Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Development of an Electronic Interdisciplinary Chronic Obstructive Pulmonary Disease (COPD) Proforma (E-ICP) to Improve Interdisciplinary Guideline Adherence in the Emergency Department: Modified Delphi Study
Authors Issac H ![]() , Keijzers G, Yang IA, Lea J, Taylor M
, Keijzers G, Yang IA, Lea J, Taylor M ![]() , Moloney C
, Moloney C
Received 13 January 2022
Accepted for publication 11 April 2022
Published 6 May 2022 Volume 2022:17 Pages 1089—1106
DOI https://doi.org/10.2147/COPD.S358254
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Hancy Issac,1,2 Gerben Keijzers,3– 5 Ian A Yang,6,7 Jackie Lea,1,2 Melissa Taylor,1,2 Clint Moloney1,8,9
1School of Nursing and Midwifery, University of Southern Queensland, Toowoomba, QLD, Australia; 2Centre of Health Research, University of Southern Queensland, Toowoomba, QLD, Australia; 3Department of Emergency Medicine, Gold Coast University Hospital, Gold Coast, QLD, Australia; 4Faculty of Health Sciences and Medicine, Bond University, Gold Coast, QLD, Australia; 5School of Medicine, Griffith University, Gold Coast, QLD, Australia; 6Thoracic Medicine, The Prince Charles Hospital, Brisbane, QLD, Australia; 7Faculty of Medicine, The University of Queensland, Brisbane, QLD, Australia; 8College of Health and Biomedicine, Nursing and Midwifery, Victoria University, Melbourne, VIC, Australia; 9Institute for Health and Sport, Victoria University, Melbourne, VIC, Australia
Correspondence: Hancy Issac, School of Nursing and Midwifery, University of Southern Queensland, Toowoomba, QLD, Australia, Email [email protected]
Introduction: Chronic obstructive pulmonary disease guideline non-adherence is associated with a reduction in health-related quality of life in patients (HRQoL). Improving guideline adherence has the potential to mitigate fragmented care thereby sustaining pulmonary function, preventing acute exacerbations, reducing economic health burdens, and enhancing HRQoL. The development of an electronic proforma stemming from expert consensus, including digital guideline resources and direct interdisciplinary referrals is hypothesised to improve guideline adherence and patient outcomes for emergency department (ED) patients with COPD.
Aim: The aim of this study was to develop consensus among ED and respiratory staff for the correct composition of a COPD electronic proforma that aids in guideline adherence and management in the ED.
Methods: This study adopted a mixed-method design to develop the most important indicators of care in the ED. The study involved three phases: (1) a systematic literature review and qualitative interdisciplinary staff interviews to assess barriers and solutions for guideline adherence and qualitative interdisciplinary staff interviews, (2) a modified Delphi panel to select interventions for the proforma, and (3) a consensus process through three rounds of scoring through a quantitative survey (ED and Respiratory consensus) and qualitative thematic analysis on each indicator.
Results: The electronic proforma achieved acceptable and good internal consistency through all iterations from national emergency department and respiratory department interdisciplinary experts. Cronbach’s alpha score for internal consistency (α) in iteration 1 emergency department cohort (EDC) (α = 0.80 [CI = 0.89%]), respiratory department cohort (RDC) (α = 0.95 [CI = 0.98%]). Iteration 2 reported EDC (α = 0.85 [CI = 0.97%]) and RDC (α = 0.86 [CI = 0.97%]). Iteration 3 revealed EDC (α = 0.73 [CI = 0.91%]) and RDC (α = 0.86 [CI = 0.95%]), respectively.
Conclusion: Electronic proformas have the potential to facilitate direct referrals from the ED leading to reduced hospital admissions, reduced length of hospital stays, holistic care, improved health care and quality of life and improved interdisciplinary guideline adherence.
Keywords: COPD, electronic proforma, modified Delphi study, interdisciplinary, guideline adherence, COPD-X plan
Introduction
Chronic obstructive pulmonary disease exacerbations are the leading cause of unplanned hospital admissions worldwide.1 COPD is the second leading cause of avoidable Australian hospital admissions.2 Preventing COPD readmissions following an exacerbation has been identified as an international priority to sustain pulmonary function, reduce economic health burdens and improve health-related quality of life with COPD patients.1 The World Health Organization has predicted COPD to become the third leading cause of death by 2030 considering its recent increase in prevalence and morbidity.2,3 Australasian research reports that 5% of all emergency department (ED) presentations include shortness of breath and 14% of these presentations were diagnosed with COPD.4 An exploratory systematic review and interdisciplinary qualitative reviews revealed contributing factors towards guideline non-adherence to be decreased awareness, lack of familiarity, lack of knowledge of referral process, role confusion, lack of interdisciplinary communication and a lack of cues/guidelines in the working environment.5,6 Economic data from an Australian review of three major tertiary hospitals revealed a total annual health service cost of 20 million AUD for ED presentations across three major health service districts.7 That study reported that 41.1% of ED presentations assessed as Australian Triage Scale category 3 (urgent) or 4 (semi-urgent) were discharged home on the same day.7 A lack of integrated care and discharge planning from the ED is associated with COPD readmissions and exacerbations resulting in breathlessness, reduced activity levels, malnutrition, social isolation, a loss of independence, and depression which all lead to a reduced health-related quality of life (HRQoL).8–13
The main research aim is to develop a proforma for implementation in the ED to improve guideline adherence and the secondary aim and potential benefit is holistic primary-care referrals, and reduced hospital admissions to ED. An electronic proforma has the potential to serve as a pragmatic implementation research initiative specifically focussed on the needs of ED interdisciplinary staff.14,15 Challenges in the acute clinical setting include a lack of a single integrated platform, supporting infrastructure, interdisciplinary staff capacity, lack of clinician training and support for under-confident clinicians to use digital devices, and a lack of critical information at point of care.13,16,17 An electronic proforma acquires the desired capabilities if integrated with an existing electronic medical record to reduce interdisciplinary staff cognitive burden, and in the provision of consistent information through guidelines, consistent patient resources and information, integration of clinical data and decision making at point of care, one-step referrals within outpatient clinics and primary care, as well as consistent staff training.18–20 Developing relevant ED-focussed quality indicators have been noted as important in improving care outcomes.7,13,21 Appropriate delegation and handover of chronic care referrals potentially can reduce ED COPD readmissions and improve HRQoL for these patients.7,15 This study aimed to develop a proforma for ED departments to improve guideline adherence amongst ED interdisciplinary clinicians. The imperative perspective here is from ED interdisciplinary staff verified and validated by respiratory interdisciplinary staff.
Methods
A modified Delphi approach has been recognised as a valid and pivotal approach to understanding departmental-based needs, with this research involving respiratory and ED interdisciplinary clinicians.22–24 This process has aided in achieving the aim of gaining consensus on the indicators and feasibility of electronic COPD guideline recommendations embedded in intranet systems specifically in the ED. Ethics was approved at the University of Southern Queensland (H21REA007). All participants were provided with a research participation information sheet and consent obtained prior to each iteration completion.
