Back to Journals » OncoTargets and Therapy » Volume 8
Differences in clinical features between laparoscopy and open resection for primary tumor in patients with stage IV colorectal cancer
Authors Kim IY, Kim BR, Kim HS, Kim Y
Received 30 July 2015
Accepted for publication 21 October 2015
Published 19 November 2015 Volume 2015:8 Pages 3441—3448
DOI https://doi.org/10.2147/OTT.S93420
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Giuseppe Tonini
Ik Yong Kim,1,* Bo Ra Kim,2,* Hyun Soo Kim,2 Young Wan Kim1
1Department of Surgery, Division of Colorectal Surgery, 2Department of Internal Medicine, Division of Gastroenterology, Yonsei University Wonju College of Medicine, Wonju, Gangwon-do, Korea
*These authors contributed equally to this work
Purpose: To identify differences in clinical features between laparoscopy and open resection for primary tumor in patients with stage IV colorectal cancer. We also evaluated short-term and oncologic outcomes after laparoscopy and open surgery.
Methods: A total of 100 consecutive stage IV patients undergoing open (n=61) or laparoscopic (n=39) major resection were analyzed. There were four cases (10%) of conversion to laparotomy in the laparoscopy group.
Results: Pathological T4 tumors (56% vs 26%), primary colon cancers (74% vs 51%), and larger tumor diameter (6 vs 5 cm) were more commonly managed with open surgery. Right colectomy was more common in the open surgery group (39%) and low anterior resection was more common in the laparoscopy group (39%, P=0.002). Hepatic metastases in segments II, III, IVb, V, and VI were more frequently resected with laparoscopy (100%) than with open surgery (56%), although the difference was not statistically significant. In colon and rectal cancers, mean operative time and 30-day complication rates of laparoscopy and open surgery did not differ. In both cancers, mean time to soft diet and length of hospital stay were shorter in the laparoscopy group. Mean time from surgery to chemotherapy commencement was significantly shorter with laparoscopy than with open surgery. In colon and rectal cancers, 2-year cancer-specific and progression-free survival rates were similar between the laparoscopy and open surgery groups.
Conclusion: Based on our findings, laparoscopy can be selected as an initial approach in patients with a primary tumor without adjacent organ invasion and patients without primary tumor-related symptoms. In selected stage IV patients, tumor factors such as primary rectal tumor, peritoneal carcinomatosis, or liver metastasis may not be absolute contraindications for a laparoscopic approach.
Keywords: colorectal neoplasms, laparoscopy, neoplasm metastasis
Introduction
Laparoscopy for colorectal cancer has numerous short-term benefits such as less postoperative pain, shorter hospital stay, and an earlier return to work.1–3 In addition, laparoscopy is as effective as open surgery in terms of oncologic outcomes.4,5 However, information regarding optimal indications for laparoscopy is not readily available in patients with stage IV colorectal cancer, because a metastatic disease is frequently excluded from clinical trials.
Approximately 20%–25% of patients have synchronous metastasis at the initial diagnosis of colorectal cancer.6,7 There are various clinical scenarios regarding optimal first-line treatment in patients with stage IV disease.8,9 Removal of the primary tumor only, synchronous resection of metastatic tumor, or first-line chemotherapy can be considered. The primary tumor should be resected in symptomatic patients, but this method is still controversial in patients without primary tumor-related symptoms.10 Surgeons should determine which is the most appropriate treatment strategy. If a first-line surgery is chosen for primary tumor resection, either laparoscopy or open surgery must be selected.
Several studies have compared outcomes between laparoscopy and open surgery in patients with stage IV disease, and all reported favorable short-term11–18 and comparable oncologic outcomes11–16,18 between the two approaches. However, the clinical features associated with selecting surgical approaches such as laparoscopy or open resection for stage IV disease have not been investigated extensively. We postulated that certain patient or tumor factors are related to selecting surgical approaches and that identifying these factors could offer surgeons objective evidence and allow more patients with stage IV disease to be managed with a laparoscopic approach. This study aimed to identify differences in clinical features between laparoscopy and open resection for primary tumor in patients with stage IV colorectal cancer. We also evaluated short-term and oncologic outcomes after laparoscopy and open surgery.
Methods
Patients
This is a retrospective clinical study at a single tertiary center. The STrengthening the Reporting of OBservational studies in Epidemiology guidelines were used to report this observational study.19 This study was approved by the Institutional Review Board of Wonju Severance Christian Hospital (YWMR-14-5-080). Between March 1, 2007 and December 31, 2012, 100 consecutive patients undergoing primary tumor resection for stage IV colorectal cancer were enrolled. Eligibility criteria included patients with histologically confirmed colorectal cancer who underwent major colorectal resection with or without liver resection. Patients undergoing extra-abdominal organ surgery (eg, pneumonectomy), nonresectional procedures for colorectal cancer, emergent operation, or bypass procedures for colorectal cancer were excluded from this study population.
