Back to Journals » Journal of Multidisciplinary Healthcare » Volume 9
Development of the parental needs scale for rare diseases: a tool for measuring the supportive care needs of parents caring for a child with a rare disease
Authors Pelentsov L, Fielder A, Laws T, Esterman A ![]()
Received 30 May 2016
Accepted for publication 6 July 2016
Published 9 September 2016 Volume 2016:9 Pages 425—433
DOI https://doi.org/10.2147/JMDH.S113898
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Lemuel J Pelentsov,1 Andrea L Fielder,2,3 Thomas A Laws,4 Adrian J Esterman1,2,5
1School of Nursing and Midwifery, 2Sansom Institute for Health Research, 3School of Pharmacy and Medical Sciences, University of South Australia, Adelaide, SA, Australia; 4School of Nursing and Midwifery, Faculty of Health, Keele University, Staffordshire, UK; 5Australian Institute for Health and Tropical Medicine, James Cook University, Cairns, QLD, Australia
Background: Children and families affected by rare diseases have received scant consideration from the medical, scientific, and political communities, with parents’ needs especially having received little attention. Affected parents often have limited access to information and support and appropriate health care services. While scales to measure the needs of parents of children with chronic illnesses have been developed, there have been no previous attempts to develop a scale to assess the needs of parents of children with rare diseases.
Objective: To develop a scale for measuring the supportive care needs of parents of children with rare diseases.
Method: A total of 301 responses to our Parental Needs Survey were randomly divided into two halves, one for exploratory factor analysis and the other for confirmatory factor analysis (CFA). After removing unsuitable items, exploratory factor analysis was undertaken to determine the factor structure of the data. CFA using structural equation modeling was then undertaken to confirm the factor structure.
Results: Seventy-two items were entered into the CFA, with a scree plot showing a likely four-factor solution. The results provided four independent subscales of parental needs: Understanding the disease (four items); Working with health professionals (four items); Emotional issues (three items); and Financial needs (three items). The structural equation modeling confirmed the suitability of the four-factor solution and demonstrated that the four subscales could be added to provide an overall scale of parental need.
Conclusion: This is the first scale developed to measure the supportive care needs of parents of children with rare diseases. The scale is suitable for use in surveys to develop policy, in individual clinical assessments, and, potentially, for evaluating new programs. Measuring the supportive care needs of parents caring for a child with a rare disease will hopefully lead to better physical and psychological health outcomes for parents and their affected children.
Keywords: rare diseases, parents, scale, supportive care needs, measure, factor analysis
Background
Most rare diseases are life-threatening or chronically debilitating illnesses, the majority of which are genetic based, originate during fetal development, are associated with significant disability, and have no cure, preexisting pathways of care, or personalized medical intervention strategies.1,2 There exist >8,000 distinct rare diseases, many of which have no formal title, are difficult to diagnose, and, in combination, affect 6%–10% of the total population.3,4 Notably, the definition of a rare disease differs between countries; the European Union defines a rare disease as affecting 1:2,000, the United States as one affecting <200,000, and Australia as 1:10,000,5 though many individuals suffer from diseases that are far rarer.
Children and families affected by rare diseases have traditionally received limited consideration from medical, scientific, and political communities,6 with parents’ needs especially having received very little attention. Due to the rarity of many of these diseases, parents often have limited access to information and support and appropriate health care services. This includes a lack of experienced health professionals with knowledge and awareness of their child’s disease to aid them in their child’s care and informed decision making regarding long-term care provision.7 In addition, in order to appropriately care for their child with a rare disease, parents often require additional specialist health literacy and knowledge, caregiving skills, and resources beyond those normally required by parents.8,9 Although parents of children with chronic health problems face similar issues, parents of children with rare diseases often have additional problems. This may be due to delayed or undetermined diagnosis, a lack of support groups, and limited health care skills and resources.10
Assessing needs
Being able to identify and measure the supportive care needs of parents caring for children with rare diseases is beneficial. First, it can be used by local and national authorities to establish the prevalence of parents in need and to plan and develop suitable policies and programs to meet those needs. Second, at the individual level, measuring needs can be used by health professionals to screen parents for suitable referral to appropriate services. Finally, at the population level, measuring needs can be used to evaluate health programs or services established to assist parents of children affected by rare diseases. To date, no such tool exists for assessing the needs of parents caring for a child with a rare disease. However, four existing instruments assessing the needs of families caring for a child with a chronic illness have been developed.
