Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Dietary Intake, Stress, Anxiety, and Satisfaction with Nutrition Services in Patients with and without COVID-19
Authors Rodas-Vargas NA, Huayta-Quispe DZ, Ruiz Mamani PG, Javier-Aliaga DJ, Morales-García WC ![]() , Saintila J
, Saintila J ![]()
Received 2 December 2022
Accepted for publication 24 February 2023
Published 28 March 2023 Volume 2023:16 Pages 827—836
DOI https://doi.org/10.2147/JMDH.S399978
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Neil A Rodas-Vargas,1,2 Danitza Z Huayta-Quispe,1 Percy G Ruiz Mamani,3 David J Javier-Aliaga,4 Wilter C Morales-García,5 Jacksaint Saintila6
1Unit of Public Health, Postgraduate School, Peruvian Union University, Lima, Perú; 2Hospital II Pasco, EsSalud, Pasco, Perú; 3School of Nursing, San Juan Bautista Private University, Lima, Perú; 4School of Human Nutrition, Peruvian Union University, Lima, Peru; 5School of Medicine, Peruvian Union University, Lima, Perú; 6School of Medicine, Señor de Sipán University, Chiclayo, Perú
Correspondence: Jacksaint Saintila, School of Medicine, Señor de Sipán University, Km 5, Carretera a Pimentel, Chiclayo, Lambayeque, 14001, Perú, Email [email protected]
Background: Dietary intake constitutes a fundamental support in hospitalized patients to reduce morbimortality, risk of complications, and hospital stay.
Objective: We compared dietary intake, stress, anxiety, and satisfaction with the nutrition service in patients with and without COVID-19; we also analyzed the correlation between the variables mentioned.
Methods: A cross-sectional, comparative, and correlational study was carried out. A total of 215 patients were selected by non-probability convenience sampling (97 with COVID-19 and 118 without COVID-19).
Results: Patients with COVID-19 presented a higher percentage of “all the dish served” consumption (63.9%), as well as a higher percentage of “high” anxiety (18.6%) and “very high” satisfaction (28.9%) compared to their counterparts without COVID-19. The stress variable was predominantly moderate in both groups (57.7% vs 55.9%). Statistically significant and indirect correlation was found between satisfaction and stress level (rho = − 0.289; p< 0.01) in patients without COVID-19; similarly, between intake and stress level (rho =− .254; p< 0.05) in patients with COVID-19. Both groups presented a statistically significant and direct correlation between anxiety and stress level (rho =0.432 without COVID-19, rho = 0.525 with COVID-19; p< 0.01).
Conclusion: The findings suggest a multidisciplinary intervention, in which the improvement of mental health in the study population is contemplated and to coadunate the negative effects on the perception of the quality of care of the nutrition service and on dietary intake.
Keywords: COVID-19, dietary intake, stress, anxiety, degree of satisfaction, patients
Introduction
The COVID-19 pandemic has globally affected societies and health systems in socioeconomic terms. Moreover, the disease has become one of the leading causes of morbidity and mortality in the world.1 According to the World Health Organization (WHO), of the total number of cases reported worldwide, 42.6% corresponds to the Americas region.2 In Peru, reported cases represent 5% of the total population, of which 0.89% required hospitalization. It is worth mentioning that chronic risk factors such as cardiovascular disease, diabetes, obesity, and hypertension are associated with a worse prognosis.3
Patients presenting this respiratory viral infection recently described with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) are usually characterized by a severe inflammatory state and hyporexia, accelerating catabolism and weight loss, which associated with gastrointestinal disorders (vomiting, diarrhea), decreased food intake with the consequent presence of malnutrition.4–6 However, there is a group of patients who present malnutrition on admission; these patients have a higher risk of infectious complications, reduced immune response, ineffectiveness of treatment, and prolonged hospital stay, which leads to a higher risk of morbidity and mortality.7–9 Although studies on dietary intake of patients with and without COVID-19 are not abundant, however, a study of 101 hospitalized patients with COVID-19 reported that the most frequent feeding and nutrition problems were inadequate oral intake, inadequate energy intake, and malnutrition observed in 46.7%, 18.9%, and 18.4% of patients, respectively.10 Therefore, adequate nutritional management including enteral nutrition, dietary supplements, and multivitamin and multimineral supplement therapy are required, accompanied with constant monitoring.10
There are findings from previous studies that demonstrate that an adequate and timely nutritional intake, characterized by proteins and some micronutrients such as selenium and zinc, are associated with optimal immune function, lower risk of infection, decreased morbidity and mortality, lower risk of complications and hospital stay,7,11 and increased resistance to infection.12,13 Therefore, the evaluation of intake and the factors that influence it should be considered as part of the patient’s daily management.14,15
However, it is important to emphasize that psychological manifestations, such as anxiety and stress, may occur concomitantly16 and may alter eating patterns and dietary intake.17,18 Indeed, the available evidence shows that hospitalized patients often experience psychological distress and other mental problems.19 This could be due to the unpredictability and uncertainty characteristics of COVID-19, which expose patients to stressful situations. In addition, fear of the deadly consequences of the disease, coupled with anxiety and stress, can create unfavorable mental and physical conditions in the patient. One study reported that patients hospitalized for COVID-19 present a high level of stress during the first week of hospitalization, but the relationship between stress and COVID-19 is unknown.20 However, the relationship with dietary intake during this period is unknown.
