Back to Journals » Clinical Epidemiology » Volume 12
Differences in Psychotropic Drug Prescribing Between Ethnic Groups of People with Dementia in the United Kingdom
Authors Jones ME, Petersen I ![]() , Walters K
, Walters K ![]() , Bhanu C
, Bhanu C ![]() , Manthorpe J, Raine R, Mukadam N, Cooper C
, Manthorpe J, Raine R, Mukadam N, Cooper C
Received 5 July 2019
Accepted for publication 4 November 2019
Published 20 January 2020 Volume 2020:12 Pages 61—71
DOI https://doi.org/10.2147/CLEP.S222126
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Vera Ehrenstein
Mary Elizabeth Jones, 1 Irene Petersen, 1 Kate Walters, 1 Cini Bhanu, 1 Jill Manthorpe, 2 Rosalind Raine, 3 Naaheed Mukadam, 4 Claudia Cooper 4
1Department of Primary Care and Population Health, University College London, London, UK; 2NIHR Health and Social Care Workforce Research Unit, King’s College London, London, UK; 3Epidemiology and Public Health, University College London, London, UK; 4Division of Psychiatry, University College London, London, UK
Correspondence: Claudia Cooper
Division of Psychiatry, University College London, 6th Floor, Maple House, Tottenham Court Road, London W1T 7BN, UK
Tel +44 7759703235
Email [email protected]
Purpose: To test hypotheses that minority ethnic people with dementia in the UK receive fewer anti-dementia drugs and more psychotropic and anticholinergic drugs associated with harms.
Patients and Methods: We analyzed UK primary care electronic health records from The Health Improvement Network (THIN) database (2014– 2016), comparing psychotropic drug prescribing initiation and duration between people with dementia from White, Black, and Asian ethnic groups. We repeated analyses in people (aged 50+) without dementia, to explore whether any differences found reflected prescribing patterns in the general older population, or were specific to dementia.
Results: We included 53,718 people with and 1,648,889 people without dementia. Among people with dementia, compared to White ethnic groups, Asian people were less likely to be prescribed anti-dementia drugs when they were potentially indicated (adjusted prevalence rate ratio 0.86 (95% Confidence Interval 0.76– 0.98)), and received them for on average 15 days/year less. Compared to White groups, Asian and Black individuals with dementia were no more likely to take an antipsychotic drug, but those that had were prescribed them for 17 and 27 days/year more, respectively (190.8 (179.6– 199.1) and 200.7 (191.1– 206.5) days). Black people were less likely to be prescribed anxiolytics/hypnotics (0.60 (0.44– 0.8)), but the duration these drugs were prescribed was similar across ethnic groups. Asian people were more likely to be prescribed anticholinergic drugs (1.43 (1.19– 1.73)), in analyses unadjusted for cardiovascular comorbidities. Among people without dementia, those in the Asian and Black ethnic groups were less likely to be prescribed psychotropic drugs, relative to people from White groups.
Conclusion: Among people with dementia, Asian groups received less potentially beneficial symptomatic treatments, and Asian and Black groups were prescribed antipsychotic drugs for longer than White ethnic groups. Our findings may indicate care inequalities.
Keywords: ethnicity, prevalence rate ratio, medication, prescription duration
Introduction
Around 850,000 people live with dementia in the UK.1 The number of minority ethnic people with dementia in England and Wales is projected to increase seven-fold in the next 40 years.2 In the UK, people from Black ethnic groups have higher rates of dementia, but fewer cases are diagnosed in a timely manner, compared with White ethnic groups.2,3 Their increased dementia risk may be explained by higher rates of dementia risk factors, including hypertension, diabetes, stroke and heart disease.2,3 Equality of care is a cornerstone of most National Dementia Strategies, including those of the UK,4 but there are concerns that current dementia services may not be culturally competent.2
We investigated whether there are inequalities between the UK’s ethnic groups in the likelihood of receiving good quality mental healthcare after a dementia diagnosis. Previous studies have found inequalities in the treatment of common mental disorders in the UK.5,6 People with dementia from minority ethnic groups appear to present later to services, when symptoms are more severe. In a USA study, people from African American ethnic groups were less likely to receive anti-dementia medication than those from non-Hispanic White ethnic groups; minority ethnic people are also under-represented in dementia drug trials.7 Large studies in Australia and the USA have concluded that minority ethnic groups access anti-dementia treatments later8 or are more likely to discontinue.9
We defined good quality mental healthcare as: access to cholinesterase inhibitors or memantine (anti-dementia drugs) to treat dementia symptoms where they are indicated; low antipsychotic, hypnotic, and anxiolytic medication use, due to the associated risks of cognitive decline, falls, cerebrovascular events and death;10 and low use of anticholinergic drugs, which are associated with worse cognition and quality of life.11 The Choosing Wisely recommendations and other guidelines advocate limiting initiation and duration of antipsychotic prescribing for behavioural and psychological symptoms of dementia (BPSD) as far as possible.12
We tested our hypothesis that people with dementia from Black and Asian ethnic groups are less likely to receive good quality mental healthcare as defined above, compared with the White majority population. We compared these results to rates of psychotropic drug prescriptions in older people (aged 50+) without dementia, by ethnic group, to explore whether any differences reflected prescribing in the general older population, or were specific to dementia.
Methods
Data
We used primary care electronic health records from The Health Improvement Network (THIN) database, which is broadly representative of the UK population.13 At time of data collection, this contained data from 744 contributing general practices and 15.6 million patients. During routine primary care consultations, General Practitioners (GPs) record patients’ medical conditions, symptoms and diagnoses using the Read hierarchical classification system.14 Around 90% of UK, NHS contacts and almost all first contacts for symptoms are in general practice.15 Information about drug prescriptions is automatically entered. THIN also captures demographic information, including sex, year of birth, and Townsend score, a measure of social deprivation based on the patient’s postcode and information from the 2011 UK census.16
The National Health Service (NHS) South-East Multi-Centre Research Ethics Committee approved the use of THIN for scientific research in 2003. The IQVIA World Publications Scientific Review Committee granted scientific approval for this study in March 2017 (reference 17THIN019).