The Parent Experience of Chronic Illness11 questionnaire is a 25-item self-reported scale designed to measure illness-specific adjustment in parents with a child diagnosed with a brain tumor. It consists of four subscales: Guilt and Worry; Unresolved Sorrow and Anger; Long-term Uncertainty; and Emotional Resources.
The Impact on Family Scale12,13 is a 24-item interviewer-administered measure designed to assess parents’ perceptions of the impact of their child’s chronic illness on the family. The four subscales include Financial burden; Familial/social impact; Personal strain; and Mastery.
The Family Needs Assessment Tool14 is a 54-item self-reported measure designed to evaluate the needs of families with a chronically ill child, as perceived by the parents themselves rather than by health professionals. It contains three subscales: Special services; Information needs; and Obstacles to treatment.
The Family Needs Survey15 is a 35-item parent-completed instrument developed to assess the functional needs of families of young children with developmental disabilities and to assist in the preparation of individualized family service plans and school-and community-based programs. Items are grouped into six domains of needs: Needs for Information; Needs for Support; Explaining to Others; Community Services; Financial Needs; and Family Functioning.
Of the aforementioned four scales, one was developed for parents of a child with a brain tumor, one was for parents of physically handicapped children, and two for parents of a child with a chronic condition. While the studies used to develop these scales were reasonably well conducted, only one (Impact on Family Scale) actually asked parents directly what their needs were (ie, using a qualitative approach) in order to develop suitable questions to elucidate such needs. Although there is certainly some overlap of needs between parents of a child with a chronic condition and those with a child with a rare disease, it is likely that these existing scales do not cover all the domains of supportive care needs of parents with a child with a rare disease.16,17
In summary, to date, few well-constructed scales exist that can delineate the many complex facets of parenting a child with a rare disease, can comprehensively assess the needs of parents caring for a child with a rare disease, and can be used across a wide range of diseases.13 These findings highlight the need for a new measurement tool to comprehensively assess the domains of unmet supportive care needs of parents of children with rare diseases. The study presented here describes the development of a new scale aimed at measuring important aspects of supportive care needs for parents of a child with a rare disease.
Methods
The scale presented here was developed from the Parental Needs Survey, a survey designed to establish the supportive care needs of parents of a child with a rare disease.18 The Parental Needs Survey comprised 45 questions (108 items) and was separated into six sections: 1) Demographics; 2) Equity in care; 3) Practical care needs; 4) About your relationships; 5) About your emotions; and 6) Summary. The survey was made available online for a 4-month period (February–May 2015) to parents living in Australia and New Zealand. A total of 301 parents representing >130 distinct rare diseases completed the survey. These parents were primarily mothers (91%, n=275/301). The age brackets of parents ranged from 15 years to 55+ years. The exact ages of parents were not obtained. The majority of parents were either in a married or de facto relationship (86%, n=258/301). Most respondents had at least one child living with them with a rare disease. Twelve parents reported that their child remained undiagnosed or was yet to receive a confirmed diagnosis. One-third of parents (33%, n=95/301) who completed the survey were living in a country/rural area.
The Parental Needs Survey was developed after undertaking a scoping review of the literature16 and qualitative research.17 The scoping review was undertaken to identify existing knowledge regarding the supportive care needs of parents caring for a child with a rare disease. Needs that were identified were categorized into one of seven domains outlined in the widely used Supportive Care Needs Framework19 and included social, informational, emotional, practical, physical, spiritual, and psychological. Four focus groups were then undertaken with parents of children with a variety of rare diseases to gain further insights into their needs in caring for their child. Three major themes were identified from the focus group data, including feeling boxed in outside the box (which describes the unique problems seen in parents of a child with a rare disease); practicalities of care (which describes the daily care challenges of these parents); and relationships (which describes the relational impact on partner and siblings of the affected child). From the scoping review, physical health needs and spiritual needs were discounted, as the former were not considered relevant to parents and the latter scarcely appeared in the literature. Careful consideration of the remaining supportive care needs domains, along with the three themes identified in the focus group data, lead to the final sections in the Parental Needs Survey. This study was approved by the University of South Australia Human Research Ethics Committee (protocol: 0000031772) and informed consent was obtained when participants completed the survey online.