Study purposes
The primary purpose was to identify differences in clinical features between laparoscopy and open surgery for primary tumor resection in patients with stage IV colorectal cancer. The secondary purpose was to evaluate short-term and oncologic outcomes after laparoscopy and open surgery.
Surgery, chemotherapy, and follow-up
All surgeries were performed by two colorectal surgeons. Type of surgical procedure, either laparoscopic or open, was decided at the surgeon’s discretion. Laparoscopic and open procedures were explained to patients and their families before surgery, and informed consent was obtained from all patients. After standardized preoperative preparation, affected colon and rectal segments were removed based on standard surgical procedures.20,21 Detailed operative procedures are described elsewhere.22 All patients were registered in a prospectively maintained colorectal database after surgery and followed at 3- or 6-month intervals for 5 years and then yearly thereafter.
After recovery from surgery, all stage IV patients were recommended to receive chemotherapy according to the National Comprehensive Cancer Network guidelines.8,9 Chemotherapy regimens included 5-fluorouracil with leucovorin, capecitabine, or oxaliplatin/irrinotecan, or in combination with targeted agents.
Outcome measures
All laparoscopic data were analyzed according to the intention-to-treat principle. Postoperative complications were defined as events that required additional treatment within 30 days of surgery, based on the Clavien–Dindo classification.23 Conversion to open surgery was defined as stopping the laparoscopic approach and using a conventional laparotomy incision to complete the surgical procedure. Treatments requiring admission to an intensive care unit (ICU) or blood transfusions were included when patients needed these interventions within 48 hours after primary surgery. ICU admissions and transfusions due to postoperative complications were not considered.
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 21.0 (IBM, Armonk, NY, USA) and MedCalc Statistical Software, Version 15.2.2 (MedCalc Software bvba, Ostend, Belgium). Categorical variables were described by frequencies and percentages, and were compared by chi-square test or Fisher’s exact tests when appropriate. Continuous variables were described as mean and standard deviation, and were analyzed by Student’s t-test. Survival analysis was performed by the Kaplan–Meier method with log rank tests. P<0.05 was considered statistically significant.
Results
Patient characteristics
A total of 100 consecutive stage IV patients were analyzed based on primary surgical approach of open (n=61) or laparoscopic procedures (n=39). Pathological T4 tumors (56% vs 26%), primary colon cancers (74% vs 51%), and larger tumor diameter (6 vs 5 cm) were more commonly observed in the open surgery group than the laparoscopy group. There were no significant differences in age, sex, American Society of Anesthesiologists (ASA) score, body mass index, and history of previous abdominal surgery between the open and laparoscopy groups.
In terms of operation types, right colectomy was more common in the open surgery group (39%) and low anterior resection was more common in the laparoscopy group (39%, P=0.002). Proportions with liver resection did not differ between the two groups. Although the difference was not statistically significant, hepatic metastases in segments II, III, IVb, V, and VI were more frequently managed with laparoscopy (100%) than with open surgery (56%). There were four cases (10%) of conversion to laparotomy in the laparoscopy group, and all were colon cancer cases. Tumor fixation to adjacent organs (n=3) and thorough irrigation of the abdominal cavity due to a perforated tumor (n=1) were reasons for open conversion. The R0 resection rate was 41% in the laparoscopy group and 26% in the open surgery group (P=0.132). Detailed patient characteristics are presented in Table 1.
