Back to Journals » Infection and Drug Resistance » Volume 16
Diagnostic Significance of Targeted Next-Generation Sequencing in Central Nervous System Infections in Neurosurgery of Pediatrics
Authors Li J, Zhang L, Yang X, Wang P, Feng L, Guo E, Chen Y
Received 10 January 2023
Accepted for publication 12 April 2023
Published 15 April 2023 Volume 2023:16 Pages 2227—2236
DOI https://doi.org/10.2147/IDR.S404277
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Jihong Li,1,* Lili Zhang,2,* Xiaohui Yang,2 Pan Wang,2 Lijie Feng,2 Erkun Guo,3 Yuan Chen2
1Department of Laboratory Medicine, The Second Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050000, People’s Republic of China; 2Department of Pediatrics, The Second Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050000, People’s Republic of China; 3Department of Neurosurgery, The Second Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuan Chen, Department of Pediatrics, The Second Hospital of Hebei Medical University, 215 Heping West Road, Shijiazhuang, 050000, Hebei, People’s Republic of China, Tel +86-311-66002936, Email [email protected]
Background: Cerebrospinal fluid (CSF) pathogen culture suffers from the drawbacks of prolonged cycle time and a low positivity rate in diagnosing intracranial infections in children. This study aims to investigate the diagnostic potential of targeted next-generation sequencing (tNGS) in pediatric neurosurgery for central nervous system (CNS) infections.
Methods: A retrospective study was conducted on children under 14 with suspected intracranial infections following craniocerebral trauma or surgery between November 2018 and August 2020. Routine, biochemical, smear, and pathogen culture tests were performed on CSF during treatment. The main parameters of CSF analysis encompassed white blood cells (WBC, × 106/L) count, percentage of multinucleated cells (%), protein levels (g/L), glucose concentration (GLU, mmol/L), chloride levels (mmol/L), and pressure (mmH2O). The outcomes of tNGS were assessed through the Receiver Operating Characteristic (ROC) curve and pertinent diagnostic parameters.
Results: Among the 35 included pediatric patients, 22 were clinically diagnosed with CNS infection in neurosurgery, tNGS was confirmed in 18 cases. The sensitivity and specificity of tNGS were 81.8% and 76.9%, respectively, while the traditional method of CSF cultures and smears exhibited a sensitivity of 13.6% and a specificity of 100%. ROC curve analysis indicated an area under the curve (AUC) of 0.794 for tNGS and 0.568 for the CSF cultures and smears. CSF analysis indicated that the two groups exhibited statistically significant differences in terms of WBC count [330.0 (110.00– 2639.75) vs 14.00 (4.50– 26.50), P< 0.001] and percentage of multinuclear cells (%) [87.50 (39.75– 90.00) vs 0 (0– 10.00), P< 0.001]. However, the remaining parameters did not statistically significant differences between the groups (all P> 0.05).
Conclusion: tNGS demonstrates a high degree of diagnostic accuracy when detecting infections within the CNS of pediatric neurosurgery patients. tNGS can effectively establish for diagnosing CNS infections by detecting pathogenic microorganisms and their corresponding virulence and/or resistance genes within the test samples.
Keywords: targeted next-generation sequencing, neurosurgery, central nervous system infections, cerebrospinal fluid, diagnostic
Introduction
Neurosurgical infections affecting the central nervous system (CNS) encompass post-operative epidural abscesses, subdural pus, meningitis, brain abscesses, intracranial infections resulting from craniocerebral trauma, extraventricular and lumbar pool drainage, shunts, and meningitis associated with implants.1,2 In children, CNS infections can have a profound impact on neurological development. Acute symptoms may include fever, headache, vomiting and signs of cerebral edema. Altered mental and conscious states can lead to intracranial hemorrhage, seizures, and permanent neurological complications like deafness, ataxia, hemiparesis, paralysis, epilepsy, inattention, memory impairment, speech disorders, and cerebral edema.3–5
Studies have revealed a wide range of 1–30% for the prevalence of post-craniotomy infections in children,6–10 potentially attributed to distinct etiologies causing diverse modes of craniotomy in children and varying inclusion criteria. Moreover, the incidence of post-traumatic meningitis alone is 0.38%, which is significantly elevated in the presence of CSF leakage.11 A positive pathogen diagnosis is confirmed when the patient’s specimen smear, drainage tube, and CSF pathogen culture all indicate the presence of pathogens. Nevertheless, this diagnostic approach has limitations, such as a long cycle time, a low positivity rate, and reduced accuracy if patients have received prior antibiotic treatment.12,13 In the same vein, detecting Mycobacterium tuberculosis, viruses, and fungi in CSF cultures presents a more significant challenge.14,15 However, next generation sequencing (NGS) technology offers a swift and precise means of obtaining microbial genomic data, making it a formidable tool in microbial molecular ecology research.16 Macrogenomic Next Generation Sequencing (mNGS) enables high-throughput sequencing of a specimen’s biological genome. However, targeted NGS (tNGS) offers the benefits of simplicity and expediency in comparison.17 By employing ultra-multiplex polymerase chain reaction (PCR) amplification and high-throughput sequencing technology, tNGS has proven helpful in identifying tens to hundreds of known pathogenic microorganisms, along with their virulence and/or resistance genes in the samples being analyzed. TNGS is increasingly garnering attention in clinical testing due to its lower sequencing cost and clear pathogenic spectrum range, in contrast to mNGS.14,18 Prof. Peng Hu’s team’s research has demonstrated that tNGS can achieve comparable efficacy to mNGS in identifying pneumonia pathogens.19 Nevertheless, there need to be more studies examining the use of tNGS in critically ill pediatric children.20–22 Furthermore, there currently needs to be more research focused on the pathogens responsible for CNS infections in children undergoing neurosurgery, making it difficult to understand the range of infections affecting this population entirely. By leveraging the increased sensitivity of NGS over traditional diagnostic methods like CSF culture, it is possible to obtain valuable pathogenic information for children with suspected intracranial infections. While the use of tNGS may initially entail higher costs and require additional steps for primer or probe synthesis, it can substantially enhance the sensitivity of identifying known pathogens in comparison to mNGS. Additionally, tNGS offers the advantage of integrating both DNA and RNA processes, which not only reduces detection time but also provides a cost-effective and highly customizable solution.
