Back to Journals » Journal of Pain Research » Volume 16
Development of the Chronic Pain Cognition Scale: A Culture-Sensitive Pain Measurement in Chinese
Authors Wu CH ![]() , Chou WH, Long YH, Yang HH, Lin T, Yang CC, Sun WZ, Chen CC, Lin CP
, Chou WH, Long YH, Yang HH, Lin T, Yang CC, Sun WZ, Chen CC, Lin CP ![]()
Received 9 June 2023
Accepted for publication 22 August 2023
Published 6 September 2023 Volume 2023:16 Pages 3075—3084
DOI https://doi.org/10.2147/JPR.S422197
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Chih-Hsun Wu,1,2 Wei-Han Chou,3 Yi-Hsun Long,2 Hao-Han Yang,1 Tung Lin,1 Chi-Cheng Yang,1,4 Wei-Zen Sun,3 Chih-Cheng Chen,5 Chih-Peng Lin3
1Department of Psychology, National Chengchi University, Taipei, Taiwan; 2Clinical Psychology Center, National Taiwan University Hospital, Taipei, Taiwan; 3Department of Anesthesiology, National Taiwan University Hospital, Taipei, Taiwan; 4Holistic Mental Health Center, Taipei City Hospital, Taipei, Taiwan; 5Institute of Biomedical Sciences, Academia Sinica, Taipei, Taiwan
Correspondence: Chih-Peng Lin, Department of Anesthesiology, National Taiwan University Hospital, 7 Chung Shan S. Road, Taipei, 100225, Taiwan, Tel +886 2 23123456 #262158, Fax +886 2 23415736, Email [email protected]
Purpose: People with pain problems are highly vulnerable to cultural disparities, and it is imperative to reduce these inequalities. This cross-sectional study aimed to develop a culturally sensitive Chronic Pain Cognition Scale (CPCS) for Chinese-/Chinese dialect-speaking populations and investigate its psychometric properties.
Patients and Methods: Adult patients with chronic low back pain or chronic neck pain who visited pain clinics at a medical center in northern Taiwan were enrolled. Participants completed the demographic, intensity of pain, and two other related sensations, “Sng (痠)” and “Ma (麻)”, often reported in Chinese-speaking populations, CPCS, Chronic Pain Acceptance Questionnaire-8, and Pain Self-Efficacy Questionnaire.
Results: 200 patients were included. Patients’ mean age was 64.84 ± 14.33, 126 (63.0%) were female, and 83 (41.5%) had 13+ years of education. The average duration of pain was 77.25 ± 97.46 months, the intensity of pain was 6.04 ± 2.50, Ma was 3.43 ± 3.24, and Sng was 4.54 ± 3.14. The CPCS comprised four factors: pain impact (how pain impact one’s life), losing face (how one being disrespected due to pain), helplessness, and avoidance, with good structural validity and adequate reliability (Cronbach α, 0.60– 0.81) and satisfactory criterion-related validity. Moreover, losing face, an essential concept in Chinese relationalism, was significantly related to pain, Sng, and Ma (r = 0.19, 0.15 and 0.16), but not to pain acceptance or self-efficacy, indicating a culturally specific element in pain measurement.
Conclusion: The CPCS has good psychometric properties and is suitable for evaluating chronic pain in the clinical setting, and might be generalizable to other Chinese-/Chinese dialect-speaking populations.
Keywords: low back pain, neck pain, pain impact, losing face, helplessness, avoidance
Introduction
Reducing inequality is a significant issue in people with pain problems. Because pain is not merely nociception of physical damage but “an unpleasant sensory and emotional experience associated with, or resembling, actual or potential tissue damage”.1 In 2020, the IASP added six notes to emphasize further that “pain is always a personal experience that is influenced to varying degrees by biological, psychological, and social factors” and “people learn the concept of pain through their life experiences”.2 These statements accentuated that “pain is learned”, thus, it is impossible to ignore the influence of ethnicity/race and the culture in which one is raised.
A recent topical review appealed to the importance of understanding how socioeconomic positions affect pain by psychosocial, behavioral, and biological mechanisms.3 The study indicated that poorer socioeconomic positions, such as low education, low occupational positions, financial hardship, and living in a deprived area, are related to higher pain incidence, prevalence, intensity, frequency, and pain-related disability. In addition, some reviews on ethnicity/race noted that ethnic minority backgrounds are related to lower pain tolerance4 and more pain-related suffering.5
Culture can also affect how one experiences pain. Review studies have found cultural variations in illness perception, self-efficacy, coping strategies, locus of control, pain attitudes,6 avoidance behavior, and pain intensity7 in chronic pain. A study reviewed studies from 2000 to 2020 found that being minorities (mainly Blacks, Hispanics, and Asians), compared to the White population, negatively influenced the clinical decision-making of chronic pain.8 The pain of minorities, especially Blacks, was often underestimated by physicians, less likely to receive opioids, and were monitored closer for possible opioids misuse.8 Thus, it is imperative to combat these disparities in pain management.