Likewise, the degree of satisfaction with respect to hospital diets (complete or therapeutic) has been evaluated by some authors to include improvements in nutritional care processes, but without relating them to the variables described above.21–25 Several investigations that studied the percentage of food waste of the hospital diet to quantify the intake or determine the acceptability of the diets served, resulted in an average value between 30–40%, which has a direct effect on the nutritional status of the patient.15,26–29 In a study of nutritional therapy in hospitalized patients by COVID-19, nutritional intake was found to be at the lower limit or below the recommended amounts.30 Consequently, the provision and consumption of diet should be considered as an integral part of treatment to aid patient recovery.31
During hospital stay, patients depend on the food provided by the hospital to cover their nutritional requirements; however, there is no evidence on how the relationship between dietary intake, anxiety, stress, and satisfaction with hospital nutritional care may impact patients hospitalized for COVID-19. Therefore, in the present study we determined dietary intake, stress, anxiety, and satisfaction with the nutrition service in patients with and without COVID-19; in addition, we analyzed the correlation between the mentioned variables in patients with and without COVID-19.
Materials and Methods
Research Design and Participants
A cross-sectional, comparative and correlational study was carried out. A total of 215 adult patients between 18 and 59 years of age were selected by non-probabilistic convenience sampling. There were 97 patients hospitalized by COVID-19 and 118 patients hospitalized in general services in EsSalud hospital of the Pasco Health Care Network with COVID-19 hospital care, from March to August 2021. In both groups, all patients who had received at least 3 meals of the Hyperproteic Hypoglycaemic or Hyperproteic Bland diet and those who voluntarily accepted to provide information and were in adequate conditions to answer the questionnaires were selected. Patients who did not meet the criteria of age, type of diet, and those with a diagnosis of psychiatric pathology, disorders of consciousness, or difficulty in communicating were excluded.
Ethical Aspects
Prior to data collection, participants were informed of the objective of the study and the purpose of data collection. Subsequently, they were invited to be part of the study and voluntarily accepted. In addition, their informed consent was obtained and the study received the approval of the Research Ethics Committee of the Universidad Peruana Unión (approval number: 2021-CEUPeU-0026) and the authorization of the EsSalud research committee (approval number: 002-Dr. MCCH-PCI-HIIP-RAPA-ESSALUD-2021). Finally, data collection was performed according to the guidelines established by the Helsinki Declaration.
Dietary Intake
To calculate dietary intake, the double weighing technique was used, using a digital balance32 using a digital scale. Previously, the preparation for the Hyperproteic Hypoglycaemic and Hyperproteic Soft diets was standardized, including the weight of the utensils used in dispensing the food. The ration was weighed before being given to the patient and afterwards the residues of the three meal times that the patient received in one day (breakfast, lunch, and dinner). After knowing the initial and final weight of the dish, and considering the weight of the container, the weight of the ration received and that ingested was calculated. Intake was categorized into: None = 0–19.9%, Almost none = 20–39.9%, Half = 40–59.9%, Almost all = 60–79.9% and All = 80–100%.33
Stress
Stress was measured using a modified version of the Perceived Stress Scale (EPP-10) related to the COVID-19 (EPP-10-c) and has a Cronbach’s alpha of 0.86.34 The questionnaire is composed of 10 items with Likert-type response from 0 (never) to 4 (very often). Items 1, 3, 9 and 10 are scored directly from 0 to 4 and items 2, 4, 5, 6, 7 and 8, inversely, from 4 to 0. The scale score ranges from 0 to 40, where 0–13 = low stress, 14–26 = moderate stress, and 27–40 = high stress.
Anxiety
Anxiety was measured with the translated questionnaire “Coronavirus Anxiety Scale (CAS)35 which has 5 items and presented a Cronbach’s alpha of 0.89. The items are scored on a 5-point Likert scale, where 0 = Not at all and 4 = Almost every day; a score of 0–8 indicates low anxiety and 9–20 indicates high anxiety.36
Satisfaction with the Nutrition Service
To determine the degree of satisfaction with the nutrition service of the participants, the SERVNUT instrument was used, consisting of 15 items, adapted, and validated with a Cronbach’s alpha of 0.848. The categorization was: Very low = 15–26, low = 27–38, medium = 39–50, high = 51–62 and very high = 63–75.37 Data on these three variables were collected through a self-applied Google survey and delivered by trained health personnel.
