")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Diagnostic Values of Serum Levels of Homocysteine, Heat Shock Protein 70 and High-Sensitivity C-Reactive Protein for Predicting Vascular Cognitive Impairment
Received 14 December 2021
Accepted for publication 3 February 2022
Published 8 March 2022 Volume 2022:18 Pages 525—533
DOI https://doi.org/10.2147/NDT.S354022
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Taro Kishi
Li Cao,1,2 Zhongwu Sun1
1Department of Neurology, The First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, 230022, People’s Republic of China; 2Department of Neurology, Anhui No.2 Provincial People’s Hospital, Hefei, Anhui, 230041, People’s Republic of China
Correspondence: Zhongwu Sun, Department of Neurology, The First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, 230022, People’s Republic of China, Email [email protected]
Introduction: Vascular cognitive impairment is one of the main clinical manifestations of cerebral small vessel disease (CSVD). Reliable molecular markers are needed urgently to predict cognitive impairments in CSVD patients. This study aimed to investigate the possible diagnostic values of serum levels of Hcy, Hsp70 and hs-CRP for predicting vascular cognitive impairment in patients with CSVD.
Methods: According to the presence of CSVD and cognitive impairment (CI), healthy patients and CSVD patients were divided into three groups. Serum Hcy, HSP70 and hs-CRP were abnormal in the CI group. Clinical characteristics and MOCA cognitive function score statistics were performed for the three groups: the control group, CSVD without cognitive impairment group and CSVD with cognitive impairment group. Finally, Hcy, HSP70 and hs-CRP were correlated with MOCA to analyze the correlation between serum Hcy, HSP70 and hs-CRP and cognitive dysfunction caused by CSVD.
Results: The levels of serum Hcy, Hsp70, and hsCRP had significantly higher expression in the CSVD groups than those in the control group (p< 0.05). Moreover, basic clinical characteristics, cardiovascular risk factors and other clinical details had no significantly differences among the three groups. Serum Hcy, Hsp70 and hs-CRP levels were negatively correlated with MoCA total scores.
Conclusion: Serum levels of Hcy, HSP70 and hs-CRP were negatively correlated with cognitive impairment caused by CSVD, which could be used as a predictor to predict the risk of cognitive impairment caused by CSVD.
Keywords: cerebral small vessel disease, homocysteine, heat shock protein 70, high-sensitivity C-reactive protein, vascular cognitive impairment
Introduction
Cerebral small vessel disease (CSVD) is regarded as a group of pathological neurological processes.1 It has various etiologies and affects the small venules, arterioles, arteries and capillaries in the brain.2 Persons above the age of 80 years are common suffering from CSVD and at high risk of progressing to dementia or Alzheimer’s disease.3 CSVD is mainly caused by static focal cerebrovascular diseases, which are initiated by elevated blood-brain barrier permeability, including lacunar infarction, cerebral micro-bleeding, and micro-leukoaraiosis.4,5 Vascular cognitive impairment is one of the main clinical manifestations of CSVD, such as poor verbal fluency, poor word list generation, fading memory, short sustained attention, impaired motor programming and other executive function deficits.6–8 Vascular mild cognitive impairment (VMCI) is caused by vascular diseases and at risk of developing cognitive impairment.9 Most patients with VMCI have mild symptoms and not severe cognitive deficits, which do not reach the level of dementia.9,10 Along with the aging of population, dementia became a social problem disturbing our life. Reliable molecular markers are needed urgently to predict cognitive impairments in CSVD patients.
Homocysteine (Hcy) has been proposed to be a risk factor for cognitive impairment and dementia.11 Hcy can alter methylation reaction and directly affect brain function.11 It was proven that Hcy level has a positive correlation with SVD, especially leukoaraiosis and silent brain infarctions.12 Heat shock protein 70 (Hsp70) is typically expressed at low levels in brain but becomes the most abundant protein in all cells following ischemia, heat shock and other injuries.13 It is a crucial regulator of proteostasis and helps misfolded proteins in neurodegenerative diseases to amend incorrect folds by aggregation, refolding or degradation.13 Hsp70 may play a therapeutic role for the assistance of vascular reactivity and treatment of neurodegenerative diseases associated with cognitive disturbances, such as Alzheimer’s disease.14,15 High-sensitivity C-reactive protein (hs-CRP), an acute inflammatory biomarker, has a critical role in our immune system.16 The concentration of hs-CRP in the body is associated with long-term cognitive impairment and dementia.17 It means that a higher level of hs-CRP is always along with worse cognitive function. Thus, hs-CRP may serve as a potential biomarker for cognitive decline.17 For these reasons, this study aimed to investigate the possible diagnostic values of serum levels of Hcy, Hsp70 and hs-CRP for predicting vascular cognitive impairment in patients with CSVD.