Therefore, how to measure pain in a culturally sensitive way is an indispensable first step in research and in clinical settings.9,10 Nevertheless, most pain measurements were developed in Western cultures and might not fit the needs of other cultures, such as Taiwan. For instance, the widely used McGill Pain Questionnaire (MPQ)11 is a good example to illustrate that people in different cultures might experience pain and describe pain differently. The MPQ evaluates how one feels the pain by asking people to choose a word that best describes their pain experience in each of the 20 categories (eg, choosing from jumping, flashing, and shooting in the spatial category). Most of the concepts/words used in the MPQ were universal and suitable for Chinese speaking population. However, some of the words was difficult to translate correctly into Chinese, and our patients seldom described their sensations in these ways. On the other hand, some of the discomforting sensations that the Taiwanese frequently expressed, such as “Sng(痠)” or “Ma(麻)” do not have suitable English words to convey these sensations perfectly nor be listed in the current pain taxonomy. Sng (pronounced səŋ in Taiwanese dialect) is a word that represents the state of soreness while at the same time imitating the natural vocalization of humans feeling sore.12 Some studies have found that Sng (soreness sensation) might decrease muscle strength and activities of daily living and affect patients’ quality of life.13 Ma (pronounced mâ in Taiwanese dialect) is less studied. In brief, Ma is a Taiwanese word that describes the feeling of numbness and tingling pain simultaneously. Furthermore, the concepts of Ma and Sng also exist in many Chinese dialects.
Consequently, this study aimed to develop a scale that could accurately evaluate how patients with chronic pain think of their pain, especially in an Eastern cultural background. We used exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) to verify the structural validity of the scale, and confirmed criterion-related validity through relevant pain assessment tools.
Materials and Methods
Participants
This cross-sectional study was focused on patients with chronic lower back pain or chronic neck pain. It was conducted at an outpatient pain clinic in a medical center in northern Taiwan. It complied with the Declaration of Helsinki, approved by the National Taiwan University Hospital’s research ethics committee (reference number: 201605046RIND), and all participants signed written informed consent. Eligible participants were adult patients with chronic lower back pain or chronic neck pain (pain duration >3 months) who visited the pain clinic during 2016 to 2021. Patients with communication problems (eg, hearing and vision problems), dementia or other severe neurocognitive problems, cancer diagnosis, and life expectancy <6 months were excluded from the study. Research assistants first explained the study, and if the patient agreed to join, then they asked them to sign the informed consent form and answer the study questionnaires. Most patients completed the questionnaires within 15–25 minutes. If patients had some difficulties in completing the questionnaires (eg, presbyopia), research assistants assisted them throughout the process.
Measurements
Demographical Variables and Pain Intensity
Pain, Ma (numbness and tingling pain), and Sng (soreness pain) intensities during the past week were evaluated using a numerical rating scale (NRS) ranging from 0 (no pain) to 10 (extreme pain; the worse pain as you can imagine). Pain duration, sex, age, and educational level were also assessed.
Chronic Pain Cognition Scale (CPCS)
Thirty-five patients with chronic pain (25 women and 10 men; age range, 47–87 years) were interviewed to develop the Chronic Pain Cognition Scale (CPCS) items. The following topics were derived from the New Patient Questionnaire of the Stanford Pain Management Center14 were discussed during the interview for a more comprehensive understanding of their life experiences: pain (intensity, quality, duration, and frequency), how the pain starts, what caused (the reason for) the pain, patient’s attitude toward the pain, how the pain affects daily life (eg, sleep and daily activities), how to cope with the pain, medical experiences, what treatment works, substance use (eg, smoking, alcohol, and prescription drugs), life before the pain (eg, major life events and childhood), family’s (significant others) attitude toward the patient’s pain, and subjective social support.
Approximately 60 items were drafted from the patients’ interview transcripts. After deleting items that were difficult to read, those with similar wording, those with specific experience (eg, not all patients had been treated by injection), and those that might be misunderstood, 13 items were selected to compose the CPCS, as shown in Table 1 (or please refer to the CPCS in the Supplementary 1 (English Version) and Supplementary 2 (Traditional Chinese Version)). The instruction of the CPCS was as follows: “The following items are some descriptions about pain. Please rate how much you agree with each item as it applies to you”. The participants were asked to rate each item on a 5-point Likert scale: 1, totally disagree; 2, disagree; 3, half-and-half; 4, agree; and 5, totally agree.
