")
Back to Journals » International Journal of Women's Health » Volume 15
Diagnostic Performance of Anti-Müllerian Hormone, Luteinizing Hormone to Follicle-Stimulating Hormone Ratio, Testosterone, and Prolactin to Predict Polycystic Ovary Syndrome Among Sudanese Women
Authors Alhassan S, Elmugadam A , Elfadil GA, Abubaker N, Elfaki EM , Hamza A , Abdalhabib EK , Karar T
Received 1 January 2023
Accepted for publication 5 May 2023
Published 29 May 2023 Volume 2023:15 Pages 837—843
DOI https://doi.org/10.2147/IJWH.S403347
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Samia Alhassan,1 Abdelgadir Elmugadam,1 Ghada A Elfadil,1 Nuha Abubaker,1 Elyasa M Elfaki,2 Alneil Hamza,2 Ezeldine K Abdalhabib,2 Tarig Karar3,4
1Department of Clinical Chemistry, College of Medical Laboratory Science, Sudan University of Science and Technology, Khartoum, Sudan; 2Department of Clinical Laboratory Sciences, College of Applied Medical Sciences, Jouf University, Al-Qurayyat, Saudi Arabia; 3Clinical Laboratory Sciences Department, College of Applied Medical Sciences, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 4King Abdullah International Medical Research Centre, Riyadh, Saudi Arabia
Correspondence: Elyasa M Elfaki, Department of Clinical Laboratory Sciences, College of Applied Medical Science, Jouf University, Omer bin Alkhattab Street, Al-Qurayyat, 77452, Saudi Arabia, Tel +966500769479, Email [email protected]
Background: Polycystic ovary syndrome (PCOS) is one of the most important contributing factors to infertility. The diagnosis of PCOS is not an easy procedure, as the signs and symptoms are heterogeneous and of undefined etiology. There are only a few published studies that address the diagnostic performance of anti-Müllerian hormone in diagnosis of PCOS in sub-Saharan Africa including Sudan.
Objective: This study aims to assess anti-Müllerian hormone (AMH), luteinizing to follicle-stimulating hormone ratio (LH: FSH), total testosterone (TT), and prolactin (PRL) levels among PCOS. In addition, we determine if AMH can be used as a predictor of PCOS among Sudanese women.
Methods: There were 600 women enrolled in this observational cross-sectional study, 300 of whom had PCOS, and 300 of whom healthy women; PCOS was diagnosed using the Rotterdam criteria. On days 2– 4 of the menstrual cycle, serum LH, FSH, AMH, TT, and PRL levels were measured for all participants. Diagnostic performance of these parameters for PCOS was determined by receiver operating characteristic (ROC) curve.
Results: Significantly higher means among PCOS regarding their BMI, AMH; LH: FSH ratio; TT; PRL, whereas significantly inverse in FSH compared with normal ovulatory women. On ROC analysis, AMH had the largest operating characteristic curve at cut-off > 3.95 ng/mL; AUC = 0.999 with Youden’s index 0.99%, followed by LH: FSH ratio at cut-off 0.749; AUC=0.932; Youden’s index 0.813%, TT cut-off 0.82 mIU/L, AUC=0.852 with Youden’s index 0.58, while PRL showed the lowest AUC=0.627 with cut-off 15.3 ng/mL, Youden’s index was 0.18%, P. value< 0.001.
Conclusions: Sudanese women with PCOS had higher serum AMH level, LH:FSH ratio, and TT level. Moreover, AMH level has better discriminative power and good diagnostic potency for the diagnosis of PCOS among Sudanese.
