")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Diagnosis of Epilepsy by Traditional Healers and Its Implications on Management in the Selected Rural Communities of Limpopo and Mpumalanga Provinces: A Qualitative Study
Authors Nemathaga M , Maputle MS , Makhado L , Mashau NS
Received 6 October 2022
Accepted for publication 5 January 2023
Published 18 April 2023 Volume 2023:19 Pages 973—983
DOI https://doi.org/10.2147/NDT.S392479
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Muofheni Nemathaga,1 Maria S Maputle,1 Lufuno Makhado,2 Ntsieni Stella Mashau2
1Department of Advanced Nursing, University of Venda, Thohoyandou, South Africa; 2Department of Public Health, University of Venda, Thohoyandou, South Africa
Correspondence: Maria S Maputle, Email [email protected]
Introduction: Epilepsy is a neurological disorder which causes seizures and may be accompanied by loss of unconsciousness and control of bowel or bladder function. However, other types of epilepsy are only characterised by rapid blinking or a few seconds of staring into space. Many people living with epilepsy in rural communities consult traditional healers as their first line of treatment for epilepsy. Second preference is given to medical practitioners which causes unnecessary delay in the early diagnosis and treatment of epilepsy. This study aimed to explore how traditional healers diagnose epilepsy and its implications on management in the selected rural communities of Limpopo and Mpumalanga Provinces.
Methods: A qualitative approach using explorative, descriptive and contextual designs was adopted. Purposive sampling was used to sample six villages in Limpopo and Mpumalanga Provinces. Snowball sampling was used to sample twenty traditional healers. Data were collected through in-depth individual interviews at the participant’s homes. Data were analysed using Tesch’s eight steps of open coding data analysis.
Results: This study found that traditional healers have varied beliefs and misconceptions regarding the causes and diagnosis of epilepsy, hence this greatly influencing the management. The misconceptions on the causes include a calling by ancestors, urine contents, snake in the stomach, contaminated digestive system and witchcraft. The management included using herbal plants, insects, foam excreted during seizures and urine of the person living with epilepsy.
Recommendation: It is recommended that for effective management of epilepsy, there should be coordination between traditional healing and western medicine. Future research should look at the integration of traditional medicine and western medicine.
Keywords: epilepsy, diagnosis, management, implications
Introduction
Epilepsy is a chronic non-communicable neurological disorder that affects individuals of all ages.1,2 Approximately 50 million people globally live with epilepsy, making it one of the most common neurological diseases worldwide.3 In Sub-Saharan Africa, roughly 10 million people are living with epilepsy, and there is a considerable treatment gap among people living with epilepsy (PLWE) who are not receiving the required antiepileptic drugs (AEDs). Nearly 80% of people living with Epilepsy live in low- and middle-income countries.4 In India, it is estimated that there are more than 10 million PLWE and the treatment gap is over 75% in most low-income areas.5 Approximately one-third of PLWE seek traditional healing before seeking medical treatment. Even when medical care can be accessible, PWLE often concurrently or first seek care from traditional healers.5 These healers include herbalists who use medicinal plants in their treatments. In traditional Indian medicine, Ziziphus jujube (Red date or Chinese date) is one of the plants used as an anticonvulsant.6 A study conducted in Northern Peru revealed that all traditional healers stated that they were aware epilepsy and they all used convulsions to diagnose it.7 Additional symptoms such as inflammation, heartburn, “cardiac paralysis”, stomach problems, and salivation were described by traditional healers.7
In sub-Saharan Africa, the biological (organic) nature of epilepsy is acknowledged, but it is also believed to have supernatural causes, including demonic possession, witchcraft, ancestor calling, and divine punishment. Thus, the diagnosis is made through spiritual methods.8 The majority of traditional healers indicated that ultimately, ancestor spirits will direct the diagnosis and treatment regimen.8 In Namibia, Traditional healers cited that they are guided by supernatural influences while determining the origin of a client’s sickness. To make a diagnosis, the directions from divination are put together with the client’s knowledge on other ailments, family history, and an explanation of the seizures.9
In South Africa, epilepsy is believed to be caused by evil spirit, demonic possessions, ancestral spirits and witchcraft.10 The symptoms that were most frequently observed for a diagnosis included jerking of the body, twisting of the eyes, frothing at the mouth, stiffening of the fingers, passing out, and losing consciousness.10 In addition, diagnosis was made through history taking from the clients or family members. However, the treatment for epilepsy varies according to the identified causes.
