Back to Journals » Infection and Drug Resistance » Volume 19
Diagnostic Yield of Nontuberculous Mycobacteria Testing in Patients with Chronic Lung Diseases: A Retrospective Cohort Study
Authors Jankovic Makek M, Tolic E, Lange C, Zvonar M, Darapi Marušić D, Marekovic I, Badovinac S ![]() , Glodic G, Marcic K, Zielinski N, Reimann M
, Glodic G, Marcic K, Zielinski N, Reimann M ![]()
Received 17 February 2026
Accepted for publication 27 April 2026
Published 26 June 2026 Volume 2026:19 598718
DOI https://doi.org/10.2147/IDR.S598718
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Mateja Jankovic Makek,1,2 Ena Tolic,2 Christoph Lange,3– 6 Matea Zvonar,2 Dora Darapi Marušić,2 Ivana Marekovic,1,7 Sonja Badovinac,2 Goran Glodic,2 Kristijan Marcic,1 Nika Zielinski,3– 5 Maja Reimann3– 5
1School of Medicine, University of Zagreb, Zagreb, Croatia; 2Department for Respiratory Diseases, University Hospital Centre Zagreb, Zagreb, Croatia; 3Clinical Infectious Diseases, Research Centre Borstel, Borstel, Germany; 4German Centre for Infection Research (DZIF), Partner Site Hamburg-Lübeck-Borstel-Riems, Borstel, Germany; 5Respiratory Medicine & International Health, University of Lübeck, Lübeck, Germany; 6Department of Paediatrics, Texas Children’s Hospital; The Global Tuberculosis Program; Immigrant and Global Health, Baylor College of Medicine, Houston, TX, USA; 7Department for Microbiology, University Hospital Centre Zagreb, Zagreb, Croatia
Correspondence: Maja Reimann, Clinical Infectious Diseases, Research Centre Borstel, Borstel, Germany, Email [email protected]
Objective: Obstructive lung disease (OLD), that is, chronic obstructive pulmonary disease (COPD), asthma, and pulmonary malignancies, is a common comorbidity in patients with nontuberculous mycobacterial pulmonary disease (NTM-PD). However, there are limited data on the yield of nontuberculous mycobacterial (NTM) testing in these patient groups. This study aimed to assess the prevalence of NTMs and NTM-PD in patients with OLD and/or pulmonary malignancy.
Methods: A retrospective analysis of all mycobacterial cultures obtained from respiratory samples of patients with OLD (either during exacerbation or during stable disease) and/or pulmonary malignancies referred to our center from January 2021 to January 2023 was performed. International definitions were applied to assess the NTM-PD.
Results: NTM was isolated in 0.5% (4/834) of bronchopulmonary specimens from patients with pulmonary malignancies, 2.4% (13/553) from patients with stable OLD, and 3.5% (8/228) from patients with exacerbation of OLD. NTM-PD criteria were met in 32% (8/25) of the patients in the OLD cohort. In the OLD cohort, the likelihood of NTM isolation was higher in patients with lower BMI (p = 0.030), frequent exacerbations (p = 0.004), and use of inhaled corticosteroids (ICS) (p = 0.012). NTM-PD was more likely in patients with a lower BMI (p = 0.043) and frequent exacerbations (p = 0.023), but not in those using ICS (p = 0.482), regardless of the dose.
Conclusion: The yield of NTM isolation from patients with OLD and/or lung malignancy is generally low. However, routine microbiological testing for NTM from bronchopulmonary specimens and assessment of the presence of NTM-PD could be considered in patients with OLD with a low BMI and/or frequent exacerbations. The infographic presents data on mycobacterial cultures from 1615 patient episodes involving 1538 patients. It categorizes episodes into lung malignancy (834 episodes, 819 patients), stable OLD (553 episodes, 525 patients) and OLD in exacerbation (228 episodes, 222 patients). Total NTM isolations are 25 out of 1615 (1.5 percent), with confirmed NTM-PD in 8 cases (32 percent), all in the OLD group. The NTM isolation rate is shown in a bar graph: lung malignancy (4/834, 0.48 percent), stable OLD (13/553, 2.4 percent) and exacerbated OLD (8/228, 3.5 percent). In the OLD cohort, NTM isolation is more likely in patients with lower BMI (p=0.03), frequent exacerbators (p=0.0004) and those on inhaled corticosteroid therapy (p=0.043). NTM-PD is more likely in patients with lower BMI (p=0.043) and frequent exacerbators (p=0.023).Infographic on NTM isolation rates in lung conditions with patient data and risk factors.
Keywords: screening, atypical mycobacteria, chronic obstructive lung disease, asthma, lung cancer
Introduction
Nontuberculous mycobacteria (NTM) are opportunistic pathogens ubiquitous in the environment.1 Although there are more than 200 known NTM species, some species (such as M. avium, M. intracellulare, M. kansasii, M. xenopi, and M. abscessus) are more pathogenic than others. They predominantly cause pulmonary disease (NTM-PD), a serious chronic progressive disease often present in patients with underlying lung conditions, such as bronchiectasis, cystic fibrosis (CF), chronic obstructive pulmonary disease (COPD) and asthma.1 A recent meta-analysis2 confirmed bronchiectasis and a history of TB as comorbid respiratory diseases with the most significant increase in the odds ratio (OR) for NTM-PD. However, underlying diseases were also found to be associated with an increased OR for NTM-PD, including interstitial lung disease (OR 6.39; 95% CI 2.65–15.37), COPD (OR 6.63; 95% CI 4.57–9.63), asthma (OR, 4.15; 95% CI 2.81–6.14), solid tumors (OR, 4.66; 95% CI 1.04–20.94), as well as the use of inhaled corticosteroids (OR, 4.46; 95% CI 2.13–9.35).