For the purposes of scale development, the 301 parents who responded to the Parental Needs Survey were randomly divided into two halves, one for exploratory factor analysis (EFA) to create the initial scale and the other for confirmatory factor analysis (CFA) to validate the scale. There is no consensus about required sample sizes for both EFA and CFA; however, a minimum sample of 100 has been proposed.20
Exploratory factor analysis
The first random half of the data set consisted of 144 respondents. An EFA was undertaken using SPSS 22 (IBM Corporation, Armonk, NY, USA). Demographic items (n=16) and open-ended items (n=8) were first removed. Any items that were not considered applicable to all respondents (eg, questions related to partners; n=12) were also removed, leaving 72 out of the original 108 items. Missing values for the 72 items ranged from 12.5% to 26.4%. The 72 items were then entered into the EFA, and principal components extraction was used to provide a scree plot to determine the likely number of factors. For this analysis, missing values were replaced by means. The scree plot indicated that there were likely four factors. A second principal components extraction was then undertaken forcing a four-factor solution. An oblique rotation using Direct Oblimin was used to determine whether the factors extracted were correlated. Since all correlations between factors were close to zero, an orthogonal rotation using a Varimax solution was finally undertaken. To assist in interpretation, factor loadings were sorted by size, and loading <0.5 not displayed. Hair et al21 recommended a cutoff of 0.5 for factor loadings with a sample size of that used in our EFA.
Confirmatory factor analysis
The second random half of the data consisted of 157 respondents. CFA was undertaken using the Stata 14 structural equation model procedure. In particular, the four-factor solution found from the EFA was entered into the procedure, plus a latent overall score derived from the four factors. For estimation, the mlmv (maximum likelihood missing values) method was used. Goodness-of-fit of the model was assessed using the root mean squared error of approximation and comparative fit index (CFI) measures. Modification indices were assessed to check whether modification to any paths would provide a better fit. The final scale and subscales were assessed for internal consistency using Cronbach’s alpha.
Results
Exploratory factor analysis
Table 1 is a summary of the EFA results. After Varimax rotation, sorting factor loadings into size order, and ignoring factor loadings <0.50, the four extracted factors had clear interpretations.
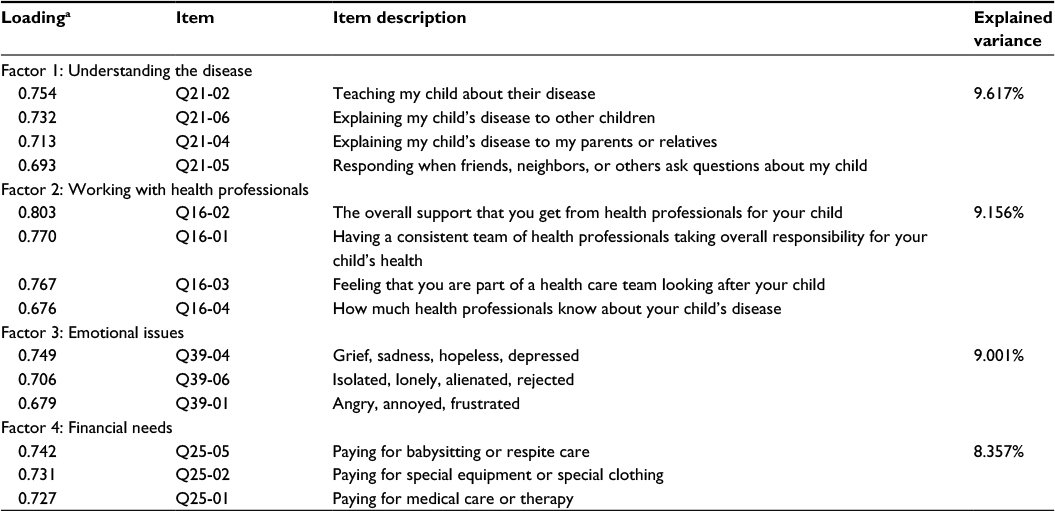 | Table 1 Summary of EFA results using principal factor axis rotation with a Varimax orthogonal solution (n=144) Note: aCorrelation between factor and item. Abbreviation: EFA, exploratory factor analysis. |
The first factor, which was named Understanding the disease, loaded on four items related to parent’s level of knowledge and understanding of their child’s disease and their ability to communicate and teach others. The second factor, Working with health professionals, also loaded on four items and assesses parents’ level of support from health professionals and feeling part of a health care team caring for their child. The third factor labeled Emotional issues comprised three items specific to the emotions commonly expressed by parents in caring for their child. The fourth and final factor called Financial needs also comprised three items and measures the financial impact of having a child with a rare disease.
