Back to Journals » Journal of Pain Research » Volume 19
Diagnostic Accuracy and Reliability of the Thai Version of the Leeds Assessment of Neuropathic Symptoms and Signs Pain Scale in Adults With Chronic Pain
Authors Seangrung R ![]() , Thitirangsee R
, Thitirangsee R
Received 10 April 2026
Accepted for publication 31 May 2026
Published 20 June 2026 Volume 2026:19 616021
DOI https://doi.org/10.2147/JPR.S616021
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rodrigo Diez-Tafur
Rattaphol Seangrung,1 Rada Thitirangsee2
1Department of Anesthesiology, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, 10400, Thailand; 2Department of Anesthesiology, Vachira Phuket Hospital, Phuket, 83000, Thailand
Correspondence: Rattaphol Seangrung, Department of Anesthesiology, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, 10400, Thailand, Tel +66-2-201-1513, Email [email protected]
Background: The Leeds Assessment of Neuropathic Symptoms and Signs (LANSS) Pain Scale is a practical screening tool for identifying neuropathic pain (NP), but a validated Thai version has not been available. This study aimed to translate and cross-culturally adapt the LANSS into Thai and to evaluate its reliability and diagnostic performance in Thai adults with chronic noncancer pain.
Methods: This prospective diagnostic accuracy and psychometric validation study was conducted at a tertiary pain clinic in Thailand. Using a quota-based 2-group design, 120 adults were enrolled, including 60 patients with predominantly NP and 60 with predominantly nociceptive pain based on an independent pain specialist diagnosis as the reference standard. The index test was the Thai LANSS, which was administered by a blinded investigator. Internal consistency, inter-rater reliability, test–retest reliability, and diagnostic performance were assessed.
Results: The Thai LANSS showed acceptable internal consistency (Cronbach’s alpha = 0.725). Inter-rater reliability in a pilot phase (n = 10) was excellent (intraclass correlation coefficient [ICC] = 0.975, 95% confidence interval [CI]: 0.921– 0.994). Test–retest reliability over 2– 3 weeks (n = 30; 15 per group) was also excellent (ICC = 0.984, 95% CI: 0.941– 0.996). The Thai LANSS demonstrated good discriminatory performance, with an area under the receiver operating characteristic curve of 0.81 (95% CI: 0.75– 0.88). At the original cutoff of ≥ 12, sensitivity was 73.33% (95% CI: 62.14– 85.52) and specificity was 90.00% (95% CI: 82.40– 97.59).
Conclusion: In this tertiary pain clinic sample, the Thai LANSS showed good discriminatory performance and strong reliability and may serve as a useful screening aid for NP rather than a stand-alone diagnostic tool. Further validation in broader, more heterogeneous Thai populations is warranted.
Keywords: neuropathic pain, leeds assessment of neuropathic symptoms and signs, Thai, reliability, diagnostic accuracy
Introduction
Chronic pain, typically defined as pain lasting longer than 3 months, is clinically important because underlying pain mechanisms may influence diagnosis and treatment.1,2 According to the current International Association for the Study of Pain definition, neuropathic pain is pain caused by a lesion or disease of the somatosensory nervous system.3 In routine clinical practice, however, pain mechanisms may overlap, and patients may present with predominantly neuropathic, predominantly nociceptive, or mixed pain features.2,3
Identifying NP in clinical settings can be challenging because symptom descriptors are often imprecise and clinical presentations may overlap.1 Early recognition of NP is important because treatment strategies may differ according to the underlying pain mechanism.1,3 These challenges support the use of practical screening tools to aid structured clinical assessment, although such tools complement rather than replace comprehensive clinical assessment.
Several screening tools have been developed to help identify NP.4–8 Among them, the Leeds Assessment of Neuropathic Symptoms and Signs (LANSS) Pain Scale is practical for clinical use because it combines symptom descriptors with brief bedside sensory testing.5,9 Other commonly used instruments, such as the Douleur Neuropathique en 4 questions (DN4), are also used in routine practice, but differ in content and scoring structure.7,10,11 The LANSS was developed to distinguish pain of predominant neuropathic origin from pain of predominant nociceptive origin, and the original cutoff of ≥12 suggests that neuropathic mechanisms are likely to contribute to the pain.5,12
The original English version of the LANSS has shown good diagnostic performance and acceptable internal consistency.5 The instrument has also been translated and validated in several languages, including Turkish, Spanish, Chinese, Brazilian Portuguese, and Japanese.12–15 However, a validated Thai version has not been available. In the Thai clinical context, although a Thai version of the DN4 has been available,11 a validated Thai screening instrument that combines structured symptom descriptors with brief bedside sensory testing has been lacking. Therefore, this study aimed to translate and cross-culturally adapt the LANSS into Thai and to evaluate its reliability and diagnostic performance in Thai adults with chronic noncancer pain.