Statistical Analysis
The data were recorded and sorted using Microsoft Excel version 365. SPSS version 24 statistical software (SPSS Inc., Chicago, IL, USA) was used for data processing and analysis. Frequency tables and percentages were used for descriptive analysis. In addition, the Mann–Whitney U-test, Cohen’s d, Pearson’s Chi-square, and Fisher’s exact test were used to evaluate the degree of difference of the variables between the study groups. Correlation analysis was carried out between the variables dietary intake, stress, anxiety, and satisfaction with the nutrition service using Spearman’s Rho test (p) because the data did not present a normal distribution according to the Kolmogorov Smirnov statistical test (p>0.05). A significance level of 5% was considered.
Results
A total of 215 samples were performed (Table 1); 97 of them (45.1%) in patients with COVID-19 and 118 (54.9%) in patients without COVID-19. The mean age of patients with COVID-19 was 43.03 years (SD 9.97) and without COVID-19 was 35.52 (SD 9.56). Female sex was predominant in both groups, 61.9% and 83.9% respectively, “Higher” educational degree evidenced higher proportion in patients with COVID-19 (39.2%) and “Secondary” in patients without COVID-19 (41.5%). Appetite was normal (83.5% and 85.6%), but patients with COVID-19 presented a higher percentage of low appetite (15.5%); the length of hospital stay when applying the instruments was less than 1 week (85.6% and 95.8%) and the type of diet with the highest prescription was Hyperproteic Soft (53.6% and 96.6%). These variables showed a statistically significant difference between both groups (p < 0.05).
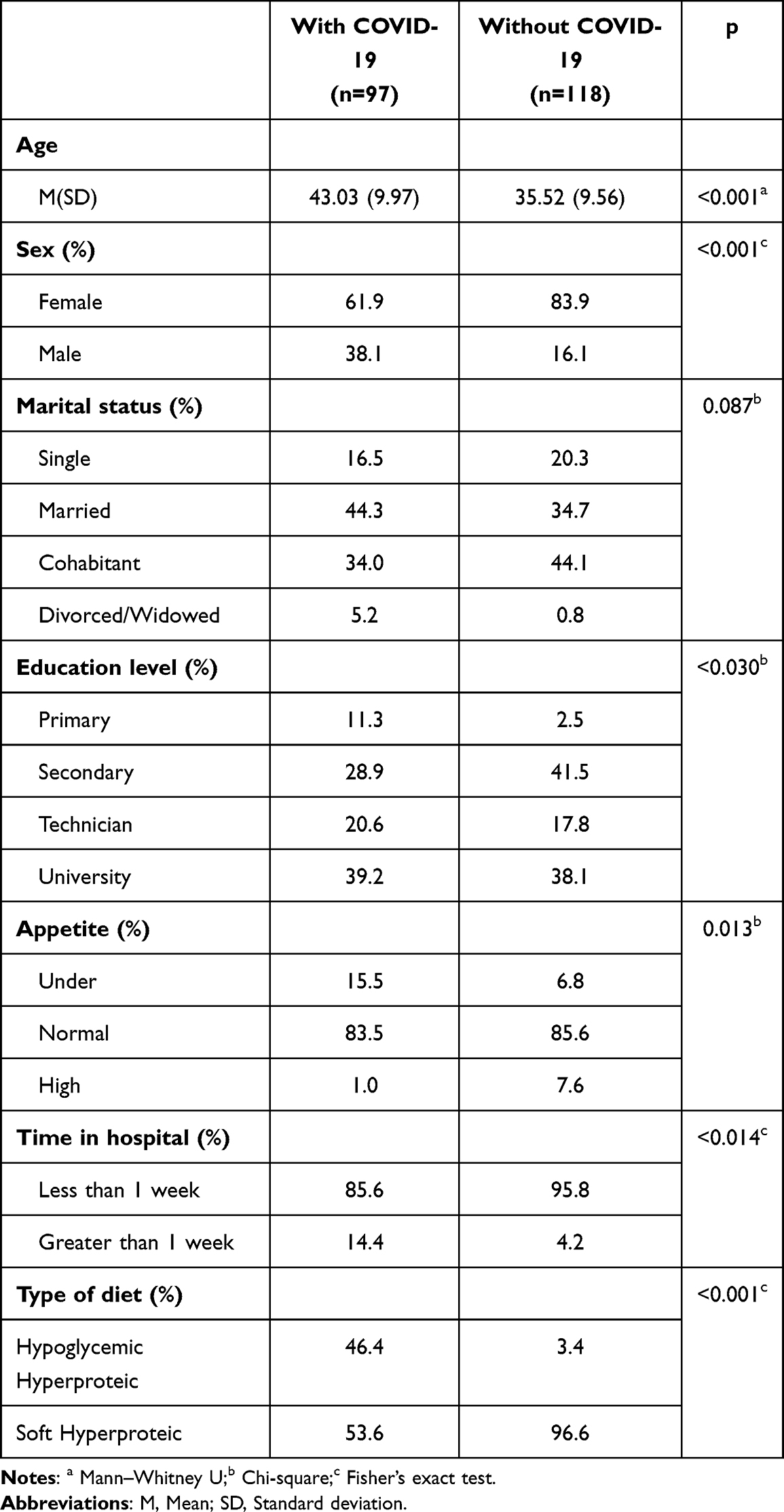 |
Table 1 Sociodemographic Characteristics of Patients with and without COVID-19 |
In both groups (Table 2), at the categorical level, dietary intake, anxiety, and satisfaction with the nutrition service showed statistically significant differences (p<0.05). Regarding intake, COVID-19 patients presented a higher percentage of consumption of “all the dish served” (63.9%), in addition, a higher percentage of “high” anxiety (18.6%) and “very high” satisfaction (28.9%) compared to their counterparts without COVID-19. The stress variable did not present a statistically significant difference and in both groups there was a predominance of moderate stress (57.7% vs 55.9%).