The primary aim of this study was to assess the diagnostic efficacy of tNGS in detecting pathogens responsible for intracranial infections related to neurosurgical procedures, specifically in pediatric patients undergoing craniotomy or experiencing head trauma.
Materials and Methods
Study Subjects
Data were collected on children with suspected intracranial infection after craniocerebral trauma or surgical operations and aged <14 years old who were admitted to the pediatric intensive care unit of the Second Hospital of Hebei Medical University between November 2018 and August 2020. The data gathered for this study encompassed various parameters such as gender, age, underlying medical condition, type of surgery, antibiotic usage, clinical manifestations, treatment regimen, and therapeutic outcomes. Both traditional and tNGS-based diagnostic test results were tabulated to determine their respective positivity rates. Before conducting the study, ethical clearance was obtained from the Ethics Committee of the Second Hospital of Hebei Medical University under the approval number 2019-R280, and the ethical principles conformed to the current Declaration of Helsinki. Furthermore, written informed consent was obtained from the legal guardians of the children after explaining the study’s objective and ensuring complete comprehension.
The eligibility criteria for participation in this study comprised of two main aspects: (1) the presence of clinical symptoms indicative of CNS infection, such as fever, altered mental status, and meningeal irritation signs; (2) the absence of conclusive evidence for or against intracranial infection, necessitating further investigation. Conversely, exclusion criteria consisted of (1) children who did not undergo craniocerebral trauma or surgical interventions; (2) children with insufficient CSF samples for analysis.
Diagnostic Gold Standard
The Chinese Expert Consensus on the Diagnosis and Management of Neurosurgical CNS Infections is the definitive standard for diagnosing intracranial infections related to neurosurgical procedures (Version 2021).23 Including, (1) Clinical manifestations: systemic inflammatory reaction, altered consciousness and mental status, signs and symptoms of increased intracranial pressure, signs of meningeal irritation and other complications such as electrolyte disorders; (2) Routine blood leukocytes >10.0×109/L, neutrophil ratio >0.8; (3) Intracranial pressure and CSF-related tests: CSF pressure >200 mmH2O, CSF properties such as turbid or yellow, total white blood cell count >100*106/L, neutrophil ratio >0.7, CSF glucose <2.2 mmol/L, etc.; (4) Imaging manifestations: cranial CT or MRI of meningitis is not specific, and cerebral abscess can appear with typical circumferential enhancement; (5) Positive bacterial cultures of specimen smears, drainage tips, implants and CSF, subject to the exclusion of bacterial contamination and colonization. In the above inclusion criteria, the clinical diagnosis of CNS infection can be made if (1)-(4) are met. When a child has a fever, intracranial hypertension, turbid or purulent cerebrospinal fluid, increased white blood cells, glucose <2.2mmol/L, and cerebrospinal fluid glucose content/serum glucose content ≤0.4, the clinical diagnosis of intracranial infection in children can be established. All children in the positive clinical diagnosis group have symptoms such as fever, intracranial hypertension, turbid or purulent cerebrospinal fluid, and increased white blood cells. However, not all children have decreased cerebrospinal fluid glucose.
Collection, Preservation and Testing of Specimens
In suspected cases of intracranial infection following surgery or trauma in children, prompt lumbar puncture should be performed under sterile conditions to obtain CSF specimens. For children with lumbar cistern drainage, lumbar puncture is no longer necessary, and the CSF in the lumen is discarded while ensuring a sterile technique. The collected CSF specimens underwent routine biochemical, smear, and culture tests and were preserved for tNGS analysis. Put the cerebrospinal fluid into the centrifuge and centrifuge at 3000rpm for 15 minutes. Inoculate the centrifuged material on Columbia agar, Chocolate agar, MacConkey agar, and Sabouraud (SDA) agar. Then, observe the results and place the agar plates in a cultural environment of 35 degrees Celsius and 5% carbon dioxide for 18–24 hours. All of the agar plates were purchased from Oxoid (Japan). Subsequently, the specimens were stored at −80°C until further testing. The microbiological assessment was conducted using the Curetis Unyvero™ system. The samples were automatically processed following a predefined protocol using the Lysator, which liquefies each sample within 30 minutes through lysis buffer and Proteinase K, thereby inactivating any infectious pathogens. The nucleic acids were then automatically extracted using the Biotek extractor and quantified by the Unyvero system before being amplified by polymerase chain reaction (PCR) using a multiplex primer set and internal process control primers. Target capture and library creation were accomplished via purification using magnetic beads, and the qualified DNA libraries were sequenced on the Illumina high-throughput sequencing platform.
