Back to Journals » Infection and Drug Resistance » Volume 19
Diagnostic Value of Copeptin and Growth Differentiation Factor-15 for Sepsis-Related Myocardial Injury
Authors Yan X, Chen Q ![]() , Li T
, Li T ![]() , Zhao Y, Shao Z, Cao Z, Li H, Qu L, Zhu L, Zhao Z, Huang Y
, Zhao Y, Shao Z, Cao Z, Li H, Qu L, Zhu L, Zhao Z, Huang Y ![]() , Gao K, Gao X, Li W, Jiang W
, Gao K, Gao X, Li W, Jiang W ![]() , Hu B
, Hu B ![]()
Received 15 March 2026
Accepted for publication 24 June 2026
Published 9 July 2026 Volume 2026:19 607414
DOI https://doi.org/10.2147/IDR.S607414
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Xiaofei Yan,1,2,* Qi Chen,2,3,* Ting Li,2,* Yuechu Zhao,2 Zhuang Shao,2 Zhi Cao,2 Hongbin Li,1,2 Lingying Qu,2,3 Lixia Zhu,4 Zichao Zhao,2 Yiwen Huang,5 Kai Gao,2 Xiaoxin Gao,2 Weifeng Li,2 Wenqiang Jiang,2 Bei Hu1,2
1Department of Emergency Medicine, Guangdong Cardiovascular Institute, Guangzhou, Guangdong, People’s Republic of China; 2Department of Emergency Medicine, Guangdong Provincial People’s Hospital (Southern Medical University), Guangzhou, Guangdong, People’s Republic of China; 3School of Medicine, South China University of Technology, Guangzhou, Guangdong, People’s Republic of China; 4Department of Emergency Medicine, Foresea Life Insurance General Hospital, Guangzhou, Guangdong, People’s Republic of China; 5Department of Emergency Medicine, Guangzhou First People’s Hospital, Guangzhou, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wenqiang Jiang, Email [email protected] Bei Hu, Email [email protected]
Background: Biomarkers play a critical role in the diagnosis and clinical decision-making for sepsis-related myocardial injury (SMI). SMI has no single accepted definition. Copeptin and growth differentiation factor-15 (GDF-15), which are associated with stress response and systemic inflammation, have emerged as potential diagnostic markers. This study aimed to investigate the expression levels of copeptin and GDF-15 in SMI patients and evaluate their diagnostic utility.
Methods: This case-control study enrolled 148 sepsis patients admitted to the emergency department and 43 healthy controls. Patients with sepsis were divided into the SMI group and the non-SMI group. SMI was defined as cTnT > 40.0 pg/mL and/or LVEF < 50% in patients with sepsis, after excluding clear alternative causes of myocardial injury. Blood samples were collected within 48 hours after admission, and serum copeptin and GDF-15 levels were measured and compared with clinical indicators. Univariate and multivariate logistic regression analyses were performed to identify factors associated with SMI. The diagnostic performance of copeptin and GDF-15 was evaluated using receiver operating characteristic (ROC) curve analysis.
Results: Copeptin and GDF-15 levels were significantly elevated in SMI patients compared to both sepsis patients without myocardial injury and healthy controls (P < 0.01). Multivariate analysis confirmed that copeptin (OR 1.018, 95% CI: 1.001– 1.035) and GDF-15 (OR 1.266, 95% CI: 1.102– 1.454) were independently associated with SMI. ROC analysis demonstrated diagnostic performance for SMI, with an AUC of 0.884 (95% CI: 0.837– 0.931) for copeptin and 0.862 (95% CI: 0.810– 0.914) for GDF-15. The combined use of both biomarkers further improved diagnostic accuracy (AUC = 0.911, 95% CI: 0.871– 0.951).
Conclusion: Serum copeptin and GDF-15 levels were elevated in patients with SMI and may provide complementary value for identifying myocardial injury in patients with sepsis, with enhanced diagnostic capability when used in combination. Further validation in larger multicenter studies is needed before these biomarkers can be used in routine clinical practice.
Keywords: sepsis-related myocardial injury, biomarkers, copeptin, GDF-15, diagnostic utility
Introduction
Sepsis, a life-threatening condition characterized by organ dysfunction resulting from a dysregulated host response to infection, is primarily driven by an uncontrolled inflammatory response leading to organ damage.1 Li et al reported an increasing incidence of sepsis-related hospitalizations, further intensifying the associated healthcare burden.2 Cardiac involvement is common in sepsis and covers a broad spectrum, ranging from sepsis-related myocardial injury (SMI) to overt sepsis-induced cardiomyopathy (SIC).3,4 SIC may manifest as left ventricular (LV) systolic/ diastolic dysfunction or right ventricular (RV) dysfunction,5 with a reported prevalence of 10% to 70%.6 SMI is also an important manifestation of cardiac involvement in patients with sepsis.4,7 In routine clinical practice, myocardial injury markers are often detected even when a definite cardiomyopathy phenotype has not yet been established.
Traditional cardiac biomarkers, including cardiac troponin and brain natriuretic peptide (BNP), are commonly used to assess myocardial injury and cardiac stress in patients with sepsis. However, elevated admission levels of high-sensitivity troponin I (hs-TnI) alone do not reliably identify sepsis-induced cardiomyopathy.8 BNP can be influenced by ventricular loading conditions, renal function, and disease severity, limiting its specificity for SMI.9 These limitations highlight the need for additional biomarkers to improve the identification of SMI.
