Back to Journals » Journal of Inflammation Research » Volume 18
Diagnostic Value of Long Non-Coding RNA NORAD in Acute Coronary Syndrome: A Diagnostic Biomarker Study
Authors Xin W, Li Q, Deng X, Li R, Wang P
Received 10 June 2025
Accepted for publication 3 November 2025
Published 17 November 2025 Volume 2025:18 Pages 15985—15994
DOI https://doi.org/10.2147/JIR.S540975
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rongxue Wu
Wenhao Xin, Qiang Li, Xianzhu Deng, Runan Li, Pengxiang Wang
Department of Cardiology, Nanyang Central Hospital, Nanyang, People’s Republic of China
Correspondence: Wenhao Xin, Email [email protected]
Purpose: Acute coronary syndrome (ACS), a critical condition with high morbidity and mortality, lacks reliable non-invasive biomarkers for timely diagnosis. Traditional biomarkers like troponins lack sensitivity in unstable angina, and troponin levels often remain within the normal range in the early phase of myocardial infarction. Long non-coding RNAs (lncRNAs), implicated in vascular inflammation and atherosclerosis, may serve as novel biomarkers. This study evaluated four lncRNAs (NORAD, MIR181A1HG, HEAT4, MERRICAL) for ACS diagnosis and their correlation with inflammatory cytokines [Interleukin (IL)-1β, IL-6, Tumor Necrosis Factor-alpha (TNF-α)].
Patients and Methods: A total of 156 ACS patients and 100 non-coronary artery disease (CAD) chest pain patients were enrolled from April 2021 to April 2023, with an independent validation cohort (36 ACS and 24 non-CAD) recruited from May to August 2023. Serum levels of lncRNAs were measured via quantitative polymerase chain reaction (qPCR; normalized to GAPDH), and inflammatory cytokines via Enzyme-Linked Immunosorbent Assay (ELISA). Multivariable logistic regression, receiver operating characteristic (ROC) analysis, and Spearman correlation were used to assess diagnostic performance and associations.
Results: NORAD (P< 0.0001) and MIR181A1HG (P=0.0279) were significantly upregulated in ACS patients, whereas HEAT4 and MERRICAL did not differ significantly. Multivariate regression identified NORAD as an independent predictor of ACS [adjusted odds ratio (OR)=2.567, 95% confidence interval (CI) 1.724– 3.823, P< 0.001]. ROC analysis showed NORAD alone achieved an Area Under the Curve (AUC) of 0.726 (95% CI 0.661– 0.790), with sensitivity 81.1% and specificity 56.0% at the optimal cutoff. Incorporating NORAD into a model with traditional risk factors improved diagnostic accuracy (AUC: 0.700 vs 0.763, P=0.024), validated in the independent cohort (AUC: 0.823 vs 0.690, P=0.015). NORAD levels correlated positively with IL-1β (R=0.40, P< 0.001) and IL-6 (R=0.34, P< 0.001), but not TNF-α.
Conclusion: NORAD is a promising diagnostic biomarker for ACS. Its correlation with inflammatory cytokines underlying its involvement in ACS pathogenesis.
Keywords: acute coronary syndrome, vascular inflammation, lncRNA, NORAD, inflammatory cytokine
Introduction
Acute coronary syndrome (ACS) represents a spectrum of life-threatening conditions caused by the rupture or erosion of atherosclerotic plaques in the coronary arteries.1,2 Given the high morbidity and mortality associated with ACS, accurate diagnosis is crucial for improving patient outcomes.1–5 Coronary angiography (CAG), although considered the gold standard for diagnosing coronary artery disease (CAD), has significant limitations.6–10 As an invasive procedure, it carries inherent risks, including potential contrast-related allergies, coronary artery perforation, dissection, and complications in patients with severe heart failure, arrhythmias, or impaired liver and kidney function. Moreover, traditional biomarkers like cardiac troponins,11–14 which are widely used for diagnosing myocardial infarction, only begin to elevate several hours after the onset of injury, typically three or more hours post-infarction. Furthermore, troponins are not elevated in cases of unstable angina,15 a common form of ACS where ischemia does not lead to myocardial necrosis. These limitations highlight the urgent need for novel and reliable biomarkers that can provide accurate diagnostic information for detecting ACS in patients with chest pain.
Long non-coding RNAs (lncRNAs) are a class of RNA molecules that do not encode proteins and are involved in various crucial biological processes.16–18 These molecules can be released into the blood by different cell types, and some studies have indicated that serum lncRNAs might serve as potential biomarkers for predicting diseases.19,20 Recently, several lncRNAs related to vascular inflammation and atherosclerosis have been identified. For example, NORAD has been shown to promote pyroptosis in THP-1-derived macrophages and worsen atherosclerosis,21 while MIR181A1HG can activate the NLRP3 inflammasome in vascular endothelial cells.22 HEAT4 enhances an anti-inflammatory phenotype in CD16+ monocytic cells and exacerbates injury-induced vascular healing.23 Macrophages lacking MERRICAL exhibit reduced expression of Ccl3 and Ccl4, as well as diminished chemotaxis and inflammatory responses.24 Most current studies on lncRNAs have focused primarily on basic experimental research. However, clinical investigations exploring whether lncRNAs can serve as diagnostic or prognostic biomarkers remain limited, and their translational potential as clinical biomarkers has not been fully explored. Therefore, given the harmful impact of vascular inflammation on the progression of atherosclerosis, we propose that these four lncRNAs could serve as valuable diagnostic biomarkers for ACS.
This study aims to assess the diagnostic value of these recently identified lncRNAs associated with vascular inflammation in predicting ACS in patients presenting with chest pain. Additionally, we aim to explore the correlation between these lncRNAs and the levels of inflammatory cytokines (IL-1β, IL-6, and TNF-α) in peripheral blood serum.