Library Preparation Protocol and Pipeline for Bioinformatics Analysis
The Biological Information Analysis™ system was used to detect microbial genes rapidly. In the detection system, 200µL of the cerebrospinal fluid sample was added, and the sample tubes were processed completely automatically according to a pre-selected protocol. Sample tubes are uniformly sealed with a cap and contain proteinase K, lysozyme, Staphylococcus lysate, snail enzyme, and an internal control gene as part of the quality control workflow for each sample. When combined with lysis buffer and proteinase K, each sample was liquefied within 30 minutes, and all potential infectious pathogens were inactivated. After lysis, a Biotek extractor was applied for automated nucleic acid extraction. The nucleic acid is quantified using the Unyvero system, then amplified by polymerase chain reaction (PCR). The PCR detection method includes multiplex primer sets and internal process controls for the primer combinations. The product has established target capture and sequencing libraries using magnetic bead-based methods. Qualified DNA libraries were sequenced on the Illumina high-throughput sequencing platform. The sequencing data is automatically normalized based on the amplification calibration coefficient. A total of 10,000 sequencing reads are analyzed for each sample.
Statistical Analysis
The data were organized and analyzed using SPSS 25.0 and MedCalc software. Categorical variables were presented as frequencies and percentages. In contrast, continuous variables that followed a normal distribution were expressed as mean ± standard deviation. Those not following normal distribution were presented as the median and interquartile range (25%, 75%). Diagnostic efficacy measures, such as sensitivity, specificity, positive predictive value, negative predictive value, and the Youden index, were calculated by comparing tNGS and traditional methods against the clinical diagnosis of CNS infection as the standard. The receiver operating characteristic (ROC) curve was plotted to determine the area under the curve (AUC). A P-value of less than 0.05 was considered statistically significant. Two continuous data sets were compared using the t-test (normal distribution) or the nonparametric Mann–Whitney (non-normal distribution) test.
Results
Clinical Data of the Children
A total of 40 patients were included in this study according to the inclusion and exclusion criteria. Subsequently, we performed tNGS testing of CSF on them. Out of them, five cases were excluded due to incomplete data, resulting in a final valid specimen volume of 35 cases. There were 22 children with intracranial infections and 13 with non-intracranial infections, according to the Chinese Expert Consensus on diagnosing and treating CNS infections in neurosurgery (version 2021). The basic information of the two groups is shown in Table 1. A total of fifteen males and seven females were in the intracranial infection group; the age quartile was 76.5 months (30.0–115.33). Six males and seven females were in the non-intracranial infection group, with a mean age of 77.4 months. The frequency of symptoms such as fever, nausea, vomiting, dizziness, headache, signs of meningeal irritation, pathological signs, and neurological impairment (including hypotonia of the extremities, dull pupil-to-light reflex, blurred vision, and poor swallowing) was found to be higher in children with intracranial infections compared to the non-infection group. Conversely, seizures and changes in mental consciousness were lower in the intracranial infection group than in the non-infection group (Table 1). Of all pediatric patients, 34 (97.1%) experienced intracranial hypertension. Further imaging revealed five patients developed postoperative or traumatic cerebral edema, including 4 cases in the infection group and 1 in the non-infection group (Figure 1).
