrate a FEV1/FVC ratio < 0.7.
Multiple studies have demonstrated significantly lower LFPs, in particular lower FVC and FEV1 values, amongst Indigenous people.14–17 These studies have consistently demonstrated that spirometric values could be up to 20 to 30% lower among Indigenous people compared to Caucasian counterparts, even among “apparently healthy” Indigenous adults.18–21 However, normative spirometric reference values for adult Indigenous Australians are yet to be established.
Currently there is sparse evidence in the literature demonstrating how spirometry parameters display in the presence of underlying COPD amongst the Indigenous Australian population in comparison to their non-Indigenous peers. Moreover, in the absence of normative spirometry reference values for adult Indigenous Australians, and in the presence of a high burden of COPD, this information is sorely needed. Hence, it is imperative to investigate the spirometric parameters among an Indigenous cohort with a diagnosis of COPD against non-Indigenous Australians. Thus, the aim of this study was to ascertain the differences in the spirometric parameters between these two diverse ethnic populations among those who had undergone spirometry testing in the TEHS region of the NT of Australia.
Patients and Methods
Setting and Study Participants
This study was undertaken at the Respiratory and Sleep service based at the Royal Darwin Hospital and Darwin Respiratory and Sleep service/Darwin Private Hospital in the TEHS region of the NT of Australia. The study participants included all patients that performed acceptable and repeatable spirometry between 2012 and 2020. Also included were datasets from previously published studies of cohorts of participants from the TEHS region NT which included Indigenous and non-Indigenous populations.15,16,21,22 This study was conducted and reported according to strengthening and reporting of health research involving Indigenous people, including consultation with local institute Indigenous Australian representatives.23 Individual consent from the study participants was not obtained, as the study was retrospective in nature and no active interventions were investigated in this study. More details regarding the setting and study participants are available from our previous reports, including details regarding lung function testing protocol and clinical data collection.14–16,21 This study was approved by the Human Research Ethics Committee of the NT, TEHS and Menzies School of Health Research (Reference no: HREC 2019–3445) and was conducted according to the Declaration of Helsinki.
Spirometry Measurements
All spirometry tests were performed according to the American Thoracic Society and the European Respiratory Society guidelines and recommendations, including calibration of equipment and quality assurance.13 Spirometry was measured using the EasyOne Pro® (ndd Medical Technologies Inc. Zurich, Switzerland). Each individual volume-time and flow-volume graph was inspected for acceptability to assess session quality. Only spirometric tests that were graded as acceptable for session quality were included in this study.
When appropriate, all patients undergoing elective spirometry testing were instructed to refrain from smoking for at least two to four hours prior to spirometry testing. Patients using airway-directed inhaled pharmacotherapy were asked to withhold their medication for 12–24 hours prior to testing. Spirometry was repeated 15–20 minutes after inhalation of 400 µg of salbutamol via a spacer to assess BD responsiveness.1,2 Throughout this study the National Health And Nutrition Examination Survey (others/Caucasian) reference values were utilised, as is standard in clinical practice in this setting.24 If the study participants were identified to have undergone multiple LFTs during the study period, the earliest acceptable test for session quality was utilised for analysis. Spirometry parameters included were pre- and post-BD FEV1, FVC absolute values, % predicted and lower limits of normal (LLN), and FEV1/FVC (absolute and LLN).
Inclusion Criteria for Presence of COPD
To ascertain the presence of COPD, post-BD FEV1/FVC ratio < 0.7 was used according to GOLD and the Australian concise tool for COPD (COPD-X) recommendations.1,3
Matching of Indigenous and Non-Indigenous Patients with COPD
To assess differences in spirometry parameters, a sub-set analysis was conducted in a cohort of matched Indigenous and non-Indigenous patients. Matching of Indigenous and non-Indigenous patients was conducted based on four categories: sex (male/female); smoking status (never/former/current smoker); age (18–35, 36–50, 51–65, 66–75, 76–85, >85 years); height (cm) (females: < 150, 150–170, > 170, males: < 160, 160–180, > 180). These categorisation criteria were first applied to the Indigenous patient cohort of 240 patients with COPD, and then to the non-Indigenous cohort to identify patients with matched categories. There was an excess of Indigenous patients in multiple categories as compared to the non-Indigenous cohort. There was a greater proportion of Indigenous patients in the younger, shorter and current smoking categories. As such, further refinement was conducted to give an equal number of Indigenous and non-Indigenous patients for each category. In the case of an inadequate number of non-Indigenous patients fitting to an Indigenous patient category or vice versa, the excess patients were dropped from the dataset, resulting in a total of 222 matched patients (111 Indigenous, 111 non-Indigenous).
Statistical Analysis
Continuous parameters were tested for normality via the Shapiro Wilks distribution test, with body mass index (BMI) and smoking pack years displaying a non-parametric distribution, and other continuous variables approximating normal distribution. Non-parametric parameters were presented as medians (interquartile ranges (IQR)), normally distributed parameters as means (95% confidence intervals (CIs)), and categorical parameters as numbers (%). Clinical characteristics were compared between Indigenous and non-Indigenous patients by 2-tailed Student's t-test for normally distributed parameters. Equality of medians test was used for non-parametrically distributed parameters and 2-tailed proportions z-test for categorical parameters. LFPs were compared between Indigenous and non-Indigenous patients by 2-tailed Student's t-test. For both matched and unmatched cohorts Hedges G effect size was calculated for FVC % predicted, FEV1% predicted and FEV1/FVC ratio and reported as G (95% CI).25 Hedges G effect size was classified as small (0.2 < 0.5), moderate (0.5 < 0.8) or large (>0.8). All data were analysed in STATA IC 15 (StataCorp, Texas) and alpha set to 0.05 throughout.