Keywords: PCOS women, AMH, LH:FSH ratio, TT, PRL, Sudan
Introduction
Polycystic ovary syndrome (PCOS) is a heterogeneous endocrine disorder characterized by endocrine variation, the presence of ovarian cysts, and anovulation, all of which have a significant impact on a woman’s life.1,2 Disruption of reproductive hormones such as follicle-stimulating hormone (FSH), luteinizing hormone (LH), total testosterone (TT), and estrogen disrupts the normal menstrual cycle, resulting in oligomenorrhea and amenorrhea-like irregularities. PCOS is characterized by hyperandrogenism, menstrual irregularities, and ovarian cysts of varying sizes, despite significant individual variation. This multifactorial disorder improves initially in adolescents who are at high risk of developing multiple comorbidities, such as cardiovascular disorders, type II diabetes, obesity, infertility, endometrial dysplasia, and mental disorders.3,4 The updated Rotterdam criteria, which were recently adopted by an international evidence-based PCOS guideline, are used to diagnose PCOS.5,6
AMH is also a key hormonal indication in the development and maturation of ovarian follicles in PCOS women.7 AMH overproduction inhibits follicular growth, resulting in ovarian dysfunction. Inadequate folliculogenesis is caused by an accumulation of androgens that inhibit normal androgen production. During the early gonadotropin phase, the increased androgens stimulate the primordial follicles formation and antral follicles proliferation.8 The hypothalamic GnRH secretion will stimulate the pituitary’s gonadotropin hormone secretion. LH acts on the LH receptor to stimulate the production of androgen in ovarian theca cells, while FSH stimulates the follicle growth in ovarian granulosa cells by converting androgens to estrogens.9
It has been hypothesized that neuroendocrine system dysregulation leads to hypothalamic-pituitary-ovarian axis imbalance, resulting in overproduction of gonadotropin. The GnRH increase enhances LH over FSH, resulting in a significant increase in the LH:FSH ratio in PCOS.10,11
Due to the extensive heterogeneity of PCOS’s clinical presentation, there are numerous reasons to believe that many PCOS-affected women have been misdiagnosed. In addition, the rising obesity epidemic may increase the prevalence of PCOS, as obesity may exacerbate the endocrine and metabolic profile of PCOS.12 To our knowledge, there is a limited data in Sudan that considered the diagnostic efficacy of AMH, LH:FSH ratio, LH, and PRL level in diagnostic performance and predictors of PCOS among Sudanese women.
Materials and Methods
This observational cross-sectional, hospital-based study was conducted in the state of Khartoum– Sudan, between October 2020 and September 2021. Sudan’s Ministry of Health in Khartoum approved the research protocol. This research was conducted in conformity with ethical principles of the responsible foundation and the Helsinki Declaration. Written informed consents were signed by all study participants.
In this study, there are 300 Sudanese women with PCOS as a case group compared with 300 fertile Sudanese women with non-PCOS as a control group enrolled to determine the cut-off value of common hormones (AMH, LH, LH:FSH ratio, TT, and prolactin) abnormality relevant to polycystic ovary syndrome.
Women age 20–39 years with confirmed PCOS. The European Society for Human Reproduction and Embryology (ESHRE) and the American Society of Reproductive Medicine (ASRM) have set criteria for the diagnosis of PCOS (Rotterdam 2003).7 The Rotterdam criteria include oligo-anovulation (OA) (cycles greater than 35-day intervals or 8 cycles or less per year), hyperandrogenism (HA), and polycystic ovary morphology (PCOM) (ovarian volume of 10 mL and/or an antral follicle count [AFC] of more than 12 cysts of 2–9 mm in diameter, any two being enough for the diagnosis of PCOS).6
Fertile healthy women without PCOS, who had regular menstrual cycles (21 to 35 days), without polycystic ovary morphology on ultrasonography or hirsutism, comprised the control group. The women who were taking ovulation induction agents, anti-androgenic medications, oral contraceptives, or estrogenic glucocorticoids prior to the study were excluded. Medical history of gynecological (fertility, menstrual pattern, and hirsutism) and socio-demographic characteristics were collected using a validated questionnaire, followed by comprehensive general and pelvic examinations.
