")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Diagnostic Value of Pulmonary Ultrasound and Arterial Blood Gas Analysis in Acute Patients with Severe Injuries Complicated by Respiratory Failure-A Retrospective Study
Authors Gu D, Zhang B, Li J, Li Y, Wang Z, Diao J
Received 6 June 2023
Accepted for publication 1 September 2023
Published 13 September 2023 Volume 2023:16 Pages 2707—2714
DOI https://doi.org/10.2147/JMDH.S424667
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dongming Gu, Bo Zhang, Jing Li, Yanpeng Li, Zhihua Wang, Jianjun Diao
Department of Emergency, Shanghai Pudong Hospital, Fudan University Pudong Medical Center, Shanghai, 201399, People’s Republic of China
Correspondence: Jianjun Diao; Zhihua Wang, Department of Emergency, Shanghai Pudong Hospital, Fudan University Pudong Medical Center, 2800 Gongwei Road, Pudong, Shanghai, 201399, People’s Republic of China, Tel +86-18918355085 ; +86-18918355561, Email [email protected]; [email protected]
Background: To investigate the early application of pulmonary ultrasonography and arterial blood gas analysis in critical patients with severe multiple injuries exacerbated by respiratory failure.
Patients and Methods: The retrospective selection was performed on 81 patients admitted to our critical care unit between January 2020 and January 2021 with severe multiple injuries rendered worse by respiratory failure. Based on the different examination procedures, the patients were categorised into three groups (n=27): group A; diagnosed with pulmonary ultrasonography, group B; diagnosed with arterial blood gas; and group C; diagnosed with both pulmonary ultrasonography and arterial blood gas analyses. Patients were subsequently divided into a survival group (n = 65) and a death group (n = 16). On an annual basis, patients’ prognoses were examined in relation to the predictive value of pulmonary ultrasound.
Results: Initial diagnosis, diagnosis, and initial correct treatment times were significantly shorter in groups B and C than group A (P< 0.05). In contrast, initial diagnosis time, diagnosis time, and initial correct treatment times were potentially shorter in group C than in group B (P< 0.05). Compared to groups B and C, group A had a considerably lower diagnosis rate for the examination methods (P< 0.05). The right diaphragm displacement and left diaphragm displacement in the survival group were potentially higher than the LUS score (P < 0.05). In contrast, the survival group’s lung ultrasound score (LUS) was considerably lower than the death group’s. Statistical analysis showed that the predictive values of right diaphragm displacement, left diaphragm displacement, and mean diaphragm displacement were significant compared with the LUS score. The findings of the receiver operating characteristic curve demonstrated that the right, left, and average diaphragm displacements had high predictive values.
Conclusion: In the early evaluation of patients with severe multiple injuries complicated by respiratory failure, pulmonary ultrasonography combined with arterial blood gas analysis is crucial for the rapid diagnosis and prognosis prediction of patients.
Keywords: pulmonary ultrasound, arterial blood gas analysis, severe multiple injuries, respiratory failure
Introduction
The term “severe multiple injuries” often refers to chest injuries and trauma-related chest injury sequelae, which manifest quickly and cause disease progression.1 The application of imaging examinations in critical patients can help diagnose and provide timely and effective treatment, which is essential for patient outcomes. Chest computed tomography (CT) examination, the gold standard for determining chest injuries in patients with multiple injuries, has a high detection rate. Still, its use is constrained by the requirement to transfer the patient, the slow detection rate, and radiation exposure.2 However, due to its mobility and rapid injury detection capabilities, bedside ultrasonography is becoming increasingly popular in the emergency room for detecting and treating numerous severe injuries.3 Respiratory failure is frequently observed in patients with severe multiple injuries, resulting in severe conditions. Blood gas analysis is a standard procedure in emergency medicine that is useful for identifying different types of respiratory failure and diagnosing respiratory failure.4 Previous studies showed that bedside ultrasound shows some diagnostic performance for severe multiple injuries complicated by respiratory failure.5
Monitoring diaphragmatic motion in patients using ultrasound has clinical value in predicting the patients’ prognosis with respiratory failure.6 However, limited clinical investigations were reported using pulmonary ultrasonography and arterial blood gas in patients with severe injuries exacerbated by respiratory failure. Therefore, we compared and analyzed the value of pulmonary ultrasound combined with arterial blood gas analysis in the early management stage of patients with multiple severe injuries complicated by respiratory failure and investigated the clinical diagnosis and prognostic significance of each test method in this study.