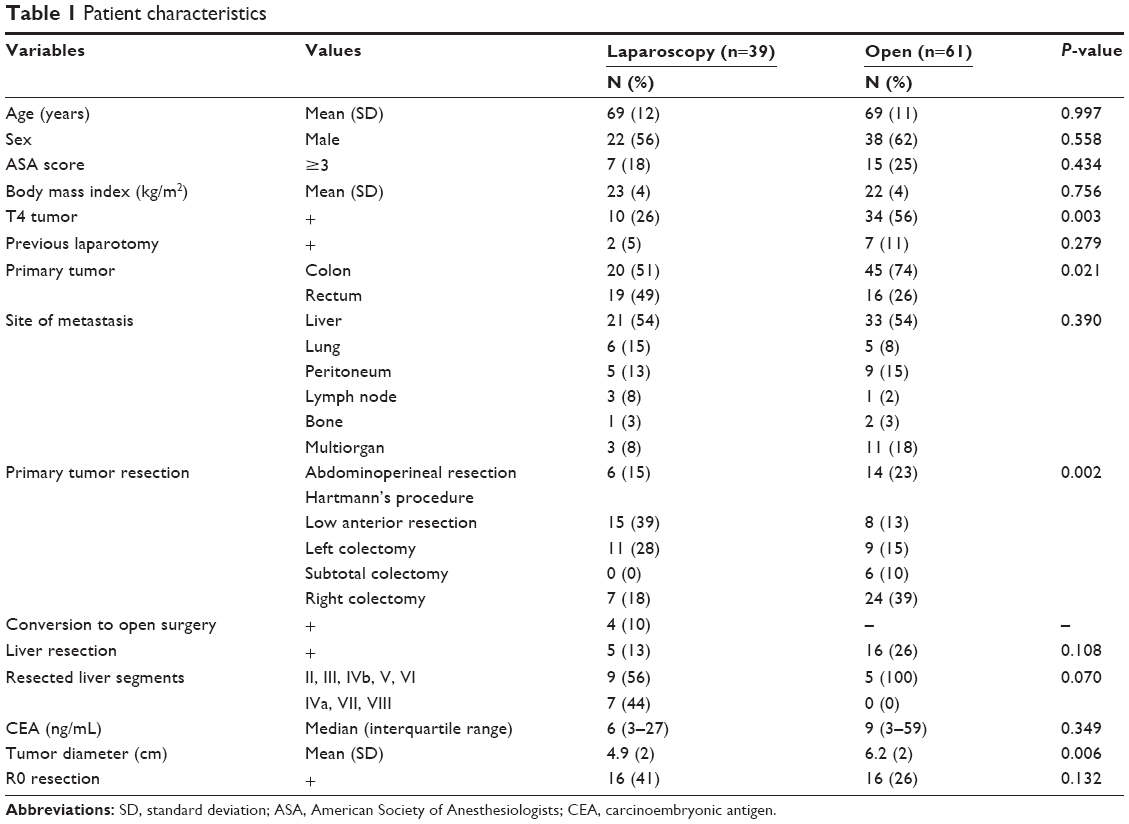 | Table 1 Patient characteristics |
Primary tumor-related symptoms
Asymptomatic patients with colon cancer were more frequently managed with laparoscopy (35% vs 13%, P=0.044). Similarly, asymptomatic patients with rectal cancer were more commonly treated with laparoscopy (37% vs 6%, P=0.032). Obstruction was the most common symptom in both colon and rectal cancer groups (Table 2).
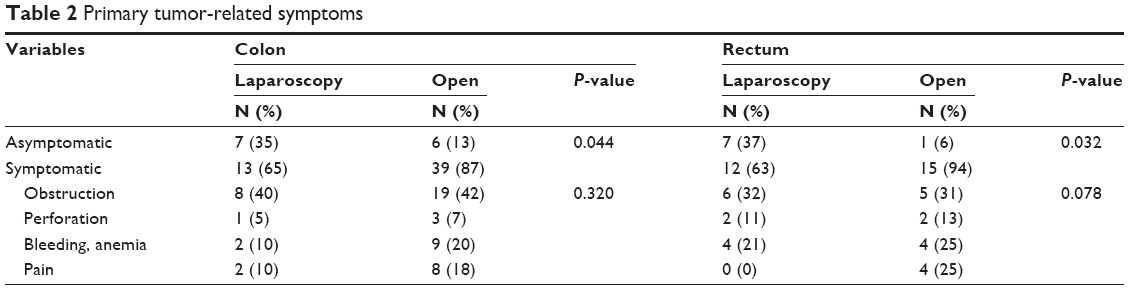 | Table 2 Primary tumor-related symptoms |
Short-term outcomes
In patients with colon cancer, mean operative time (175 vs 174 minutes) and blood loss did not differ between the two groups. There were no differences in 30-day complication rates between laparoscopy (25%) and open surgery (44%) (P=0.779). There was one death from pneumonia in a patient with underlying chronic obstructive pulmonary disease in the open surgery group. ICU admissions (P=0.010) and blood transfusions (P=0.019) were more common in the open surgery group. Time to soft diet (4 vs 6 days, P=0.019) and length of hospital stay (11 vs 17 days, P=0.001) were shorter in the laparoscopy group. The percentages of patients who received chemotherapy were 65% in the laparoscopy group and 64% in the open surgery group (P=0.966). Mean time from surgery to chemotherapy commencement was significantly shorter with laparoscopy (32 days) than with open surgery (40 days, P=0.020).
In patients with rectal cancer, mean operative time (212 vs 225 minutes, P=0.687) and blood loss did not differ between the two groups. There were no differences in 30-day complication rates between laparoscopy (26%) and open surgery (19%) (P=0.595). ICU admission (P=0.013) was more common in the open surgery group. Time to soft diet (4 vs 6 days, P=0.044) and length of hospital stay (10 vs 18 days, P=0.037) were shorter in the laparoscopy group. The percentages of patients who received chemotherapy was 74% in the laparoscopy group and 69% in the open surgery group (P=0.748). Mean time from surgery to chemotherapy commencement was significantly shorter with laparoscopy (29 days) than with open surgery (38 days, P=0.032) (Table 3).
