Back to Journals » International Journal of General Medicine » Volume 19
Difference in Clinical Features and Risk Factors of Ischemic Stroke Between Young and Elderly Adults: A Retrospective Observation from an Island Population
Authors Li L ![]() , Liu J, Xu Y, Dong J, He S, Dai F, Liu H
, Liu J, Xu Y, Dong J, He S, Dai F, Liu H ![]()
Received 11 December 2025
Accepted for publication 3 March 2026
Published 25 March 2026 Volume 2026:19 585465
DOI https://doi.org/10.2147/IJGM.S585465
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Ling Li,1,2 Jingjing Liu,3 Yiwei Xu,2 Jiaoxuan Dong,2 Songbin He,2 Fangyu Dai,2 Haipeng Liu4– 6
1Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Neurology, Zhoushan Hospital, Wenzhou Medical University, Zhoushan, People’s Republic of China; 3Department of Pulmonary and Critical Care Medicine, General Hospital of Pingmei Shenma Group, Pingdingshan, People’s Republic of China; 4Centre for Technology Transfer, Universidad Santa Paula, Curridabat, San José, Costa Rica; 5National Medical Research Association, Leicester, UK; 6Cardiovascular Analytics Group, Hong Kong SAR, People’s Republic of China
Correspondence: Fangyu Dai, Department of Neurology, Zhoushan Hospital, Wenzhou Medical University, No. 739 Dingshen Road, Lincheng New District, Zhoushan, People’s Republic of China, Email [email protected] Haipeng Liu, Centre for Technology Transfer, Universidad Santa Paula, C123, Ayarco Sur, Curridabat, San José Province, 11803, Costa Rica, Email [email protected]
Purpose: The incidence of ischemic stroke in young adults has been increasing. However, there is a lack of in-depth understanding of relevant clinical features, particularly in specific geographic and climatic settings. This study aimed to comprehensively investigate the clinical features, including etiology and characteristics, of ischemic stroke in young adults compared with elderly patients from an island population characterized by a subtropical monsoon climate.
Patients and Methods: A total of 1,010 patients with ischemic stroke were included and divided into a young group (454 patients, aged 18– 50 years) and an elderly group (556 patients, aged > 50 years). Clinical and radiological data were collected and compared between the two groups. Continuous and categorical variables were compared using the t-test (or non-parametric tests) and chi-square test, respectively. Binary logistic regression analyses were used to investigate differences between the two groups.
Results: Body mass index, leukocyte count, lymphocyte count, uric acid, and triglyceride levels were higher in the young group than in the elderly group, whereas vitamin B12 levels were lower. In addition, the proportions of cardiogenic embolism, other etiologies and unexplained strokes, and infarcts in the basal ganglia region were significantly higher in the young group. These results suggest age-related differences in clinical characteristics within this island study population.
Conclusion: High body mass index, leukocyte count, uric acid, triglyceride levels, and low vitamin B12 levels are associated with ischemic stroke in young adults. Young adult patients had a higher prevalence of basal ganglia infarction, with a different subtype distribution from elderly patients. These findings highlight the importance of considering geographic specificity and age-related differences when developing stroke prevention and management strategies, formulating public health policies, and allocating medical resources for ischemic stroke.
Keywords: ischemic stroke, young adults, cardioembolism, island population, clinical features
Introduction
Stroke is a significant global health challenge, affecting over 15 million individuals annually, with a one-third fatality rate and two-thirds left with disabilities.1 Cerebral infarction, or ischemic stroke, caused by a blockage in a blood vessel in the brain, accounts for approximately 87% of strokes.2 10–14% of ischemic stroke cases occur in individuals under 50, which is referred to as young strokes.3–5 The incidence of ischemic stroke in young adults (18–50 years old)6 has increased from 6.6 to 11.4 cases per 100,000 persons per year, generating a new public health concern.6–8 Although young individuals have a higher likelihood of surviving strokes, the aftermath often includes emotional, social, or physical sequelae that affect their quality of life.9,10 Stroke can be a devastating experience for young adults and their families due to prolonged disability, frequent caregiving, exposure to comorbidities, and severe socioeconomic consequences for those with decades of life expectancy.5
The etiology of strokes in young adults presents geographical variability with greater heterogeneity than in older patients.4 The Trial of ORG 10172 in Acute Stroke Treatment (TOAST) categorizes ischemic stroke causes into five groups, i.e., large-artery atherosclerosis, small vessel occlusion, cardioembolism, stroke of other determined etiology, and stroke of undetermined etiology.11 In young stroke patients, cardioembolism and other determined causes are more prevalent, while strokes attributed to large or small vessel disease are uncommon.12 Despite recent advancements in diagnostic and management techniques, about one-third of cases remain unexplained, leading to a diagnosis of cryptogenic ischemic stroke.13 The unclear etiology remains a significant challenge for young patients and clinicians.14 Accurate classification of stroke, which plays a crucial role in guiding intervention and management, is an unmet need in young adults and warrants more investigation, especially in geographically distinct populations.