Study Population
We included individuals aged 50–105 years contributing data to THIN between 1 January 2014 and 31 December 2016. Patients with dementia were defined by a Read code indicating dementia or an anti-dementia drug prescription (prescribed only for dementia), as in previous THIN dementia studies.3,17 We carried out a retrospective cohort study; the cohort was dynamic, with individuals entering and leaving the study at different times. For the dementia cohort, we included people who had a dementia diagnosis for the whole or part of the study period. Individuals were followed from the latest of: 1 January 2014, their 50th birthday, date of registration with the practice, when the practice met standard criteria for Acceptable Mortality Reporting (AMR) and Acceptable Computer Usage (ACU),18,19 or the first indication of dementia or an anti-dementia drug prescription. The end date was defined as the earliest of: patient’s death, their 105th birthday, patient leaving the practice, practice leaving THIN or 31 December 2016. We excluded patients with less than 6 months of follow-up. For the non-dementia cohort, individuals were followed from the latest of: 1 January 2014, their 50th birthday, date of registration with the practice, when the practice met standard criteria for AMR and ACU.18,19 The end date was defined as the earliest of: patient’s death, their 105th birthday, patient leaving the practice, practice leaving THIN or 31 December 2016. We excluded patients with less than 6 months of follow-up or with any indication of dementia since registration.
Outcome and Risk Factor Measurements
We identified patients that received a prescription for an anticholinergic, antipsychotic, or anxiolytic or hypnotic drug, or for an anti-dementia drug for those in the dementia cohort. We identified drugs in these categories using the British National Formulary, except for anticholinergic drugs. Receipt of an anticholinergic drug was defined as receiving a prescription for a drug with definite anticholinergic burden, as listed in previous work,20 two or more times in a calendar year. We excluded one-off prescriptions, as these are less likely to result in harm and in many cases, these would have been prescribed but not taken, as most drugs with definite anticholinergic burden are not prescribed as single prescriptions. We excluded patients with a dementia diagnosis that contraindicated anti-dementia drugs (vascular or frontotemporal dementia) from anti-dementia drug analyses.
GPs record information about ethnicity in patient records, based on self-report. Ethnicity was grouped into White (British or other white background), Asian (Indian, Pakistani, Bangladeshi, or other Asian background), Black (African, Caribbean, or other black background), and mixed/other ethnic groups (mixed, Chinese, Arab), based on the Office for National Statistics (ONS) classification and a previous THIN study.3 Individuals from mixed/other ethnic groups were excluded due to small numbers (<0.10% of the cohort). Covariates included age, sex, and Townsend score (in quintiles, with quintile 1 being least deprived). Age was analyzed in 10-year categories; the last category was 90–105 years due to small numbers of individuals aged over 100. The Prescribing Index indicates the number of British National Formulary chapters from which patients received prescriptions (excluding vaccines and anesthetic drugs, and for this study excluding anti-dementia drugs). It is a valid measure for comorbidity.21 The Prescribing Index was used in describing the cohorts but not as a covariate, as this would have adjusted for the drug categories that were used as the outcome measure.
Analyses
We analyzed data using Stata version 15.1 (Stata Corp, College Station, Texas). For the period 2014–2016, we estimated overall prescribing prevalence of anti-dementia, anticholinergic, antipsychotic, and anxiolytic and hypnotic drugs in patients with dementia; and of anticholinergic, antipsychotic, and anxiolytic and hypnotic drugs in the non-dementia cohort. We used multivariable Poisson regression to investigate the association of ethnicity with these outcomes, adjusting for 10-year age bands, sex, and Townsend score. GP practice was fitted as a random effect in the models to account for variation in individual practices. Prevalence rate ratios were calculated for each outcome in the dementia and non-dementia cohorts. Interactions between age and sex, sex and ethnicity, and age and ethnicity were explored and none were found.
For the dementia cohort, we defined duration of all prescription episodes during the study period for the anti-dementia, antipsychotic, and anxiolytic and hypnotic drug categories. Duration was not estimated for anticholinergic drugs due to the heterogeneity of this drug category. For each drug category, a prescription episode was defined as the time from a prescription during the study period and any subsequent prescriptions that were prescribed in less time than the 80% inter-arrival density, or the time required for 80% of patients to receive their next prescription. The 80% inter-arrival density was calculated using the waiting time distribution.22 Patients could have multiple prescription episodes during the study period for each drug category. The sum of time from all of a patient’s prescription episodes for a drug category was estimated, and for each ethnicity, a proportion was calculated of the time on a prescription (in days) over total follow-up time (in years).
We conducted complete case analyses (Supplementary Tables 3 and 4) and with missing ethnicity and Townsend data imputed using multiple imputation by chained equations. Compared to complete case analysis, multiple imputation can provide unbiased and statistically more powerful results by using information from individuals with incomplete data.23 This approach operates under the missing at random assumption,24 which cannot be ascertained from the observed data alone. To increase the plausibility of this assumption, a range of auxiliary variables was included in the imputation model that may predict missing values of ethnicity or the likelihood of ethnicity being recorded, as in a previous THIN study.3 After 50 cycles of the chained equations, 50 imputed data sets were created. Each imputed data set was analyzed identically, and results combined using Rubin’s rules.25,26 While we report results from both complete case and multiple imputation analyses, we consider our primary results to be those from the multiple imputation analyses.