Materials and Methods
Design
The retrospective selection was performed on 81 patients hospitalised in our critical care unit in Shanghai between January 2020 and January 2021 with severe multiple injuries exacerbated by respiratory failure.
General Information
There were 57 males and 24 women, ranging in age from 18 to 82, with a mean age of 46. Forty-one traffic incidents resulted in injuries, 18 of which involved falls from a height, 12 of which involved crush injuries, and 10 of which involved falls. The hospital’s ethics committee has approved this study, and all participating patients signed an informed consent form. The patients were divided into three groups: group A; who received only pulmonary ultrasonography diagnoses, group B; who received only arterial blood gas diagnoses; and group C; who received both pulmonary ultrasonography and arterial blood gas analyses diagnoses. A comparison of the baseline data for the three groups is shown in Table 1. Patients were subsequently divided into a survival group (n = 65) and a death group (n = 16). On an annual basis, patients’ prognoses were examined in relation to the predictive value of pulmonary ultrasound. Table 2 compares the baseline data for both groups.
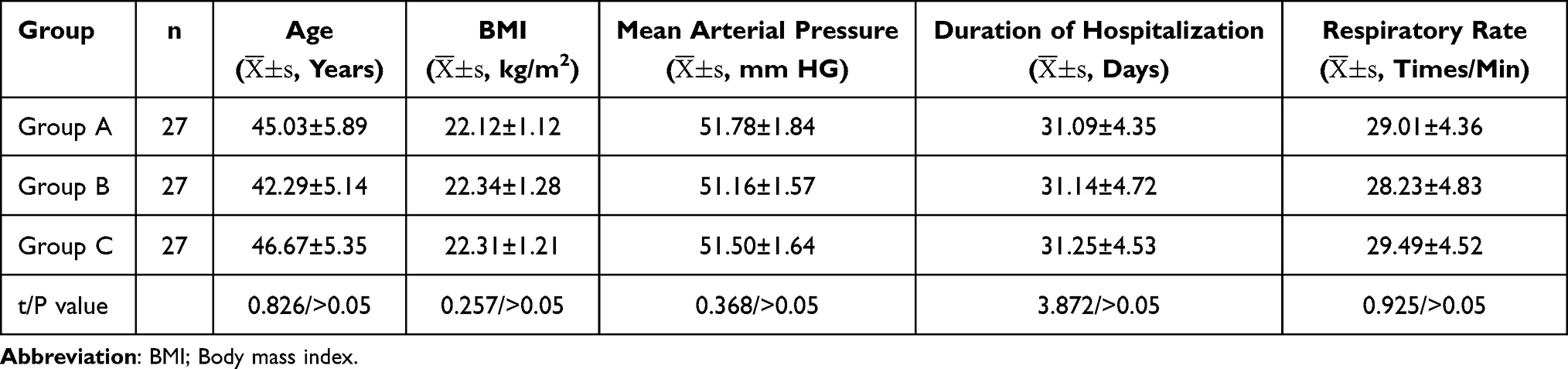 |
Table 1 Comparison of the Baseline Data Between the Three Groups |
 |
Table 2 Comparison of the Baseline Data Between the Two Groups |
The inclusion criteria were: (a) All patients had multiple severe injuries and met the diagnostic criteria for acute respiratory failure in “Respiratory Medicine”,7 and clinical manifestations and laboratory tests confirmed the diagnosis and chest computed tomography (CT), (b) Intubation and ventilator use for assisted breathing.
The following were the exclusion requirements:
- Patients with a history of chronic respiratory illness.
- Those with congenital sternal malformation.
- Those with a recent history of severe pneumonia or other infectious diseases.
- Those experiencing respiratory distress because of a haematological condition or another systemic disease.
- Those who are unable to cooperate or communicate well.
