Back to Journals » Infection and Drug Resistance » Volume 19
Diagnostic Performance of Droplet Digital PCR for Detecting Pathogens and Resistance Genes in Patients with Suspected Bloodstream Infections
Authors Wu S, Xu C, Fu Y, Zhang L, Zhang L
Received 2 October 2025
Accepted for publication 19 January 2026
Published 31 January 2026 Volume 2026:19 570142
DOI https://doi.org/10.2147/IDR.S570142
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Shengjun Wu,1 Chen Xu,2– 4 Ying Fu,2– 4 Lu Zhang,2– 4 Linyue Zhang2– 4
1School of Medical Technology and Information Engineering, Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 2Department of Clinical Laboratory, Sir Run Run Shaw Hospital, Zhejiang University, Hangzhou, People’s Republic of China; 3Key Laboratory of Precision Medicine in Diagnosis and Monitoring Research of Zhejiang Province, Hangzhou, People’s Republic of China; 4Zhejiang Provincial Engineering Research Center for Innovative Pathogen Precision Detection Instruments, Hangzhou, People’s Republic of China
Correspondence: Linyue Zhang, Department of clinical laboratory, Sir Run Run Shaw Hospital, Zhejiang University, No. 3 Qingchun East Road, Hangzhou, Zhejiang Province, People’s Republic of China, Email [email protected]
Purpose: We aimed to evaluate the diagnostic performance and clinical impact of droplet digital PCR (ddPCR) in patients with suspected bloodstream infections (BSIs) and demonstrated how ddPCR can benefit diagnostic and antimicrobial stewardship efforts.
Patients and Methods: We conducted a prospective study in a tertiary hospital in China, 50 patients with suspected BSIs were recruited and 50 blood samples were collected for ddPCR and blood culture (BC).
Results: In terms of diagnostic performance, ddPCR exhibited a superior detection rate (64% vs 30%), a relatively high sensitivity (86.67%), and less turn-around time (27.16 ± 13.95 hours vs 70.87 ± 15.8 hours, P < 0.0001) compared to BC. The presence of blaKPC and Klebsiella pneumoniae was detected by ddPCR and later confirmed by BC in three patients. Based on the rapid ddPCR results, the antimicrobial therapy was adjusted to ceftazidime/avibactam (2.5 g q8h) to target the pathogen. This case showed that ddPCR could reduce the time to diagnosis and promotes precise antibiotic use.
Conclusion: The clinical value of ddPCR is to detect and quantify pathogens and resistance genes early to provide appropriate guidance for therapeutic options.
Keywords: droplet digital PCR, antibiotic resistance genes, clinical application, carbapenem resistance
Introduction
Bloodstream infection (BSI) is a major public health burden with estimated overall mortality rates ranging from 15% to 30%.1 Administering the right antimicrobial medications promptly is one of the most effective ways to decrease mortality.2 In a clinical context, early and empirical antibiotic treatment is started before the pathogen and its susceptibility are reported. The physician must weigh the advantages of widespread coverage against the expenses of the antibiotic, adverse effects, and development of resistance.3 For hospitalized patients with bacterial infections, inappropriate empirical antibiotic treatment was associated with an increased risk of death.4 The more rapidly appropriate antimicrobials are prescribed, the lower the mortality.5 Proper management of patients with BSI involves a thorough diagnostic evaluation to identify the source of infection, appropriate antibiotics, and timely source control. Additionally, the duration of therapy should be carefully considered.6 Prompt identification of the responsible pathogen in the early stages allows clinicians to implement appropriate antibiotic therapy timely.
Blood culture (BC) is the gold standard for the diagnosis of BSIs and sepsis pathogens.7 Nevertheless, when applying BC, it could take approximately 1 day from the time of specimen collection to obtain Gram stain results, 2 days to identify organisms, and 3 days to report antimicrobial susceptibility results.8 Although BC has been the gold standard and most common method for bloodstream pathogens diagnosis, it could be enhanced with more advanced methods that can reduce the turn-around time (TAT) from several days to a few hours. Molecular testing without culturing significantly improves the timeliness of targeted therapy compared to BC, rapid molecular testing combined with direct communication with physicians is associated with a significant decrease in mortality.5
Polymerase chain reaction (PCR) is a molecular biology technique used to multiply certain DNA fragments. Droplet digital polymerase chain reaction (ddPCR) represents a biotechnological advancement of traditional PCR techniques. ddPCR is similar to quantitative PCR (qPCR) in that it uses amplification reagents and that successful amplification of target molecules is registered by fluorescent readout. The main difference between ddPCR and qPCR is that the former may be more accurate and sensitive in quantifying DNA.9,10 When performing ddPCR, a sample with various nucleic acids is mixed with PCR reagents and divided into millions of separate partitions, each typically containing less than one copy of the template DNA. These partitions undergo thermal cycling and are then examined for fluorescent signals that confirm successful amplifications of the target of interest. By quantifying the partitions with successful amplifications, the absolute concentration of the original target molecules can be determined using Poisson statistics.10 Recently, ddPCR has emerged as a promising tool for detecting various pathogens such as bacteria, fungi, and viruses.11 In practice, ddPCR effectively identifies bacterial pathogens,12,13 and detects the presence of tuberculosis quantitatively and resistance-conveying mutations concurrently.14 For viral pathogens, ddPCR excels in detecting RNA viruses like SARS- CoV-2 in clinical and environmental samples.15 It also demonstrates a good performance for pulmonary invasive fungal infection diagnosis.16,17
In addition, the rise in antibiotic resistance in bacterial pathogens emerges and represents one of the biggest challenges in treating bacterial infections.18 Drug-resistant BSIs are associated with increased mortality.19 Carbapenems have a wide range of activity and are highly potent against Gram-negative bacteria. They are frequently utilized as “last-line agents” or “antibiotics of last resort” for patients who are critically ill or suspected of carrying resistant bacteria.20 The acquisition of carbapenemase is associated with carbapenem resistance, genes coding for carbapenemase in β-lactamase (bla) include blaKPC, blaNDM, blaOXA-48, blaVIM, and blaIMP. These genes are found in many bacteria, such as E. coli, K. pneumoniae, Salmonella spp., Acinetobacter spp., and Pseudomonas spp.21 For Gram-positive bacteria, methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus spp. (VRE) have become a significant health concern worldwide. The acquired mecA gene encodes penicillin-binding protein 2a (PBP2a), which takes over the activities of endogenous PBPs and, due to its low affinity for β-lactam antibiotics, is the main determinant of MRSA.22 The van genes, particularly vanA and vanM were the main determinants conferring resistance to vancomycin.23 Genes are the main drivers for antimicrobial resistance, ddPCR assay designed for rapid identification of common pathogens and specific resistance genes could be crucial for avoiding misuse of last-resort antibiotics.