Results
A total of 5321 patients were referred for at least one spirometry test between 2012 and 2020. From the total cohort, 240/742 (32%) Indigenous and 873/4579 (19%) non-Indigenous patients were identified as meeting diagnostic criteria for COPD (Figure 1). There was a significantly larger proportion of Indigenous patients with COPD compared to non-Indigenous patients (32% vs 19%, p <0.0001). The demographic/clinical factors for these patients differed significantly by Indigenous status (Table 1).
 |
Table 1 Clinical Characteristics of Indigenous and Non-Indigenous Patients with COPD |
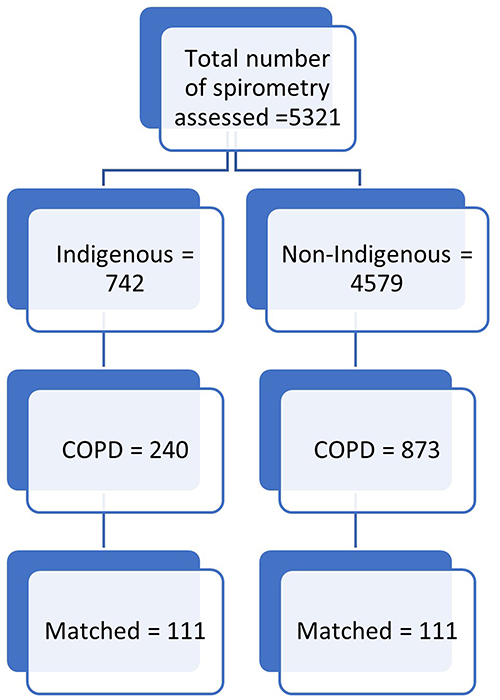 |
Figure 1 Flow chart of Indigenous and non-Indigenous study participants’ inclusion criteria. Abbreviation: COPD, chronic obstructive pulmonary disease. |
Indigenous patients had significantly lower values for all spirometry parameters, aside from FEV1 LLN values (Table 2). The post-BD FVC % predicted, FEV1% predicted and FEV1/FVC ratio were a mean 17%, 17%, and 2 points lower respectively among Indigenous patients with COPD in comparison to non-Indigenous patients. In addition to having FEV1/FVC ratio < 0.7, a significantly greater proportion of the Indigenous cohort also displayed FEV1/FVC ratio < LLN (92% vs 71%, p<0.001). Hedges G effect size for differences in percent predicted values was large for FVC (0.91, 95% CI 0.77, 1.06), FEV1 (0.87, 95% CI 0.72, 1.01), and small for FEV1/FVC (absolute) (0.25, 95% CI 0.11, 0.39).
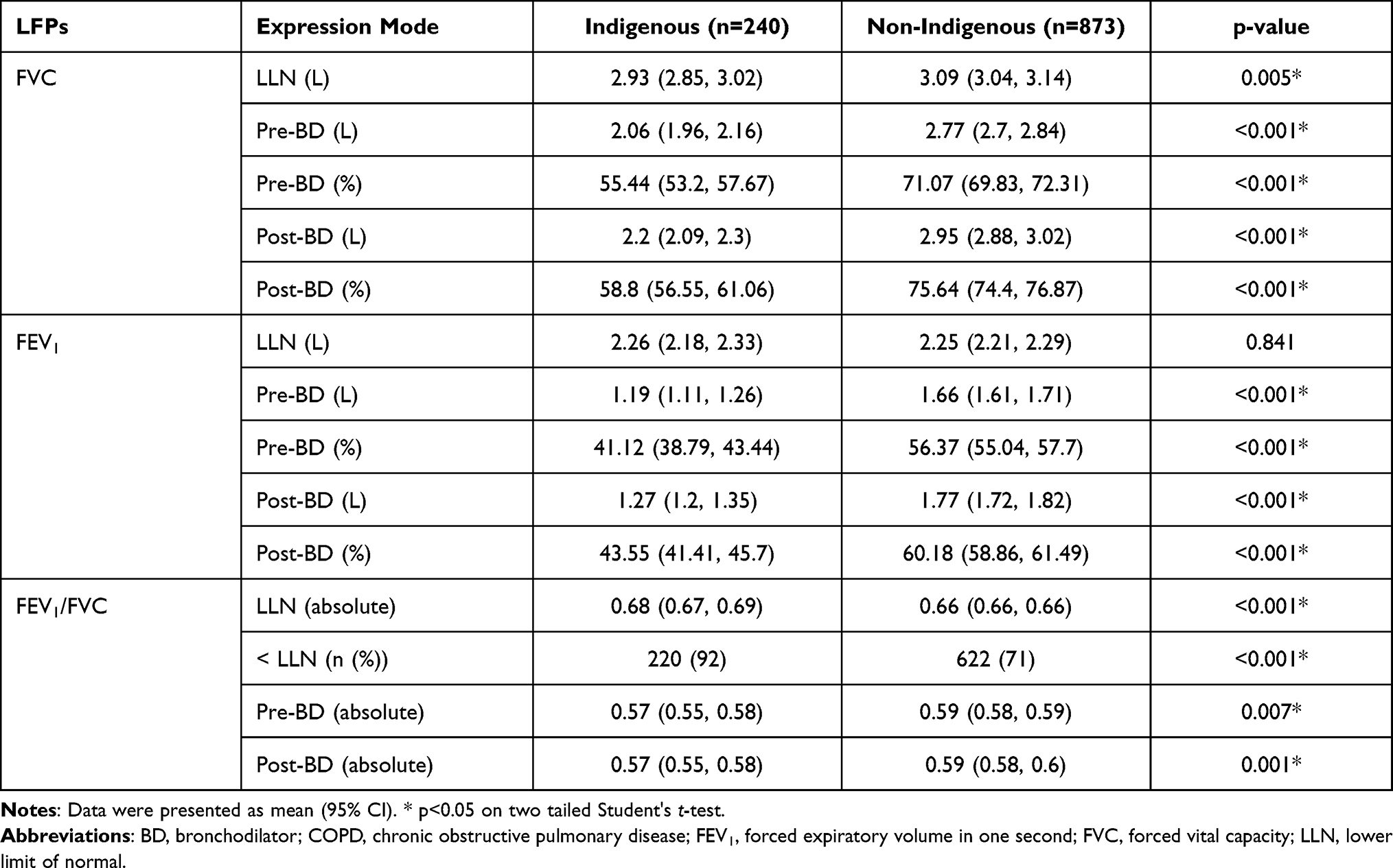 |
Table 2 Lung Function Parameters (LFPs) of Indigenous and Non-Indigenous Patients with COPD |
Matched Data for Indigenous and Non-Indigenous with COPD
A total of 222 patients were matched (111 Indigenous, 111 non-Indigenous) with no statistically significant differences in age, sex, height or smoking status. Despite matching, among the Indigenous cohort a greater proportion of patients were in the underweight BMI category, and among the non-Indigenous patients a greater median pack years of smoking was reported (Table 3). LFPs between the Indigenous and non-Indigenous patients with COPD in each sub-divided aged groups (18–35, 36–50, 51–65, 66–75, 76–85, >85 years) are represented in Table 1S.