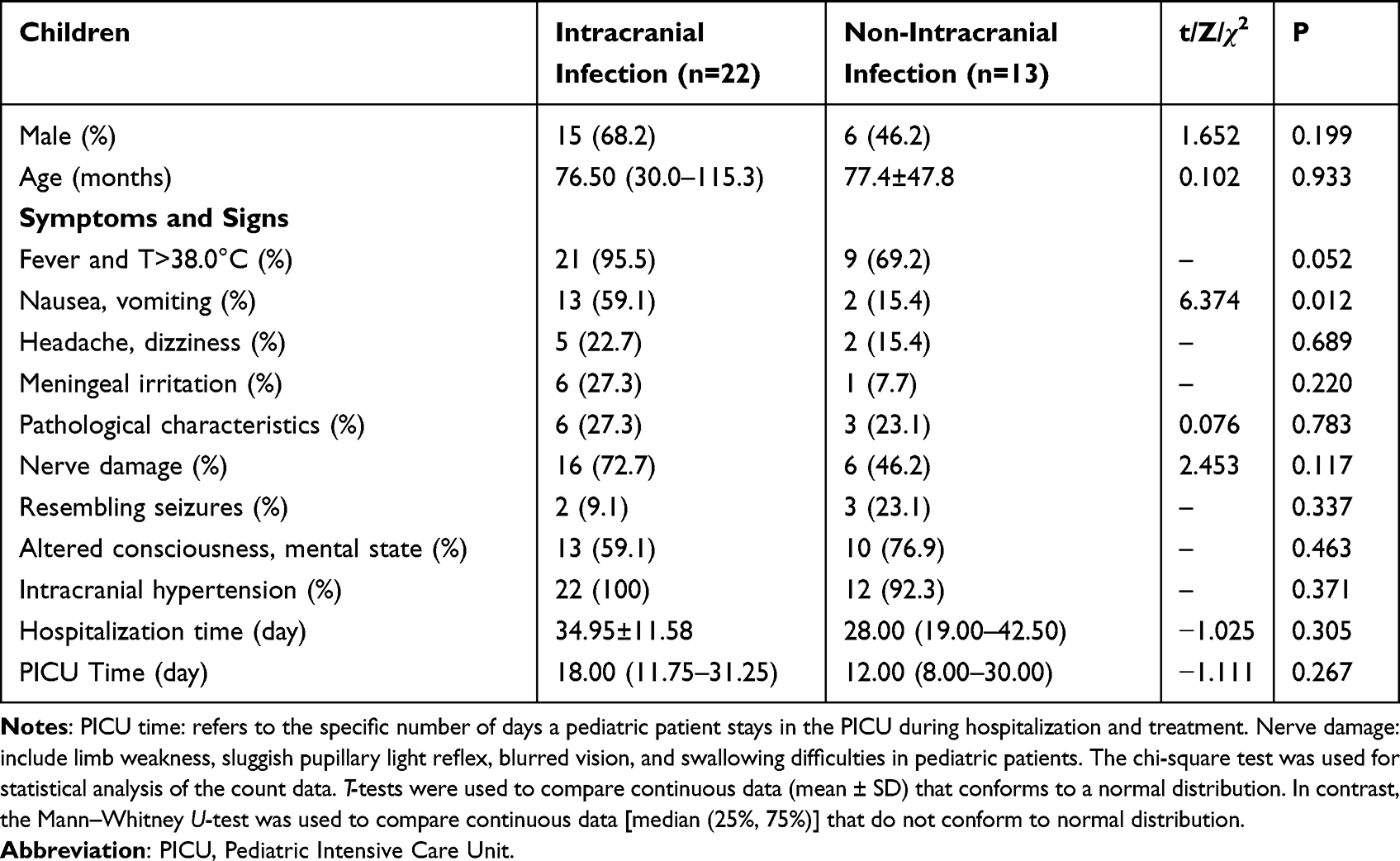 |
Table 1 Baseline Characteristics of the Children |
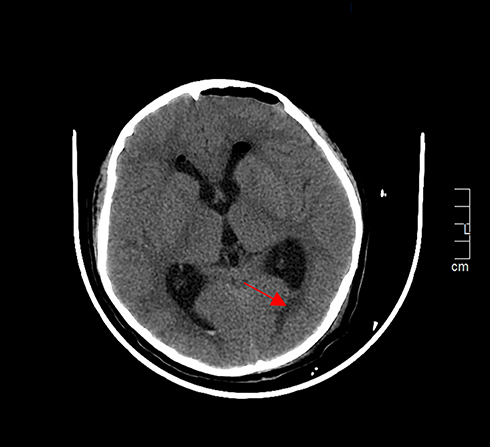 |
Figure 1 Imaging of children presenting with cerebral edema (red arrows represent edema sites). |
Among the 35 included pediatric patients, 28 cases underwent neurosurgery due to causes such as tumors, vascular malformations, arteriovenous malformations, or transparent septum cysts that resulted in infection, six cases were due to head trauma, and one case involved a child with head trauma and a tumor. Among the six children with superficial traumatic brain injury, three underwent emergency surgery, two did not, and one underwent subdural puncture. One child with traumatic brain injury, intracranial hemorrhage, and tumor underwent craniotomy. Among the 22 children, a total of 3 cases had head injury, tNGS was performed in a child with basal fracture, sinus fracture and CSF tinnitus. The results showed that this child was infected with pathogens, including Staphylococcus haemolyticus, Staphylococcus epidermidis, and Human herpesvirus type 6. Among the two children who tested negative for tNGS, one had frontal bone fractures, and the other had left temporoparietal fractures. All except one child received antibiotic prophylaxis before craniotomy with drugs such as cefuroxime sodium, cefamandole sodium, ceftriaxone sodium, and tazobactam sodium. After surgery, 14 children in the infected group and 10 in the non-infected group received external drainage, and 4 children in the infected group received V-P shunts after the infection had improved. The total length of stay and pediatric ICU stays did not differ significantly between the two groups (P>0.05, respectively) (Table 1). Children with intracranial infection had more symptoms, such as fever, nausea and vomiting, dizziness, headache, and signs of meningeal irritation, along with neurological impairment. The proportion of seizures and changes in mental consciousness was lower compared to the non-infected group.
Pathogenic Test
The pathogenic diagnosis of 22 children with intracranial infection was clarified by conventional pathogenic testing methods such as CSF smear or culture in 3 cases, accounting for 13.63% of the children with intracranial infection; among them, 2 cases of CSF smear were Gram-negative bacilli, and 1 case of CSF culture was Enterococcus faecalis. tNGS tested twenty-two specimens of CSF, and among all the detected microorganisms, Gram-negative bacilli had the highest detection rate (48.6%), with Stenotrophomonas maltophilia (3 cases), Legionella (3 cases), and Pseudomonas aeruginosa (2 cases) being the most common; followed by Gram-positive bacteria (31.4%), with Staphylococcus in 4 cases, and Streptococcus crista in 2 cases; viruses had the lowest composition ratio (20%), with Cytomegalovirus being the most common (3 cases), and mixed infections with bacteria (Table 2).