Materials and Methods
Study Design
Participants were enrolled using a quota-based two-group sampling strategy with predefined group sizes (60 with predominantly NP and 60 with predominantly nociceptive pain), as determined by an independent pain specialist diagnosis serving as the reference standard. This approach was used to ensure adequate representation of both groups for psychometric and diagnostic-performance analyses. Because this design does not reflect the natural prevalence of NP in routine practice, predictive values were interpreted cautiously. Figure 1 shows the study flow diagram.
 |
Figure 1 Study flow diagram showing translation, clinical validation, and analysis subsets of the Thai LANSS. Arrows indicate the sequence from translation and cultural adaptation to clinical validation and the analysis subsets used for diagnostic accuracy and reliability assessment. |
This was a prospective diagnostic accuracy and psychometric validation study conducted from June 2024 to March 2025 at the Pain Clinic, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand. The study comprised two phases: (1) translation and cross-cultural adaptation of the original English version of the LANSS into Thai and (2) clinical validation of the Thai version of the LANSS. The index test was the Thai LANSS, and the reference standard was an independent clinical diagnosis made by a pain specialist on the basis of clinical history, physical examination, and relevant investigations, as appropriate. The reference standard was selected because no single objective diagnostic test is available for neuropathic pain, and expert clinical assessment remains the most clinically relevant comparator in routine pain practice. A formal neuropathic pain grading system was not systematically applied. Adults with chronic noncancer pain lasting longer than three months were classified as having predominantly NP or predominantly nociceptive pain. The reference diagnosis was established before administration of the Thai LANSS. Because the reference diagnosis was established before administration of the Thai LANSS, pain specialists did not have access to the Thai LANSS score when making the reference diagnosis. The Thai LANSS was administered by an investigator who was blinded to the reference diagnosis, and standardized sensory testing followed the original LANSS protocol (allodynia using cotton wool and altered pinprick threshold using a blunt needle or paper clip). This study aimed to evaluate the reliability and diagnostic performance of the Thai LANSS, including internal consistency, inter-rater reliability, test–retest reliability, discrimination, and clinically relevant cutoff values. This study was reported in accordance with STARD 201516 (see Supplementary Information File 1).
Participants
Participants were adults aged 18 years or older who attended the pain clinic because of chronic noncancer pain lasting longer than three months. All participants were native Thai speakers, were able to complete an interviewer-administered questionnaire, and had acceptable cognitive function, defined as a Thai Cognitive Impairment Test score of 0–7. The reference diagnosis (predominantly NP vs predominantly nociceptive pain) was established independently by pain specialists after comprehensive clinical assessment, including history taking, physical examination, and radiologic or electrophysiological investigations when appropriate. Patients with mixed pain mechanisms were excluded to improve diagnostic separation between the two groups for validation analyses. Patients who declined participation or did not provide written informed consent were also excluded.
Development and Validation of the Thai Version of the LANSS Questionnaire
The LANSS Pain Scale was translated from English into Thai in accordance with established cross-cultural adaptation principles for patient-reported outcome measures.17 Two independent forward translations were performed by native Thai speakers, followed by reconciliation by an expert panel comprising pain specialists, language experts, and researchers experienced in questionnaire validation. The reconciled Thai version then underwent two independent back-translations by bilingual translators who were blinded to the original instrument. The research team and expert panel reviewed the back-translated versions against the original English version, resolved discrepancies, and finalized the Thai version to ensure semantic, conceptual, and cultural equivalence. The final Thai LANSS was approved for use in the validation phase. The Thai version of the LANSS is available from the corresponding author upon reasonable request.