In China, numerous herbal medicines, such as Ginkgo biloba (Maiden hair tree) and Huperzia Serrata (firmoss), are commonly used to treat epilepsy.11,12 In Kilifi, Kenya, and Bobo-Dioulasso, Burkina Faso, traditional therapeutic treatments for epilepsy are popular.13 For a first seizure, a nail is swiftly located and hammered into the spot where the person’s skull was initially touched during the seizure, with the healer exclaiming, “It shall stay here!” The person then grasps the trunk of a young tree. While chanting, a healer slashes the neck of a hen, and the hen’s blood is rubbed on the individual’s upper body.13 Unless the tree dies or the person eats any chicken flesh, the epilepsy is considered cured. In addition, the healer chants while a pillow is packed with hay. Afterward, the pillow is boiled, and its water is sprayed on the individual, and lastly the pillow thrown into the river.13 Following that, the healer cuts a nail from the individual, scarifies the back of the neck, and injects a small amount of his own blood into the individual; the nail is then crushed and mixed with candle wax at sunset, and the healer dresses the individual in “enchanted” clothing, and the individual lies in a doorway with his head outside facing the sun.13 Due to supernatural beliefs linked with epilepsy and the assumption that traditional healers can give a cure for the spiritual cause of epilepsy rather than medication to manage seizures, the majority of PLWE in Sub-Saharan Africa (SSA) typically consult traditional healers first.3,10 Most PLWE in Guinea seek traditional healing from traditional healers, and they receive traditional remedies for an average of more than three years before obtaining medical help and starting AEDs.14 Garlic, oranges, whiskey, or a grain paste pasted into the PLWE’s nose or mouth are some of the traditional healer’s techniques.14
According to a study done in Mali, traditional healing in Africa involves many therapeutic techniques, including plants, spirits, and magic formulas.15 Traditional healers in Mali use medicinal herbs that have anticonvulsant effects. In contrast, others, such as bush tea, are used in treating epilepsy by traditional healers, but it can cause severe complications such as worsening seizures in children.15 Herbal baths and contextual references, such as the burning of animal dung, blowing air, interacting with spirits and portraits, providing animal sacrifices, and wearing protective amulets, were also used as exorcizing cures.15
In South Africa, many consider PLWE to be possessed, and the condition is often viewed as a punishment for family’s wrongdoings or ancestral calling.16,17 Epilepsy is frequently treated with traditional remedies. Most PLWE eventually turn to traditional healers for help because they believe Epilepsy must be treated with traditional medicine.16,17 These ideas significantly impact PLWE’s treatment decisions and are extremely influential. If the seizures are thought to be caused by witchcraft or possession by bad spirits, the treatment must be more spiritual, and it cannot be given in a hospital. In South Africa, most PLWE seek care from traditional healers initially, with medical practitioners receiving second priority at a later stage, resulting in unnecessary delays in epilepsy diagnosis and treatment. The Traditional Health Practitioners Act (Act No 22, 2007) demonstrates that 80% of all South Africans consult traditional healers before seeking medical assistance from Western doctors; traditional healers’ holistic treatment methods are generally favoured over Western medicine. Thus, this study aims to explore the diagnosis of epilepsy by traditional healers and its implication on treatment.
Methods
This study was conducted in the rural communities of Limpopo and Mpumalanga Provinces of South Africa. The selected rural communities in Limpopo, included Malavuwe, Mtititi, and Bochum, while for Mpumalanga included Clara, Acornhoek, and Jerusalem. The community members have diverse cultures with various beliefs and practices. These communities were selected based on the cultural beliefs, practices and the management of epilepsy.
A qualitative approach using explorative, descriptive and contextual designs was used to achieve the objectives of this study.18,19 The researcher personally engaged with the participants to obtain in-depth data. Inclusion criteria: 1. traditional healers who manage epilepsy in the selected rural communities of Limpopo and Mpumalanga Provinces 2. willing to participate and gave consent. Pre-test was done prior the actual data collection. The selected participants were interviewed to check whether the question was phrased in a manner that they understood. The participants who were interviewed for the pre-test were not part of the study. The duration of the pre-test was 20 to 40 minutes. Purposive sampling was used to sample the villages based on cultural diversity.20 Snowball sampling was used to select traditional healers. The sample size comprised 20 traditional healers. The study’s sample size was determined based on data saturation during data analysis.
Measures to Ensure Trustworthiness
Trustworthiness was ensured using the criteria of credibility, transferability, dependability and confirmability.20 Credibility was ensured through prolonged engagement, persistent observation and member checking to ensure transferability, biographical information was obtained; a dense description of the research methodology and the findings were provided. Furthermore, transferability was ensured by densely describing the background information of participants.18,19 To address the dependability issue more directly, the processes of this study were reported in detail to allow future researchers to repeat the work, if not necessarily to gain the same results.18,19 In-depth methodological description was done to allow the integrity of research findings to be scrutinized.
Data Collection
Data were collected through in-depth individual interviews at the participants’ homes. The duration of the interviews was 30 to 45 minutes. The interviews were conducted in local languages; Sepedi, Xitsonga and Tshivenda. A voice recorder to capture data was used after obtaining consent from participants. The interviews were guided by the following central question: “Kindly share with me how you diagnose and manage clients presenting with epilepsy at your practice?”
Probing questions were asked, which emanated from the participants’ answers, to allow them to give more clarity. Skills such as listening, clarifying, reflecting, focusing, and paraphrasing were used to obtain more information from the participants. Minimal verbal responses by nodding the head, saying “mm”, “Yes”, and “continue” allowed a free flow of information and encouraged participants to talk. This made participants feel more relaxed and more willing to discuss their management.
Data Analysis
This study adopted the open coding data analysis guide developed by Tesch’s to analyse data following Creswell.19 The researchers listened to the tape and transcribed it verbatim. Thereafter, researchers read through one transcript at a time to acquire a good picture of what participants said. Similar categories were scribbled and grouped together. Sub-themes formed, which were then grouped into columns. Following that, a list of themes was created for each topic. Columns were formed by grouping similar themes together. To make the process easier, several coloured pens were employed. The researchers then abbreviated the subjects as codes and wrote them next to the relevant segments. To present the results of the analysis, the researcher used tables. The tables were organized according to the researcher’s theme, categories, and subcategories.