Screening for NTM and NTM-PD is recommended in guidelines for patients with bronchiectasis or CF.3,4 However, despite the evidence of increased risk,2–7 neither the current COPD guidelines8 nor the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2023 report9 discusses screening for NTM or NTM-PD. In addition, it is unclear whether solid tumors (especially lung tumors) or antitumor treatments increase the risk of NTM-PD.2 A recently published Delphi consensus by European experts provides insights into the symptoms and clinical characteristics that should prompt an assessment of NTM-PD.10
However, the majority of the studies assessing NTM isolation/disease risk in patients with different lung diseases assessed the rate of comorbidities in patient’ cohorts with already isolated NTM and there is a significant gap in the knowledge regarding the yield of the testing in broader patient populations such as patients with lung malignancy or patients with obstructive lung diseases with or without lung malignancy.
In our center, there is a “reflex” testing policy for mycobacteria. This means that every bronchoscopy sample was automatically sent for mycobacterial cultures. Furthermore, the same recommendation was in place for sputum analyses, and most of the physicians were automatically sending sputum samples of patients with chronic diseases (especially those with obstructive diseases) for mycobacterial cultures. Given this background, the aim of this study was to determine the diagnostic yield of mycobacterial testing in patients with pulmonary malignancy and patients with obstructive lung disease (OLD) (COPD, asthma, and COPD/asthma overlap) with or without associated pulmonary malignancies. Given our experience with automatic testing and our centralized overview of NTM isolation rates, our hypothesis was that NTM testing yield is low in patients with pulmonary malignancy while it might be feasible in patients with obstructive lung diseases.
Methods
We retrospectively identified all patients who underwent evaluation for the presence of mycobacteria in respiratory specimens at the Department for Respiratory Diseases of the University Hospital Centre Zagreb, Croatia between January 2021 and January 2023. Patients with diagnosed pulmonary malignancy and patients with OLD with or without associated pulmonary malignancy were then included into this study and further analyzed. Respiratory specimens, including self-expectorated sputum, bronchial aspirate, bronchial wash and bronchoalveolar lavage, were directly assessed for acid-fast bacilli (AFB) and cultured for mycobacteria (both on liquid and solid media; incubation period up to 8 weeks), as previously described.11 All NTM species were identified by molecular methods (GenoType® CM/AS; Hain Lifescience GmbH, Nehren, Germany). The specimen type, collection, and number of specimens were determined by the treating physician at the time of the visit. For patients with OLD, we determined whether samples were collected during exacerbation or stable disease. COPD exacerbation and asthma were defined according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) and Global Initiative for Asthma (GINA), respectively.9,12 Separate isolation episodes for the same patient were defined as samples taken during exacerbation and stable disease at different time points during the study period. In the case of multiple sampling during stable disease or exacerbations, separate isolation episodes were defined as samples taken more than six months apart.
The main outcomes in this study were positive mycobacterial cultures, prevalence of nontuberculous mycobacteria (NTM), and the clinical significance of NTM isolates in these patient populations. According to our previous nationwide analysis,11,13 we divided NTM isolates as either potentially clinically relevant (ie., M. avium complex (MAC), M. xenopi, M. kansasii) or as species that rarely cause pulmonary disease (ie., M. fortuitum, M. gordonae, M. terrae complex). The latest criteria from four societies (ATS/IDSA/ERS/ESCMID)14 were used to assess the clinical significance of NTM isolates by assessing NTM pulmonary disease (NTM-PD).
In addition to the main demographic data, we recorded comorbidities, severity of the OLD (according to the GOLD and/or GINA criteria), medications taken for the OLD, use of immunosuppressive drugs, and the number of exacerbations in the year prior to sampling. The type and equivalent dose of inhaled corticosteroid (ICS) were also recorded.12 For patients with COPD, frequent exacerbator phenotypes were defined by the number and severity of exacerbation episodes in the previous year according to the GOLD.9 Prior history of tuberculosis or NTM-PD was defined as guideline based treatment for either tuberculosis or NTM-PD with microbiological negativisation (defined by at least 3 separately taken respiratory samples) and a minimum 12-month period between the end of treatment and current sampling episode. All data were handled confidentially and analyzed in a de-identified format to ensure the protection of patient privacy.
For statistical analysis, patient characteristics were summarized using absolute and relative frequencies and medians with interquartile ranges (IQR). Differences between patients with and without NTM infection were assessed using the Wilcoxon rank-sum test or Fisher exact test, as appropriate. Statistical significance was defined as a two-sided p-value <0.05. All analyses were performed using R software (version 4.3.2) using the packages readxl, mosaic, descr, car, and coin.