Data Collection and Measurements
After written informed consent was obtained, eligibility was confirmed and baseline demographic and clinical data were recorded, including age, sex, weight, height, educational level, financial status, pain duration, comorbidities, and pain intensity at rest and during movement using the Numerical Rating Scale. Cognitive function was screened using the Thai Cognitive Impairment Test. The reference diagnosis (predominantly NP vs predominantly nociceptive pain) was determined and documented by pain specialists before administration of the Thai LANSS. The reference diagnosis and Thai LANSS assessment were performed during the same study visit, and no clinical intervention occurred between the two assessments. The Thai LANSS was then administered by a blinded investigator who was not involved in the clinical diagnosis. The investigator read each item, clarified wording when necessary, and performed standardized sensory testing for allodynia and altered pinprick threshold according to the LANSS protocol. For diagnostic-performance analyses, we prioritized evaluation at the original LANSS cutoff (≥12) to facilitate comparison with previous studies. We also explored the optimal Thai cutoff using the Youden index to inform future local validation.
Sample Size Calculation
The sample size was determined pragmatically to support both psychometric evaluation and reasonably precise estimation of diagnostic-performance measures. Guidance for questionnaire validation studies suggests that at least five participants per item may be appropriate,17 and we aimed to recruit a substantially larger sample to improve the stability of reliability estimates and cutoff-based diagnostic analyses. A total of 120 participants, with balanced representation of predominantly neuropathic and predominantly nociceptive pain, was considered sufficient for evaluating the reliability, discrimination, and clinically relevant cutoff values of the Thai LANSS in this validation study. The study was not specifically powered to achieve a prespecified confidence interval width for sensitivity or specificity estimates.
Statistical Analysis
Statistical analyses were performed using Stata version 18.0 (StataCorp, College Station, TX, USA). Continuous variables were assessed for normality and were presented as mean ± standard deviation or median and interquartile range, as appropriate. Between-group comparisons were performed using the Student’s t-test or Mann–Whitney U-test for continuous variables and the Pearson’s chi-square test or Fisher’s exact test for categorical variables. A two-sided p-value <0.05 was considered statistically significant. Baseline between-group comparisons were descriptive and were included to characterize the study sample rather than as primary inferential outcomes.
Diagnostic performance of the Thai LANSS was evaluated using receiver operating characteristic (ROC) curve analysis, and the area under the ROC curve (AUC) was calculated to assess discriminatory performance. We prioritized reporting sensitivity and specificity at the original LANSS cutoff of ≥12 to facilitate comparison with previous studies. We also explored the performance of an optimal Thai cutoff identified using the Youden index. These diagnostic accuracy measures, together with ICC and Cronbach’s alpha, were selected because they are standard and directly relevant metrics for diagnostic accuracy and psychometric validation studies. Because the study used a quota-based two-group design rather than a prevalence-based clinical sample, predictive values were interpreted cautiously.
Internal consistency was assessed using Cronbach’s alpha, with values ≥0.70 considered acceptable Inter-rater reliability for the total LANSS score was evaluated during a pilot standardization phase (n = 10) using the intraclass correlation coefficient (ICC) with 95% confidence intervals. Test–retest reliability was assessed in a subset of participants who completed a repeat assessment after 2–3 weeks (n = 30; 15 with predominantly NP and 15 with predominantly nociceptive pain), also using ICC with 95% confidence intervals. ICC values of 0.75–0.90 were considered good, and values >0.90 were considered excellent.
Ethical Approval
This study was approved by the Human Research Ethics Committee, Faculty of Medicine, Ramathibodi Hospital, Mahidol University (MURA2024/387). Written informed consent was obtained from all participants. This study was conducted in accordance with the Declaration of Helsinki.
Results
Figure 1 shows the study flow diagram for the quota-based two-group design. A total of 120 participants were enrolled, including 60 patients with predominantly NP and 60 with predominantly nociceptive pain. Baseline characteristics of the two groups are presented in Table 1. All 120 enrolled participants completed both the reference diagnosis and the Thai LANSS assessment and were included in the primary analysis; there were no missing index test or reference standard data and no indeterminate results.