Results
Characteristics of the Sample
We included 53,718 individuals aged 50 to 105 in our dementia cohort. Ethnicity was recorded in 53.1% of the dementia cohort; those without an ethnicity record had characteristics most similar to individuals with a recorded White ethnicity (Supplementary Table 1). We included incident and prevalent cases of dementia and reported the imputed patient characteristics (Table 1). Of the dementia cohort, 96.6% of individuals were classified as being from a White ethnic group, 2.2% from an Asian and 1.2% from a Black ethnic group. Among the dementia cohort, less than 0.1% had a frontotemporal dementia diagnosis, while 1.0% had a mixed dementia diagnosis, 18.1% had a vascular dementia diagnosis, 19.3% had an Alzheimer’s diagnosis, 1.4% dementia with Parkinson’s disease or Lewy Body dementia, 0.5% alcohol-related dementia, 1.0% had another specified dementia diagnosis, and 58.7% of patients had an unspecified diagnosis (Table 1). The prevalence of vascular dementia was nearly 6% higher in Asian patients than Black patients; the prevalence of the other diagnoses did not vary by more than 3% between ethnicities. The diagnosis prevalence for frontotemporal dementia was too low to report by ethnicity. We included 1,648,889 people in the non-dementia cohort with imputed ethnicity and Townsend score, of whom 95.1% were classified as being from a White ethnic group, 3.3% from an Asian, and 1.6% from a Black ethnic group. These were individuals who had no indicators of dementia diagnosis during or prior to the study period (Supplementary Table 2).
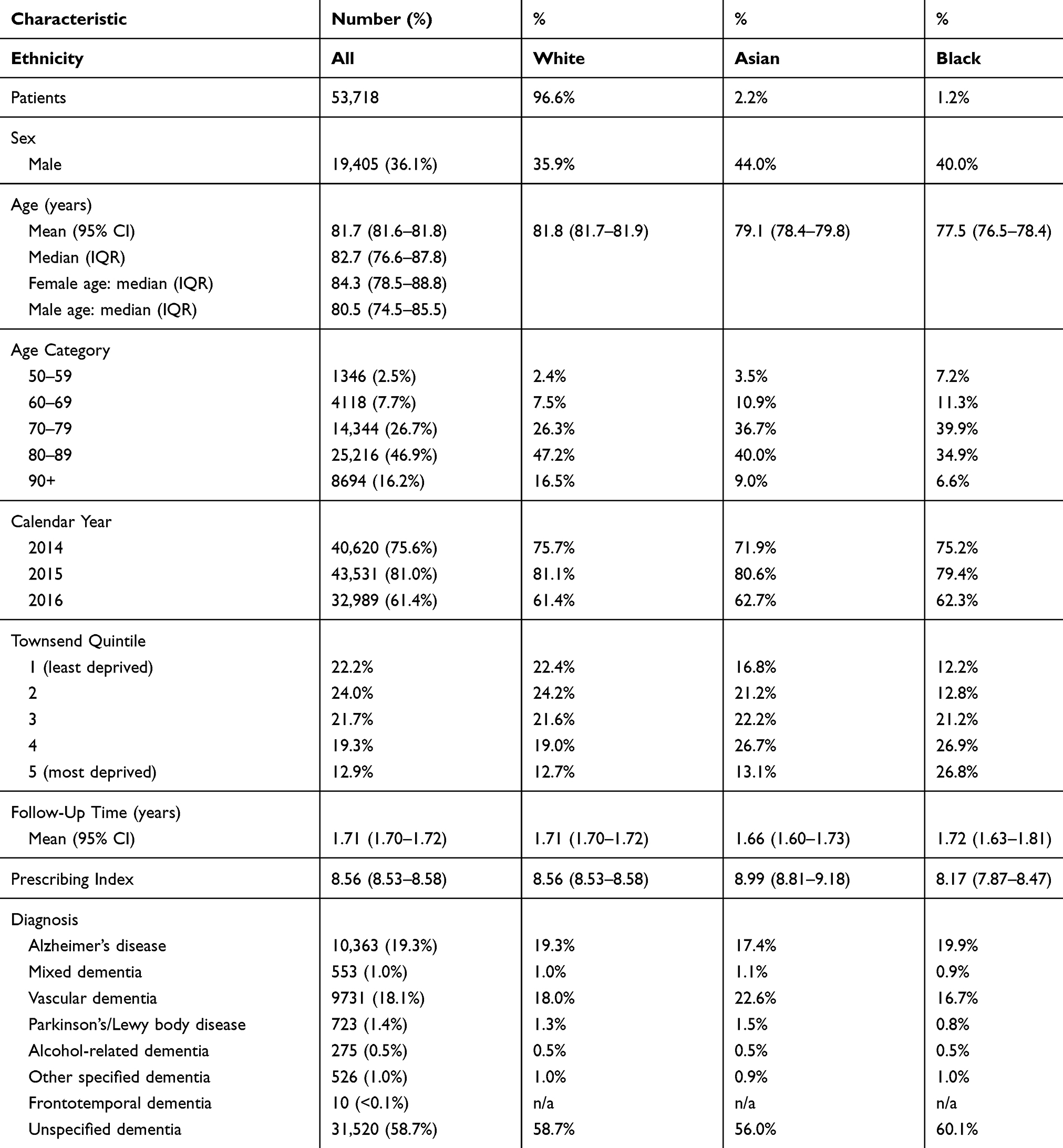 |
Table 1 Participant Characteristics of Cohort of Patients with Dementia, Total and by Each Ethnicity. As Ethnicity and Townsend Score of Social Deprivation Were Imputed and Sample Sizes Should Not Be Reported for Imputed Data, Only Percentages are Reported for Characteristics of Each Ethnicity and for Townsend Score |
Comparing Anti-Dementia Drugs in Dementia Cohort
Among individuals with a dementia diagnosis that did not contraindicate anti-dementia drug prescribing, individuals in the Asian ethnic group were less likely to be prescribed an anti-dementia drug during the study period compared to those in the White ethnic group [adjusted prevalence rate ratio (PRR) 0.86 (95% CI 0.76–0.98)]. Among patients who received an anti-dementia drug during the follow-up period, those in the Asian ethnic group were treated for, on average 15 days less a year than those from the White ethnic group [258 (95% CI 255.6–260.4) compared with 273 days (95% CI 272.7–273.8) per year, respectively]. Neither the likelihood nor duration of prescribing of these drugs differed significantly between Black and White ethnic groups (Tables 2 and 3). When we restricted our analysis to people with any recorded diagnosis of Alzheimer’s disease, mixed dementia, a dementia diagnosis with Parkinson’s disease or Lewy Body dementia (n=11,859), PRR estimates were similar but differences were no longer significant in anti-dementia drug prescribing between White (PRR=1) and Asian [adjusted PRR=0.88 (95% CI 0.70–1.10)] ethnic groups, due to the smaller sample size and wider confidence intervals.