This modified Delphi approach used a mixed-method design utilising quantitative survey questions and qualitative thematic analysis to develop a COPD proforma with specific clinical-driven content for ED. Most important indicators of care in the ED were selected (a set of evidence-based interventions applied to improve clinical outcomes) involving three phases: (1) a systematic literature review to assess barriers and solutions for guideline adherence,25 (2) a modified Delphi panel to select interventions for the bundle, and (3) consensus process through three rounds of scoring quantitative survey and qualitative thematic analysis on each indicator (see Figure 1). An E-Delphi technique appeared to be the most suitable method to gain consensus among emergency department and respiratory department interdisciplinary experts to develop and determine content validity and realistic implementation probability of the E-ICP considering the primary aim was to increase guideline adherence utilising E-ICP.23 The protocol for methods and stages of each iteration of this study is published elsewhere.26 A national panel of experts was created by utilising systematic review authorship. Participants were recognised from systematic review authorship and had an established academic profile in COPD research practice and/or were recognised by expert clinicians through peer referral as a COPD clinician expert or ED speciality interdisciplinary staff A modified Delphi method or E-Delphi method where all iterations are administered online was conducted with quasi anonymity. The respondents did not know each other, however the research team was not blinded of participant responses. Anonymity assisted participants and stakeholders from different disciplines, organisations, and career stages to provide input without domination between ED and respiratory experts to develop E-ICP for ED. In round one, a panel of experts were asked to rate the importance of care indicators and provide additional suggestions for revisions or new items. Consensus was considered reached if at least 70% of the panel strongly agreed that an item should be included or excluded from the proforma. Where agreement was not reached or there were suggestions for altered or new items, these were taken to round two together with an aggregated summary of round one responses. Following the second round, a ranking of indicators was developed, and the final template distributed to panel members for approval. The E-Delphi process facilitates easier accessibility of experts, timely and confidential panel responses, and ease in dissemination of information from previous rounds.
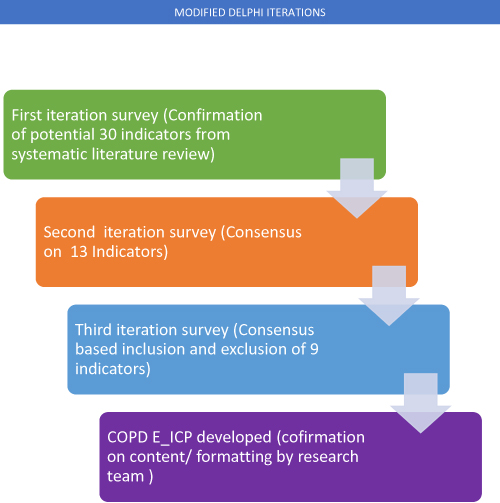 |
Figure 1 Graphical representation of modified Delphi iterations and processes from systematic review phase for identification of indicators to final development of E-ICP. |
The exploratory phase of the research included a systematic literature review to identify barriers and indicators to develop the first iteration of the Delphi questionnaire. A comprehensive three-tier search strategy was utilised to search nine databases (COCHRANE, EBSCO HOST, MEDLINE, SCIENCE DIRECT, JBI, SCOPUS, WEB OF SCIENCE, WILEY and DARE) in May 2020.6 This protocol was also published elsewhere.6 We included all articles that reported on international guideline adherence (GOLD) and national guideline adherence (COPD-X plan) within the last decade. The literature proposed 30 indicators as potential barriers and probable solutions to COPD guideline concordance. These indicators were included in the survey questionnaire to understand the level of agreement between interdisciplinary clinicians (see Table 1).
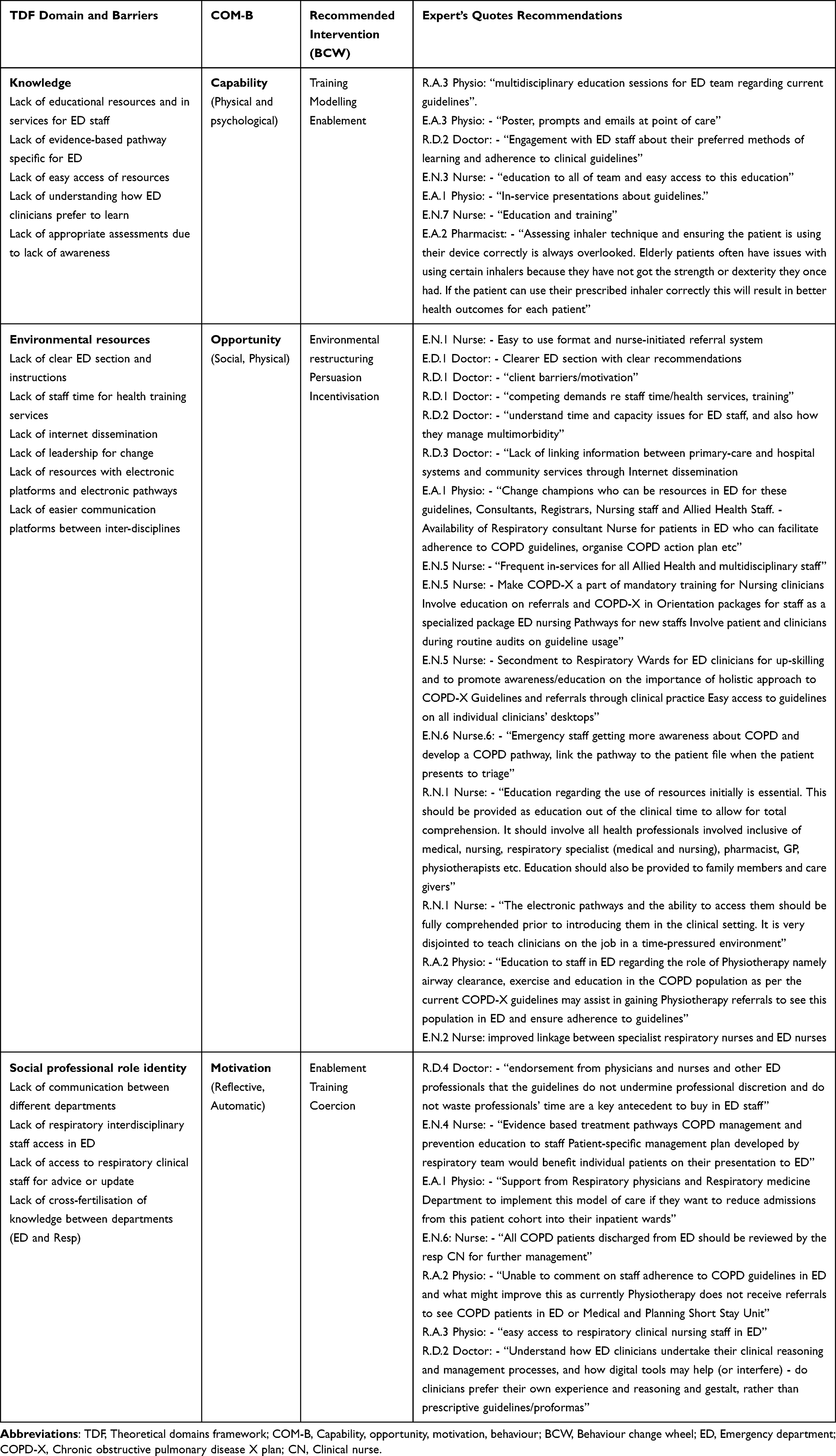 |
Table 1 Qualitative Thematic Analysis of Expert Quotes to TDF Domains and BCW |
Results
Iteration 1
Qualitative thematic analysis of iteration 1 confirmed the barriers and inscribed potential solutions to improve the proforma content (see Table 1). Theoretical domains framework (TDF) domains are bracketed throughout the Results section for clarity along with Table 1. Interdisciplinary staff expressed a preferred method of learning that must be discussed with staff and embedded to their educational resources through ED orientation packages, posters, electronic prompts, in-service education, electronic self-learning modules, as well as easy access to resources at point of care digital platforms (knowledge). A respiratory team cross-fertilisation of knowledge and collaboration plan with ED clinicians to initiate patient-specific management plans, evidence-based treatment pathways and electronically linking the plan to the patient file when the patient presents to triage were some suggested resolutions (knowledge, environmental context and resources, social/professional role identity). Patient or care-giver education on inhaler technique is indispensable for COPD patients discharged from the ED especially if age, strength, or dexterity is affected (knowledge). Lack of linking patient baseline pulmonary function information from primary care, lack of intranet dissemination of guidelines with specific sections for ED care have a substantial role in low guideline adherence (environmental context and resources). Lack of professional role clarity, interdepartmental communication and access to respiratory clinical nurses or specialists in ED subsequently causes patient discharges with inadequate community support or unwanted hospital admission for multidisciplinary care (social/professional role identity, environmental context, and resources).