 |
Table 2 Comparative Analysis of the Scores by Categories of the Study Variables in Patients with and without COVID-19 |
Table 3 shows a statistically significant mean score difference (p<0.001) and moderate effect size for anxiety (d=0.763) and satisfaction with the nutrition service (d=0.770). The means of the other study variables did not present statistically significant differences.
 |
Table 3 Difference in the Mean Scores of the Study Variables in Patients with and without COVID-19 |
The level of stress presented a statistically significant and direct correlation with the level of anxiety (rho =0.432) and an indirect correlation with the degree of satisfaction (rho =−.289) in patients without COVID-19 (see Table 4).
 |
Table 4 Correlation Analysis Between Stress, Anxiety, and Satisfaction with the Nutrition Service on Dietary Intake in Patients Without COVID-19 |
Table 5 shows that the level of stress is statistically significantly and indirectly correlated with intake (rho =−.254) and directly correlated with the level of anxiety (rho = 0.525) in patients with COVID-19.
 |
Table 5 Correlation Analysis Between Stress, Anxiety, and Satisfaction with the Nutrition Service on Dietary Intake in Patients with COVID-19 |
Discussion
Dietary intake, satisfaction with hospital services, and care of mental health aspects play a fundamental role in the treatment and recovery of hospitalized patients. However, there are few studies that address these issues; therefore, the purpose of this study was to determine dietary intake, stress, anxiety, and satisfaction with the nutrition service and the correlation between the study variables in patients with and without COVID-19.
Hospitalized patients with COVID-19 have a decreased dietary intake, which is caused by several factors such as dysosmia, dysgeusia, and low appetite, which, in turn, increases the risk of malnutrition and morbidity and mortality38 which, in turn, increase the risk of malnutrition and morbidity and mortality.39 In this study, it was observed that patients with COVID-19 had a higher percentage of low appetite compared to those without COVID-19, however, they were also those who had a higher dietary intake, ie, the highest percentage consumed the entire plate served. The dietary intake observed in the current study is different from that found in a study conducted in hospitalized patients in non-COVID-19 areas, where 50% of cases ingested the entire plate served, however, they only evaluated the sum of lunch and dinner of the day.33 Another study evaluated only lunch and found that 38% of patients ingested all food on the tray.24 Our study included the total intake of the day (breakfast, lunch, and dinner); but, as in other studies, there were a group of patients who did not ingest the total amount served.24,27,28,33 This could be due to the fact that patients with COVID-19 are concerned about the deadly consequences of the disease and, consequently, would be more motivated to consume the hospital diet.
In relation to the level of stress, both groups presented a higher percentage of moderate stress. This finding could be explained by the fact that the COVID-19 pandemic condition can alter the patient’s mental state, causing greater stress.40 Additionally, our results indicate that the mean anxiety level in both groups was found to be below the CAS cut-off score ≥9, but patients with COVID-19 presented a higher score compared to their counterparts without COVID-19; moreover, when comparing the levels of high anxiety in both groups, patients with COVID-19 presented a higher percentage. The level of high anxiety observed in our study was different from that reported in COVID-19 patients from Wuhan during the “first wave”, where the prevalence of anxiety was 38.5%.41 The difference observed in the present study could be related to the period of information gathering (“second wave”) when the pandemic in Peru and specifically in the Pasco region was decreasing considerably in addition to the fact that the population was receiving the vaccine as a preventive measure and had more and better information regarding the situation of the Health Emergency. These aspects are associated with a lower psychological impact on the prevalence of stress and anxiety.42
On the other hand, patients with COVID-19 reported greater satisfaction with the nutrition service. The evaluation of service satisfaction included dimensions such as empathy (food preferences and treatment of care staff), responsiveness (schedule and promptness of care), and gastronomic experience, which considered the hospital diet. Our results could be due, albeit partially, to the fact that the greatest proportion of patients with COVID-19 were satisfied with the empathy of the service’s nutritionists. For example, when asked about the nutritionist’s treatment, an average score of 4.5 on a scale from 1 to 5 was obtained. On the other hand, although the hospital diet is not always well received by patients, nevertheless, those who presented COVID-19 reported better satisfaction with the diet (gastronomic experience) during the hospital stay. It is worth mentioning that similar studies21–25 conducted in patients without COVID-19, found that hospitalized patients reported high levels of satisfaction with the hospital diet. These results could indicate the adequate progress in the quality of care by the nutrition service staff and with the diet served. In addition, the increase in the number of health care personnel hired for personalized nutritional care may have been beneficial.
