")
Back to Journals » Infection and Drug Resistance » Volume 16
Diagnosis of Acute Q Fever in a Patient by Using Metagenomic Next-Generation Sequencing: A Case Report
Authors Wang D , Zhang L, Cai Z, Liu Y
Received 22 January 2023
Accepted for publication 23 March 2023
Published 31 March 2023 Volume 2023:16 Pages 1923—1930
DOI https://doi.org/10.2147/IDR.S405697
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Dong Wang,1,* Litao Zhang,1,* Zhifang Cai,2 Yumei Liu2
1Department of Clinical Laboratory, Wuhan Asia General Hospital, Wuhan Asia General Hospital Affiliated to Wuhan University of Science and Technology, Wuhan, Hubei Province, 430056, People’s Republic of China; 2Pulmonary and Critical Care Medicine, Hankou Hospital of Wuhan, Hankou Hospital Affiliated to Wuhan University of Science and Technology, Wuhan, Hubei Province, 430012, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yumei Liu, Email [email protected]
Background: Q fever is a zoonotic disease caused by Coxiella burnetii infection, with domestic ruminants as the main source of infection and tick bites as one of the transmission vectors. The clinical manifestations of Q fever are varied and atypical. For the reason that C. burnetii is a strictly intracellular pathogen, it is difficult to be diagnosed by traditional culture methods. Additionally, serological and molecular diagnostic methods to assist in the diagnosis of Q fever are not routinely performed in most clinical laboratories. Therefore, early and rapid diagnosis of Q fever is a challenge.
Case Presentation: In the present study, a 34-year-old male patient presented with an acute onset and symptoms such as high fever, lethargy, pulmonary infection, and liver damage. In addition, he had a history of tick bites. Despite conducting relevant laboratory and radiological examinations, the etiology remained unknown. Subsequently, we detected the sequence reads of C. burnetii in a venous blood sample using metagenomic next-generation sequencing (mNGS), and the symptoms of patients were significantly improved after timely treatment with the special drug tetracycline. To our knowledge, this is the first report of Q fever associated with C. burnetii detected directly from venous blood sample in Wuhan, China.
Conclusion: Metagenomic next-generation sequencing is a new diagnostic technology that provides rapid and accurate detection of unexplained infections, including Q fever. Its application plays a crucial role in clinical diagnosis for identifying elusive pathogens.
Keywords: Q fever, Coxiella burnetii, metagenomic next-generation sequencing, case report
A Letter to the Editor has been published for this article.
A Response to Letter by Mr Dany has been published for this article.
Background
Q fever is a zoonotic disease caused by Coxiella burnetii infection, the main source of infection is domestic ruminants.1 The most common reservoirs are cattle, sheep, and goats.2 C. burnetii mainly exists in the urine, feces, amniotic fluid, and other excreta of infected animals, and it can survive in the environment for several years, and can form aerosols to transmit Q fever under certain conditions.3 Animals transmit to each other mainly through ticks.4 Humans can become infected by consuming unpasteurized dairy products and inhaling contaminated aerosols,2 and infection through tick bites has also been suggested. C. burnetii has been detected in many species of ticks (mainly Ixodes, Rhipicephalus, Amblyomma and Dermacentor).5 It has been demonstrated that C. burnetii could be transmitted through ticks in experimental systems and occasionally in the wild.5 Several case reports suggested this possibility.6,7 Q fever mainly occurs in hilly, mountainous, agricultural, and pastoral areas, however, the cases reported in Wuhan, China are very rare.
Q fever can manifest as a systemic infection and can be divided into acute and chronic according to the course of the disease.1,8 Early diagnosis and treatment will improve outcomes for people with Q fever. However, its clinical symptoms and imaging manifestations lack specificity, and it is easily missed and misdiagnosed. The pathogenic diagnosis of C. burnetii relies on nucleic acid and serological detection because it is a strictly intracellular pathogen and difficult to be detected by traditional culture methods.9,10 Additionally, serological and molecular diagnostic methods to assist in the diagnosis of Q fever are not routinely performed in most clinical laboratories. Metagenomic next-generation sequencing (mNGS) can detect a wide range of pathogens, including those that are difficult to culture, and can provide comprehensive coverage of pathogen species through direct detection of nucleic acids, which has a high reference value for the clinical diagnosis of new infections, complex infections, mixed infections and unknown pathogens.11–13
In this case, a patient who presented with an acute onset of high fever, lethargy, pulmonary infection, and liver damage was initially misdiagnosed as pneumonia. However, C. burnetii was detected by mNGS as the causative pathogen of Q fever, which guided efficient clinical medication and treatment.