Consensus above 80% existed on barriers such as lack of point of care resources (87.2%), lack of time (85.2%), lack of clarity on referral points (ED or inpatient units or GP) (84.2%) and lack of functional care pathways (81.4%) (see Table 2). Each of these considerably contributed to guideline non-concordance. High consensus also existed on prospective solutions where the electronic proforma can provide transfer of knowledge through discharge templates and other COPD educational resources (80%), time-efficient processes of care (87.2%), assisting with evaluation audits and future research to target areas of improvement (87.2%), consistent pharmacological management (85.8%), automatic electronic linkage between hospital and community COPD services will reduce ED utilisation time (88.6%). Simple preformatted order sets (proforma) integrated into the electronic health record platforms (85.2%) were identified to enhance guideline adherence in the ED acting as an educational aid to clinicians (82.8%), interdisciplinary staff and patients. Respiratory clinical nurses consulting with patients in ED to provide referrals and supportive community management highlight key outcomes in reducing length of stay, readmissions, and remissions to inpatient departments (82.8%).
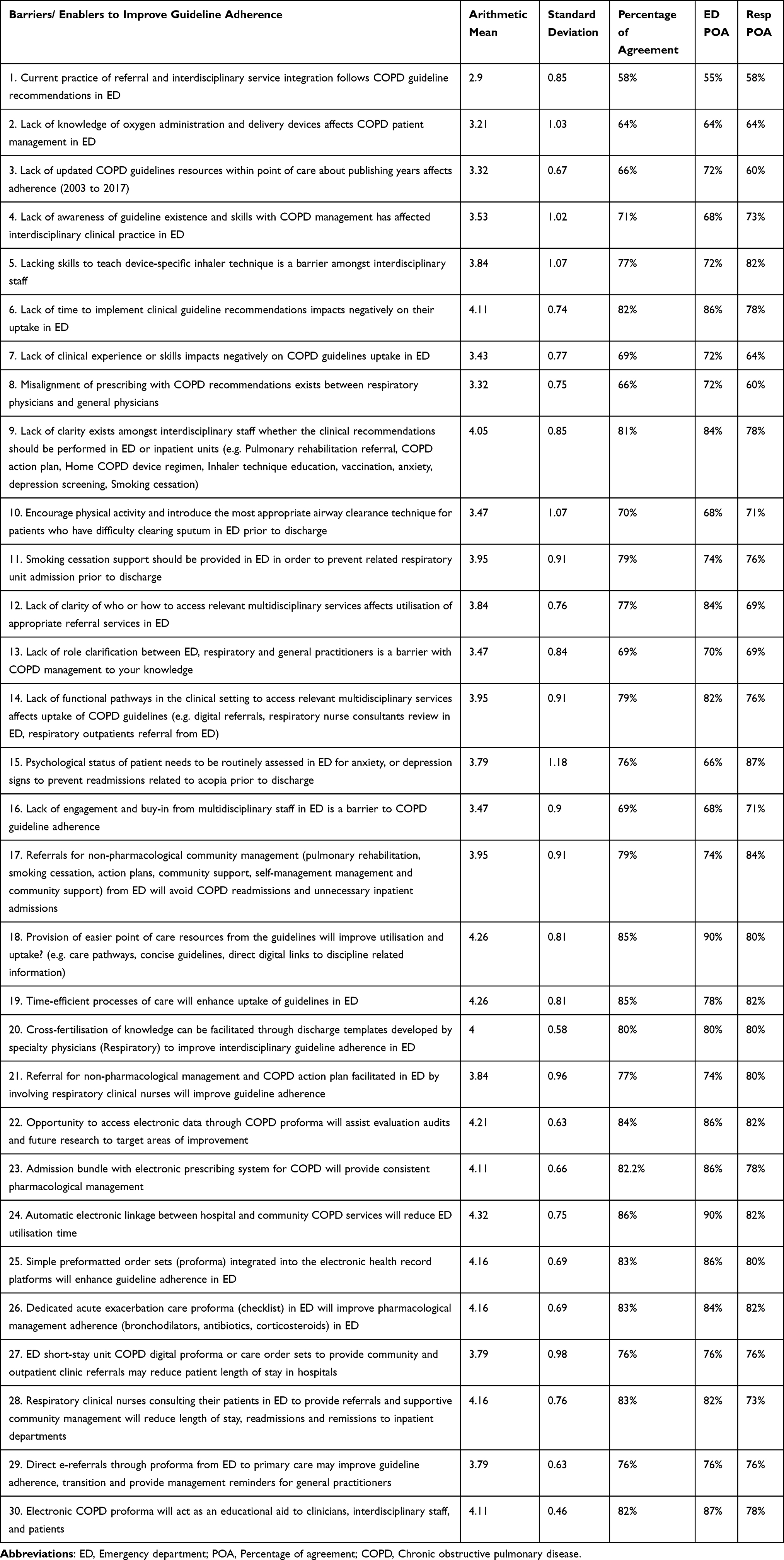 |
Table 2 Iteration 1 Results |
Prominent barriers that aggregated 70–80% expert consensus are lack of smoking cessation support (77.2%) in ED, role clarification between interdepartmental practitioners (74.2%), clarity on how to access relevant multidisciplinary services (75.8%), engagement and buy-in from multidisciplinary staff, clinical experience (70%), lack of respiratory skills (75.8%), and inaccurate prescription(s) (70%). Potential solutions with expert consensus of >70% included referrals for non-pharmacological community management from the ED, short-stay ED unit COPD digital proforma or care order sets to provide community and outpatient clinic referrals to reduce patient length of stay and avoid hospital admissions. Direct e-referrals through the proforma from the ED to primary care has prospects to improve guideline adherence, care transition, and provide clinical management reminders for general practitioners. Referral for non-pharmacological management and COPD action plan development or review facilitated in the ED has worth by involving respiratory clinical nurses. These nurses will facilitate consistent referrals and holistic care from acute settings back to the community.