Methodology
Pulmonary ultrasound: All pulmonary ultrasound examinations were carried out using a portable Philips IE33 ultrasound machine using the patient supine and the heart as the marker. The breadth of the inferior vena cava and the transhepatic inferior vena cava at the mid-axillary line of the right abdomen both changed with breathing. The examination included the upper blue point, lower blue point, diaphragmatic point, transverse line of the right little finger, posterior blue point, and bilateral images were compared.
Markers evaluation: (a) Bilateral chest and lungs were observed for the presence of pneumothorax and pleural effusion, A-line or B-line sign. (b) Lung ultrasound score (LUS), carried out by two investigators who were qualified in critical care ultrasound, based on scoring the LUS score of images on a 4-point scale: 1) smooth A-line or less than two isolated B-lines; 2) the presence of a large number of well-defined B-lines spaced more than 7 mm apart. (c) Diaphragmatic displacement measurement method: after examining the patient’s diaphragm, the probe was placed in the right anterior axillary line and left mid-axillary line, with the probe facing the apex of the diaphragm to focus on the diaphragm position. The maximum amplitude of diaphragmatic movement in the inspiratory phase was measured, and diaphragmatic displacement and movement time were recorded. The mean diaphragmatic displacement was calculated as the average of multiple measurements.
Ultrasound images of the lungs of some patients are presented in Figure 1. Pleural effusion: the images indicate the separation of the walls of the pleural cavity, and the space is filled with fluid. A hypoechoic lung “suspension” might be observed in the sonolucent area, and the fluid volume can be roughly calculated based on the sonolucent zone. Hydropneumothorax: Ultrasound reveals a significant volume of fluid deposited in the pleural cavity, and the gas-liquid mirror can reveal the effusion’s surface. Pneumothorax: images display prominent lung spots, lung movement loss, and stratosphere symptoms.
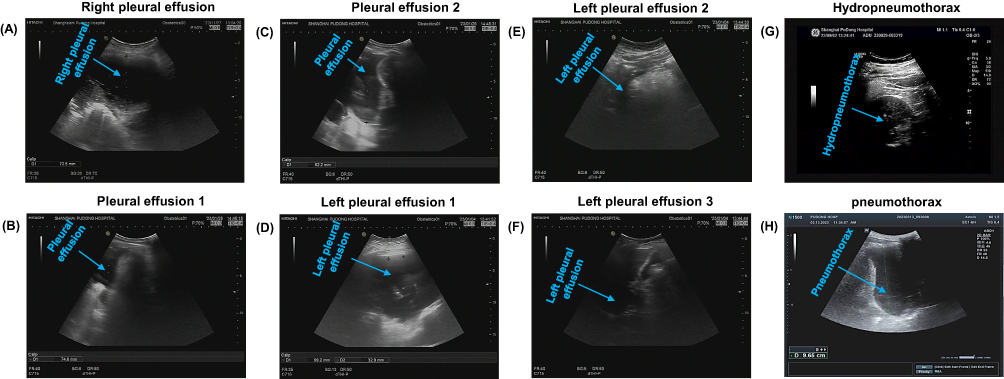 |
Figure 1 Bedside ultrasound. (A-H): Right pleural effusion is the accumulation of fluid in the area between the layers of the pleura around the right lung, pleural effusion is the separation of the walls of the pleural cavity, and the space is filled with fluid, hydropneumothorax is the unusual accumulation of air and fluid in the pleural space and pneumothorax shows significant lung patches, decreased lung movement, and stratosphere symptoms. |
Blood gas analysis: All blood gas analysis examinations were performed using a Siemens fully automated blood gas analyzer (RAPID Lab 1265) to measure the arterial partial pressure of oxygen (PaO2) and arterial partial pressure of carbon dioxide (PaCO2), and blood pH.
Markers Observation
(a) The time to initial diagnosis, time to diagnosis confirmation, and time to initial correct treatment in the patients in each group were observed. (b) The diagnosis confirmation rates for each examination method were compared. (c) All lung ultrasound score (LUS) images were scored by two imaging physicians qualified in critical care ultrasound to assess their predictive value.