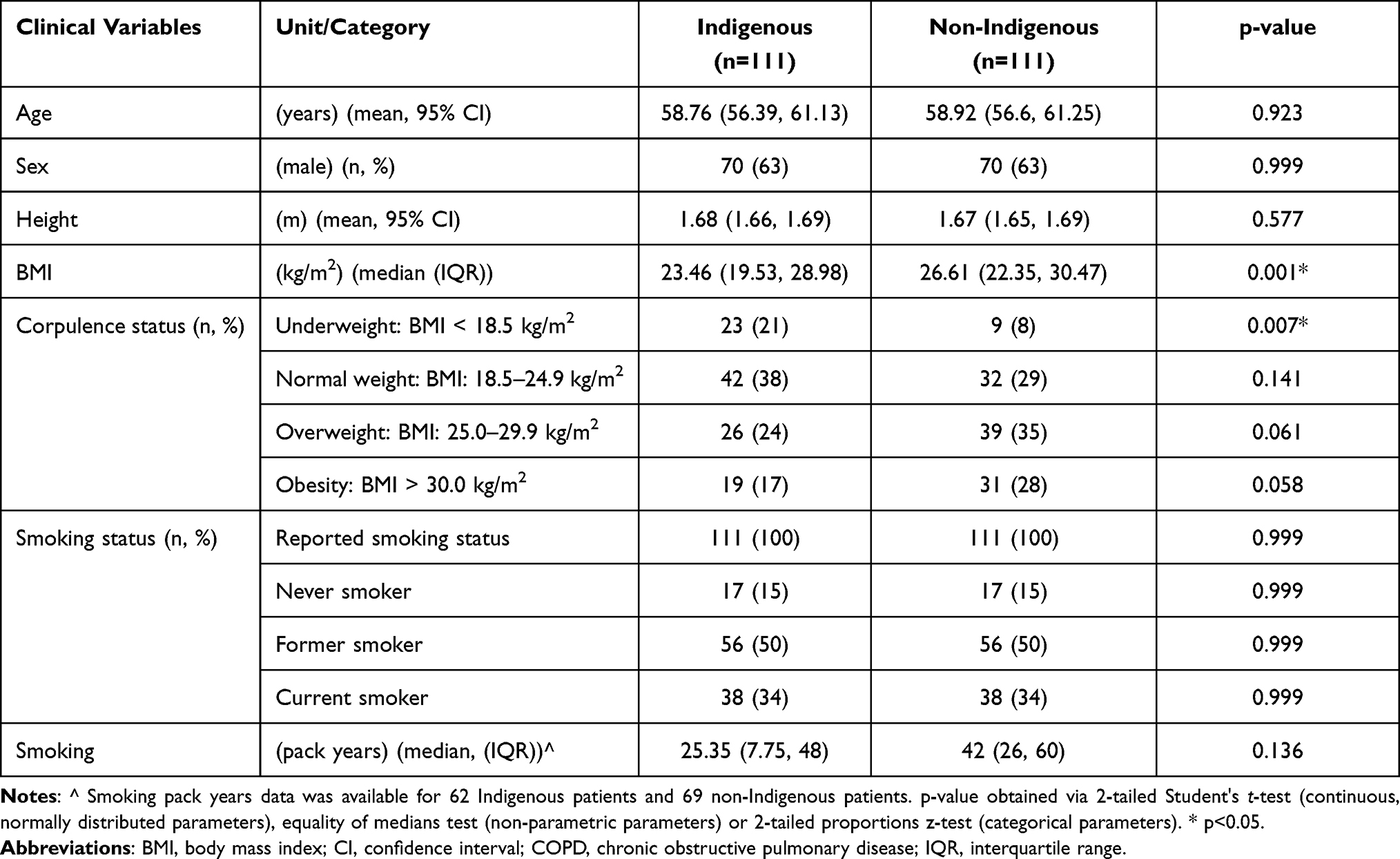 |
Table 3 Clinical Characteristics of Patients Included in Matched Cohorts (n=222) |
Among the matched cohort significant differences were noted in all LFPs aside for LLN values, once again with Indigenous patients displaying lower values than non-Indigenous patients with COPD (Table 4). Post-BD percent predicted values for FVC, FEV1, and FEV1/FVC ratio again displayed a mean 16%, 16%, and 4 points lower respectively among Indigenous patients with COPD in comparison to non-Indigenous patients (Figure 2). Hedges G effect size was large for FVC % predicted (0.94, 95% CI 0.66, 1.22), FEV1% predicted (0.92, 95% CI 0.64, 1.19) and small for FEV1/FVC ratio (0.41, 95% CI 0.15, 0.68).