Consensus below 70%, experts ranked and excluded were lack of knowledge (67.2%), awareness (68.6%), lack of resources based on publishing/updated years as reasons contributing to non-adherence (68.6%), and physiotherapy for sputum clearance in the ED (68.6%). Consistent agreement existed between the ED interdisciplinary staff for the specific ED section with clear recommendations of management, considering staff time/health services training time, ED staffing and capacity issues to manage co-morbidities being the key to improve guideline adherence in ED. Link information and internet dissemination possibilities between primary-care and hospital systems and community services exploration and implementation could potentially assist elevating guideline adherence. Clinicians and other interdisciplinary staff require to be informed how digital tools may assist and prescriptive guidelines and resources to utilise if necessary, while this does not affect their own clinical reasoning and gestalt. Easy guideline referrals through clinician desktops and clinicians actively being involved in routine audits have potential to improve adherence.
Nursing and allied health experts recommended a user-friendly nurse-initiated referral system, improved electronic linkage between respiratory nurses and emergency department nurses and engagement with ED staff about their preferred methods of learning or adherence to clinical guidelines. Interdisciplinary education to all teams and easy access to this education, evidence-based treatment pathways for COPD management/prevention, mandatory training for ED nursing staff during orientation, education on referrals in nursing orientation packages were some implementation initiatives suggested by ED interdisciplinary staff. Increasing awareness among emergency staff on COPD pathway and linking the pathway to the patients when they present to triage followed by mandatory respiratory clinical nurse review or referral for further management will explicitly reduce chances of defragmented care for this cohort of patients when discharged from ED. Psychology and allied health experts (physiotherapist, pharmacist, and occupational therapist) suggested endorsement from physicians and nurses and other ED professionals that the guidelines do not undermine professional discretion and do not waste professionals’ time are a key antecedent to buy-in from physicians, nurses, and other ED professionals. Frequent in-services for all allied health and multidisciplinary staff, with education outside clinical duty time to allow total comprehension is pivotal. Family and care-givers self-management and support modules with resources that clinicians could hand out on discharge will be an additional benefit to this cohort of patients and staff.
Iteration 2
Iteration 2 formed 13 indicators from iteration 1 and COPD X plan recommendations comprised the first draft of the electronic proforma (see Supplementary File 1). Qualitative analysis comprised three TDF domains (see Table 3). Multiple ED interdisciplinary staff voiced concerns regarding referral requirements from ED being too onerous and time consuming and the need for a single point of contact referral identified (Environmental context and resources). Explicitly both ED and respiratory staff agree that inhaler technique requires checking prior to discharge as this potentially becomes the most immediate reason for readmission with COPD patients (knowledge). All other referrals may be followed up in outpatient’s clinic or community referrals may be provided by respiratory clinical nurse consultant (RCNC) as single point of ED referral facilitating registering ED discharges within the system (environmental context and resources and social/professional role identity). ED interdisciplinary staff implored mandatory RCNC review as a single point of contact could assist in accelerating guideline utilisation and community referrals for patients discharged from ED. Patients do not have to wait in the ED if they are well enough to be discharged, however, they must be admitted for multidisciplinary referral with mandatory RCNC referral for ED discharges (social/professional role identity). RCNC referrals from the ED will capture this cohort (ED discharges) in the system for later date follow-up or facilitation of community referrals. Inclusion of the integrated electronic medical records (ieMR) into hospital systems mean the possibility of direct referrals to primary care through ieMR smart referrals may be possible in the near future.27 This is an area where future research is required on specific integration with primary-care partners.
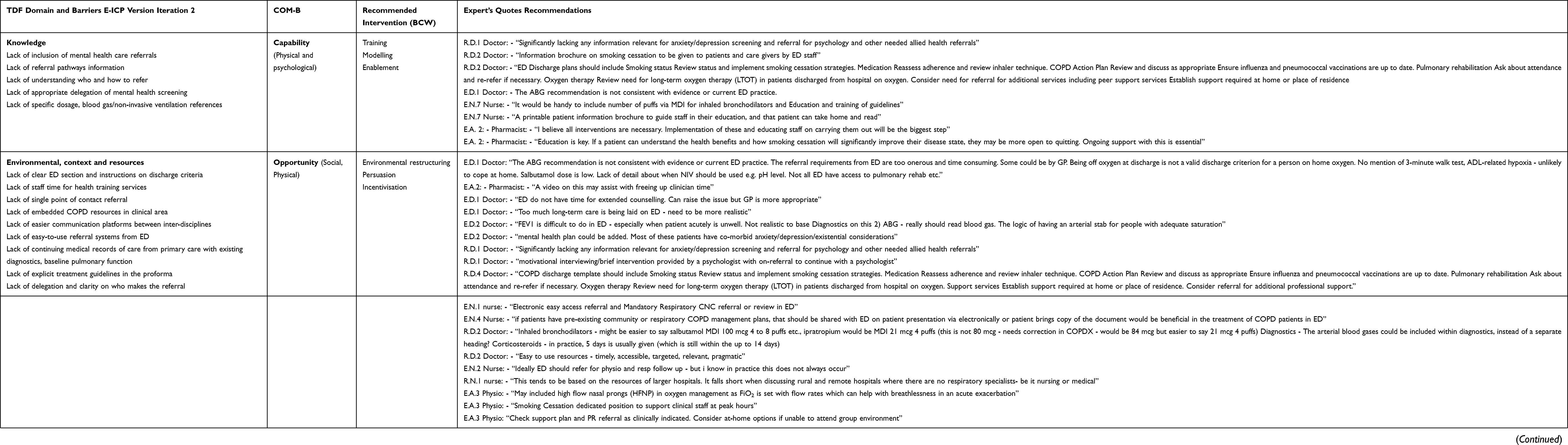 |
Table 3 Iteration 2 Qualitative Responses to TDF Domain and BCW |
Cronbach’s alpha score for inter-rater reliability overall was 0.86 (ED: 0.85), Resp: 0.86) (see Table 4). High consensus indicators to be performed prior to ED discharge included respiratory nurse referral (Respiratory department consensus (RDC): 90%, Emergency department consensus (EDC): 84%), ED interdisciplinary staff (Doctors/Nurses/Physios/Pharmacist) inhaler technique assessment (EDC: 86%, RDC: 92.5%). ED discharge criteria (EDC: 86%, RDC: 85%) and community nurse or pharmacist referral for community medications and inhaler technique review (EDC: 75.5% and RDC: 85%) scored high consensus as this is an area mostly reported with fragmented care. This version significantly lacked mental health screening and assessments in the ED or any information relevant for anxiety/depression screening and referral for psychology and other needed allied health referrals as most of these patients have co-morbid anxiety/depression/existential considerations (knowledge). ED staff raised 75% consensus on having proforma accurately based on their discipline and requirements. ED discharge criteria consensus comprised clinical stability indicators revealing consistent consensus between both departments. Moderate consensus above 70% included community pharmacist or community respiratory nurse referral to check inhaler technique prior to ED discharge (EDC: 75.5%, RDC: 85%). Further clarity for the next iteration was requested by experts on reiterating guideline references for ABG, NIV, corticosteroid doses, and bronchodilator doses.