Serum growth differentiation factor 15 (GDF-15), a member of the transforming growth factor-β (TGF-β) superfamily, exhibits minimal baseline expression in myocardial tissue under physiological conditions, with high mRNA levels restricted primarily to human placental terminal chorionic villous cells and prostate epithelial cells.10 However, oxidative stress and pro-inflammatory cytokines, particularly interleukin-6 (IL-6) and tumor necrosis factor (TNF), trigger macrophage activation and a marked upregulation of GDF-15 expression.11 Emerging evidence underscores GDF-15’s clinical relevance in cardiovascular pathology. Elevated concentrations of GDF-15 have been identified in cardiovascular disease progression,3,12 hypertension,13 myocardial infarction,12,14 and coronary artery disease.15 Notably, Huan Li et al identified high GDF-15 levels as a sensitive diagnostic and prognostic indicator, correlating with the severity of organ dysfunction in sepsis patients.16 The 2022 Chinese expert consensus endorsed GDF-15 as a novel biomarker for early diagnosis, severity assessment, and prognostic prediction in acute coronary syndromes, advocating its combined use with traditional markers to enhance diagnostic sensitivity.4 Critically, recent studies reveal that serum GDF-15 levels are significantly elevated in SIC, suggesting its potential utility as an early biomarker for this condition.17
Copeptin, a glycosylated 39-amino acid peptide (~5 kDa), is the C-terminal fragment cleaved from pre-pro-arginine vasopressin (pre-proAVP).18 It is co-synthesized with arginine vasopressin in the hypothalamus and released in equimolar amounts from the neurohypophysis into systemic circulation in response to physiological stressors, including hyperosmolality, hypotension, and circulatory insufficiency.19,20 Due to its structural stability and prolonged half-life compared to the labile arginine vasopressin, copeptin has emerged as a more reliable surrogate biomarker.21,22 Previous studies have shown that copeptin levels are significantly elevated in sepsis, severe sepsis, and septic shock, and tend to increase with disease severity. In addition, admission copeptin levels are significantly higher in non-survivors than in survivors.23–25 These findings suggest that copeptin may serve as a useful adjunctive biomarker for the early assessment and risk stratification of patients with sepsis. Clinical studies further support its cardiovascular applications: The AROMI trial (Pedersen CK et al) demonstrated that prehospital copeptin combined with in-hospital high-sensitivity troponin T (hs-TnT) facilitated rapid exclusion of acute myocardial infarction, reducing hospitalization time without increasing 30-day major adverse cardiac events.26 In a 6.5-year cohort study of 5,217 moderate-to-severe chronic kidney disease (CKD) patients, elevated copeptin levels predicted cardiovascular mortality and heart failure hospitalizations, highlighting its role in identifying high-risk nephropathy patients.27
The diagnostic criteria for SMI remain inadequately defined, highlighting the critical need for reliable biomarkers to enable early detection. While both copeptin and GDF-15 have shown individual promise in cardiovascular pathologies, their combined diagnostic value for SMI has been scarcely investigated. In this study, we aimed to evaluate the diagnostic value of copeptin and GDF-15 levels for identifying SMI, facilitating early intervention to improve clinical outcomes and reduce mortality.
Materials and Methods
Study Design and Participants
This case-control study retrospectively enrolled 148 consecutive sepsis patients admitted to the Emergency Department between October 2023 and July 2025. Participants were stratified into two groups: sepsis patients without myocardial injury (Non-SMI group, n=64) and those with myocardial injury (SMI group, n=84), based on predefined cardiac biomarkers and echocardiographic criteria. An additional 43 healthy volunteers were recruited as controls during the same period. Blood samples were collected upon admission. We compared copeptin and GDF-15 levels among three groups to find their association with SMI at admission. Informed consent was obtained from all participants or their legal representatives.
Data Collection
Comprehensive clinical data were extracted from electronic medical records (EMRs), including demographic characteristics and clinical presentation at admission, laboratory parameters, diagnostic imaging results, therapeutic interventions, and clinical outcomes.
Inclusion Criteria
The inclusion criteria for sepsis patients were as follows: 1) met the Sepsis-3.0 diagnosis criteria, 2) age ≥18 years. The diagnosis criteria for patients with SMI were as follows:3,28 1) met the Sepsis-3.0 diagnosis criteria, 2) evidence of myocardial injury, defined as either left ventricular ejection fraction (LVEF) <50% on echocardiography, or cardiac troponin T (cTnT) >40.0 pg/mL (normal range at our hospital:0–40 pg/mL).
Exclusion Criteria
Patients were excluded for any of the following: (1) age <18 years. (2) pregnancy or lactation, (3) active malignancy or immune disorders, (4) chronic kidney disease (estimated glomerular filtration rate <60 mL/min/1.73m2 > 3 months); (5) pre-existing cardiac conditions: acute coronary syndromes, myocarditis, structural heart disease (valvular, dilated, or pulmonary cardiomyopathies), cardiac surgery history, acute pulmonary embolism, recent cardiopulmonary resuscitation, (6) death within 48 hours of admission, (7) lack of informed consent.
Data Collection and Variables
Clinical Information
For all study participants, the following clinical data were collected: demographic characteristics (gender, age, admission time), cardiac biomarkers (troponin T (cTnT), N-terminal pro-B-type natriuretic peptide (NT-proBNP), creatine kinase-MB (CK-MB), and left ventricular ejection fraction), inflammatory and infection markers (procalcitonin (PCT), C-reactive protein (CRP), white blood cell count (WBC), neutrophil count, neutrophil percentage, and lactate (Lac)), renal and metabolic parameters (blood urea nitrogen (BUN), creatinine, and albumin (ALB)), disease severity scores (Acute Physiology and Chronic Health Evaluation II (APACHE II) and Sequential Organ Failure Assessment (SOFA) scores).
Transthoracic echocardiography was performed by specialist ultrasonographers within 48 hours after admission, according to the routine clinical protocol of our hospital. LVEF was obtained from the echocardiographic report.
Laboratory Assays
Upon admission, 5 mL of venous blood was collected from emergency patients. The samples were centrifuged at 3000 × g for 15 min to separate the serum. The supernatant was aliquoted into EP tubes and stored at −80°C until analysis. To perform copeptin analyses, use the BRAHMS KRYPTOR compact PLUS time-resolved fluorescence immunoassay analyzer (Thermo Fisher Scientific, China) and its corresponding reagents. According to the manufacturer’s specifications, the acceptable coefficient of variation (CV) was <8% for within-lot precision and <15% for between-lot precision.
Serum GDF-15 levels were quantified using a double-antibody sandwich enzyme-linked immunosorbent assay (ELISA) (Fine Test; distributed by FIEN Biologicals), in strict accordance with the manufacturer’s protocol. For each assay run, standards at seven different concentration levels were measured in duplicate to generate the standard curve, and the R2value > 0.99. All serum samples were measured in duplicate, and the mean absorbance value was used to calculate the final GDF-15 concentration. The intra-assay coefficients of variation for the samples were less than 8%, and the inter-assay coefficients of variation were less than 10%.
Sample Size Estimation
Sample size estimation was performed for the primary diagnostic analysis based on ROC curve analysis. As this was a retrospective case-control study, the cohort size was determined by the number of eligible consecutive patients during the study period. Based on a previous study reporting an AUC of 0.971 for GDF-15 in diagnosing sepsis-induced cardiomyopathy, we used a conservative expected AUC of 0.85 for the present assessment.17 Using PASS 2025 software, with a two-sided α of 0.05 and a power of 90%, at least 12 patients were required in each sepsis subgroup. In our final cohort, 84 patients with SMI and 64 patients without SMI were included, which met this requirement. The 43 healthy controls were used for additional comparisons among groups.
Statistical Analysis
Statistical analyses were conducted using SPSS 26.0 (IBM Corp., Armonk, NY, USA) and GraphPad Prism 10.0 (GraphPad Software, San Diego, CA, USA), and R version 4.5.2 (R Foundation for Statistical Computing, Vienna, Austria). Continuous variables with normal distribution were expressed as mean ± standard deviation and compared among the three groups using one-way analysis of variance with Bonferroni post hoc correction. Non-normally distributed variables were presented as median with interquartile range (IQR; M[QL, QU]) and analyzed using Mann–Whitney U-tests between two groups, as appropriate. For comparisons among the three groups, variables were analyzed using the Kruskal–Wallis H-test followed by post-hoc pairwise comparisons with Bonferroni correction. For continuous variables, replace the missing values with the mean or median when <15% were missing. Categorical variables were expressed as counts (percentages) and compared using χ2-tests or Fisher’s exact tests when expected cell frequencies were <5. Correlation analyses between biomarkers and clinical indicators were determined with the use of Spearman’s rank correlation coefficients. Univariate and multivariable logistic regression were performed to explore potential factors independently associated with SMI. Variables with a p-value <0.05 in the univariate logistic analysis were considered for the multivariate model, which were subsequently refined through backward stepwise regression with Akaike information criterion serving as the stopping rule. Multicollinearity among final variables in a multivariate model was assessed by checking the variance inflation factor (VIF). If the VIF of a variable was found to be greater than 3, it was removed from the model.