Case Presentation
On April 26, 2022, a 34-year-old male patient presented at the fever clinic of Wuhan Hankou Hospital with a fever lasting for five days. The patient was subsequently admitted to the Department of Respiratory and Critical Care Medicine with a provisional diagnosis of pulmonary infection. The patient reported having experienced fever without an obvious cause, with a maximum temperature of 41.0°C. The patient denied having a cough, purulent sputum, chest tightness or pain, abdominal pain, diarrhea, urinary frequency or urgency. The patient had no known history of hypertension, diabetes, or cardiovascular disease, and was considered to be in good overall health. The patient had received clindamycin and cefotaxime sodium treatment for three days prior to admission at the outpatient clinic, but showed no improvement. On April 24, our hospital conducted an outpatient chest computed tomography (CT) scan, which revealed several interstitial lesions in both lungs, emphysema, and bullae. Additionally, laboratory tests conducted on the same day showed an elevated C-reactive protein (CRP) level of 91.64 mg/L, and a white blood cell (WBC) count of 11.50×109/L. After admission, physical examinations were performed and the findings were as follows: temperature, 36.5°C (normal range, 36.3–37.2°C); respiratory rate, 20 breaths/minute (normal range, 16–18 breaths/minute); and blood pressure, 100/80 mmHg (normal range, 90–140/60–90 mmHg). The patient had thick breath sounds in both lungs and a few moist rales in both lower lungs. Although the patient’s body skin was not yellowed, his sclera appeared slightly yellowed. The patient had a regular heart rhythm, and auscultation of the heart valves did not reveal any pathological murmurs. Other physical examinations were normal. The results of laboratory tests were as follows (Figure 1): total white blood cell count, 5.00×109/L (normal range, 3.50 × 109–9.50×109/L); neutrophil count, 3.90×109/L (normal range, 1.80 × 109–6.30×109/L); hemoglobin, 149 g/L (normal range, 130–175 g/L); platelet count, 71×109/L (normal range, 125 × 109–350×109/L); C-reactive protein, 93.15 mg/L (normal range, 0.00–5.00 mg/L); Procalcitonin 2.13 ng/mL (normal range, 0.00–0.50 ng/mL); total protein, 63.5 g/L (normal range, 65.0–85.0 g/L); alanine aminotransferase, 167 U/L (normal range, 9–50 U/L); aspartate aminotransferase, 143 U/L (normal range, 15–40 U/L); total bilirubin, 28.9μmol/L (normal range, 0.0–26.0 μmol/L); direct bilirubin, 19.0 μmol/L (normal range, 0.0–8.0 μmol/L); fibrinogen content, 4.53g/L (normal range, 2.00–4.00 g/L); and D-dimer content, 1.75 ug/mL (normal range, 0.00–0.50 ug/mL). Serological tests for hepatitis viruses, human immunodeficiency virus (HIV), and syphilis (RPR) were performed and all of them were negative. Moreover, a brain CT scan showed no abnormalities. The patient was empirically administrated with piperacillin-tazobactam (4.5g, q8h) intravenously.