Statistical Analysis
Quantitative data were expressed as (± s) and compared using a t-test. All data were analysed using IBM SPSS 22.0 statistical software. Qualitative data were compared using the χ2 test and presented as n (%). The lung ultrasonography prognostic LUS score and diaphragm displacement were investigated in patients with severe multiple injuries exacerbated by respiratory failure. The predictive power of pulmonary ultrasound and blood gas analysis for severe multiple injuries complicated by respiratory failure was explored by analyzing the area under the receiver operating characteristic (ROC) curve, optimal threshold, sensitivity, and specificity. Statistical significance for the difference was set at P<0.05.
Results
Comparison of Diagnosis and Treatment Times for Patients in Each Group
The time to initial diagnosis, time to diagnosis, and time to initial correct treatment were significantly shorter in groups B and C than in group A. The time to initial diagnosis, time to diagnosis, and time to initial correct treatment were significantly faster in group C than group B (P<0.05). The results are presented in Table 3.
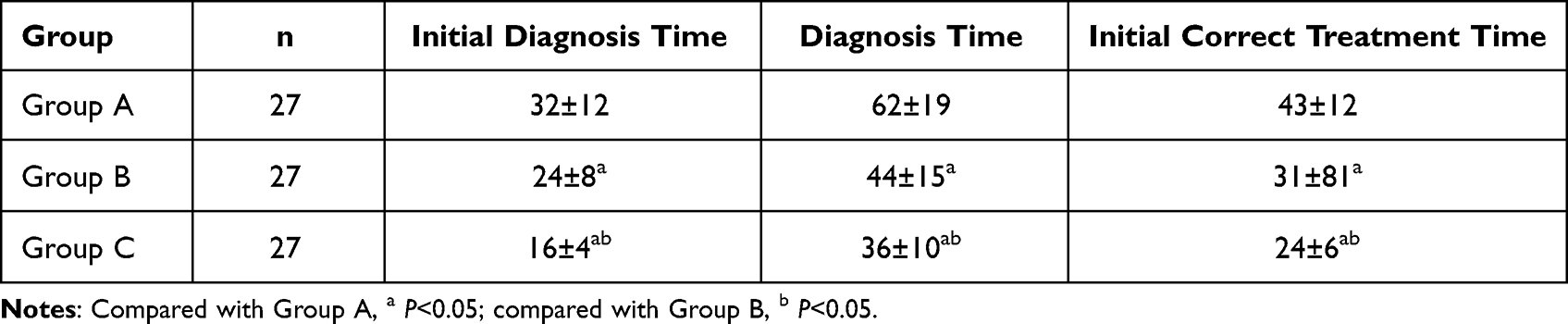 |
Table 3 Time to Diagnose and Treat in the Three Patients’ Group |
Comparison of Patient Diagnosis Rates Among the Different Groups
To investigate the diagnosis rates among the different groups of patients, we compared the diagnosis rates data in groups A, B, and C patients. The data demonstrated that the examination method used in group A had a significantly lower diagnostic confirmation rate than in groups B and C (P<0.05). The results are presented in Table 4.
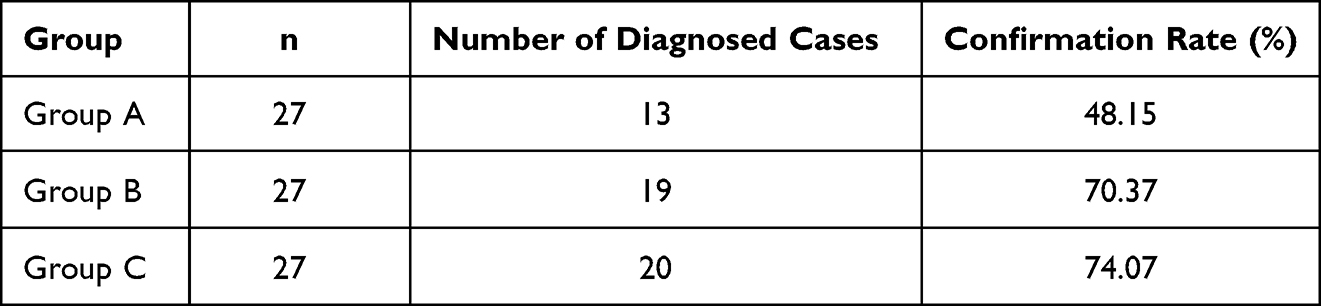 |
Table 4 Patients’ Diagnostic Rate in Each Examination Method Group |
LUS Scores and Diaphragm Displacement Comparison Between the Two Groups
LUS scores and diaphragm displacement were analysed between the survival and death groups. The data showed that right diaphragmatic displacement, left diaphragmatic displacement, and mean diaphragmatic displacement were considerably higher than those in the LUS score were, and the LUS score was significantly lower in the survival group than in the death group (P<0.05). The results are shown in Table 5.