Methods
Participants
A total of two hundred ninety-two participants were enrolled in our study, dividing into two groups: healthy group (n=103) and CSVD group (n=189). All applicants or their legal guardians agreed to participate by informing the research content and signing informed consent. Our study conformed to the Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects and was fully approved by the Ethics Committee of Anhui No.2 Provincial People’s Hospital.
The control group were randomly selected based on physical examination. All healthy applicants should satisfy the criteria: 1) no history of cognitive dysfunction and dementia; 2) no history of brain injury or intracranial lesions; 3) no visual or hearing loss. The patients in the CSVD group with the following criteria were included in our research: 1) radiological phenotype up to the diagnostic criteria of CSVD, including small deep brain infarcts, white matter lesions, deep brain haemorrhages and microbleeds) 2) a definite diagnosis of leukoaraiosis or lacunar infarction 3) a definite diagnosis of lesions less than 15 mm in size under the cerebral cortex; 4) no communication barriers; 5) no treatment of nootropic drugs; 6) no severe system diseases, such as heart, kidney or hematopoietic diseases; 7) no history or diagnosis of cognitive dysfunction and dementia.18,19 Two hundred sixty-nine eligible participants from 292 applicants were tested by the Montreal Cognitive Assessment (MoCA) to evaluate the level of patients’ cognitive function.20 Twenty-three persons were excluded due to refused MoCA, meaningless or not interested and incomplete processes. All eligible participants were divided into three group: the control group (n=92), CSVD without cognitive impairment group (CSVD-non-CI group) (n=87) and CSVD with cognitive impairment group (CSVD-CI group) (n=90). The diagnosis of cognitive impairment was based on Guidelines for dementia and cognitive impairment in China: the diagnosis and treatment of mild cognitive impairment.
Data Collection
The basic parameters of the participants were recorded at their First admissions, including sex, age, education history, smoking history, alcohol history, body mass index (BMI) and past medical history (eg, hypertension, hyperlipidemia and diabetes history). Routine and neurological physical examination were coordinately performed for all participants, followed by cranial MRI, carotid and cardiac ultrasound, electrocardiography, brain CT and other examinations. Overnight fasting venous blood samples obtained to detect the levels of Hcy, Hsp70, hs-CRP, blood glucose, triglyceride, cholesterol, low-density lipoprotein cholesterol (LDL-CH) and high-density lipoprotein cholesterol (HDL-CH) in the body. Brain CT and cranial MRI examined the healthy group.
Laboratory Procedures
All the blood samples were collected venipuncture into Ethylene Diamine Tetraacetic Acid-vacutainer (BD Vacutainer®, USA) and centrifuged as soon as possible. Serum samples were obtained after centrifugation at 500g for 15min and stored as aliquots at minus 80°C until use. Concentrations of Hcy, Hsp70 and hs-CRP were measured by chemiluminescence immunoassay. Each experiment was repeated at least three times.
Statistical Analysis
Statistical Package for the Social Sciences (SPSS) Version 23.0 software (SPSS Inc., Chicago, IL) was used for data analysis and calculation. All data were represented as mean ± standard deviation (SD) with at least three independent repeated tests. Comparisons between the two groups were performed by the t-test, while comparisons among multiple groups were performed by one-way analysis of variance (ANOVA). Pearson’s correlation was performed to analyze the correlation between variables. P<0.05 was considered as statistically significant.
Results
Flow Diagram of the Study
As shown in Figure 1, a flow chart summarized the derivation of the incidence sample in the study. A total of 269 applicants were taken in the final MoCA test except for 23 participants refusing cognitive function assessment, ten persons feeling meaningless or not interested, and 13 persons with unfinished all processes. The remaining participants were divided into three groups and collected their blood samples.