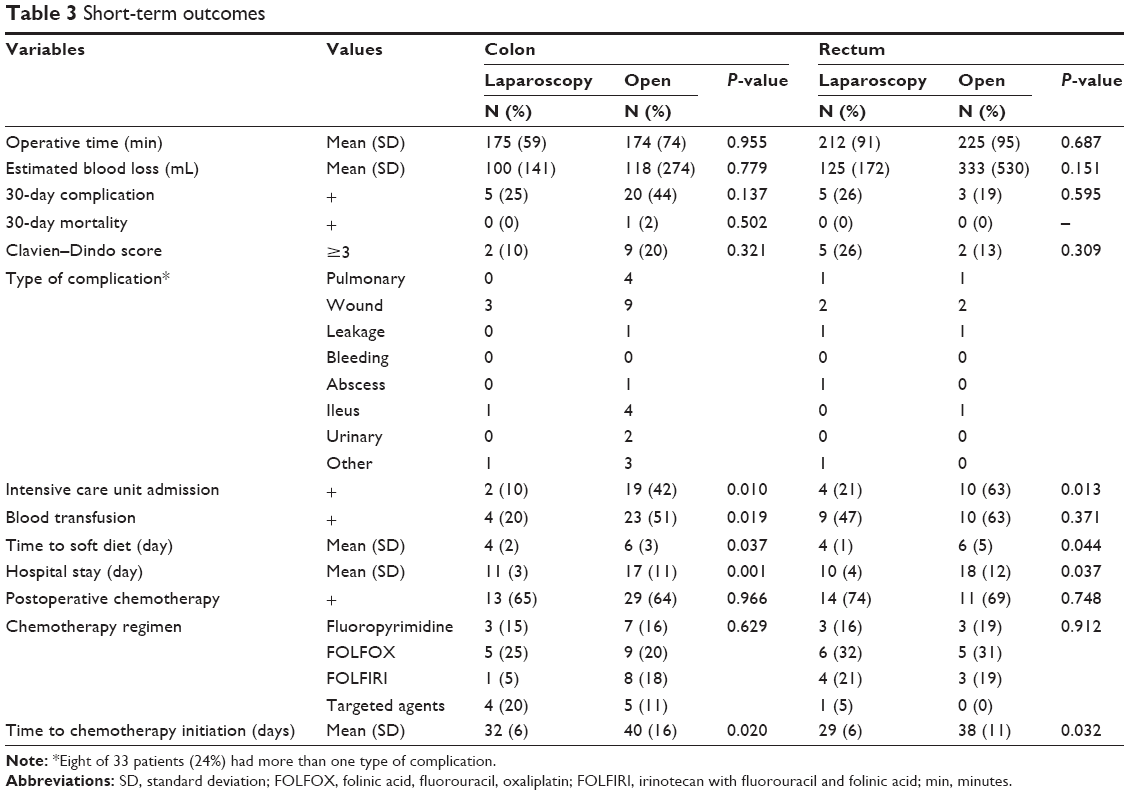 | Table 3 Short-term outcomes |
Oncologic outcomes
Kaplan–Meier survival analysis showed that in patients with colon cancer, 2-year cancer-specific survival rates were 60.8% and 49.8% for the laparoscopy and open surgery groups, respectively (P=0.590). In patients with rectal cancer, 2-year cancer-specific survival rates were 54.9% and 46.9% for the laparoscopy and open surgery groups, respectively (P=0.598) (Figure 1A).