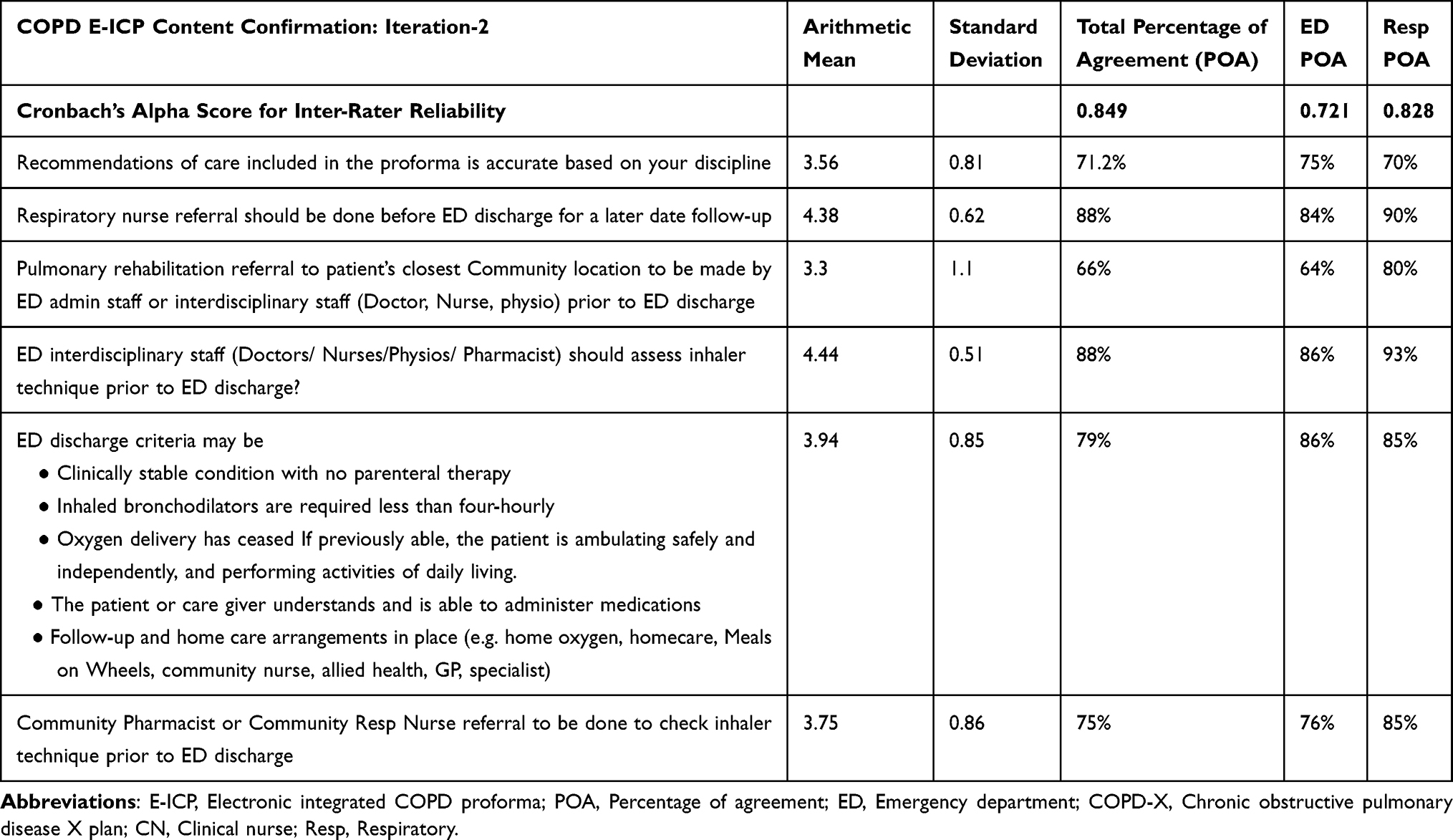 |
Table 4 Ed E-ICP Development Survey Iteration 2 Quantitative Responses |
The results indicated implementation initiatives should be timely, accessible, targeted, relevant, and pragmatic. A smoking cessation dedicated position to support clinical staff at peak hours, if patients have pre-existing community or respiratory COPD management plans was included and shared with the ED on patient presentation either electronically or the patient bringing a copy of the document would be beneficial in the treatment of COPD patients in ED (environmental context and resources). Implementation of these and educating staff on procedural requirements will be the biggest step. This includes checking on interdisciplinary staff motivation and knowledge (self-learning modules). Ongoing support and videos for patient education may assist with freeing up clinician time (videos or self-learning modules for patients) (knowledge and environmental context and resources). Education and training for the COPD checklist (online), In services and self-learning modules/with refreshers potentially provided through the electronic proforma for all interdisciplinary staff (environmental context and resources). The discharge summary ideally should mention reconsideration of additional allied health referrals and reasons for this action plan, smoking cessation activities and liaison, vaccinations and pulmonary rehabilitation. Environmental barriers such as a lack of access to pulmonary rehabilitation, rural and remote hospitals where there are no respiratory specialists be it nursing or medical was raised by experts. Electronic proforma implementation was not always possible in rural and remote areas, however eventually we are moving towards a digital health-care industry (environmental context and resources).
Iteration 3
Qualitative thematic analysis imposed several themes such as forced expiratory volume (FEV1) referred to being driving investigations is not appropriate as almost universally not done/available in ED (environmental context and resources) (see Table 5). Performing FEV1 being difficult, and the accuracy of this step was questioned by experts to be performed in ED (environmental context and resources). Consensus existed between ED and respiratory clinicians that patients who still have an exacerbation or too unwell for spirometry do not require FEV1 performed in the ED, besides many EDs do not have functioning, well-calibrated spirometers. In the context of the modified Medical Research Council (mMRC) Scale not being relevant to ED as it does not address change in function from baseline during the exacerbation, consensus existed amongst both departments that mMRC may be utilised for assessment of breathlessness for initial assessment of severity, and then long-term management as an alternative in the absence of FEV1 data. ED clinicians expressed concern regarding justification for arterial blood gas (ABG) if venous blood gas (VBG) shows normal PH to which respiratory clinicians responded that ABG is not required unless chronic hypercapnia is suspected. High consensus existed between interdisciplinary staff that it would be beneficial if chronic COPD patients presenting to EDs carry some form of documentation mentioning their baseline lung function, FEV1, CO2 retaining status, pressures normally used for NIV etc. as this would be beneficial for patients who are new or do not have any clear documentation (knowledge/social/professional role identity).
 |
Table 5 Qualitative Responses to TDF Domains Iteration 3 |
Iteration 3 comprised 9 indicators from the previous iterations of 13 indicators after exclusion of indicators that obtained less than 70% consensus (see Supplementary File 2). This iteration revealed Cronbach’s alpha score EDC (α = 0.73 [CI = 0.91%]) and RDC (α = 0.86 [CI = 0.95%]) (seeTable 6). Consensus >80% was achieved on bronchodilator doses (88%), corticosteroid doses (84%), NIV blood gas indicator references (84%), inhaler technique check prior to ED discharge (92%), respiratory CNC referral for community or outpatient’s non-pharmacological management as single point of contact (EDC: 86% and RDC: 87%). Addition of high flow nasal prong therapy (HFNP) received consensus of 79% whilst other indicators that acquired consensus between 70–80% were modified Medical Research Council (mMRC) Dyspnoea Scale utility in the absence of FEV1 spirometry, ABG to be considered if VBG pH ≤7.34 in ED, patient self-learning videos (e.g., inhaler technique) to assist education in ED utilising digital resources. CAT mental health screening tool was highly recommended compared with other tools such as SGRQ questionnaire and HADS even though COPD-X plan suggests the latter. Low consensus below 70% and excluded indicators are Three minutes or Six minutes’ walk test prior to discharge. All these changes were addressed in the final iteration of the proforma (see Figure 2).
