Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Development of a Rule-Based Chatbot for Supporting Family Caregivers After Psychiatric Hospital Discharge: An Exploratory Qualitative Study in Indonesia
Authors Rizkiyah M, Rinawan FR, Hermansyah FR, Herawati DMD ![]() , Sukma RM
, Sukma RM
Received 13 March 2026
Accepted for publication 2 June 2026
Published 11 June 2026 Volume 2026:19 609048
DOI https://doi.org/10.2147/JMDH.S609048
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jagdish Khubchandani
Memy Rizkiyah,1– 3 Fedri Ruluwedrata Rinawan,2 Fajar Rachmat Hermansyah,3 Dewi Marhaeni Diah Herawati,2 Rifaz Muhammad Sukma4
1Master of Public Health Study Programme, Faculty of Medicine, Padjadjaran University, Bandung, West Java, Indonesia; 2Department of Public Health, Faculty of Medicine, Padjadjaran University, Bandung, West Java, Indonesia; 3Provincial Psychiatric Hospital, West Bandung, West Java, Indonesia; 4Department of Informatics, Faculty of Science and Informatics, Jenderal Achmad Yani University, Cimahi, West Java, Indonesia
Correspondence: Fedri Ruluwedrata Rinawan, Department of Public Health, Faculty of Medicine, Padjadjaran University, Jl. Ir. Soekarno No. km. 21, Sumedang, 45363, Indonesia, Email [email protected]
Purpose: Family caregivers play a crucial role in supporting patients with mental disorders after hospital discharge. However, caregivers often experience difficulties related to limited information, caregiving burden, and restricted access to mental health services. This study aimed to explore the informational and skill-related needs of caregivers of psychiatric patients after hospital discharge and to develop a prototype chatbot-based consultation system tailored to these needs in Indonesia.
Materials and Methods: An exploratory qualitative design guided by Social Cognitive Theory was employed to explore caregiver needs and support the development of a preliminary rule-based chatbot prototype. Data were collected through semi-structured interviews with eight participants (five mental health professionals and three family caregivers), supported by analysis of 67 anonymized WhatsApp consultation records and five discharge education documents. Data were analyzed using inductive thematic analysis following Braun and Clarke’s framework and organized using NVivo. Trustworthiness was enhanced through triangulation, member checking, and peer debriefing. The identified themes were translated into chatbot features including psychoeducation, caregiving guidance, relapse support, and referral navigation, followed by expert validation involving six multidisciplinary experts.
Results: Thematic analysis identified nine domains of caregiver needs: patient condition understanding, treatment and medication management, home care practices, community support, caregiver burden and coping strategies, supporting health services, barriers in online consultation systems, expectations for digital media, and future challenges in chatbot implementation. Caregivers emphasized the need for continuous psychoeducation, clear guidance for relapse prevention, and accessible consultation channels after discharge. Based on these findings, the identified caregiver needs were translated into a preliminary rule-based decision tree chatbot prototype (KJOL-ITEUNGBOT) designed to support caregiving information and referral navigation.
Conclusion: Family caregivers of psychiatric patients in Indonesia face complex informational and psychosocial challenges after hospital discharge. A chatbot-based consultation system may serve as a potentially useful tool for supporting caregiver access to information and post-discharge guidance. Future research should evaluate the usability, effectiveness, and scalability of the chatbot in broader clinical settings.