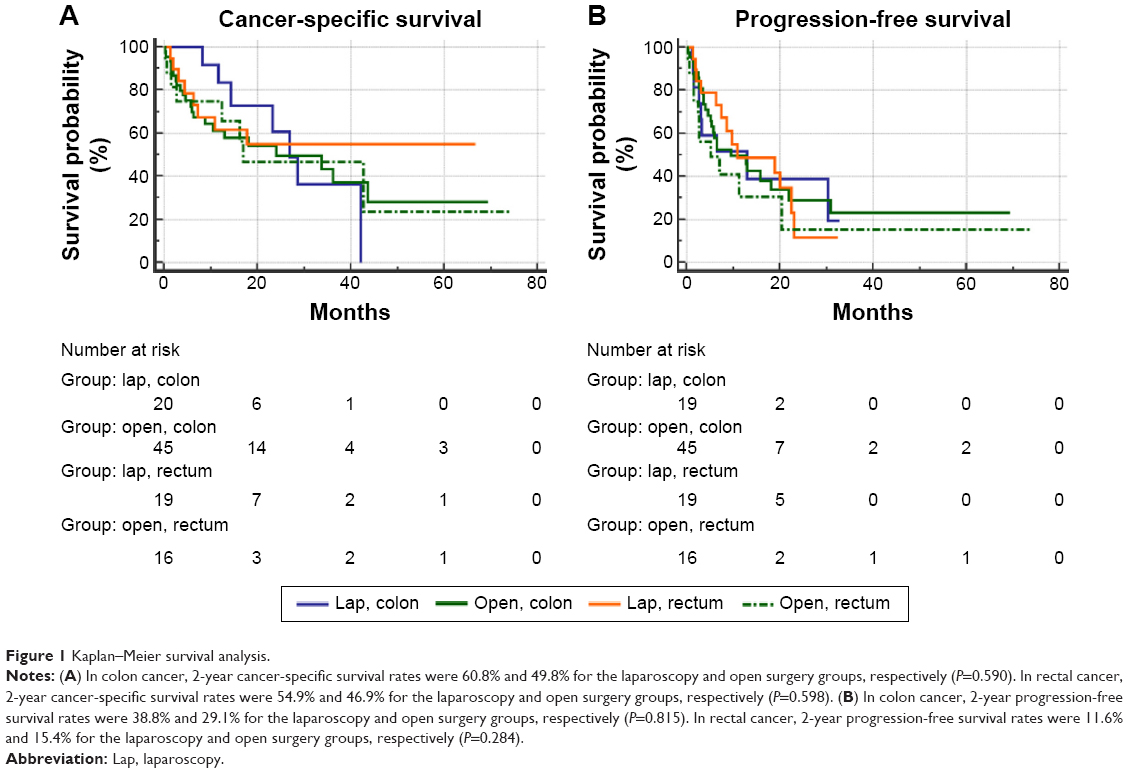 | Figure 1 Kaplan–Meier survival analysis. |
In colon cancer, 2-year progression-free survival rates were 38.8% and 29.1% for the laparoscopy and open surgery groups, respectively (P=0.815). In rectal cancer, 2-year progression-free survival rates were 11.6% and 15.4% for the laparoscopy and open surgery groups, respectively (P=0.284) (Figure 1B).
Discussion
The major finding of this study is that tumor factors such as pathological T4 tumors (56% vs 26%), primary colon cancers (74% vs 51%), and larger tumor diameter (6 vs 5 cm) were related to selecting a surgical approach (open resection) for primary tumor resection. Patients with asymptomatic primary tumor were more frequently managed by laparoscopy (colon cancer: 35% vs 13%, P=0.044 and rectal cancer: 37% vs 6%, P=0.032). Laparoscopy for primary tumor resection was associated with short-term advantages such as less ICU admission, shorter time to soft diet, reduced length of hospital stay, and shorter time from surgery to chemotherapy commencement in patients with both colon and rectal cancers. Cancer-specific and progression-free survival rates were also similar between the laparoscopy and open surgery groups in patients with colon and rectal cancers.
Clinical features
Success of laparoscopy is affected by patient, tumor, and surgeon factors.24 Patient or tumor factors include primary tumor-related symptoms, intra-abdominal adhesion, visceral obesity, comorbidities, and locally advanced tumor. If surgical difficulties are anticipated, surgeons tend to abandon a laparoscopic approach.25 When considering laparoscopic resection for primary tumors in patients with stage IV disease, the choice of laparoscopy or open surgery is largely dependent on the surgeon,11,12,16,18 patient,15 or both.13,14 Objective data regarding laparoscopic indications are lacking. Only one study has described the exclusion of patients with adjacent organ invasion17 (Table 4).