Materials and Methods
Human Subjects and Sample Collection
In this research, we employed a total sampling approach, and a total of 156 patients diagnosed with ACS were enrolled between April 2021 and April 2023 at the cardiology department of Nanyang Central Hospital. Participants were selected based on the following inclusion criteria: they were diagnosed with ACS for the first time and confirmed through CAG. The exclusion criteria were as follows: (1) individuals with severe hepatic or renal dysfunction, (2) those suffering from advanced heart failure, (3) patients with uncontrolled, severe arrhythmias, (4) those diagnosed with cancer, and (5) individuals with significant infections. Additionally, we included 100 patients who presented with chest pain between April 2021 and April 2023, but were ultimately ruled out for CAD via CAG or coronary computed tomography angiography (CTA).
To confirm the predictive value of these lncRNAs for ACS, a prospective validation group was formed, consisting of 36 ACS patients from the same hospital and 24 chest pain patients who were excluded from CAD diagnoses based on CAG or coronary CTA results From May 2023 to August 2023. This validation cohort was completely temporally distinct from the primary cohort.
Serum samples were collected from all participants during their hospitalization or outpatient visits. The study protocol was reviewed and approved by the ethics committee of Nanyang Central Hospital, and all procedures were carried out in full compliance with the most recent version of the Declaration of Helsinki. Prior to participation, written informed consent was obtained from all patients.
RNA Isolation and Quantitative PCR
For the analysis of lncRNA expression (NORAD, MIR181A1HG, HEAT4, and MERRICAL), real-time PCR was performed. Total RNA was extracted from each sample using the Trizol® reagent (Invitrogen, Carlsbad, CA) according to the manufacturer’s protocol. RNA quality and concentration were assessed by measuring absorbance at 260 nm and 280 nm with a Nanodrop ND-3000 spectrophotometer (Thermo Fisher Scientific, Waltham, MA). 300 ng of RNA from each sample was reverse-transcribed into cDNA using a cDNA synthesis kit (Thermo Fisher Scientific, Waltham, MA), following the provided guidelines. The resulting cDNA was then subjected to real-time qPCR using the Taqman Gene Expression Assay kit (Invitrogen, Carlsbad, CA) on a StepOnePlus qPCR system (Invitrogen, Carlsbad, CA) as per the manufacturer’s instructions.
For normalization, the expression of the lncRNAs was compared to GAPDH levels. The relative expression of each lncRNA was calculated using the ΔCt method, where ΔCt is defined as the difference between the Ct values of the lncRNA and GAPDH (ΔCt = Ct[lncRNA] - Ct[GAPDH]). The relative expression level was then calculated using the formula 2(-ΔCt). The lncRNA expression in ACS patients was normalized to the average expression levels in the non-CAD group, yielding a fold change representing ACS vs non-CAD expression levels.
Sequences of primers for this assay:
NORAD
Forward: GGAAGAGGGAGAAGAGGA
Reverse: CACAATGAACACAGGCAC
MIR181A1HG
Forward: CTCAACCTTCCAGGCTCAAG
Reverse: CTATTGTTGGGCCTCCATGT
HEAT4
Forward: CCTGGCTCACATTCCGATTG
Reverse: TCGTCTTCTCTGCACTCCAA
MERRICAL
Forward: TGAAAAAGGAAATGAGGAGAAAAG
Reverse: CTTCACAAAACCTCCCTTTACAAT
GAPDH
Forward: GGAGCGAGATCCCTCCAAAAT
Reverse: GGCTGTTGTCATACTTCTCATGG
To evaluate the reproducibility of qPCR assays, quality control (QC) samples were prepared by pooling serum from 20 randomly selected participants among the 256 individuals. The pooled QC sample was included on each qPCR plate in eight replicate wells. Intra-assay variability was calculated based on the ΔCt values of these eight replicates within the same plate. For inter-assay variability of each lncRNA, the mean ΔCt value of the eight QC replicates was calculated for each plate, and the coefficient of variation (CV) was then determined across the mean ΔCt values obtained from different plates. The intra-assay CVs for all qPCR assays were ≤5%, and the inter-assay CVs for all targets were ≤10%.
Measurement of Inflammatory Cytokines Using ELISA
To quantify the concentrations of inflammatory cytokines (IL-1β, IL-6, and TNF-α) in peripheral serum, we followed the manufacturer’s instructions (ELISA array kit, Boster, Wuhan, China) in a cohort of 156 ACS patients.
To evaluate the reproducibility of ELISA assays, the pooled QC sample was also used as the standard control. Intra-assay variability was determined by measuring the QC sample in eight replicate wells within the same plate, and inter-assay variability was assessed by calculating the CV across the mean concentrations of the QC sample measured on different plates. The intra-assay CVs for all ELISA measurements were ≤10%, and the inter-assay CVs were ≤15%.
We confirm that all laboratory analyses were performed under blinded conditions. Samples were relabeled with anonymized study IDs by a coordinator who was not involved in qPCR/ELISA, and the operators were blinded to clinical grouping and outcomes until all primary analyses were finalized.
Statistical Analysis
Continuous variables were presented as either the mean ± standard deviation (for normally distributed data) or median (25th–75th percentiles) for non-normally distributed data. Comparisons between groups were performed using the independent sample t-test or Mann–Whitney U-test as appropriate. Categorical variables were reported as counts (proportions) and analyzed using the chi-squared test or Fisher’s exact test when applicable.
Multivariable logistic regression was employed to explore the associations between lncRNAs and ACS, adjusting for common cardiovascular risk factors, such as age, sex, hypertension, smoking, diabetes, and dyslipidemia. The results were expressed as odds ratios (ORs) with 95% confidence intervals (CIs).