This retrospective study was conducted in accordance with the ethical standards of the institutional research committee and the principles of the World Medical Association Declaration of Helsinki. Ethical approval was obtained from the appropriate Institutional Review Board prior to data collection and analysis (02/013 AG). Given the retrospective design of the study, which involved review of existing medical records without direct patient contact or intervention, the requirement for informed consent was waived by the Institutional Review Board.
Results
In the two-year period, 2267 consecutive mycobacterial cultures from respiratory samples were obtained from 1538 patients with OLD and/or lung malignancies. Of those, 1459 had one sampling episode, 75 patients had two sampling episodes, and four patients had three sampling episodes during the study period. In total, 1621 patient sampling episodes were observed. The average number of samples taken per sampling episode (including self-expectorated sputum, bronchial aspirate, bronchial washing or bronchial lavage) was 1.4 per patient episode in the overall cohort, while it amounted to 1.7 per patient episode in patients with OLD exacerbation. The majority of the samples originated from bronchoscopy (63%; 1021/1621), 27.3 from sputum alone (442/1621) while in the remaining 9.7% (158/1621) of sampling episodes, samples originated from both bronchoscopy and the self-expectorated sputum of the same patient.
Mycobacterium tuberculosis was detected in six patients. These patients were removed from further analyses. A detailed flowchart of the number of patients and NTM isolation episodes in each subgroup is shown in Figure 1. In brief, we divided patients into those having pulmonary malignancy without OLD (n = 819) and those having OLD (with or without associated pulmonary malignancy) (n = 747). Patients with OLD were further divided into those sampled during stable OLD (n = 525) and those sampled during exacerbations (n = 222).
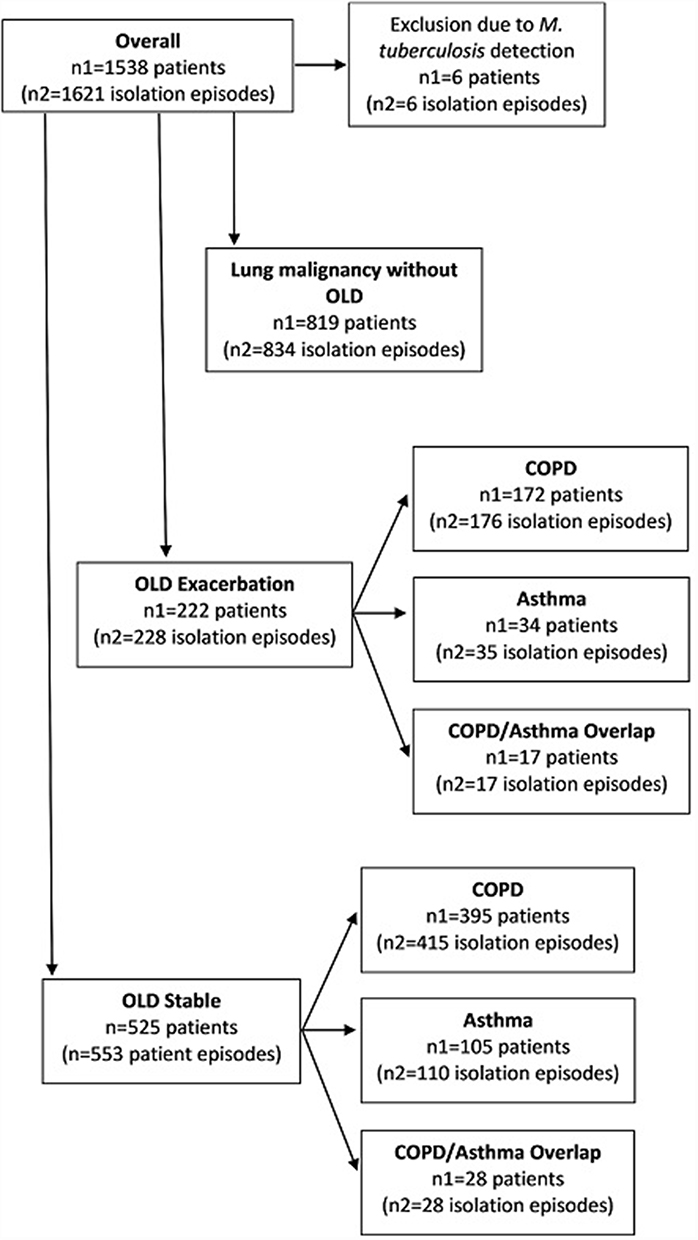 |
Figure 1 Flowchart of all patients (n1) and isolation episodes (n2) tested for nontuberculous mycobacteria during the study period. Patients subgroups included: patients with lung malignancy without obstructive lung diseases (OLD), patients with OLD (either chronic obstructive pulmonary disease (COPD) or asthma) in exacerbation, and patients with OLD in the stable phase of the disease. Patients having both OLD and malignancy were included in the OLD subgroups. Note: Patients may appear in multiple subgroups; totals do not sum to 100%. |
Of the 1615 patient episodes, mycobacteria were isolated from 25 (1.6%). In total, 19 NTM isolates were species of potential clinical relevance (12 MAC and 7 M. xenopi), while the remaining six were M. gordonae (n = 2), M. fortuitum (n = 2), M. mucogenicum (n = 1), and Mycobacterium spp. (n = 1). The prevalence of NTM isolation was 0.48% (4/834) in patients with episodes of lung malignancies, 2.4% (13/553) in those with stable OLD, and 3.5% (8/228) in those with OLD exacerbation. Nineteen (19/25, 76%) NTM isolation episodes originated from patients diagnosed with OLD and four NTM (4/25, 16%) were isolated from patients with lung malignancy without OLD, while two NTM isolates (2/25; 8%) came from patients with both lung malignancy and OLD. Overall, 8/25 (32%; 5 MAC and 3 M. xenopi) isolation episodes met the criteria for NTM-PD in all patients with OLD. In patients with lung malignancies, there was only one potentially clinically relevant NTM isolate (M. avium); however, there were no criteria for NTM-PD. The likelihood of NTM mycobacterial isolation in the overall episodes was significantly higher in patients with lower BMI (p = 0.005), prior history of TB or NTM-PD (p = 0.004), bronchiectasis (p = 0.003), asthma (p = 0.021), COPD (p = 0.039), frequent exacerbations (p = 0.004), and ICS therapy (p = 0.012), whereas it was less likely in patients with pulmonary malignancies (p < 0.001) (Table 1).