The diagnostic performance of relevant biomarkers was evaluated by calculating the area under the receiver operating characteristic curve (AUC), along with corresponding sensitivity and specificity. The DeLong method was used to assess the differences in AUCs. To reduce the risk of overfitting in the combined diagnostic models, internal validation was performed using bootstrap resampling. A two-tailed P-value <0.05 was considered statistically significant.
Results
Patient Characteristics and Study Flow
Between October 2023 and July 2025, we screened 203 consecutive patients admitted to our emergency department with suspected sepsis. After applying exclusion criteria, we excluded: 8 patients with malignant tumors, 30 patients with pre-existing cardiac conditions (acute coronary syndrome, cardiomyopathy, severe valvular heart disease, or chronic heart failure), 10 patients with chronic renal failure, and 7 patients with incomplete laboratory data. The final study cohort comprised 148 patients, among whom 84 (56.8%) met diagnostic criteria for SMI. Additionally, we enrolled 43 age- and sex-matched healthy individuals as controls (Figure 1).
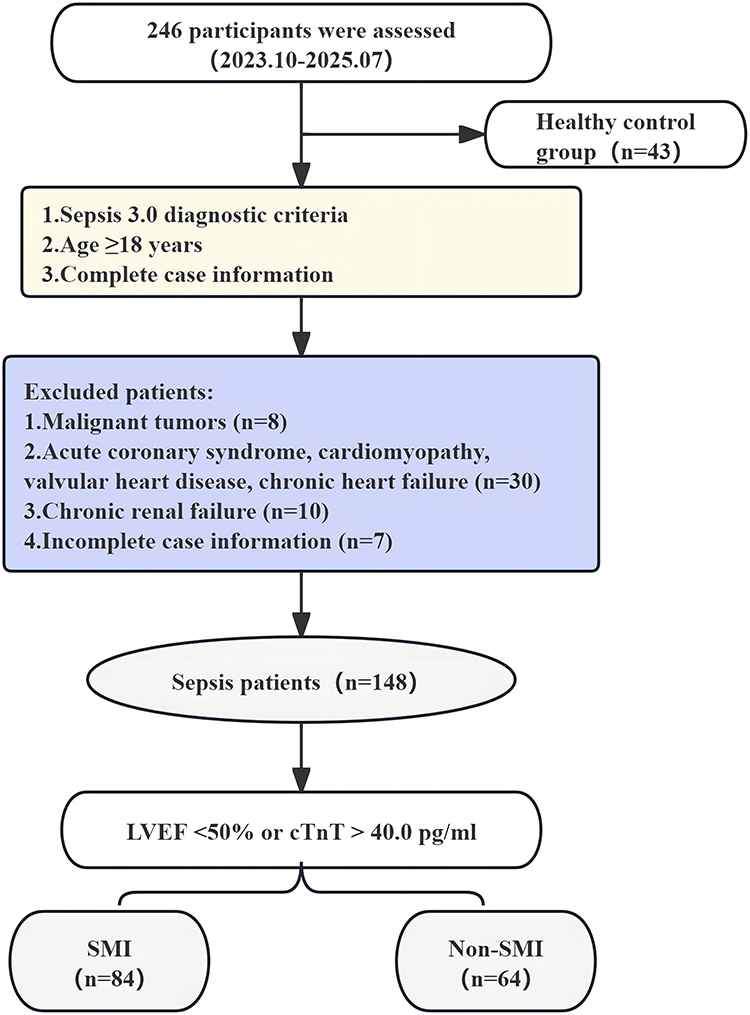 |
Figure 1 Study enrollment flowchart of patients with suspected sepsis. Flowchart showing the screening, exclusion, and final enrollment of patients with suspected sepsis and healthy controls. Patients with sepsis were subsequently classified into the SMI and non-SMI groups according to the predefined diagnostic criteria. Abbreviations: SMI, sepsis-related myocardial injury; LVEF, left ventricular ejection fraction; cTnT, cardiac troponin T. |
Demographic and Clinical Characteristics (Table 1)
No significant differences in gender distribution were observed among the three groups (P > 0.05). However, marked differences in inflammatory markers were evident, with the SMI group exhibiting significantly higher levels of white blood cells, neutrophils, neutrophil ratio, procalcitonin, and C-reactive protein compared to both the sepsis without myocardial injury and healthy control groups (all P < 0.001). Specifically, the SMI group demonstrated: (1) significantly elevated neutrophil ratio and PCT levels versus both comparison groups (P < 0.05); (2) markedly increased cardiac biomarkers, including N-terminal pro-B-type natriuretic peptide and cardiac troponin T levels (P < 0.05); and (3) greater disease severity as reflected by higher SOFA and APACHE II scores (P < 0.05).