The present study found a direct association between stress and anxiety in patients with and without COVID-19. There is evidence that mental conditions may be linked in patients with COVID-1916 and without COVID-19.43–45 These results demonstrate that mental health problems may manifest concomitantly and may cause a deterioration in the mental health of patients during hospitalization.
There was also evidence of an indirect association between satisfaction with the nutrition service and stress in patients without COVID-19, showing that the greater the stress, the lower the satisfaction. Although various authors who have evaluated satisfaction with hospital services46–48 showed that the performance or empathy provided by health personnel improves patient satisfaction with the service; stress, as an intrinsic cause, can worsen it.49 This consequence shows that the patient’s mental condition may interfere in the assessment of the quality of care provided during hospitalization.
Likewise, stress and dietary intake in COVID-19 patients presented an indirect association, showing that the higher the stress, the lower the dietary intake. These findings coincide with similar results reported in a group of patients who, with a high level of stress, presented an inadequate food intake.18 In general, stress is associated with a higher intake of unhealthy palatable foods, however, there is evidence that stress is associated with a higher intake of unhealthy palatable foods.50–52 However, there is evidence that higher perceived stress is associated with lower intake of healthy foods and nutrients such as fruits, vegetables, and protein.53 In fact, the presence of severe and acute stress may be associated with suppression of food intake.54
Considering these results, a multidisciplinary intervention is important, in which the improvement of mental health in the study population is contemplated to contribute to the negative effects of stress on the perception of the quality of care of the nutrition service and on dietary intake and the consequent hospital malnutrition.
Limitations
The study results should be interpreted considering certain limitations. First, little information was considered regarding sociodemographic parameters, clinical and nutritional status of the patients, because these parameters were not evaluated and could influence the satisfactory behavior of the care provided or in response to the psychological manifestations regarding intake. Secondly, the nutritional intake (macronutrient and micronutrient intake) related to COVID-19 patients has not been collected, which would evidence a better knowledge of the nutritional requirements consumed. Therefore, future studies should take into account clinical aspects, nutritional and anthropometric caloric intake in patients with or without COVID-19. Finally, the information collected was only for a period of six months, since after that, the hospitalization of COVID-19 patients was considerably low.
Conclusion
In the current study, relative to the comparison analyses, patients with COVID-19 had the highest dietary intake, ie, the highest percentage reported consuming “all the dish served”. In addition, both groups presented a higher percentage of moderate stress. On the other hand, patients with COVID-19 presented a higher anxiety score, in addition, they reported higher satisfaction with the nutrition service compared to their counterparts without COVID-19. Regarding the association analyses, a direct association was found between stress and anxiety in patients with and without COVID-19. It was also found that the greater the stress, the lower the satisfaction. Finally, stress and dietary intake in COVID-19 patients presented an indirect association, showing that the greater the stress, the lower the dietary intake.
Acknowledgment
We thank the study participants and Dr Varisier Noel for their support.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no conflicts of interest to declare.
References
1. Chang D, Chang X, He Y, Tan KJK. The determinants of COVID-19 morbidity and mortality across countries. Sci Rep. 2022;12(1):5888. doi:10.1038/s41598-022-09783-9
2. OMS. Panel de control de coronavirus (COVID-19) de la OMS [Internet]. OMS; 2021. Available from: https://www.who.int/es/emergencies/diseases/novel-coronavirus-2019.
3. Li B, Yang J, Zhao F, et al. Prevalence and impact of cardiovascular metabolic diseases on COVID-19 in China. Clin Res Cardiol. 2020;109(5):531–538. doi:10.1007/s00392-020-01626-9
4. Abate SM, Chekole YA, Estifanos MB, Abate KH, Kabthymer RH. Prevalence and outcomes of malnutrition among hospitalized COVID-19 patients: a systematic review and meta-analysis. Clin Nutr ESPEN. 2021;43:174–183. doi:10.1016/j.clnesp.2021.03.002
5. Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–513. doi:10.1016/S0140-6736(20)30211-7
6. Vásconez A, Moyón M. Recomendaciones nutricionales para pacientes hospitalizados con infección respiratoria grave (IRAG) sospechosa o confirmada por COVID-19. Rev Colomb Cirugía. 2020;35(2):98.