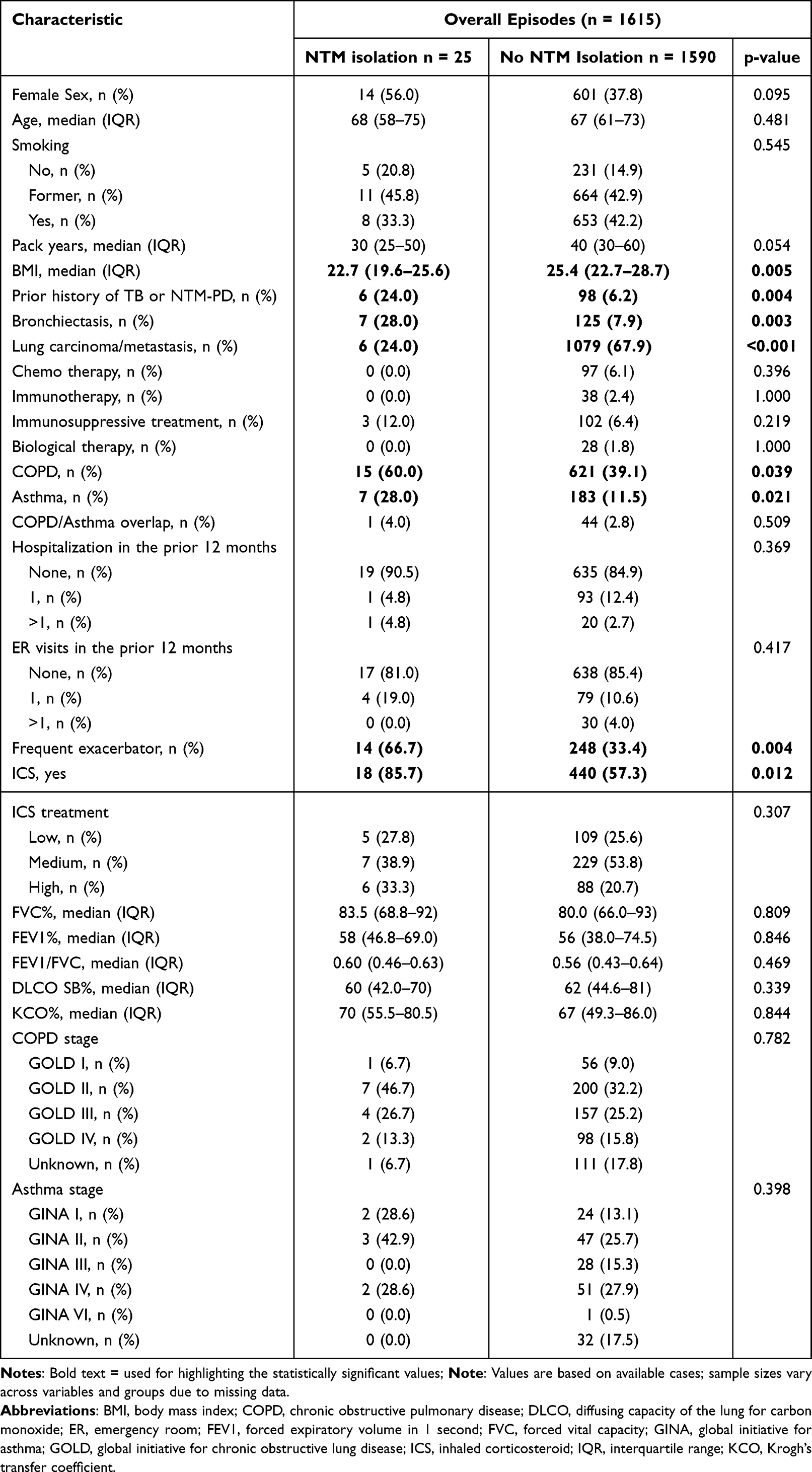 |
Table 1 Comparison of Characteristics Between Patients with and without Nontuberculous Mycobacteria (NTM) Isolation in All Recorded Episodes |
In total, 781 (48.2%) episodes occurred in patients with OLD, with or without malignancy. Within the OLD sub-cohort, 553 (70.8%) patient episodes were recorded during periods of stable disease, while the remaining 228 (29.2%) patient episodes were recorded during exacerbation of the underlying obstructive disease. Patients with COPD constituted the majority of both the stable OLD subgroup (443/553; 79.8%) and the OLD exacerbation subgroup (193/228; 84.5%). In the OLD sub-cohort, the likelihood of isolating NTM was higher in patients with lower BMI (p = 0.030), frequent exacerbators (p = 0.004), and patients receiving ICS treatment (p = 0.012). The frequency of exacerbator type and ICS treatment remained significant in the OLD exacerbation subgroup (p = 0.009 and 0.057, respectively) but showed no significance in the stable OLD subgroup (Table 2).