The prevention of stroke depends on early identification of emerging risk factors. Several stroke risk factors have been identified, including diabetes mellitus, hypertension, heart disease, current smoking, chronic heavy alcohol consumption, dyslipidemia, and low physical activity, particularly among young adults.4,8,15 These modifiable factors not only correlate with long-term mortality in young ischemic stroke patients but also contribute substantially (80%) to the overall causative factors in this demographic.8,16 Meanwhile, the etiology and risk factors for stroke in young adults diverge from those observed in their older counterparts. In contrast to older adults, standard cardiovascular risk factors and large- or small-vessel disease play a less prominent role in young adult stroke cases.16 Protein Z, a vitamin K-dependent glycoprotein essential to the coagulation process, has been linked to an increased risk of thrombotic events when deficient, potentially contributing to the prevalence of cryptogenic strokes in young adults.17 Despite the identified risk factors, considering the geographical variability, some researchers have reported region-specific results of etiology and risk factors of stroke in young adults, which warrants more observations from diverse geographic regions.18 Marked differences in stroke risk factors have been observed across age groups and geographic regions. However, ethnoracial background, socioeconomic factors, geography, and climate are often interrelated, and the mechanisms linking these contextual factors to stroke risk remain incompletely understood, particularly across different age groups.19,20 Evidence from island populations is limited, and the potential contribution of regional and climatic context to age-related stroke patterns has not been sufficiently clarified.
To address this gap, this study aimed to compare the clinical, laboratory, and imaging characteristics of ischemic stroke in young adults with those in elderly patients in an island setting. In addition to conventional risk-factor comparisons, we further assessed whether young adults exhibited distinct distributions of etiological subtypes and infarct patterns compared with elderly patients. We hypothesized that young adults would present a different etiological and risk-related profile from elderly patients in this regional context. The results may provide region-specific insights into ischemic stroke in young adults and may inform age-targeted prevention and management strategies.
Materials and Methods
General Information
This study was approved by the Ethics Committee of Zhoushan Hospital (No. 20240031). Due to its retrospective nature, the requirement for informed consent was waived. Zhoushan Hospital is the only national advanced stroke center in Zhoushan, China, serving the Zhoushan Archipelago, which comprises over 1,000 islands. Most patients with stroke from these islands receive treatment at Zhoushan Hospital. This was a retrospective, single-center observational study. Consecutive patients with ischemic stroke admitted to Zhoushan Hospital between September 2016 and February 2023 were reviewed retrospectively. Electronic medical records for research purposes were accessed on April 1, 2024. All potentially identifiable patient information was removed before statistical analysis to ensure confidentiality and compliance with human participant requirements.
After ethical approval, data were extracted in a standardized manner by two neurologists according to predefined inclusion and exclusion criteria. The inclusion criteria were a diagnosis of acute ischemic stroke by cranial computed tomography (CT) or magnetic resonance imaging (MRI), and age 18 years or older with no history of stroke. The exclusion criteria were severe disorders of consciousness, transient ischemic attack, hemorrhagic stroke, subarachnoid hemorrhage, intracranial infection, intracranial hemorrhage, intracranial tumors, traumatic injuries, or neurodegenerative disorders; cardiac, hepatic, or renal insufficiency; hematological disorders or malignant neoplasm; pulmonary infections; and lower-extremity venous thrombosis. For the elderly group, eligible patients were selected by simple random sampling from the remaining pool. Patients with incomplete clinical information were excluded during screening.
Etiology Classification
The diagnosis of ischemic stroke was based on the presence of focal neurological deficits that had lasted for at least 24 hours, regardless of whether a corresponding ischemic lesion was evident on brain imaging. To further support the diagnosis and accurately categorize ischemic stroke types, we systematically reviewed all available imaging reports, blood laboratory examination results, and other clinical recordings in the stroke unit. We used the TOAST classification to determine the etiology of stroke and categorized strokes into distinct types.11 TOAST etiological classification was independently performed by two senior attending neurologists trained in stroke etiological assessment, with assessors blinded to age-group assignment during assessment. Disagreements were resolved by a senior chief neurologist to reach the final classification.
Clinical Data, Blood Tests and Radiological Indicators
Clinical data were collected systematically for all subjects, including sex, age, smoking history, alcohol consumption history, body mass index (BMI), hypertension, diabetes mellitus, history of atrial fibrillation, and admission scores on the National Institutes of Health Stroke Scale (NIHSS) and modified Rankin Scale (mRS). A comprehensive evaluation, including neurological assessment, cardiological assessment, electrocardiography (ECG), and laboratory testing, was performed after admission. Fasting blood samples were collected in the morning of the second hospital day. Hematological and biochemical variables included leukocyte, neutrophil, lymphocyte, and platelet counts, as well as total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), uric acid, fibrinogen, vitamin B12 (VB12), folic acid, and homocysteine.
Upon admission, all patients underwent comprehensive cranial CT and/or MRI to determine stroke location, including the lobes, basal ganglia, brainstem, corona radiata, cerebellum, thalamus, centrum semiovale, corpus callosum, and multiple regions; some patients were negative on MRI/CT scans. The hemorrhagic transformation (HT) following the infarction was also identified on CT/MRI images. Most patients underwent carotid CT angiography or carotid and vertebral artery ultrasonography. Some patients underwent cranial CT perfusion imaging with symptom onset within 24 hours. For patients with suspected cardiogenic embolism, additional Doppler ultrasound examinations were performed. Patients with undetermined etiology underwent a comprehensive evaluation tailored to their specific clinical condition, to the extent that conditions permitted. Radiological variables were extracted from the imaging database using a predefined data collection form.