The weight was measured twice in accordance with protocol standards. After calibration, OMRON BF508l Body Fat Scales (China) were utilized. Participants were instructed to take out their bulky clothing and footwear. The calculated weights were within 0.1 kg, and their height was measured twice using a portable stadiometer (SECA-213 model, Germany). The BMI of Quetelet was calculated using the conventional formula (weight in kilograms divided by height in meter2). The WHO categories were used to describe BMI; normal (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), underweight (<18.5 kg/m2), and obese from (30 kg/m2) and higher. Ultrasonography was performed using Mindray (model: DP-50, Germany) during the follicular phase, and a vaginal transducer that confirmed or ruled out the presence or absence of ovarian cysts. If cysts were observed, the volume and number of small follicles in each ovary were determined.
Women were instructed to return between 2 and 5 days after spontaneous menstruation, or on a convenient date if they had amenorrhea. Between 8:00 and 9:00 a.m., while fasting, 5 mL of the venous blood was obtained in the plain container. Blood was centrifuged using a Hettich (D-78532 Tuttlingen, Germany) centrifuge; then, serum was extracted and stored at −20 degrees Celsius until the assay. According to the manufacturer’s instructions, enzyme-linked immunosorbent assay (ELISA); ASYS (model: Expert Plus; type G020150; serial number: 28382; Austria) was used to measure the serum LH, FSH by indirect method; TT by competitive methods; PRL by direct method, and AMH by sandwich method with final fluorescent detection).
The data were coded and statistical analysis was carried out using the social package of statistical science version 26.0 (SPSS Inc., IBM, Chicago, IL, USA). For testing the normality of continuous data, the Kolmogorov–Smirnov was utilized. All data was skewed. The median with interquartile ranges were used to present continuous variables. Whereas qualitative data was expressed as a percentage (%). The relationship between PCOS and non-PCOS group was assessed by Mann–Whitney U-test and chi-square test. The predictive ability of the parameters and establishing the best cut-off values for predicting PCOS were examined using receiver operating characteristic curve analysis. The areas under the receiver operating characteristic curves (AUCs) were determined to identify the optimum parameters, and the ideal cut-off values were selected using the greatest Youden’s index (sensitivity plus specificity-1), P. value considered significant at level≤0.05.
Results
A total of 600 Sudanese adult women were enrolled. Their mean age was 28.9 (5.9) years. 300 had PCOS as a case group and 300 fertile women as a control group. Women with PCOS significantly increased in BMI compared with fertile women. Also, 76.6% (n=240) were overweight/obese based on their BMI (Table 1). Moreover, 52.3% (n=157) had menstrual cycle irregularity and 59.0% (n=177) had positive family history to PCOS (results not showed in table).
 |
Table 1 Age, Body Mass Index Among Study Group |
Furthermore, there was a significantly increased median of LH, PRL, TT, AMH, and LH:FSH ratio levels and inversed median FSH level among PCOS women compared with non-PCOS counterpart P-value <0.001 (Table 2). The ROC curves plotted for each hormone marker are shown in Figure 1. The optimum cut-off values are determined from the ROC curve analysis in Table 3. Moreover, among PCOS women most of them (n=297) had high level of AMH; 86.3% (n=259) had increased LH: FSH ratio; 71.0% (n=213) had hyperandrogenemia and 58.0% (n=174) had hyperprolactinemia based on their cut-off values Table 2.