Confirmatory factor analysis
To evaluate construct validity and to confirm the four factors identified in the EFA, a CFA was undertaken. In addition, further testing was undertaken to determine whether the four factors could be combined into an overall needs score. Table 2 presents the results of the CFA. Notably, the paths (standardized coefficients) from the 14 items to their respective factors were all highly statistically significant. Further, the paths from the four factors to the overall needs score were also highly statistically significant. For goodness of fit, the root mean square error and the CFI were estimated. The goodness of fit results (Table 2) indicate that the model provided a reasonable fit to the data. In particular, it is recommended that the root mean squared error of approximation should be <0.09 and the CFI >0.9, which is the case with our model. An examination of modification indices found no better fit to the data.
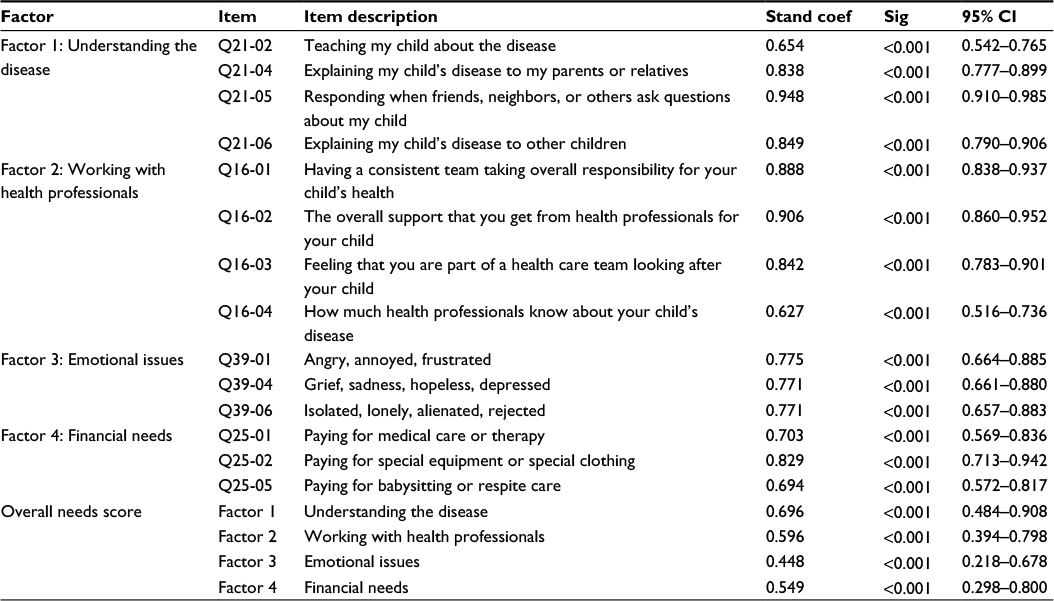 | Table 2 Summary of CFA results using maximum likelihood estimation and imputation of missing values (n=157) Notes: Goodness of fit: root mean square error of approximation =0.075, 90% CI: 0.054–0.096; comparative fit index =0.942. Abbreviations: CFA, confirmatory factor analysis; Stand coef, standardized coefficients; Sig, significance; CI, confidence interval. |
For each factor (or subscale), a summative score was created by adding the score for each item and converting it to a 0–25 score with the overall score obtained by summing each of the subscale scores so that 0 represents a parent with no needs whatsoever and 100 a parent who is in desperate need of support.
Finally, Table 3 shows the mean and standard deviations for the four subscales and overall score for all 301 respondents.