Statistical Analysis
Data were analyzed using SPSS 26.0 software (IBM, USA). Quantitative variables with normal distribution are presented as mean ± standard deviation (SD), and between-group comparisons were performed using the independent-samples t-test. Quantitative variables with skewed distribution are presented as median and interquartile range (IQR), and between-group comparisons were performed using the Mann–Whitney U-test. Categorical variables are presented as counts and percentages [n (%)], and comparisons were performed using the χ2-test. Variables with statistical significance in univariate analyses were entered into a multivariable binary logistic regression model to identify factors associated with the young-age group among patients with ischemic stroke. Results from the logistic regression are presented as odds ratios (OR) with 95% confidence intervals (95% CI) to assess the strength and precision of the associations. Significant difference was defined as p < 0.05.
Results
Patient Characteristics
A total of 572 young patients with ischemic stroke were enrolled during the study period. In these patients, 14 had a history of ischemic stroke, 72 had various comorbidities, and 32 had incomplete data, which were all excluded. Finally, 454 young patients were included in the final analysis. For the elderly group, out of an initial 6,714 ischemic stroke patients, 467 had a history of ischemic stroke, and 2,531 were excluded due to multiple comorbidities. From the remaining 3,716 patients, 600 were randomly selected. After excluding 44 patients with incomplete clinical information, 556 elderly patients were finally included. The patient screening process is shown in Figure 1.
 |
Figure 1 Flowchart of the patient screening process. |
The young adult group had a mean age of 44.17±5.67 years, while the elderly group had a mean age of 60.66±7.06 years. The NIHSS and mRS scores were lower in the younger group compared to the elderly group. In univariate analyses, the younger group had higher rates of smoking and drinking, higher BMI, and higher levels of leukocytes, lymphocytes, platelets, uric acid, and TG. The prevalence of hypertension, diabetes, and atrial fibrillation was significantly lower in the younger group, as were the levels of HDL-C and VB12, compared to the elderly group (p < 0.05). There were no significant differences between the two groups in the proportion of male patients or in HT, neutrophils, TC, LDL-C, fibrinogen, folic acid, and homocysteine levels (Table 1).
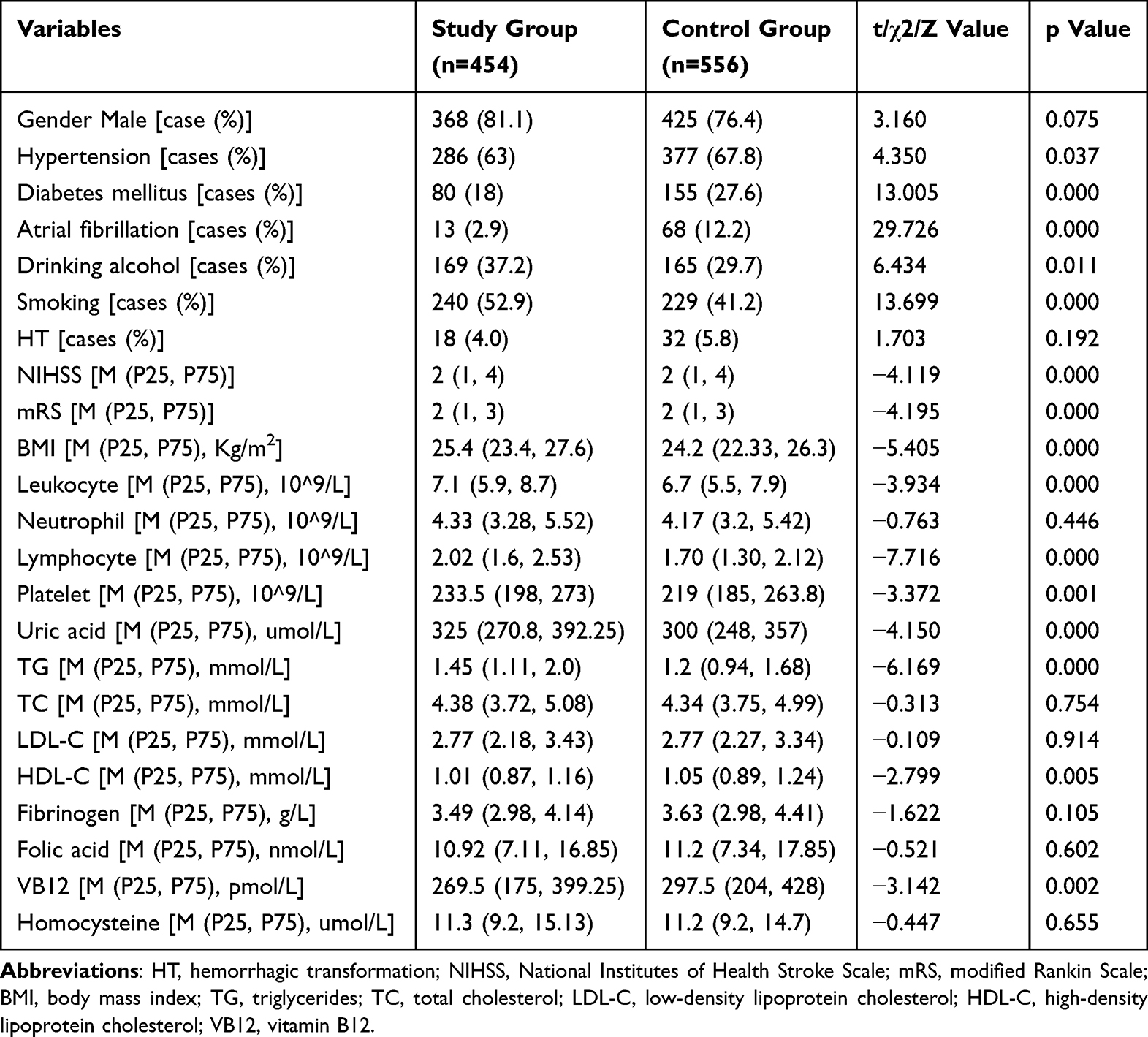 |
Table 1 Data Characteristics of the Two Groups of Subjects |
Factors Associated with Young Age Among Patients with Ischemic Stroke
Binary logistic regression analyses were performed using the significant variables from the univariate analyses as independent variables. The results (Table 2) showed that higher BMI, leukocyte count, lymphocyte count, uric acid, and TG levels, as well as lower VB12 levels, were associated with being in the young group among patients with ischemic stroke. Additionally, the prevalence of atrial fibrillation and diabetes mellitus was low in the young group.