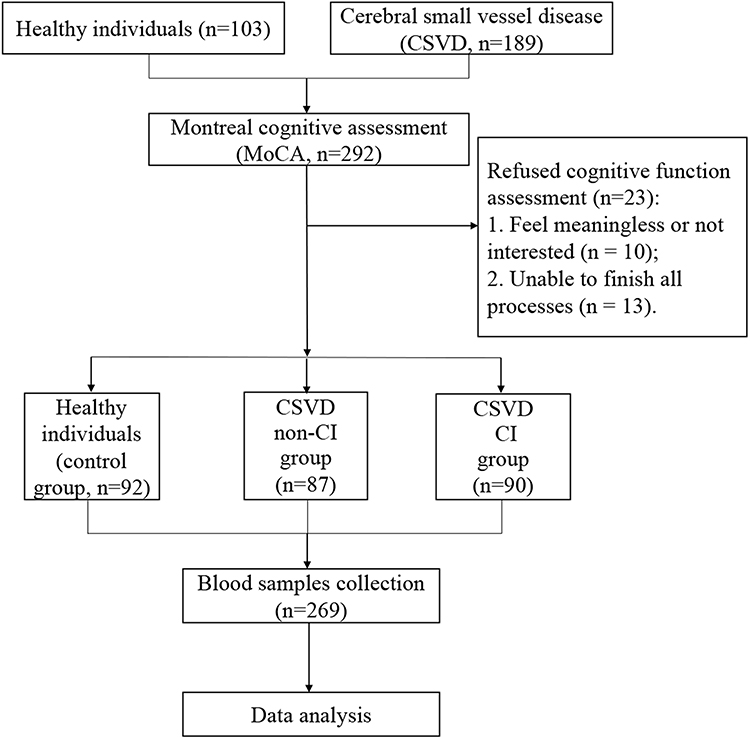 |
Figure 1 Flow diagram of the study. |
Characteristics of the Participates
The participants’ basic characteristics in the control group, CSVD-non-CI group and CSVD-CI group were detailed in Table 1. There was no significant difference in age, gender, education year, BMI, hypertension history, hyperlipidemia history, diabetes history, smoking history and alcohol history among the three groups (p>0.05). No distinctive difference was found among the three groups in blood glucose, triglyceride, cholesterol, HDL-CH and LDL-CH (P>0.05). However, serum Hcy, Hsp70 and hs-CRP levels were dramatically higher in the CSVD-CI group than those in the control group (P<0.01). The concentrations of serum Hcy, Hsp70 and hs-CRP in the CSVD-non-CI group were lower than those in the CSVD-CI group.
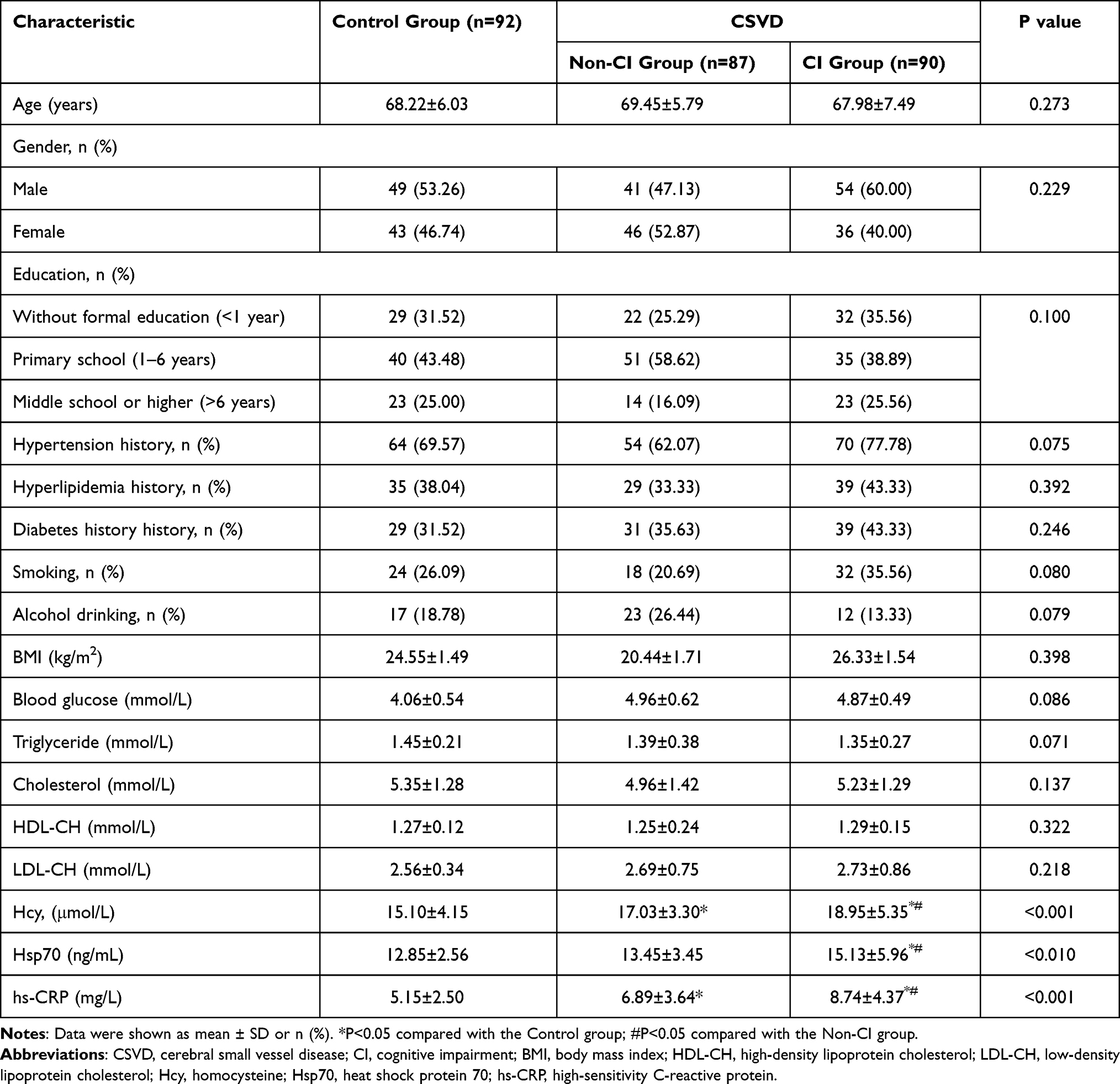 |
Table 1 Clinical Characteristics of Control Group, CSVD Non-CI Group and CSVD CI Group |