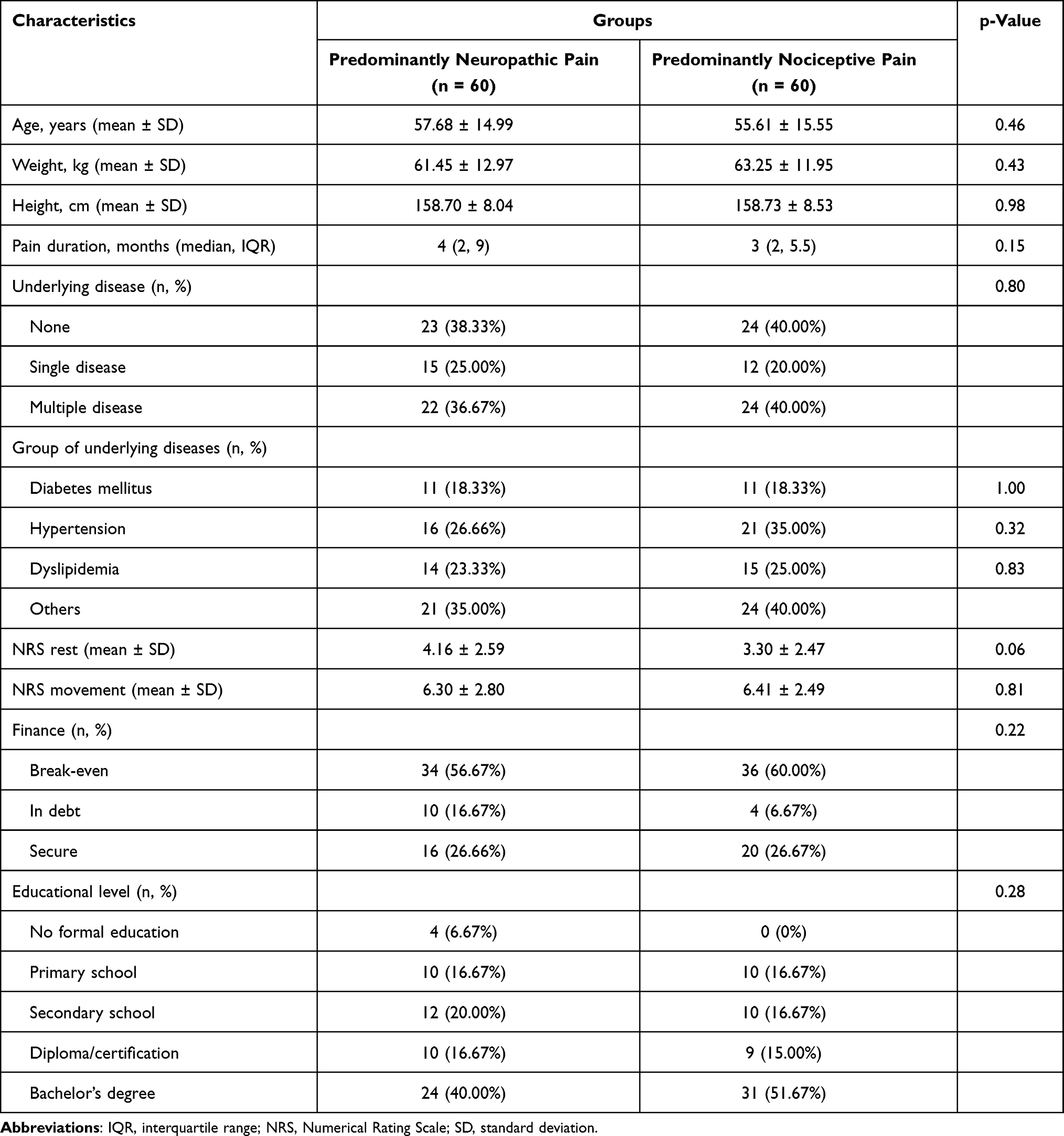 |
Table 1 Characteristics of the Participants According to Diagnostic Group |
The Thai version of the LANSS showed good discriminatory performance (Figure 2), with an AUC of 0.81 (95% CI: 0.75–0.88). At the original LANSS cutoff of ≥12, sensitivity was 73.33% (95% CI: 62.14–85.52), specificity was 90.00% (95% CI: 82.40–97.59), positive predictive value was 88.00% (95% CI: 78.99–97.01), and negative predictive value was 77.14% (95% CI: 67.31–86.98) (Table 2). Table 3 shows the cross-tabulation of Thai LANSS classification at the original cutoff against the reference standard. At this cutoff, 44 of 60 participants with predominantly neuropathic pain were classified as positive, whereas 54 of 60 participants with predominantly nociceptive pain were classified as negative. For local clinical interpretation, Supplementary Table 1 presents the classification performance of an exploratory Thai-derived cutoff identified using the Youden index (approximately ≥9).