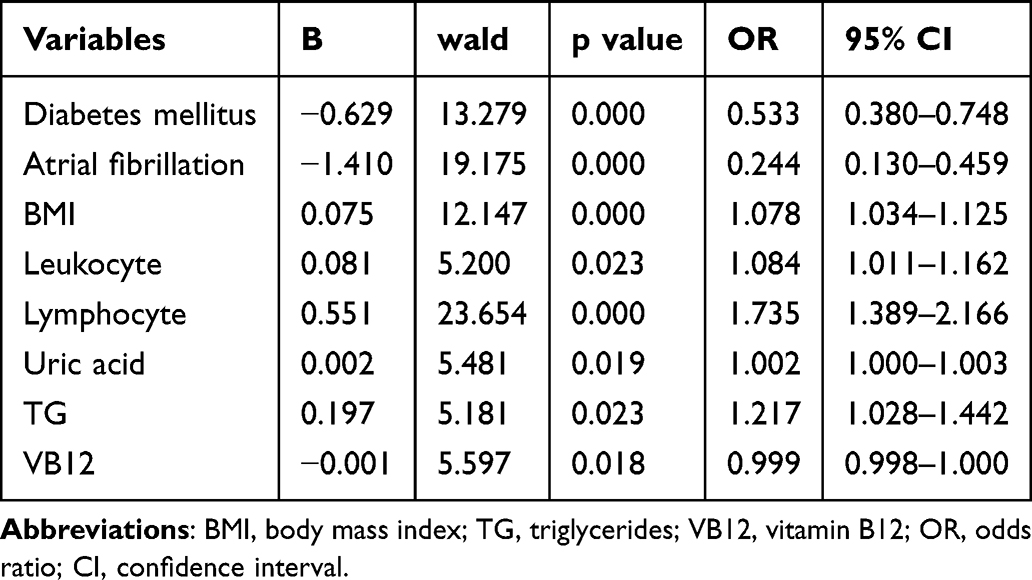 |
Table 2 Factors Associated with Young Age Among Patients with Ischemic Stroke |
Etiologic Characteristics
Figure 2 displays the etiological characteristics of stroke in both groups. The percentage of patients with cardiogenic embolism, other etiologies, and unknown causes was significantly higher in the young group. The differences were statistically significant (p < 0.05).
 |
Figure 2 The Trial of ORG 10172 in Acute Stroke Treatment (TOAST) typing of patients in the two groups. |
Ischemic Stroke Region
The two groups were similar in the proportions of most stroke regions (difference within ±3.5%) except for those of the basal ganglia region and multiple regions, where the younger group was much higher (18.9% vs. 11.9%) and lower (26.9% vs. 33.8%) than the elderly group, respectively (Figure 3).
 |
Figure 3 Ischemic stroke regions in the two groups. |
In young patients with basal ganglia infarction, large vessel occlusion and perfusion abnormalities were uncommon on carotid CT angiography and perfusion images, respectively (Figure 4a–d). In comparison, stenosis in large arteries was observed in some elderly patients with basal ganglia infarction, despite non-significant perfusion abnormalities (Figure 4e–h). Multi-region infarction was most common in the elderly group, where significant narrowing or occlusion in large vessels and perfusion abnormalities were observed (Figure 4i–l).