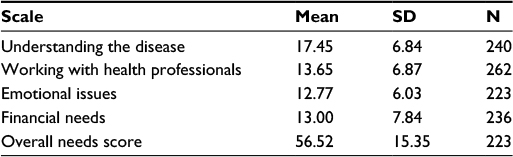 | Table 3 Descriptive statistics for subscales (n=301) Abbreviation: SD, standard deviation. |
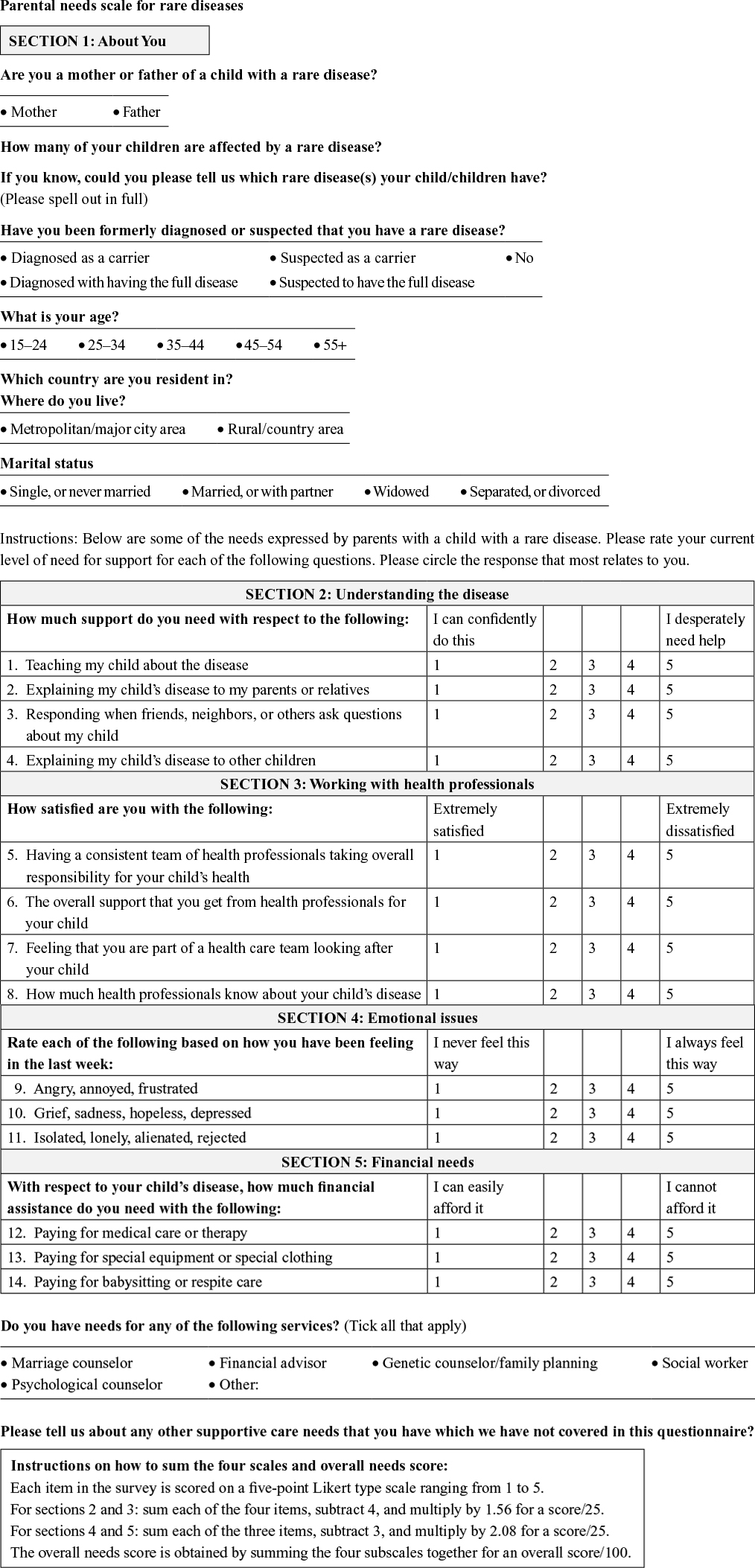
The overall scale and four subscales all showed good internal consistency by Cronbach’s alpha: Overall needs score (α=0.870); Understanding the disease (α=0.892); Working with health professionals (α=0.883); Emotional issues (α=0.811); and Financial needs (α=0.761). Out of the four subscales, the greatest need appears to be related to the need for parental knowledge of disease, followed by greater support from health professionals. Supplementary material contains the revised questionnaire based on these results, to be used to measure the four subscales and overall needs score, and instructions for scoring.