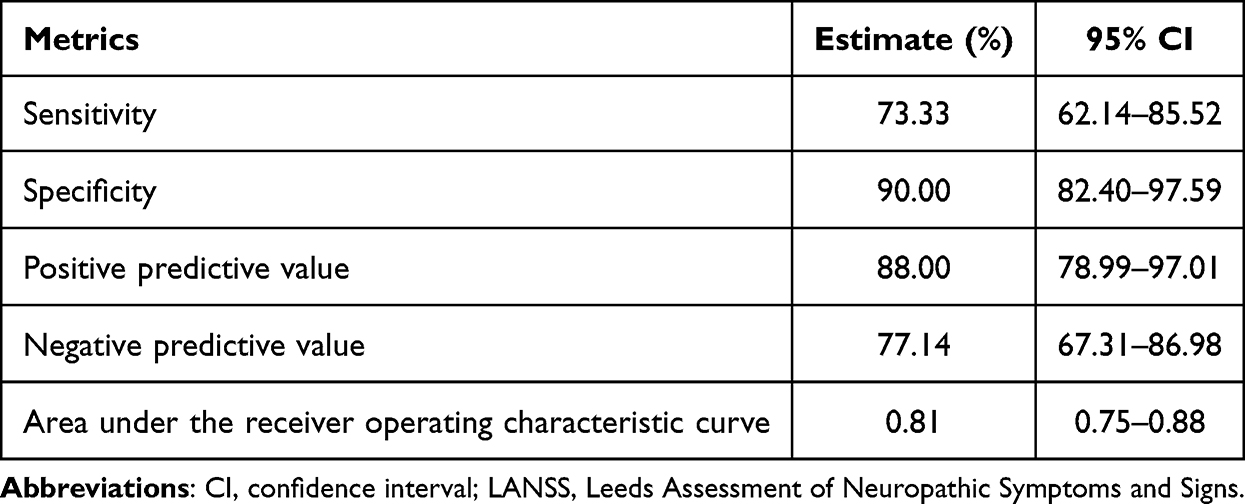 |
Table 2 Diagnostic Performance of the Thai LANSS at the Original Cutoff of ≥12 |
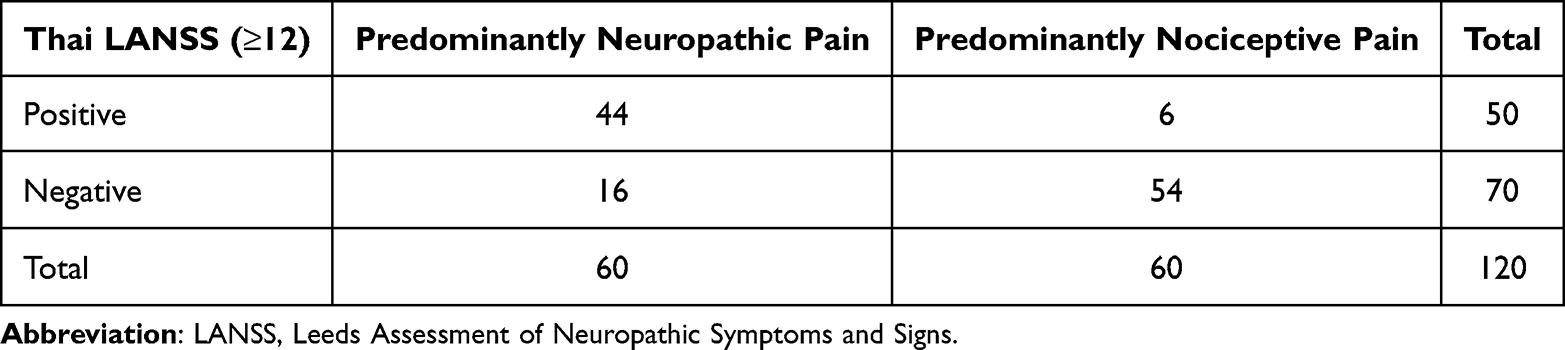 |
Table 3 Cross-Tabulation of the Thai LANSS at the Original Cutoff of ≥12 Against the Reference Standard |
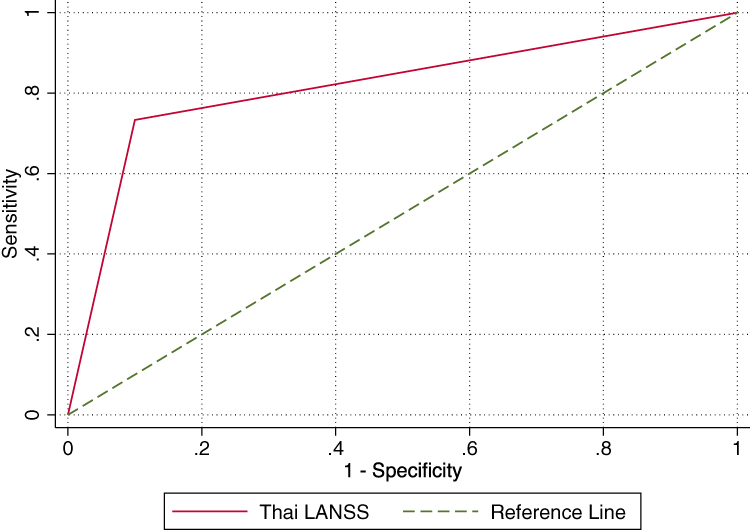 |
Figure 2 Receiver operating characteristic curve of the Thai LANSS for identifying predominantly neuropathic pain. The area under the curve was 0.81 (95% CI 0.75–0.88). At the original cutoff of ≥12, sensitivity was 73.33%, and specificity was 90.00%. Abbreviations: AUC, area under the curve; LANSS, Leeds Assessment of Neuropathic Symptoms and Signs. |
Internal consistency of the Thai LANSS was acceptable (Cronbach’s alpha = 0.725). In the pilot standardization phase (n = 10), inter-rater reliability for the total score was excellent (ICC = 0.975, 95% CI: 0.921–0.994). Test–retest reliability over 2–3 weeks (n = 30; 15 per group) was also excellent (ICC = 0.984, 95% CI: 0.941–0.996).
Discussion
This study translated, cross-culturally adapted, and validated a Thai version of the LANSS Pain Scale using a rigorous forward–backward process with expert review, supporting linguistic and cultural equivalence to the original instrument. In this tertiary pain clinic sample, the Thai LANSS showed good discriminatory performance, with an AUC of 0.81. To facilitate international comparability, we prioritized reporting performance at the original cutoff of ≥12. At this cutoff, the Thai LANSS showed a sensitivity of 73.33%, specificity of 90.00%, PPV of 88.00%, and NPV of 77.14%.