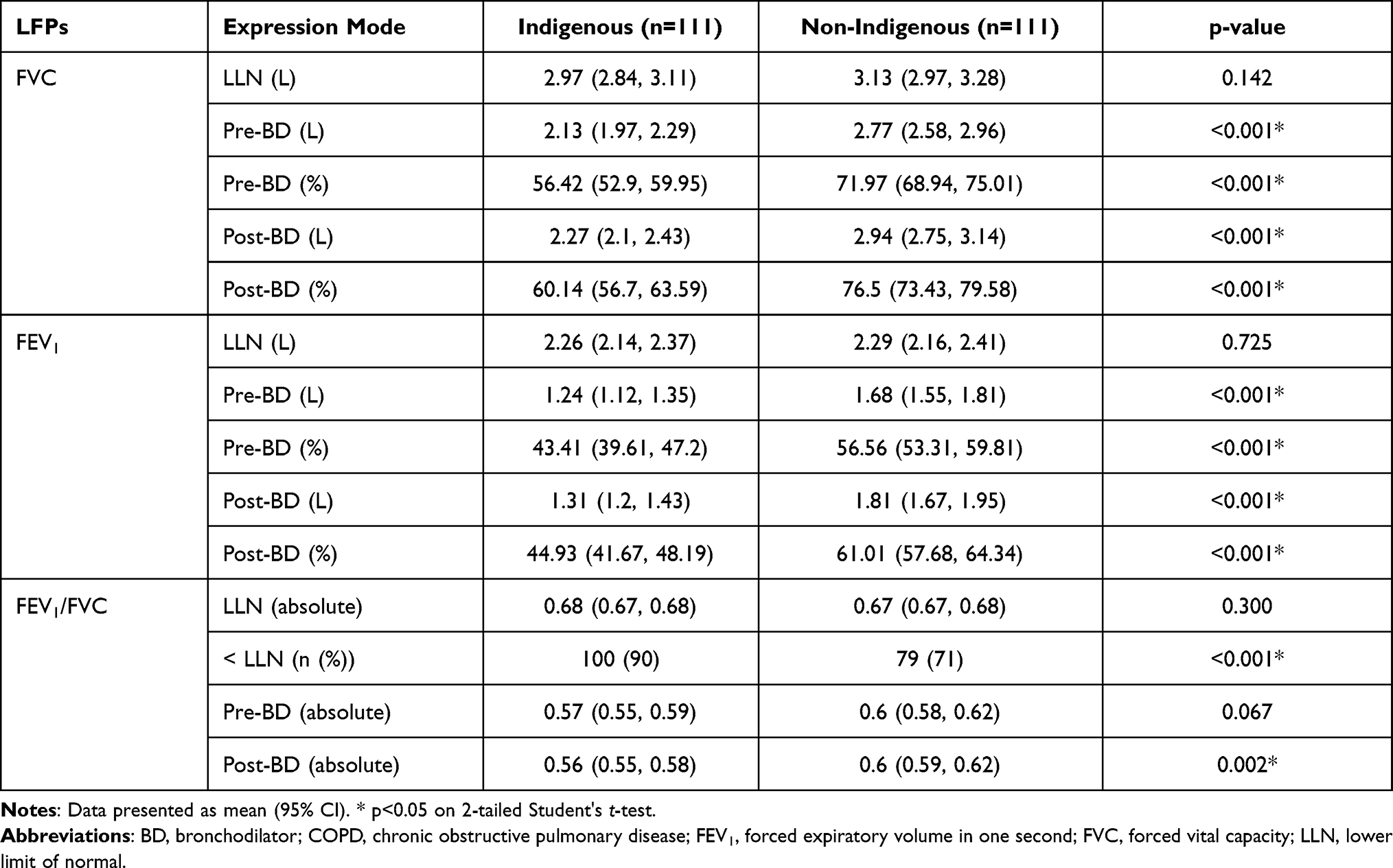 |
Table 4 Lung Function Parameters (LFPs) for Matched Indigenous and Non-Indigenous Patients with COPD |
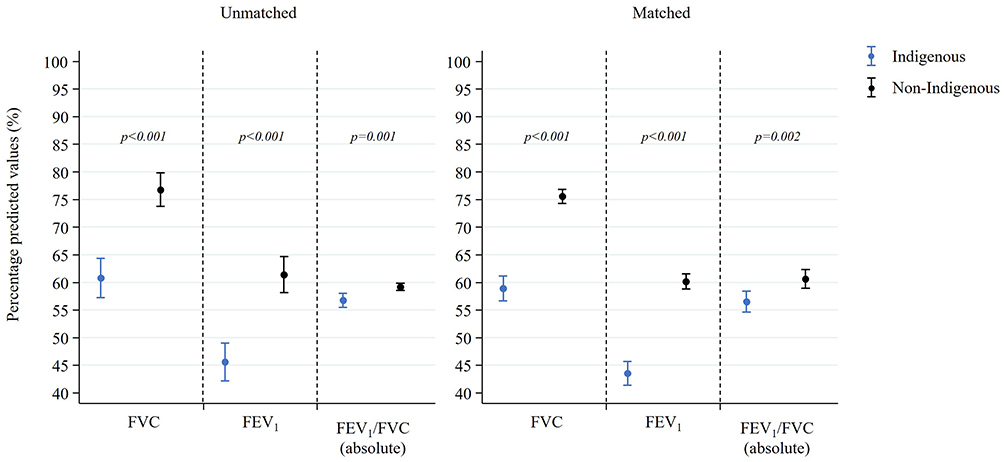 |
Figure 2 Percentage predicted values of FVC, FEV1 and FEV1/FVC ratio (mean (95% CI)) post-BD for unmatched and matched cohorts of Indigenous and non-Indigenous patients with post-BD FEV1/FVC < 0.7. Abbreviations: BD, bronchodilator; FEV1, forced expiratory volume in one second; FVC, forced vital capacity. |
Sub-Set Analysis
Within the cohort of COPD patients 220/240 (92%) Indigenous and 622/873 (71%) non-Indigenous patients were recorded to have FEV1/FVC < LLN, of which 150 (75 Indigenous and non-Indigenous) were able to be matched (Tables 2S and 5). Pre- and post-BD parameters for FVC and FEV1 were significantly lower among the Indigenous cohort in both matched and unmatched subgroups (mean difference in post-BD FVC % predicted and FEV1% predicted; matched: 15% and 12% and unmatched 15% and 13%). In the unmatched subgroup, LLN significantly differed for FVC and FEV1/FVC, while in the matched subgroup there were no significant differences. FEV1/FVC values did not significantly differ between Indigenous and non-Indigenous patients in the matched subgroup.
 |
Table 5 Lung Function Parameters for Matched Indigenous and Non-Indigenous Patients with FEV1/FVC < LLN |
Discussion
To the best of the authors’ knowledge, this is the first study to match and compare spirometry parameters between Indigenous and non-Indigenous Australian patients diagnosed with COPD, specifically from the NT of Australia. This study has demonstrated several key findings:
- In patients with COPD, Indigenous patients are significantly younger, and have lower BMI compared to non- Indigenous patients.