In this study, we employed ddPCR panels to simultaneously identify pathogens and antibiotic resistance genes (ARGs) directly from clinical blood samples. The evaluation was conducted in a real-time clinical setting to assess both the diagnostic performance of ddPCR and its impact on diagnostic timelines and therapeutic decision-making. Among 50 patients with suspected bloodstream infections, we analyzed how ddPCR can support diagnostic workflows and advance antimicrobial stewardship (AMS) objectives. Specifically, we aimed to determine whether ddPCR-facilitated pathogen detection can enable earlier targeted therapy—through appropriate escalation or de-escalation—and help reduce the empirical use of broad-spectrum antibiotics, which are core goals of AMS programs.
Materials and Methods
Study Design
This single-center prospective cohort study with no control group was conducted at Sir Run Run Shaw Hospital in Hangzhou, China. The study has been approved by Sir Run Run Shaw Hospital’s ethical committee (2023–0247). All experiments were performed in accordance with guidelines. Informed consent was obtained from all participants and/or their legal guardians (oral or written) and this study adhered to the guidelines of the Declaration of Helsinki. A total of 50 patients were recruited from February 3 to July 4, 2023. The inclusion criteria were age >18 years and suspected BSIs. For this study, a “suspected BSI” case was defined as a patient meeting both of the following criteria. Criterion 1: Evidence of Infection or Suspected Infection. This was determined by the presence of at least one of the following: (a) Acute (within 72 hours) fever or hypothermia. (b) Elevated or decreased total white blood cell count. (c) Elevated levels of C-reactive protein (CRP) or interleukin-6 (IL-6). (d) A confirmed or clinically suspected site of infection. Criterion 2: Clinical Severity Indicator. This required the presence of at least one of the following: (a) A quick Sequential Organ Failure Assessment (qSOFA) score ≥2. (b) A Sequential Organ Failure Assessment (SOFA) score of 1. (c) A National Early Warning Score (NEWS) between 4 and 6. The combination of Criterion 1 and Criterion 2 constituted the clinical suspicion for BSIs. Patients with any terminal-stage disease, mental disorders, or pregnant women were excluded from the study. When a BSI was suspected, whole blood samples were collected for BC and ddPCR. Each patient had two sets of BC, with each set comprising one aerobic bottle and one anaerobic bottle, 8–10 mL of blood was inoculated into each bottle. About 5 mL whole blood samples were obtained for ddPCR using cell-free DNA storage tubes (Jiangsu Cowin Biotech Co., Ltd). The clinical and laboratory data of each patient were collected from the electronic medical records system. This study was conducted within the framework of an antimicrobial stewardship program at Sir Run Run Shaw Hospital. The antimicrobial stewardship program team was led by infectious disease specialists, clinical microbiologists, and clinical pharmacists. These include formulary restrictions with pre-authorization requirements for certain agents (eg, carbapenems), and the promotion of institution-specific treatment guidelines based on local antimicrobial resistance data.