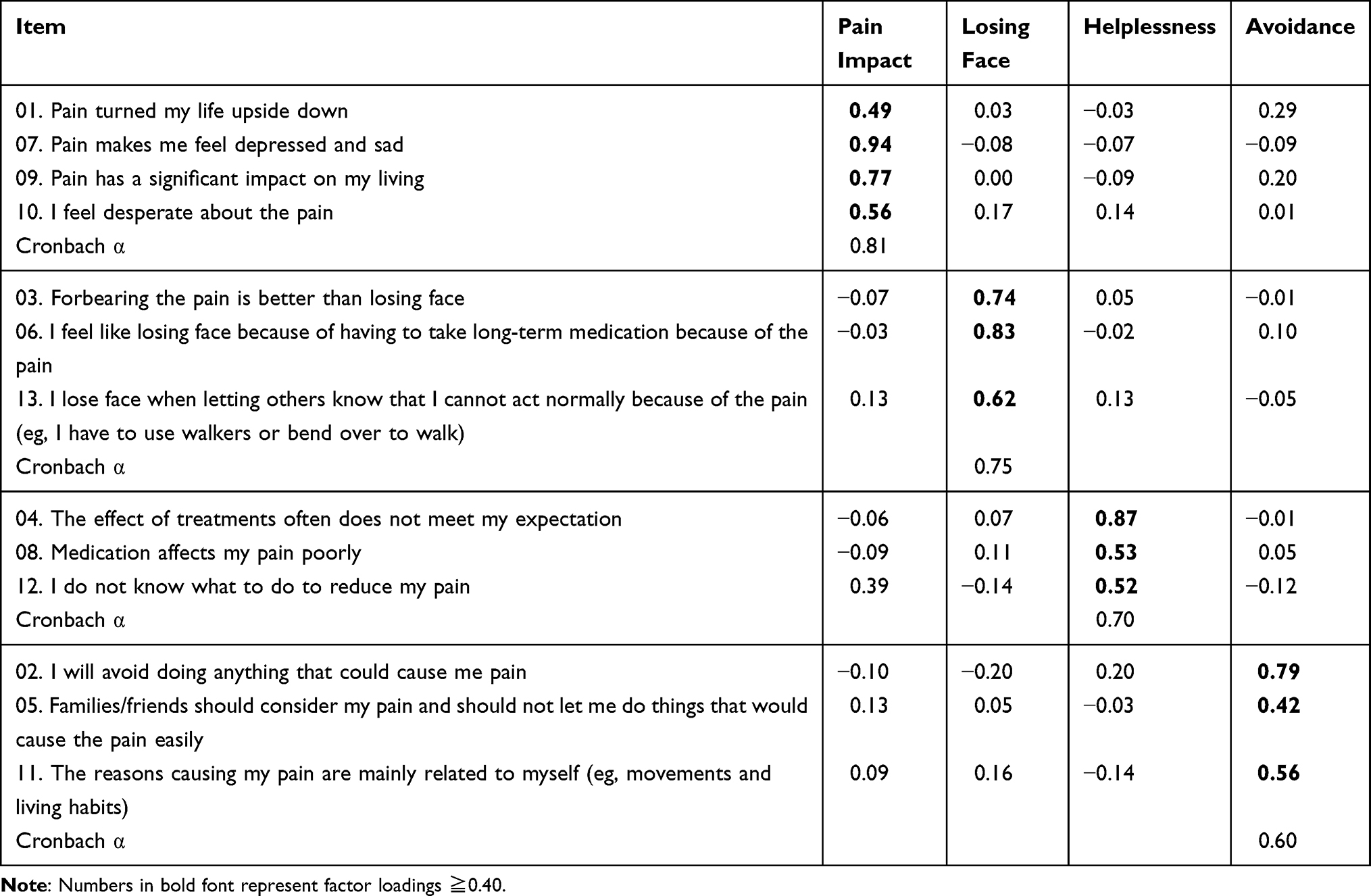 |
Table 1 Results of Exploratory Factor Analysis: Factor Loadings and Internal Consistency |
Validity Measures
The study aims to develop a scale to evaluate how people think of pain. The Chronic Pain Acceptance Questionnaire-8 (CPAQ-8) measures “Pain Acceptance”, which refers to people understanding that pain will persist and thus will think of possible ways to achieve a better quality of life and not only fixate on dealing with the pain. The Pain Self-Efficacy Questionnaire (PSEQ) measures “Pain Self-Efficacy”, which refers to how one considers pain to influence their abilities to enjoy life, engage in social activities, perform household tasks, work, and achieve life goals, and their ability to cope with pain. Thus, the CPAQ-8 and the PSEQ were used as validity measures since they both assess how people think of their pain, but in partially different aspects.