 |
Figure 4 Three-dimensional angiography, perfusion imaging, and magnetic resonance imaging in different ischemic stroke cases. Case 1 (a–d): A 48-year-old male patient with basal ganglia infarction. (a) Three-dimensional computed tomography angiography (CTA); (b) time-to-maximum (Tmax) perfusion map; (c) cerebral blood flow (CBF) map; (d) diffusion-weighted imaging (DWI) showing basal ganglia infarction (arrow). Case 2 (e–h): A 72-year-old male patient with basal ganglia infarction and ipsilateral middle cerebral artery stenosis. (e) CTA showing ipsilateral middle cerebral artery stenosis (arrow); (f) Tmax perfusion map; (g) CBF map; (h) DWI showing basal ganglia infarction (arrow). Case 3 (i–l): A 59-year-old female patient with multi-regional infarction and middle cerebral artery occlusion, accompanied by hemorrhagic transformation. (i) CTA showing middle cerebral artery occlusion (arrow); (j) Tmax perfusion map; (k) CBF map; (l) DWI showing multi-regional infarction with hemorrhagic transformation (arrow). |
Discussion
Summary of Results and the Significance
This study showed that clinical characteristics differ between young and older patients with ischemic stroke in an island population. Young individuals are at a higher risk of recurrent ischemic stroke and mortality, which has often been attributed to non-atherosclerotic arterial disease, rare genetic factors, and other uncommon causes.6,8 Regional disparities in stroke prevention and management strategies are substantial. In low-income countries there are critical resource gaps among different regions and populations. Even in high-income countries, stroke epidemiology and outcomes vary by race, ethnicity, and geography.19,21 Risk profiles for ischemic stroke in young adults also show marked heterogeneity across regions and ethnoracial groups, highlighting the need for improvement in stroke prevention and management strategies in low- and middle-income countries.20 Region-specific epidemiological patterns of ischemic stroke are critical for public health decision-making.22 Patient characteristics and care pathways for ischemic stroke vary across island and coastal regions where primary and secondary prevention practices are not uniform.22 Studies from southern coastal cities in China with a subtropical marine monsoon climate have reported that high temperatures during hot months may trigger first-ever stroke, and low atmospheric pressure may exacerbate the effect.23 The Zhoushan Archipelago is characterized by a subtropical monsoon climate and geographically dispersed islands. The specific lifestyle patterns, healthcare accessibility, and referral pathways may jointly influence age-stratified stroke presentations in this island population. Our findings may provide evidence to support region-specific, age-stratified prevention and management strategies towards better outcomes of ischemic stroke.
New Findings on Potential Risk Factors of Ischemic Stroke in Young Adults
Our findings indicate that conventional stroke risk factors, including diabetes mellitus and atrial fibrillation, were also observed among young patients with ischemic stroke, albeit with a lower prevalence than in older cohorts.6,24 This study and previous studies suggest potential associations between lifestyle factors (eg., alcohol consumption and smoking) and stroke in younger individuals.8,25 Additionally, we observed higher BMI in young adults with ischemic stroke, highlighting the growing concern of obesity as a global health risk.26,27 Consistent with prior research, our study also indicates that high triglycerides might be associated with ischemic stroke in young adults.28 In island regions, these findings highlight the importance of addressing lifestyle factors, including diet, alcohol consumption, physical activity, obesity, and lipid management, for the primary prevention of stroke in young patients.
The young group showed significantly higher uric acid levels compared to the older group. Previous studies have shown that high uric acid levels are a risk factor for patients experiencing acute ischemic stroke, with associations established with poor prognosis, future vascular events, and stroke recurrence.29–31 A cross-sectional study found high uric acid levels to be a risk factor for major stroke in young patients in highland areas.32 A retrospective study found that young adults with an elevated serum uric acid to serum creatinine ratio had an increased risk of ischemic stroke recurrence.33 There are potential associations between uric acid and inflammatory factors, increased reactive oxygen species production, as well as heightened oxidative stress.34 However, it is important to note that the relationship between uric acid and ischemic stroke is still uncertain. Several studies have reported that higher uric acid levels may be associated with less severe neurological deficits and better clinical outcomes after ischemic stroke.35,36 Therefore, additional prospective studies are warranted to clarify the complex relationship between uric acid and ischemic stroke in young adults, particularly in island populations.
Inflammation is a crucial factor in all stages of stroke. We observed a significant increase in leukocyte counts in the young group compared to the older group. It is worth noting that high leukocyte count upon admission has been linked to poor outcomes during hospitalization in patients with acute cerebral infarction.37 An observational cohort study identified a significant correlation between elevated leukocyte counts and the prevalence of vascular disease, its associated risk factors, and the severity of ischemic stroke in young patients.38 Conversely, decreased lymphocyte counts are frequently observed in patients with acute ischemic stroke.39 We observed that the young group had higher lymphocyte counts compared to the older group. Lymphocytes play a key role in the inflammatory response, regulating the exacerbated inflammatory process. Lower lymphocyte counts are associated with clinical neurological dysfunction and have a negative impact on long-term functional recovery.39–41 A retrospective study observed an increase in peripheral circulating neutrophil counts and a corresponding decrease in lymphocyte counts following ischemic stroke.42 Our findings indicate that the decline in lymphocyte counts may be less severe in young patients, possibly due to milder neurological deficits at the time of hospital admission.43
We observed a stronger association between low VB12 levels and ischemic stroke in young adults compared to older adults. VB12 deficiency has been identified as a significant risk factor for ischemic stroke,44 although the underlying mechanisms remain unclear.44,45 It has been proposed that intestinal dysbiosis associated with VB12 deficiency may be linked to immune dysfunction, which could potentially contribute to stroke severity and clinical outcomes.45 As suggested by previous studies, screening for VB12 levels, adopting healthy lifestyles, and correcting VB12 deficiency when appropriate may contribute to stroke risk reduction in young adults.46 Further studies are warranted to clarify the underlying mechanisms and to develop targeted preventive and therapeutic strategies for young patients with ischemic stroke.