Comparisons of the MoCA Scores Among the Control, CSVD-Non-CI, and CSVD-CI Groups
As shown in Table 2, normal controls had an average score of 27.5, compared with 26.29 in the CSVD-non-CI group and 23.25 in the CSVD-CI group. The mean MoCA score of the CSVD-CI group was significantly lower than that in the CSVD-non-CI group and control group (P<0.001) (Figure 2D). The scores of all cognitive domains in the CSVD-non-CI group were significantly higher than those in the CSVD-CI group (P<0.05). Among all the domains, Abstract thinking, Delayed recall, and Orientation were gradually dramatically lower from healthy group to cognitive impairment group (P<0.05). The scores of the subdomain Language ability, Visuospatial ability and executive function and Object naming in the CSVD-non-CI group performed the highest among the three groups.
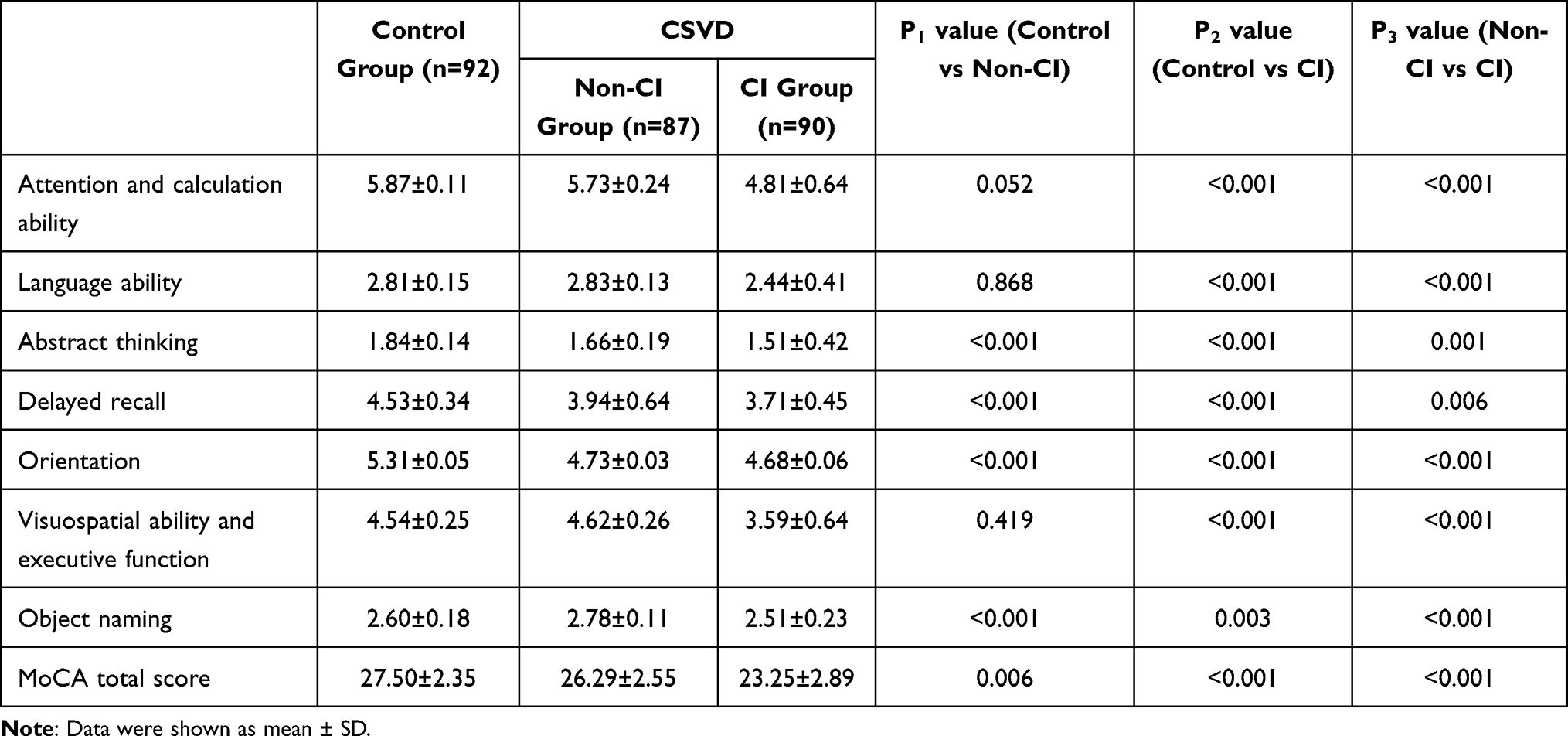 |
Table 2 The MoCA Total Scores of Control Group, CSVD Non-CI Group and CSVD CI Group |
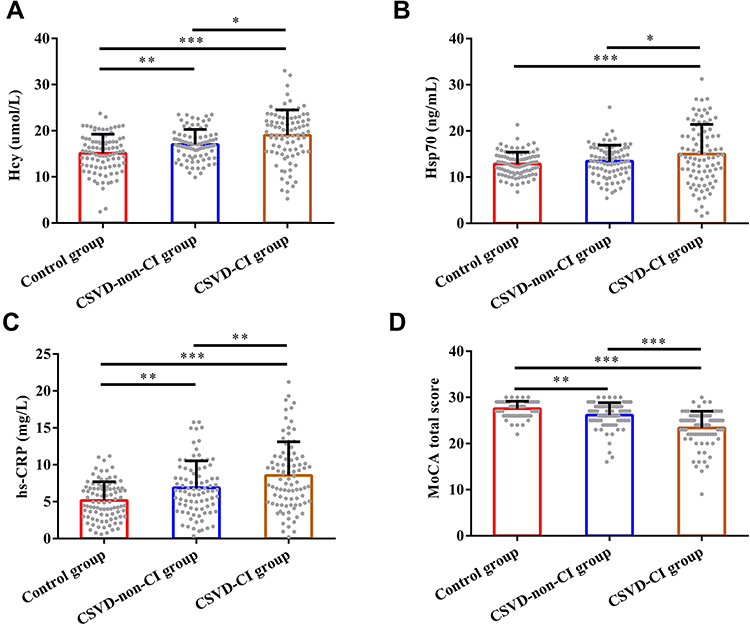 |
Figure 2 Comparisons of Hcy (A), Hsp70 (B), hs-CRP (C) and MoCA total score (D) according to the changes of control group, CSVD non-CI group and CSVD CI group. The data presented are mean ± SD showing all the data points. *p < 0.05, **p < 0.01, ***p < 0.001. |
Comparisons of Serum Hcy, Hsp70 and hs-CRP Levels Among the Control, CSVD-Non-CI, and CSVD-CI Groups
The levels of serum Hcy and hs-CRP in the CSVD groups were significantly increased compared with the healthy controls (all p<0.01) (Figure 2A and C). Serum Hcy, Hsp70 and hs-CRP levels in the CI group were significantly higher than those in the non-CI group (all p<0.05). There was no significant difference in serum hsp70 levels between the control and CSVD-non-CI groups (Figure 2B).
Then, we demonstrated Pearson correlation to further clarify the correlation between MoCA scores and the concentrations of Hcy, Hsp70, hs-CRP in the CI group (Figure 3). It showed that serum Hcy, Hsp70 and hs-CRP levels were negatively correlated with MoCA total scores (all p<0.01).