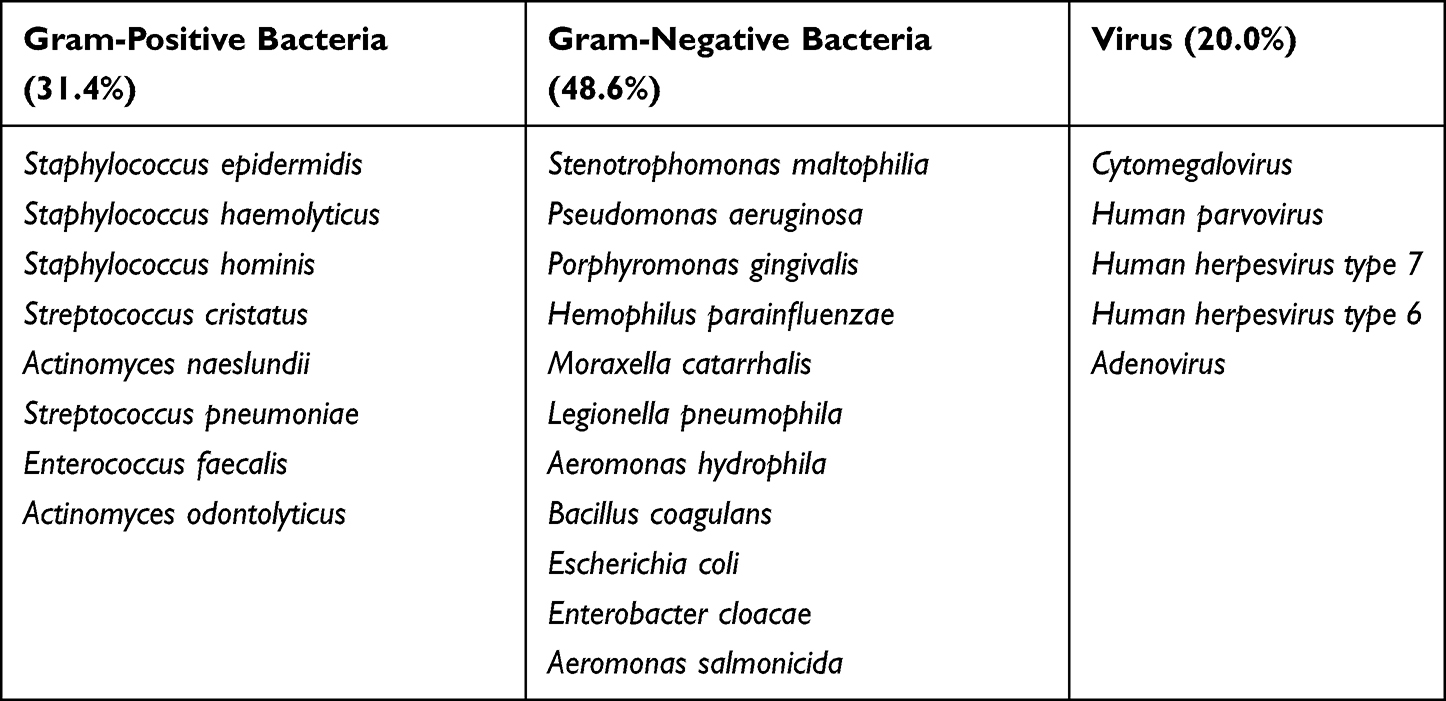 |
Table 2 Pathogenetic Test Results of tNGS |
Evaluation of the Diagnostic Efficacy of tNGS and Traditional Methods
The detailed test results of the traditional method and tNGS are shown in Table 3. Twenty-two children with intracranial infection were clinically diagnosed, and 3 cases had positive results of the traditional method, among which one case had the same smear result and tNGS result, both were gram-negative bacilli; 1 case had gram-negative bacilli in smear and negative tNGS result; 1 case had Enterococcus faecalis in culture and maltophilic narrow-feeding monococcus in tNGS result. The tNGS test results showed a total of 18 positive cases. The diagnosis of 16 cases was positive by tNGS and negative by traditional methods, among which 10 cases were mixed infections; 3 cases were negative by both tNGS and traditional methods. The AUC of tNGS was 0.794 (95% CI: 0.629–0.958), sensitivity 81.8%, specificity 76.9%, positive predictive value 85.7%, negative predictive value 71.4%, and Youden index is 0.587; the conventional method had an AUC of 0.568 (95% CI: 0.375–0.761), the sensitivity of 13.6%, specificity of 100%, the positive predictive value of 100%, the negative predictive value of 59.1%, and Youden index is 0.136 (Figure 2).
 |
Table 3 Comparison of Clinical, Targeted NGS, and Conventional Methods for Diagnosing CNS Infections (N=35) |
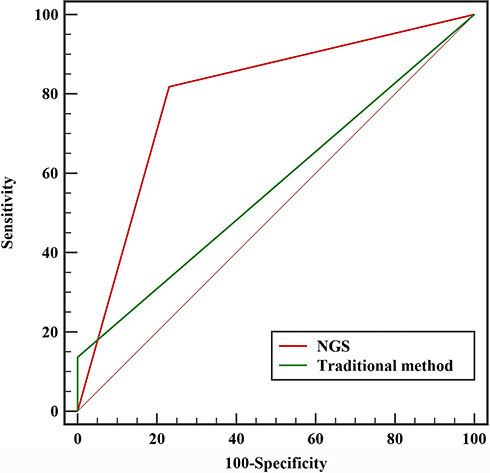 |
Figure 2 Area under the ROC curve for tNGS and conventional diagnostic methods. |
CSF Characteristics
We conducted a statistical analysis of protein, glucose, and other parameters in the CSF of children in both groups. The median values of CSF leukocytes were 330.0×10^6/L and 14.0×10^6/L in the intracranial infected and non-infected groups, respectively, with a statistically significant difference between the two groups (P<0.001). The infected group showed a higher percentage of polynuclear cells in the CSF than the non-infected group, with a statistically significant difference (P<0.001). However, the two groups had no statistically significant differences in CSF pressure, protein, glucose, and chloride (P=0.300, 0.0932, 0.116, and 0.054, respectively) (Table 4).