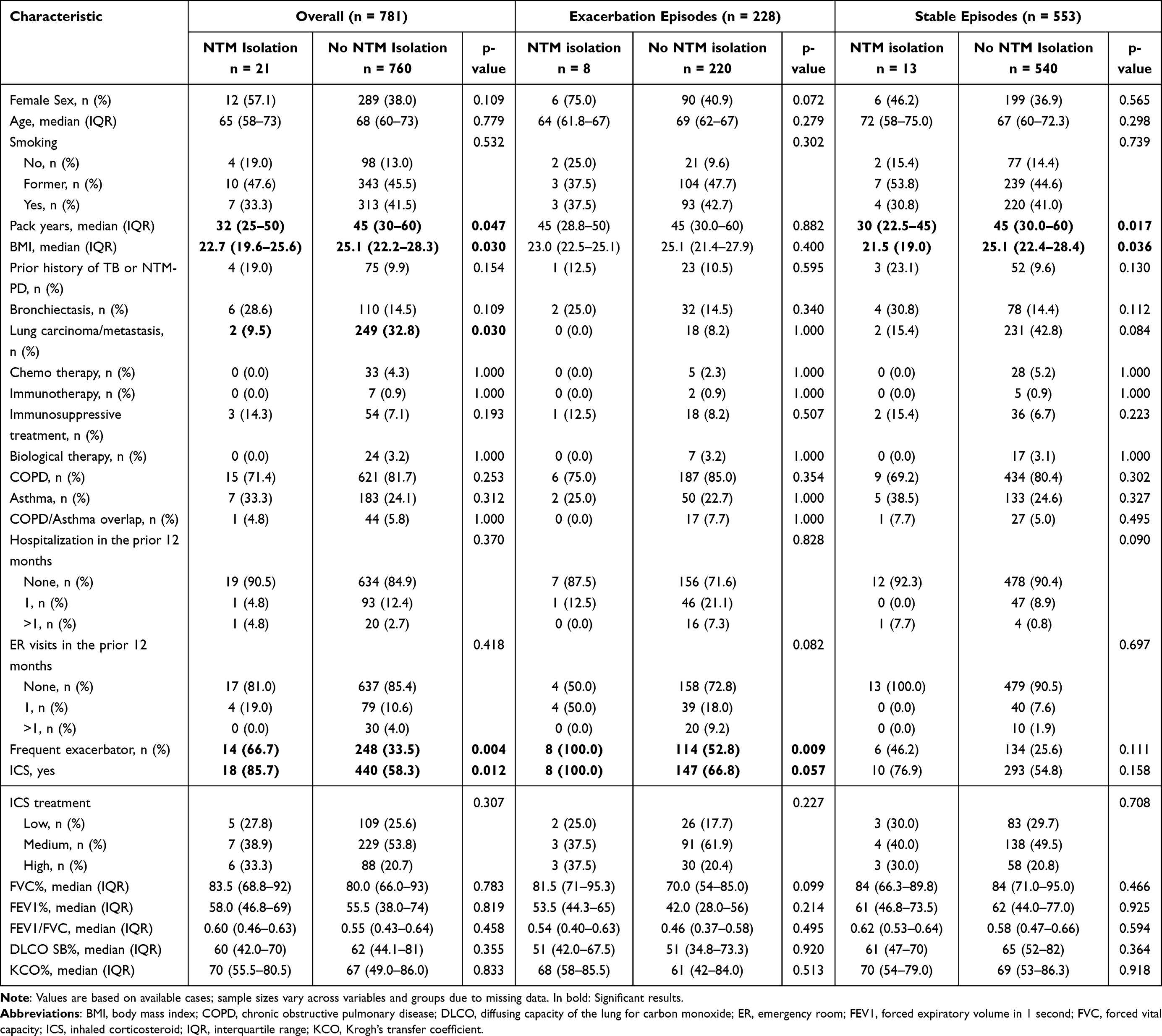 |
Table 2 Comparison of Characteristics Between Patients with and without Nontuberculous Mycobacteria (NTM) Isolation in Obstructive Lung Diseases Episodes, Additionally Differentiated by Exacerbation and Stable Phases of Disease |
Within the NTM isolation episodes in the OLD cohort, NTM-PD was diagnosed in 4/8 (50%) patients with OLD exacerbation and in 4/8 (50%) patients with stable OLD. The likelihood of having NTM-PD in the OLD cohort was significantly higher in patients with a lower BMI (p = 0.043), prior history of TB or NTM-PD (p = 0.038), and frequent exacerbations (p = 0.023); however, there was no difference in relation to associated bronchiectasis or severity of the disease (obstruction) according to GOLD or GINA (Table 3).