Chronic Pain Acceptance Questionnaire-8
Pain acceptance was measured using the 8-item Chronic Pain Acceptance Questionnaire-8 (CPAQ-8).15 The CPAQ-8 instructs the patients to “rate the truth of each statement as it applies to you” on a 7-point Likert scale: 0, never true to 6, always true. The CPAQ-8 has two factors: 1) activity engagement refers to the “pursuit of life activities regardless of pain” and 2) pain willingness refers to the “recognition that avoidance and control are often unworkable methods of adapting to chronic pain”. Higher scores reflect better pain acceptance. The CPAQ-8 had good internal consistency and 6–8-week test-retest reliability in activity engagement (Cronbach α = 0.79, r = 0.86) and pain willingness (Cronbach α = 0.77, r = 0.68), and good structural and criterion-related validity.
Pain Self-Efficacy Questionnaire
Pain self-efficacy was measured using the 10-item Pain Self-Efficacy Questionnaire (PSEQ).16 The PSEQ instructs the patients to “rate how confident you are that you can do the following things at present, despite the pain” on a 7-point Likert scale: 0, not at all confident to 6, completely confident. Higher scores reflect better pain self-efficacy. The PSEQ has a single factor with excellent internal consistency (Cronbach α = 0.92), good 3-month test-retest reliability (r = 0.73), and sound structural and criterion-related validity.
Statistical Analysis
First, to clarify and further confirm the factor structure of the CPCS, the current study randomly split the sample into two groups described in the following. The chi-square test and t-test were used to examine if there were any significant differences in sex, education, age, and pain intensity between the two groups. The two groups were treated as parallel samples if no significant differences were found. Group 1 was used in the EFA, and group 2 was used in the CFA.
The Kaiser–Meyer–Olkin (KMO) test and Bartlett test of sphericity were used to examine whether the data were suitable for the EFA. The principal axis method was used for factor extraction, and the promax method was used for factor rotation. The number of factors was determined using parallel analysis, the scree test, and eigenvalues. The inclusion criterion was set at an absolute value of factor loading ≥0.4. Finally, the internal consistency reliability (Cronbach α) was calculated for each factor and for the entire scale.
In the CFA, the factor structure of the model specification followed the EFA results. Maximum likelihood was used for the model estimation. To evaluate model fit, the chi-square, root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR), Bentler comparative fit index (CFI), and goodness-of-fit index (GFI) were used as model fit indices. An RMSEA ≤0.06,17 GFI ≥0.90, CFI ≥0.90, and SRMR ≤0.05 represent excellent model fitness, and an SRMR between 0.05 and 0.08 is considered a good fit for the model.18
As for criterion-related validity, the Pearson correlation between the CPCS factor scores, CPCS total score, pain intensity, numb pain, soreness pain, pain self-efficacy, activity engagement, and pain willingness for pain acceptance were calculated. Missing data were excluded pair-wise in the Pearson correlation analyses. A p-value < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS and SPSS Amos (version 21.0; IBM Corp.). The current study’s data are not publicly available due to the funding contract. However, it is available via contacting the corresponding author if there is any need for the data or the study analysis code for research purposes.
Results
In total, 200 patients with chronic low back pain or neck pain were included in the study. All the patients responded to the demographic, pain duration, and intensity of pain surveys and the CPCS. However, 34 (17%) could not finish the PSEQ and 64 (32%) could not finish the CPAQ-8 because they had problems understanding the items or time limitations. Overall, 64.7%/60.9% of those who could not finish the PSEQ/CPAQ-8 had <9 years of formal education. The missing data were eliminated pair-wise in the Pearson correlation analysis.
Patients’ mean age was 64.84 ± 14.33, 126 (63.0%) were female, and 83 (41.5%) had 13+ years of education. The average duration of pain was 77.25 ± 97.46 months, average intensity of pain was 6.04 ± 2.50, Ma was 3.43 ± 3.24, and Sng was 4.54 ± 3.14. Descriptive and comparative statistics of the two groups are presented in Table 2. The chi-square test and t-test showed no significant differences in sex, education, age, and pain intensity between the group. Thus, the two groups could be treated as parallel samples.