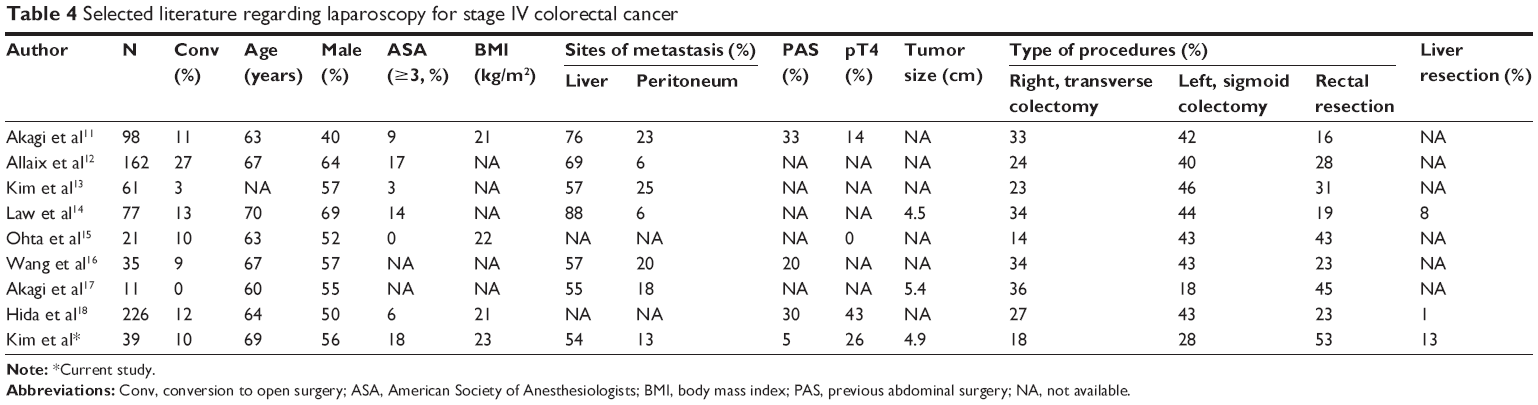 | Table 4 Selected literature regarding laparoscopy for stage IV colorectal cancer |
In our study, difficult surgical situations such as pT4 tumors and larger tumors were more frequently managed with an open surgical approach. The proportion of T4 tumors was 14%11 and 43%18 in previous studies and 26% in our study. Mean tumor size was 4.514 and 5.4 cm17 in earlier studies and 4.9 cm in this study. Rectal resection varied from 16% to 45%11–18 and was 53% in this study. Allaix et al12 reported that primary rectal cancer as well as a bulky tumor increased conversion to laparotomy. In this study, colon cancer (specifically right hemicolectomy) was more commonly managed with an open surgical approach, partly due to difficulties in stenting for proximal colon obstruction. Obstruction was the most common symptom in the open (42%) group. In recent years, most cases can be palliated with colonic stents. However, stenting of proximal colonic lesions is difficult because colonoscopic procedures that reach the proximal obstructing site are more technically demanding.26 In our study, four converted cases were all colon cancers, and the reasons for conversion were tumor fixation to adjacent organs (n=3) and perforated tumor (n=1). This finding indicates that laparoscopic rectal resection can be a reasonable approach for stage IV disease in the absence of tumor fixation. However, this is a retrospective series, and a future prospective study would be valuable for defining clear indications for laparoscopic rectal surgery in stage IV disease.
Patients with asymptomatic primary tumor were more frequently managed by laparoscopy (colon cancer: 35% vs 13% and rectal cancer: 37% vs 6%) in this study. However, Law et al14 reported that rates of laparoscopy (5%) and open surgery (8%) were not different for resecting asymptomatic primary tumor in patients with stage IV colorectal cancer. Kim et al13 also reported that rates of laparoscopy (54%) and open surgery (58%) were not different for patients who had an asymptomatic primary tumor. In terms of patient factors, mean age varied from 60 to 70 years.11,12,14–18 Proportions of male patients were 40%–69%.11–18 The proportion of patients with a high ASA score (3 or higher) ranged from 0% to 17% of study populations11–15,18 and was 18% in this study. Mean body mass index ranged from 21 to 23 kg/m2.11,15,18 Peritoneal carcinomatosis was reported in 6%–25% of cases11–14,16,17 and was present in 13% of cases in this study. Among patients, 20%–30% had a history of prior abdominal surgery in previous studies11,16,18 and only 5% fell in this category among our patients. Laparoscopic liver resection rate varied from 1%18 and 8%14 in previous studies and was 13% in our study. Collectively, these data suggest that patient factors such as higher ASA score (≥3) and a history of prior surgery, and tumor factors such as peritoneal carcinomatosis or liver metastasis may not be absolute contraindications for laparoscopy. We believe that laparoscopic liver resection can be more actively considered in patients with liver metastasis. It is known that segments II, III, IVb, V, or VI metastases are more convenient for a laparoscopic approach than segments IVa, VII, or VIII metastases.27 Indeed, metastatic nodules in segments II, III, IVb, V, or VI were more frequently resected with laparoscopy (100%) compared with open surgery (56%) in our study. Even in patients with segments IVa, VII, or VIII metastases, laparoscopic radiofrequency ablation offers an alternative to resection.
In addition to patient factors, surgeon factors such as level of technical skill and experience are crucial for laparoscopic surgery. The surgeon-dependent factor was controlled in this study, as all laparoscopic and open surgeries were performed by two experienced colorectal surgeons who have extensive experience with both laparoscopic and open surgery.28
Short-term and oncologic outcomes
As expected, laparoscopy was associated with short-term advantages such as less ICU admission, shorter time to soft diet,13,16,17 reduced length of hospital stay,11–18 and shorter time from surgery to chemotherapy commencement in both colon and rectal cancer patients.16 In the current study, the laparoscopy group started chemotherapy 8 days earlier in colon cancer and 9 days earlier in rectal cancer. Wang et al16 observed that mean time to initiate chemotherapy was 3.6 days shorter in their laparoscopy group, but other studies did not find any difference.11,17,18 The postoperative complication rate varied from 9% to 32.8% in previous reports11–18 and was 26% in this study.