Screening tools commonly used to identify neuropathic pain in clinical practice include the LANSS and the Douleur Neuropathique en 4 questions (DN4).5,7 These instruments may support structured screening and symptom characterization, but they do not replace comprehensive clinical assessment. The LANSS combines symptom descriptors with bedside sensory testing, which may be clinically useful but also makes the instrument more dependent on standardized physical examination and therefore potentially vulnerable to inter-rater variation.5,9,10 The DN4 is generally quicker to administer, whereas the LANSS uses a more detailed scoring approach.7,9–11 Because a Thai version of the DN4 has been available, but a validated Thai version of the LANSS has not, our findings provide an additional clinically usable option for Thai healthcare providers when neuropathic pain is suspected.11
Our findings are broadly consistent with the original LANSS study and previous language adaptations, with sensitivity within the range reported across studies and specificity comparable to or higher than that reported in several translated versions.12–15,18 In addition to reporting performance at the original cutoff, we explored a Thai-derived cutoff identified using the Youden index (approximately ≥9), presented in Supplementary Table 1, to inform future local evaluation. This exploratory cutoff should be interpreted cautiously and should not be regarded as externally validated or ready for routine implementation. Differences in optimal cutoffs across studies are expected and may reflect differences in case mix, symptom profiles, comorbidities, cross-cultural interpretation of symptom descriptors, sensory testing procedures, and the reference standard used. In our study, classification was based on an independent pain specialist diagnosis in a tertiary care setting, which may differ from approaches used in previous cohorts.