7. Mendes A, Serratrice C, Herrmann FR, et al. Nutritional risk at hospital admission is associated with prolonged length of hospital stay in old patients with COVID-19. Clin Nutr. 2021;156.
8. Yu Y, Ye J, Chen M, et al. Malnutrition Prolongs the Hospitalization of Patients with COVID-19 Infection: a Clinical Epidemiological Analysis. J Nutr Heal Aging. 2021;25(3):369–373. doi:10.1007/s12603-020-1541-y
9. Viveros-García J. Ortogeriatría en México: un futuro posible. Med Int Méx. 2019;35(1):150–153.
10. Ansu V, Papoutsakis C, Gletsu‐Miller N, et al. Nutrition care practice patterns for patients with COVID‐19—A preliminary report. J Parenter Enter Nutr. 2021;45(8):1774–1778. doi:10.1002/jpen.2106
11. Wilkens Knudsen A, Beck AM, Østergaard T, Højgaard Rasmussen H, Munk T. Assessment of nutritional risk and intake in Danish hospitalized patients. Clin Nutr ESPEN. 2020;40:469. doi:10.1016/j.clnesp.2020.09.190
12. Calder P, Carr A, Gombart A, Eggersdorfer M. Optimal Nutritional Status for a Well-Functioning Immune System Is an Important Factor to Protect against Viral Infections. Nutrients. 2020;12(4):1181. doi:10.3390/nu12041181
13. Maggini S, Pierre A, Calder P. Immune Function and Micronutrient Requirements Change over the Life Course. Nutrients. 2018;10(10):1531. doi:10.3390/nu10101531
14. Molero IG, Olveira Fuster G, Liébana MI, Oliva L, Laínez López M, Aguilar AM. Influence of temperature on food intake in hospitalized patients. Nutr Hosp. 2008;23(1):54–59.
15. Salvador-Monferrer L, Fernández-Olea M, Murillo-Sanchis J. Malnutrition and factors that influence the food intake in hospitalized patients: a review. Nutr Clín Diet Hosp. 2014;34(3):80–91.
16. Parker C, Shalev D, Hsu I, et al. Depression, Anxiety, and Acute Stress Disorder Among Patients Hospitalized With COVID-19: a Prospective Cohort Study. J Acad Consult Psychiatry. 2021;62(2):211–219.
17. Rodríguez M, Bernal-Gómez TY, Vergara M, et al. Percepción subjetiva de manejo emocional, ansiedad y patrones de ingesta relacionados con aislamiento por COVID-19 * Subjective Perception of Emotional Management, Anxiety and Intake Patterns Related to Isolation by COVID-19. Univ Psychol. 2020;19:1–9. doi:10.11144/Javeriana.upsy19.psme
18. Brunori EHFR, Lopes CT, Cavalcante AMRZ. Consumo alimentar e estresse em pacientes com síndrome coronariana aguda. Rev Bras Enferm. 2015;68(5):810–816. doi:10.1590/0034-7167.2015680507i
19. Zandifar A, Badrfam R, Yazdani S, et al. Prevalence and severity of depression, anxiety, stress and perceived stress in hospitalized patients with COVID-19. J Diabetes Metab Disord. 2020;19(2):1431–1438. doi:10.1007/s40200-020-00667-1
20. Matalon N, Dorman-Ilan S, Hasson-Ohayon I, et al. Trajectories of post-traumatic stress symptoms, anxiety, and depression in hospitalized COVID-19 patients: a one-month follow-up. J Psychosom Res. 2021;143:110399. doi:10.1016/j.jpsychores.2021.110399
21. Guillén N, Torrentó M, Alvadalejo R, Salas-Salvadó J. Assessment of the acceptance of set meals served at the “Sant Joan de Reus” University Hospital | evaluación de la aceptación de los menús servidos en el Hospital Universitari de Sant Joan de Reus. Nutr Hosp. 2004;19(5):277–280.
22. Lechón A, Ruiz I, Reyes L, Salazár A. Nivel de satisfacción de los pacientes hospitalizados, respecto a la dieta del Hospital San Vicente de Paúl de Ibarra, 2018. La U Investig. 2019;6(2):33–53.