Keywords: digital health, hospital discharge, mental health, family caregiver, qualitative study, chatbot
Introduction
The global prevalence of severe mental health illness is an ongoing public health issue with significant connotations. Citing the World Health Organization (WHO), disorders like schizophrenia, bipolar illness, and major depressive disorder touch approximately one in four individuals at some point within their lives, and the prevalence of the disorders continues to increase globally. More recent meta-analyses indicate that the lifetime prevalence of significant depressive illness may be as high as 20.6%, with an associated significant increase in disability-adjusted lifespan.1 Furthermore, the economic burdens of mental health illness are severe, with the costs globally expected to be as high as $16 trillion in the year 2030 due to lost productivity and healthcare utilization.2 The risk of relapse in patients after being admitted in psychiatry is especially high, with estimates indicating that approximately 40% of the patients experience a recurrence within one year after discharge and consequently lead to more disability as well as higher healthcare expenditure.3
Family caregivers are crucial in post-hospital rehabilitation of the patients. Empirical research highlights that the knowledge, skill, and emotional support of the caregivers are important in facilitating adherence to the therapeutic regimen as well as the incidence of relapse.4 The participation of the caregivers in the therapy process is fundamental in improving the patients’ outcomes.5 The caregivers’ burden is high, more so in low- and middle-income countries (LMICs) such as Indonesia, whereby the health services are often limited. The caregivers in LMICs face difficulties such as high stress levels, poor training, and stigma related to mental illness that may disrupt their effectiveness in offering efficient support.6
In spite of the acknowledged value of caregivers, the available hospital-centric discharge instruction and associated support systems present glaring deficiencies. Research findings unveil that information conveyed at discharge is frequently poorly comprehended and memorized, with the consequence of the maintenance of knowledge deficits among caregivers and associated distress.7 A systematic review reported that poor instruction material is responsible for the high relapse and readmission risk within one month of discharge.3 The issue is aggravated by the absence of personalized, accessible support systems, such as digital solutions, following discharge from psychiatry units.8 Digital health solution, specifically chatbots in digital psychiatry, provide promising strategies in response to the identified challenges. Chatbots offer information and support accessibility at any time and place through 24/7 access, thus becoming an economical and scalable means in improving the resources of caregivers.8 They also allow users the capability of getting information anonymously and conveniently, which could provide some mitigation in the worry over stigma related to getting aid. Compared with other conventional digital health interventions, including telemedicine and psychoeducation applications, chatbots can provide sustained engagement while offering the distinctive interactive experience.9 Systematic reviews document the effectiveness of digital mental health interventions in asserting that digital mental health strategies can effectively contribute in the management of psychological well-being as well as in the adherence in care protocols.10
It is important to note that, despite the substantial increase in research concerning chatbot-assisted interventions for mental health, the majority of studies have predominantly focused on the experiences and management of patients, while the requirements of family caregivers, particularly in post-discharge scenarios within developing countries, have been largely overlooked.11 In light of Indonesia’s distinct socio-economic context and the urgent demand for effective mental health strategies, it represents an appropriate case study for examining innovative support systems for caregivers. Therefore, an exploratory qualitative investigation is necessary to gain a deeper insight into the informational and skill-related requirements of these caregivers, which could facilitate the development of a customized chatbot intervention that addresses their specific challenges and improves their ability to assist their loved ones.4,7 In a recent research using PsyBot app, demonstrated the effectiveness of chatbot-based psychological assistance in reducing loneliness and improving the emotional well-being of users in Indonesia.12
Despite increasing interest in digital mental health interventions, limited studies have explored how caregiver experiences and informational needs can be systematically translated into chatbot architectures, particularly in post-discharge psychiatric care settings in low- and middle-income countries. This study aimed to explore caregiver informational and psychosocial needs following psychiatric hospital discharge and to translate these findings into a preliminary rule-based chatbot prototype for caregiver support.
Materials and Methods
Study Design
The present study utilized an exploratory qualitative design in order to develop some understanding of the informational and competency requirements of family caregivers, along with their requirements for a framework of chatbot. This study began on May 14, 2025, after the research protocol was approved by the institutional ethics committee, and was completed on February 15, 2026. The exploratory qualitative method is particularly useful when involved in the development of user-focused digital health applications, as this involves the systematic examination of the lived experience and views of caregivers.13,14 The adoption of this methodology allows the attainment of specific needs and wants that can be used in the development of tailored responses. Qualitative research is particularly effective at the production of richly contextualized information, something that is critical when examining the richly complex and diverse realities in which caregivers live mental health situations.14
Theoretical Framework: Social Cognitive Theory
This study was guided by Social Cognitive Theory (SCT), which explains that health-related behaviors are influenced by cognitive, behavioral, and environmental factors. SCT was considered relevant because caregivers of psychiatric patients frequently experience uncertainty, emotional burden, stigma, limited caregiving confidence, and restricted access to mental health information following hospital discharge.15–17 In this study, SCT constructs were also used as a conceptual framework to guide the design and structuring of chatbot features. Caregiver difficulties related to relapse management, medication adherence, caregiving skills, and access to mental health services were translated into psychoeducation, caregiving guidance, relapse support, and referral navigation pathways within the chatbot prototype. The SCT framework was applied not to evaluate behavioral outcomes, but to support the development of a preliminary caregiver-centered chatbot prototype.