Blood Culture, Pathogen Identification and Antimicrobial Susceptibility Testing (AST)
The blood samples for BC were processed using BD BACTEC ™ FX Blood Culture System (Becton Dickinson, USA) and incubated routinely for 7 days. All positive blood cultures were Gram-stained followed by subculture on a Columbia blood agar plate and a chocolate blood agar plate. After overnight incubation, colonies on the blood agar were identified by matrix-assisted laser desorption-ionization time of flight (MALDI-TOF) mass spectrometry (Bruker, Bremen, Germany). Susceptibility testing was performed by VITEK-2 Compact system (bioMérieux, Marcy l’Etoile, France) and Kirby-Bauer (K-B) disk diffusion method. The antibiotic susceptibility was interpreted according to the Clinical and Laboratory Standards Institute guidelines.24
Blood Sample Preparation and ddPCR Assay
The ddPCR assay in this study consists of five panels (Table 1) which could detect eighteen pathogens and five ARGs (Pilot Gene Technologies. Hangzhou, China). After centrifugation at 1500 × g for 10 minutes, plasma was isolated. DNA was then extracted from 2 mL of plasma, which included 10 μL of internal control A425, using the Magnetic Plasma DNA Extraction Kit (Pilot Gene Technologies. Hangzhou, China), and the Auto-Pure 10B Nucleic Acid Purification System (Hangzhou Allsheng Instruments Company, Hangzhou, China) following the manufacturer’s protocol. DNA was eluted in 100 μL of elution buffer for the following ddPCR assay. Synthesized DNA fragments were used as a positive control, and DNase-free water was used as a negative control. Each ddPCR panel utilized a master mix with a final volume of 15 μL, consisting of 1 × ddPCR premix, 1 μM of both forward and reverse primers, 300 nM for each probe, and 5 μL of isolated plasma DNA. Droplets were generated using sample preparation instrument DG32 (Pilot Gene Technologies. Hangzhou, China) and the PCR procession was performed using PCR amplification instrument TC1 (Pilot Gene Technologies, Hangzhou, China). After PCR amplification, droplet counts and fluorescence signals were analyzed using a chip scanner CS7 and GenePMS-CS7 software (v1.0.4) (Pilot Gene Technology Company, Hangzhou, China). The ddPCR results were reported in the form of copies of each targeted pathogen or ARG.
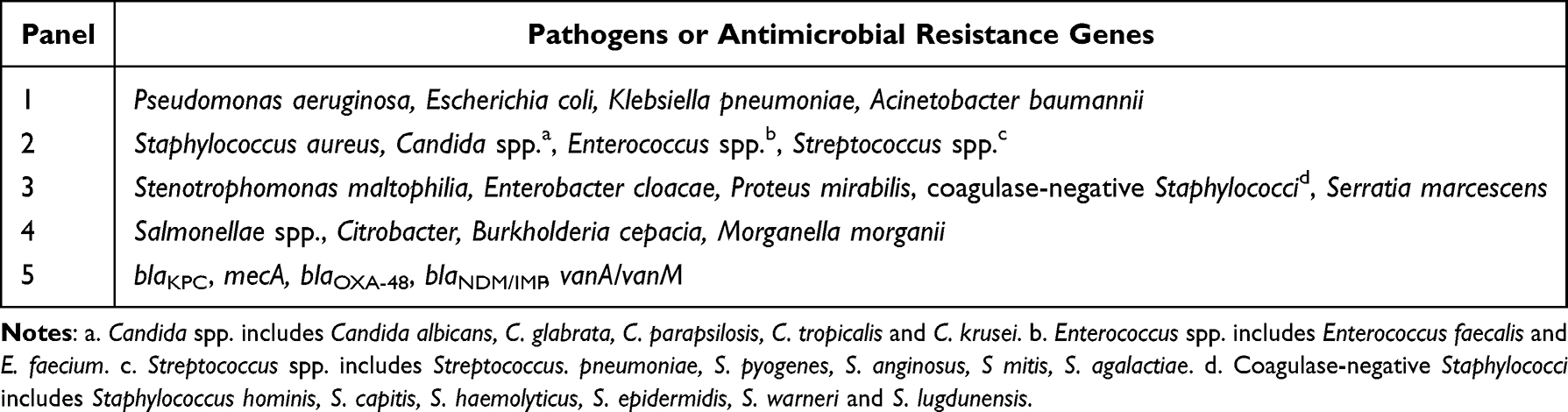 |
Table 1 Target Pathogens and Antimicrobial Resistance Genes in ddPCR Panels |
Statistical Analysis
The primary outcomes included the sensitivity, specificity, as well as positive and negative predictive values of ddPCR, with BC results considered as the gold standard. For patients with positive BC results, we defined “clinical rational therapy regimens” as the antimicrobial regimens showed in vitro activity against the bacteria detected by BC. An unfavorable outcome was defined as 28-day all-cause mortality after admission. Continuous data were presented using the mean and standard deviation (SD) or the median and corresponding interquartile range (IQR), as applicable. Categorical data were reported as counts and percentages. Quantitative variables with a normal distribution were compared using the t-test, while non-normally distributed variables were assessed using the Mann–Whitney test. The comparison of categorical variables was performed using either the χ2 test or Fisher’s exact test.
Results
General Clinical Characteristics of Recruited Patients
A total of 50 patients with suspected BSIs were consecutively recruited in this study, blood samples were collected from each patient for BC and ddPCR assay. Most patients were recruited from the intensive care unit (ICU) (48%) and the emergency department (34%), followed by the department of hematology (14%), the department of nephropathy (2%), and the department of cardiology (2%). The baseline characteristics and outcomes of patients are presented in Table 2. The median age of the patients was 67 years (IQR, 59–74 years), the youngest patient was 22 years old and the oldest was 94 years old. Male patients accounted for 76% of all patients. All patients received empirical antibiotic therapy before BC and the 28-day mortality was 28% (14/50).