23. Benítez Brito N, Oliva García JG, Delgado Brito I, et al. Análisis del grado de satisfacción alimentaria percibido por los pacientes en un hospital de tercer nivel. Nutr Hosp. 2016;33(6):1361–1366. doi:10.20960/nh.796
24. Rubio-Martín E, Rojo-Martínez G, Caracuel Á, et al. Satisfacción con el menú hospitalario e incorporación del queso de cabra como postre en comparación con el queso de vaca. Nutr Hosp. 2015;32(4):1766–1772. doi:10.3305/nh.2015.32.4.9526
25. Fernández-Martínez B, Alguacil-Pau AI, Crespo-Sevilla R, García-Vega A. Predictores de la satisfacción de los pacientes con la alimentación de un hospital público de Madrid. Rev Calid Asist. 2013;28(3):155–162. doi:10.1016/j.cali.2012.09.005
26. Simzari K, Vahabzadeh D, Nouri Saeidlou S, Khoshbin S, Bektas Y. Ingesta y desperdicio de alimentos y su asociación con la desnutrición hospitalaria. Nutr Hosp. 2017;34(6):1376–1381. doi:10.20960/nh.1102
27. Williams P, Walton K. Plate waste in hospitals and strategies for change. E Spen Eur E J Clin Nutr Metab. 2011;6(6):e235–41. doi:10.1016/j.eclnm.2011.09.006
28. Van Bokhorst-De Van Der Schueren MAE, Roosemalen MM, Weijs PJM, Langius JAE. High waste contributes to low food intake in hospitalized patients. Nutr Clin Pract. 2012;27(2):274–280. doi:10.1177/0884533611433602
29. Barton AD, Beigg CL, Macdonald IA, Allison SP. High food wastage and low nutritional intakes in hospital patients. Clin Nutr. 2000;19(6):445–449. doi:10.1054/clnu.2000.0150
30. Pironi L, Sasdelli AS, Ravaioli F, et al. Malnutrition and nutritional therapy in patients with SARS-CoV-2 disease. Clin Nutr. 2021;40(3):1330–1337. doi:10.1016/j.clnu.2020.08.021
31. Edwards JSA, Hartwell HJ. Hospital food service: a comparative analysis of systems and introducing the “Steamplicity” concept. J Hum Nutr Diet. 2006;19(6):421–430. doi:10.1111/j.1365-277X.2006.00730.x
32. Cruz R, Herrera T. Procedimientos Clínicos para la Atención Nutricional. Lima: Iidenut SA; 2013.
33. Calleja Fernández A, Vidal Casariego A, Cano Rodríguez I, Ballesteros Pomar MD. Cuestionario semicuantitativo para la valoración de la ingesta dietética del paciente hospitalizado: una herramienta sencilla para la práctica clínica. Nutr Hosp. 2016;33(2):324–329. doi:10.20960/nh.112
34. Campo-Arias A, Pedrozo-Cortés MJ, Pedrozo-Pupo JC. Escala de estrés percibido relacionado con la pandemia de COVID-19: una exploración del desempeño psicométrico en línea. Rev Colomb Psiquiatr. 2020;49(4):229–230. doi:10.1016/j.rcp.2020.05.005
35. Caycho Rodriguez T, Barboza Palomino M, Ventura León J, et al. Traducción al español y validación de una medida breve de ansiedad por la COVID-19 en estudiantes de ciencias de la salud. ScieneDirect - Anciedad y Estrés. 2020;26(2–3):174–180. doi:10.1016/j.anyes.2020.08.001
36. Ahn MH, Lee J, Suh S, et al. Application of the Stress and Anxiety to Viral Epidemics-6 (SAVE-6) and Coronavirus Anxiety Scale (CAS) to Measure Anxiety in Cancer Patient in Response to COVID-19. Front Psychol. 2020;11:604441. doi:10.3389/fpsyg.2020.604441
37. Rojas Apolinario E, Roldan Arbieto L. Validación de un instrumento para medir el nivel de satisfacción de pacientes hospitalizados con respecto al servicio de nutrición. Rev la Fac Med Humana. 2018;18(4):65–73.
38. Aziz M, Goyal H, Haghbin H, Lee-Smith WM, Gajendran M, Perisetti A. The Association of “Loss of Smell” to COVID-19: a Systematic Review and Meta-Analysis. Am J Med Sci. 2021;361(2):216–225. doi:10.1016/j.amjms.2020.09.017
39. Álvarez J, Lallena S, Bernal M. Nutrición y pandemia de la COVID-19. Programa Form Méd Contin Acreditado. 2020;13(23):1311–1321. doi:10.1016/j.med.2020.12.013
40. Paredes Pérez PM, Dawaher Dawaher JE, Chérrez Paredes MF. Impacto del COVID-19 en la salud mental de los pacientes hospitalizados. Rev Fac Cienc Méd Univ Cuenca. 2020;55–64.
41. Nie X-D, Wang Q, Wang M-N, et al. Anxiety and depression and its correlates in patients with coronavirus disease 2019 in Wuhan. Int J Psychiatry Clin Pract. 2021;25(2):109–114. doi:10.1080/13651501.2020.1791345
42. Wang C, Pan R, Wan X, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020;17(5):1729. doi:10.3390/ijerph17051729
43. Martínez-Martínez CA. Depresión y ansiedad en pacientes hospitalizados en el servicio de Medicina Interna del Hospital Escuela Universitario de Honduras. Rev Psicol LA SALUD. 2021;9(1):453.