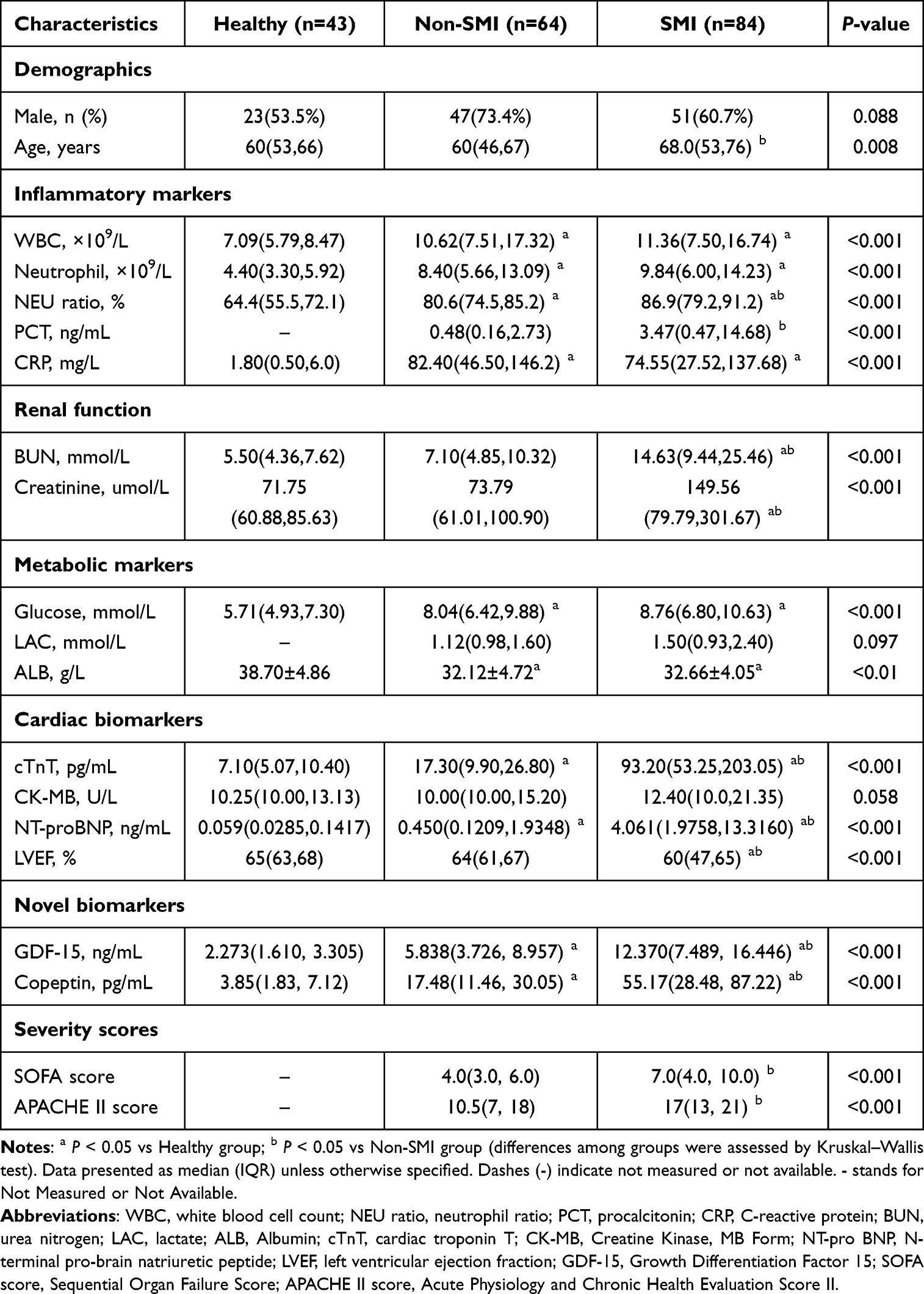 |
Table 1 Baseline Characteristics of the Study Population |
Serum Copeptin and GDF-15 Levels (Table 1)
Both biomarkers demonstrated significant intergroup differences (P < 0.001). The SMI group showed substantially elevated median copeptin levels (55.17 pg/mL, IQR 28.48–87.22) compared to both the sepsis group (17.48 pg/mL, P < 0.05) and healthy controls (3.85 pg/mL, P < 0.05). Similarly, GDF-15 levels were markedly higher in the SMI group (12.370 ng/mL, IQR 7.489, 16.446) than in either the sepsis group (5.838 ng/mL, P < 0.01) or healthy controls (2.273 ng/mL, P < 0.01).
Correlation Analysis of Biomarkers with Clinical Parameters
Spearman’s rank correlation analysis was conducted to assess the relationships between copeptin, GDF-15, and clinical indicators (Figure 2). The analysis revealed that GDF-15 showed significant positive correlations with inflammatory markers (PCT: r=0.273, P=0.016), disease severity scores (SOFA score: r=0.365, P<0.01; APACHE II score: r=0.363, P<0.01), and myocardial injury biomarkers. In contrast, copeptin demonstrated no significant associations with either myocardial injury markers or inflammatory indicators (all P>0.05).
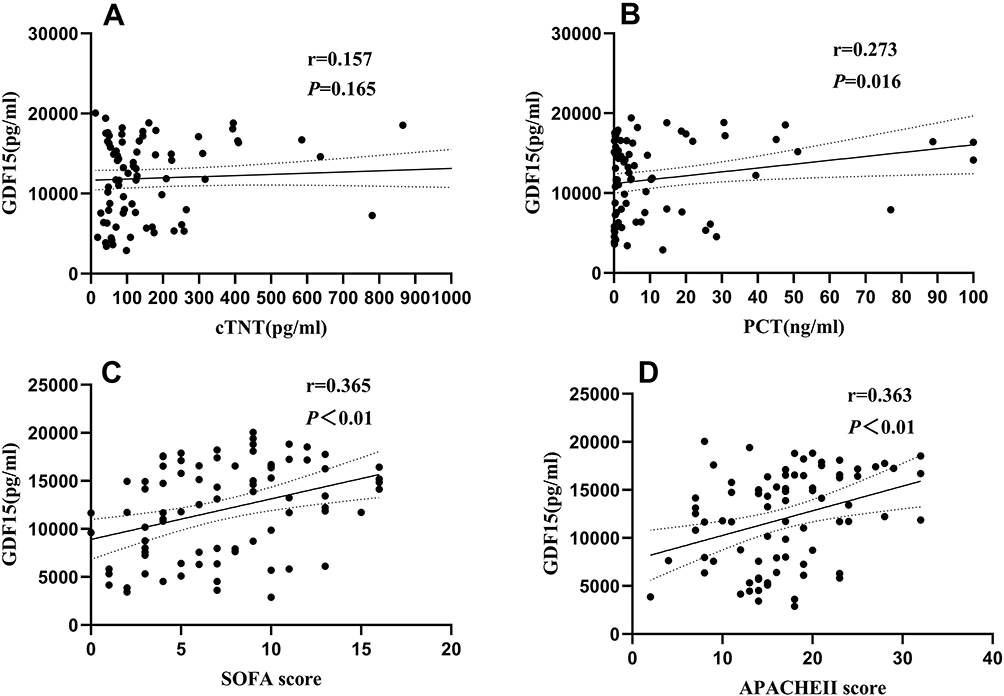 |
Figure 2 Correlation between serum GDF-15 and other clinical indicators. Spearman correlation analysis showing the relationships between serum GDF-15 levels clinical indicators. (A) Correlation between GDF-15 and cTnT. (B) Correlation between GDF-15 and PCT. (C) Correlation between GDF-15 and SOFA score. (D) Correlation between GDF-15 and APACHE II score. Abbreviations: GDF-15, growth differentiation factor 15; cTnT, cardiac troponin T; PCT, procalcitonin; SOFA, Sequential Organ Failure Assessment; APACHE II, Acute Physiology and Chronic Health Evaluation II. |
Factors Independently Associated with Sepsis-Related Myocardial Injury
The results of the univariate logistic regression analysis are shown in Supplementary Figure 1. Multiple variables significantly associated with SMI include age, glucose, elevated inflammatory markers (WBC, neutrophil ratio, PCT, CRP), impaired renal function (BUN, creatinine), cardiac dysfunction (reduced LVEF, elevated NT-proBNP, CK-MB), disease severity scores (SOFA and APACHE II), and novel biomarkers (elevated GDF-15 and copeptin). Lower albumin levels were also linked to increased SMI risk.