 |
Table 2 Clinical Characteristics of Patients |
Diagnostic Performance of ddPCR
Eighteen Pathogens and five ARGs included in the ddPCR panels are showed in Table 1. The ddPCR assay was positive in 64% (32/50) samples while the positive rate of BC was only 30% (15/50). When divided into BC positive group and BC negative group, we found that the results of BC and ddPCR were consistent in 10 BC positive episodes and 16 BC negative episodes (Figure 1), thus the concordance rate between BC and ddPCR was 52% (26/50). We further analyzed the reason underlying the 24 inconsistent results (5 BC positive episodes and 19 BC negative episodes) (Table S1). For 3 BC-positive episodes, ddPCR detected one or two additional pathogens beyond the single species grown in BC. In contrast, for two other BC-positive episodes (involving Aeromonas veronii and Streptococcus sanguinis, respectively), ddPCR yielded negative results as both pathogens fell outside the detection range of the pre-designed panel. These cases underscore the inherent limitation of targeted molecular assays: ddPCR can produce false-negative results when the causative pathogen is not included in its detection spectrum. For the remaining 19 BC negative episodes, all 19 samples were positive in ddPCR assays with one or two pathogens. Escherichia coli, Klebsiella pneumoniae, and Staphylococcus aureus were the top three identified pathogens in both BC and ddPCR (Figure 2).
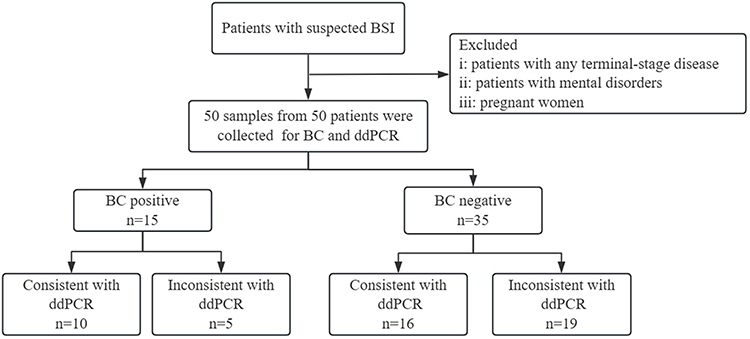 |
Figure 1 Flow chart for enrollment and results of BC and ddPCR. ddPCR, droplet digital PCR; BC, blood culture. |
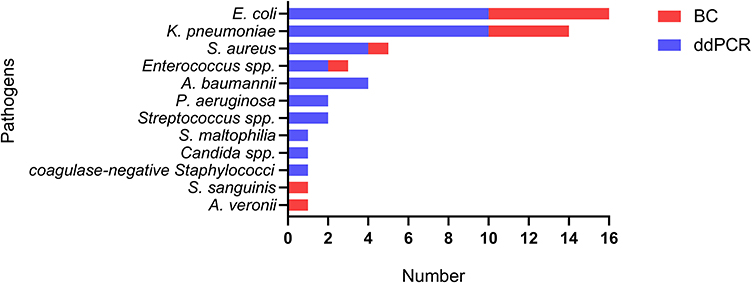 |
Figure 2 Distribution of pathogens detected by ddPCR and BC. S. sanguinis and A. veronii were not in the detection scope of ddPCR. Abbreviations: ddPCR, droplet digital PCR; BC, blood culture. |
The diagnostic performance of ddPCR is presented in Table 3. In this study, ddPCR reported 86.67% sensitivity and 88.89% negative predictive value compared to BC in patients with suspected BSIs. The specificity was 45.71% and the positive predictive value was 40.63% compared to BC. We compared the DNA concentrations of pathogens between the BC positive group and the BC negative group among patients with positive ddPCR results. For patients with both BC and ddPCR positive results, the DNA concentrations were significantly higher than those with ddPCR positive but BC negative results (Figure 3).
 |
Table 3 Positive and Negative Agreement of ddPCR versus Blood Culture (BC) |
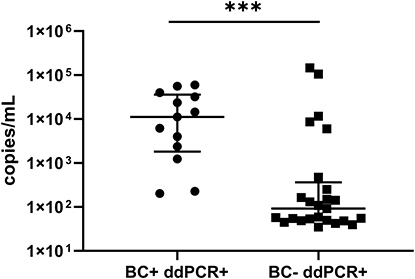 |
Figure 3 Comparison of the DNA concentrations of pathogens between BC positive group and BC negative group among patients with positive ddPCR results. ***, P < 0.001 (Mann Whitney test). Abbreviations: ddPCR, droplet digital PCR; BC, blood culture. |
In addition to pathogens, ddPCR could also detect ARGs including mecA, blaKPC, blaOXA-48, blaNDM/IMP, and vanA/vanM. Among all 50 samples, mecA was detected once in ddPCR alongside S. aureus, the BC and AST results proved the presence of Methicillin-resistant Staphylococcus aureus (MRSA), indicating the consistence with the ARG and the susceptibility phenotype. The carbapenem resistance gene blaKPC was detected four times and K. pneumoniae was simultaneously detected in all four cases by ddPCR (Table S2). BC only proved the existence of K. pneumoniae in three out of four cases, and the following AST results showed that all three strains were resistant to meropenem, imipenem, and ertapenem (Table S3), which could be defined as carbapenem-resistant Klebsiella pneumoniae (CRKP). For the remaining one, the BC was negative after a 7-day culture. The remaining three ARGs, blaOXA-48, blaNDM/IMP, and vanA/vanM were not detected in this study.