Discussion
This study provides initial psychometric data and describes the development of a new scale for assessing the needs of parents with children with rare diseases. To our knowledge, this is the first scale that has been developed that focuses specifically on measuring the supportive care needs of parents caring for a child with a rare disease.
Our initial EFA determined that the questionnaire data contained four factors or subscales, and these were confirmed using structural equation modeling. Importantly, we were able to show using the structural equation modeling that the four subscales could be added together to create an overall needs score, which we have labeled the parental needs scale for rare diseases (PNS-RD).
Typically, questionnaires can be developed in two ways. If the area of interest is already well researched and the developers of a questionnaire are confident that they understand all potential issues, then a questionnaire can be designed based on the current literature and clinical experience. However, for areas of interest not so well understood, the alternative is to undertake qualitative research with the population of interest, soliciting their feedback in order to determine the domains of need and develop suitable question items.22,23 For the four previously developed existing scales that purport to measure needs of parents of a child with a chronic condition,11,12,14,15 in the development of three of these scales,11,14,15 the authors assumed that they already knew what domains of need were important from their own knowledge and the literature and derived an initial list of questionnaire items. In contrast, no such assumptions were made during the development of the PNS-RD. In the development of the PNS-RD, extensive qualitative research was undertaken asking affected parents themselves what their supportive care needs were. As rare disease research relating to parents is scarce and poorly understood, it was felt necessary to incorporate a qualitative research component in order to develop a tool that was comprehensive and appropriate to the population of interest.
Further, the majority of existing scales were developed for parents of a child with a specific single condition. In the development of the PNS-RD, parents of >130 different rare diseases were involved, which likely allows the results to be generalizable to all parents of a child with a rare disease, at least in Australia and New Zealand.
We believe the PNS-RD scale to be psychometrically robust, simple to use, and quick to complete. As the impact of a child’s disease can vary on the family unit, the PNS-RD will make it possible for health professionals to accurately assess and reassess the supportive care needs of parents at any stage in their child’s disease journey or child’s age. Further, we believe the tool will aid governments and nongovernmental support agencies to more appropriately allocate time, money, and resources in meeting the needs of parents and address knowledge gaps with how best to provide support. Finally, the tool may prove useful in evaluating existing programs/interventions aimed at supporting parents affected by rare diseases, thus helping to reduce the overall cost burden to health and maximizing the way services are delivered to these groups in need.
Limitations of study
As well as the previously discussed strengths of the current studies approach, the study also has some limitations. The first stems from sampling issues with mothers accounting for the vast majority of responses to the survey. Fathers accounted for only a small percentage (8.6%, n=26/301) of responses despite repeated recruitment efforts, and thus, their perspectives on issues related to parental supportive care needs remained underrepresented in the development of the PNS-RD scale. While this study did report on >130 rare diseases, this number could still be considered small given that >8,000 rare diseases have been identified. Rare diseases by definition are rare, and recruitment challenges and small sample sizes are a common dilemma for researchers working in the area of rare diseases.24,25 The findings of this study are limited to parents living in Australia and New Zealand. While we can assume that parents caring for a child with a rare disease share common needs regardless of disease or country of residence, we cannot generalize these findings to other countries where access to health care services can differ. Therefore, further research is required to validate these findings in other countries. Like all internet surveys of this type, we were unable to establish response rates since there was no sampling frame. Finally, the PNS-RD scale still needs to be assessed for test–retest reliability and convergent validity in further research.
Conclusion
Most children and families affected by rare diseases have in the past received very little support. Being able to identify and measure their needs is therefore beneficial in helping them cope with the multicomplex burden of having a child with a rare disease. The absence of measures that suitably identify the needs of parents has led us to develop a tool designed specifically to assess the supportive care needs of parents caring for children with rare diseases. This is the first study to develop a tool purposed specifically for the rare disease population. This 14-item scale should prove useful in assessing parental supportive care needs, ensuring parents are given support that is tailored to their actual needs. We envisage that the tool will provide government and nongovernmental support agencies with clearer direction on where to focus future efforts in order to improve delivery of care and access to support.