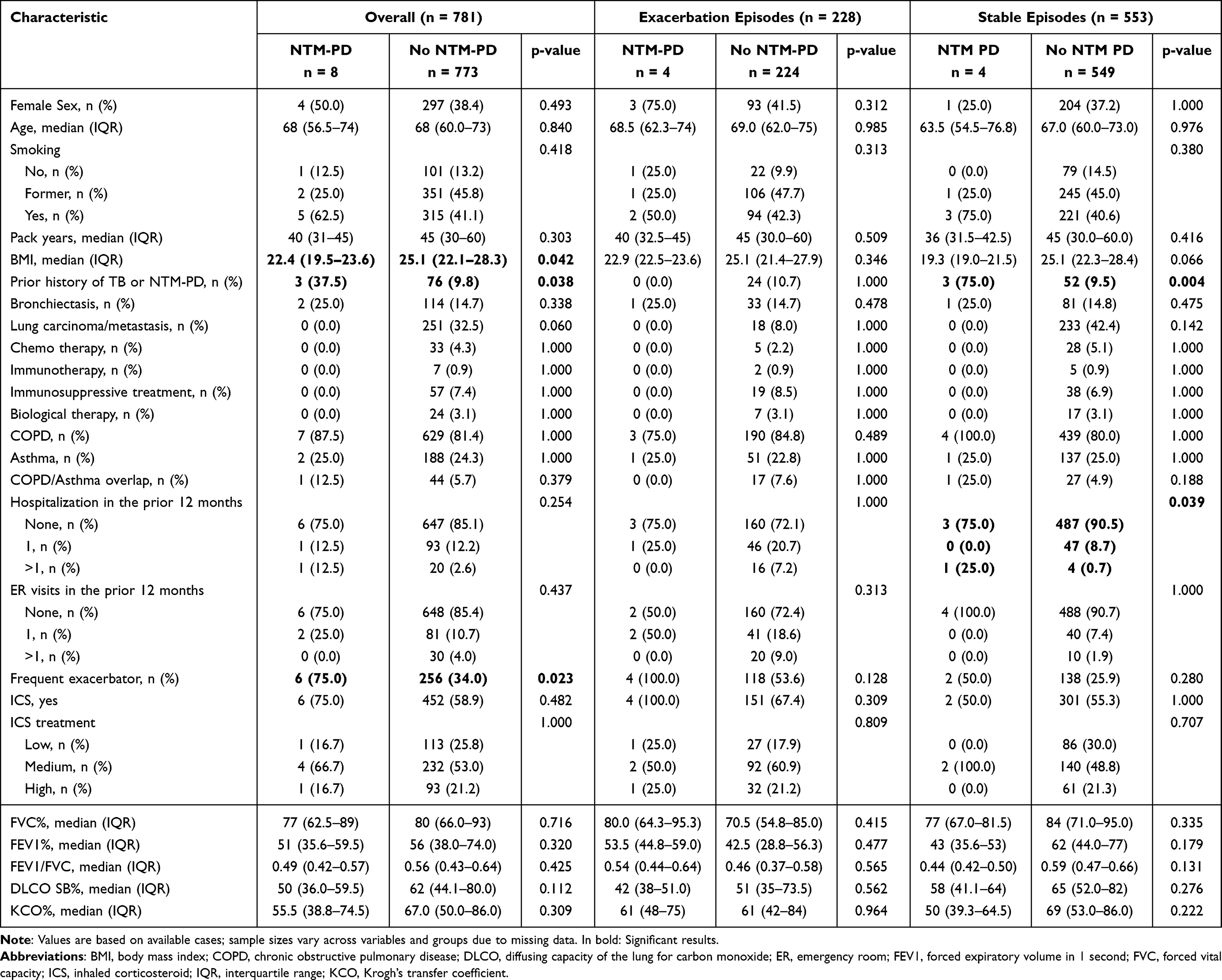 |
Table 3 Comparison of Characteristics Between Patients with and without Nontuberculous Mycobacteria Pulmonary Disease (NTM-PD) in Obstructive Lung Diseases Episodes, Additionally Differentiated by Exacerbation and Stable Phases of Disease |
Discussion
This study assessed the yield of NTM testing in patients with OLD (with or without pulmonary malignancy or pulmonary malignancies alone), and the relevance of NTM isolation from bronchopulmonary specimens in individuals from these groups. While the yield of NTM isolation was generally low in patients in our cohort, and standardized testing for NTMs cannot be recommended in our setting in these patient groups, routine evaluation for NTM-PD could be considered in OLD patients with low BMI and/or frequent exacerbations.
In our cohort, the yield of NTM testing was low, particularly in patients with pulmonary malignancies without an OLD. In a recent meta-analysis of risk factors, the presence of solid tumors was shown to be associated with NTM-PD (OR 4.66; 95% CI 1.04–20.94) but it was also emphasized that the association might be a result of cancer therapy rather than the cancer itself.2 Indeed, in our cohort, the majority of patients were tested for NTM at the time of malignancy diagnosis (754/834; 90.4%) rather than during systemic oncological treatment. However, all four NTM isolates originated from patients who were not receiving oncological treatment, and none had clinical significance.