- Indigenous patients with COPD display significantly lower spirometry results, both as absolute values and as a percent of predicted in comparison to their non-Indigenous counterparts, even after matching against age, sex, height and smoking status.
- The FVC and FEV1 parameters are significantly lower for Indigenous patients, despite no significant difference in the LLN values between the groups, especially among the matched cohort.
- Most Indigenous patients who demonstrate airflow obstruction, defined by a fixed FEV1/FVC ratio of < 0.7, also have a FEV1/FVC ratio below the LLN.
The burden of chronic respiratory diseases is reported to be highly prevalent among various Indigenous populations globally.7–11,26–29 Existing literature has demonstrated that LFPs generally tend to be lower among Indigenous people.14–21 There is, however, sparse published quantitative data directly comparing LFPs for patients with COPD among diverse ethnic populations, including the Indigenous Australian population. Hence, the results represented in this study are of significant relevance in bridging our gap in knowledge. Moreover, this study further strengthens the notion that indeed, Indigenous Australians have lower LFPs even in the presence of underlying respiratory conditions such as COPD.
In this study, the absolute FEV1 and percent predicted values in Indigenous patients with COPD was observed to be significantly lower in comparison to non-Indigenous patients. It may be reasonable to speculate this truly reflects the severity of underlying disease among Indigenous patients with COPD, hence, the lower FEV1 values noted. However, even after controlling for age, sex, height and smoking status, these differences still persisted. Hence, an alternative explanation is plausible for this observation.
In line with observed lower FEV1, the FVC value was also similarly lower among Indigenous patients. The lower FVC values have consistently been observed in previous reports among Indigenous Australians.14,16,19,21,30,31 This may be suggestive of a restrictive ventilatory impairment or a combination of obstructive and restrictive impairments (ie; mixed impairment). The authors do acknowledge that static lung volumes as measured by plethysmography are required to accurately identify restrictive ventilatory impairment. However, it was beyond the scope of this study to assess plethysmography data. Nonetheless, in the real-world scenario, irrespective of the presence of any form or type of underlying respiratory condition, a restrictive ventilatory impairment is one of the most common spirometry patterns observed in this Indigenous population, including among a significant proportion of patients with COPD.16 The lower FVC (a restrictive ventilatory impairment) may indicate the presence of underlying conditions such as interstitial lung disease (ILD), chest wall deformities or neuromuscular disorders.32 However, the aforementioned respiratory conditions are very unlikely, as previous reports on chest radiological data have shown that respiratory conditions such as ILD are very rarely observed among this Indigenous Australian population.8,9 Similar to this study, the lower FVC has been reported in a subset of African ethnic population, indicating certain ethnic populations inherently demonstrate lower FVC values.33 Hence, it may be reasonable to speculate that a myriad of intrinsic or extrinsic factors34 may be responsible for the observed lower FVC values in this population, such as: genetics,35 ethnicity,36 birth weight,37 nutrition,38 childhood infections,39 and smoking.40
Although controversy exists if FEV1/FVC fixed ratio < 0.7 or the FEV1/FVC < LLN should be utilised in accurately diagnosing patients with COPD,41–43 it appears that the FEV1/FVC< LLN criteria is gaining popularity.44 However, due to lack of established spirometry reference norms for adult Indigenous Australians, currently there is sparse published data in the literature to demonstrate how the LLN parameters would display among Indigenous patients in comparison to non-Indigenous patients.45 In this study, we observed that the LLN values did not significantly differ between the Indigenous and non-Indigenous patients. Moreover, among Indigenous patients who demonstrated airflow obstruction by FEV1/FVC fixed ratio < 0.7 criteria, 92% of them also demonstrated to fit the FEV1/FVC < LLN criteria, whereas only 71% of the non-Indigenous patients did so. In light of this study’s findings and in the absence of spirometry reference norms for adult Indigenous Australians, in the authors’ opinion, the LLN parameters may be a better marker in the clinical decision making for the adult Indigenous Australians.
This study has highlighted that health practitioners caring for Indigenous patients should be aware of the implications in utilising spirometry criteria in COPD diagnosis and severity classification when adopting reference values drawn from non-Indigenous populations. A recent study has highlighted, irrespective of which of the recommended classifications used, COPD-X46 or GOLD,1 most Indigenous patients with COPD will likely fall into either the “severe” or “very severe” category.22 Indigenous patients in this study demonstrated 16–17% lower values for FVC and FEV1, compared to non-Indigenous patients. It is inevitable that an Indigenous patient with COPD will likely be assessed to have a higher disease burden by adopting spirometry reference values for the non-Indigenous population. In the aforementioned report on spirometry data in Indigenous population, creating a model by arbitrarily inflating FVC and FEV1 values by 15% (arbitrarily applying a correction factor for Indigenous patients) resulted in a re-categorization of 80% of patients to either “mild” or “moderate” airflow obstruction severity categories - A much closer approximation to the distribution found in non-Indigenous populations.22
Understandably, lack of normative lung function reference values may impose unprecedented diagnostic and management challenges among adult Indigenous patients with respiratory conditions, including COPD. Nonetheless, this study has highlighted that there are significant differences along with lower spirometry parameters among the adult Indigenous patients with COPD, in comparison to non-Indigenous patients. Furthermore, despite no significant differences in the LLN FEV1/FVC ratio values, the FEV1 values were noted to be substantially lower for Indigenous patients. Once again, as mentioned above, it is unclear at this stage if this truly reflects greater COPD disease burden due to higher smoking prevalence9,10 amongst Indigenous people or if it is due to inherent lower LFPs values in this Indigenous population.14,16,19,21,30,31 Indeed, future research should be directed toward elucidating the lived experience of Indigenous Australian patients with respiratory conditions in order to better correlate LFPs with the subjective experience on quality of life and the appropriateness of varied management and treatment plans.