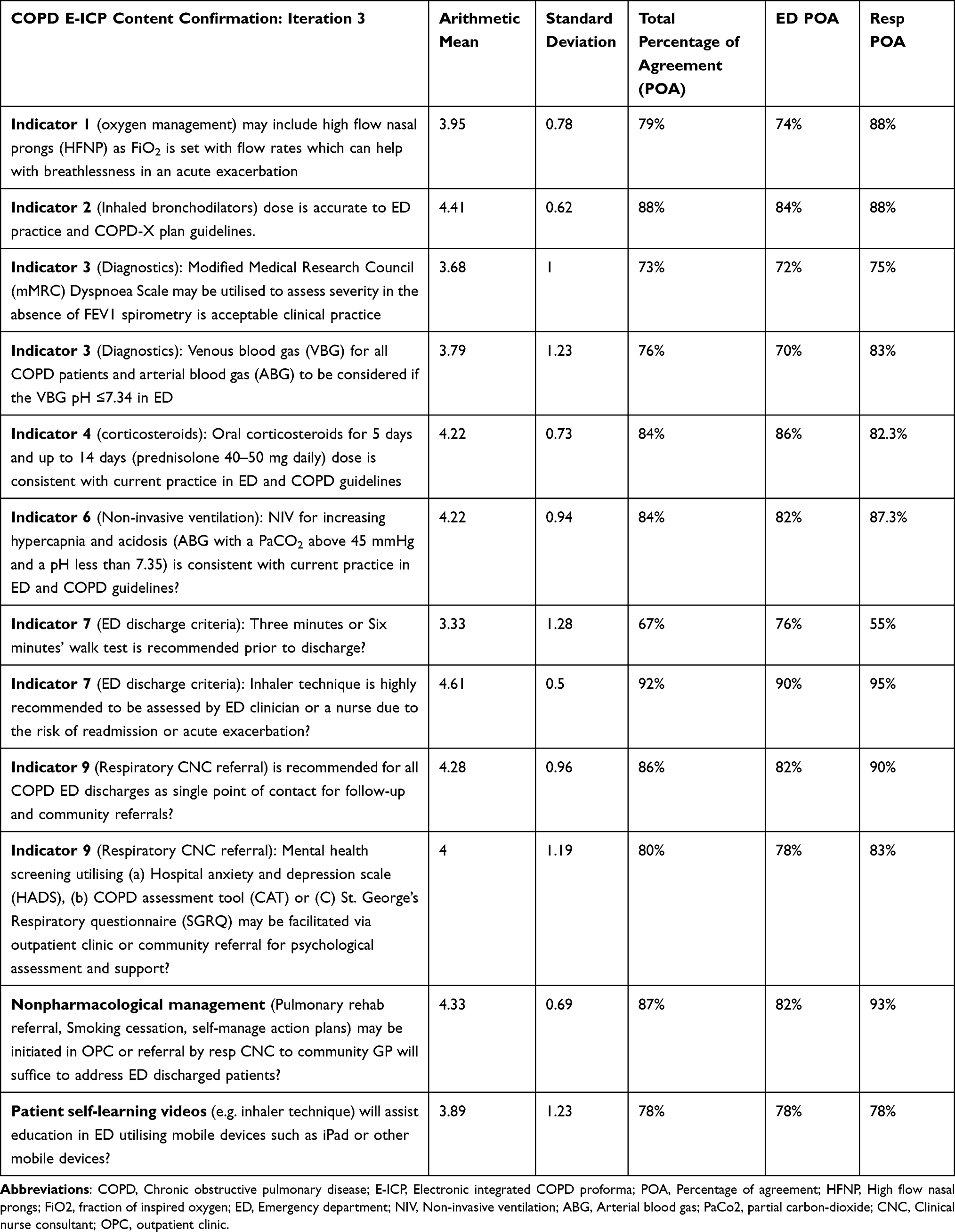 |
Table 6 E-ICP Development Results Summary Iteration 3 |
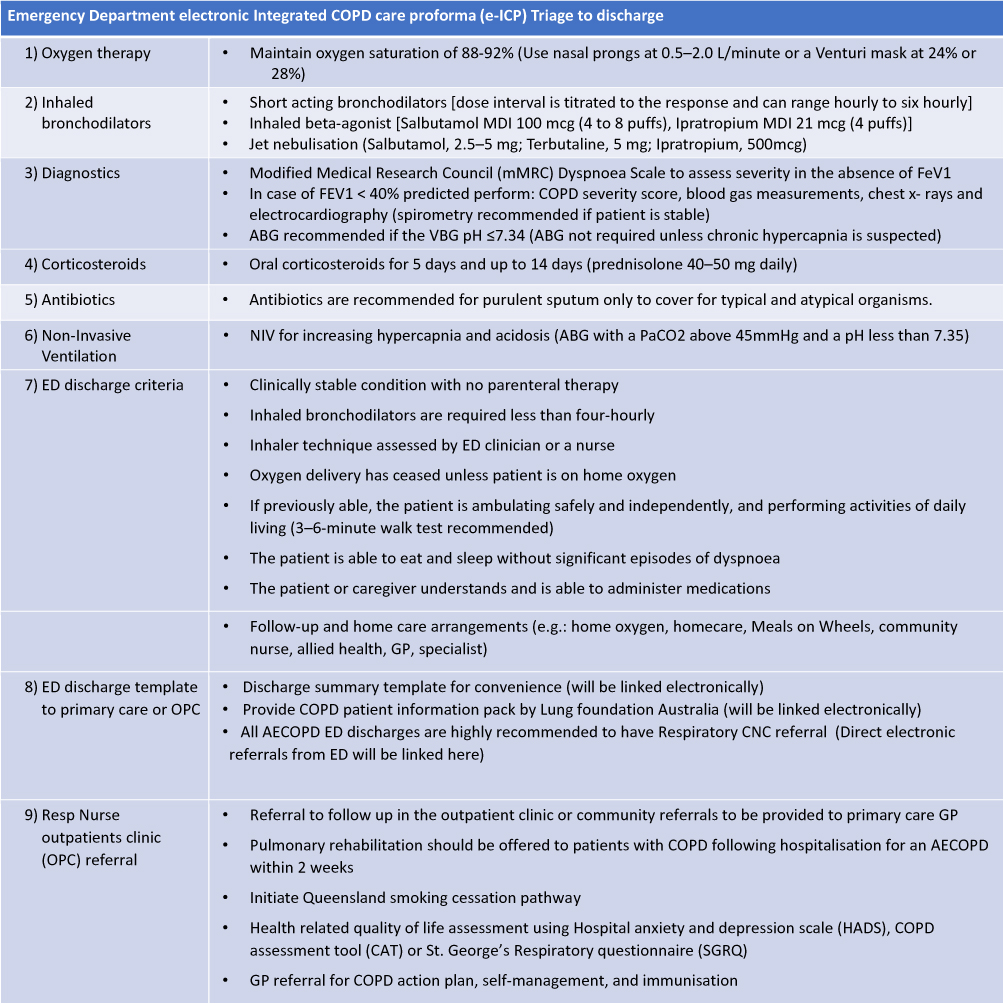 |
Figure 2 E-ICP final version for implementation in the Emergency department. |
Discussion
This study provided an opportunity to understand both Emergency and Respiratory departments’ interdisciplinary staff perspectives on pragmatic feasibility of COPD guideline adherence. Prioritising indicators for acute exacerbation in ED and clarity on where to perform highly reported discordant indicators such as pharmacological/acute ED COPD management (bronchodilator dose, corticosteroid dose, antibiotic dose, ABG, NIV indication) and non-pharmacological indicators (smoking cessation, inhaler technique check, pulmonary rehab, self-management education, community and outpatient referrals). Our findings suggest a single point of referral contact prior to discharge will potentially increase guideline adherence and interconnect hospital and primary-care interdisciplinary support. Education and updated guideline requirements on treatment and management may be provided through an electronic platform by installing COPD E-ICP in the ED desktops and intranet systems. Installing resources for staff and patients will aid clinicians to provide consistent information to COPD patients and interdisciplinary staff despite their experience and knowledge in treating respiratory patients. Our findings also suggest due to lack of patient and primary-care history, staff would really appreciate transfer of self-management plans, and action plans that are accessible by ED clinicians. Clinical informatics and digital assistance in the clinical environment have escalated guideline adherence and improved patient HRQoL.27 There is a level of disagreement between COPD guidelines and what is feasible in the emergency department, for instance clinician discretion on performing ABG or utilising NIV. Interestingly, GOLD guidelines suggest performing spirometry during the acute stage, however COPD-X guidelines do not make such restrictions.28 FEV1 still is the standard gold diagnostic investigation to assess severity and lack of clarity exists within international and national guidelines on diagnostics in the ED. Lack of availability of spirometry results in the emergency department were suggested to be tackled by utilising modified Medical Research Council (mMRC) dyspnoea scores and cigarette smoking/smoke exposure assumption in ED which had minimal consensus by both ED and respiratory department clinicians which is an area that needs further research.25,29 Interdisciplinary staff consistently agreed upon COPD patients bringing forward documentation with their last baseline pulmonary function measures in primary care to assist with early identification of probable hypercapnic respiratory failure.
Contrary to the exploratory review findings, experts ranked low consensus and excluded lack of knowledge (67.2%), awareness (68.6%), lack of resources based on publishing/ updated years as reasons contributing to non-adherence (68.6).9,30–33 A substantial difference was noted between ED and respiratory staff with referrals to be made by ED staff in the initial iterations of this study, however consensus was obtained by having a single point of contact (respiratory CNC referral) by both cohorts as time, staffing and pragmatic challenges were noted. Lack of consensus was apparent between ED clinicians and respiratory clinicians in terms of utilising ABG over VBG pH ≤7.34 and NIV criteria in ED as per COPD -X plan guidelines which indicates pragmatic dissemination to improve knowledge of COPD X guidelines is inevitable. Summarising the indicators of care in ED and referrals being managed by a single point of contact to respiratory clinical nurse the proforma will provide consistent guideline adherence and capture ED discharges for continuous care.5,25 The electronic proforma will be potentially capable of facilitating chronic care support appropriately through community or outpatients referrals. Electronic proformas are only