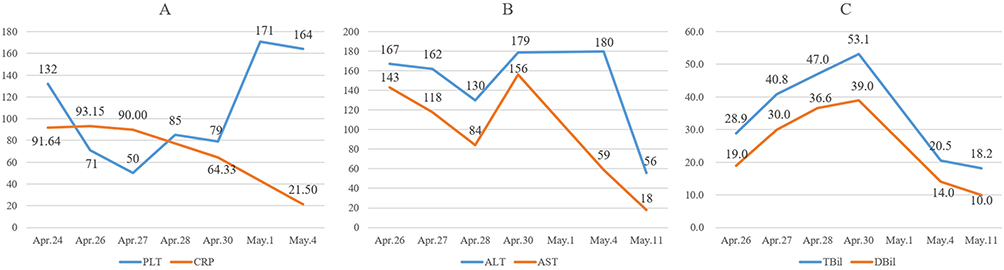 |
Figure 1 The patient’s laboratory dynamic monitoring indicators. (A) The dynamic monitoring of the level of PLT and CRP (PLT normal range, 125×109–350×109/L; CRP normal range, 0.00–5.00 mg/L); (B) The dynamic monitoring of the level of ALT and AST (ALT normal range, 9–50 U/L; AST normal range, 15–40 U/L); (C) The dynamic monitoring of the level of TBiL and DBiL (TBil normal range, 0.0–26.0 μmol/L; DBil normal range, 0.0–8.0 μmol/L). Abbreviations: PLT, platelet; CRP, C-reactive protein; ALT, alanine transaminase; AST, aspartate aminotransferase; TBiL, total bilirubin; DBiL, direct bilirubin. |
During the ward round on April 27, the patient presented with a persistent fever, with a maximum body temperature of 39.4°C, accompanied by fatigue, headache, and poor appetite and mood. The patient’s total abdominal CT showed no significant abnormalities, but lower lung infection and inflation were observed. Additionally, the patient’s D-dimer levels were critically high at 5.32 ug/mL. On the ward round on April 28, the patient continued to have a fever, with a body temperature of up to 39.2°C, and reported experiencing an irritating headache on the top of the right skull. However, brain magnetic resonance imaging (MRI) scans showed no obvious abnormalities. Treatment with piperacillin-tazobactam was not effective, and considering the possibility of atypical pathogen infection, levofloxacin (0.4g, qd) was added for anti-infective therapy.
Further investigation into the patient’s medical history revealed that the patient’ occupation was raising pigs and he had a history of insect bites on the left lower extremity more than two weeks prior. The bite had caused redness, swelling, and pain, which had now subsided, leaving only a reddish skin scab at the site. Given these findings, rare pathogen infection caused by tick bites was suspected. Since the throat swab and blood culture taken at admission were negative, mNGS examination was recommended to rule out tick-borne diseases. However, the patient needed to consider whether to do this examination. At present, the patient’s condition was considered to be caused by a combination of upper respiratory tract infection and pulmonary infection, but infection with rare pathogens could not be ruled out.
On April 30, tetracycline (250mg, q6h) was added empirically to the original treatment for anti-tick infection (Figure 2). Subsequently, the patient agreed to undergo mNGS examination to assist the diagnosis. The mNGS was performed using the Illumina NextSeq platform (Illumina, San Diego, CA, USA), and the detection content is pathogenic microorganism next-generation sequencing (DNA + RNA). The detection range covered bacteria (including Mycobacterium, Mycoplasma, Chlamydia, Rickettsia, and Spirochetes), fungi, viruses (DNA viruses, RNA viruses), parasites, and drug resistance genes.
 |
Figure 2 Longitudinal analysis of temperature change and therapeutic drug. After using specific drugs—tetracycline, the temperature was under control. Abbreviations: TZP, piperacillin-tazobactam; LEV, levofloxacin; TC, tetracycline. |
On May 1, one day after the patient’s blood sample was sent for the mNGS, the mNGS results suggested the existence of Coxiella burnetii (mapping sequence number 79, relative abundance 15.96%) (Figure 3). Combining the patient’s history of insect bites, occupation, symptoms and signs, and auxiliary examination results, the patient was diagnosed with acute Q fever infection with pneumonia.
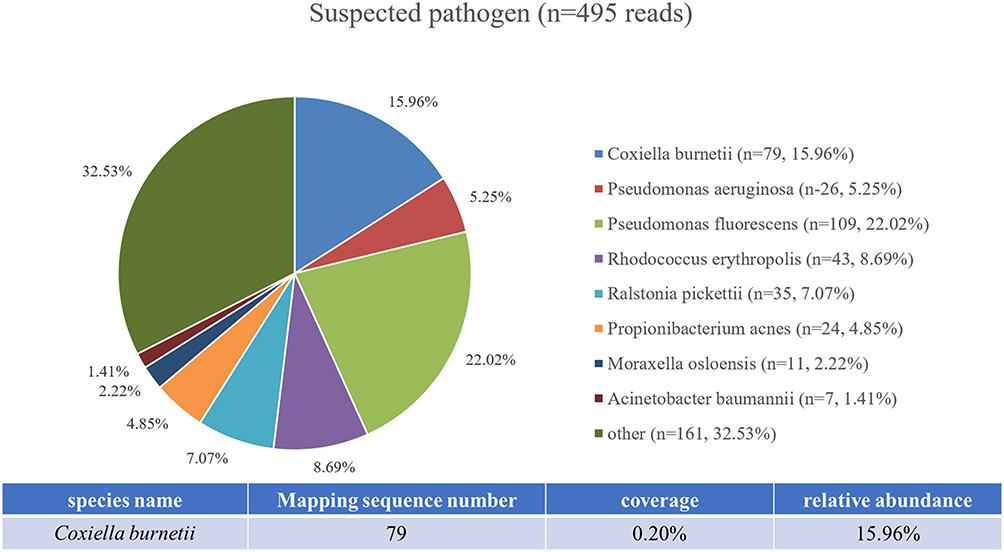 |
Figure 3 The results of metagenomic next-generation sequencing in blood. “Mapping sequence number” means that the number of reads can be uniquely mapped to the genome of Coxiella burnetii, but cannot be mapped to other species. The 79 reads covered 0.20% of C. burnetii genome. The “relative abundance” reflected the relative proportion of genomes in the corresponding classification of the pathogen. |