 |
Table 4 The Value of CSF Between the Infection Group and Non-Infection Group |
Discussion
Surgical procedures such as craniotomy and craniocerebral trauma can weaken the blood-brain barrier in children, making them susceptible to intracranial infections. Prophylactic antibiotics are commonly administered in clinical practice to reduce the incidence of postoperative CNS infections; however, this approach limits the ability to identify bacterial or viral species through culture-based methods. There needs to be more literature on the pathogenic diversity of surgically relevant intracranial infections in children. A study by Dong et al on the analysis of the diagnosis and management of multi-drug resistant bacteria in intracranial infections after craniotomy in children showed that Gram-positive cocci (including Staphylococcus epidermidis, Staphylococcus intermedius, and Staphylococcus haemolyticus) accounted for 70% of the CSF cultures in children with intracranial infections after neurosurgery. Gram-negative bacilli (including Klebsiella pneumonia, Klebsiella acidophilus, and Escherichia coli) accounted for only about 30% of the cases, and there are complex infections.24 A study of CNS infections in neurosurgical patients, including adults and children, found that Gram-positive organisms remain the most common pathogens. However, there has been a yearly increase in the incidence of Gram-negative pathogens.25,26 Lau et al11 reported a study of post-traumatic meningitis. Their study had six cases of post-traumatic meningitis in children; four were pneumococci, one was a group A Streptococcus spp., and one was E. coli. This study showed a 0.38% incidence of post-traumatic meningitis. Post-traumatic meningitis was significantly higher in patients with CSF leaks.
Rapid and accurate pathogenic diagnosis of intracranial infections is crucial for effective antimicrobial treatment and improving patient outcomes. Second-generation sequencing technology, such as tNGS, offers a unique reference tool for the pathogenic diagnosis of infectious diseases in clinical settings. By combining ultra-multiplex PCR amplification and high-throughput sequencing, tNGS can detect dozens to hundreds of known pathogenic microorganisms, including their virulence and/or resistance genes, with a high positive rate and fast detection speed. Unlike CSF culture, tNGS can simultaneously detect pathogenic bacteria, colonizing bacteria, rare bacteria, viruses, fungi, parasites, and other microorganisms, providing a comprehensive pathogen spectrum for clinicians. Compared to pathogen metagenomic next-generation sequencing (mNGS), tNGS has a clear pathogen spectrum range and lower sequencing costs. In this study, tNGS identified pathogenic infections in 18 out of 22 children with intracranial infections, yielding a positive rate of 81.82%. Among all infected children, Gram-negative bacteria were detected most frequently, followed by Gram-positive bacteria, while viruses had the lowest proportion. The diagnostic efficacy of tNGS was higher than that of conventional assays, as shown by its AUC of 0.794, which was significantly better than traditional assays. Overall, this study demonstrated that tNGS is a valuable tool for rapid and accurate diagnosis of intracranial infections, with a high agreement with the standard gold diagnosis.
The mechanism behind oral colonization of the CNS still needs to be precise. Previous studies have shown that infections involving the head and neck region can present symptoms such as fever, headache, and hypothermia in CNS infections.27,28 The mechanism by which oral colonizing bacteria cause intracranial infections in the CNS is currently unknown. Previous studies on intracranial bacterial infections of oral origin have shown that dental diseases such as gingivitis, periodontitis, and oral and other surgeries can cause intracranial infections. Hematogenous transmission is typically the primary mode of infection, although blood cultures were negative in 88.9% of reported studies. The diversity and complexity of odontogenic microorganisms make them challenging to culture. When intracranial infections of oral origin are suspected, they are usually treated empirically with broad-spectrum antibiotics, which can impact pathogen cultures.29 Unfortunately, we cannot elaborate on their correlation due to the limited number of cases involving CSF leakage in our study and the fact that the NGS test results did not reveal any oral colonizing infections. However, diagnosing oral pathogens using tNGS may provide an essential reference for treating children with neurosurgical CNS infections. tNGS testing can identify oral bacteria, including Streptococcus crests, Porphyromonas gingivalis, Actinomyces caries, and Bacillus coagulans. Among the patients in this study, 6 children, who had all undergone craniotomy, developed infections caused by oral colonizing bacteria. One case was treated with neuroendoscopic transsphenoidal saddle area mass excision, and the NGS test result showed Actinomyces caries. The other five patients underwent quadruple ventriculotomy to excise occupying lesions and tumors in the right jugular foramen area. Actinomyces caries is considered part of the normal oropharyngeal flora and is a conditional pathogen.