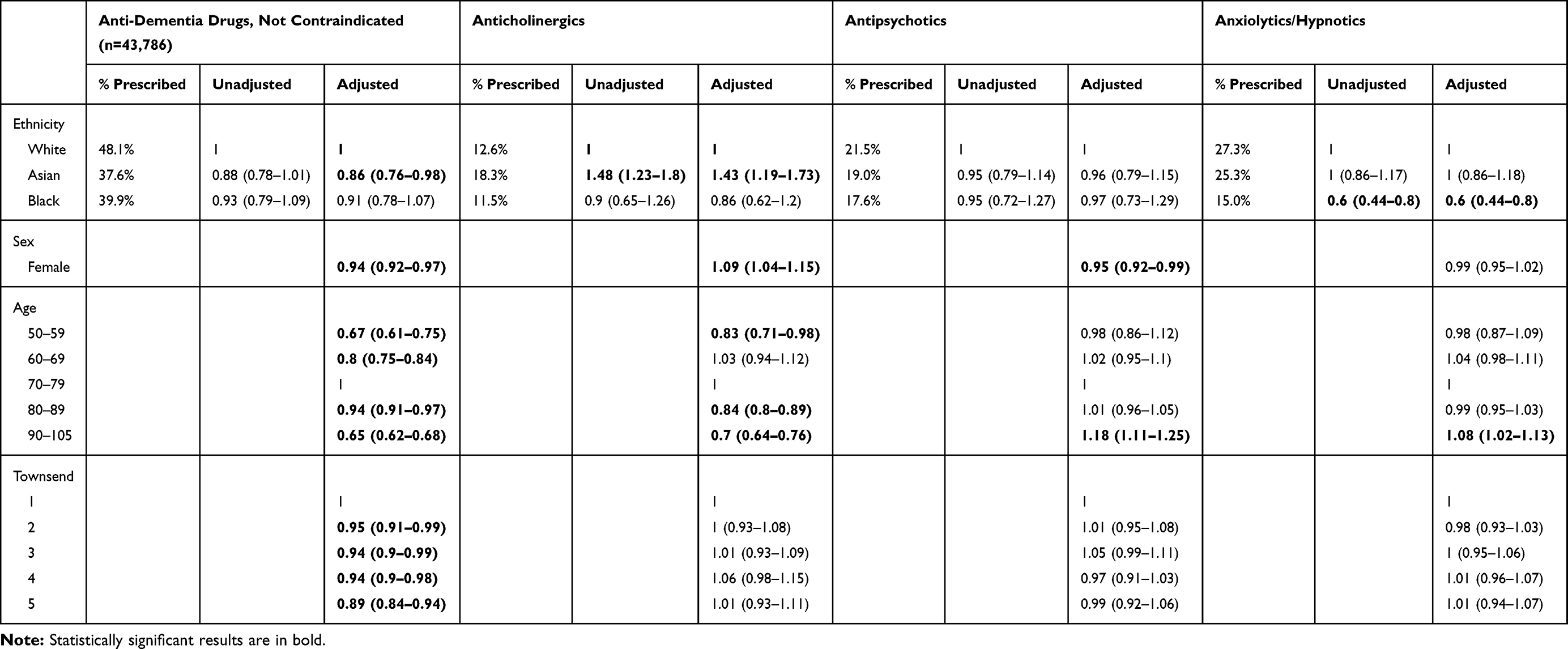 |
Table 2 Prevalence Rate Ratio and 95% Confidence Interval (CI) for Each of the Four Prescribing Outcomes in the Dementia Cohort (n=53,718). Results are Shown for Unadjusted Models and Models Adjusted for the Characteristics Listed |
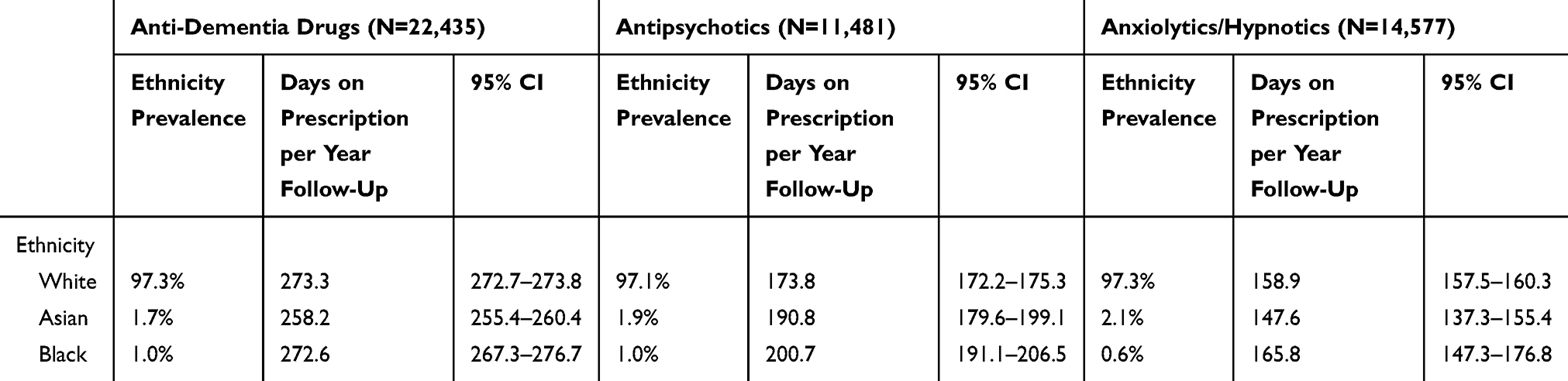 |
Table 3 The Proportion and 95% Confidence Intervals (CI) of Time Spent on a Prescription in a Given Drug Category, in Days (Proportion of Time Multiplied by 365), Over the Time Under Follow-Up, in Years, for Each Ethnicity in the Dementia Cohort |
Comparing Antipsychotic Drugs in Dementia Cohort
There was no significant difference in the likelihood of people with dementia from White, Black or Asian ethnic groups receiving an antipsychotic drug prescription during the follow-up period (Table 2). Patients with a dementia diagnosis in the Black and Asian ethnic groups who received an antipsychotic drug were treated for significantly longer, on average 27 days and 17 days more per year than people in the White ethnic group [200.7 (191.1–206.5), 190.8 (179.6–199.1) and 173.8 (172.2–175.3) respectively] (Table 3).