Participants
Participants in this study were caregivers of people with severe mental illness such as schizophrenia, bipolar illness, and major depressive illness who had just discharged of psychiatric care. The inclusion requirements were as follows: (1) adult caregivers who were over the age of 18 years; (2) being responsible mainly for the care of the carer’s patients; and (3) being able to communicate well in Bahasa Indonesia. The exclusion caregivers who were unwilling to give informed consent. Caregivers were approached using theoretical sampling techniques, which allowed focused sampling that identified caregivers who were most relevant to the study objectives.18,19 Healthcare professionals were also recruits in this study.
Participant Cohort
A total of eight subjects, five mental health professionals and three caregivers were included in the interview. The sample size was determined in line with the requirements of thematic saturation, whereby data collection should cease when no new theme emerges during the interview. Sample adequacy was evaluated based on the richness and repetition of qualitative data rather than statistical representativeness. Although the caregiver subgroup was relatively small, recurring patterns across interviews supported thematic saturation and provided sufficient depth to explore caregiver experiences and informational needs.20 Eight participants contributed to multiple interview sessions, and data collection continued until no new themes emerged, indicating thematic saturation.
Data Collection
All interviews were conducted by researchers with prior experience in qualitative health research and mental health services. The interviewers received training in semi-structured interviewing and reflexive qualitative methods. Data was collected by in-depth semi-structured interviews with caregivers, following an interview protocol aimed at garnering rich responses regarding their informational and affective needs using an interview guide developed based on the study objectives and Social Cognitive Theory framework. The 45–60-minute-long interviews either occurred in consultation rooms of hospitals or over secure online platforms, following participants’ choices and providing a convenient space facilitating open discussion.13 Document reviews of patients’ current online psychiatric consultation records over WhatsApp also added to the richness of participants’ experiences. The interviews, audio-recorded with participants’ permission, had field notes kept in sight to obtain observational insights.
Data Analysis
All interview audio recordings were transcribed verbatim following each interview session. Interview transcripts and anonymized WhatsApp consultation records from the KJOL consultation service were analyzed using inductive thematic analysis following Braun and Clarke’s approach.21,22 Coding was conducted manually by the research team, with NVivo software used to organize the data and support systematic theme development. A structured coding process was applied, involving iterative review of the transcripts to achieve data familiarization, followed by the identification of significant phrases and recurring patterns to generate initial codes capturing the core meanings of participants’ experiences. These codes were subsequently refined through constant comparison and grouped into categories, which were then developed into overarching themes.
The analysis was conducted concurrently with data collection to ensure iterative thematic analysis and theme saturation monitoring. Two researchers independently coded the data, and discrepancies were resolved through discussion until consensus was achieved. Purposive sampling was done to extract WhatsApp consultations that dealt with caregiving issues such as worries about relapses, issues with medication, caregiver emotional burdenand the need for aftercare support post-discharge.
Trustworthiness
In order to guarantee the study’s rigor, methodologies compliant with the COREQ standards were used.23 The findings’ credibility was enhanced through member checking and triangulation of data sources (caregiver and professional interviews, WhatsApp chat reviews). Transferability was ensured by providing thick descriptions of the study context and participant characteristics. Eight participants contributed to multiple interview sessions, and data collection continued until no new themes emerged, indicating thematic saturation. Dependability was supported through a maintained audit trail that documented research procedures and decision-making processes, while confirmability was ensured through the researcher’s reflexivity during the study’s duration. These methodologies reflect the Lincoln and Guba-established trustworthiness standards that are fundamental in qualitative research.13,18,21
Expert Validation
Expert review was carried out to validate the themes identified for their appropriateness and feasibility as a means of implementing them through the development of a chatbot application. The identified themes were used to inform the conceptual and structural development of the chatbot, ensuring a clear linkage between qualitative findings and system design. The six experts comprised a psychiatrist, a psychiatric nurse practitioner, a medical social worker, a pharmacist, a public relations expert, and an IT expert who reviewed the output of thematic analyses and suggested the structure of the chatbot. Their feedback contributed to refinement of caregiver need categorization, information structure, and practical system implementation.24
Qualitative-to-Chatbot Translation Process
In the current study, a translation framework from qualitative data collected from interviews with caregivers, healthcare practitioners, and WhatsApp consultations was utilized in order to design a rule-based chatbot prototype. Thematic analysis enabled identifying themes related to medication adherence, relapse prevention, caregiver stress, communication issues, and barriers to mental health care. SCT constructs informed chatbot design, including self-efficacy (caregiving guidance), behavioral capability (psychoeducation), and reinforcement (continuous access to support). Each theme identified from the qualitative analysis was translated into decision-tree nodes, while categories informed branching structures and codes were used to construct specific chatbot response content. Decision tree method was applied to ensure the consistency of responses and the safety of interactions within the field of mental health service delivery. The prototype was developed as an information-support tool, not to replace the expert opinion of mental health specialists during consultations.