We presume that the results of this study may be of interest for Indigenous health practitioners and primary care physicians. It is not clear at this stage if a correction factor for spirometry could be utilised in day-to-day diagnostic and clinical decision making for Indigenous patients presenting with COPD. There has been significant progress in the recent past in addressing respiratory health issues among the adult Indigenous Australian population, especially, from the Top End NT of Australia.7–11,14–17,21,22,47–59 Further studies, however, may be useful to better understand if our study findings are comparable to other Indigenous population both in other parts of Australian and globally, that may change the diagnostic and management of COPD paradigm among Indigenous populations.
Limitations
Caution must be exercised in relation to the applicability of the study outcomes in other Indigenous populations, as such, our data is only representative of patients residing in the TEHS region of the NT of Australia. Moreover, the Indigenous population in Australia is a diverse group of people. There exists a proportion of individuals who are descendants of inter-racial relationships, many of whom identify as Indigenous. Furthermore, although we could anticipate and extrapolate a similar trend to other Indigenous population, there may be other variables such as climate (desert vs tropical) or living environments (remote vs metropolitan) that could affect the development of lung and LFPs. The authors also acknowledge that the number of study participants in the matched group may be less than desired and radiological data was not assessed for the severity of underlying COPD between the two groups. It may be reasonable to accept this limitation, as such significant proportion of Indigenous people reside in remote and regional communities, hence imposing substantial challenges in conducting prospective studies. Furthermore, even among the matched cohort, the BMI significantly differed, indicating much reduced weight among the Indigenous cohort, which is reflective of the socioeconomic situation of many Indigenous patients. This study also did not include static lung volumes and DLCO data. Nonetheless, this is the first study to demonstrate differences in the spirometry parameters among Indigenous patients with COPD against non-Indigenous patients and there may be avenues in the future for further prospective research.
Conclusion
Our current approach to all patients with COPD is often based on guidelines that provide recommendations drawn from non-Indigenous general population. In this study we have demonstrated that Indigenous patients with COPD have substantially lower spirometry values for FVC and FEV1, even after matching for age, sex, height and smoking status. In light of this study’s findings, a more tailored approach to the diagnosis and management of this unique Indigenous population with COPD is required, enabling us to improve quality of life and close the health gap.60
Abbreviations
BD, bronchodilator; BMI, body mass index; CI, confidence interval; COPD, chronic obstructive pulmonary disease; COPD-X, concise tool for chronic obstructive pulmonary disease; DLCO, diffusing capacity for carbon monoxide; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; GOLD, global initiative for chronic obstructive lung disease; ILD, interstitial lung disease; IQR, interquartile range; LFPs, lung function parameters; LLN, lower limit of normal; NT, Northern territory; TEHS, top end health service.
Acknowledgments
We sincerely thank all the respiratory technologists and Respiratory Clinical Nurse Consultants from Darwin Respiratory and Sleep Health and Royal Darwin Hospital, Darwin Private Hospital, Darwin, Australia during this study. We also thank Ms Amelia Skaczkowskit, Flinders University, Northern Territory Medical Program medical student for helping with data collection for this research. We also extend our sincere appreciation to our remote community Indigenous health workers and also Mr Izaak Thomas (Australian Indigenous Luritja descendent) from the respiratory chronic respiratory disease co-ordination division in approving this research addressing much needed data in the diagnosis and management of adult Indigenous patients with respiratory disorders and for the appropriateness and respect in relation to the Indigenous context represented in this study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
Nil to declare.
Disclosure
All authors declare no conflicts of interest for this study.
References
1. Global initiative for chronic obstructive lung disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease; 2021. Available from: http://www.goldcopd.org.
2. Toelle BG, Xuan W, Bird TE, et al. Respiratory symptoms and illness in older Australians: the Burden of Obstructive Lung Disease (BOLD) study. Med J Aust. 2013;198(3):144–148. doi:10.5694/mja11.11640
3. Yang IA, George J, Jenkins S, et al. The COPD-X plan: Australian and New Zealand guidelines for the management of Chronic Obstructive Pulmonary Disease 2021. Version 2.63; February, 2021. Available from: https://copdx.org.au.
4. Australian Institute of Health and Welfare. Chronic obstructive pulmonary disease (COPD). Cat. no. ACM 35. Canberra: AIHW; 2020. Available from: https://www.aihw.gov.au/reports/chronic-respiratory-conditions/copd.
5. Australian Institute of Health and Welfare. Deaths in Australia. Cat. no. PHE 229. Canberra: AIHW; 2021. Available from: https://www.aihw.gov.au/reports/life-expectancy-death/deaths-in-australia.
6. Australian Bureau of Statistics. Estimates of Aboriginal and Torres Strait Islander Australians. Canberra, Australia: ABS; 2016.
7. Mehra S, Chang AB, Lam CK, et al. Bronchiectasis among Australian aboriginal and non-aboriginal patients in the regional and remote population of the Northern Territory of Australia. Rural Remote Health. 2021;21(2):6390. doi:10.22605/RRH6390
8. Heraganahally SS, Timothy TP, Sorger L. Chest computed tomography findings among adult Indigenous Australians in the Northern Territory of Australia. J Med Imaging Radiat Oncol. 2021;66(3):337–344. doi:10.1111/1754-9485.13295
9. Kruavit A, Fox M, Pearson R, Heraganahally S. Chronic respiratory disease in the regional and remote population of the Northern Territory Top End: a perspective from the specialist respiratory outreach service. Aust J Rural Health. 2017;25(5):275–284. doi:10.1111/ajr.12349
10. Heraganahally S, Wasgewatta SL, McNamara K, et al. Chronic obstructive pulmonary disease in aboriginal patients of The Northern Territory of Australia: a landscape perspective. Int J Chron Obstruct Pulmon Dis. 2019;14:2205–2217. doi:10.2147/COPD.S213947
11. Heraganahally SS, Wasgewatta SL, McNamara K, et al. Chronic obstructive pulmonary disease with and without bronchiectasis in aboriginal Australians – a comparative study. Int Med J. 2020;50(12):1505–1513. doi:10.1111/imj.14718