Comparing Anxiolytic/Hypnotics in Dementia Cohort
Individuals in the Black ethnic group with dementia were less likely to be prescribed anxiolytics or hypnotics than those in the White ethnic group [adjusted PRR 0.60 (95% CI 0.44–0.80)]. The likelihood of being prescribed these drugs did not differ significantly between Asian and White ethnic groups. The duration for which these drugs were prescribed did not differ significantly between the ethnic groups studied (Table 3).
Comparing Anticholinergics in Dementia Cohort
People with dementia in the Asian ethnic group were more likely to be prescribed two or more drugs with an anticholinergic burden in a year than those in the White ethnic group [adjusted PRR of 1.43 (95% CI 1.19–1.73)], while the likelihood of being prescribed two or more of these drugs did not differ significantly between Black and White ethnic groups. The most common anticholinergic drugs prescribed to people with dementia in the Asian and White ethnic groups were risperidone, furosemide, and atenolol; and in the Black group were risperidone, venlafaxine, and furosemide.
Comparing Psychotropics in People Without Dementia
Among older individuals (aged 50+) without dementia, those in the Asian and Black ethnic groups were less likely to be prescribed drugs from anticholinergic, antipsychotic and anxiolytic/hypnotic drug categories, compared to individuals in the White ethnic group (Table 4). For the Black ethnic group, this difference was not significant for antipsychotic drugs in the complete case analysis.
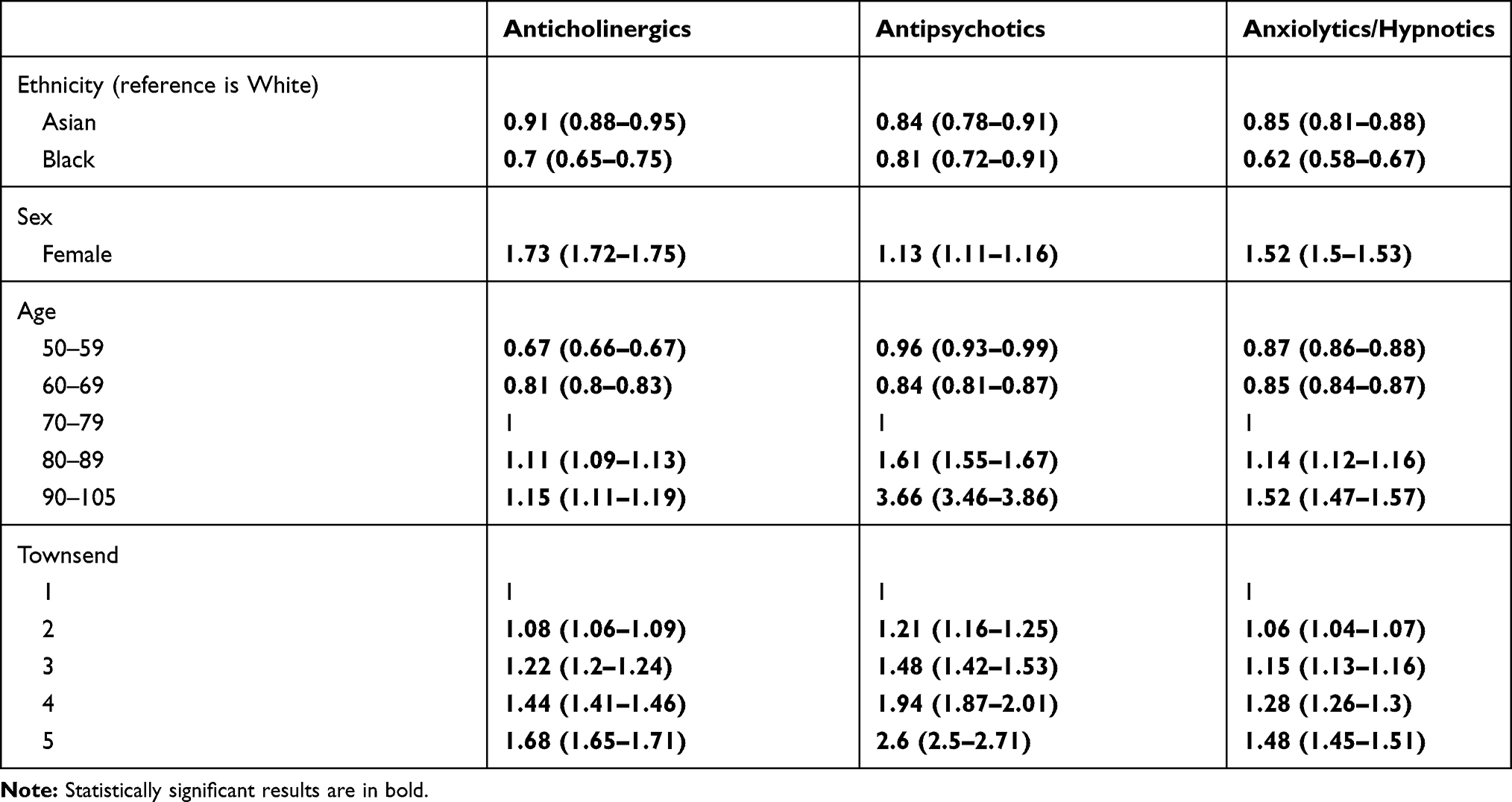 |
Table 4 Prevalence Rate Ratio and 95% Confidence Interval (CI) for the Non-Dementia Cohort Prescribing Outcomes (n=1,648,889). Results are for Models Adjusted for Sex, Age Category, and Townsend Score |
Discussion
Individuals with dementia in the Asian ethnic group were prescribed anti-dementia drugs less, and for less time, compared with other ethnic groups. They were also more likely to be prescribed two or more anticholinergic drugs in a year compared with the White ethnic group. People from Black ethnic groups with dementia were less likely to be initiated on hypnotic and anxiolytic drugs, but took them for a similar duration of time to those from White ethnic groups. People with dementia from White ethnic groups were prescribed less antipsychotic treatment, compared to Black and Asian ethnic groups. In the older (aged 50+) population without a dementia diagnosis, people from minority ethnic groups received fewer prescriptions for the medications studied, compared with the White majority population.