Ethical Considerations
The study comprised human subjects as participants and therefore the researcher adhered to the Declaration of Helsinki. Ethical clearance was obtained from the University of Venda Human and Clinical Trial Research Ethics Committee (SHS/20/PDC/49/1301) to ensure ethical adherence. Permission to access the villages from the Traditional Councils and participants. The ethical considerations of this study included the principle of respect for persons, informed consent, privacy, confidentiality, and anonymity.18,19
Results
Demographic Profile
Table one illustrates the demographic profile of the participants. Table 1. The population comprised 20 participants and included males (n=9) and females (n=11). The age of participants ranged between 35 and 62 years. Most participants (n=11) were from Limpopo, and the rest (n=9) were from Mpumalanga Province. All male participants (n=9) were married and trained for traditional healing. Only a few females were married and qualified (n=4). The remaining female participants (n=7) were not married. Tshivenda was the most common language spoken, followed by Xitsonga and Sepedi. The qualified traditional healer in this study refers to those who went to initiation school for training, passed the test and licensed to practice alone without supervision.
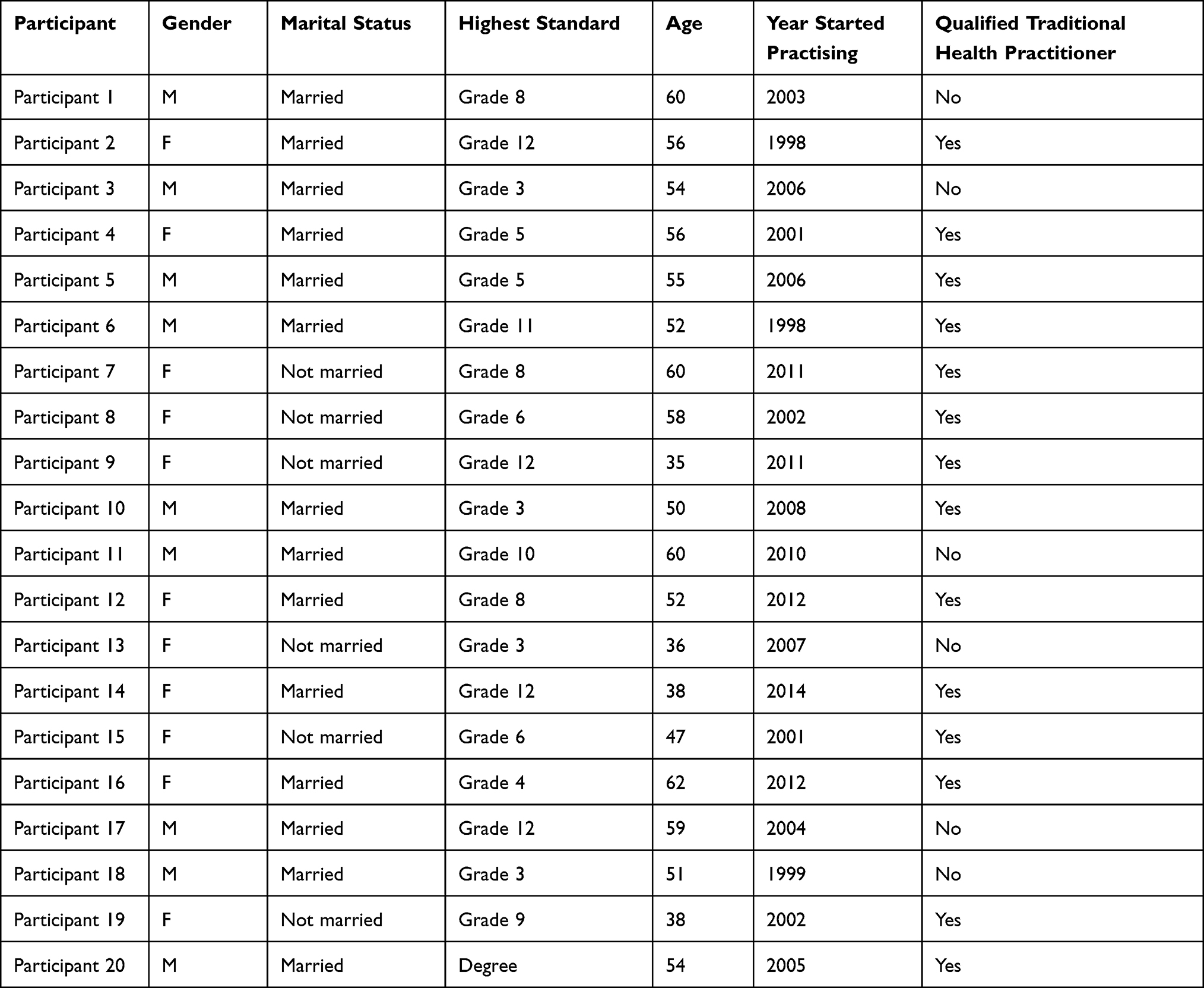 |
Table 1 Demographic Profile |
Most participants who had completed matriculation were females and therefore certified to practice traditional healing. Female participants are mostly between the ages of 30 and 38. However, they have less experienced than male participants. Most males began traditional healing after “mbidzo” (calling by ancestors), and because most lack matric, they have more years of experience. Male participants were between the ages of 40 and 60. Unlike the female participants, all the male participants were married.