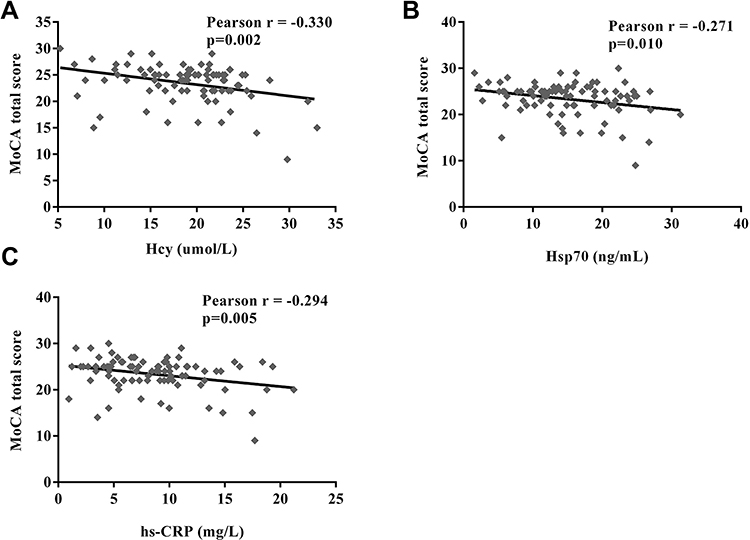 |
Figure 3 Spearman correlations between MoCA total score and Hcy (A), Hsp70 (B), hs-CRP (C) in CSVD with CI. |
Discussions
Small vessel diseases could affect various organs and areas in our body. Nowadays, CSVD was thought to be one of the leading causes of vascular cognitive impairment.2 The clinical features of vascular cognitive impairment associated with CSVD include balance dysfunction (having frequent falls or unable to walk),21 mood disturbances (apathy or depressive symptoms),22 and urinary disturbances (incontinence).23 In the early stage, these dysfunctions usually are indistinct and hard to realize. The final stage is cognitive deficits which fit the criteria for dementia. The patients with cognitive impairment usually have blood supply problems. The thalamus is a deep cerebral structure which is sensitive to changes in blood supply.24 The thalamic nuclein, particularly the pulvinar nucleus, is extensively connected with cortical (sensory cortices, posterior parietal cortex, prefrontal cortex) and subcortical regions (superior colliculus, amygdala).25–27 The previous studies have shown that the pulvinar is indispensable in both multisensory processing and cognitive and emotional functions.25,26,28,29 Therefore, due to blood supply problems in the pulvinar nucleus, vascular cognitive impairment can cause abnormal sensory, emotional, and cognitive response. It was considered that vascular cognitive impairment associated with CSVD is a chronic and progressive decline of cognitive status, final to dementia.30
In this study, we aimed to find valuable targets to predict vascular cognitive impairment in patients with CSVD. Our study assessed the diagnostic values of serum Hcy, Hsp70 and hs-CRP levels for predicting vascular cognitive impairment in patients with CSVD. The results showed that the levels of serum Hcy, Hsp70 and hsCRP had significantly higher expression in the CSVD groups than those in the control group (p<0.05). Moreover, basic clinical characteristics (age, gender, BMI and education), cardiovascular risk factors (hypertension, hyperlipidemia, diabetes) and other clinical details (smoking, drinking history) had no significantly differences among the three groups. It meant Hcy, Hsp70 and hs-CRP might be potential predictors for the occurrence of vascular cognitive impairment in patients with CSVD.
Homocysteine (Hcy) is a thiol-containing amino acid and a precursor for the metabolism of methionine.31 Hcy level could affect brain function and associate with CSVD.11,12 It was also known the toxicity of Hcy was related to neurons and neurodegenerative disease32,33 and associated with proteins involved in blood vessel.34 Increased concentrations of plasma total Hcy may be a risk factor for cognitive impairment, which induced DNA damage in neurons then associates with vascular disease.35,36 A higher level of Hcy showed to be associated with severer cognitive decline.37 Elevated homocysteic acid, a metabolite of homocysteine, may also cause neuronal dysfunction.38 As a cellular defense response to misfolded proteins, heat shock proteins are essential regulators in normal neural, physiological function and cell stress responses.39 Hsp70 is abundantly expressed in all cell types following cerebral ischemia, responding to misfolded proteins.13 In neurodegenerative diseases, Hsp70 is a crucial regulator of proteostasis, which induces misfolded proteins to alter incorrect folds by aggregation, refolding or degradation.13 It was demonstrated that overexpression of Hsp70 could cross the blood-brain barrier and protect the brain against cerebral infarction.40 Therefore, it may play a role in the treatment of neurodegenerative diseases associated with cognitive disturbances.14,15
Elevated CRP concentration is a cardiovascular risk factor associated with cognitive disorders and dementia.41 CRP is an acute hepatic biomarker in systemic inflammation correlated with cognitive function.42 It also demonstrated that higher concentrations of hs-CRP in patients led to cognitive dysfunction after cerebral infarction.42 Therefore, it could be a potential clinical biomarker to evaluate the level of cognitive decline.17
In our study, the concentrations of serum Hcy, hs-CRP in the CSVD groups were significantly higher than those in the healthy controls. Serum Hcy, Hsp70 and hs-CRP levels in the CI group were significantly higher than those in the non-CI group. Then we investigated the correlation between MoCA scores and the levels of Hcy, Hsp70 and hs-CRP in the CSVD-CI group. The results showed that serum Hcy, Hsp70 and hs-CRP levels were negatively correlated with MoCA total scores (all p<0.01). These results indicated that Hcy Hsp70 and hs-CRP might be potential predictors to predict the risk of vascular cognitive impairment caused by CSVD.