 |
Table 2 Luteinizing Hormone, Follicle-Stimulating Hormone, Prolactin, Total Testosterone, Anti-Mullerian Hormone Among Study Group |
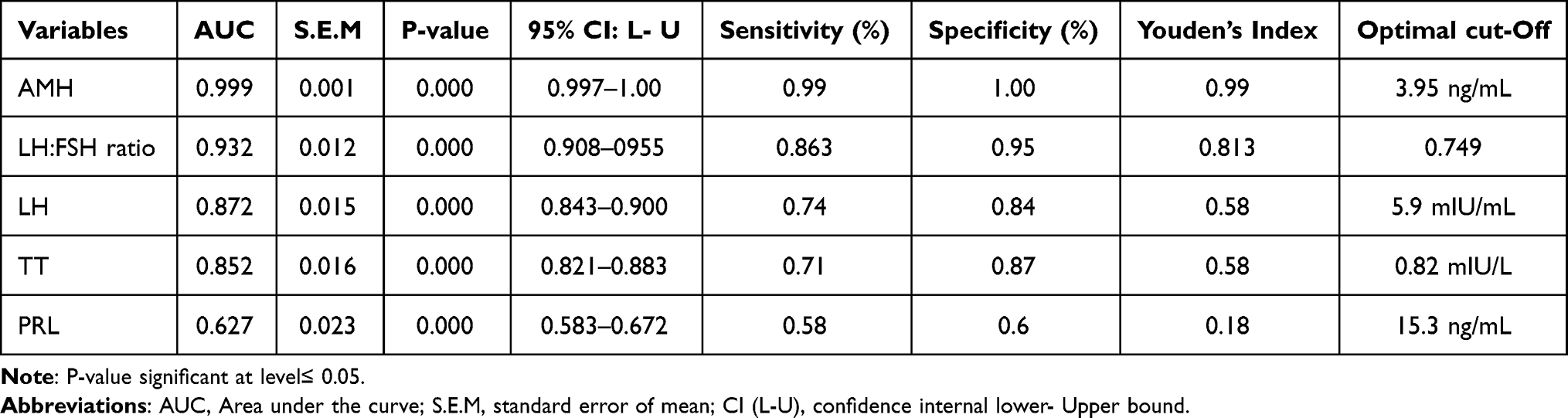 |
Table 3 Performance of Hormones Marker as Predictors of PCOS from ROC Curve Analysis in Reproductive Age Women |
 |
Figure 1 Receiver operating characteristic curve for discriminating between different hormones markers in diagnosing polycystic ovarian syndrome. *p value <0.05 is considered significant. Abbreviations: LH, luteinizing hormone; FSH, follicle stimulating hormone; AMH, anti-Mullerian hormone. |
Moreover, among Sudanese PCOS women of reproductive age, the ROC curves pointed out that AMH had a better AUC (0.999) with cut-off 3.95 ng/mL (sensitivity = 99% and specificity = 100%); followed by LH: FSH ratio AUC (0.932) with cut-off 0.749 (sensitivity = 86.3% and specificity = 95%); and prolactin had smaller AUC (0.627) with cut-off 15.3 (sensitivity = 62.7% and specificity = 60%). Furthermore, AMH and LH: FSH ratios had the highest Youden’s index (0.99%, 0.813%, respectively). Both LH and TT had the same value of Youden’s index (0.58%) Table 3.
Discussion
PCOS still does not have a clear cause, and subjective phenotypes make it hard to make a complete diagnosis. It is commonly known that PCOS is linked to insulin resistance. If this is combined with a delayed or imprecise diagnosis of PCOS, the prognosis for type 2 diabetes as well as cardiovascular disease may be worsened.13–15 Moreover, evaluating PCOM via ultrasound of abdominal area can be challenging, especially in obese or virgin women. Consequently, simpler, more precise, and more quantitative diagnostic criteria are required.
In this study, a sample of Sudanese women was assessed for serum AMH, LH:FSH ratio, TT, and PRL. In addition, we determine if AMH can be used as a predictor of PCOS whatever the patient phenotype. Our study revealed that women diagnosed with PCOS had higher BMI measurements and hormonal indicator levels, except for FSH, which was observed with insignificant differences compared with non-PCOS. The ROC curves mainly showed good specificity and sensitivity for AMH, LH:FSH ratio, LH, and TT. Serum AMH can also function within diagnostic parameters, as AMH concentration has demonstrated a significant correlation with PCOS, and reflect its severity.16,17 Additionally, it is easily measurable at any point in a woman’s cycle.18 The results of this research revealed a statistically significant difference in AMH levels between the PCOS cases and controls. Similar to the findings of previous studies, the latter showed a threefold increase in AMH relative to controls.19,20 In addition, study revealed that AMH more than 3.95 ng/mL was significantly associated with PCOS with a sensitivity of 99%; specificity 100% and Youden’s index 0.99%. Tola et al found that AMH greater than 3.1 ng/mL has diagnostic efficiency in Sudanese PCOS women (sensitivity 96%; specificity 92%).21 In Saudi population, the AMH diagnostic cut-off has been 3.19 ng/mL22 Caucasians 4.7–5 ng/mL,23 and 10 ng/mL in Japanese and Korean women.24,25 This variation in ethnicity may be associated with variable AMH levels. Moreover, the threshold of AMH can be attributed to numerous variables, including ethnicity and methodological variations.26 This may be the result of elevated androgen levels in women with PCOS disorder, leading to relative suppression of FSH production and abnormalities in the ovaries hormone. The finding of current study is consistent with the results described by Siebert et al.27 In their study, Sahmay et al they found a significant difference in the level of FSH, LH, and LH:FSH ratio of PCOS women compared to controls.28
Conclusion
In this study, AMH was found to be a useful diagnostic tool for PCOS. Future studies in various Sudanese regions should be conducted to validate the cut-off.