Stroke in young individuals is an unexpected event with a more diverse etiology than in the older population.47 We observed that the young group showed a higher prevalence of cardiogenic embolism, other identifiable causes, or unknown causes than in the older population, which is consistent with previous studies.12 Imaging features play a crucial role in understanding the characteristics of ischemic stroke. Our results revealed a unique imaging pattern, ie., a higher proportion of strokes in the basal ganglia region in the young group, despite the similar prevalence of hypertension in both groups. The basal ganglia are highly susceptible to ischemic events, possibly due to their complex vascular anatomy and intricate network of small vessels. This vulnerability has been consistently observed in previous studies.48,49 Meanwhile, in the elderly group, we observed more multi-regional infarctions and stenosis in large arteries, which is potentially associated with the long-term development of atherosclerosis in cerebral arteries.
For the age-related stroke features observed in island populations, clinical practice may consider region- and population-structure–adapted management pathways, including strengthened public education on stroke symptoms and promotion of timely medical attention, particularly in areas with limited transportation and constrained inter-island transfer capacity.50 Based on the present findings, developing individualized strategies that account for regional context and age-related factors may help improve stroke outcomes.
Limitations and Future Directions
There are some limitations in this preliminary study. Firstly, it was a retrospective study conducted at a single center with a relatively small number of patients. Inaccurate or incomplete case identification may exist and lead to bias in patient selection. Second, given the cross-sectional observational design, the findings reflect age-related differences in factors associated with ischemic stroke, and causal relationships between these factors and young-onset stroke cannot be established. Furthermore, it is possible that some cases with undetermined etiology could be reclassified but limited by the means of observation. Although the elderly cohort was randomly sampled, the two age groups were not fully matched and the differences in residential distribution and healthcare accessibility may still have introduced selection bias and residual confounding. To validate these findings, further elucidate the underlying mechanisms, and develop tailored clinical guidelines and public health strategies, prospective multicenter studies are warranted. Incorporating environmental and climatic indicators may further improve the performance of the age-stratified stroke risk assessment model.
Conclusion
In this island study population, higher leukocyte count, triglyceride levels, and BMI, together with lower vitamin B12 levels, were associated with young age among patients with ischemic stroke. Young adult patients may have a higher prevalence of basal ganglia infarction, as well as a higher proportion of cardiogenic embolic infarction and strokes of other determined or undetermined etiologies. These findings highlight the importance of considering geographic specificity and age-related differences when formulating public health policies and allocating medical resources for ischemic stroke, and provide region-specific evidence to support prevention and management strategies in island populations.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding authors (Fangyu Dai and Haipeng Liu) upon reasonable request.
Ethics Approval and Consent to Participate
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Zhoushan Hospital (No. 20240031). Given the retrospective nature of the study, the requirement for written informed consent was waived. All patient data were anonymized prior to analysis and handled with strict confidentiality.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Medical and Health Science and Technology Plan Project of Zhoushan, grant number 2025RC03.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Johnston SC, Mendis S, Mathers CD. Global variation in stroke burden and mortality: estimates from monitoring, surveillance, and modelling. Lancet Neurol. 2009;8(4):345–12. doi:10.1016/S1474-4422(09)70023-7
2. McCarty JL, Leung LY, Peterson RB, et al. Ischemic Infarction in Young Adults: a Review for Radiologists. Radiographics. 2019;39(6):1629–1648. doi:10.1148/rg.2019190033
3. Nedeltchev K, der Maur TA, Georgiadis D, et al. Ischaemic stroke in young adults: predictors of outcome and recurrence. J Neurol Neurosurg Psychiatry. 2005;76(2):191–195. doi:10.1136/jnnp.2004.040543
4. Ji R, Schwamm LH, Pervez MA, Singhal AB. Ischemic stroke and transient ischemic attack in young adults: risk factors, diagnostic yield, neuroimaging, and thrombolysis. JAMA Neurol. 2013;70(1):51–57. doi:10.1001/jamaneurol.2013.575
5. Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics—2020 update: a report from the American Heart Association. Circulation. 2020;141(9):e139–e596. doi:10.1161/CIR.0000000000000757
6. Ekker MS, Boot EM, Singhal AB, et al. Epidemiology, aetiology, and management of ischaemic stroke in young adults. Lancet Neurol. 2018;17(9):790–801. doi:10.1016/S1474-4422(18)30233-3
7. Griffiths D, Sturm J. Epidemiology and etiology of young stroke. Stroke Res Treat. 2011;2011:209370. doi:10.4061/2011/209370
8. Aigner A, Grittner U, Rolfs A, et al. Contribution of established stroke risk factors to the burden of stroke in young adults. Stroke. 2017;48(7):1744–1751. doi:10.1161/STROKEAHA.117.016599
9. Kappelle LJ, Adams Jr HP, Heffner ML, et al. Prognosis of young adults with ischemic stroke. A long-term follow-up study assessing recurrent vascular events and functional outcome in the Iowa Registry of Stroke in Young Adults. Stroke. 1994;25(7):1360–1365. doi:10.1161/01.STR.25.7.1360
10. Neau JP, Ingrand P, Mouille-Brachet C, et al. Functional recovery and social outcome after cerebral infarction in young adults. Cerebrovasc Dis. 1998;8(5):296–302. doi:10.1159/000015869
11. Knight-Greenfield A, Nario JJQ, Gupta A. Causes of Acute Stroke: a Patterned Approach. Radiol Clin North Am. 2019;57(6):1093–1108. doi:10.1016/j.rcl.2019.07.007
12. Adams JHP, Biller J. Classification of subtypes of ischemic stroke: history of the trial of org 10 172 in acute stroke treatment classification. Stroke. 2015;46(5):e114–e117. doi:10.1161/STROKEAHA.114.007773
13. Calvet D. Ischemic stroke in the young adult. Rev Med Interne. 2016;37(1):19–24. doi:10.1016/j.revmed.2015.08.004
14. Yahya T, Jilani MH, Khan SU, et al. Stroke in young adults: current trends, opportunities for prevention and pathways forward. Am J Prev Cardiol. 2020;3:100085. doi:10.1016/j.ajpc.2020.100085
15. You RX, McNeil JJ, O’Malley HM, et al. Risk factors for stroke due to cerebral infarction in young adults. Stroke. 1997;28(10):1913–1918. doi:10.1161/01.STR.28.10.1913
16. Naess H, Waje-Andreassen U, Nyland H. Risk factor burden predicts long-term mortality in young patients with arterial cerebral infarction. Acta Neurol Scand. 2013;127(2):92–96. doi:10.1111/j.1600-0404.2012.01681.x
17. Zhang L, Segal AZ, Leifer D, et al. Circulating protein Z concentration, PROZ variants, and unexplained cerebral infarction in young and middle-aged adults. Thromb Haemost. 2017;117(1):149–157. doi:10.1160/TH16-04-0277
18. Naess H, Nyland HI, Thomassen L, Aarseth J, Myhr KM. Etiology of and risk factors for cerebral infarction in young adults in western Norway: a population-based case-control study. Eur J Neurol. 2004;11(1):25–30. doi:10.1046/j.1351-5101.2003.00700.x
19. Prust ML, Forman R, Ovbiagele B. Addressing disparities in the global epidemiology of stroke. Nat Rev Neurol. 2024;20(4):207–221. doi:10.1038/s41582-023-00921-z
20. Jacob MA, Ekker MS, Allach Y, et al. Global Differences in Risk Factors, Etiology, and Outcome of Ischemic Stroke in Young Adults-A Worldwide Meta-analysis: the GOAL Initiative. Neurology. 2022;98(6):e573–e588. doi:10.1212/WNL.0000000000013195
21. Feigin VL, Brainin M, Norrving B, et al. World Stroke Organization: global Stroke Fact Sheet 2025. Int J Stroke. 2025;20(2):132–144. doi:10.1177/17474930241308142
22. Lu X, Lin X, Shen Y, et al. Effect of coastal and island geographic environments on patients with acute ischemic stroke in southeastern China. J Int Med Res. 2024;52(10):3000605241285141. doi:10.1177/03000605241285141
23. Bao J, Guo Y, Wang Q, et al. Effects of heat on first-ever strokes and the effect modification of atmospheric pressure: a time-series study in Shenzhen, China. The Science of the Total Environment. 2019;654:1372–1378. doi:10.1016/j.scitotenv.2018.11.101
24. Yesilot Barlas N, Putaala J, Waje-Andreassen U, et al. Etiology of first-ever ischaemic stroke in European young adults: the 15 cities young stroke study. Eur J Neurol. 2013;20(11):1431–1439. doi:10.1111/ene.12228
25. Putaala J, Yesilot N, Waje-Andreassen U, et al. Demographic and geographic vascular risk factor differences in European young adults with ischemic stroke: the 15 cities young stroke study. Stroke. 2012;43(10):2624–2630. doi:10.1161/STROKEAHA.112.662866
26. Khan SS, Ning H, Wilkins JT, et al. Association of Body Mass Index With Lifetime Risk of Cardiovascular Disease and Compression of Morbidity. JAMA Cardiol. 2018;3(4):280–287. doi:10.1001/jamacardio.2018.0022
27. Gjærde LK, Gamborg M, Ängquist L, et al. Association of Childhood Body Mass Index and Change in Body Mass Index With First Adult Ischemic Stroke. JAMA Neurol. 2017;74(11):1312–1318. doi:10.1001/jamaneurol.2017.1627
28. Park JB, Kim DH, Lee H, et al. Effect of Moderately but Persistently Elevated Lipid Levels on Risks of Stroke and Myocardial Infarction in Young Korean Adults. J Am Heart Assoc. 2021;10(12):e020050. doi:10.1161/JAHA.120.020050
29. Mohsin M, Das SN, Haque MF, et al. Serum Uric Acid Level among Acute Stroke Patients. Mymensingh Med J. 2016;25(2):215–220.