Author contributions
Lemuel J Pelentsov, Andrea L Fielder, Thomas A Laws, and Adrian J Esterman were involved in study design and conception, design and acquisition of data, analysis and interpretation of the data, and drafting the manuscript and revising it critically. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Aymé S, Schmidtke J. Networking for rare diseases: a necessity for Europe. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2007;50(12):1477–1483. | ||
Elliott E, Zurynski Y. Rare diseases are a ‘common’ problem for clinicians. Aust Fam Physician. 2015;44(9):630–633. | ||
Feltmate K, Janiszewski P, Gingerich S, Cloutier M. Delayed access to treatments for rare diseases: who’s to blame? Respirology. 2015;20(3):361–369. | ||
Spagnolo P, du Bois R. The challenges of clinical research in orphan diseases. In: Cottin V, Cordier J-F, Richeldi L, editors. Orphan Lung Diseases. London: Springer; 2015:5–15. | ||
Zurynski Y, Frith K, Leonard H, Elliott E. Rare childhood diseases: how should we respond? Arch Dis Child. 2008;93(12):1071–1074. | ||
Anderson M, Elliott E, Zurynski Y. Australian families living with rare disease: experiences of diagnosis, health services use and needs for psychosocial support. Orphanet J Rare Dis. 2013;8(1):22. | ||
Anderson D, Dumont S, Jacobs P, Azzaria L. The personal costs of caring for a child with a disability: a review of the literature. Public Health Rep. 2007;122(1):3–16. | ||
Kirk S, Glendinning C. Developing services to support parents caring for a technology-dependent child at home. Child Care Health Dev. 2004;30(3):209–218. | ||
Sartore G, Lagioia V, Mildon R. Peer Support Interventions for Parents and Carers of Children with Complex Needs. The Cochrane Library; 2013. | ||
Jaffe A, Zurynski Y, Beville L, Elliott E. Call for a national plan for rare diseases. J Paediatr Child Health. 2010;46(1–2):2–4. | ||
Bonner M, Hardy K, Guill A, McLaughlin C, Schweitzer H, Carter K. Development and validation of the parent experience of child illness. J Pediatr Psychol. 2006;31(3):310–321. | ||
Stein R, Riessman C. The development of an impact-on-family scale: preliminary findings. Med Care. 1980;18(4):465–472. | ||
Stein R, Jessop D. The impact on family scale revisited: further psychometric data. J Dev Behav Paediatr. 2003;24(1):9–16. | ||
Rawlins P, Rawlins T, Homer M. Development of the family needs assessment tool. West J Nurs Res. 1990;12(2):201–214. | ||
Bailey D, Simeonsson R. Assessing needs of families with handicapped infants. J Spec Educ. 1988;22(1):117–127. | ||
Pelentsov L, Laws T, Esterman A. The supportive care needs of parents caring for a child with a rare disease: a scoping review. Disabil Health J. 2015;8(4):475–491. | ||
Pelentsov L, Fielder A, Esterman A. The supportive care needs of parents with a child with a rare disease: a qualitative descriptive study. J Pediatr Nurs. 2016;31(3):e207–e218. | ||
Pelentsov L, Fielder A, Laws T, Esterman A. The supportive care needs of parents with a child with a rare disease: results of an online survey. BMC Fam Pract. 2016;17:88. | ||
Fitch M. Needs of patients living with advanced disease. Can Oncol Nurs J. 2005;15(4):230–242. | ||
Iacobucci D. Structural equations modeling: fit indices, sample size, and advanced topics. J Consum Psychol. 2010;20(1):90–98. | ||
Hair J, Black W, Babin B, Anderson R, Tatham R. Multivariate Data Analysis. Upper Saddle River, NJ: Pearson Prentice Hall; 2006. | ||
Boynton P, Greenhalgh T. Selecting, designing, and developing your questionnaire. BMJ. 2004;328(7451):1312–1315. | ||
Nassar-McMillan S, Borders L. Use of focus groups in survey item development. Qual Rep. 2002;7(1):1–12. | ||
Khangura S, Karaceper M, Trakadis Y, et al. Scoping review of patient- and family-oriented outcomes and measures for chronic pediatric disease. BMC Pediatr. 2015;15(1):1–9. | ||
Walker K. Rare disease-specific social media sites: an opportunity for collaboration. J Commun Healthc. 2013;6(1):71–76. |
Supplementary material
 |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.