Data Sharing Statement
This research article includes all data generated or analyzed during this study.
Acknowledgment
We would like to express our gratitude and appreciation to everyone who helped make this study a success.
Disclosure
The authors report that there are no conflicts of interest in this work.
References
1. Escobar-Morreale HF. Polycystic ovary syndrome: definition, a etiology, diagnosis and treatment. Nat Rev Endocrinol. 2018;14(5):270. doi:10.1038/nrendo.2018.24
2. Franks S. Polycystic ovary syndrome. N Engl J Med. 1995;333(13):853–861. doi:10.1056/NEJM199509283331307
3. El Hayek S, Bitar L, Hamdar LH, Mirza FG, Daoud G. Poly cystic ovarian syndrome: an updated overview. Front Physiol. 2016;7:124. doi:10.3389/fphys.2016.00124
4. Goodarzi MO, Dumesic DA, Chazenbalk G, Azziz R. Polycystic ovary syndrome: etiology, pathogenesis and diagnosis. Nat Rev Endocrinol. 2011;7(4):219–231. doi:10.1038/nrendo.2010.217
5. Teede H, Misso M, Costello M, et al. International evidence-based guideline for the assessment and management of polycystic ovary syndrome. National Health and Medical Research Council (NHMRC); 2018:1–198.
6. Fauser BCJM, Tarlatzis F, Chang A, et al. Consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Hum Reprod. 2003;2004(19):41–47.
7. Broekmans FJ, Visser JA, Laven JS, Broer SL, Themmen AP, Fauser BC. Anti-Müllerian hormone and ovarian dysfunction. Trend Endocrinol Metabol. 2008;19(9):340–347. doi:10.1016/j.tem.2008.08.002
8. Rosenfield RL, Ehrmann DA. The pathogenesis of polycystic ovary syn- drome (PCOS): the hypothesis of PCOS as functional ovarian hyperandrogenism re- visited. Endocr Rev. 2016;37(5):467–520. doi:10.1210/er.2015-1104
9. Ashraf S, Nabi M, Rashid F, Amin S. Hyperandrogenism in polycystic ovarian syndrome and role of CYP gene variants: a review. Egypt J Med Hum Genetics. 2019;20(1):25. doi:10.1186/s43042-019-0031-4
10. Walters KA, Gilchrist RB, Ledger WL, Teede HJ, Handelsman DJ, Campbell RE. New perspectives on the pathogenesis of PCOS: neuroendocrine origins. Trend Endocrinol Metabol. 2018;29(12):841–852. doi:10.1016/j.tem.2018.08.005
11. Tsutsumi R, Webster NJ. GnRH pulsatility, the pituitary response and reproductive dysfunction. Endocr J. 2009;56(6):729–737. doi:10.1507/endocrj.K09E-185
12. Hoeger KM. Role of lifestyle modification in the management of polycystic ovary syndrome. Best Pract Res Clin Endocrinol Metab. 2006;20:293–310. doi:10.1016/j.beem.2006.03.008
13. Teede H, Hutchison S, Zoungas S, Meyer C. Insulin resistance, the metabolic syndrome, diabetes, and cardiovascular disease risk in women with PCOS. Endocrine. 2006;30:45–53. doi:10.1385/ENDO:30:1:45
14. Diamanti-Kandarakis E, Dunaif A. Insulin resistance and the polycystic ovary syndrome revisited: an update on mechanisms and implications. Endocr Rev. 2012;33:981–1030. doi:10.1210/er.2011-1034
15. Barthelmess EK, Naz RK. Polycystic ovary syndrome: current status and future perspective. Front Biosci. 2014;6:104–119.