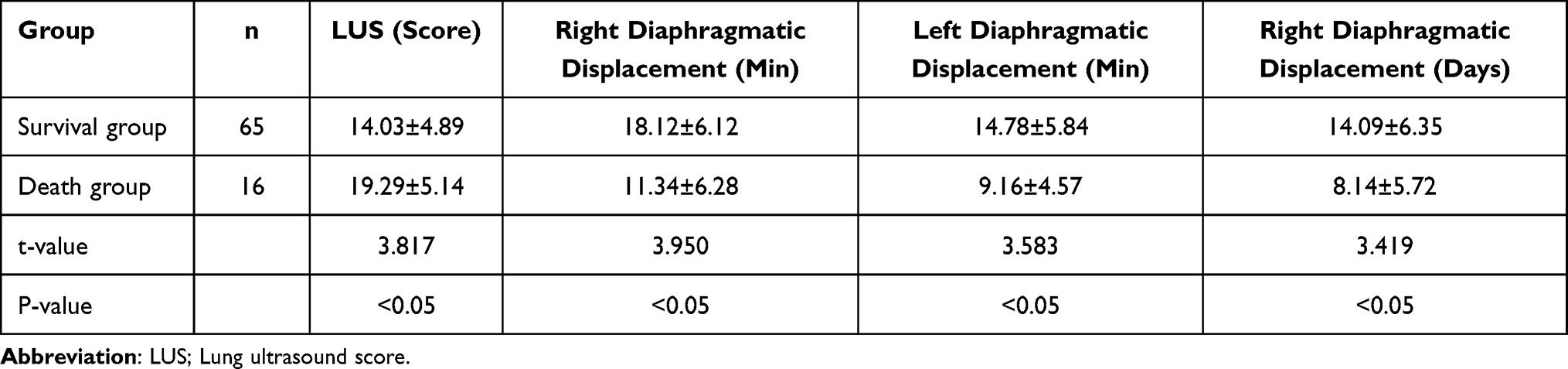 |
Table 5 LUS Scores and Diaphragmatic Displacement are Compared Between the Two Groups |
LUS Score and Diaphragmatic Displacement are Evaluated for Their Prognostic Significance in Patients with Severe Multiple Injuries
To evaluate the predictive values of LUS score and diaphragmatic displacement in patients with severe multiple injuries, we compared the data among the different markers, including LUS score, right diaphragmatic displacement, left diaphragmatic displacement, and mean diaphragmatic displacement. Statistical analysis and plotting the ROC curves showed that the predictive values of right diaphragm displacement, left diaphragm displacement, and mean diaphragm displacement were significant compared with the LUS score (Table 6 and Figure 2).