The Thai LANSS also showed strong reliability. Internal consistency was acceptable (Cronbach’s alpha = 0.725), inter-rater reliability in the pilot phase was excellent (ICC = 0.975), and test–retest reliability over 2–3 weeks was also excellent (ICC = 0.984). Taken together, these findings suggest that the Thai LANSS can be administered consistently and can provide stable total scores over a clinically relevant interval. However, these reliability estimates should also be interpreted in the context of the study design, because the structured 2-group sampling strategy and diagnostic separation between groups may have contributed to apparently stronger reliability estimates than might be observed in more heterogeneous clinical populations.
Several limitations should be acknowledged. First, participants were recruited from a single university-based pain clinic, which may limit generalizability to other Thai clinical settings. Second, the reference standard was an independent clinical diagnosis made by pain specialists; although clinically relevant, this approach remains subject to diagnostic subjectivity and potential classification bias. A formal neuropathic pain grading system was not systematically applied. In addition, because the reference diagnosis and index test were performed during the same visit in a face-to-face clinical setting, patient-mediated disclosure of clinical information to the blinded investigator could not be entirely ruled out. Third, patients with mixed pain mechanisms were excluded to improve diagnostic separation between groups, but this does not fully reflect routine pain practice, where mixed pain presentations are common, and may have inflated the apparent diagnostic performance of the instrument. Fourth, because predefined group sizes were used in a quota-based two-group design, PPV and NPV should be interpreted cautiously, as they depend on disease prevalence and may differ in routine clinical settings. Fifth, although the sample size was adequate for validation, it may not have provided narrow precision for all diagnostic estimates. Finally, concurrent analgesic treatment and other potential clinical confounders were not systematically controlled and may have influenced symptom reporting or examination findings.
The Thai LANSS should be regarded as a screening aid rather than a stand-alone diagnostic tool. Future studies should validate its use in larger, more diverse multicenter Thai populations that better reflect mixed pain mechanisms and routine clinical case-mix, and compare its performance directly with other neuropathic pain screening tools, such as the DN4, in the same patients. Longitudinal studies are also needed to assess responsiveness to change and confirm performance across clinically relevant subgroups, including further external evaluation of alternative cutoff values when appropriate.
Conclusion
In this tertiary pain clinic sample, the Thai LANSS demonstrated good discriminatory performance and strong reliability. Reporting performance at the original cutoff facilitates comparison with previous studies, whereas the Thai-derived cutoff should be regarded as exploratory and may inform future local validation rather than immediate clinical implementation. Given the single-center, quota-based design, the Thai LANSS may be useful as a structured screening aid for neuropathic pain, but further validation in broader and more heterogeneous Thai populations is needed.
Abbreviations
AUC, area under the receiver operating characteristic curve; CI, confidence interval; DN4, Douleur Neuropathique en 4 questions; ICC, intraclass correlation coefficient; IQR, interquartile range; LANSS, Leeds Assessment of Neuropathic Symptoms and Signs; NP, neuropathic pain; NPV, negative predictive value; NRS, Numerical Rating Scale; PPV, positive predictive value; ROC, receiver operating characteristic; SD, standard deviation; STARD, Standards for Reporting Diagnostic Accuracy Studies.
Data Sharing Statement
The datasets generated and/or analyzed during the current study, as well as the Thai version of the LANSS, are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The current study was approved by the Human Research Ethics Committee, Faculty of Medicine, Ramathibodi Hospital, Mahidol University (MURA2024/387). A written informed consent was obtained from all participants. The study was conducted in accordance with the Declaration of Helsinki.
Consent for Publication
All participants provided consent for the publication of anonymized data.
Acknowledgments
We would like to thank the pain medicine physicians for their support and assistance throughout the research process. The authors also acknowledge Mr. Witthawin Saelee for his valuable assistance with the sample size calculation, statistical analysis, and data management.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Ramathibodi Research Grant, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand. The funders had no role in the study design, data collection, analysis, interpretation, manuscript preparation, or the decision to publish.