Our finding that Asian people living with dementia received less potentially beneficial symptomatic treatments concords with international studies that have found racial disparities in dementia prescribing. These include a large USA study, in which people from Black and Hispanic ethnic groups were more likely to discontinue anti-dementia medication, relative to people from White ethnic groups.9 In a large Australian care homes study, anti-dementia medication was initiated earlier in residents who spoke English as a first language.8 There are international variations in subsidisation of anti-dementia medications. Few of the people in our dementia cohort would have paid for prescriptions (people aged 60 or over and many below this age experiencing physical health or financial problems are exempt from prescription charges), so medication costs are unlikely to explain the inequalities we found, although the greater socioeconomic disadvantages experienced by minority ethnic groups in the UK may have influenced decisions not to attend appointments where prescribing takes place. In previous qualitative studies, South Asian people living in England have reported barriers to seeking a dementia diagnosis and treatment including: conceptualising dementia as normal ageing or arising from spiritual, psychological, physical or social causes rather than illness; not seeking help because caring for older people was considered a personal or family responsibility, shame and stigma, or a belief that nothing could help; and negative experiences of health services.28,29 Increasing access to UK memory services may be increasing dementia diagnoses rates for minority ethnic groups, as one study showed in London.30 However, referral to a memory service does not necessarily result in appropriate treatment, and services nationally may differ from London, the UK’s most ethnically diverse city. There was also a non-significant trend towards people from Black ethnic groups receiving fewer anti-dementia medications, which may reflect a significant difference that our study lacked power to detect. Alternatively, perhaps while Black people face barriers accessing timely diagnosis, but fewer barriers to receiving good quality post-diagnostic treatment compared to those from Asian groups, for example, fewer linguistic barriers as most are first language English speakers in the UK.
The greater likelihood of people from Asian ethnic groups being prescribed drugs with anticholinergic burden (most commonly risperidone, furosemide, and atenolol) is striking, because among without dementia, people from Asian groups were less likely to be prescribed all the drug classes investigated. These findings may relate to a greater physical or mental health burden in Asian people diagnosed with dementia, who are more frequently diagnosed later when they are mental and physical frail.7,31 The relatively higher Prescribing Index score in Asian compared with White ethnic groups (Table 1) would support this, though we do not know dementia severity in this study. Furosemide and atenolol were among the most commonly prescribed drugs with cholinergic burden, so perhaps greater vascular comorbidity in the Asian group explains their higher rates of anticholinergic drug prescriptions.
The greater duration of antipsychotic prescribing in Black and Asian people with dementia compared with White ethnic groups could indicate a care inequality. This contrasts with a much lower rate, though not duration, of anxiolytic/hypnotic prescribing in the Black population with dementia compared to the White population. Both antipsychotic and anxiolytic/hypnotic drugs are associated with harms. In dementia, antipsychotic medications are more likely to be prescribed for psychosis/agitation, and anxiolytic/hypnotic drugs for agitation/anxiety, with considerable overlap in their usages.32 Perhaps Black people are preferentially prescribed antipsychotics over anxiolytics/hypnotics. The lack of precision in our estimate of anxiolytic/hypnotic prescribing duration in the Black group limits conclusions. We do not know whether the increase in antipsychotic prescribing duration in Black and Asian people with dementia is related to clinically important risks, but we think it merits further explanation and communication of this potential inequality to clinical services. The mean duration of prescribing we found in all ethnic groups exceeded the recommended treatment duration of BPSD (Behavioural and Psychological Symptoms of Dementia) of 6 weeks. A recent Australian care home study similarly indicated that antipsychotics are systematically over-prescribed.33 We did not adjust for or exclude people with serious mental illness, but the rates of antipsychotic prescribing were not higher in Black older people without dementia, suggesting that, as reported in other studies, most antipsychotics prescribed to people with dementia are for behavioural and psychological symptoms of dementia.32
We have previously reported that while men with dementia are more likely to be initiated on a psychotropic medication than women with dementia, women took psychotropic medication for longer. We concluded that there may be a gender inequality in the frequency of review of these medications.17 Perhaps people from Black and Asian ethnic groups are less likely to have their antipsychotic medication reviewed and reduced, even though we have reported elsewhere that Asian people with dementia were as likely as White people with dementia to consult primary care at least once per year, when a medication review could take place (Bhanu C, Jones M, Walters K, Petersen I, Cooper C. Personal communication, July, 2019).