Three themes emerged from the findings, namely beliefs on causes of Epilepsy, diagnosis of Epilepsy and management of Epilepsy as discussed herein:
Theme 1: Beliefs on Causes of Epilepsy
Epilepsy is a condition that is associated with misconceptions and various beliefs. This study revealed that ten (10) traditional healers believe that epilepsy is caused by witchcraft. While three (3) traditional healers believed that epilepsy is caused the presence of snake/s in the stomach. Five (5) of them believed that it is caused by heredity and the two (2) healers believed that epilepsy is caused by contents in urine and that epilepsy is contagious. The following quotes supported the findings:
A male participant number 1 aged 60 years from Mpumalanga verbalized,
Many things can cause epilepsy, firstly you don’t sit on “ecansini” (Reed mat) of a person with Epilepsy because it’s contagious, you don’t eat food that was left by the epileptic patient.
Another female participant number 4 aged 56 from Limpopo reported,
I mean that all the waste in the body forms “mutambuluwo” (urine) causes Epilepsy. That is why we use urine to cure epilepsy. The illness is caused by the “mutambuluwo” (urine). The illness starts from the body and then travels to the brain.
One male participant number 20 aged 54 from Limpopo verbalized,
That illness can just develop from nowhere, but for most people, it’s generational, some it isn’t generational but just the illness itself. Some families have Epilepsy, with those ones; even if we run and do this and that, you can’t heal them.
A female participant number 9 aged 35 years from Mpumalanga cited,
Epilepsy is caused by contamination in the digestive system and sometimes it can be caused by witchcraft because some people are so evil. As a traditional healer I mix herbs to produce a traditional enema to cleanse the client.
Theme 2: Diagnosis of Epilepsy
Findings of this study indicate that most traditional healers diagnose Epilepsy in different ways, including diagnosis through observation of epileptic seizures, diagnosis using bones and diagnosis by history taking. Eight (8) traditional healers indicated that the diagnose epilepsy is based on information provided by relatives. Four (4) traditional healers reported they use “tinhlolo” (bones) to diagnose epilepsy, as discussed herein:
Most traditional healers fourteen (14) observed clients having seizures and made a diagnosis based on those observations. Emphasis was further made on what happens during the seizures. One female participant number 2 aged 56 from Mpumalanga verbalized:
The patient falls and has involuntary movements, then from there, the patient will be confused, not knowing what is happening. “The brain is totally disturbed; these illnesses totally disturb the brain.
The same participant added:
If there is no one nearby during seizures, the patient will bite the tongue and the mouth. If you want to be sure that it is Epilepsy, the patient wets him or herself during seizures then from there the patient will be confused, unaware of what is happening.
A male participant number 3 aged 54 from Mpumalanga verbalized,
If a person is living with Epilepsy you see her fall every month, some fall twice, biting teeth, and releasing foam that’s when we say this person has epilepsy.
A female participant number 12 aged 52 from Limpopo cited,
It takes roughly 5 minutes while the client is busy making jerky movements. After that the patient losses energy, he or she becomes tired because this patient was fighting a battle.
This concludes that traditional healers also diagnose epilepsy through observation of epileptic seizures accompanied by other symptoms such as unconsciousness, although beliefs on the causes are different.
Findings also indicate that few traditional healers use “tinhlolo” (bones) to diagnose epilepsy. The bones verify that indeed the client has epilepsy as the ancestors communicate with the healer for confirmation. This was elaborated on the following quote:
A male participant number 06 aged 52 verbalized:
I first look in “tinhlolo” (bones) because we work using them. When I look there I ask if really the person that has come to me has epilepsy because it may be assumed that its epilepsy while it isn’t” then, “tinhlolo” would show me that indeed its epilepsy.
The findings of this study further show that some traditional healers observed seizures from their own family members who were living with epilepsy. Traditional healers also diagnose epilepsy through information provided by relatives or clients during history taking. The following quotes supported this:
A female participant number 8 aged 58 years from Limpopo verbalized,
Sometimes, we diagnose based on the information provided by the relatives during consultation. I then ask the relatives about the frequency and severity of the seizures so that I can be sure that its ‘vhulwadze ha u wa’. (epilepsy)
A female participant number 4 aged 56 years from Limpopo cited,
The person who accompanies the patient explains how the patient falls and everything that happens when the patient falls, like passing flatus, urine or feaces. The patient can also be confused for a moment.
History taking is also significant for traditional healers as it assists them in obtaining important information regarding the person living with epilepsy.
Theme 3: Management of Epilepsy
Management of Epilepsy varies according to traditional healers and treatment depends on the cause. The management includes the use of traditional herbs, foam released during seizures, urine and insect as discussed below:
The findings of this study revealed that traditional healers use traditional herbs described as mixtures of different trees to manage epilepsy. The herbs are burnt then the client inhales through steaming. Some traditional healers use nails, underarm and pubic hair from the PLWE. The nails and hair are then burned, mixed with herbs, and the PLWE inhaled for a cure. The steam from burnt herbs is believed to cure Epilepsy. This was elaborated on the following quotes:
A female participant number 8 aged 58 from Limpopo verbalized,
We make fire until it produces a lot of ashes, then we take a piece of ‘tshidongo’ (broken clay pot) and put those ashes together with the herbs. After that, the patient is covered with a mini blanket for steaming.