Spearman correlation was used to assess the relationships between variables. To evaluate the diagnostic potential of these lncRNAs for predicting ACS, receiver operating characteristic (ROC) curves were generated to determine sensitivity, specificity, and the area under the curve (AUC). The optimal cut-off values were established using the Youden index, and AUC comparisons for these lncRNAs were performed using DeLong test in R (version 4.2.0) with the pROC package.
A p-value of less than 0.05 was considered statistically significant, and all statistical tests were two-sided. Statistical analyses were performed using SPSS (version 22.0) and R (version 4.2.0).
Results
Baseline Characteristics of Non-CAD Patients and ACS Patients
Table 1 outlines the baseline characteristics of the 100 non-CAD patients and 156 ACS patients included in the study. As indicated, ACS patients were generally older and had a higher proportion of current smokers. In addition, these patients had elevated white blood cell counts, neutrophil percentages, as well as increased levels of total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), triglycerides (TG), HbA1c, and hs-CRP when compared to non-CAD patients. However, the incidence of other cardiovascular risk factors, such as diabetes and hyperlipidemia, did not show significant differences between the two groups.
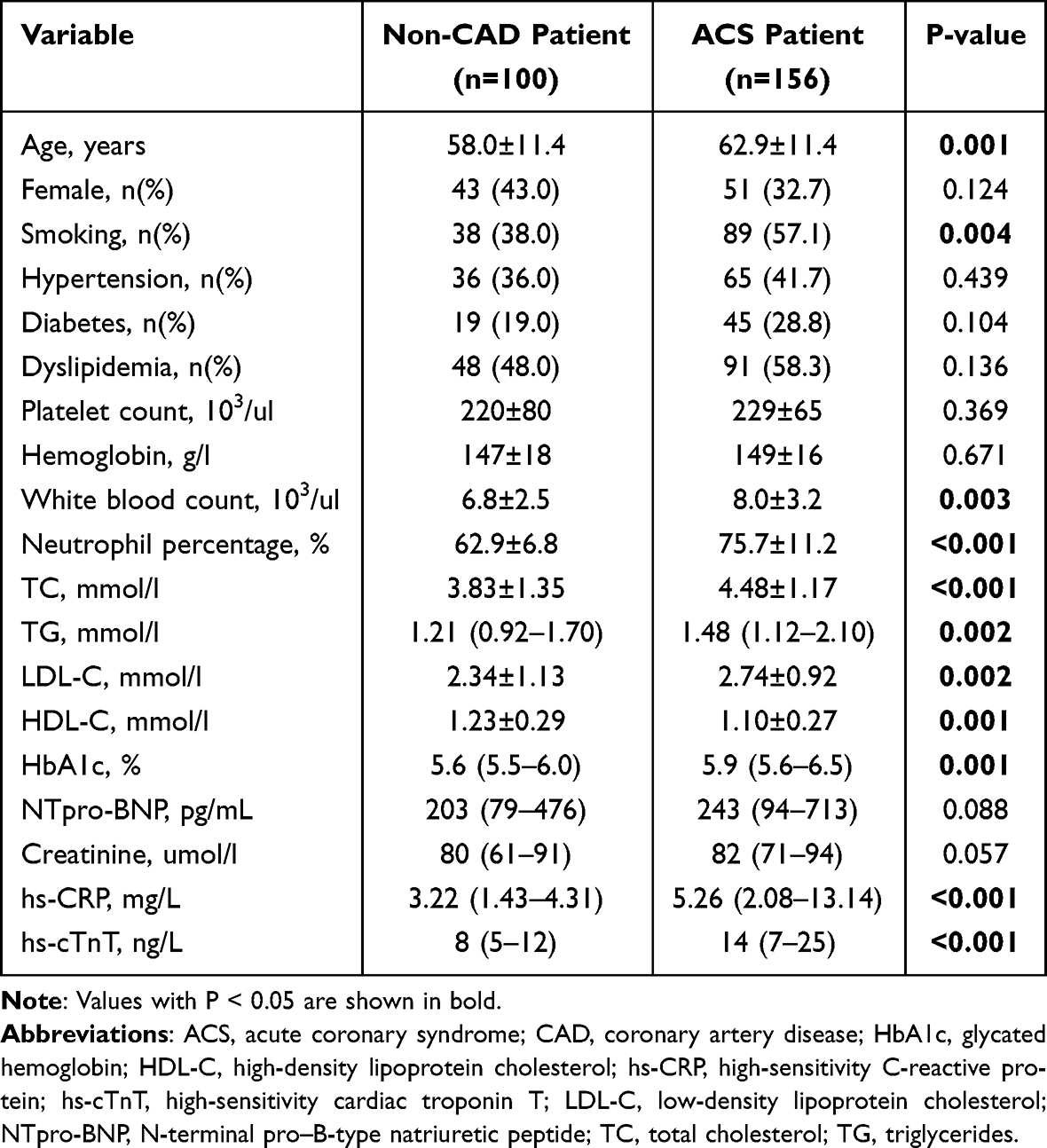 |
Table 1 Baseline Characteristics of Non-CAD Patients and ACS Patients |
Differential Expression of LncRNAs in ACS Patients
Figure 1A and B demonstrates that the relative expression levels of NORAD and MIR181A1HG were significantly higher in ACS patients (n=156) compared to non-CAD patients (n=100) [Mann–Whitney U-test, 1.29 (0.99–1.74) vs 0.86 (0.66–1.23), P<0.0001; 1.03 (0.89–1.20) vs 0.96 (0.82–1.13), P=0.0279]. No significant differences were observed in the relative expression levels of HEAT4 and MERRICAL between the two groups [Mann–Whitney U-test, 0.94 (0.76–1.24) vs 0.95 (0.69–1.21), P=0.408; 0.89 (0.71–1.19) vs 0.94 (0.70–1.24), P=0.690; Figure 1C and D].