12. Ranu H, Wilde M, Madden B. Pulmonary function tests. Ulster Med J. 2011;80(2):84–90.
13. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. “ATS/ERS task force: standardisation of lung function testing”. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
14. Schubert J, Kruavit A, Mehra S, Wasgewatta S, Chang AB, Heraganahally S. Prevalence and nature of lung function abnormalities among Indigenous Australians referred to specialist respiratory outreach clinics in the Northern Territory. Int Med J. 2019;49(2):217–224. doi:10.1111/imj.14112
15. Heraganahally SS, Ponneri TR, Howarth TP, Saad HB. The effects of inhaled airway directed pharmacotherapy on decline in lung function parameters among indigenous Australian adults with and without underlying airway disease. Int J Chron Obstruct Pulmon Dis. 2021;16:2707–2720. doi:10.2147/COPD.S328137
16. Heraganahally SS, Howarth T, Mo L, Sorger L, Saad HB. Critical analysis of spirometric patterns in correlation to chest computed tomography among adult Indigenous Australians with chronic airway diseases. Expert Rev Respir Med. 2021;15(9):1229–1238. doi:10.1080/17476348.2021.1928496
17. Howarth TP, Saad HB, Perez AJ, Atos CB, White E, Heraganahally SS. Comparison of diffusing capacity of carbon monoxide (DLCO) and total lung capacity (TLC) between Indigenous Australians and Australian Caucasian adults. PLoS One. 2021;16(4):e0248900. doi:10.1371/journal.pone.0248900
18. de Hamel FA, Glass WJ. Observations on Maori-European lung function differences. Aust N Z J Med. 1975;5(1):44–48. doi:10.1111/j.1445-5994.1975.tb03254.x
19. Cooksley NA, Atkinson D, Marks GB, et al. Prevalence of airflow obstruction and reduced forced vital capacity in an Aboriginal Australian population: the cross-sectional BOLD study. Respirology. 2015;20(5):766–774. doi:10.1111/resp.12482
20. Veale AJ, Peat JK, Salome CM, Woolcock AJ, Thompson JE. ‘Normal’ lung function in rural Australian aborigines. Aust N Z J Med. 1997;27(5):543–549. doi:10.1111/j.1445-5994.1997.tb00962.x
21. Heraganahally SS, Howarth T, White E, Sorger L, Biancardi E, Ben Saad H. Lung function parameters among Australian Aboriginal “apparently healthy” adults: an Australian Caucasian and global lung function initiative (GLI-2012) various ethnic norms comparative study. Expert Rev Respir Med. 2020;23:1–11. doi:10.1080/17476348.2021.1847649
22. Heraganahally S, Howarth TP, White E, Ben Saad H. Implications of using the GLI-2012, GOLD and Australian COPD-X recommendations in assessing the severity of airflow limitation on spirometry among an Indigenous population with COPD: an Indigenous Australians perspective study. BMJ Open Respir Res. 2021;8(1):e001135. doi:10.1136/bmjresp-2021-001135
23. National Health and Medical Research Council. Ethical conduct in research with Aboriginal and Torres Strait Islander Peoples and communities: guidelines for researchers and stakeholders. Canberra: Commonwealth of Australia; 2018.
24. Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general US population. Am J Respir Crit Care Med. 1999;159(1):179–187. doi:10.1164/ajrccm.159.1.9712108
25. Olejnik S, Algina J. Measures of effect size for comparative studies: applications, interpretations, and limitations. Contemp Educ Psychol. 2000;25(3):241–286. doi:10.1006/ceps.2000.1040
26. State of the world’s Indigenous peoples. Indigenous peoples’ access to health services. United nations; 2018. Available from: https://www.un.org/development/desa/indigenouspeoples/wp-content/uploads/sites/19/2018/03/The-State-of-The-Worlds-Indigenous-PeoplesWEB.pdf.
27. Bird Y, Moraros J, Mahmood R, et al. Prevalence and associated factors of COPD among Aboriginal peoples in Canada: a cross-sectional study. Int J Chron Obstruct Pulmon Dis. 2017;30(12):1915–1922. doi:10.2147/COPD.S138304
28. Australian institute of health and welfare. Indigenous Australians more likely to die from CHD and COPD, but some positive trends emerging - Australian Institute of Health and Welfare; 2014. Available from: https://www.aihw.gov.au/news-media/media-releases/2014/june/indigenous-australians-more-likely-to-die-from-chd.
29. Ospina MB, Voaklander DC, Stickland MK. Prevalence of asthma and chronic obstructive pulmonary disease in Aboriginal and non-Aboriginal populations: a systematic review and meta-analysis of epidemiological studies. Can Respir J. 2012;19(6):355–360. doi:10.1155/2012/825107
30. White E, James A, de Klerk N, Musk A, Hall G. Selection of appropriate spirometry reference values in Aboriginal Australians. Australian Indigenous Health Bulletin; 2019;19.
31. Hall GL, Pearson G. Reduced forced vital capacity in Aboriginal Australians: biology or missing evidence? Respirology. 2015;20(5):693–694. doi:10.1111/resp.12552
32. Martinez-Pitre PJ, Sabbula BR, Cascella M. Restrictive lung disease. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 [Updated July 31, 2021]. Available from https://www.ncbi.nlm.nih.gov/books/NBK560880/.