The yield of testing was higher in the OLD cohort, especially in the subgroup of patients with samples taken during the exacerbation of obstructive disease, which amounted to 3.5% (8/228). This finding is somewhat higher than that of a study from Hong Kong showing a 1.4% prevalence of positive NTM cultures in patients with acute exacerbations of COPD (AECOPD) but significantly lower than the 22% prevalence in AECOPD patients in a study from the Netherlands.15,16 Both of these studies were prospective but had differences in the mycobacterial cultivation methods (only solid media was used in Ko et al),16 as well as geographically different populations. The difference in the prevalence of NTM isolation between our cohort and the cohort from the Netherlands might partly be explained by the retrospective nature of our study, the inclusion of both asthma and COPD patients, and the differences in the overall NTM prevalence between geographic regions. However, despite the differences in NTM isolation rates, the prevalence of NTM-PD in our cohort (1.75%, 4/229) was similar to that in the Netherlands cohort (1.4%, 1/73).15 Furthermore, although our cohort also included patients with asthma, the majority of NTM isolates and NTM-PD cases were from COPD patients. The connection between NTMs and COPD exacerbations is not fully understood. It is possible that changed airway environment predisposes for NTM but also that prior colonization with NTM drives the exacerbations. Additionally, higher uptake of both inhaled and systemic corticosteroids during acute exacerbations might be an additional factor driving increased rates of NTM detection. However, part of the association might also be selection bias given that clinicians are more likely to send for mycobacterial cultures during exacerbations than in the stable phase of the disease.
Both asthma (OR 4.15; 95% CI 2.81–6.14) and COPD (OR 6.63; 95% CI 4.57–9.63) have been associated with an increased risk of NTM-PD in a recent meta-analysis.2 Furthermore, other factors associated with immunosuppression, including the use of inhaled corticosteroids (OR, 4.46; 95% CI 2.13–9.35) and oral corticosteroids (OR 3.37, 95% CI 0.82–13.75), medications often used in the treatment of these respiratory diseases. This was also confirmed in a nationwide study conducted in the Croatian population of patients with NTM-PD.6 In our current study, ICS treatment and a frequent exacerbator phenotype were significantly associated with a greater likelihood of NTM isolation both in the overall OLD cohort, as well as in the AEOLD subgroup but showed no significance in the subgroup of patients with stable OLD. Expectedly, low BMI was significantly associated with both the likelihood of NTM isolation but also with the likelihood of NTM-PD in the overall cohort. Namely, diagnosis of NTM-PD in the OLD cohort was associated with lower BMI (p = 0.043), prior history of TB or NTM-PD, and frequent exacerbator phenotype; however, there was no difference in relation to associated bronchiectasis or severity of the disease (obstruction) according to GOLD or GINA. In our study, ICS therapy was not associated with the likelihood of NTM-PD. It is possible that ICS therapy may facilitate transient airway colonization by NTM but that progression to NTM-PD requires additional host and disease-specific factors. Further prospective studies are needed to fully understand the role of ICS in the development of NTM-PD in patients with chronic obstructive diseases.
The major strength of this study is the cohort size and the fact that it is, to our best knowledge, the only one that evaluated the prevalence of NTM in patients with stable asthma or COPD and/or patients with pulmonary malignancies and one of a very few that assessed the yield of mycobacterial cultures in patients with exacerbation of chronic obstructive diseases.
Given the growing interest in NTM-PD and NTM testing in patients with respiratory comorbidities, studies such as ours are necessary to address the feasibility of unstructured testing/screening for NTM in such patient populations. According to our results, the yield of NTM testing in patients with OLD and/or lung malignancies was generally low. However, testing might be feasible in patients with OLD with low BMI and/or frequent exacerbations.
Although our study has several strengths, it has some limitations. The major weakness of this study is that it was conducted at a single center and was retrospective. However, our center is the largest respiratory center in Croatia and has a history of an “automatic” testing for mycobacteria during bronchoscopy and in patients with productive cough, especially those with obstructive lung diseases. Therefore, we were able to collect a large cohort that likely reflects the overall patient population that gravitates to our center. Furthermore, although the average number of samples amounts to 1.4 per patient in the overall cohort (and 1.7 in the subgroup with OLD exacerbation), the majority of samples (>60%) originated from bronchoscopy and roughly 10% patients had mycobacterial cultures from both sputum as well as samples taken through bronchoscopy. Nevertheless, because this was a retrospective study, there is a potential selection bias associated with physician-directed sampling and we cannot be fully sure that the yield would not be higher in a prospective study. Also, another limitation is a relatively small overall rate of NTM detection. It is well known that NTM isolation frequency and NTM-PD prevalence vary across different continents and European countries, our findings cannot be fully translatable to other countries. However, they might be a reference point for countries with a similar incidence and prevalence of NTM-PD.
Conclusion
In this study, the yield of NTM testing in patients with OLD and/or lung malignancies was low. Routine microbiological testing for NTM from bronchopulmonary specimens and assessment of the presence of NTM-PD could be considered in patients with OLD with low BMI and/or frequent exacerbations.