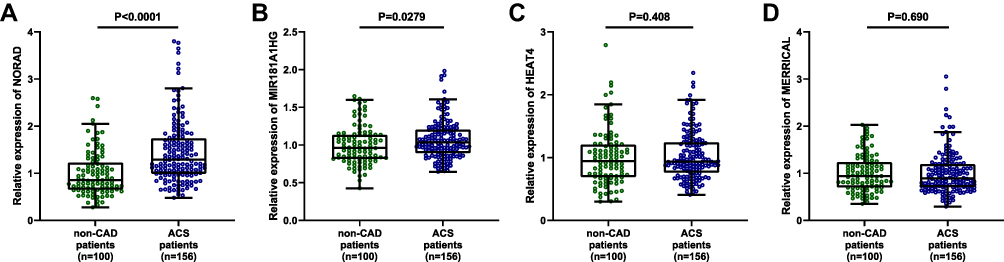 |
Figure 1 Relative Expression levels of four vascular inflammation-associated lncRNAs: Relative expression levels of NORAD (A), MIR181A1HG (B), HEAT4 (C), and MERRICAL (D) in peripheral blood serum between non-CAD patients (n=100), and ACS patients (n=156). P-values are for Mann–Whitney U-test. Boxplots represented the median, interquartile (box) and 1.5 interquartile range (whiskers). |
NORAD Could Serve as an Independent Predictor of ACS
To determine whether these lncRNAs could serve as independent predictors of ACS in patients presenting with chest pain, we conducted a multivariate logistic regression analysis, adjusting for age, gender, and cardiovascular risk factors. The results indicated that elevated levels of NORAD were independently associated with the occurrence of ACS [Per standard deviation (SD): Unadjusted model: OR=2.674, 95% CI 1.827–3.912, P<0.001; Adjusted model 1: OR=2.721, 95% CI 1.837–4.029, P<0.001; Adjusted model 2: OR=2.567, 95% CI 1.724–3.823, P<0.001; Table 2], whereas the other three lncRNAs did not show an independent association with ACS.
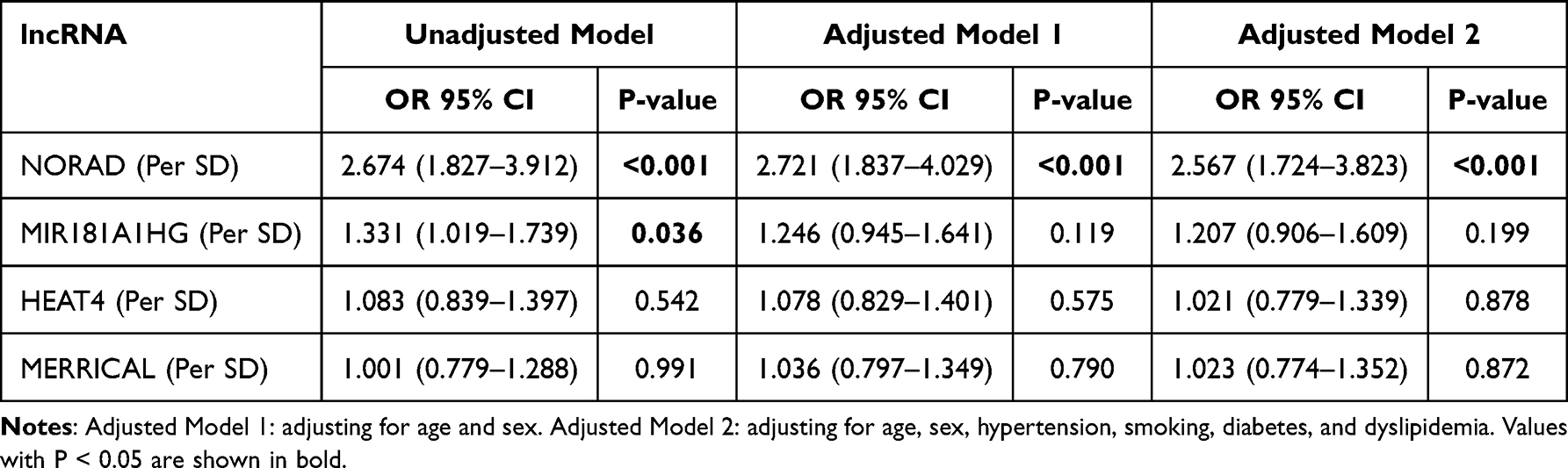 |
Table 2 Tables for the Associations Between lncRNA and ACS |
Furthermore, subgroup analyses revealed no significant interaction effects across any of the subgroups. The association between elevated NORAD levels and the occurrence of ACS is consistent across different subgroups (Figure 2).