Older people without dementia from Asian and Black groups received fewer psychotropic prescriptions compared to individuals from White ethnic backgrounds. This probably reflects differences in how primary care is accessed between ethnic groups. Most mental disorders are more prevalent in minority ethnic groups compared with the White majority population, probably reflecting greater socioeconomic disadvantage and other risk factors for mental disorder.34 In the English Adult Psychiatric Morbidity Survey, people from minority ethnic groups with common mental disorders were less likely to receive treatments for these disorders, after controlling for level of needs.34
The THIN primary care database comprises around 6% of the UK population, and is broadly representative in terms of demographic and health variables, although patients included in THIN are more likely to live in affluent areas compared with the general population.13 While we think therefore that our sample are broadly representative of people who have a dementia diagnosis, people from Black ethnic groups are less likely to receive a dementia diagnosis.3 Together with our previous paper, our work has identified two barriers to receipt of good quality dementia care: a lesser likelihood of receiving a diagnosis, and of receiving symptomatic treatment if diagnosed. People from Black and Asian groups were less likely to have their ethnicity recorded in THIN than the White majority population, and while we imputed ethnicity, this is a limitation. We reported findings from our multiple imputation analysis as primary results because they included a greater proportion of the cohort and increased precision of results (sample size was increased from 26,394 in a complete case analysis to 53,718 in the multiple imputation analysis of the dementia cohort; the non-dementia cohort similarly increased from 882,993 to 1,648,889). Findings from complete case and multiple imputation analyses were very similar. The only difference was that patients without dementia from Black ethnic backgrounds were less likely to receive antipsychotic prescriptions than patients from the White ethnic group according to the multiple imputation, but not complete case analysis. The high proportion of missing ethnicity data is nonetheless a limitation.
Our primary exposure was self-reported ethnic group. We reported ethnicity as Black, Asian, White, or Mixed/Other because data at more detailed levels were less well recorded. Ethnicity is a complex construct and ideas about how it should be defined have evolved over the past decades. Ethnic groups are considered to be those sharing a common ancestry, culture, historical memories, attachment to a homeland and feeling of solidarity with one another. There is wide variation within minority ethnic groups in country of origin, language, religion, socio-economic power, and experiences, but there is also enough shared culture with regards to family structures, identity and health beliefs to make ethnicity a relevant factor with respect to health behaviours.29 We report prescriptions issued, but do not know whether they were dispensed or taken. Our analyses may have been confounded by unmeasured variables, in particular, the illnesses treated by the drugs prescribed. This applies especially to our analyses of drugs with cholinergic burden, as we did not measure vascular comorbidity directly or control for comorbidity in analyses.
We excluded people with dementia subtype diagnoses for which anti-dementia drugs are contra-indicated (vascular and frontotemporal dementias) but included those with an unspecified dementia subtype in our main analyses. Dementia subtype may be recorded as unspecified because a patient does not want or is unable to attend further investigation, or because subtype is known but not recorded. Though dementia with unspecified subtype is not a more common diagnosis in Black and Asian, compared with White groups, it is possible that due to greater prevalence of cardiovascular illnesses in minority ethnic populations,27 relatively more Black and Asian people with unspecified dementia subtype had vascular dementia. However, if anti-dementia drugs were not being prescribed for this reason, best practice would be to record this in the patient’s records. If Asian people are more likely not to be prescribed anti-dementia medication because the clinician considers vascular dementia is likely but does not record it, this could indicate an inequality in recording and transparency of decision-making, which is also likely to represent an inequality in care quality.
Conclusion
Compared to people from White and Black ethnic backgrounds, people with dementia from Asian backgrounds had a lower likelihood of receiving anti-dementia drugs (symptomatic treatments) where indicated. This adds to the international literature showing that minority ethnic groups consistently receive these treatments less. We do not know whether the increased duration of antipsychotic prescribing in Black and Asian ethnic groups is sufficient to cause harm, but it is concerning and reflects other large studies in the developed world. Campaigns such as Choosing Wisely to reduce antipsychotic prescribing in dementia are not being implemented sufficiently in any ethnic group and there may be ethnic disparities in how they benefit the population. Research is needed to explore how care pathways differ between ethnic groups, and where future campaigns to reduce inequalities should be focused.
Abbreviations
THIN, The Health Improvement Network; UK, United Kingdom.
Data Sharing Statement
Authors that signed a data usage agreement for the dataset had access to the data for this study and have on-going access. The dataset consists of pseudonymized primary care records that are only accessible via password-protected systems to authorized users.
Acknowledgment
We would like to thank our lay advisors.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
Mary Elizabeth Jones reports grants from Dunhill Medical Trust, during the conduct of the study; and has been offered and accepted a position at GlaxoSmithKline, a pharmaceutical company, taken up after this paper’s submission. The company does not manufacture drugs addressed in this submitted work. The authors report no other conflicts of interest in this work.
References
1. Prince M, Bryce R, Albanese E, Wimo A, Ribeiro W, Ferri C. The global prevalence of dementia: a systematic review and metaanalysis. Alzheimer’s Dement J Alzheimer’s Assoc. 2013;9(1):63–75. (). doi:10.1016/j.jalz.2012.11.007
2. House of Commons All-Party Parliamentary Group on Dementia. Dementia Does Not Discriminate. London; 2013. Available from: https://www.alzheimers.org.uk/sites/default/files/migrate/downloads/appg_2013_bame_report.pdf. Accessed January 05, 2020.
3. Pham T, Petersen I, Walters K, et al. Trends in dementia diagnosis rates in UK ethnic groups: analysis of UK primary care data. Clin Epidemiol. 2018;10:949–960. doi:10.2147/CLEP.S152647
4. Prince M, Knapp M, Guerchet M, et al. Dementia UK,
5. Cooper C, Bebbington P, McManus S, et al. The treatment of common mental disorders across age groups: results from the 2007 adult psychiatric morbidity survey. J Affect Disord. 2010;127(1–3):96–101. doi:10.1016/j.jad.2010.04.020
6. Cooper C, Spiers N, Livingston G, et al. Ethnic inequalities in the use of health services for common mental disorders in England. Soc Psychiatry Psychiatr Epidemiol. 2013;48(5):685–692. doi:10.1007/s00127-012-0565-y
7. Cooper C, Tandy A, Balamurali T, Livingston G. A systematic review and meta-analysis of ethnic differences in use of dementia treatment, care, and research. Am J Geriatr Psychiatry. 2010;18(3):193–203. doi:10.1097/JGP.0b013e3181bf9caf
8. Lind KE, Gray LC, Raban MZ, Georgiou A, Westbrook JI. Antidementia medication use by aged care facility residents with dementia. Int J Geriatr Psychiatry. 2019;34(7):1029–1040. doi:10.1002/(ISSN)1099-1166
9. Thorpe CT, Fowler NR, Harrigan K, et al. Racial and ethnic differences in initiation and discontinuation of antidementia drugs by medicare beneficiaries. J Am Geriatr Soc. 2016;64(9):1806–1814. doi:10.1111/jgs.14403
10. Banerjee S. The Use of Antipsychotic Medication for People with Dementia: Time for Action. London; English Department of Health 2009. Available from: https://www.jcpmh.info/wp-content/uploads/time-for-action.pdf. Accessed Janaury 05, 2020.