 |
Table 6 Lung Ultrasonography Prognostic LUS Score and Diaphragm Displacement in Patients with Severe Multiple Injuries Complicated by Respiratory Failure |
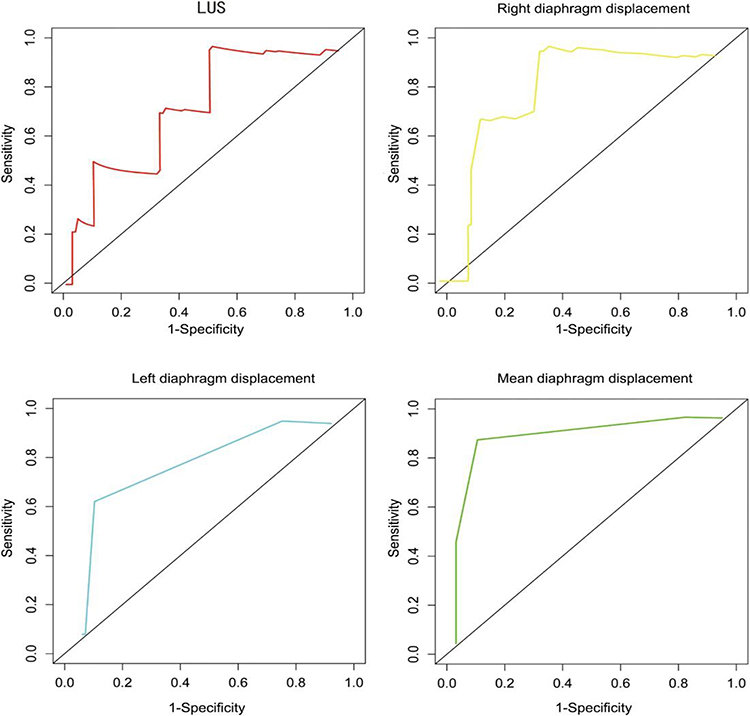 |
Figure 2 ROC curve showing prediction results for various markers. |
Discussion
Multiple serious injuries are often observed with chest injuries and cause impaired pulmonary ventilation or pulmonary exchange, leading to severe injuries complicated by respiratory failure and increased patient morbidity and mortality.8 Previous studies have reported that bedside ultrasound allows investigators to make rapid diagnostic results, improving diagnostic accuracy and reducing the time for diagnosis confirmation.9 In this study, we compared the diagnostic performance of different examination methods in patients with severe multiple injuries complicated by respiratory failure. The results showed that the time to initial diagnosis, time to confirmation of diagnosis, and time to initial correct treatment were significantly shorter in patients who underwent combined pulmonary ultrasound and blood gas analysis examinations than in the other groups, suggesting that combined tests were more efficient and enabled patients to receive prompt and effective treatment. The diagnostic performance results showed no significant difference between the blood gas analysis and the combined examination. This is due to the high diagnostic value of the blood gas analysis itself.10 Still, the relatively convenient and rapid application of bedside ultrasound in emergency department work also has a corresponding clinical value.11
This study aimed to investigate the value of bedside ultrasound in emergency medicine. A study showed that pulmonary ultrasound is valuable in determining the prognosis of patients with respiratory failure.12 Therefore, patients were stratified according to their prognosis in this study, and pulmonary ultrasound imaging was used for analysis. The results showed significant differences between the images of patients in the survival and death groups. LUS is a strong manifestation of altered pulmonary ventilation and can assess the severity of respiratory failure in patients.13 However, in this study, only right diaphragmatic displacement, left diaphragmatic displacement, and mean diaphragmatic displacement had a significant predictive value. LUS did not have a high predictive prognostic value, possibly because of the small sample size. An imbalance in respiratory load and muscle strength can lead to a poor prognosis in patients with respiratory failure. The major respiratory muscle in the human body is the diaphragm, especially during spontaneous breathing, and observation of the diaphragm is a potential method for determining the prognosis of patients.14 More information about diaphragmatic function can be obtained using bedside ultrasound, such as clear anatomical images and diaphragm activity patterns. In addition, right diaphragmatic displacement, left diaphragmatic displacement, and mean diaphragmatic displacement have predictive value for the clinical weaning of ventilators.15 Therefore, applying pulmonary ultrasound in patients with severe multiple injuries complicated by respiratory failure is clinically important.
Limitations
There are several limitations to this study. a) The clinical data may be biased because this was retrospective research. b) The sample size was small in this study. Future research may take advantage of a larger sample size. However, the present study could provide significant insight into the early assessment of patients with multiple severe injuries complicated by respiratory failure and provide important clinical significance in the timely treatment and prediction of patient prognosis.
Conclusions
In this research, we investigated the diagnostic performance of arterial blood gas analysis and pulmonary ultrasonography in patients with severe multiple injuries accompanied by respiratory failure. We observed that pulmonary ultrasound combined with arterial blood gas analysis is of significant value in the early assessment of patients with multiple severe injuries complicated by respiratory failure and has important clinical significance in the timely treatment and prediction of patient prognosis. To verify our present study findings, we will recruit a large number of sample size in subsequent investigations.
Ethics
Shanghai Pudong Hospital, Fudan University Pudong Medical Center ethics committee approved (SPH-01-2020) this study, and it conforms to the provisions of the Declaration of Helsinki. All participating patients in this study were provided with their written consent.