16. Piouka A, Farmakiotis D, Katsikis I, Macut D, Gerou S, Panidis D. Anti-Mullerian hormone levels reflect severity of PCOS but are negatively influenced by obesity: relationship with increased luteinizing hormone levels. Am J Physiol Endocrinol Metab. 2009;296:E238–E243. doi:10.1152/ajpendo.90684.2008
17. Wiweko B, Maidarti M, Priangga MD, et al. Anti-mullerian hormone as a diagnostic and prognostic tool for PCOS patients. J Assist Reprod Genet. 2014;31:1311–1316. doi:10.1007/s10815-014-0300-6
18. La marca A, Stabile G, Artenisio AC, Volpe A. Serum anti-Mullerian hormone throughout the human menstrual cycle. Hum Reprod. 2006;21:3103–3107. doi:10.1093/humrep/del291
19. Sathyapalan T, Al-Qaissi A, Kilpatrick ES, Dargham SR, Atkin SL. Anti-Mullerian hormone measurement for the diagnosis of polycystic ovary syndrome. Clin Endocrinol. 2018;88:258–262. doi:10.1111/cen.13517
20. Saxena U, Ramani M, Singh P. Role of AMH as diagnostic tool for polycystic ovarian syndrome. J Obstet Gynaecol India. 2018;68:117–122. doi:10.1007/s13224-017-1066-4
21. Tola H, Abbas M, Alhassan EA, Shrif NE, Rida M. Assessment of the role of the anti-mullerian hormone, luteinizing hormone/follicle stimulating hormone ratio in the diagnosis of polycystic ovary syndrome in Sudanese women. Open Access Maced J Med Sci. 2018;6(7):1244–1247. doi:10.3889/oamjms.2018.260
22. Ahmed N, Batarfi AA, Bajouh OS, Bakhashab S. Serum anti-müllerian hormone in the diagnosis of polycystic ovary syndrome in association with clinical symptoms. Diagnostics. 2019;9:136. doi:10.3390/diagnostics9040136
23. Pigny P, Gorisse E, Ghulam A, et al. Comparative assessment of five serum anti-Müllerian hormone assays for the diagnosis of polycystic ovary syndrome. Fertil Steril. 2016;105:1063–1069. doi:10.1016/j.fertnstert.2015.12.023
24. Song DK, Oh JY, Lee H, Sung YA. Differentiation between polycystic ovary syndrome and polycystic ovarian morphology by means of an anti-Mullerian hormone cut-off value. Korean J Intern Med. 2017;32:690–698. doi:10.3904/kjim.2016.038
25. Matsuzaki T, Munkhzaya M, Iwasa T, et al. Relationship between serum anti-Mullerian hormone and clinical parameters in polycystic ovary syndrome. Endocr J. 2017;64:531–541. doi:10.1507/endocrj.EJ16-0501
26. Iliodromiti S, Kelsey TW, Anderson RA, Nelson SM. Can anti-Mullerian hormone predict the diagnosis of polycystic ovary syndrome? A systematic review and meta-analysis of extracted data. J Clin Endocrinol Metab. 2013;98:3332–3340. doi:10.1210/jc.2013-1393
27. Tal R, Seifer DB. Potential mechanisms for racial and ethnic differences in antimullerian hormone and ovarian reserve. Int J Endocrinol. 2013;2013:818912. doi:10.1155/2013/818912
28. Sahmay S, Atakul N, Aydogan B, Aydin Y, Imamoglu M, Seyisoglu H. Elevated serum levels of anti-Müllerian hormone can be introduced as a new diagnostic marker for polycystic ovary syndrome. Acta Obstet Gynecol Scand. 2013;92:1369–1374. doi:10.1111/aogs.12247
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.