33. Obaseki DO, Erhabor GE, Awopeju OF, et al. Reduced forced vital capacity in an African population. Prevalence and risk factors. Ann Am Thorac Soc. 2017;14(5):714–721. doi:10.1513/AnnalsATS.201608-598OC
34. Stanojevic S, Wade A, Stocks J. Reference values for lung function: past, present and future. Eur Respir J. 2010;36(1):12–19. doi:10.1183/09031936.00143209
35. Kumar R, Seibold MA, Aldrich MC, et al. Genetic ancestry in lung-function predictions. N Engl J Med. 2010;363(4):321–330. doi:10.1056/NEJMoa0907897
36. Braun L, Wolfgang M, Dickersin K. Defining race/ethnicity and explaining difference in research studies on lung function. Eur Respir J. 2013;41(6):1362–1370. doi:10.1183/09031936.00091612
37. Westrupp EM, D’Esposito F, Freemantle J, Mensah FK, Nicholson JM. Health outcomes for Australian Aboriginal and Torres Strait Islander children born preterm, low birthweight or small for gestational age: a nationwide cohort study. PLoS One. 2019;14(2):e0212130. doi:10.1371/journal.pone.0212130
38. Gaultier C, Crapo R. Effects of nutrition, growth hormone disturbances, training, altitude and sleep on lung volumes. Eur Respir J. 1997;10(12):2913–2919. doi:10.1183/09031936.97.10122913
39. Howarth T, Brunette R, Davies T, et al. Antibiotic use for Australian Aboriginal children in three remote Northern Territory communities. PLoS One. 2020;15(4):e0231798. doi:10.1371/journal.pone.0231798
40. Fenton ME, Graham BL, Stanojevic S, Whitford L, Ironstand L. Interpretation of Spirometry in Saskatchewan First Nations Adults. Ann ATS. 2018;15(10):1237–1239. doi:10.1513/AnnalsATS.201711-909RL
41. Swanney MP, Ruppel G, Enright PL, et al. Using the lower limit of normal for the FEV1/FVC ratio reduces the misclassification of airway obstruction. Thorax. 2008;63(12):1046–1051. doi:10.1136/thx.2008.098483
42. Hoesein FAAM, Zanen P, Lammers JJ. Lower limit of normal or FEV1/FVC <0.70 in diagnosing COPD: an evidence-based review. Respir Med. 2011;105(6):907–915. doi:10.1016/j.rmed.2011.01.008
43. Dijk WV, Tan W, Li P, et al. Clinical relevance of fixed ratio vs lower limit of normal of FEV1/FVC in COPD: patient-reported outcomes from the CanCOLD cohort. Ann Fam Med. 2015;13(1):41–48. doi:10.1370/afm.1714
44. Stanojevic S, Kaminsky DA, Miller M, et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur Respir J. 2021:2101499. doi:10.1183/13993003.01499-2021.
45. Blake TL, Chang AB, Petsky HL, et al. Spirometry reference values in Indigenous Australians: a systematic review. Med J Aust. 2016;205(1):35–40. doi:10.5694/mja16.00226
46. Stepwise management of stable COPD. Lung Foundation Australia; 2021. Available from https://lungfoundation.com.au/resources/stepwise-management-of-stable-copd/.
47. Heraganahally SS, Silva SAMS, Howarth TM, Kangaharan N, Majoni SW. Comparison of clinical manifestation among Australian Indigenous and non‐ Indigenous patients presenting with pleural effusion. Int Med J. 2021. doi:10.1111/imj.15310
48. Heraganahally SS, Mortimer N, Howarth T, et al. Utility and outcomes among Indigenous and non-Indigenous patients requiring domiciliary oxygen therapy in the regional and rural Australian population. Aust J Rural Health. 2021;29(6):918–926. doi:10.1111/ajr.12782
49. Heraganahally SS, Kruavit A, Oguoma VM, et al. Sleep apnoea among Australian Aboriginal and Non- Aboriginal patients in the Northern Territory of Australia– a comparative study. Sleep. 2020;43(3):zsz248. doi:10.1093/sleep/zsz248
50. Mehra S, Ghimire RH, Mingi JJ, et al. Gender differences in the clinical and polysomnographic characteristics among Australian aboriginal patients with obstructive sleep apnea. Nat Sci Sleep. 2020;12:593–602. doi:10.2147/NSS.S258330
51. Garg H, Er XY, Howarth T, Heraganahally SS. positional sleep apnea among regional and remote Australian population and simulated positional treatment effects. Nat Sci Sleep. 2020;12:1123–1135. doi:10.2147/NSS.S286403
52. Heraganahally SS, Kerslake C, Issac S, et al. Outcome of public hospital-funded continuous positive airway therapy device for patients with obstructive sleep apnoea: an Australian perspective study. Sleep Vigilance. 2020;4(2):195–204. doi:10.1007/s41782-020-00114-4
53. Heraganahally SS, Zaw KK, Tip S, et al. Obstructive sleep apnoea and adherence to continuous positive airway therapy among Australian women. Int Med J. 2022;52(3):440–450. doi:10.1111/imj.15076
54. Heraganahally SS, Rajaratnam B, Silva SAAS, et al. Obstructive sleep apnoea and cardiac disease among aboriginal patients in the Northern Territory of Australia. Heart Lung Circ. 2021;30(8):1184–1192. doi:10.1016/j.hlc.2021.01.007
55. Benn E, Wirth H, Short T, Howarth T, Heraganahally SS. The Top End Sleepiness Scale (TESS): a new tool to assess subjective daytime sleepiness among indigenous Australian adults. Nat Sci Sleep. 2021;13:315–328. doi:10.2147/NSS.S298409
56. Heraganahally SS, Howarth TP, Wirth H, Short T, Benn E. Validity of the New “Top End Sleepiness Scale” (TESS) against the STOP-bang tool in predicting obstructive sleep apnoea among Indigenous Australian Adults. Intern Med J. 2021. doi:10.1111/imj.15633
57. Heraganahally SS, White S. A cost-effective novel innovative box (C-box) to prevent cockroach infestation of continuous positive airway pressure equipment: a unique problem in Northern Tropical Australia. Am J Trop Med Hyg. 2019;101(4):937–940. doi:10.4269/ajtmh.19-0434
58. Heraganahally SS, Ghimire RH, Howarth T, Kankanamalage OM, Palmer D, Falhammar H. Comparison and outcomes of emergency department presentations with respiratory disorders among Australian Indigenous and non-Indigenous Patients. BMC Emerg Med. 2022;22(1):11. doi:10.1186/s12873-022-00570-3
59. Heraganahally SS, Howarth T, Sorger L, Ben Saad H. Sex differences in pulmonary function parameters among Indigenous Australians with and without chronic airway disease. PLoS One. 2022;17(2):e0263744. doi:10.1371/journal.pone.0263744
60. Closing the Gap: Indigenous Health Campaign. Closing the gap in partnership: everyone enjoys long and healthy lives. Canberra: Australian Human Rights Commission; March 18, 2021. [cited May 4, 2021]. Available from: https://www.closingthegap.gov.au/everyone-enjoys-long-and-healthy-lives.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.