However, our study also had some limitations which should be addressed in the future. Firstly, the current number of final participants was lack of statistical power and limited the accuracy of the results. Only 292 persons were included in the study. Further studies should recruit more eligible participants to ensure accurate and specific results. Secondly, we only demonstrate the correlations but did not quantify the strength of the correlations between three factors’ levels and risk of cognitive impairment associated with CSVD. Odds ratios and logistic regression comparisons should be evaluated in the follow-up study. In addition, white hyperintensities have been found in other neurodegenerative disorders. We would take more neurodegenerative disorders into consider in the further research.
Conclusion
In conclusion, Serum levels of Hcy, HSP70 and hs-CRP were negatively correlated with cognitive impairment caused by CSVD, which could be used as a predictor to predict the risk of cognitive impairment caused by CSV.
Funding
This study was funded by Natural Science Foundation of China (81771154) and National Key R & D Program of China (2016 YFC1305900)
Disclosure
All of the authors declare that they have no competing interests.
References
1. Thompson CS, Hakim AM. Living beyond our physiological means: small vessel disease of the brain is an expression of a systemic failure in arteriolar function: a unifying hypothesis. Stroke. 2009;40:e322–330.
2. Pantoni L. Cerebral small vessel disease: from pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol. 2010;9:689–701.
3. Varghese V, Chandra SR, Christopher R, et al. Factors determining cognitive dysfunction in cerebral small vessel disease. Indian J Psychol Med. 2016;38:56–61.
4. Zhang AJ, Yu XJ, Wang M. The clinical manifestations and pathophysiology of cerebral small vessel disease. Neurosci Bull. 2010;26:257–264.
5. Rouhl RP, Damoiseaux JG, Lodder J, et al. Vascular inflammation in cerebral small vessel disease. Neurobiol Aging. 2012;33:1800–1806.
6. Staekenborg SS, Van Straaten EC, Van der Flier WM, et al. Small vessel versus large vessel vascular dementia. J Neurol. 2008;255:1644–1651.
7. Rosenberg GA. Inflammation and white matter damage in vascular cognitive impairment. Stroke. 2009;40:S20–S23.
8. Wen Y-D, Zhang H-L, Qin Z-H. Inflammatory mechanism in ischemic neuronal injury. Neurosci Bull. 2006;22:171–182.
9. Consoli A, Pasi M, Pantoni L. Vascular mild cognitive impairment: concept, definition, and directions for future studies. Aging Clin Exp Res. 2012;24:113–116.
10. Wada M, Takahashi Y, Iseki C, et al. Plasma fibrinogen, global cognitive function, and cerebral small vessel disease: results of a cross-sectional study in community-dwelling Japanese elderly. Intern Med. 2011;50:999–1007.
11. Ravaglia G, Forti P, Maioli F, et al. Homocysteine and folate as risk factors for dementia and Alzheimer disease–. Am J Clin Nutr. 2005;82:636–643.
12. Feng C, Bai X, Xu Y, et al. Hyperhomocysteinemia associates with small vessel disease more closely than large vessel disease. Int J Med Sci. 2013;10:408–412.
13. Sharp FR, Zhan X, Liu DZ. Heat shock proteins in the brain: role of Hsp70, Hsp 27, and HO-1 (Hsp32) and their therapeutic potential. Transl Stroke Res. 2013;4:685–692.
14. Bobkova NV, Garbuz DG, Nesterova I, et al. Therapeutic effect of exogenous hsp70 in mouse models of Alzheimer’s disease. J Alzheimers Dis. 2014;38:425–435.
15. de Oliveira AA, Nunes KP. An additional physiological role for HSP70: assistance of vascular reactivity. Life Sci. 2020;256:117986.
16. Du Clos TW. Function of C-reactive protein. Ann Med. 2000;32:274–278.
17. Zheng F, Xie W. High-sensitivity C-reactive protein and cognitive decline: the English Longitudinal Study of Ageing. Psychol Med. 2018;48:1381–1389.
18. Wang T, Sun ZW, Shao LQ, et al. Diagnostic values of serum levels of homocysteine and uric acid for predicting vascular mild cognitive impairment in patients with cerebral small vessel disease. Med Sci Monit. 2017;23:2217–2225.