Clinical Impact of ddPCR
We compared the turn-around time (TAT) and the rationality of antibiotic treatment in 15 patients with positive BC results, the rationality was evaluated based on the AST reports and the antibiotic usage records. For BC, the mean value of TAT required for a final report was 70.87 ± 15.8 hours, while the ddPCR spent significantly less time (27.16 ± 13.95 hours) to identify the pathogens and ARGs (P < 0.0001) (Figure 4). All 15 patients received the empirical antimicrobial therapy on the date of blood sampling. Twelve of them were proven to receive appropriate empiric antibiotic therapy as the applied antibiotic could eliminate the causative pathogens (Table 4). Three patients were proved to have BSI caused by K. pneumoniae harboring blaKPC by ddPCR, indicating resistance to carbapenems. The following AST results proved that all three strains were CRKP (Table S3). The empirical antimicrobial therapy they initially received contained meropenem so the therapy could not eliminate the causative pathogens. The ddPCR results were immediately reported to the doctors and the antimicrobial therapy was adjusted to ceftazidime/avibactam 2.5 g q8h to eliminate CRKP. The adjusted antimicrobial therapy was considered rational as the AST report indicated that ceftazidime/avibactam showed in vitro activity to the pathogens in each of the three patients.
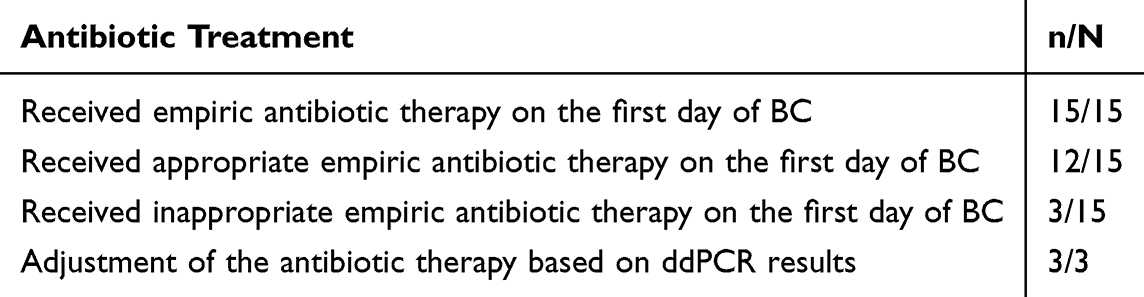 |
Table 4 Antibiotic Treatment Among Patients with Positive BC Results |
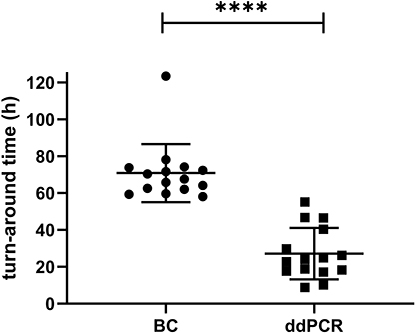 |
Figure 4 Comparison of turn-around time (TAT) between ddPCR and BC among the patients with positive BC results. ****, P < 0.0001. Abbreviations: ddPCR, droplet digital PCR; BC, blood culture. |
Discussion
The rapid identification of BSIs and the timely application of effective treatment would significantly influence clinical outcomes. Therefore, the development and integration of rapid diagnostic tools are of paramount importance.25 Our study provides more information about the diagnostic performance and clinical impact of ddPCR for patients with suspected BSI in a tertiary hospital in China. The detection rate of ddPCR is more than twice that of BC (64% vs 30%). Besides, ddPCR showed a relatively high sensitivity of 86.67% and 88.89% negative predictive value compared to BC. Considering that all patients received empirical antibiotic therapy before BC, the reduced sensitivity of BCs could stem from low bacterial abundance and prior antibiotic treatment before sampling. Applications of ddPCR for BSI diagnosis have been reported in several studies, all of which have shown the superiority of ddPCR over conventional methods.13,26–28 A retrospective study encompassed 355 episodes from 280 elderly patients with suspected BSI showed that ddPCR demonstrated significantly higher detection rates compared to BC in BSI group (59.33% versus 20.57%).29 Sheng Yin et al investigated the diagnostic value of ddPCR in combination with conventional inflammatory markers [interleukin-6 (IL-6) and procalcitonin (PCT)], the sensitivity of ddPCR was markedly higher compared to the culture method (74.71% vs 31.03%). A positive correlation existed between bacterial load and levels of inflammatory markers [IL-6 (P = 0.0182), PCT (P = 0.0029), and CRP (P = 0.0005)]. Qualitative ddPCR results can more precisely assess sepsis progression and treatment prognosis in BSI patients.30
Given the high sensitivity of ddPCR, a rigorous multi-parameter algorithm needs to be employed to differentiate true bloodstream infection from potential contamination. In this study, two ICU patients had negative blood cultures but positive ddPCR results of two pathogens: Acinetobacter baumannii (42.3 copies/mL) and Enterococcus spp. (49.05 copies/mL) in Patient 1, and Escherichia coli (129.6 copies/mL) and Coagulase-Negative Staphylococci (92.25 copies/mL) in Patient 2. The copy numbers in these cases were substantially lower than the range typically seen in ddPCR/blood culture co-positive patients (202–23,699 copies/mL). In clinical practice, such cases necessitate a comprehensive approach to differentiate contamination from infection.31 This involves correlating the results with the patient’s clinical presentation and other laboratory infection markers, repeating both blood culture and ddPCR to assess consistency, reviewing microbiological data from other sites, and incorporating additional testing such as metagenomic or targeted next-generation sequencing (mNGS/tNGS). Similar situation was also observed by Jiayi Peng et al, when detecting Streptococcus, coagulase-negative Staphylococci (CoNS), Acinetobacter baumannii complex, and Candida, they established diagnostic thresholds of 132.55, 182.70/262.24, and 174.78 copies/mL, respectively, to help differentiate false-positive results.29 For each bacterial species and resistance gene, more robust research findings are needed to progressively establish their diagnostic thresholds.