tNGS can also be crucial in diagnosing children with non-intracranial infections, especially when CSF leukocyte count is not significantly elevated, for instance, a child with head trauma presented with fever, lethargy, and marked cerebral edema. Although their CSF was yellow and turbid with a higher than normal CSF protein, the leukocyte count was below 100x10^6/L. The patient’s condition improved after anti-infective treatment with ceftriaxone sodium, tazobactam sodium, desmethyl vancomycin, and meropenem, highlighting the importance of using tNGS to identify potential pathogens in such cases. CSF tNGS testing suggested that the patient’s intracranial infections were Actinobacillus carcinogens, human staphylococcus, and Enterococcus faecalis infections. One child developed postoperative fever, vomiting, poor mental health, and neck resistance. The patient had elevated CSF pressure, a leukocyte count of 20×106/L in the CSF, and a slightly higher protein concentration. The patient improved after being given his ceftriaxone tazobactam sodium anti-infective treatment. The CSF tNGS showed Haemophilus influenzae infection. This suggests that when intracranial infection occurs in children, the type of infecting agent, clinical presentation and indicators such as leukocytes in the CSF may not be entirely consistent.
tNGS technology also has some limitations. For example, the test may have false negative results. In this study, one child was diagnosed with Cytomegalovirus by tNGS. However, this diagnosis was inconsistent with his clinical symptoms. One child was diagnosed with Enterococcus faecalis by CSF culture, but the diagnosis of Stenotrophomonas maltophilia by tNGS. The inconsistency of the above diagnosis may be related to the prolonged delivery time of the tNGS test and the quality of the retained specimen. False-positive results in tNGS can arise from specimen collection, reagent contamination during testing, and the influence of host-derived gene sequences, especially in neurosurgical children with intracranial bleeding or disruption of the blood-brain barrier that leads to the mixing of blood cells into the CSF. Furthermore, there is currently no standardized approach for interpreting tNGS results. Experienced clinicians must interpret the findings in the context of the child’s clinical symptoms and other ancillary tests, introducing an element of subjectivity.
The tNGS test provides a more comprehensive pathogen spectrum for intracranial infections in neurosurgical children than CSF cultures. It has a high positive rate and is faster, able to detect pathogenic, colonizing, rare, and causative bacteria, viruses, fungi, and parasites simultaneously. Compared with mNGS, tNGS sequencing is more sensitive to genotyping, with fewer read segments, and offers the advantages of high sensitivity, efficiency, and economy. This study evaluated the value of tNGS multi-pathogen results in diagnosing central neurosurgical infections based on the therapeutic diagnosis. The results demonstrate that CSF NGS is a powerful supplement for diagnosing neurosurgical intracranial infections and can compensate for the low positive rate of CSF culture. However, tNGS test results cannot be the gold standard for diagnosing intracranial infections but can be used with other indicators for a synergistic diagnosis. Further sample studies, detailed and comprehensive detection procedures, and standardized interpretation criteria are necessary to optimize its use in clinical practice.
Conclusion
The incidence of post-craniotomy infection in children may be grossly underestimated because of the impaired blood-brain barrier. This study shows that tNGS can compensate for the low positive detection rate of traditional CSF pathogenic microorganism culture and can be used as an excellent auxiliary diagnostic method in diagnosing intracranial infections in clinical practice. The tNGS technology can effectively help clinical doctors identify the pathogen types that cause intracranial infections, which is crucial for the subsequent treatment of patients.
Acknowledgments
Jihong Li and Lili Zhang share first authorship.
Funding
The project was supported by the S&T Program of Hebei No.20377785D.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Van Wyck DW, James ML. Central nervous system infection in neurosurgical critical care. In: Essentials of Neurosurgical Anesthesia & Critical Care: Strategies for Prevention, Early Detection, and Successful Management of Perioperative Complications. Springer; 2020:619–626.
2. LaPenna PA, Roos KL. Bacterial Infections of the Central Nervous System. Thieme Medical Publishers; 2019:334–342.
3. Kuchar E, Nitsch-Osuch A, Rorat M, et al. Etiology and complications of central nervous system infections in children treated in a pediatric intensive care unit in Poland. J Child Neurol. 2014;29(4):483–486. doi:10.1177/0883073813477689
4. Chen T, Liu G. Long‐term outcome of acute central nervous system infection in children. Pediatr Investig. 2018;2(3):155–163. doi:10.1002/ped4.12054
5. van der Velden FJ, Battersby A, Pareja-Cebrian L, Ross N, Ball SL, Emonts M. Paediatric focal intracranial suppurative infection: a UK single-centre retrospective cohort study. BMC Pediatr. 2019;19(1):1–10. doi:10.1186/s12887-019-1486-7
6. Proust Houdemont S, De Carli E, Delion M, et al. Short-term neurological outcome of children after surgery for brain tumors: incidence and characteristics in a pediatric intensive care unit. Childs Nerv Syst. 2011;27(6):933–941. doi:10.1007/s00381-010-1373-x
7. Lassen B, Helseth E, Egge A, Due-Tønnessen BJ, Rønning P, Meling TR. Surgical mortality and selected complications in 273 consecutive craniotomies for intracranial tumors in pediatric patients. Neurosurgery. 2012;70(4):936–943. doi:10.1227/NEU.0b013e31823bcc61
8. Von Lehe M, Kim H-J, Schramm J, Simon M. A comprehensive analysis of early outcomes and complication rates after 769 craniotomies in pediatric patients. Childs Nerv Syst. 2013;29(5):781–790. doi:10.1007/s00381-012-2006-3
9. Phung J, Mathern GW, Krogstad P. Timing and predictors of fever and infection after craniotomy for epilepsy in children. Pediatr Infect Dis J. 2013;32(5):450. doi:10.1097/INF.0b013e318287b408
10. Wang Z, Gong J. Analysis of risk factors for intracranial infection after craniotomy in children. Chin J Clin Neurosurg. 2021;26(6):457–459.