A female participant number 9 aged 35 from Mpumalanga verbalized:
I give them herbs that I get from the river, I take the roots of ‘RINKA (traditional herb)’, which I grind and soak in water. I grind this medicine, and if it’s a small child, I mix it with Danone (Yoghurt); for infants, I mix it with soft porridge, and for adults, I give the one teaspoon three times a day.
A male participant aged 50 years from Limpopo reported:
There are those who come having a seizure. We start by mixing our herbal medicine in a clay pot for the client to inhale, so if the client comes without an attack, we prepare medicine for them to drink at home.
A male participant number 11 aged 60 from Mpumalanga explained,
I have one tree next to the sand you see with a show of hand is the one that tires the disease, the other is the one they cut off over there, and the third one is next to the gate. They are three, but you mix them not that they work alone.
A female participant number 8 aged 58 verbalized,
At home, we have this condition (Epilepsy) in almost all our households. My child was diagnosed by an old lady who gave her the traditional medication to drink. When the old lady died, I started using this medication on others, and it helped. I’ve since graduated as a traditional healer.
A female participant number 7 aged 61 from Limpopo explained,
My child had a seizure when he was four now, he is 22 years. I went to church and the clinic it did not help. My friend told me that her husband was helped by traditional herbs from Tzaneen, which he started to use. I also went to Tzaneen and started harvesting this medicine.
According to the findings, the management of epilepsy also includes the use of insect and urine whereby insects are crushed and burnt then livestock is used as a medium to transfer the illness. The management of epilepsy varies according to traditional healers. Some healers are trained to use fly (“gonono”), which is burnt and crushed. Ancestors provide this kind of training in visions while the traditional healer is sleeping.
A female participant number 4 aged 56 from Limpopo province elaborated:
Meaning if the traditional healer uses gonono for treatment, he or she will cut the client with a razor and apply the crushed gonono mixed with herbs on the open area of the skin. If the patient has seizures like gonono, we conclude that it was inserted in his body.
The fly is perceived to have epileptic seizures because it lies on its back and makes jerky movements hence used for the treatment of Epilepsy. However, some traditional healers use the fly “gonono” for steaming only. They do not cut or apply anything on the patient. This as elaborated on the following quote:
Epilepsy is treated using gonono. It is found at the bushes, usually where there is cow dung and it is so scarce. If a patient consults for treatment of epilepsy, I take the gonono, mix it with traditional herbs in a piece of broken clay pot. Thereafter the patient steams, covered with a blanket. I add more firewood to increase the heat. Once the patient sneeze, epilepsy is cured.
The findings of this study further indicate that some traditional healers believe that epilepsy is caused by urine; hence urine is used in combination with water and blood to treat epilepsy. The following quote supported this:
A female participant aged 56 from Limpopo verbalized:
We then make a small cut on the chicken then apply the client’s blood. We also use his or her urine and mix it with water. The urine contains epilepsy, so we mix herbs and use a razor to make small cuts on the chicken, and the client then applies to the open cuts.
Traditional healers believe that epilepsy can be transferred from PLWE to a chicken, and after that, the PLWE will be cured. However, PLWE do acknowledge the western treatment of epilepsy though it is given second preference. In case of traditional treatment failure, PLWE are referred to the hospital by traditional healers for further management.
Discussion
Beliefs on Causes of Epilepsy
The findings of this study revealed that there are various perceived causes of epilepsy by traditional healers in Limpopo and Mpumalanga Provinces. The causes include witchcraft, snake in the stomach, curse, heredity, contents in urine and epilepsy is contagious. These findings are like those of a study conducted in Guinea, which indicates that epilepsy is perceived as contagious and can be spread by feaces, saliva, urine or flatus, often excreted during a seizure.21
Furthermore, it is perceived that epilepsy may be caused by witchcraft, curse in the family by gods, punishment of wrongdoers and ancestral calling. Epilepsy can also be acquired from spiritualists. In addition, other perceived causes of epilepsy include supernatural powers, black magic, birds, and punishment by God.21
Similarly, a study conducted in Nigeria revealed that epilepsy is believed to be contagious through saliva, urine, and sexual intercourse as the major route of infection. However, a significant percentage also believed that epilepsy could be contracted by watching or observing epileptic attacks.22,23
In addition, epilepsy is widely perceived in SSA as a mystical condition caused by supernatural forces or witchcraft, with many people believing that demons or evil spirits possess those who suffer from it. These findings of widespread spiritual and supernatural beliefs align with other SSA investigations that show strong belief in these forces as the cause of seizures.24,25 Contrary to the above findings, Wagner26 shows that epilepsy is caused by structural, genetic, infectious, metabolic, immunological, and unknown reasons, which include brain damage caused by prenatal or perinatal causes, congenital abnormalities, or hereditary diseases with accompanying brain deformities. A severe head injury: a stroke that reduces oxygen to the brain; a brain infection like meningitis, encephalitis, or neurocysticercosis; some genetic diseases; and a brain tumour.
Similarly, a study conducted by Idculla27 found that epilepsy is caused by excessive bioelectric discharge in the brain cell. Other causes include prenatal brain injuries, vascular malformations, cerebral abnormalities, and atrioventricular malformation. In addition, according to Watila,28 excessive alcohol consumption, recreational drug use, traumatic brain injury, and meningitis are all variables that may lead to the development of epilepsy. Furthermore, in older persons, brain tumours were a more common cause of Epilepsy than in younger ones.