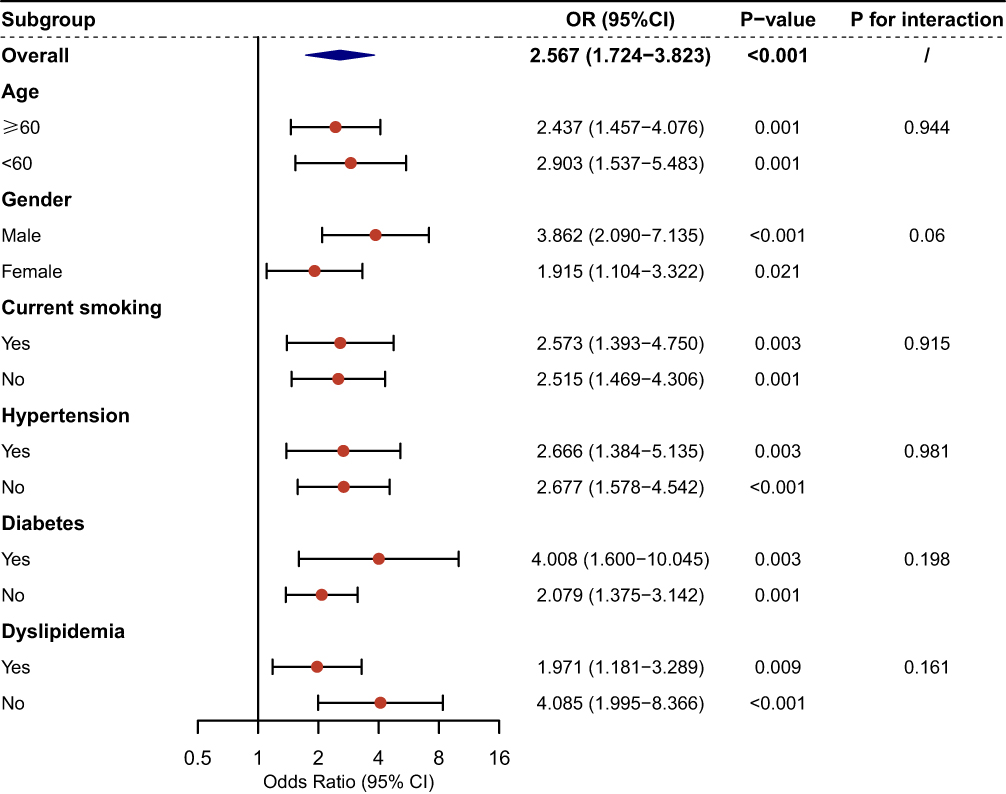 |
Figure 2 Subgroup analysis for the association between NORAD expression (per SD increase) and ACS across traditional cardiovascular risk factors. The forest plot displays odds ratios (ORs) derived from logistic regression models, with NORAD expression standardized per standard deviation (SD). Red circles represent point estimates of ORs, horizontal lines indicate 95% confidence intervals (95% CI), and the vertical line marks the null value (OR=1). The diamond summarizes the overall OR for the entire cohort. Subgroup analyses were stratified by age, gender, smoking status, hypertension, diabetes, and dyslipidemia, with interaction P-values (P for interaction) assessing heterogeneity across subgroups. |
Diagnostic Performance of NORAD in Identifying ACS
After establishing the independent association between NORAD and ACS, we further examined its diagnostic value in predicting ACS in patients presenting with chest pain. ROC analysis revealed that NORAD alone demonstrated a good predictive ability (AUC=0.726, 95% CI 0.661–0.790, P<0.001; Figure 3A). The optimal cutoff value for the relative expression of NORAD in predicting ACS was determined to be 0.944, yielding a sensitivity of 81.1%, a specificity of 56.0%, a positive predictive value (PPV) of 73.9%, and a negative predictive value (NPV) of 64.3% (Figure 3B). To assess the added diagnostic value of NORAD, we incorporated it into a model that included established ACS risk factors, such as age, sex, hypertension, smoking, diabetes, and dyslipidemia. Notably, the inclusion of NORAD significantly enhanced the model’s performance (AUC: 0.700 vs 0.763, DeLong test P = 0.024, Figure 3A). For this model, the optimal cutoff probability was 0.418, which resulted in a sensitivity of 92.3%, a specificity of 48.0%, a PPV of 73.4%, and a NPV of 80.0% (Figure 3C).
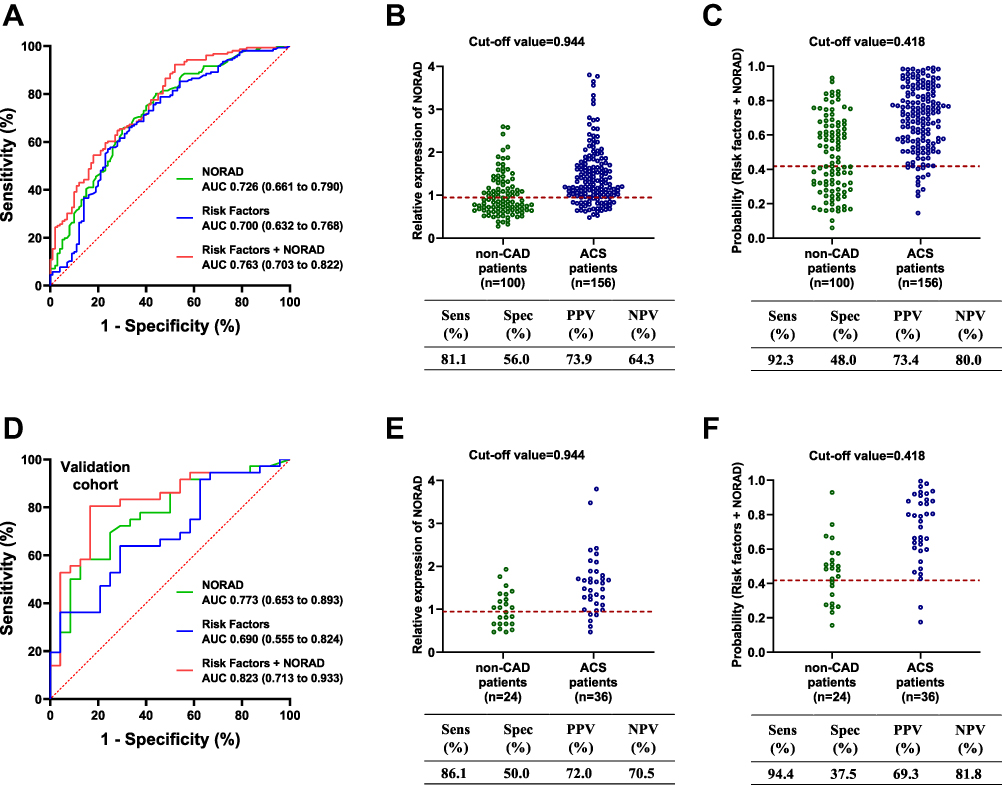 |
Figure 3 Diagnostic Value of NORAD. Receiver operating characteristic (ROC) curves showing the diagnostic performance of NORAD alone, traditional risk factors (age, sex, hypertension, smoking, diabetes, and dyslipidemia), and the combination of risk factors with NORAD in the primary cohort (A). The predictive ability of NORAD was further evaluated using optimal cut-off values for the relative expression of NORAD (B) and the probability derived from a logistic regression model combining risk factors with NORAD (C), with comparisons between non-CAD patients and ACS patients. The validation cohort confirmed these findings, demonstrating ROC analysis (D) and predictive performance based on the same logistic regression models and cut-off values (E and F). |
To further validate the predictive capacity of NORAD levels and the model incorporating NORAD, we tested it in an validation cohort consisting of 24 non-CAD patients and 36 ACS patients. ROC analysis showed that adding NORAD to the model improved its predictive ability (AUC: 0.690 vs 0.823, DeLong test P = 0.015, Figure 3D). The sensitivity, specificity, PPV, and NPV in the validation cohort (Figure 3E and F) were consistent with those previously found (Figure 3B and C), at the same optimal cutoff value, demonstrating the robustness of NORAD’s diagnostic performance across both cohorts.