Aside from higher sensitivity, ddPCR also requires less TAT than BC (27.16 ± 13.95 hours vs 70.87 ± 15.8 hours, P < 0.0001). The whole procedure of ddPCR would take around 4 hours, but the TAT (27.16 ± 13.95 hours) was much longer than 4 hours in this study. TAT is obtained by calculating the difference between the time of blood sampling and the time of sending the final report to doctors. Researchers who performed ddPCR collected blood samples at a fixed time, which may delay TAT. This suggests that when applying ddPCR in clinical practice, it is recommended to have dedicated personnel available for testing at any time. The automation level of the ddPCR process also needs to be improved.
Early identification of pathogens is of paramount importance for guiding rapid, effective, and targeted therapy.32 A meta-analysis and our study showed that ddPCR can detect pathogenic microorganisms in patients with sepsis earlier than BC. Therefore, digital PCR can be used as a causative pathogen-related molecular diagnostic strategy without cultivating organisms.33 Fidalgo et al assessed the clinical and prognostic implications of real-time communication of microbiological information in patients with BSIs. Their findings demonstrated that promptly relaying clinically relevant microbiological data from blood culture isolates, especially in rapidly growing bacteria (eg, Enterobacterales), could influence clinical outcomes.34 E. coli and K. pneumoniae were members of Enterobacterales and were the top two identified pathogens in this study, earlier reports of these two pathogens may have positive impacts on patient outcomes. There are other developing tools for BSI diagnosis which could be rapid and commercial. Technologies such as multiplex real-time PCR (FilmArray), fluorescence in situ hybridization with peptide nucleic acid probes (QuickFISH), and MALDI-TOF/MS, which are available for clinical use and have less than 60 min TAT, but these technologies still rely on positive blood culture as their sample input. This requirement limits them from supplanting blood culture.35 In contrast, ddPCR is a culture-independent diagnostic test and provides an absolute quantification.
The emerging antibiotic resistance among pathogens in BSI was reported recently.18,36 Treating severe infections due to multidrug-resistant bacteria is a great challenge for clinicians as the resistance pattern remains unrecognized until the identification of pathogens and the following AST reports. Thus, the early information of pathogen identification is not enough, the AST phenotype is also required in the early stage of BSIs. Research indicated that around 20% patients with BSIs in US hospitals were administered inappropriate initial antibiotic therapy, which was strongly linked to infections caused by antibiotic-resistant pathogens. Early detection of bloodstream pathogens and their resistance profiles is likely to enhance overall outcomes at a population level.37 Swift administration of the appropriate antibiotic not only enhances the likelihood of patient survival but also notably decreases hospitalization duration and related healthcare expenses.38 In our study, all enrolled patients received empirical antibiotic therapy on the date of blood sampling. For 15 patients with positive BC results, K. pneumoniae and blaKPC were detected by ddPCR in three of them, indicating the infection of CRKP. These patients were treated with carbapenem initially. According to the ddPCR result, antibiotic regimen was adjusted to ceftazidime/avibactam, which showed in vitro activity in the AST reports. Therefore, ddPCR could function as a swift and dependable approach for identifying causative pathogens and ARGs, subsequently aiding in treatment decision-making during the initial phases of BSIs. Although ddPCR could provide a swift prediction of the resistance phenotype, it should be noted that the presence of ARGs does not always correlate with phenotypic resistance, which could be a limitation of the ddPCR method.39 Due to challenges in measuring the minimum inhibitory concentration (MIC), genotypic AST assays are restricted to facilitating drug avoidance rather than guiding clinicians in selecting optimal therapeutics. Blood culture-free rapid antimicrobial susceptibility testing is needed to confirm the resistance phenotype. A phenotype-based AST platform capable of performing drug susceptibility profiling directly from the patient’s whole blood needs to be introduced during the ddPCR workflow.40,41
To cover potential pathogens, it is quite important to take into account the specific microbiological epidemiology of the local region. In our study, Enterobacter cloacae, Proteus mirabilis, Serratia marcescens, Salmonellae spp., Citrobacter, Burkholderia cepacia complex, and Morganella morganii were included in the ddPCR panels but were not detected in the blood samples in this study. A. veronii and Streptococcus sanguinis were detected in BC but were not detected by ddPCR because these two pathogens were not included in the panels. Optimizing ddPCR panel combinations needs to be considered when implementing ddPCR into the laboratory workflow to maximize cost-effectiveness.
Overall, we investigated the feasibility of ddPCR in comparison to BC. The detection rate, sensitivity, and TAT of ddPCR are superior to BC. Still, the workflow of ddPCR needs further optimization to shorten TAT, and the detection scope of the ddPCR panels should be further expanded. The positive results of ARGs and the prediction of drug resistance phenotypes require the support of AST results. This study has limitations. First, the sample size was small and the study was a single-center study, the results and conclusions may not readily translate to all hospitals. Secondly, we did not set a control group consisting of patients who only underwent blood culture. Thirdly, for multiple pathogens detected by ddPCR, we failed to interpret whether pathogens of a low DNA load are clinically relevant because of lacking more clinical evidence.