feasible in larger hospitals with intranet resources and fall short when discussing rural and remote hospitals where there are no medical or nursing respiratory specialists. More work and research are required in this space particularly with the use of telehealth and internet dissemination into the primary-care area. This also falls under the strength of this study as nationally there is migration towards digitalisation from paper utilising integrated electronic medical records which increases the feasibility of the electronic COPD proforma.34 Mandatory respiratory CNC referral potentially increases continuity, accountability, and defragmentation of care. Dedicated and holistic bundles of care have proven to improve care and guideline adherence in studies in the UK, Australia, and Ireland,15,35,36 hence we presume adopting electronic COPD proforma will facilitate the same for Australia and other countries of similar health-care systems.
Conclusion
Variability in utilisation of COPD guideline recommendations by interdepartmental/interdisciplinary staff may be mitigated by utilisation of the electronic proforma. Through different iterations of this study, we have developed COPD care indicators to be initiated in the ED and primary-care referrals facilitation utilising a single point of referral (respiratory nurse specialist). This proforma will aid to resolve major barriers of knowledge, environmental resources, and professional role clarity in the management of COPD patients in the ED. Further research is warranted to explore alternatives for diagnostics and management in the ED due to unavailability of baseline pulmonary function scores during acute exacerbation episodes. Further research is also recommended to pilot the electronic COPD proforma in clinical settings to evaluate its impact on knowledge, guideline dissemination and impact on patient outcome in terms of holistic support.
Abbreviations
COPD, chronic obstructive pulmonary disease; E-ICP, electronic integrated COPD proforma.
Ethics
Ethics were reviewed and approved by University of Southern Queensland (H21REA007). All participants were provided research participation information sheet and consent obtained prior to each iteration completion.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding has been received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Harries TH, Thornton H, Crichton S, et al. Hospital readmissions for COPD: a retrospective longitudinal study. NPJ Prim Care Respir Med. 2017;27(1):1–6. doi:10.1038/s41533-017-0028-8
2. Quaderi S, Hurst J. The unmet global burden of COPD. Glob Health Epidemiol Genom. 2018;3. doi:10.1017/gheg.2018.1
3. World Health Organisation. WHO Global Health Estimates: The Top 10 Causes of Death. World Health Organisation; 2020.
4. Kelly AM, Holdgate A, Keijzers G, et al. Epidemiology, treatment, disposition and outcome of patients with acute exacerbation of COPD presenting to emergency departments in Australia and South East Asia: an AANZDEM study. Respirology. 2018;23(7):681–686. doi:10.1111/resp.13259
5. Hancy Issac MT, Lea J, Lea J, Lea J. Exploring factors contributing to Chronic Obstructive Pulmonary Disease (COPD) guideline non-adherence and potential solutions in the emergency department: interdisciplinary staff perspective. J Multidiscip Healthc. 2021;14:767. doi:10.2147/JMDH.S276702
6. Issac H, Moloney C, Taylor M, et al. Protocol: mapping of modifiable barriers and facilitators with interdisciplinary chronic obstructive pulmonary disease (COPD) guidelines concordance within hospitals to the Theoretical Domains Framework: a mixed methods systematic review protocol. BMJ Open. 2020;10(7):e036060. doi:10.1136/bmjopen-2019-036060
7. Rana R, Gow J, Moloney C, et al. Does distance to hospital affect emergency department presentations and hospital length of stay among COPD patients? Intern Med J. 2020. doi:10.1111/imj.15014
8. Migone C, O’Connor M, Kelly E, McDonnell TJ. Patients hospitalised with an acute exacerbation of COPD: is there a need for a discharge bundle of care? Ir Med J. 2015;108(9):273–275.