Median survival was reported at 16–25.9 months11,14,16,18 and earlier studies demonstrated comparable oncologic outcomes of laparoscopy in stage IV disease.11–16,18 We also observed that cancer-specific and progression-free survival rates of colon and rectal cancers were similar between the laparoscopy and open surgery groups. Interestingly, patients who underwent laparoscopic surgery started chemotherapy 8 (colon cancer) and 9 days (rectal cancer) sooner; however, earlier use of chemotherapy did not influence cancer-specific or progression-free survival.
According to the current National Comprehensive Cancer Network guidelines, resection of a primary tumor is recommended only if patients present with primary tumor-related symptoms such as obstruction, hemorrhage, and perforation.8,9 However, asymptomatic patients can still undergo surgery for primary tumor-induced problems during their chemotherapy courses. In addition, a number of investigators demonstrated that primary tumor resection improved oncologic outcomes.29–31 Thus, there remains controversy regarding which is a better first approach in stage IV patients with asymptomatic primary tumor. In this study, decisions regarding surgery or chemotherapy were made after multidisciplinary team meetings.32 This study is limited because a small number of patients were included and the data were collected retrospectively. Various clinical scenarios such as survival according to the use of chemotherapy or chemotherapy regimens could not be stratified due to the limited study population. In terms of oncologic outcomes, this study has many biases, and definite conclusions could not be drawn. However, this is the first study to investigate factors related to the choice of laparoscopy in patients with stage IV disease.
Conclusion
In summary, laparoscopy can be selected as an initial approach in patients with a primary tumor without adjacent organ invasion, and patients without primary tumor-related symptoms, based on our findings. In selected stage IV patients, tumor factors such as primary rectal tumor, peritoneal carcinomatosis, or liver metastasis may not be absolute contraindications for laparoscopic approach. Laparoscopy for primary tumor resection yielded favorable short-term and similar oncologic outcomes. Further studies in larger cohorts are needed to develop optimal indications for laparoscopy in patients with stage IV colorectal cancer.
Acknowledgment
The authors would like to thank Hyun Jun Kwon for helping them to maintain a colorectal database and perform statistical analyses.
Author contributions
Study concept and design: YWK, IYK, and BRK. Acquisition and interpretation of data: YWK, BRK, and HSK. Drafting of the manuscript: YWK, BRK, and HSK. Critical revision of the manuscript: YWK, IYK, and BRK.
Disclosure
The authors report no conflicts of interest in this work.
References
Veldkamp R, Kuhry E, Hop WC, et al. Laparoscopic surgery versus open surgery for colon cancer: short-term outcomes of a randomised trial. Lancet Oncol. 2005;6(7):477–484. | ||
Guillou PJ, Quirke P, Thorpe H, et al. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre, randomised controlled trial. Lancet. 2005;365(9472):1718–1726. | ||
Clinical Outcomes of Surgical Therapy Study Group. A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med. 2004;350(20):2050–2059. | ||
Bonjer HJ, Deijen CL, Abis GA, et al. A randomized trial of laparoscopic versus open surgery for rectal cancer. N Engl J Med. 2015;372(14):1324–1332. | ||
Jayne DG, Thorpe HC, Copeland J, Quirke P, Brown JM, Guillou PJ. Five-year follow-up of the Medical Research Council CLASICC trial of laparoscopically assisted versus open surgery for colorectal cancer. Br J Surg. 2010;97(11):1638–1645. | ||
Tebbutt NC, Norman AR, Cunningham D, et al. Intestinal complications after chemotherapy for patients with unresected primary colorectal cancer and synchronous metastases. Gut. 2003;52(4):568–573. | ||
Mella J, Biffin A, Radcliffe AG, Stamatakis JD, Steele RJ. Population-based audit of colorectal cancer management in two UK health regions. Colorectal Cancer Working Group, Royal College of Surgeons of England Clinical Epidemiology and Audit Unit. Br J Surg. 1997;84(12):1731–1736. | ||
National Comprehensive Cancer Network. National Comprehensive Cancer Network guidelines, colon cancer (Version 2.2015). Available from: http://www.nccn.org/professionals/physician_gls/pdf/colon.pdf. Accessed May 1, 2015. | ||