Furthermore, in the primary cohort, we directly compared the diagnostic performance of NORAD with that of high-sensitivity cardiac troponin T (hs-cTnT), a widely used biomarker for ACS. ROC curve analysis demonstrated that there was no significant difference in the AUC values between NORAD and hs-cTnT (AUC: 0.726 vs 0.702, DeLong test, P = 0.64; Figure S1A). The optimal cutoff for hs-cTnT was 14 ng/L, corresponding to a sensitivity of 48.7% and a specificity of 91.0% (Figure S1B). We further evaluated the diagnostic performance of combining NORAD with hs-cTnT. Specifically, NORAD expression and the natural logarithm–transformed hs-cTnT values were incorporated into a logistic regression model to construct a new predictive model, yielding a combined AUC of 0.776 (Figure S1A), which was significantly higher than that of either biomarker alone (DeLong test, P = 0.034 and 0.010, respectively). These findings indicate that while NORAD demonstrates comparable diagnostic performance to hs-cTnT, their combination provides superior diagnostic accuracy for ACS.
Correlation Between NORAD and Inflammatory Cytokines
A previous study demonstrated that NORAD enhances pyroptosis in THP-1-derived macrophages. In our study, we measured the concentrations of three key inflammatory cytokines (IL-1β, IL-6, and TNF-α) involved in macrophage pyroptosis in the peripheral serum of ACS patients and examined their relationship with NORAD expression. Pearson’s correlation analysis revealed a moderate positive correlation between NORAD levels and the concentrations of IL-1β (R=0.40, P<0.001; Figure 4A) and IL-6 (R=0.34, P<0.001; Figure 4B). However, no significant correlation was observed with TNF-α (R=0.09, P=0.26; Figure 4C).
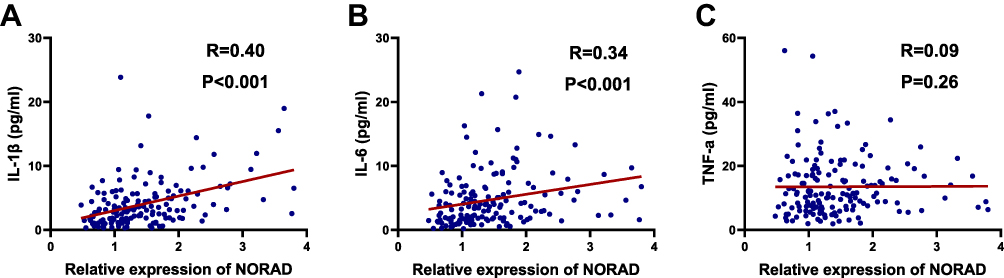 |
Figure 4 Spearman correlation analysis of the expression of NORAD with inflammatory cytokines. Inflammatory cytokines: IL-1β (A), IL-6 (B), and TNF-α (C). P-values and R-values are for Spearman correlation analysis. |
Furthermore, we also assessed the correlation (Figure S2) between three other lncRNAs and the inflammatory cytokines, but no significant associations were found.
Discussion
Numerous studies have highlighted that lncRNAs play a crucial role in regulating the development of atherosclerosis and vascular injury.25–29 In our analysis, we explored the predictive value of four newly identified lncRNAs21–24 associated with atherosclerosis and vascular inflammation in chest pain patients. Our results showed that NORAD performed particularly well. NORAD, a lncRNA that is activated by DNA damage, is located on chromosome 20q11.23 in humans.30 It plays a critical role in maintaining chromosomal stability and is involved in mitotic processes.30 Earlier studies have linked NORAD to several types of cancer,31–33 including breast, lung, and prostate cancers. Recent evidence21 has further elucidated the molecular mechanism through which NORAD regulates macrophage inflammation. NORAD was shown to aggravate atherosclerosis by promoting macrophage pyroptosis via the miR-106b-5p/TXNIP/NLRP3 axis. Mechanistically, NORAD functions as a competing endogenous RNA (ceRNA) that directly binds to miR-106b-5p, thereby preventing miR-106b-5p from repressing its downstream target, thioredoxin-interacting protein (TXNIP). The upregulation of TXNIP subsequently activates the NLRP3 inflammasome, leading to caspase-1 activation, gasdermin-D cleavage, and enhanced secretion of IL-1β and IL-18. These processes amplify the inflammatory response and promote plaque instability. This mechanistic link supports our findings that NORAD levels are positively correlated with pyroptosis-related cytokines in ACS patients, suggesting that NORAD may contribute to coronary inflammation and plaque rupture by regulating inflammasome-mediated macrophage pyroptosis.