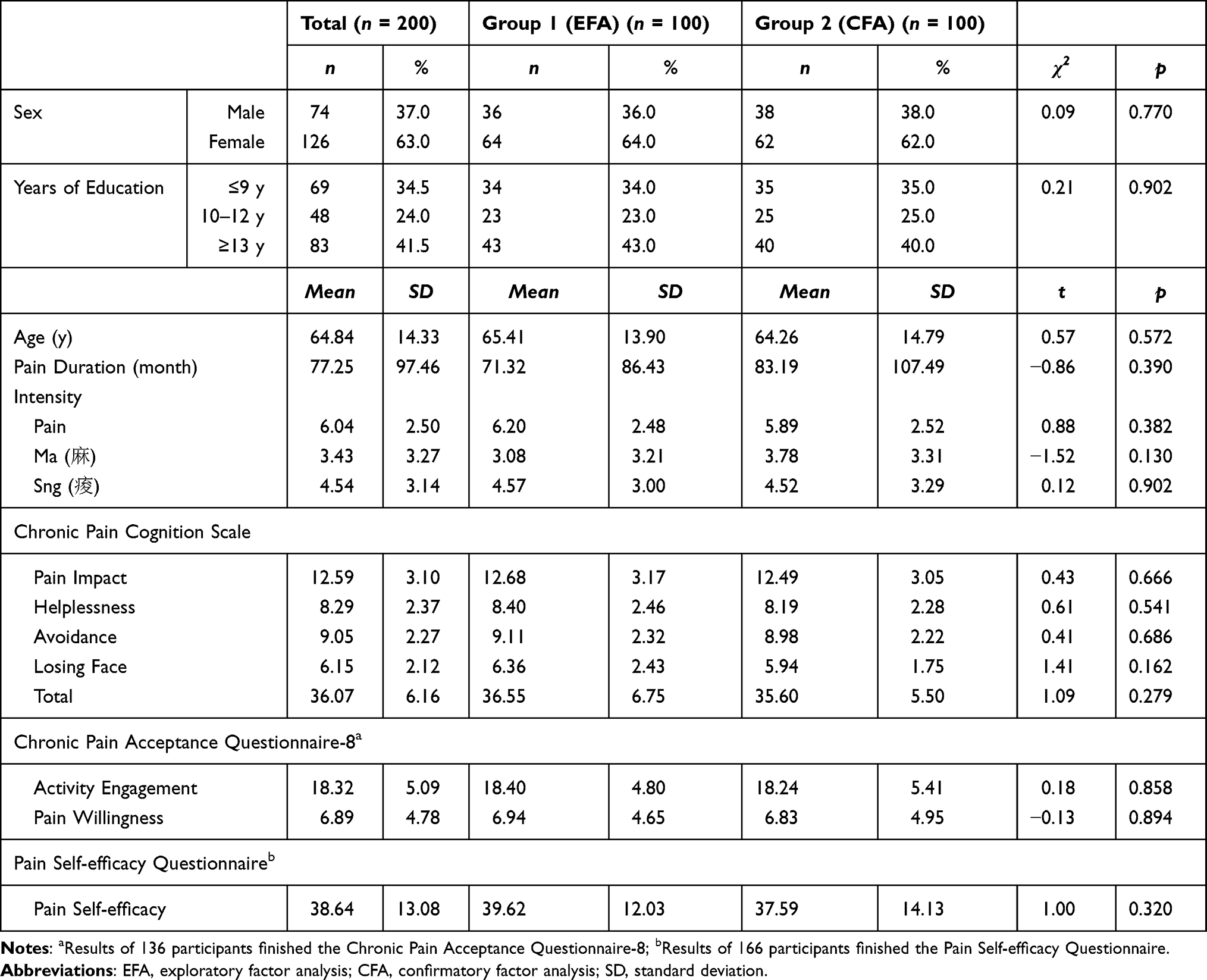 |
Table 2 Descriptive and Comparative Statistics on Demographic and Pain-Related Variables of the Groups |
First, item analysis was conducted. The means of the items ranged from 1.73 to 3.38, and the standard deviations ranged from 0.68 to 1.09. The skewness values ranged from 0.02 to 1.37, and kurtosis values ranged from −0.71 to 4.90. These results indicated that the data distribution of each item was acceptable (ie, skewness <3 and kurtosis <10)19 for further analysis.
The EFA results showed that the KMO test result was 0.73, and the Bartlett sphericity test result was significant, indicating that the data were suitable for EFA. The parallel analysis, scree test, and eigenvalues results suggested that the CPCS has a four-factor structure. The results of the factor structure, factor loadings, and internal consistency coefficients (Cronbach α) are listed in Table 1. The first factor, pain impact, included four items; the other three factors, losing face, helplessness, and avoidance, had three items. The reliability of the scale and four factors were examined. The Cronbach α of the full CPCS was 0.77, ranging from 0.60 to 0.81 for the four CPCS factors, which reflects a reasonable internal consistency of the CPCS.