Multivariate Logistic Regression analysis of the influencing factors for SMI patients (Table 2): elevated GDF-15 levels (OR 1.266, 95% CI 1.102–1.454; P<0.01), increased copeptin concentrations (OR 1.018, 95% CI 1.001–1.035; P<0.05), reduced LVEF (OR 0.886, 95% CI 0.818–0.960; P<0.05), elevated creatinine levels (OR 0.993, 95% CI 0.987–0.999; P<0.05), elevated CRP levels (OR 0.988, 95% CI 0.979–0.998; P<0.05), and elevated blood urea nitrogen levels (OR 1.228, 95% CI 1.079–1.398; P<0.05). All variables maintained statistical significance after adjustment for potential confounders in the final model.
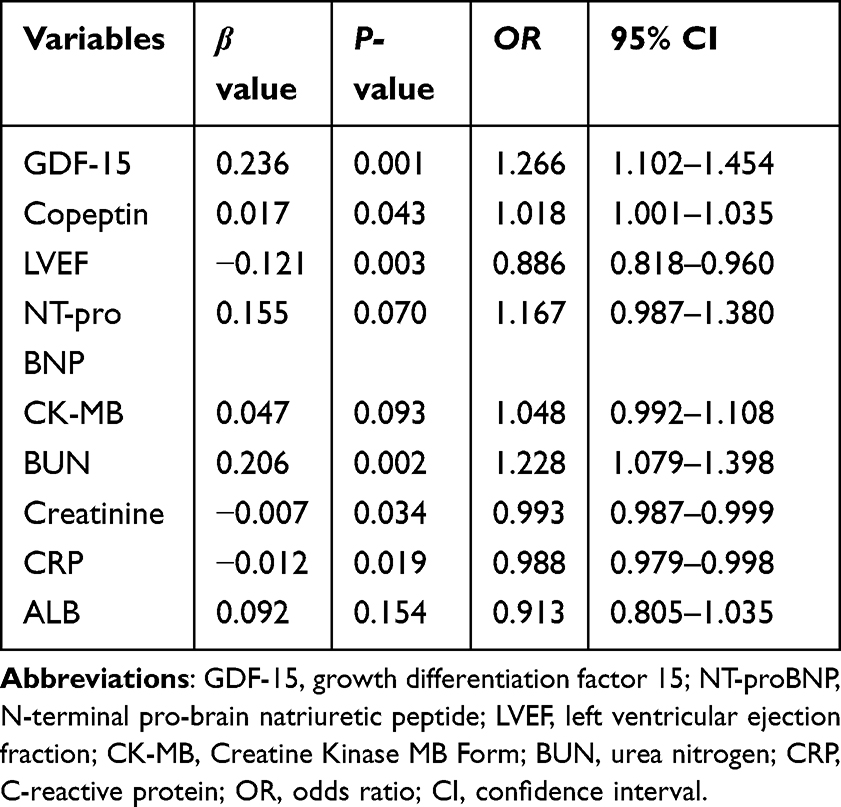 |
Table 2 Multivariate Logistic Regression Analysis of the Influencing Factors for SMI Patients |
Diagnostic Performance of Biomarkers for Sepsis-Related Myocardial Injury
Receiver operating characteristic (ROC) curve analysis was conducted to assess the diagnostic value of serum biomarkers for SMI (Table 3, Figure 3). The analysis revealed that copeptin exhibited excellent diagnostic accuracy (AUC = 0.884, 95% CI 0.837–0.931) with 69.5% sensitivity and 92.4% specificity, while GDF-15 similarly demonstrated diagnostic performance (AUC = 0.862, 95% CI 0.810–0.914) with 75.6% sensitivity and 80.2% specificity. The combination of copeptin and GDF-15 showed good diagnostic discrimination for SMI, with AUC of 0.911 (95% CI 0.871–0.951), sensitivity of 79.3% and specificity of 88.6%. However, the DeLong test revealed that the AUC of this combination was not statistically superior to that of NT-proBNP alone (AUC = 0.902, P = 0.770) (Supplementary Table 1). The comprehensive model, including copeptin, GDF-15, LVEF, CRP, creatinine, and blood urea nitrogen, achieved discriminative performance (AUC = 0.963, 95% CI 0.939–0.987; sensitivity = 94.8%; specificity = 90.4%). The DeLong test indicates that the AUC of the comprehensive model is superior to other indicators (P<0.05, Supplementary Table 1). Bootstrap internal validation showed that both combined diagnostic models retained good discrimination after optimism correction, with corrected AUCs of 0.908 for the biomarker model and 0.950 for the comprehensive model (Supplementary Table 2). These findings indicate that copeptin and GDF-15, either alone or in combination, demonstrated good discrimination for SMI.
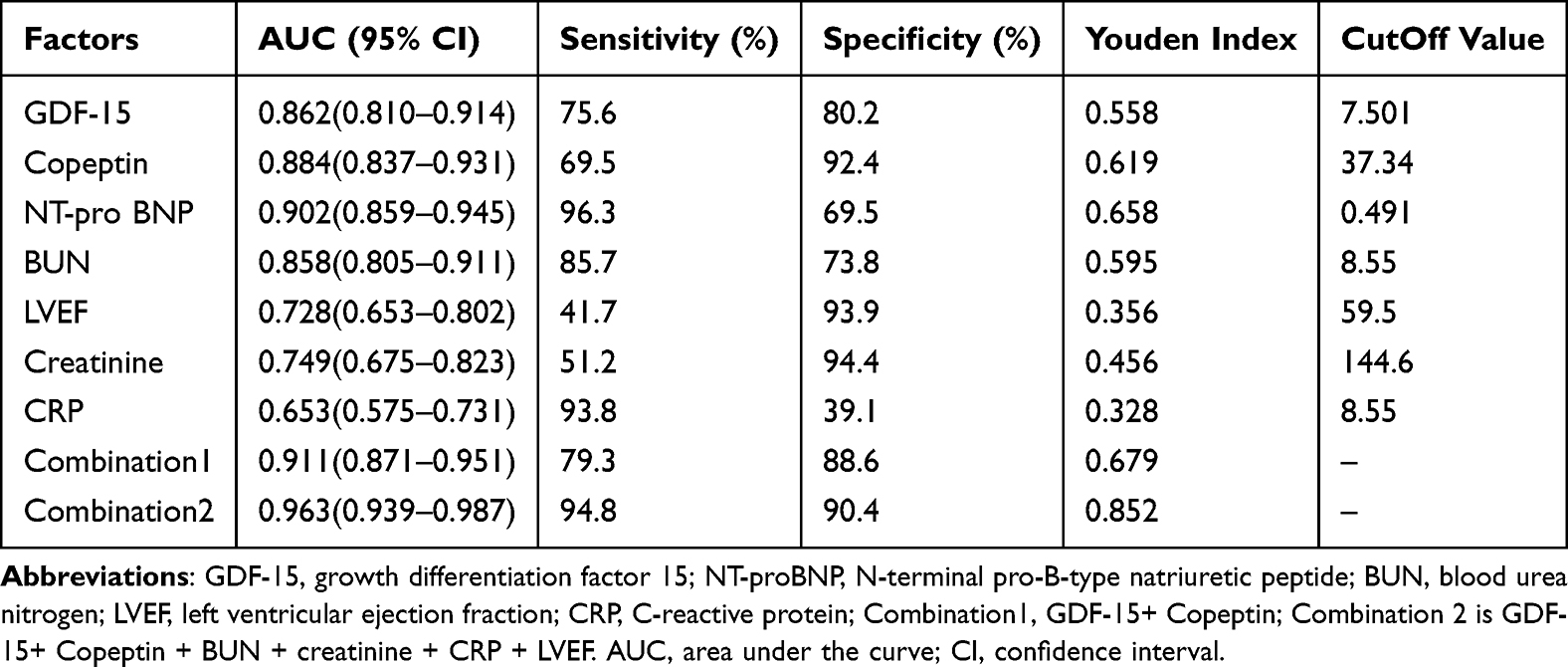 |
Table 3 Diagnostic Performance of Biomarkers and Their Combinations for SMI |
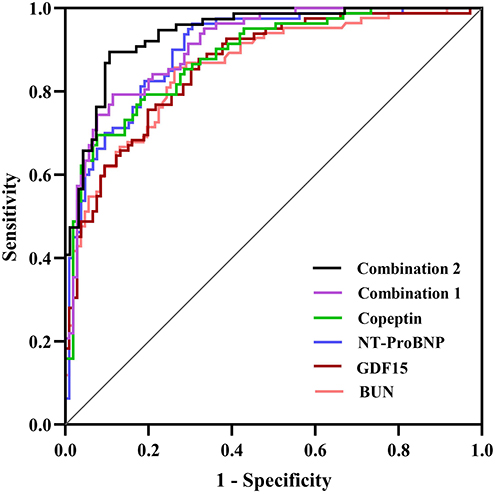 |
Figure 3 ROC curve of biomarkers in the diagnosis of SMI. Receiver operating characteristic curves showing the diagnostic performance of GDF-15, copeptin, NT-proBNP, BUN, and two combined models for identifying SMI. Combination 1 comprised GDF-15 and copeptin. Combination 2 comprised GDF-15, copeptin, BUN, creatinine, CRP, and LVEF. Abbreviations: ROC, receiver operating characteristic; SMI, sepsis-related myocardial injury; GDF-15, growth differentiation factor 15; NT-proBNP, N-terminal pro-B-type natriuretic peptide; BUN, blood urea nitrogen; CRP, C-reactive protein; LVEF, left ventricular ejection fraction. |
Discussion
In this case-control study evaluating 148 septic patients (84 with myocardial injury) and 43 healthy controls, we demonstrated the clinical significance of serum copeptin and GDF-15 for SMI. Our findings revealed significantly elevated levels of both biomarkers in SMI patients compared to non-SMI sepsis patients and healthy controls (all P<0.05). GDF-15 levels exhibited positive correlations with inflammatory markers (PCT: r=0.273, P=0.016) and disease severity scores (SOFA: r=0.365; APACHE II: r=0.363; both P<0.01). Multivariable analysis identified copeptin and GDF-15 as independent risk factors for SMI (adjusted ORs [95% CIs]: 1.018 (1.001–1.035) and 1.266 (1.102–1.454), respectively), while ROC analysis demonstrated superior diagnostic performance when combining both biomarkers (AUC=0.911, 95% CI 0.871–0.951) compared to individual measurements.