11. Lau Y, Kenna A. Post-traumatic meningitis in children. Injury. 1986;17(6):407–409. doi:10.1016/0020-1383(86)90082-3
12. Kanegaye JT, Soliemanzadeh P, Bradley JS. Lumbar puncture in pediatric bacterial meningitis: defining the time interval for recovery of cerebrospinal fluid pathogens after parenteral antibiotic pretreatment. Pediatrics. 2001;108(5):1169–1174. doi:10.1542/peds.108.5.1169
13. Singhi S, Angurana SK. Principles of management of central nervous system infections. Indian J Pediatr. 2019;86(1):52–59. doi:10.1007/s12098-017-2583-y
14. Cameron ES, Schmidt PJ, Tremblay BJM, Emelko MB, Müller KM. Enhancing diversity analysis by repeatedly rarefying next generation sequencing data describing microbial communities. Sci Rep. 2021;11(1):22302. doi:10.1038/s41598-021-01636-1
15. Gu J, Chen L, Zeng C, et al. A retrospective analysis of metagenomic next generation sequencing (mNGS) of cerebrospinal fluid from patients with suspected encephalitis or meningitis infections. J Healthc Eng. 2022;2022:1–6. doi:10.1155/2022/5641609
16. Chen T, Zhang L, Huang W, et al. Detection of pathogens and antimicrobial resistance genes in ventilator-associated pneumonia by metagenomic next-generation sequencing approach. Infect Drug Resist. 2023:923–936. doi:10.2147/IDR.S397755
17. Deurenberg RH, Bathoorn E, Chlebowicz MA, et al. Application of next generation sequencing in clinical microbiology and infection prevention. J Biotechnol. 2017;243:16–24. doi:10.1016/j.jbiotec.2016.12.022
18. Gulilat M, Lamb T, Teft WA, et al. Targeted next generation sequencing as a tool for precision medicine. BMC Med Genomics. 2019;12(1):1–17. doi:10.1186/s12920-019-0527-2
19. Li S, Tong J, Liu Y, Shen W, Hu P. Targeted next generation sequencing is comparable with metagenomic next generation sequencing in adults with pneumonia for pathogenic microorganism detection. J Infect. 2022;85(5):e127–e129. doi:10.1016/j.jinf.2022.08.022
20. Giardino G, Gallo V, Somma D, et al. Targeted next-generation sequencing revealed MYD88 deficiency in a child with chronic yersiniosis and granulomatous lymphadenitis. J Allergy Clin Immunol. 2016;137(5):1591–1595. doi:10.1016/j.jaci.2015.09.050
21. Wang H, Lu Z, Bao Y, et al. Clinical diagnostic application of metagenomic next-generation sequencing in children with severe nonresponding pneumonia. PLoS One. 2020;15(6):e0232610. doi:10.1371/journal.pone.0232610
22. Fusaro M, Rosain J, Grandin V, et al. Improving the diagnostic efficiency of primary immunodeficiencies with targeted next-generation sequencing. J Allergy Clin Immunol. 2021;147(2):734–737. doi:10.1016/j.jaci.2020.05.046
23. Neurocritical Care Expert Committee of the Neurosurgeons Branch of the Chinese Medical Association, Neurosurgery Critical Care Group of the Beijing Medical Association. Chinese expert consensus on the diagnosis and treatment of central nervous system infections in neurosurgery (2021 edition). Chin Neurosurg J. 2021;37(1):14.
24. Dong Y, Du K, Zhang X, Jia T. Analysis of multi-drug resistant bacteria diagnosis and treatment of intracranial infections in children after craniotomy. Chin J Pract Nerv Dis. 2016;19(10):89–91.
25. Srihawan C, Castelblanco RL, Salazar L, et al. Clinical Characteristics and Predictors of Adverse Outcome in Adult and Pediatric Patients with Healthcare-Associated Ventriculitis and Meningitis. Oxford University Press; 2016.
26. Palabiyikoglu I, Tekeli E, Cokca F, et al. Nosocomial meningitis in a university hospital between 1993 and 2002. J Hosp Infect. 2006;62(1):94–97. doi:10.1016/j.jhin.2005.06.010
27. Sampaio-Maia B, Caldas I, Pereira M, Pérez-Mongiovi D, Araujo R. The oral microbiome in health and its implication in oral and systemic diseases. Adv Appl Microbiol. 2016;97:171–210.
28. Fan B, Wu X. Disseminated actinomycosis in an immunocompetent patient: one case report and literature review. Chin J Infect Chemother. 2020;20(6):638–644.
29. Moazzam AA, Rajagopal SM, Sedghizadeh PP, Zada G, Habibian M. Intracranial bacterial infections of oral origin. J Clin Neurosci. 2015;22(5):800–806. doi:10.1016/j.jocn.2014.11.015
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.