Previous research has highlighted that the expression of various lncRNAs is notably different between ACS patients and healthy controls, suggesting their potential as novel biomarkers for ACS prediction.19,20 In our study, we observed elevated serum levels of NORAD in ACS patients. Logistic regression analysis, which was adjusted for traditional cardiovascular risk factors, further indicated that NORAD is independently associated with ACS. Moreover, when NORAD was integrated into a predictive model that included traditional cardiovascular risk factors, the model’s ability to predict ACS was significantly improved. Importantly, internal validation using an additional cohort from our center, which included both non-CAD and ACS patients, confirmed the model’s robust predictive performance.
When used alone as a biomarker, NORAD showed relatively high sensitivity but only moderate specificity for predicting ACS. This moderate specificity may be explained by the fact that some patients in the control group presented with chest pain caused by other acute conditions such as pulmonary embolism, aortic dissection, or pericarditis. These conditions are often associated with systemic stress and heightened inflammation, which could elevate the expression of inflammation-related lncRNAs such as NORAD. Therefore, the clinical potential of NORAD may lie in its combination with established biomarkers, particularly high-sensitivity cardiac troponin T (hs-cTnT). Although hs-cTnT is widely used for the diagnosis of myocardial infarction,11–14 it cannot be applied to patients with unstable angina and typically remains within the normal range during the first three hours after symptom onset. In our study, combining NORAD with hs-cTnT significantly improved diagnostic performance compared with either biomarker alone. Collectively, our results indicate that NORAD represents a novel and complementary biomarker that could improve current diagnostic strategies for ACS when used alongside conventional markers.
Although both the animal study and our clinical data provide new insights into the association between NORAD and ACS, further research is needed to validate its clinical potential. First, the sample size of our internal validation cohort was relatively small, so larger external cohorts are required to confirm NORAD’s ability to differentiate ACS in patients with chest pain. Second, it remains to be determined whether peripheral blood levels of NORAD in ACS patients can serve as an independent predictor of major adverse cardiovascular events. Finally, investigating the potential for combining NORAD with other ACS-related lncRNAs to improve diagnostic accuracy is a promising avenue for future research.
Conclusions
In conclusion, we assessed the levels of four vascular inflammation-associated lncRNAs in the peripheral blood of chest pain patients. Our results show that NORAD expression is significantly higher in the peripheral serum of ACS patients compared to those without CAD, and it correlates with IL-1β and IL-6 levels. Importantly, NORAD acts as an independent predictor of ACS and may assist in identifying ACS among patients presenting with chest pain.
Ethics Approval and Informed Consent
The study protocol was reviewed and approved by the ethics committee of Nanyang Central Hospital, and all procedures were carried out in full compliance with the most recent version of the Declaration of Helsinki. Prior to participation, written informed consent was obtained from all patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not funded.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bergmark BA, Mathenge N, Merlini PA, Lawrence-Wright MB, Giugliano RP. Acute coronary syndromes. Lancet. 2022;399(10332):1347–1358. doi:10.1016/S0140-6736(21)02391-6
2. Libby P. The changing landscape of atherosclerosis. Nature. 2021;592(7855):524–533. doi:10.1038/s41586-021-03392-8
3. Wang Y, Zeller M, Auffret V, et al. Sex-specific prediction of cardiogenic shock after acute coronary syndromes: the SEX-SHOCK score. Eur Heart J. 2024;45(43):4564–4578. doi:10.1093/eurheartj/ehae593
4. Bouzid Z, Sejdic E, Martin-Gill C, et al. Electrocardiogram-based machine learning for risk stratification of patients with suspected acute coronary syndrome. Eur Heart J. 2025;46(10):943–954. doi:10.1093/eurheartj/ehae880
5. Wenzl FA, Wang P, Arrigo M, et al. Proenkephalin improves cardio-renal risk prediction in acute coronary syndromes: the KID-ACS score. Eur Heart J. 2025;46(1):38–54. doi:10.1093/eurheartj/ehae602
6. Sheikh MA, Hussain R, Khan MI. Cortical blindness post coronary angiogram: a rare but frightening complication. Int J Cardiol. 2016;221:1143. doi:10.1016/j.ijcard.2016.06.229
7. Khan S, Kamani A, Strauss BH, Zipursky J. Successful coronary angiography following rapid intravenous desensitization for refractory contrast allergy. Can J Cardiol. 2020;36(7):1161e1161–1161e1162.
8. Gray AJ, Roobottom C, Smith JE, et al. Early computed tomography coronary angiography in patients with suspected acute coronary syndrome: randomised controlled trial. BMJ. 2021;374:n2106.
9. James MT, Har BJ, Tyrrell BD, et al. Effect of clinical decision support with audit and feedback on prevention of acute kidney injury in patients undergoing coronary angiography: a randomized clinical trial. JAMA. 2022;328(9):839–849. doi:10.1001/jama.2022.13382
10. Oguri M, Ishii H, Shigematsu T, et al. Safety of clinical engineer-assisted percutaneous coronary intervention. Cardiovasc Interv Ther. 2023;38(1):96–103. doi:10.1007/s12928-022-00884-w
11. Camaro C, Aarts GWA, Adang EMM, et al. Rule-out of non-ST-segment elevation acute coronary syndrome by a single, pre-hospital troponin measurement: a randomized trial. Eur Heart J. 2023;44(19):1705–1714. doi:10.1093/eurheartj/ehad056
12. Doudesis D, Lee KK, Boeddinghaus J, et al. Machine learning for diagnosis of myocardial infarction using cardiac troponin concentrations. Nat Med. 2023;29(5):1201–1210. doi:10.1038/s41591-023-02325-4
13. Lee KK, Doudesis D, Ferry AV, et al. Implementation of a high sensitivity cardiac troponin I assay and risk of myocardial infarction or death at five years: observational analysis of a stepped wedge, cluster randomised controlled trial. BMJ. 2023;383:e075009.