19. Moran C, Phan TG, Srikanth VK. Cerebral small vessel disease: a review of clinical, radiological, and histopathological phenotypes. Int J Stroke. 2012;7:36–46.
20. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53:695–699.
21. Baezner H, Blahak C, Poggesi A, et al. Association of gait and balance disorders with age-related white matter changes: the LADIS study. Neurology. 2008;70:935–942.
22. O’Brien J, Ames D, Chiu E, et al. Severe deep white matter lesions and outcome in elderly patients with major depressive disorder: follow up study. BMJ. 1998;317:982–984.
23. Poggesi A, Gouw A, van der Flier W, et al. Cerebral white matter changes are associated with abnormalities on neurological examination in non-disabled elderly: the LADIS study. J Neurol. 2013;260:1014–1021.
24. Bordes S, Werner C, Mathkour M, et al. Arterial Supply of the Thalamus: a Comprehensive Review. World Neurosurg. 2020;137:310–318.
25. Chou XL, Fang Q, Yan L, et al. Contextual and cross-modality modulation of auditory cortical processing through pulvinar mediated suppression. Elife. 2020;9:76.
26. Fang Q, Chou XL, Peng B, et al. A differential circuit via retino-colliculo-pulvinar pathway enhances feature selectivity in visual cortex through surround suppression. Neuron. 2020;105:355–369 e356.
27. Ibrahim LA, Mesik L, Ji XY, et al. Cross-modality sharpening of visual cortical processing through Layer-1-Mediated Inhibition and Disinhibition. Neuron. 2016;89:1031–1045.
28. McFadyen J, Mattingley JB, Garrido MI. An afferent white matter pathway from the pulvinar to the amygdala facilitates fear recognition. Elife. 2019;8:47.
29. McFadyen J, Dolan RJ, Garrido MI. The influence of subcortical shortcuts on disordered sensory and cognitive processing. Nat Rev Neurosci. 2020;21:264–276.
30. Pantoni L, Poggesi A, Inzitari D. Cognitive decline and dementia related to cerebrovascular diseases: some evidence and concepts. Cerebrovasc Dis. 2009;27:191–196.
31. Sen U, Mishra PK, Tyagi N, et al. Homocysteine to hydrogen sulfide or hypertension. Cell Biochem Biophys. 2010;57:49–58.
32. Folstein M, Liu T, Peter I, et al. The homocysteine hypothesis of depression. Am J Psychiatry. 2007;164:861–867.
33. Obeid R, Herrmann W. Mechanisms of homocysteine neurotoxicity in neurodegenerative diseases with special reference to dementia. FEBS Lett. 2006;580:2994–3005.
34. Bourckhardt GF, Cecchini MS, da Silveira Hahmeyer ML, et al. Impact of homocysteine on vasculogenic factors and bone formation in chicken embryos. Cell Biol Toxicol. 2019;35:49–58.
35. Irizarry M, Gurol M, Raju S, et al. Association of homocysteine with plasma amyloid β protein in aging and neurodegenerative disease. Neurology. 2005;65:1402–1408.
36. Kruman II, Kumaravel T, Lohani A, et al. Folic acid deficiency and homocysteine impair DNA repair in hippocampal neurons and sensitize them to amyloid toxicity in experimental models of Alzheimer’s disease. J Neurosci. 2002;22:1752–1762.
37. Narayan SK, Saxby BK, Firbank MJ, et al. Plasma homocysteine and cognitive decline in older hypertensive subjects. Int Psychogeriatr. 2011;23:1607.
38. Hassan A, Hunt BJ, O’Sullivan M, et al. Homocysteine is a risk factor for cerebral small vessel disease, acting via endothelial dysfunction. Brain. 2004;127:212–219.
39. Stetler RA, Gan Y, Zhang W, et al. Heat shock proteins: cellular and molecular mechanisms in the central nervous system. Prog Neurobiol. 2010;92:184–211.
40. Rajdev S, Hara K, Kokubo Y, et al. Mice overexpressing rat heat shock protein 70 are protected against cerebral infarction. Ann Neurol. 2000;47:782–791.
41. Kuo H-K, Yen C-J, Chang C-H, et al. Relation of C-reactive protein to stroke, cognitive disorders, and depression in the general population: systematic review and meta-analysis. Lancet Neurol. 2005;4:371–380.
42. Ran F, Liu F, Zhang Y, et al. Serum Uric Acid and High-Sensitivity C-Reactive Protein as Predictors of Cognitive Impairment in Patients with Cerebral Infarction. Dement Geriatr Cogn Disord. 2020;49:235–242.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.