On May 6, the patient still had intermittent low-grade fever after orally taking tetracycline tablets for 7 days, but no other discomfort was reported. Therefore, the patient requested to be discharged, but we informed him that he did not meet the discharge criteria. However, due to personal reasons, the patient strongly requested to be discharged. One week after the patient was discharged from the hospital, we contacted the patient for a follow-up visit. The patient reported that he had intermittent low-grade fever, the chest CT showed no lung infection, and his laboratory test indicators were normal. Half a month after discharge, the patient reported no physical discomfort and no recurrence of fever during a telephone follow-up.
Discussion and Conclusion
In 1937, an unexplained fever was identified in Queensland, Australia, and subsequently named Q fever.1 Q fever is one of the most widespread zoonotic diseases worldwide, caused by Coxiella burnetii, which is distributed in all global regions.1 There are various host species of Q fever, including rodents, birds, ticks, ruminants, and humans, with cattle, sheep, horses, and dogs being the main sources of infection.1,14
The clinical manifestations of Q fever are varied, with some patients exhibiting severe acute or chronic infectious symptoms, while others may only experience mild clinical signs and symptoms, usually with no or only low-grade fever.15 Pneumonia is a manifestation of acute Q fever, with either a sudden or gradual onset, and the disease is somewhat self-limited. The early imaging of the disease may appear normal, and it rarely progresses to acute respiratory failure or acute respiratory distress syndrome. As a result, Q fever is often misdiagnosed as influenza or common pneumonia.1,16 In the case presented, the patient remained high fever after admission, and the disease continued to progress despite the empirical anti-infective treatment. Laboratory examination suggested an acute infection, impaired liver function, abnormal coagulation function, thrombocytopenia, negative blood culture, and an undetermined the etiology of infection.
Upon re-questioning the patient’s medical history, it was revealed that the patient had a history of tick bites, leading to consideration of the possibility of a rare pathogen infection caused by ticks. Ticks are considered to be the most significant transmission vector of Q fever, and animals primarily transmitting the infection to one another through tick bites.4 Various ticks can carry C. burnetii, which is passed on to other animals through blood-sucking.17 Clinical manifestations of Q fever are nonspecific, and laboratory testing is the main method of diagnosis at present, including serology, nucleic acid, etc.9,10 Serology is a common method for detecting antibodies to the disease, but it is not suitable for early diagnosis due to a possible false-negative diagnosis, especially when antibiotics are used or the patient has low immune function.18 Enzyme-linked immunosorbent assay (ELISA) and indirect immunofluorescence assay (IFA) are commonly used serologic tests for the diagnosis of Q fever, but they cannot distinguish between acute and chronic Q fever.18 In addition, the use of serological methods is limited by the techniques used to obtain antigens, and inconsistencies in analytical standards can affect accuracy, making it challenging to use on a broad scale.19 Molecular detection, such as PCR, can be positive when the acute infection is suspected prior to the antibody response.10,20 However, targeted assays can only be performed when clinicians suspect Q fever in acutely febrile patients. Therefore, the diagnosis of Q fever is a challenge, especially in the early stages of infection.