44. Hernández GG, Orellana VG, Kimelman JM, Nuñez MC, Ibáñez HC. Trastornos de ansiedad en pacientes hospitalizados en Medicina Interna. Rev Med Chil. 2005;133(8):895–902. doi:10.4067/S0034-98872005000800005
45. Martín AG, Soler RS, Picart PA, Comas Casanovas P. Niveles de ansiedad y depresión en enfermos hospitalizados y su relación con la gravedad de la enfermedad. Med Clin (Barc). 2003;120(10):370–375. doi:10.1016/S0025-7753(03)73707-5
46. Pérez Milian JM, Berrio Aguila JE, Ojeda YP, Rodríguez Quesada NY, Fernández Pérez SE, Aranguren Torriente D. Evaluación de la satisfacción de pacientes atendidos por la COVID-19 en el Hospital Universitario Clínico Quirúrgico Cmdte. Manuel Fajardo Rivero Medicentro. 2020;24(3):630–641.
47. Vizcaíno AD-J, Vizcaíno-Marín VD-P, Fregoso-Jasso GS. Análisis de la satisfacción de pacientes del servicio de urgencias en un hospital público de Jalisco. Horiz Sanit. 2018;18(1):27–36.
48. Piedra-Valoy I, Lipa-Chancolla CA. Calidad de la atención y grado de satisfacción de los pacientes atendidos en el servicio de Emergencia del Hospital Essalud II Vitarte. Rev la Soc Peru Med Interna. 2018;31(4):137–142.
49. Sopen Kunsrikoaw C, Wallapa Chaibourkeaw K. Patient Satisfaction with Nursing Care Received during the Intrapartum Period. Thai J Nurs Res. 2003;7:83–92.
50. León-Paucar SD, Calderón-Olivos BC, Calizaya-Milla YE, Saintila J. Depression, dietary intake, and body image during coronavirus disease 2019 quarantine in Peru: an online cross-sectional study. SAGE Open Med. 2021;9:205031212110519. doi:10.1177/20503121211051914
51. Davila-Torres DM, Vilcas-Solís GE, Rodríguez-Vásquez M, Calizaya-Milla YE, Saintila J. Eating habits and mental health among rugby players of the Peruvian pre-selection during the second quarantine due to the COVID-19 pandemic. SAGE Open Med. 2021;9:205031212110437. doi:10.1177/20503121211043718
52. Banda-Ccana DE, Infantes-Ruiz VH, Calizaya-Milla YE, Saintila J. Diet and risk of mental illness in Peruvian adults, cross-sectional study [Dieta y riesgo de enfermedades mentales en adultos peruanos, estudio transversal]. Arch Latinoam Nutr. 2021;71(3):199–207. doi:10.37527/2021.71.3.004
53. Laugero KD, Falcon LM, Tucker KL. Relationship between perceived stress and dietary and activity patterns in older adults participating in the Boston Puerto Rican Health Study. Appetite. 2011;56(1):194. doi:10.1016/j.appet.2010.11.001
54. Smith KR, Jansen E, Thapaliya G, et al. The influence of COVID-19-related stress on food motivation. Appetite. 2021;163:105233. doi:10.1016/j.appet.2021.105233
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Psychological Impact of Quarantine During the COVID-19 Pandemic on Quarantined Non-Healthcare Workers, Quarantined Healthcare Workers, and Medical Staff at the Quarantine Facility in Saudi Arabia
Alfaifi A, Darraj A, El-Setouhy M
Psychology Research and Behavior Management 2022, 15:1259-1270
Published Date: 17 May 2022
Spiritual Well-Being, Depression, Anxiety, and Stress in Indonesian Muslim Communities During COVID-19
Hamka, Suen MW, Ramadhan YA, Yusuf M, Wang JH
Psychology Research and Behavior Management 2022, 15:3013-3025
Published Date: 17 October 2022
Pre- and Post-Pandemic (COVID-19) Mental Health of International Students: Data from a Longitudinal Study
Jamshaid S, Bahadar N, Jamshed K, Rashid M, Imran Afzal M, Tian L, Umar M, Feng X, Khan I, Zong M
Psychology Research and Behavior Management 2023, 16:431-446
Published Date: 15 February 2023
Dietary Supplement Consumption and Mental Health in Indonesian Adults During Second Wave of COVID-19 Pandemic
Yusof J, d'Arqom A, Andriani AP, Nasution MZ, Fatimah N, Mustika A, Handayani S, Syed Abdul Kadir SZ
Patient Preference and Adherence 2023, 17:1799-1811
Published Date: 24 July 2023
Longitudinal Problematic Social Media Use in Students and Its Association with Negative Mental Health Outcomes
Shannon H, Bush K, Shvetz C, Paquin V, Morency J, Hellemans KGC, Guimond S
Psychology Research and Behavior Management 2024, 17:1551-1560
Published Date: 8 April 2024