Sepsis-related myocardial injury involves multiple pathological pathways, including myocardial inhibitory factors, adrenergic pathway downregulation, oxidative/nitrosative stress, mitochondrial dysfunction, and coronary microcirculation alterations.3 Emerging evidence suggests GDF-15 plays a protective role in sepsis through its anti-inflammatory, antioxidant, and anti-apoptotic properties,29–31 while also serving as a prognostic marker in cardiovascular diseases.12 Our findings of elevated GDF-15 levels in SMI align with previous reports,17,32 with GDF-15 demonstrating significant correlations with inflammatory markers (PCT) and disease severity scores (SOFA, APACHE II; all p<0.01). Mechanistically, GDF-15 regulates triglyceride metabolism via β-adrenergic signaling to enhance inflammatory tolerance,29 modulates macrophage polarization by inhibiting AK1/STAT3 and NF-κB pathways while enhancing phagocytosis,16 and promotes M2 polarization through PI3K/Akt activation.30 Supporting evidence from GDF-15 KO mice shows exacerbated cardiac inflammation (elevated IL-6, TNF-α, MCP-1) and increased cell death following LPS challenge,33 while clinical studies confirm its role as a mitochondrial dysfunction marker (14/15 studies showing statistical significance).34 The correlation between GDF-15 and established sepsis markers (PCT, severity scores) suggests its potential as a systemic “stress sensor” whose expression is driven by inflammatory mediators, mitochondrial dysfunction, and multi-organ stress responses.
Copeptin, the surrogate marker of arginine vasopressin, is raised in sepsis, confirming arginine vasopressin system activation and reflecting acute stress responses in sepsis.18 Copeptin concentrations were documented that could be employed as an early marker to identify patients at increased risk of COVID-19-related complications (particularly acute kidney injury and sepsis) and mortality.35 Clinical studies demonstrate positive correlations between copeptin and the stress marker cortisol,36 with Qian Zhang et al reporting progressive increases in serum copeptin, total/free cortisol, and ACTH corresponding to sepsis severity,37 supporting sepsis-induced hypothalamic-pituitary-adrenal axis (HPAA) activation and subsequent free cortisol elevation.37,38 Both copeptin and arginine vasopressin are co-secreted from the posterior pituitary in response to diverse stressors, including systemic inflammation, circulatory compromise, and physiological stress, with arginine vasopressin mediating vasoconstriction and HPAA stress response modulation.
B-type natriuretic peptide is released under ventricular wall stress, reflecting the myocardial loading conditions. Biomarkers of myocardial cell injury (troponin) and myocardial loading conditions (BNP) are often elevated in sepsis,6,39 but their lack of specificity complicates SMI assessment.39–41 Copeptin and GDF-15 were higher in the SMI group than in the non-SMI sepsis group in our study, they may provide insights into different biological processes in SMI. The findings suggest that copeptin and GDF-15 may help identify myocardial injury in sepsis patients and may support early risk assessment in emergency and critical care unit.
However, copeptin and GDF-15 should be regarded as adjunctive markers rather than specific diagnostic markers for SMI. GDF-15 may increase in systemic inflammation, oxidative stress, and cardiovascular disease,12,15,16,29,30 while copeptin may increase in sepsis, septic shock, hemodynamic instability and other critical illnesses.18,23–25 Therefore, copeptin and GDF-15 should not be employed as sole diagnostic markers for SMI. They should be interpreted together with clinical assessment, cardiac troponin, echocardiography, and other laboratory findings. The optimal cut-off values for copeptin and GDF-15 identified by ROC analysis in this study should also be interpreted with caution. The cut-off values were derived from a single-center retrospective cohort and should be considered exploratory rather than definitive clinical thresholds. They may be influenced by patient characteristics, assay platform, sampling time, disease severity, and diagnostic criteria. Further multicenter studies with standardized assays and external validation are needed before these thresholds can be used in routine clinical practice.