CFA was used to examine the structural validity of the CPCS. The four-factor model of the EFA was used for model specification in CFA. Furthermore, the factor loading of pain impact on item 7 was set to 0.94, that of losing face on item 6 was set to 0.83, that of helplessness on item 4 was set to 0.87, and that of avoidance on item 2 was set to 0.79 to fix the scales. The estimation results on model fit showed a chi-square value of 85.08 (p =0.015), GFI of 0.89, CFI of 0.92, RMSEA of 0.07, and SRMR of 0.08, which represent good model fitness excluding the GFI. The modification indices suggested that the residuals of item 8 (medication affects my pain poorly) and item 11 (the reasons causing my pain are mainly related to myself) were correlated. After modification, the estimation results on model fit showed a chi-square value of 78.35 (p =0.039), GFI of 0.90, CFI of 0.94, RMSEA of 0.06, and SRMR of 0.07, all of which represent excellent model fitness. The estimated results of the standardized coefficients in CFA are shown in Figure 1. Factor loadings for each item by factor were significant.
 |
Figure 1 Estimated standardized coefficients in confirmatory factor analysis of the Chronic Pain Cognition Scale (CPCS). |
The Pearson correlation was used to evaluate the criterion-related validity (Table 3). The results showed that the pain impact factor was positively correlated with pain (r = 0.35) and Sng (r = 0.14) intensity, and negatively correlated with activity engagement (r = −0.22), pain willingness (r = −0.29), and pain self-efficacy (r = −0.41). The helplessness factor was positively correlated with pain (r = 0.37) and Sng (r = 0.16) intensity, and negatively correlated with activity engagement (r = −0.21) and pain self-efficacy (r = −0.24). The avoidance factor was negatively correlated with pain willingness (r = −0.28). The losing face factor was positively correlated with pain (r = 0.19), Ma (r = 0.15) and Sng (r = 0.16) intensities. The total CPCS score was positively correlated with pain (r = 0.39) and Sng (r = 0.18) intensity, and negatively correlated with activity engagement (r = −0.21), pain willingness (r = −0.30), and pain self-efficacy (r = −0.31).
 |
Table 3 Concurrent Criterion-Related Validity (Pearson Correlation) |
Discussion and Conclusion
The results showed that the CPCS has good reliability (ie, internal consistency) and validity and is suitable for evaluating chronic pain in clinical settings. The CPCS comprises four factors: pain impact, losing face, helplessness, and avoidance. This structure was first established by EFA and then verified by CFA with two randomly divided samples of patients with chronic pain; the findings indicated that the CPCS has satisfactory structural validity. Furthermore, all the factors and the full scale had reasonable internal consistency.
We examined two aspects of criterion-related validity. Regarding the discomforting sensations, the results indicated that the losing face factor is positively correlated with the intensity of pain, Ma, and Sng; and the pain impact and helplessness factors are positively correlated with pain and Sng. However, the avoidance factor had no significant correlations with these sensations. Concerning the cognitive aspect of pain, pain acceptance (including activity engagement and pain willingness) and pain self-efficacy were used as criteria. The results showed that pain impact was negatively correlated with activity engagement, pain willingness, and pain self-efficacy. The helplessness factor was negatively correlated with activity engagement and pain self-efficacy, and the avoidance factor was negatively correlated with pain willingness. Nevertheless, the losing face factor did not correlate with these cognitive indicators. These results suggested that pain impact and helplessness factors have good criterion-related validity. The findings regarding the losing face and avoidance factor were a little intriguing and will be discussed further.
Interestingly, the losing face factor was significantly related to all three discomforting sensations but not to pain acceptance or self-efficacy. Therefore, this result might reveal that the losing face is a culturally specific element that other pain measures cannot reflect. To clarify the phenomena, here are some expressions that many patients with chronic pain used to describe their pain experiences during the interview for generating the items for CPCS. For example, “I lose face if others see my awkward movement (due to the pain)”. “I only took painkillers when it was necessary. I lose face and it is embarrassing if others know I need drugs to maintain a normal life”. “I do not like to go out (after having chronic pain) because it is too hard to act normally in front of other people. I do not want to lose face”.
Furthermore, evaluating the losing face factor in pain might be essential not only in Taiwan, but also Chinese- / Chinese dialect-speaking (eg, Hong Kong Cantonese) populations. Firstly, the concepts of Ma and Sng exist in many Chinese dialects with similar pronunciations. Ma and Sng have common phonology in modern standard Chinese and sixteen dialects from Northern China (eg, Běijīng dialect) to Southern China (eg, Guǎngzhōu dialect).20 Secondly, a line of study in Chinese relationalism showed that having good connections with others is crucial in Chinese-speaking societies. Good connections are indicated by respect or acceptance; others are more willing to return or give face and favor.21 Lastly, the importance of face in the Chinese dialect-speaking population is also characterized by the national item selection of the Taiwanese version and the Hong Kong version of the brief World Health Organization Quality of Life (WHOQOL-BREF) questionnaire.22 The WHOQOL-BREF comprised 26 designated items and two national-specific items, and “being respected/ accepted” is included in both Hong Kong and Taiwan versions. The Hong Kong version’s national-specific item in the “being respected/accepted (關係Gwaan hai/ 面子Min zi)” facet is “Do you think people respect you”,22 and the direct translation of the Taiwanese national-specific item number 27 is “Do you feel having ‘face(面子)’ or being respected?”23 The item had a significant factor loading on the social domain, indicating that face is an indispensable factor in Taiwanese’s social quality of life.22 Thus, it seems sensible to include losing face as an essential factor in the CPCS.