Conclusion
For patients with suspected BSI, ddPCR exhibited a superior detection rate (64% vs 30%), a relatively high sensitivity (86.67%), and less TAT (27.16 ± 13.95 hours vs 70.87 ± 15.8 hours, P < 0.0001) compared to blood culture. The clinical impact of ddPCR is to detect and quantify pathogens and ARGs while guiding therapeutic options.
Acknowledgments
This work was supported by the grants from Key Research and Development Program of Zhejiang Province (2024C03217), the National Natural Science Foundation of China (grant numbers: 82402665, 82072344, 82102476), the Department of Education of Zhejiang Province (No. Y202146202), Research Fund for Applications of High-throughput Sequencing Technology in Infectious Diseases (No.MTP2022B019). We thank all patients and the physicians from Sir Run Run Shaw Hospital for their support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hattori H, Maeda M, Nagatomo Y, et al. Epidemiology and risk factors for mortality in bloodstream infections: a single-center retrospective study in Japan. Am J Infect Control. 2018;46(12):e75–10. doi:10.1016/j.ajic.2018.06.019
2. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181–1247. doi:10.1007/s00134-021-06506-y
3. Leibovici L, Shraga I, Andreassen S. How do you choose antibiotic treatment? BMJ. 1999;318(7198):1614–1616. doi:10.1136/bmj.318.7198.1614
4. Fraser A, Paul M, Almanasreh N, et al. Benefit of appropriate empirical antibiotic treatment: thirty-day mortality and duration of hospital stay. Am J Med. 2006;119(11):970–976. doi:10.1016/j.amjmed.2006.03.034
5. Buehler SS, Madison B, Snyder SR, et al. Effectiveness of practices to increase timeliness of providing targeted therapy for inpatients with bloodstream infections: a laboratory medicine best practices systematic review and meta-analysis. Clin Microbiol Rev. 2016;29(1):59–103. doi:10.1128/CMR.00053-14
6. Giannella M, Bartoletti M, Gatti M, Viale P. Advances in the therapy of bacterial bloodstream infections. Clin Microbiol Infection. 2020;26(2):158–167. doi:10.1016/j.cmi.2019.11.001
7. Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41(2):580–637. doi:10.1097/CCM.0b013e31827e83af
8. Tabak YP, Vankeepuram L, Ye G, Jeffers K, Gupta V, Murray PR. Blood culture turnaround time in U.S. acute care hospitals and implications for laboratory process optimization. J Clin Microbiol. 2018;56(12). doi:10.1128/JCM.00500-18
9. Li H, Bai R, Zhao Z, et al. Application of droplet digital PCR to detect the pathogens of infectious diseases. Biosci Rep. 2018;38(6). doi:10.1042/BSR20181170.
10. Salipante SJ, Jerome KR. Digital PCR-an emerging technology with broad applications in microbiology. Clin Chem. 2020;66(1):117–123. doi:10.1373/clinchem.2019.304048
11. Chen B, Jiang Y, Cao X, Liu C, Zhang N, Shi D. Droplet digital PCR as an emerging tool in detecting pathogens nucleic acids in infectious diseases. Clin Chim Acta. 2021;517:156–161. doi:10.1016/j.cca.2021.02.008
12. Li Y, Huang K, Yin J, et al. Clinical evaluation of a multiplex droplet digital PCR for pathogen detection in critically ill COVID-19 patients with bloodstream infections. Infection. 2024;52(3):1027–1039. doi:10.1007/s15010-023-02157-x
13. Zheng Y, Jin J, Shao Z, et al. Development and clinical validation of a droplet digital PCR assay for detecting Acinetobacter baumannii and Klebsiella pneumoniae in patients with suspected bloodstream infections. Microbiologyopen. 2021;10(6):e1247. doi:10.1002/mbo3.1247
14. Choi YJ, Kim Y, Park HJ, et al. Development of a multiplex droplet digital PCR method for detection and monitoring of Mycobacterium tuberculosis and drug-resistant tuberculosis. Ann Clinic Microbiol Antimicrob. 2024;23(1):29. doi:10.1186/s12941-024-00687-2
15. Wang F, Sun Y, Gong L, et al. Droplet digital RT-PCR method for SARS-CoV-2 variants detection in clinical and wastewater samples. Front Microbiol. 2025;16:1635733. doi:10.3389/fmicb.2025.1635733
16. Liu Y, Tang Q, Tang S, et al. Clinical evaluation of droplet digital PCR in suspected invasive pulmonary aspergillosis. Clin Chim Acta. 2025;569:120153. doi:10.1016/j.cca.2025.120153
17. Guo J, Tian W, Lin H, et al. Analytical and clinical validation of multiplex droplet digital PCR assay for detecting pathogenic fungal infection in lungs. Mycology. 2024;15(1):110–119. doi:10.1080/21501203.2023.2296941
18. Feng Y, Wang Z, Hao Z, Du J, Jiang H. Rising drug resistance among gram-negative pathogens in bloodstream infections: a multicenter study in Ulanhot, Inner Mongolia (2017-2021). Med Sci Monit. 2023;29:e940686.
19. Hassoun-Kheir N, Guedes M, Ngo Nsoga MT, et al. A systematic review on the excess health risk of antibiotic-resistant bloodstream infections for six key pathogens in Europe. Clin Microbiol Infection. 2023;30:S14–25.