National Comprehensive Cancer Network. National Comprehensive Cancer Network guidelines, rectal cancer (Version 2.2015). Available from: http://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf. Accessed May 1, 2015. | ||
Kim YW, Kim IY. The role of surgery for asymptomatic primary tumors in unresectable stage IV colorectal cancer. Ann Coloproctol. 2013;29(2):44–54. | ||
Akagi T, Inomata M, Kitano S, et al. Multicenter study of short- and long-term outcomes of laparoscopic palliative resection for incurable, symptomatic stage IV colorectal cancer in Japan. J Gastrointest Surg. 2013;17(4):776–783. | ||
Allaix ME, Degiuli M, Giraudo G, Marano A, Morino M. Laparoscopic versus open colorectal resections in patients with symptomatic stage IV colorectal cancer. Surg Endosc. 2012;26(9):2609–2616. | ||
Kim JW, Park JW, Park SC, Kim SY, Baek JY, Oh JH. Clinical outcomes of laparoscopic versus open surgery for primary tumor resection in patients with stage IV colorectal cancer with unresectable metastasis. Surg Today. 2015;45(6):752–758. | ||
Law WL, Fan JK, Poon JT, Choi H, Lo OS. Laparoscopic bowel resection in the setting of metastatic colorectal cancer. Ann Surg Oncol. 2008;15(5):1424–1428. | ||
Ohta K, Takemasa I, Uemura M, et al. Laparoscopic surgery for stage IV colorectal cancer. Surg Laparosc Endosc Percutan Tech. 2014;24(2):153–157. | ||
Wang JH, King TM, Chang MC, Hsu CW. Comparison of the feasibility of laparoscopic resection of the primary tumor in patients with stage IV colon cancer with early and advanced disease: the short- and long-term outcomes at a single institution. Surg Today. 2013;43(10):1116–1122. | ||
Akagi T, Inomata M, Etoh T, Yasuda K, Shiraishi N, Kitano S. Laparoscopic versus conventional palliative resection for incurable, symptomatic stage IV colorectal cancer: impact on short-term results. Surg Laparosc Endosc Percutan Tech. 2011;21(3):184–187. | ||
Hida K, Hasegawa S, Kinjo Y, et al. Open versus laparoscopic resection of primary tumor for incurable stage IV colorectal cancer: a large multicenter consecutive patients cohort study. Ann Surg. 2012;255(5):929–934. | ||
von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. | ||
Kim IY, Kim BR, Kim YW. The short-term and oncologic outcomes of laparoscopic versus open surgery for T4 colon cancer. Surg Endosc. Epub 2015 Jun 27. | ||
Kim IY, Kim BR, Kim YW. Outcomes of laparoscopic and open surgery for colorectal cancer in the emergency setting. In Vivo. 2015;29(2):295–300. | ||
Kim YW, Choi EH, Kim IY, Kwon HJ, Ahn SK. The impact of mechanical bowel preparation in elective colorectal surgery: a propensity score matching analysis. Yonsei Med J. 2014;55(5):1273–1280. | ||
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–213. | ||
Kumar AS, Lee SW. Laparoscopy in colorectal surgery. Surg Clin North Am. 2013;93(1):217–230. | ||
Marks JH, Kawun UB, Hamdan W, Marks G. Redefining contraindications to laparoscopic colorectal resection for high-risk patients. Surg Endosc. 2008;22(8):1899–1904. | ||
Jung MK, Park SY, Jeon SW, et al. Factors associated with the long-term outcome of a self-expandable colon stent used for palliation of malignant colorectal obstruction. Surg Endosc. 2010;24(3):525–530. | ||
Winslow E, Hawkins WG. Laparoscopic resection of the liver for cancer. Surg Oncol Clin N Am. 2013;22(1):75–89, vi. | ||
Kim DH, Kim IY, Kim BR, Kim YW. Factors affecting the selection of minimally invasive surgery for stage 0/I colorectal cancer. Int J Surg. 2015;16(Pt A):44–48. | ||
Ferrand F, Malka D, Bourredjem A, et al. Impact of primary tumour resection on survival of patients with colorectal cancer and synchronous metastases treated by chemotherapy: results from the multicenter, randomised trial Federation Francophone de Cancerologie Digestive 9601. Eur J Cancer. 2013;49(1):90–97. | ||
Karoui M, Roudot-Thoraval F, Mesli F, et al. Primary colectomy in patients with stage IV colon cancer and unresectable distant metastases improves overall survival: results of a multicentric study. Dis Colon Rectum. 2011;54(8):930–938. | ||
Venderbosch S, de Wilt JH, Teerenstra S, et al. Prognostic value of resection of primary tumor in patients with stage IV colorectal cancer: retrospective analysis of two randomized studies and a review of the literature. Ann Surg Oncol. 2011;18(12):3252–3260. | ||
Kim IY, Kim BR, Kim YW. Factors affecting use and delay (≥8 weeks) of adjuvant chemotherapy after colorectal cancer surgery and the impact of chemotherapy-use and delay on oncologic outcomes. PLoS One. 2015;10(9):e0138720. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.