30. Weir CJ, Muir SW, Walters MR, Lees KR. Serum urate as an independent predictor of poor outcome and future vascular events after acute stroke. Stroke. 2003;34(8):1951–1956. doi:10.1161/01.STR.0000081983.34771.D2
31. Zhu HY, Zhao SZ, Zhang ML, et al. Elevated Serum Uric Acid Increases the Risk of Ischemic Stroke Recurrence and Its Inflammatory Mechanism in Older Adults. Front Aging Neurosci. 2022;14:822350. doi:10.3389/fnagi.2022.822350
32. Yang Y, Gao L, Shen F, Miao J, Liu H. A cross-sectional analysis of the relationship between ischemic stroke and uric acid in young people in highland areas. Front Endocrinol. 2023;14:1325629. doi:10.3389/fendo.2023.1325629
33. Sun X, Lv J, Wu Z, Shi J, Huang H. Serum Uric Acid to Serum Creatinine Ratio and Risk of Stroke Recurrence in Young Adults with Ischemic Stroke. Neuropsychiatr Dis Treat. 2022;18:2031–2039. doi:10.2147/NDT.S378576
34. Packer M. Uric Acid Is a Biomarker of Oxidative Stress in the Failing Heart: lessons Learned from Trials With Allopurinol and SGLT2 Inhibitors. J Card Fail. 2020;26(11):977–984. doi:10.1016/j.cardfail.2020.08.015
35. Bai H, Nie X, Leng X, et al. Increased serum uric acid level is associated with better outcome after endovascular treatment for acute ischemic stroke—a prospective cohort study. Annals of Translational Medicine. 2022;10(20):1111. doi:10.21037/atm-22-4494
36. Amaro S, Laredo C, Renú A, et al. Uric Acid Therapy Prevents Early Ischemic Stroke Progression: a Tertiary Analysis of the URICO-ICTUS Trial (Efficacy Study of Combined Treatment With Uric Acid and r-tPA in Acute Ischemic Stroke). Stroke. 2016;47(11):2874–2876. doi:10.1161/STROKEAHA.116.014672
37. Quan K, Wang A, Zhang X, Wang Y. Leukocyte Count and Adverse Clinical Outcomes in Acute Ischemic Stroke Patients. Front Neurol. 2019;10:1240. doi:10.3389/fneur.2019.01240
38. Heikinheimo T, Putaala J, Haapaniemi E, Kaste M, Tatlisumak T. Leucocyte count in young adults with first-ever ischaemic stroke: associated factors and association on prognosis. Int J Stroke. 2015;10(2):245–250. doi:10.1111/j.1747-4949.2012.00968.x
39. Juli C, Heryaman H, Nazir A, et al. The Lymphocyte Depletion in Patients with Acute Ischemic Stroke Associated with Poor Neurologic Outcome. Int J Gen Med. 2021;14:1843–1851. doi:10.2147/IJGM.S308325
40. Ren H, Liu X, Wang L, Gao Y. Lymphocyte-to-Monocyte Ratio: a Novel Predictor of the Prognosis of Acute Ischemic Stroke. J Stroke Cerebrovasc Dis. 2017;26(11):2595–2602. doi:10.1016/j.jstrokecerebrovasdis.2017.06.019
41. Zhang J, Ren Q, Song Y, et al. Prognostic role of neutrophil-lymphocyte ratio in patients with acute ischemic stroke. Medicine. 2017;96(45):e8624. doi:10.1097/MD.0000000000008624
42. Gill D, Sivakumaran P, Aravind A, et al. Temporal Trends in the Levels of Peripherally Circulating Leukocyte Subtypes in the Hours after Ischemic Stroke. J Stroke Cerebrovasc Dis. 2018;27(1):198–202. doi:10.1016/j.jstrokecerebrovasdis.2017.08.023
43. Petrone AB, Eisenman RD, Steele KN, et al. Temporal dynamics of peripheral neutrophil and lymphocytes following acute ischemic stroke. Neurol Sci. 2019;40(9):1877–1885. doi:10.1007/s10072-019-03919-y
44. Yahn GB, Abato JE, Jadavji NM. Role of vitamin B12 deficiency in ischemic stroke risk and outcome. Neural Regen Res. 2021;16(3):470–474. doi:10.4103/1673-5374.291381
45. Roth W, Mohamadzadeh M. Vitamin B12 and gut-brain homeostasis in the pathophysiology of ischemic stroke. EBioMedicine. 2021;73:103676. doi:10.1016/j.ebiom.2021.103676
46. Spence JD. Nutrition and Risk of Stroke. Nutrients. 2019;11(3):647. doi:10.3390/nu11030647
47. Uggetti C. Stroke in young people: imaging. Neurol Sci. 2003;24(Suppl 1):S15–6. doi:10.1007/s100720300029
48. Oyinloye O, Nzeh D, Adesiyun O, et al. Neuroimaging of young adults with stroke in Ilorin Nigeria. Ann Afr Med. 2015;14(2):82–88. doi:10.4103/1596-3519.149897
49. Horie N, Morofuji Y, Iki Y, et al. Impact of basal ganglia damage after successful endovascular recanalization for acute ischemic stroke involving lenticulostriate arteries. J Neurosurg. 2019;132(6):1880–1888. doi:10.3171/2019.3.JNS182909
50. Florez-Perdomo WA, Garcia-Ballestas E, Konar SK, et al. Effect of Helicopter Transportation of Acute Ischemic Stroke Patients on Mortality and Functional Outcomes: a Systematic Review and Meta-Analysis. Air Medical Journal Sep-Oct. 2022;41(5):476–483. doi:10.1016/j.amj.2022.07.001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Serum Uric Acid to Serum Creatinine Ratio and Risk of Stroke Recurrence in Young Adults with Ischemic Stroke
Sun X, Lv J, Wu Z, Shi J, Huang H
Neuropsychiatric Disease and Treatment 2022, 18:2031-2039
Published Date: 9 September 2022