mNGS can directly determine the microbial nucleic acid sequence in the sample by high-throughput sequencing technology and compare the measured sequence with the existing sequence in the database. This approach can quickly and objectively identify the pathogenic microorganisms (including viruses, bacteria, fungi, and parasites) in the samples, making it especially suitable for the diagnosis of difficult clinical cases.11
Recently, mNGS has been increasingly used to identify pathogenic microorganisms that are clinically rare or difficult to culture. In 2015, Wilson et al21 used mNGS to diagnose a case of meningitis caused by ameba barbae. Subsequently, several cases of rare pathogen detection using mNGS were reported. For example, Mai et al22 detected Japanese encephalitis virus in the urine of a 16-year-old boy with encephalitis, Du et al23 reported a case where human sparganosis was diagnosed for the first time using mNGS. These studies show that mNGS technology has significantly enhanced the detection of rare pathogens and represents an innovation and a leap forward in the field of infectious disease diagnosis. Besides, Guo-Shuai Lin24 reported a case of Q fever endocarditis diagnosed by mNGS, and Stafford25 reported two cases of murine typhus caused by Rickettsia typhi in pregnant women with unexplained fever and headache diagnosed by mNGS. The patients in these cases responded well to doxycycline treatment, confirming that Rickettsia was a pathogenic bacterium and indicating that mNGS has high sensitivity for diagnosing Rickettsia infection. Huang et al26 also reported the epidemic of acute Q fever in Zhuhai city confirmed by mNGS, demonstrating that mNGS has higher sensitivity than the 72.2% seropositivity rate and 95% quantitative real-time PCR (qPCR) positive rate. Although the cost of mNGS is currently higher than that of traditional laboratory tests, such as serological and molecular assays, these tests for Q fever are not routinely performed in most clinical laboratories in China, including our local clinical laboratories, and diagnostic kits for these tests are difficult to obtain. In addition, mNGS is becoming increasingly common in local clinical laboratories as a novel pathogen identification method. Therefore, we recommend that patients undergo mNGS examination to exclude tick infection and to clarify the etiological evidence of unexplained fever. In this case, the patient agreed to undergo mNGS 2 days after our suggestion because the previous treatment was not effective.
Although mNGS has unique advantages for clinical microbiology detection and has become increasingly popular in clinical applications, its ability to detect certain fastidious, undetectable, and low load microorganisms needs improvement. The broad spectrum of microbial coverage also poses significant challenges in the interpretation of mNGS results. Removal of host nucleic acids is a technical option being explored currently to enhance mNGS detection. There are several methods under investigation to remove/reduce host nucleic acids from samples, including physical methods such as centrifugation or filtration,27,28 and chemical methods such as differential lysis of chemical reagents.29 However, all these methods lose some of the pathogens to some extent.30 Additionally, the use of additional reagents in the de-hosting process may increase the risk of exogenous background contamination.31 Furthermore, some pathogens with thicker cell walls, such as fungi and intracellular bacteria, may have lower nucleic acid extraction efficiency, leading to lower microbial nucleic acid load during the assay, which can affect the assay performance.32,33 Significantly, when interpreting the results, mNGS needs to set individualized reporting thresholds considering the pathogenicity and pathogenic conditions of different microorganisms.34
Pseudomonas fluorescens is widely found in nature and studies have shown that it is one of the human body colonizing bacteria.35,36 In this study, the mNGS data showed that the relative abundance of Pseudomonas fluorescens (22.02%) was higher than that of C. burnetii (15.96%). However, due to Pseudomonas fluorescens being a main clinical conditional and hospital-acquired pathogens,35,36 combined with the clinical symptoms (acute hyperthermia, flaccid fever, etc.), epidemiological history (history of tick bite), and negative blood culture (Pseudomonas fluorescens is more easily cultured in blood culture), the infection was considered to be mainly attributed to C. burnetii. Although other bacteria were also detected by mNGS, such as Pseudomonas aeruginosa, Pseudomonas immobilis, and Propionibacterium are conditionally and hospital-acquired pathogens, and their low sequence number suggested secondary bacterial infection due to immunosuppression caused by C. burnetii infection. It is also possible that these bacteria were introduced into the blood samples from the skin and hospital environment during the sampling process for patients. Furthermore, when treating the Q fever infection, attention should also be given to secondary infection besides the C. burnetii infection itself.