Funding
This work is supported by - The Research Grant for Health Science and Technology of the Pudong Municipal Commission of Health Committee of Shanghai (Grant No. PW2021A-70); the Project of Key Medical Specialty and Treatment Center of Pudong Hospital of Fudan University (Grant No. Zdzk2020-15); the Scientific Research Foundation provided by Pudong Hospital affiliated to Fudan University (Project no. YJRCJJ201910).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Li L, Wu X, Kong Q, et al. Effects of dexmedetomidine on NLRP3 inflammasome during acute lung injury induced by blunt chest trauma and hemorrhagic shock-resuscitation in rats. Chinese J Anesthesiol. 2019;12:754–757.
2. Kelleher MS, Gao G, Rolen MF, Bokhari SA. Completion CT of chest, abdomen, and pelvis after acute head and cervical spine trauma: incidence of acute traumatic findings in the setting of low-velocity trauma. Radiology. 2016;279:395–399. doi:10.1148/radiol.2015151509
3. Talbot BS, Gange CP, Chaturvedi A, Klionsky N, Hobbs SK, Chaturvedi A. Traumatic rib injury: patterns, imaging pitfalls, complications, and treatment. Radiographics. 2017;37:628–651. doi:10.1148/rg.2017160100
4. McCanny P, Bennett K, Staunton P, McMahon G. Venous vs arterial blood gases in the assessment of patients presenting with an exacerbation of chronic obstructive pulmonary disease. Am J Emerg Med. 2012;30:896–900. doi:10.1016/j.ajem.2011.06.011
5. Messina A, Robba C, Bertuetti R, et al. Head to toe ultrasound: a narrative review of experts’ recommendations of methodological approaches. J Anesth Analg Crit Care. 2022;2(1):44. doi:10.1186/s44158-022-00072-5
6. Kelley RC, Ferreira LF. Diaphragm abnormalities in heart failure and aging: mechanisms and integration of cardiovascular and respiratory pathophysiology. Heart Fail Rev. 2017;22:191–207. doi:10.1007/s10741-016-9549-4
7. Wang C, Xiao F, Qiao R, Shen YH. Respiratory medicine in China: progress, challenges, and opportunities. Chest. 2013;143:1766–1773. doi:10.1378/chest.12-1854
8. Chiumello D, Brioni M. Severe hypoxemia: which strategy to choose. Crit Care. 2016;20:132. doi:10.1186/s13054-016-1304-7
9. Stevenson JG. The development of color Doppler echocardiography: innovation and collaboration. J Am Soc Echocardiogr. 2018;31:1344–1352. doi:10.1016/j.echo.2018.08.005
10. Gattinoni L, Pesenti A, Matthay M. Understanding blood gas analysis. Intensive Care Med. 2018;44:91–93. doi:10.1007/s00134-017-4824-y
11. Ryu K, Hong SS, Cha H, et al. A pancreatic hemorrhagic pseudocyst with pseudoaneurysm and the role of Doppler ultrasonography: a case report. Rev Assoc Med Bras. 2019;65(2):123–126. doi:10.1590/1806-9282.65.2.123
12. Lichtenstein D. Lung ultrasound in the critically ill. Curr Opin Crit Care. 2014;20:315–322. doi:10.1097/MCC.0000000000000096
13. Loi B, Vigo G, Baraldi E, et al. Lung ultrasound to monitor extremely preterm infants and predict bronchopulmonary dysplasia. A multicenter longitudinal cohort study. Am J Respir Crit Care Med. 2021;203:1398–1409. doi:10.1164/rccm.202008-3131OC
14. Matamis D, Soilemezi E, Tsagourias M, et al. Sonographic evaluation of the diaphragm in critically ill patients. Technique and clinical applications. Intensive Care Med. 2013;39:801–810. doi:10.1007/s00134-013-2823-1
15. Lesser TG, Schubert H, Gullmar D, Reichenbach JR, Wolfram F. One-lung flooding reduces the ipsilateral diaphragm motion during mechanical ventilation. Eur J Med Res. 2016;21:9. doi:10.1186/s40001-016-0205-1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.