Although losing face might be a specific cultural issue in Taiwanese or other Chinese-speaking populations with chronic pain, its social facet (ie, how others see me) might be a common issue in Asian (more collectivistic) cultures. For instance, a study found that Japanese people (resided in Japan) felt that pain behaviors were less acceptable than Euro-Americans (resided in the US with European descent). Thus, the Japanese were more unwilling to engage in expressive behaviors.24 Another study found that Singaporeans were less likely to seek social support and ask for assistance than Americans (90% Caucasian) were. The researchers explained that this might be because Singaporeans are more likely to perceive expressing pain as a sign of weakness.25 Thus, how one expresses, copes, and experiences differs from culture to culture. Further studies involving chronic patients with multi-culture samples are required to clarify these issues.
The avoidance factor was negatively correlated with pain willingness only. Because pain willingness refers to recognizing that avoidance is often unworkable to chronic pain, it is very reasonable that a higher avoidance score is related to lower pain willingness. Regardless, it is not expected that avoidance has no significant correlation with all discomforting sensations since many studies have found that pain intensity correlates with pain avoidance behaviors.26–28 However, a meta-analysis of fear avoidance and pain intensity revealed significant cultural variation. The researcher suggested that cultural norms and beliefs may affect the extent to which pain intensity is associated with fear avoidance.7 Thus, it is emphasized that we need to understand the function of avoidance behavior in different cultures to associate these coping strategies with patients’ cultural beliefs. In addition, it is necessary to better understand pain.
One of the limitations of this study is that it only involved patients with chronic low back or neck pain. Therefore, further studies targeting patients with different pain problems (eg, neuropathic pain and fibromyalgia) are needed to examine whether the CPCS is still a suitable measure in various clinical populations. Another limitation was the cross-sectional nature of this study. Hence, further longitudinal studies could help to better understand whether the CPCS could predict the future prognosis of patients with chronic pain. In sum, the CPCS has good psychometric properties and is suitable for evaluating chronic pain in the clinical setting in Taiwan and might be generalizable to other Chinese- / Chinese dialect-speaking populations including China, and other South-East counties. Future studies in different population are needed to further exam the generalizability of the CPCS.
Acknowledgments
We thank the participants and clinic staff for their contributions to the study.
Funding
This work was supported by the Ministry of Science and Technology, Taiwan (Reorganized as National Science and Technology Council, Taiwan in July 2022) [grant number MOST 105-2410-H-004-074, MOST 106-2410-H-004 −070 -SSS, and 110-2410-H-004-113-MY2] to the first author.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Merskey HE. Classification of chronic pain: descriptions of chronic pain syndromes and definitions of pain terms. PAIN. 1986;3(Suppl.):216–221.
2. International Association for the Study of Pain (IASP). IASP Announces Revised Definition of Pain; 2020. Available from: https://www.iasp-pain.org/PublicationsNews/NewsDetail.aspx?ItemNumber=10475.
3. Khalatbari-Soltani S, Blyth FM. Socioeconomic position and pain: a topical review. PAIN. 2022;16310:1855–1861. doi:10.1097/j.pain.0000000000002634
4. Rahim-Williams B, Riley JL, Williams AKK, Fillingim RB. A quantitative review of ethnic group differences in experimental pain response: do biology, psychology, and culture matter? Pain Med. 2012;134:522–540. doi:10.1111/j.1526-4637.2012.01336.x
5. Campbell CM, Edwards RR. Ethnic differences in pain and pain management. Pain Manag. 2012;23:219–230. doi:10.2217/pmt.12.7
6. Orhan C, Van Looveren E, Cagnie B, Mukhtar NB, Lenoir D, Meeus M. Are pain beliefs, cognitions, and behaviors influenced by race, ethnicity, and culture in patients with chronic musculoskeletal pain: a systematic review. Pain Physician. 2018;216:541–558.