Disclosure
The authors declare no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
References
1. Schestatsky P, Nascimento OJM. What general neurologists need to know about neuropathic pain? Arq Neuropsiquiatr. 2009;67:741–10. doi:10.1590/s0004-282x2009000400039
2. Treede R-D, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain. 2019;160:19–27. doi:10.1097/j.pain.0000000000001384
3. Treede R-D, Jensen TS, Campbell JN, et al. Neuropathic pain: redefinition and a grading system for clinical and research purposes. Neurology. 2008;70:1630–1635. doi:10.1212/01.wnl.0000282763.29778.59
4. Backonja -M-M, Krause SJ. Neuropathic pain questionnaire-short form. Clin J Pain. 2003;19(5):315–316. doi:10.1097/00002508-200309000-00005
5. Bennett M. The LANSS Pain Scale: the Leeds assessment of neuropathic symptoms and signs. Pain. 2001;92(1):147–157. doi:10.1016/s0304-3959(00)00482-6
6. Bouhassira D, Attal N, Fermanian J, et al. Development and validation of the neuropathic pain symptoms inventory. Pain. 2004;108:248–257. doi:10.1016/j.pain.2003.12.024
7. Bouhassira D, Attal N, Alchaar H, et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain. 2005;114(1):29–36. doi:10.1016/j.pain.2004.12.010
8. Galer BS, Jensen MP. Development and preliminary validation of a pain measure specific to neuropathic pain: the neuropathic pain scale. Neurology. 1997;48(2):332–338. doi:10.1212/wnl.48.2.332
9. Bennett MI, Smith BH, Torrance N, Lee AJ. Can pain be more or less neuropathic? Comparison of symptom assessment tools with ratings of certainty by clinicians. Pain. 2006;122(3):289–294. doi:10.1016/j.pain.2006.02.002
10. Cruccu G, Truini A. Tools for assessing neuropathic pain. PLoS Med. 2009;6(4):e1000045. doi:10.1371/journal.pmed.1000045
11. Chaudakshetrin P, Prateepavanich P, Chira-Adisai W, Tassanawipas W, Leechavengvongs S, Kitisomprayoonkul W. Cross-cultural adaptation to the Thai language of the neuropathic pain diagnostic questionnaire (DN4). J Med Assoc Thai. 2007;90(9):1860–1865.
12. Isomura T, Sumitani M, Matsudaira K, et al. Development of the Japanese Version of the Leeds Assessment of the Neuropathic Symptoms and Signs Pain Scale: diagnostic utility in a clinical setting. Pain Pract. 2017;17(6):800–807. doi:10.1111/papr.12528
13. Yucel A, Senocak M, Kocasoy Orhan E, Cimen A, Ertas M. Results of the leeds assessment of neuropathic symptoms and signs pain scale in Turkey: a validation study. J Pain. 2004;5(8):427–432. doi:10.1016/j.jpain.2004.07.001
14. Batistaki C, Lyrakos G, Drachtidi K, Stamatiou G, Kitsou M-C, Kostopanagiotou G. Translation, cultural adaptation, and validation of Leeds assessment of neuropathic symptoms and signs (LANSS) and self-complete Leeds assessment of neuropathic symptoms and signs (S-LANSS) questionnaires into the Greek language. Pain Pract. 2016;16(5):552–564. doi:10.1111/papr.12300
15. Spanos K, Lachanas VA, Chan P, Bargiota A, Giannoukas AD. Validation of the Leeds Assessment of Neuropathic Symptoms and Signs (LANSS) questionnaire and its correlation with visual analog pain scales in the Greek population. J Diabetes Complications. 2015;29(8):1142–1145. doi:10.1016/j.jdiacomp.2015.08.008
16. Bossuyt PM, Reitsma JB, Bruns DE, et al. STARD 2015: an updated list of essential items for reporting diagnostic accuracy studies. BMJ. 2015;351:h5527. doi:10.1136/bmj.h5527
17. Tsang S, Royse CF, Terkawi AS. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J Anaesth. 2017;11(5):S80–S89. doi:10.4103/sja.sja_203_17
18. Schestatsky P, Félix-Torres V, Fagundes Chaves ML, et al. Brazilian Portuguese validation of the Leeds assessment of neuropathic symptoms and signs for patients with chronic pain. Pain Med. 2011;12(10):1544–1550. doi:10.1111/j.1526-4637.2011.01221.x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.