Data Sharing Statement
The data that support the findings of this study are not publicly available owing to ethical and patient confidentiality regulations; however, aggregated data are available from the first and/or corresponding author upon reasonable request.
Ethics Approval
The study was approved by the Institutional Review Board (IRB) of University Hospital Centre Zagreb.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the University Hospital Center Zagreb, Zagreb, Croatia, and Clinical Infectious Diseases Research Center Borstel, Borstel, Germany. C.L. was funded by the German Center for Infection Research (DZIF) under Grant Agreement No.02.709.
Disclosure
Christoph Lange reports personal fees from Insmed, personal fees from Gilead, personal fees from Med Update, personal fees from Med Update Europe, personal fees from Biomerieux, outside the submitted work. The authors declare that they have no other conflicts of interest in this work.
References
1. Cowman S, van Ingen J, Griffith DE, Loebinger MR. Non-tuberculous mycobacterial pulmonary disease. Eur Respir J. 2019;54(1):1900250. doi:10.1183/13993003.00250-2019
2. Loebinger MR, Quint JK, van der Laan R, et al. Risk factors for nontuberculous mycobacterial pulmonary disease: a systematic literature review and meta-analysis. Chest. 2023;164(5):1115–13. doi:10.1016/j.chest.2023.06.014
3. Polverino E, Goeminne PC, McDonnell MJ, et al. European Respiratory Society guidelines for the management of adult bronchiectasis. Eur Respir J. 2017;50(3):1700629. doi:10.1183/13993003.00629-2017
4. Floto RA, Olivier KN, Saiman L, et al. US Cystic Fibrosis Foundation and European Cystic Fibrosis Society consensus recommendations for the management of non-tuberculous mycobacteria in individuals with cystic fibrosis. Thorax. 2016;71(suppl 1):i1–i22. doi:10.1136/thoraxjnl-2015-207360
5. Andréjak C, Nielsen R, Thomsen VØ, Duhaut P, Sørensen HT, Thomsen RW. Chronic respiratory disease, inhaled corticosteroids and risk of non-tuberculous mycobacteriosis. Thorax. 2013;68(3):256–262. doi:10.1136/thoraxjnl-2012-201772
6. Glodic G, Samarzija M, Sabol I, et al. Risk factors for nontuberculous mycobacterial pulmonary disease (NTM-PD) in Croatia. Wien Klin Wochenschr. 2021;133(21–22):1195–1200. doi:10.1007/s00508-021-01923-x
7. Archontakis Barakakis P, Tran T, You JY, et al. High versus medium dose of inhaled corticosteroid in chronic obstructive lung disease: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2023;18:469–482. doi:10.2147/COPD.S401736
8. Wedzicha JA, Calverley PMA, Albert RK, et al. Prevention of COPD exacerbations: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2017;50(3):1602265. doi:10.1183/13993003.02265-2016
9. Agustí A, Celli BR, Criner GJ, et al. Global Initiative for Chronic Obstructive Lung Disease 2023 report: GOLD executive summary. Eur Respir J. 2023;61(4):2300239. doi:10.1183/13993003.00239-2023
10. Loebinger MR, Aliberti S, Haworth C, et al. Patients at risk of nontuberculous mycobacterial pulmonary disease who need testing evaluated using a modified Delphi process by European experts. ERJ Open Res. 2024;10(5):00791–2023. doi:10.1183/23120541.00791-2023
11. Jankovic M, Sabol I, Zmak L, et al. Microbiological criteria in non-tuberculous mycobacteria pulmonary disease: a tool for diagnosis and epidemiology. Int J Tuberc Lung Dis. 2016;20(7):934–940. doi:10.5588/ijtld.15.0633
12. Global Initiative for Asthma. Global strategy for asthma management and prevention, 2023. Available from: https://ginasthma.org/.
13. Makek MJ, Glodic G, Sabol I, et al. Nationwide evaluation of treatment outcomes and survival of patients with non-tuberculous mycobacterial pulmonary disease. Int J Tuberc Lung Dis. 2024;28(10):482–487. doi:10.5588/ijtld.24.0068
14. Daley CL, Iaccarino JM, Lange C, et al. Treatment of nontuberculous mycobacterial pulmonary disease: an official ATS/ERS/ESCMID/IDSA clinical practice guideline. Eur Respir J. 2020;56(1):2000535. doi:10.1183/13993003.00535-2020
15. Hoefsloot W, van Ingen J, Magis-Escurra C, et al. Prevalence of nontuberculous mycobacteria in COPD patients with exacerbations. J Infect. 2013;66(6):542–545. doi:10.1016/j.jinf.2012.12.011
16. Ko FW, Ip M, Chan PK, et al. A 1-year prospective study of the infectious etiology in patients hospitalized with acute exacerbations of COPD. Chest. 2007;131(1):44–52. doi:10.1378/chest.06-1355
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Exercise Rehabilitation and Chronic Respiratory Diseases: Effects, Mechanisms, and Therapeutic Benefits
Xiong T, Bai X, Wei X, Wang L, Li F, Shi H, Shi Y
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1251-1266
Published Date: 19 June 2023