This study has several limitations that warrant consideration: First, the single-center retrospective case-control design and relatively small sample size may introduce selection bias and limit the generalizability of our findings; Second, SMI can manifest in various ways. LVEF reflects only the heart’s contraction function. The study did not fully evaluate all forms of sepsis-related cardiac dysfunction, impacting the generalizability of our findings; Third, although internal validation was performed for the combined diagnostic models, external validation was not available. The diagnostic performance of these models should therefore be confirmed in independent, multicenter cohorts. Finally, the absence of serial biomarker measurements restricts our analysis to a single time point, precluding assessment of temporal trends and peak expression patterns. Future multicenter studies incorporating longitudinal biomarker monitoring, other forms of cardiac dysfunction, and mechanistic investigations are needed to validate and extend our conclusions.
Conclusion
This study showed that serum copeptin and GDF-15 levels were significantly elevated in SMI patients compared with sepsis patients without SMI and healthy controls. Copeptin and GDF-15 may serve as complementary biomarkers for the early identification of SMI in patients with sepsis. However, copeptin and GDF-15 are not specific for SMI, and the ROC-derived cut-off values should be considered exploratory. Further multicenter studies with standardized methods and external validation are needed to confirm these findings.
Abbreviations
SMI, sepsis-related myocardial injury; SIC, sepsis-induced cardiomyopathy; GDF-15, growth differentiation factor-15; LV, left ventricular; RV, right ventricular; Hs-TnI, high-sensitivity troponin I; BNP, brain natriuretic peptide; TGF-β, transforming growth factor-β; IL-6, interleukin-6; AVP, arginine vasopressin; pre-proAVP, pre-pro-arginine vasopressin, WBC, white blood cell count; NEU ratio, neutrophil ratio; PCT, procalcitonin; CRP, C-reactive protein; BUN, urea nitrogen; LAC, lactate; ALB, Albumin; cTnT, cardiac troponin T; CK-MB is Creatine Kinase, MB Form; NT-pro BNP, N-terminal pro-brain natriuretic peptide; LVEF, left ventricular ejection fraction; SOFA, Sequential organ failure assessment; APACHE II score is Acute physiology and chronic health evaluation score II; OR, odds ratio; CI, confidence interval; AUC, Area under the curve; ROC, Receiver operating characteristic; IQR, Interquartile range.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to limitations of ethics approval and data confidentiality restrictions, but are available from the corresponding author, Bei Hu, on reasonable request.
Ethics Approval and Consent to Participate
The study protocol was approved by the Institutional Review Board of Guangdong Provincial People’s Hospital (Ethics Approval No: KY2025-487-04) and conducted by the Declaration of Helsinki. Informed consent was obtained from all participants or their legal representatives.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from the Noncommunicable Chronic Diseases-National Science and Technology Major Project (2023ZD0504400), Noncommunicable Chronic Diseases-National Science and Technology Major Project (2023ZD0505500), Guangdong Provincial Science and Technology Planning Project (2023B110009), and National Key Research and Development Program intergovernmental key projects (2023YFE0114300).
Disclosure
All authors declare that they have no conflicts of interest.
References
1. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–12. doi:10.1001/jama.2016.0287
2. Weng L, Yang X, Yin P, et al. National incidence and mortality of hospitalized sepsis in China. Crit Care. 2023;27(1):84. doi:10.1186/s13054-023-04385-x
3. Hollenberg SM, Singer M. Pathophysiology of sepsis-induced cardiomyopathy. Nat Rev Cardiol. 2021;18(6):424–434. doi:10.1038/s41569-020-00492-2
4. Emergency Medicine Committee of Chinese Medical Doctor Association, Emergency Medicine Committee of China Medical Women’s Association. Expert consensus on the emergency clinical application of growth differentiation factor‑15 in acute coronary syndrome. Chin J Emerg Med. 2022;31(10):1319–1325. doi:10.3760/cma.j.issn.1671-0282.2022.10.004
5. Sanfilippo F, Corredor C, Arcadipane A, et al. Tissue Doppler assessment of diastolic function and relationship with mortality in critically ill septic patients: a systematic review and meta-analysis. Br J Anaesth. 2017;119(4):583–594. doi:10.1093/bja/aex254
6. Beesley SJ, Weber G, Sarge T, et al. Septic Cardiomyopathy. Crit Care Med. 2018;46(4):625–634. doi:10.1097/CCM.0000000000002851
7. Yang W, Cao Y, Li J, et al. Pathogenesis and treatment strategies of sepsis-induced myocardial injury: modern and traditional medical perspectives. Int J Biol Sci. 2025;21(8):3478–3504. doi:10.7150/ijbs.111288
8. Kim JS, Kim M, Kim YJ, et al. Troponin testing for assessing sepsis-induced myocardial dysfunction in patients with septic shock. J Clin Med. 2019;8(2):239. doi:10.3390/jcm8020239
9. Pandompatam G, Kashani K, Vallabhajosyula S. The role of natriuretic peptides in the management, outcomes and prognosis of sepsis and septic shock. Rev Bras Ter Intensiva. 2019;31(3):368–378. doi:10.5935/0103-507X.20190060
10. Breit SN, Johnen H, Cook AD, et al. The TGF-β superfamily cytokine, MIC-1/GDF15: a pleotrophic cytokine with roles in inflammation, cancer and metabolism. Growth Factors. 2011;29(5):187–195. doi:10.3109/08977194.2011.607137
11. Moore AG, Brown DA, Fairlie WD, et al. The transforming growth factor-β superfamily cytokine macrophage inhibitory cytokine-1 is present in high concentrations in the serum of pregnant women. J Clin Endocrinol Metab. 2000;85(12):4781–4788. doi:10.1210/jcem.85.12.7007
12. Xiao QA, He Q, Zeng J, Xia X. GDF-15, a future therapeutic target of glucolipid metabolic disorders and cardiovascular disease. Biomed Pharmacother. 2022;146:112582. doi:10.1016/j.biopha.2021.112582
13. Xue H, Fu Z, Chen Y, et al. The association of growth differentiation factor-15 with left ventricular hypertrophy in hypertensive patients. PLoS One. 2012;7(10):e46534. doi:10.1371/journal.pone.0046534
14. Fuernau G, Poenisch C, Eitel I, et al. Growth-differentiation factor 15 and osteoprotegerin in acute myocardial infarction complicated by cardiogenic shock: a biomarker substudy of the IABP-SHOCK II-trial. European J of Heart Fail. 2014;16(8):880–887. doi:10.1002/ejhf.117
15. Wang J, Wei L, Yang X, Zhong J. Roles of growth differentiation factor 15 in atherosclerosis and coronary artery disease. JAHA. 2019;8(17):e012826. doi:10.1161/JAHA.119.012826
16. Li H, Tang D, Chen J, Hu Y, Cai X, Zhang P. The clinical value of GDF15 and its prospective mechanism in sepsis. Front Immunol. 2021;12:710977. doi:10.3389/fimmu.2021.710977
17. Lin W, Xiaoyan L, Lizhong Z, Yuan S. Expression and diagnostic value of growth differentiation factor 15 in patients with septic cardiomyopathy. Chin Crit Care Med. 2024;36(2):137–141. doi:10.3760/cma.j.cn121430-20230529-00404
18. Yilman M, Erenler AK, Baydin A. Copeptin: a diagnostic factor for critical patients. Eur Rev Med Pharmacol Sci. 2015;19(16):3030–3036.