7. Kroska EB. A meta-analysis of fear-avoidance and pain intensity: the paradox of chronic pain. Scand J Pain. 2016;13:43–58. doi:10.1016/j.sjpain.2016.06.011
8. Morales ME, Yong RJ. Racial and ethnic disparities in the treatment of chronic pain. Pain Med. 2020;221:75–90. doi:10.1093/pm/pnaa427
9. Narayan MC. Culture’s effects on pain assessment and management. Am J Nurs. 2010;1104:38–47. doi:10.1097/01.naj.0000370157.33223.6d
10. Tait RC, Chibnall JT. Racial/ethnic disparities in the assessment and treatment of pain: psychosocial perspectives. Am Psychol. 2014;692:131. doi:10.1037/a0035204
11. Melzack R. The McGill Pain Questionnaire: major properties and scoring methods. PAIN. 1975;13:277–299. doi:10.1016/0304-3959(75)90044-5
12. Lin JH, Hung CH, Han DS, et al. Sensing acidosis: nociception or sngception? J Biomed Sci. 2018;251. doi:10.1186/s12929-018-0486-5
13. Chang KV, Hung CH, Sun WZ, et al. Evaluating soreness symptoms of fibromyalgia: establishment and validation of the revised fibromyalgia impact questionnaire with integration of soreness assessment. J Formos Med Assoc. 2020;1197:1211–1218. doi:10.1016/j.jfma.2019.10.018
14. Stanford Pain Management Center. New patient questionnaire. Available from: https://stanfordhealthcare.org/content/dam/SHC/for-patients-component/pain-management/docs/new-patient-questionnaire.pdf.
15. Fish RA, McGuire B, Hogan M, Morrison TG, Stewart I. Validation of the Chronic Pain Acceptance Questionnaire (CPAQ) in an Internet sample and development and preliminary validation of the CPAQ-8. PAIN. 2010;1493:435–443. doi:10.1016/j.pain.2009.12.016
16. Nicholas MK. The pain self‐efficacy questionnaire: taking pain into account. Eur J Pain. 2007;112:153–163. doi:10.1016/j.ejpain.2005.12.008
17. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling. 1999;61:1–55. doi:10.1080/10705519909540118
18. Kline RB. Global Fit Testing. In: Principles and Practice of Structural Equation Modeling. New York: The Guilford Press; 2015:262–299.
19. Kline RB. Data Preparation and Psychometrics Review. In: Principles and Practice of Structural Equation Modeling. NY: The Guilford Press; 2015:64–96.
20. Gu Q, Simmons RV. Common Phonology of the Chinese Dialects. Singapore: Springer; 2020.
21. Hwang KK. Face and favor: the Chinese power game. Am J Sociol. 1987;92:944–974. doi:10.1086/228588
22. Yao G, Wu CH. Similarities and Differences Among the Taiwan, China, and Hong-Kong Versions of the WHOQOL Questionnaire. Soc Indic Res. 2009;91:79–98. doi:10.1007/s11205-008-9326-4
23. Yao G, Chung CW, Yu CF, Wang JD. Development and verification of validity and reliability of the WHOQOL-BREF Taiwan version. J Formos Med Assoc. 2002;1015:342–351.
24. Hobara M. Beliefs about appropriate pain behavior: cross-cultural and sex differences between Japanese and Euro-Americans. Eur J Pain. 2005;94:389. doi:10.1016/j.ejpain.2004.09.006
25. Thong ISK, Tan G, Lee TYC, Jensen MP. A comparison of pain beliefs and coping strategies and their association with chronic pain adjustment between Singapore and United States. Pain Med. 2017;18:1668–1678. doi:10.1093/pm/pnw237
26. Cho SK, Heiby EM, McCracken LM, Moon DE, Lee JH. Daily functioning in chronic pain: study of structural relations with posttraumatic stress disorder symptoms, pain intensity, and pain avoidance. Korean J Pain. 2011;241:13–21. doi:10.3344/kjp.2011.24.1.13
27. Cui J, Matsushima E, Aso K, Masuda A, Makita K. Psychological features and coping styles in patients with chronic pain. Psychiatry Clin Neurosci. 2009;632:147–152. doi:10.1111/j.1440-1819.2009.01934.x
28. Martinez-Calderon J, Flores-Cortes M, Morales-Asencio JM, Luque-Suarez A. Pain-related fear, pain intensity and function in individuals with chronic musculoskeletal pain: a systematic review and meta-analysis. J Pain. 2019;2012:1394–1415. doi:10.1016/j.jpain.2019.04.009
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Assessing the Genetic Causal Effects Between Blood Metabolites and Spinal Pain: A Bidirectional Two-Sample Mendelian Randomization Study
Wu S, Zhou XC, Li T, Sun JY, Chen LH, Wei ZC, Wang KZ, Hong SW, Xu HN, Lv ZZ, Lv LJ
Journal of Pain Research 2024, 17:3897-3918
Published Date: 20 November 2024