Tetracyclines are broad-spectrum agents with antibiotic activity against a wide range of microorganisms.37 They are widely used to treat infected humans and animals because of their good antimicrobial properties and minimal adverse side effects. Tetracyclines inhibit bacterial protein synthesis by preventing the binding of aminoacyl-tRNA to bacterial ribosomes,37 which then preventing the entry of new amino acids into the nascent peptide chain and thereby inhibits protein synthesis.38 As a result, tetracyclines inhibit the synthesis of proteins necessary for bacterial growth and survival, thus exerting an antibacterial effect.39 Tetracycline and doxycycline are two commonly used tetracycline antibiotics to treat acute and chronic Q fever.40 While doxycycline is the preferred regimen for the treatment of acute Q fever,1,40 we successfully treated a patient with acute Q fever with tetracycline tablets in this study. Our choice of tetracycline tablets was based on its availability at our institution and its indications for use included Q fever. Notably, a case report from China described the recovery of a 12-year-old child from acute Q fever after treatment with tetracycline tablets, providing additional evidence for the efficacy of tetracycline in treating this disease.41 Our report, in conjunction with this case report, supports the effectiveness of tetracycline in the treatment of Q fever.
In this case, the patient presented with acute Q fever, headache and other clinical symptoms, and the examination after admission showed acute Q fever manifestations, such as pulmonary inflammation with abnormal liver function. A history of tick bites, blood samples mNGS detected C. burnetii, and the symptoms of the patient were significantly improved after treatment with the special drug tetracycline, leading to a diagnosis of Q fever. In addition, mNGS assists in early diagnosis when conventional etiological tests are negative.
In summary, traditional etiological diagnostic methods presented limitations, making it challenging to diagnose C. burnetii timely. mNGS is a novel diagnostic technology, and its application can provide a rapid and accurate detection methods for clinical diagnosis, which plays a decisive role in diagnosis for cases of unexplained infections. Due to the early diagnosis of mNGS, appropriate antimicrobial therapy and symptomatic supportive care can be given as early as possible to reduce mortality. The indications of testing should be strictly clinically correlated in order to avoid abuse and increasing economic burden of the patient.
Abbreviations
mNGS, Metagenomics next-generation sequencing; CT, computed tomography; CRP, C-reactive protein; WBC, white blood cell; PLT, Platelet; ALT, alanine aminotransferase; AST, aspartate aminotransferase; TBil, total bilirubin; DBil, direct bilirubin; MRI, magnetic resonance imaging; TZP, piperacillin-tazobactam; LEV, levofloxacin; TC, tetracycline.
Data Sharing Statement
All the data in this study are included in the published articles.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Wuhan Hankou Hospital. The consent from the patient for the publication of the case was obtained.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by research and innovation fund of Wuhan Asia General Hospital (No. 2022KYCX1-B09).
Disclosure
The authors declare that there is no conflict of interest in this work.
References
1. Eldin C, Mélenotte C, Mediannikov O, et al. From Q fever to Coxiella burnetii infection: a paradigm change. Clin Microbiol Rev. 2017;30(1):115–190. doi:10.1128/CMR.00045-16
2. Im JH, Baek J, Durey A, Kwon HY, Chung MH, Lee JS. Current status of tick-borne diseases in South Korea. Vector Borne Zoonotic Dis. 2019;19(4):225–233. doi:10.1089/vbz.2018.2298
3. Candela MG, Caballol A, Atance PM. Wide exposure to Coxiella burnetii in ruminant and feline species living in a natural environment: zoonoses in a human–livestock–wildlife interface. Epidemiol Infect. 2017;145(3):478–481. doi:10.1017/S0950268816002454
4. Seo MG, Lee SH, VanBik D, et al. Detection and genotyping of Coxiella burnetii and Coxiella-like bacteria in horses in South Korea. PLoS One. 2016;11(5):e0156710. doi:10.1371/journal.pone.0156710