Other explanations are based on cultural ideas and perceptions, whereas other causes are based on scientific information. These widely held beliefs and perceptions significantly impact the management or treatment of choice, demonstrating a significant gap in knowledge about the medical causes of epilepsy. Because the preferred management is entirely based on one’s perception, the considered causes of epilepsy have a significant impact on its management.
Diagnosis of Epilepsy
Findings of this study revealed that traditional healers diagnose epilepsy through observation of seizures accompanied by stiffness, confusion, unconsciousness, urination, excretion of foam from the mouth and passing flatus in Mpumalanga and Limpopo Provinces. Participants in Limpopo further explained that seizures are classified as severe if they occur three times or more in a month. Few traditional healers use “tinhlolo” (bones) to confirm the diagnosis of epilepsy in Limpopo Province.
These findings are similar to other authors who found that epilepsy is characterized by recurring seizures that can be accompanied by unconsciousness and loss of bowel or bladder function stiff muscles, uncontrollable jerking movements of the arms and legs, dizziness, and anxiety are all symptoms of epilepsy.29,30 Epilepsy was diagnosed as a result of these observations. Furthermore, a study conducted by Nass,31 Stutton32 shows that epilepsy can be identified with basic blood tests (complete blood count, urea, creatinine, electrolytes, liver function tests, and glucose). Additionally, in appropriate circumstances, brain imaging (CT or MRI, if accessible) and cerebrospinal fluid analysis are considered during acute presentation. Traditional healers’ most prevalent diagnosis is the observation of seizures followed by various symptoms such as unconsciousness and tight muscles. Some healers, on the other hand, confirm the use of bones.
No participant verbalized the use of bones in Mpumalanga Province. Diagnosis of epilepsy through observation is common in both Provinces. These findings indicate that the traditional healers have a common diagnosis of epilepsy, although their treatment is different. Nevertheless, there is no scientific or documented proof that bones can be used for diagnosing clients. The traditional healers verbalized that the ancestors communicated with them and informed them that, the client had epilepsy through visions or consultation of bones.
Management of Epilepsy
The findings of this study show that the use of traditional herbs is the most common practice among traditional healers. The management includes the use of herbal plants, insects and urine. This practice is believed to be effective in curing epilepsy because some clients reported no longer having seizures after treatment. However, most PLWE still consult western medicine after consulting traditional healers, and some combine both western and traditional medicine, raising concern about the effectiveness of traditional herbs without the combination of any other treatment. These findings were supported by Dolo33 who stated that herbal medicines are currently the most popular complementary and other therapies and play an important role in treating epileptic seizures and antiepileptic drug side effects. Similarly, other studies indicate that herbal mixtures are commonly used for the treatment of epilepsy by traditional healers because they have strong beliefs that herbal medicine can cure epilepsy.34,35
Contrary to the above findings, a study conducted by Sign36 indicates that traditional healers’ epileptic herbal therapies are ineffective in managing epilepsy. The absence of progress in seizure attacks despite multiple consultations and treatments with several traditional healers demonstrated this. Instead of being managed or lessened, the seizures became more frequent. Herbal preparations have long been thought to be possible anticonvulsants; nevertheless, most traditional epileptic remedies have pro-convulsant effects, and these herbs could be the source of seizures in situations where herbal preparations are widely utilized for medical disorders.
However, the data of this study show that some PLWE were referred to a hospital for alternative epilepsy treatment, implying that herbal mixes may not be able to treat epilepsy at some point. Although herbal medicine is widely recognized and utilized in antiepileptic treatment, most traditional medicines lack sufficient evidence for efficacy and toxicity, indicating the necessity for collaboration with the health system.
Traditional healers described the use of insect “gonono” and chicken to treat epilepsy. It is perceived that “gonono” has epileptic seizures because it usually lies on its back and makes jerky movements to get up and fly. Traditional healers believe it can be used to cure epilepsy because it has seizures. The kind of management provided by traditional healers is based on their knowledge, attitude, practices and skills. The effectiveness of the management is based on verbal report from patients. There is no documented information for reference. Traditional healers also emphasized using urine to treat the condition as the believed that urine harbours and causes epilepsy. Urine is applied to the PLWE through open cuts made with a razor, and this practice is perceived as effective in the cure or management of epilepsy. These findings were supported by Deegbea29 who indicate that blood from bears, pigeons, worms, and various types of fish has also been used to treat epilepsy.
In addition, if a child’s epilepsy was caused by the mother witnessing an animal being slain while pregnant, the blood from that animal was the greatest option. Furthermore, the treatment of epilepsy includes using body fluids, which was once the most common method. It was said that drinking one’s own urine may prevent epilepsy. Drinking must be done with the left hand only. The PLWE could drink his or her own blood, but more frequently than not, blood from others. The mother of an epileptic child should give it three drops of her own blood Deegbea.29
However, Watila,28 Jacobs36 argue that epileptic seizures are controlled or reduced with antiepileptic drugs. The antiepileptic drugs include Phenobarbital, Phenytoin, Carbamazepine and Valproic acid, and they have been scientifically proven to be effective in the management of epilepsy. On the other hand, there is no documented evidence of effectiveness in the management of epilepsy using insects and urine. However, the evidence is based on verbal reports from clients living with epilepsy.