9. Markun S, Franzen DP, Dalla Lana K, et al. Acute exacerbated COPD: room for improvement in key elements of care. Int J Chron Obstruct Pulmon Dis. 2017;12:2969. doi:10.2147/COPD.S145496
10. Brownridge D, Zaidi S. Retrospective audit of antimicrobial prescribing practices for acute exacerbations of chronic obstructive pulmonary diseases in a large regional hospital. J Clin Pharm Ther. 2017;42(3):301–305. doi:10.1111/jcpt.12514
11. Masoompour SM, Mohammadi A, Mahdaviazad H. Adherence to the global initiative for Chronic Obstructive Lung Disease guidelines for management of COPD: a hospital-base study. Clin Respir J. 2016;10(3):298–302. doi:10.1111/crj.12215
12. Yang IA, George J, Jenkins S, et al. The COPD-X plan: Australian and New Zealand guidelines for the management of chronic obstructive pulmonary disease 2018. 2018.
13. Kelly AM, Van Meer O, Keijzers G, et al.Get with the guidelines - management of COPD in EDs in Europe and Australasia is sub-optimal. Intern Med J. 2019. doi:10.1111/imj.14323
14. McCarthy C, Brennan J, Brown L, et al. Use of a care bundle in the emergency department for acute exacerbations of chronic obstructive pulmonary disease: a feasibility study. Int J Chron Obstruct Pulmon Dis. 2013;8:605. doi:10.2147/COPD.S52883
15. Gerber A, Moynihan C, Klim S, et al. Compliance with a COPD bundle of care in an Australian emergency department: a cohort study. Clin Respir J. 2018;12(2):706–711. doi:10.1111/crj.12583
16. Overington JD, Huang YC, Abramson MJ, et al. Implementing clinical guidelines for chronic obstructive pulmonary disease: barriers and solutions. J Thorac Dis. 2014;6(11):1586–1596. doi:10.3978/j.issn.2072-1439.2014.11.25
17. Cousins JL, Wood-Baker R, Wark PAB, et al. Management of acute COPD exacerbations in Australia: do we follow the guidelines? ERJ Open Res. 2020;6(2):00270–2019. doi:10.1183/23120541.00270-2019
18. Coiera E. Guide to Health Informatics. CRC Press; 2015.
19. Chen C, Kan T, Li S, et al. Use and implementation of standard operating procedures and checklists in prehospital emergency medicine: a literature review. Am J Emerg Med. 2016;34(12):2432–2439. doi:10.1016/j.ajem.2016.09.057
20. Kerner T, Schmidbauer W, Tietz M, et al. Use of checklists improves the quality and safety of prehospital emergency care. Eur J Emerg Med. 2017;24(2):114–119. doi:10.1097/MEJ.0000000000000315
21. Considine J, Botti M, Thomas S. Emergency department management of exacerbation of chronic obstructive pulmonary disease: audit of compliance with evidence‐based guidelines. Intern Med J. 2011;41(1a):48–54. doi:10.1111/j.1445-5994.2009.02065.x
22. McPherson S, Reese C, Wendler MC. Methodology update: Delphi studies. Nurs Res. 2018;67(5):404–410. doi:10.1097/NNR.0000000000000297
23. Keeney S, McKenna H, Hasson F. The Delphi Technique in Nursing and Health Research. John Wiley & Sons; 2011.
24. Schneider P, Evaniew N, Rendon JS, et al. Moving forward through consensus: protocol for a modified Delphi approach to determine the top research priorities in the field of orthopaedic oncology. BMJ open. 2016;6(5):e011780. doi:10.1136/bmjopen-2016-011780
25. Issac H, Moloney C, Taylor M, et al. Mapping of modifiable factors with interdisciplinary Chronic Obstructive Pulmonary Disease (COPD) guidelines adherence to the theoretical domains framework: a systematic review. J Multidisciplin Health Care. 2022;Volume 15:47–79. doi:10.2147/JMDH.S343277
26. Issac H, Moloney C, Ian Yang GK, Taylor M, Lea J. Development of an Electronic Interdisciplinary Chronic Obstructive Pulmonary Disease (COPD) Proforma (e-ICP) to Improve Interdisciplinary Guideline Adherence in the Emergency Department: Modified Delphi Protocol. British Medical Journal. 2021.
27. Shepherd T, Hain S. eHealth in Queensland: progressing towards a patient centric, networked model of care. Healthc Inform Res. 2011;17(3):190–195. doi:10.4258/hir.2011.17.3.190
28. Yang IA, Brown JL, George J, et al. COPD-X Australian and New Zealand guidelines for the diagnosis and management of chronic obstructive pulmonary disease: 2017 update. Med J Australia. 2017;207(10):436–442. doi:10.5694/mja17.00686
29. Khialani B, Sivakumaran P, Keijzers G, et al. Emergency department management of acute exacerbations of chronic obstructive pulmonary disease and factors associated with hospitalization. J Res Med Sci. 2014;19(4):297–303.
30. Alsubaiei M, Frith PA, Cafarella PA, et al. COPD care in Saudi Arabia: physicians’ awareness and knowledge of guidelines and barriers to implementation. Int J Tubercul Lung Dis. 2017;21(5):592–595. doi:10.5588/ijtld.16.0656
31. Desalu OO, Onyedum CC, Adeoti AO, et al. Guideline-based COPD management in a resource-limited setting—physicians’ understanding, adherence and barriers: a cross-sectional survey of internal and family medicine hospital-based physicians in Nigeria. Prim Care Respir J. 2013;22(1):79–85. doi:10.4104/pcrj.2013.00014
32. Kim T-O, Shin H-J, Kim Y-I, et al. Adherence to the GOLD guideline in COPD management of South Korea: findings from KOCOSS study 2011–2018. Chonnam Med J. 2019;55(1):47–53. doi:10.4068/cmj.2019.55.1.47
33. Vanhaecht K, Lodewijckx C, Sermeus W, et al. Impact of a care pathway for COPD on adherence to guidelines and hospital readmission: a cluster randomized trial. Int J Chron Obstruct Pulmon Dis. 2016;11:2897. doi:10.2147/COPD.S119849
34. Queensland Health. My Health, Queensland’s Future: Advancing Health 2026. Queensland: State of Queensland; 2016.
35. McCarthy C, Brennan JR, Brown L, et al. Use of a care bundle in the emergency department for acute exacerbations of chronic obstructive pulmonary disease: a feasibility study. Int J Chron Obstruct Pulmon Dis. 2013;8:605-611. doi:10.2147/COPD.S52883
36. Sen B, Woollard M, Desira NL. Does the introduction of a COPD pro-forma improve the standards of care delivered by junior doctors in the emergency department. COPD. 2010;7(3):199–203. doi:10.3109/15412555.2010.481699
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.