5. Duron O, Sidi-Boumedine K, Rousset E, Moutailler S, Jourdain E. The importance of ticks in Q fever transmission: what has (and has not) been demonstrated? Trends Parasitol. 2015;31(11):536–552. doi:10.1016/j.pt.2015.06.014
6. Beaman MH, Hung J. Pericarditis associated with tick-borne Q fever. Aust N Z J Med. 1989;19(3):254–256. doi:10.1111/j.1445-5994.1989.tb00258.x
7. Huang J, Wang R, Gao C, et al. A case of tick-transmitted Q fever in Lishui, China diagnosed by next-generation sequencing. J Int Med Res. 2021;49(9):3000605211025398. doi:10.1177/03000605211025398
8. Kouijzer IJE, Kampschreur LM, Wever PC, et al. The value of 18F-FDG PET/CT in diagnosis and during follow-up in 273 Patients with chronic Q fever. J Nucl Med. 2018;59(1):127–133. doi:10.2967/jnumed.117.192492
9. Kampschreur LM, Oosterheert JJ, Koop AMC, et al. Microbiological challenges in the diagnosis of chronic Q fever. Clin Vaccine Immunol. 2012;19(5):787–790. doi:10.1128/CVI.05724-11
10. Schneeberger PM, Hermans MHA, van Hannen EJ, Schellekens JJA, Leenders ACAP, Wever PC. Real-time PCR with Serum samples is indispensable for early diagnosis of acute Q fever. Clin Vaccine Immunol. 2010;17(2):286–290. doi:10.1128/CVI.00454-09
11. Consensus Group of Experts On Application of Metagenomic Next Generation Sequencing In The Pathogen Diagnosis In Clinical Moderate And Severe Infections, Professional Committee of Sepsis and Shock Chinese Research Hospital Association, Professional Committee of Microbial Toxins Chinese Society for Microbiology, Professional Committee of Critical Care Medicine Shenzhen Medical Association. 宏基因组学测序技术在中重症感染中的临床应用专家共识(第一版)[Expert consensus for the application of metagenomic next generation sequencing in the pathogen diagnosis in clinical moderate and severe infections (first edition)]. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020;32(5):531–536. Chinese. doi:10.3760/cma.j.cn121430-20200228-00095
12. Xing F, Ye H, Deng C, et al. Diverse and atypical manifestations of Q fever in a metropolitan city hospital: emerging role of next-generation sequencing for laboratory diagnosis of Coxiella burnetii. PLoS Negl Trop Dis. 2022;16(4):e0010364. doi:10.1371/journal.pntd.0010364
13. Zeng X, Wu J, Li X, et al. Application of metagenomic next-generation sequencing in the etiological diagnosis of infective endocarditis during the perioperative period of cardiac surgery: a prospective cohort study. Front Cardiovasc Med. 2022;9:811492. doi:10.3389/fcvm.2022.811492
14. Gürtler L, Bauerfeind U, Blümel J, et al. Coxiella burnetii - Pathogenic Agent of Q (Query) Fever. Transfus Med Hemother. 2014;41(1):60–72. doi:10.1159/000357107
15. Hartzell JD, Wood-Morris RN, Martinez LJ, Trotta RF. Q fever: epidemiology, diagnosis, and treatment. Mayo Clin Proc. 2008;83(5):574–579. doi:10.4065/83.5.574
16. von Ranke FM, Clemente Pessoa FM, Afonso FB, et al. Acute Q fever pneumonia: high-resolution computed tomographic findings in six patients. Br J Radiol. 2019;92(1095):20180292. doi:10.1259/bjr.20180292
17. Hartelt K, Pluta S, Oehme R, Kimmig P. Spread of ticks and tick-borne diseases in Germany due to global warming. Parasitol Res. 2008;103(Suppl 1):S109–S116. doi:10.1007/s00436-008-1059-4
18. Anderson A, Bijlmer H, Fournier PE, et al. Diagnosis and management of Q fever--United States, 2013: recommendations from CDC and the Q Fever Working Group. MMWR Recomm Rep. 2013;62(RR–03):1–30.
19. Robinson MT, Satjanadumrong J, Hughes T, Stenos J, Blacksell SD. Diagnosis of spotted fever group Rickettsia infections: the Asian perspective. Epidemiol Infect. 2019;147:e286. doi:10.1017/S0950268819001390
20. Fournier PE, Raoult D. Comparison of PCR and serology assays for early diagnosis of acute Q fever. J Clin Microbiol. 2003;41(11):5094–5098. doi:10.1128/JCM.41.11.5094-5098.2003
21. Wilson MR, Naccache SN, Samayoa E, et al. Actionable diagnosis of neuroleptospirosis by next-generation sequencing. N Engl J Med. 2014;370(25):2408–2417. doi:10.1056/NEJMoa1401268