At least eight (8) traditional healers perceive that western medicine can treat epilepsy. They further indicated that a collaboration between health care system and traditional healers can be highly effective in the management of epilepsy. However, twelve (12) were against the collaboration due to the belief that epilepsy is only spiritual hence it cannot be treated by western medicine.
There were limitations in this study because some of the traditional healers were not willing to share information regarding diagnosis and management of epilepsy. However, other traditional healers shared a lot of information based on their indigenous knowledge and experiences regarding diagnosing and managing epilepsy.
Conclusion
The findings of this study revealed that the management of epilepsy by traditional healers is influenced by their beliefs in Limpopo and Mpumalanga Provinces. The traditional healer’s management is greatly influenced by their knowledge, attitude, practices, myths and misconceptions about epilepsy. The most common management is the use of traditional herbs. The use of insects and urine was only reported in Limpopo Province. However, most traditional healers in Mpumalanga Province acknowledge the need for collaboration with the health system to effectively manage epilepsy. There is a need to educate traditional healers regarding sepsis prevention and management as their practice involves open cuts on the skin. However, the management of epilepsy can be improved by developing a culture congruent intervention programme which provides management considering the beliefs of people living with epilepsy. This study recommends collaboration between traditional healers and the health system for effective diagnosis and management of epilepsy. This study also recommends health education regarding sepsis prevention and management to prevent infections.
Abbreviations
AEDs, Anti-epileptic drugs; PLWE, People living with epilepsy; CHM, Chinese herbal medicine; SSA, Sub-Saharan Africa.
Data Sharing Statement
The corresponding author will provide the data used in this study upon reasonable request.
Ethics Approval and Consent to Participate
All authors declare that all processes contributing to this work fulfil the ethical standards of the University of Venda. This study was reviewed and approved by the University of Venda Human and Clinical Trial Research Ethics Committee. The informed consent for all participants was approved before the study participation. Confidentiality and anonymity were ensured throughout data collection and analysis.
Acknowledgments
Special thanks to the participants who willingly participated in the study.
Funding
Sincerest gratitude to GladAfrica Foundation Trust and The Council for Scientific and Industrial Research (CSIR) for funding the study.
Disclosure
Authors have no conflict of interest to declare. The submitting author has been authorised by all co-authors to submit the research article. The research article is original, has not already been published in any other journal or is not currently under consideration for publication by another journal, and does not infringe any existing copyright or any other rights prescribed by law.
References
1. World Health Organisation. Epilepsy: A Public Health Imperative. Geneva: World Health Organisation. CC BY-NC-SA 3.0 IGO; 2019. Available from: https://creativecommons.org/licenses/by-nc-sa/3.0/igo.
2. Mjumbe CK, Amuri B, Zeufack LT, Kalimira RM, Kolela MM, Bora BK. Knowledge, attitude and practice of traditional healers on epilepsy in Lubumbashi. Open Access Lib J. 2020;7(6):1–8.
3. Kaddumukasa M, Nalubwama H, Kaddumukasa MN, et al. Barriers to epilepsy care in Central Uganda, a qualitative interview and focus group study involving PLWE and their caregivers. BMC Neurol. 2019;19(1):1. doi:10.1186/s12883-019-1398-z
4. Leone M, Marazzi MC, Tolno VT, Tedeschi G, Mancardi G. Epilepsy in sub-Saharan Africa: is there anything neurologists could learn from HIV/AIDS health care? Neurol Sci. 2020;41(11):3341–3343. doi:10.1007/s10072-020-04511-5
5. Singh G, Sharma M, Kumar GA, et al. The burden of neurological disorders across the states of India: the Global Burden of Disease Study 1990–2019. Lancet Global Health. 2021;9(8):e1129–e1144. doi:10.1016/S2214-109X(21)00164-9
6. Liu W, Ge T, Pan Z, Leng Y, Lv J, Li B. The effects of herbal medicine on epilepsy. Oncotarget. 2017;8(29):48385. doi:10.18632/oncotarget.16801
7. Auditeau E, Chassagne F, Bourdy G, et al. Herbal medicine for epilepsy seizures in Asia, Africa and Latin America: a systematic review. J Ethnopharmacol. 2019;24(234):119–153.
8. Chakraborty P, Sanchez NA, Kaddumukasa M, et al. Stigma reduction interventions for epilepsy: a systematized literature review. Epilepsy Behav. 2021;114:107381. doi:10.1016/j.yebeh.2020.107381
9. du Toit A, Pretorius C. Diagnostic and treatment practices for psychogenic nonepileptic and epileptic seizures in Namibia. Epilepsy Behav. 2018;83:92–102. doi:10.1016/j.yebeh.2018.03.005
10. Keikelame MJ, Swartz L. “A thing full of stories”: traditional healers’ explanations of Epilepsy and perspectives on collaboration with biomedical health care in Cape Town. Transcult Psychiatry. 2015;52(5):659–680. doi:10.1177/1363461515571626
11. Cai L. Traditional Chinese herbal medicine for epilepsy treatment should be administered according to the seizure type and epileptic syndrome. Health. 2017;9(8):1211. doi:10.4236/health.2017.98087