19. Freynhofer MK, Tajsić M, Wojta J, Huber K. Biomarkers in acute coronary artery disease. Wien Med Wochenschr. 2012;162(21–22):489–498. doi:10.1007/s10354-012-0148-2
20. Yalta K, Yalta T, Sivri N, Yetkin E. Copeptin and cardiovascular disease: a review of a novel neurohormone. Int J Cardiol. 2013;167(5):1750–1759. doi:10.1016/j.ijcard.2012.12.039
21. Morgenthaler NG, Struck J, Alonso C, Bergmann A. Assay for the measurement of copeptin, a stable peptide derived from the precursor of vasopressin. Clin Chem. 2006;52(1):112–119. doi:10.1373/clinchem.2005.060038
22. Balanescu S, Kopp P, Gaskill MB, Morgenthaler NG, Schindler C, Rutishauser J. Correlation of plasma copeptin and vasopressin concentrations in hypo-, iso-, and hyperosmolar States. J Clin Endocrinol Metab. 2011;96(4):1046–1052. doi:10.1210/jc.2010-2499
23. Bhattarai A, Shah S, Baidya S, et al. Association of copeptin levels with patient prognosis and survival in sepsis syndromes: a meta-analysis. Int J Surg. 2024;110(4):2355–2365. doi:10.1097/JS9.0000000000001069
24. Gomes DA, de Almeida Beltrão RL, de Oliveira Junior FM, et al. Vasopressin and copeptin release during sepsis and septic shock. Peptides. 2021;136:170437. doi:10.1016/j.peptides.2020.170437
25. Battista S, Audisio U, Galluzzo C, et al. Assessment of diagnostic and prognostic role of copeptin in the clinical setting of sepsis. Biomed Res Int. 2016;2016:3624730. doi:10.1155/2016/3624730
26. Pedersen CK, Stengaard C, Bøtker MT, Søndergaard HM, Dodt KK, Terkelsen CJ. Accelerated -rule-out of acute myocardial infarction using prehospital copeptin and in-hospital troponin: the AROMI study. Eur Heart J. 2023;44(38):3875–3888. doi:10.1093/eurheartj/ehad447
27. Schneider MP, Schmid M, Nadal J, et al. Copeptin, natriuretic peptides, and cardiovascular outcomes in patients with CKD: the german chronic kidney disease (GCKD) study. Kidney Med. 2023;5(11):100725. doi:10.1016/j.xkme.2023.100725
28. Lai W, Liu L, Wang S, T Q, Liu Y, Chai Y. The impact of diabetes on Sepsis-induced cardiomyopathy. Diabet Res Clin Pract. 2025;220:112001. doi:10.1016/j.diabres.2025.112001
29. Luan HH, Wang A, Hilliard BK, et al. GDF15 is an inflammation-induced central mediator of tissue tolerance. Cell. 2019;178(5):1231–1244.e11. doi:10.1016/j.cell.2019.07.033
30. Zhang X, Dong S. Protective effect of growth differentiation factor 15 in sepsis by regulating macrophage polarization and its mechanism. Bioengineered. 2022;13(4):9687–9707. doi:10.1080/21655979.2022.2059903
31. Rochette L, Dogon G, Zeller M, Cottin Y, Vergely C. GDF15 and cardiac cells: current concepts and new insights. Int J Mol Sci. 2021;22(16):8889. doi:10.3390/ijms22168889
32. Li X, Sun H, Zhang L, et al. GDF15 attenuates sepsis-induced myocardial dysfunction by inhibiting cardiomyocytes ferroptosis via the SOCS1/GPX4 signaling pathway. Eur J Pharmacol. 2024;982:176894. doi:10.1016/j.ejphar.2024.176894
33. Abulizi P, Loganathan N, Zhao D, et al. Growth differentiation factor-15 deficiency augments inflammatory response and exacerbates septic heart and renal injury induced by lipopolysaccharide. Sci Rep. 2017;7(1):1037. doi:10.1038/s41598-017-00902-5
34. Shayota BJ. Biomarkers of mitochondrial disorders. Neurotherapeutics. 2024;21(1):e00325. doi:10.1016/j.neurot.2024.e00325
35. Indirli R, Bandera A, Valenti L, et al. Prognostic value of copeptin and mid-regional proadrenomedullin in COVID-19-hospitalized patients. Eur J Clin Invest. 2022;52(5):e13753. doi:10.1111/eci.13753
36. Smaradottir MI, Andersen K, Gudnason V, Näsman P, Rydén L, Mellbin LG. Copeptin is associated with mortality in elderly people. Eur J Clin Invest. 2021;51(7):e13516. doi:10.1111/eci.13516
37. Zhang Q, Dong G, Zhao X, Wang M, Li C-S. Prognostic significance of hypothalamic–pituitary–adrenal axis hormones in early sepsis: a study performed in the emergency department. Intensive Care Med. 2014;40(10):1499–1508. doi:10.1007/s00134-014-3468-4
38. Molenaar N, Johan Groeneveld AB, Dijstelbloem HM, et al. Assessing adrenal insufficiency of corticosteroid secretion using free versus total cortisol levels in critical illness. Intensive Care Med. 2011;37(12):1986–1993. doi:10.1007/s00134-011-2342-x
39. Landesberg G, Jaffe AS, Gilon D, et al. Troponin elevation in severe sepsis and septic shock: the role of left ventricular diastolic dysfunction and right ventricular dilatation. Crit Care Med. 2014;42(4):790–800. doi:10.1097/CCM.0000000000000107
40. Sato R, Sanfilippo F, Lanspa M, Duggal A, D S. Sepsis-induced cardiomyopathy: mechanism, prevalence, assessment, prognosis, and management. Chest. 2025;168(6):1383–1394. doi:10.1016/j.chest.2025.08.013
41. Masson S, Caironi P, Fanizza C, et al. Sequential N-terminal Pro-B-type natriuretic peptide and high-sensitivity cardiac troponin measurements during albumin replacement in patients with severe sepsis or septic shock. Crit Care Med. 2016;44(4):707–716. doi:10.1097/CCM.0000000000001473
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.