14. Pareek M, Kragholm KH, Kristensen AMD, et al. Serial troponin-T and long-term outcomes in suspected acute coronary syndrome. Eur Heart J. 2023;44(6):502–512. doi:10.1093/eurheartj/ehac629
15. Sandoval Y, Apple FS, Mahler SA, et al. High-sensitivity cardiac troponin and the 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guidelines for the evaluation and diagnosis of acute chest pain. Circulation. 2022;146(7):569–581. doi:10.1161/CIRCULATIONAHA.122.059678
16. Ferrer J, Dimitrova N. Transcription regulation by long non-coding RNAs: mechanisms and disease relevance. Nat Rev Mol Cell Biol. 2024;25(5):396–415. doi:10.1038/s41580-023-00694-9
17. Pierce JB, Feinberg MW. Long noncoding RNAs in atherosclerosis and vascular injury: pathobiology, biomarkers, and targets for therapy. Arterioscler Thromb Vasc Biol. 2020;40(9):2002–2017. doi:10.1161/ATVBAHA.120.314222
18. Viereck J, Buhrke A, Foinquinos A, et al. Targeting muscle-enriched long non-coding RNA H19 reverses pathological cardiac hypertrophy. Eur Heart J. 2020;41(36):3462–3474. doi:10.1093/eurheartj/ehaa519
19. Agwa SHA, Elzahwy SS, El Meteini MS, et al. ABHD4-regulating RNA panel: novel biomarkers in acute coronary syndrome diagnosis. Cells. 2021;10(6):1512. doi:10.3390/cells10061512
20. Barbalata T, Niculescu LS, Stancu CS, Pinet F, Sima AV. Elevated levels of circulating lncRNAs LIPCAR and MALAT1 predict an unfavorable outcome in acute coronary syndrome patients. Int J Mol Sci. 2023;24(15):12076. doi:10.3390/ijms241512076
21. Liang Y, Xu XD, Xu X, et al. Linc00657 promoted pyroptosis in THP-1-derived macrophages and exacerbated atherosclerosis via the miR-106b-5p/TXNIP/NLRP3 axis. Int J Biol Macromol. 2023;253(Pt 4):126953. doi:10.1016/j.ijbiomac.2023.126953
22. Ni H, Ge Y, Zhuge Y, et al. LncRNA MIR181A1HG deficiency attenuates vascular inflammation and atherosclerosis. Circ Res. 2025;136(8):862–883. doi:10.1161/CIRCRESAHA.124.325196
23. Kneuer JM, Grajek IA, Winkler M, et al. Novel long noncoding RNA HEAT4 affects monocyte subtypes, reducing inflammation and promoting vascular healing. Circulation. 2024;150(14):1101–1120. doi:10.1161/CIRCULATIONAHA.124.069315
24. Chen J, Jamaiyar A, Wu W, et al. Deficiency of lncRNA MERRICAL abrogates macrophage chemotaxis and diabetes-associated atherosclerosis. Cell Rep. 2024;43(3):113815. doi:10.1016/j.celrep.2024.113815
25. Fasolo F, Jin H, Winski G, et al. Long noncoding RNA MIAT controls advanced atherosclerotic lesion formation and plaque destabilization. Circulation. 2021;144(19):1567–1583. doi:10.1161/CIRCULATIONAHA.120.052023
26. Haemmig S, Yang D, Sun X, et al. Long noncoding RNA SNHG12 integrates a DNA-PK-mediated DNA damage response and vascular senescence. Sci Transl Med. 2020;12(531). doi:10.1126/scitranslmed.aaw1868
27. Jiang M, Song Y, Ren MX, et al. LncRNA NIPA1-SO confers atherosclerotic protection by suppressing the transmembrane protein NIPA1. J Adv Res. 2023;54:29–42. doi:10.1016/j.jare.2023.01.017
28. Leisegang MS, Bibli SI, Gunther S, et al. Pleiotropic effects of laminar flow and statins depend on the Kruppel-like factor-induced lncRNA MANTIS. Eur Heart J. 2019;40(30):2523–2533. doi:10.1093/eurheartj/ehz393
29. Zhang W, Zhao J, Deng L, et al. INKILN is a novel long noncoding RNA promoting vascular smooth muscle inflammation via scaffolding MKL1 and USP10. Circulation. 2023;148(1):47–67. doi:10.1161/CIRCULATIONAHA.123.063760
30. Elguindy MM, Mendell JT. NORAD-induced Pumilio phase separation is required for genome stability. Nature. 2021;595(7866):303–308. doi:10.1038/s41586-021-03633-w
31. Fletcher CE, Deng L, Orafidiya F, et al. A non-coding RNA balancing act: miR-346-induced DNA damage is limited by the long non-coding RNA NORAD in prostate cancer. Mol Cancer. 2022;21(1):82. doi:10.1186/s12943-022-01540-w
32. Alves-Vale C, Capela AM, Tavares-Marcos C, et al. Expression of NORAD correlates with breast cancer aggressiveness and protects breast cancer cells from chemotherapy. Mol Ther Nucleic Acids. 2023;33:910–924. doi:10.1016/j.omtn.2023.08.019
33. Jiang Z, Person R, Lundh T, et al. Circulating lung-cancer-related non-coding RNAs are associated with occupational exposure to hexavalent chromium - A cross-sectional study within the SafeChrom project. Environ Int. 2024;190:108874. doi:10.1016/j.envint.2024.108874
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.