11. Sura S, Carnahan R, Chen H, Aparasu R. Anticholinergic drugs and health-related quality of life in older adults with dementia. J Am Pharm Assoc. 2015;55(3):282–287. doi:10.1331/JAPhA.2015.14068
12. Vance J. AMDA-choosing wisely. J Am Med Dir Assoc. 2013;14(9):639–641. doi:10.1016/j.jamda.2013.07.004
13. Blak B, Thompson M, Dattani H, Bourke A. Generalisability of The Health Improvement Network (THIN) database: demographics, chronic disease prevalence and mortality rates. Inform Prim Care. 2011;9(4):251–255.
14. Booth N. What are the read codes? Health Libr Rev. 1994;11:177–182. doi:10.1046/j.1365-2532.1994.1130177.x
15. The Kings Fund. General Practice in England: An Overview. London: The Kings Fund; 2009.
16. Townsend P, Phillimore P, Beattie A. Health and Deprivation: Inequality and the North. London: Croom Helm Ltd; 1987.
17. Cooper C, Lodwick R, Walters K, et al. Inequalities in receipt of mental and physical healthcare in people with dementia in the UK. Age Ageing. 2016;46(3):393–400.
18. Maguire A, Blak B, Thompson M. The importance of defining periods of complete mortality reporting for research using automated data from primary care. Pharmacoepidemiol Drug Saf. 2009;18(1):76–83. doi:10.1002/pds.v18:1
19. Horsfall L, Walters K, Petersen I. Identifying periods of acceptable computer usage in primary care research databases. Pharmacoepidemiol Drug Saf. 2013;22(1):64–69. doi:10.1002/pds.v22.1
20. Cai X, Campbell N, Khan B, Callahan C, Boustani M. Long-term anticholinergic use and the aging brain. Alzheimer’s Dement. 2013;9(4):377–385. doi:10.1016/j.jalz.2012.02.005
21. Brilleman S, Salisbury C. Comparing measures of multimorbidity to predict outcomes in primary care: a cross sectional study. Fam Pract. 2013;30(2):172–178. doi:10.1093/fampra/cms060
22. Stovring H, Pottegard A, Hallas J. Determining prescription durations based on the parametric waiting time distribution. Pharmacoepidemiol Drug Saf. 2016;25(12):1451–1459. doi:10.1002/pds.4114
23. Sterne J, White I, Carlin J, et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ. 2009;338:b2393. doi:10.1136/bmj.b2393
24. Rubin D. Inference and missing data. Biometrika. 1976;63:581–592. doi:10.1093/biomet/63.3.581
25. Rubin D. Multiple Imputation for Nonresponse in Surveys. John Wiley & Sons, Inc.; 1987.
26. Barnard J, Rubin D. Small-sample degrees of freedom with multiple imputation. Biometrika. 1999;86:948–955. doi:10.1093/biomet/86.4.948
27. Tillin T, Forouhi N, Jonston D, McKeigue P, Chaturvedi N, Godsland I. Metabolic syndrome and coronary heart disease in South Asians, African-Caribbeans and white Europeans: a UK population-based cross-sectional study. Diabetologia. 2005;48(4):649–656. doi:10.1007/s00125-005-1689-3
28. Berwald S, Roche M, Adelman S, Mukadam N, Livingston G. Black African and Caribbean British communities’ perceptions of memory problems: “We Don’t Do Dementia.”. PLoS One. 2016;11(4):e0151878. doi:10.1371/journal.pone.0151878
29. Mukadam N, Cooper C, Basit B, Livingston G. Why do ethnic elders present later to UK dementia services? A qualitative study. Int Psychogeriatrics. 2011;23(07):1070–1077. doi:10.1017/S1041610211000214
30. Cook L, Mukherjee S, McLachlan T, Shah R, Livingston G, Mukadam N. Parity of access to memory services in London for the BAME population: a cross-sectional study. Aging Ment Heal. 2019;23(6):693–697. doi:10.1080/13607863.2018.1442413
31. Mukadam N, Lewis G, Mueller C, Werbeloff N, Stewart R, Livingston G. Ethnic differences in cognition and age in people diagnosed with dementia: A study of electronic health records in two large mental healthcare providers. Int J Geriatr Psychiatry. 2019;34(3):504–510. doi:10.1002/gps.5046
32. Maust D, Blow F, Wiechers I, Kales H, Marcus S. National trends in antidepressant, benzodiazepine, and other sedative-hypnotic treatment of older adults in psychiatric and primary care. J Clin Psychiatry. 2017;78(4):. doi:10.4088/JCP.16m10713
33. Lind KE, Raban MZ, Georgiou A, Westbrook JI. Duration of antipsychotic medication use by aged care facility residents with dementia. Alzheimer Dis Assoc Disord. 2019;33:331–338. doi:10.1097/WAD.0000000000000336
34. McManus S, Bebbington P, Jenkins R, Brugha T. Mental Health and Wellbeing in England: Adult Psychiatric Morbidity Survey 2014. Leeds; NHS Digital 2016.Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/556596/apms-2014-full-rpt.pdf. Accessed January 05, 2020.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.