22. Mai NTH, Phu NH, Nhu LNT, et al. Central nervous system infection diagnosis by next-generation sequencing: a glimpse into the future? Open Forum Infect Dis. 2017;4(2):ofx046. doi:10.1093/ofid/ofx046
23. Du B, Tao Y, Ma J, et al. Identification of sparganosis based on next-generation sequencing. Infect Genet Evol. 2018;66:256–261. doi:10.1016/j.meegid.2018.10.005
24. Lin GS, Zhao MM, Li XQ, Yu HX. A case report of infective endocarditis with failure of the empirical treatment-Q fever endocarditis diagnosed by metagenomic next-generation sequencing. Infect Drug Resist. 2022;15:2545–2550. doi:10.2147/IDR.S361969
25. Stafford IA, Centeno FH, Al Mohajer M, et al. Successful detection of unrecognized rickettsia typhi in pregnancy using cell-free next-generation sequencing. Case Rep Obstet Gynecol. 2020;2020:6767351. doi:10.1155/2020/6767351
26. Huang M, Ma J, Jiao J, et al. The epidemic of Q fever in 2018 to 2019 in Zhuhai city of China determined by metagenomic next-generation sequencing. PLoS Negl Trop Dis. 2021;15(7):e0009520. doi:10.1371/journal.pntd.0009520
27. Ji XC, Zhou LF, Li CY, et al. Reduction of human DNA contamination in clinical cerebrospinal fluid specimens improves the sensitivity of metagenomic next-generation sequencing. J Mol Neurosci. 2020;70(5):659–666. doi:10.1007/s12031-019-01472-z
28. Bal A, Pichon M, Picard C, et al. Quality control implementation for universal characterization of DNA and RNA viruses in clinical respiratory samples using single metagenomic next-generation sequencing workflow. BMC Infect Dis. 2018;18(1):537. doi:10.1186/s12879-018-3446-5
29. Marotz CA, Sanders JG, Zuniga C, Zaramela LS, Knight R, Zengler K. Improving saliva shotgun metagenomics by chemical host DNA depletion. Microbiome. 2018;6(1):42. doi:10.1186/s40168-018-0426-3
30. Gu W, Miller S, Chiu CY. Clinical metagenomic next-generation sequencing for pathogen detection. Annu Rev Pathol. 2019;14:319–338. doi:10.1146/annurev-pathmechdis-012418-012751
31. Chiu CY, Miller SA. Clinical metagenomics. Nat Rev Genet. 2019;20(6):341–355. doi:10.1038/s41576-019-0113-7
32. Miao Q, Ma Y, Wang Q, et al. Microbiological diagnostic performance of metagenomic next-generation sequencing when applied to clinical practice. Clin Infect Dis. 2018;67(suppl_2):S231–S240. doi:10.1093/cid/ciy693
33. Zhou X, Wu H, Ruan Q, et al. Clinical evaluation of diagnosis efficacy of active mycobacterium tuberculosis complex infection via metagenomic next-generation sequencing of direct clinical samples. Front Cell Infect Microbiol. 2019;9:351. doi:10.3389/fcimb.2019.00351
34. Li N, Cai Q, Miao Q, Song Z, Fang Y, Hu B. High-throughput metagenomics for identification of pathogens in the clinical settings. Small Methods. 2021;5(1):2000792. doi:10.1002/smtd.202000792
35. Scales BS, Dickson RP, LiPuma JJ, Huffnagle GB. Microbiology, genomics, and clinical significance of the Pseudomonas fluorescens species complex, an unappreciated colonizer of humans. Clin Microbiol Rev. 2014;27(4):927–948. doi:10.1128/CMR.00044-14
36. Benito N, Mirelis B, Luz Gálvez M, et al. Outbreak of Pseudomonas fluorescens bloodstream infection in a coronary care unit. J Hosp Infect. 2012;82(4):286–289. doi:10.1016/j.jhin.2012.09.008
37. Chukwudi CU. rRNA binding sites and the molecular mechanism of action of the tetracyclines. Antimicrob Agents Chemother. 2016;60(8):4433–4441. doi:10.1128/AAC.00594-16
38. Brodersen DE, Clemons WM, Carter AP, Morgan-Warren RJ, Wimberly BT, Ramakrishnan V. The structural basis for the action of the antibiotics tetracycline, pactamycin, and hygromycin B on the 30S ribosomal subunit. Cell. 2000;103(7):1143–1154. doi:10.1016/s0092-8674(00)00216-6
39. Chopra I, Roberts M. Tetracycline antibiotics: mode of action, applications, molecular biology, and epidemiology of bacterial resistance. Microbiol Mol Biol Rev. 2001;65(2):232–260. doi:10.1128/MMBR.65.2.232-260.2001
40. Maurin M, Raoult D. Q fever. Clin Microbiol Rev. 1999;12(4):518–553. doi:10.1128/CMR.12.4.518
41. Wu JW, Zhao QQ, Ma JJ, et al. A case of acute Q fever in a child. Chin J Infect Dis. 2021;39(9):569–570. doi:10.3760/cma.j.cn311365-20210123-00026
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.