12. Lin CH, Hsieh CL. Chinese herbal medicine for treating epilepsy. Front Neurosci. 2021;2(15):798.
13. Antimov P, Tournev I, Zhelyazkova S, Sander JW. Traditional practices and perceptions of epilepsy among people in Roma communities in Bulgaria. Epilepsy Behav. 2020;1(108):107086. doi:10.1016/j.yebeh.2020.107086
14. Anand P, Othon GC, Sakadi F, et al. Epilepsy and traditional healers in the Republic of Guinea: a mixed methods study. Epilepsy Behav. 2019;1(92):276–282. doi:10.1016/j.yebeh.2019.01.017
15. Maiga Y, Albakaye M, Diallo LL, et al. Current beliefs and attitudes regarding Epilepsy in Mali. Epilepsy Behav. 2014;1(33):115–121. doi:10.1016/j.yebeh.2014.02.031
16. Mothibe ME, Sibanda M. African traditional medicine: south African perspective. Trad Complement Med. 2019;4:1–27.
17. Wagner RG, Kabudula CW, Forsgren L, et al. Epilepsy care cascade, treatment gap and its determinants in rural South Africa. Seizure. 2020;80:175–180. doi:10.1016/j.seizure.2020.06.013
18. De Vos AS, Strydom H, Fouche CB, Delport CSL, Kruger J. Research at Grass Roots: For the Social Sciences and Human Service Professions. de Vos AS, editor. Van Schaik Publishers; 2015.
19. Creswell JW. Educational Research: Planning, Conducting, and Evaluating Quantitative. NJ: Prentice Hall Upper Saddle River; 2015.
20. Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice. Lippincott Williams & Wilkins; 2017.
21. Thapa L, Bhandari TR, Shrestha S, Poudel RS. Knowledge, beliefs, and practices on epilepsy among high school students of Central Nepal. Epilepsy Res Treat. 2017;2017:1–7. doi:10.1155/2017/6705807
22. Thurman DJ, Begley CE, Carpio A, et al. The primary prevention of epilepsy: a report of the Prevention Task Force of the International League Against Epilepsy. Epilepsia. 2018;59(5):905–914. doi:10.1111/epi.14068
23. Beghi E. The epidemiology of epilepsy. Neuroepidemiology. 2020;54(2):185–191. doi:10.1159/000503831
24. Tuft M, Nakken KO, Kverndokk K. Traditional folk beliefs on epilepsy in Norway and Sweden. Epilepsy Behav. 2017;1(71):104–107. doi:10.1016/j.yebeh.2017.03.032
25. Smith CE, Kajumba M, Bobholz S, et al. Pluralistic and singular causal attributions for epilepsy in Uganda. Epilepsy Behav. 2021;114:107334. doi:10.1016/j.yebeh.2020.107334
26. Wagner RG, Bertram MY, Gómez-Olivé FX, et al. Health care utilization and outpatient, out-of-pocket costs for active convulsive Epilepsy in rural northeastern South Africa: a cross-sectional Survey. BMC Health Serv Res. 2016;16(1):1–8. doi:10.1186/s12913-016-1460-0
27. Idiculla PS, Gurala D, Philipose J, Rajdev K, Patibandla P. Cerebral cavernous malformations, developmental venous anomaly, and its coexistence: a review. Eur Neurol. 2020;83(4):360–368. doi:10.1159/000508748
28. Watila MM, Keezer MR, Angwafor SA, Winkler AS, Sander JW. Health service provision for people with Epilepsy in sub-Saharan Africa: a situational review. Epilepsy Behav. 2017;1(70):24–32. doi:10.1016/j.yebeh.2017.03.014
29. Deegbe DA, Aziato L, Attiogbe A. Beliefs of people living with Epilepsy in the Accra Metropolis, Ghana. Seizure. 2019;1(73):21–25. doi:10.1016/j.seizure.2019.10.016
30. Boumediene F, Chhour C, Chivorakoun P, et al. Community-based management of Epilepsy in Southeast Asia: two intervention strategies in Lao PDR and Cambodia. Lancet Reg Health West Pac. 2020;1(4):100042. doi:10.1016/j.lanwpc.2020.100042
31. Nass RD, Sassen R, Elger CE, Surges R. The role of postictal laboratory blood analyses in the diagnosis and prognosis of seizures. Seizure. 2017;1(47):51–65.
32. Sutton F, Barca D, Komoltsev I, et al. Testing blood and CSF in people with Epilepsy: a practical guide. Epileptic Disord. 2020;22(4):381–398. doi:10.1684/epd.2020.1191
33. Dolo H, Mandro M, Wonya’Rossi D, et al. Community perceptions of Epilepsy and its treatment in an onchocerciasis endemic region in Ituri, Democratic Republic of Congo. Infect Dis Poverty. 2018;7(1):1–9. doi:10.1186/s40249-018-0498-0
34. Kpobi L, Swartz L, Keikelame MJ. Ghanaian traditional and faith healers’ explanatory models for Epilepsy. Epilepsy Behav. 2018;1(84):88–92. doi:10.1016/j.yebeh.2018.04.016
35. Bounlu M, Auditeau E, Vorachit S, et al. Management of epilepsy in Laos: perceptions of healthcare professionals from Vientiane Capital province and traditional healers in Southern Laos. J Tradit Complement Med. 2021;11(1):46–52. doi:10.1016/j.jtcme.2019.12.003
36. Jacobs K, Julyan M, Lubbe MS, Burger JR, Cockeran M. Anti-epileptic prescribing patterns in the South African private health sector (2008–2013). South Afr Fam Pract. 2016;58(4):142–147. doi:10.1080/20786190.2016.1148337
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.