20. Papp-Wallace KM, Endimiani A, Taracila MA, Bonomo RA. Carbapenems: past, present, and future. Antimicrob Agents Chemother. 2011;55(11):4943–4960. doi:10.1128/AAC.00296-11
21. Caliskan-Aydogan O, Alocilja EC. A review of carbapenem resistance in enterobacterales and its detection techniques. Microorganisms. 2023;11(6):1491. doi:10.3390/microorganisms11061491
22. Lade H, Kim JS. Molecular determinants of beta-lactam resistance in methicillin-resistant Staphylococcus aureus (MRSA): An updated review. Antibiotics. 2023;12(9):1362. doi:10.3390/antibiotics12091362
23. Zhou W, Zhou H, Sun Y, et al. Characterization of clinical enterococci isolates, focusing on the vancomycin-resistant enterococci in a tertiary hospital in China: based on the data from 2013 to 2018. BMC Infect Dis. 2020;20(1):356. doi:10.1186/s12879-020-05078-4
24. CLSI. Performance Standards for Antimicrobial Susceptibility Testing.
25. Lamy B, Sundqvist M, Idelevich EA, Escmid Study Group for Bloodstream Infections E, Sepsis. Bloodstream infections - Standard and progress in pathogen diagnostics. Clin Microbiol Infection. 2020;26(2):142–150. doi:10.1016/j.cmi.2019.11.017
26. Wu J, Tang B, Qiu Y, et al. Clinical validation of a multiplex droplet digital PCR for diagnosing suspected bloodstream infections in ICU practice: a promising diagnostic tool. Crit Care. 2022;26(1):243. doi:10.1186/s13054-022-04116-8
27. Lin K, Zhao Y, Xu B, et al. Clinical diagnostic performance of droplet digital PCR for suspected bloodstream infections. Microbiol Spectr. 2023;11(1):e0137822. doi:10.1128/spectrum.01378-22
28. Liu W, Wang C, Pan F, et al. Clinical application of a multiplex droplet digital PCR in the rapid diagnosis of children with suspected bloodstream infections. Pathogens. 2023;12(5):719. doi:10.3390/pathogens12050719
29. Peng J, Bai H, Li Y, et al. ddPCR Enhances early diagnosis, treatment, prognosis, and pathogen verification in elderly BSI. Front Cell Infect Microbiol. 2025;15:1605795. doi:10.3389/fcimb.2025.1605795
30. Yin S, Lin Y, Wang B, et al. Reliability of droplet digital PCR alone and in combination with interleukin-6 and procalcitonin for prognosis of bloodstream infection. Infect Drug Resist. 2024;17:1051–1071. doi:10.2147/IDR.S439683
31. Long B, Gottlieb M. Emergency medicine updates: evaluation and diagnosis of sepsis and septic shock. Am J Emerg Med. 2025;90:169–178. doi:10.1016/j.ajem.2025.01.055
32. Giacobbe DR, Giani T, Bassetti M, Marchese A, Viscoli C, Rossolini GM. Rapid microbiological tests for bloodstream infections due to multidrug resistant gram-negative bacteria: therapeutic implications. Clin Microbiol Infection. 2020;26(6):713–722. doi:10.1016/j.cmi.2019.09.023
33. Li Y, Ma M, Xu X, Li Q, Ji C. Value of digital PCR in the early diagnosis of sepsis: a systematic review and meta-analysis. J Crit Care. 2022;72:154138. doi:10.1016/j.jcrc.2022.154138
34. Fidalgo B, Morata L, Cardozo C, et al. Information delay of significant bloodstream isolates and patient mortality: a retrospective analysis of 6225 adult patients with bloodstream infections. Clin Infect Dis. 2023;77(5):680–686. doi:10.1093/cid/ciad243
35. Tjandra KC, Ram-Mohan N, Abe R, et al. Diagnosis of bloodstream infections: an evolution of technologies towards accurate and rapid identification and antibiotic susceptibility testing. Antibiotics. 2022;11(4). doi:10.3390/antibiotics11040511.
36. Peri AM, Edwards F, Henden A, et al. Bloodstream infections in neutropenic and non-neutropenic patients with haematological malignancies: epidemiological trends and clinical outcomes in Queensland, Australia over the last 20 years. Clin Exp Med. 2023;23:4563–4573. doi:10.1007/s10238-023-01206-x
37. Kadri SS, Lai YL, Warner S, et al. Inappropriate empirical antibiotic therapy for bloodstream infections based on discordant in-vitro susceptibilities: a retrospective cohort analysis of prevalence, predictors, and mortality risk in US hospitals. Lancet Infect Dis. 2021;21(2):241–251. doi:10.1016/S1473-3099(20)30477-1
38. Dunbar SA, Gardner C, Das S. Diagnosis and management of bloodstream infections with rapid, multiplexed molecular assays. Front Cell Infect Microbiol. 2022;12:859935. doi:10.3389/fcimb.2022.859935
39. Nielsen TK, Browne PD, Hansen LH. Antibiotic resistance genes are differentially mobilized according to resistance mechanism. Gigascience. 2022;11:giac072.
40. Kim TH, Kang J, Jang H, et al. Blood culture-free ultra-rapid antimicrobial susceptibility testing. Nature. 2024;632(8026):893–902. doi:10.1038/s41586-024-07725-1
41. Forsyth B, Torab P, Lee JH, et al. A rapid single-cell antimicrobial susceptibility testing workflow for bloodstream infections. Biosensors. 2021;11(8). doi:10.3390/bios11080288.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.