Development of Prototype
Rule-Based Decision Tree Architecture
Chatbot intelligence has been implemented using the Python programming language and a rule-based decision tree architecture. Instead of relying on a classification algorithm, a rule-based architecture has been used, and rules were derived from thematically coded caregiver interviews carried out during the qualitative phase of the study. The decision tree architecture has been used as a knowledge representation model for the chatbot. Each decision node has represented a query or a caregiving situation, and each branch has represented a response pathway. The chatbot has helped users progress through a series of steps to obtain appropriate information or advice on caregiving.
The knowledge base has been represented by a number of thematic domains derived during the qualitative phase of the study. The thematic domains include treatment and medication adherence, patient condition monitoring, home care management, caregiver concerns, community services, and health information services. In cases where caregiver queries indicated a complex situation, the chatbot has referred caregivers to mental health professionals for advice.
System Design
The system has been designed with three components: a user interface, a knowledge base, and an inference engine. The knowledge base has been represented by rule structures derived during the qualitative phase of the study, and the inference engine has been used to process caregiver inputs and navigate a decision tree to generate appropriate responses. A MySQL database has been used to store logs and records of interactions. System interaction has been represented by using UML diagrams such as use cases, activity diagrams, sequence diagrams, and class diagrams.
Non-Functional Specifications
The system was created with the bare-minimum number of hardware requirements (dual-core 2.0 GHz processor, 4 GB RAM, stable internet connection) and the best possible settings (i3 8th gen, 8 GB RAM, SSD, 20 Mbps internet). Security measures include database authentication, frequent backups, and data handling on the administrators’ level.
System Evaluation
Chatbot evaluation has been carried out by implementing a rule-based decision tree architecture instead of a predictive model. Functional testing has been carried out to ensure that caregiver queries are appropriately navigated to decision nodes and appropriate responses are generated for a range of caregiving scenarios. Special care has been taken to ensure that caregivers are referred to mental health professionals for severe cases.
Ethical Considerations
This study was conducted in accordance with the ethical standards of the Declaration of Helsinki (1964, and its later amendments) and received ethical approval from the Research Ethics Committee of the Padjadjaran University (approval number: 417/UN6.KEP/EC/2025; registration number: 2503040330; Clinical trial number: not applicable; issued on 13th of May, 2025). Each of the subjects signed a written consent form following an explanation of the aims of the research, their freedom not to take part in the study, and the steps taken to ensure the anonymity and confidentiality of all parties involved. The signing of the consent form also included permission to quote anonymized sections of interviews and consultations. The subjects were also made clear about their rights to withdraw at any time without punishment. The above steps were taken to prevent potential ethical concerns while involving vulnerable groups.13,19 The ethical clearance was good for one year following the date of approval, with obligations of submitting progress and final results to the committee. Modifications to the protocol, extensions, or any severe adverse events (SAEs) had to be submitted promptly to the Research Ethics Committee.
Results
Participant Characteristics
Deep-level interviews were conducted among two groups of informants: caregivers of mental patients and West Java Provincial Psychiatric Hospital professionals. Informants were aged 29–60, primarily women, whose educational attainment was a diploma up to a bachelor’s degree. The medical professionals interviewed also consisted primarily of women of around 55 years of age. The following is a summary of participants’ demography and coding distribution (Table 1).
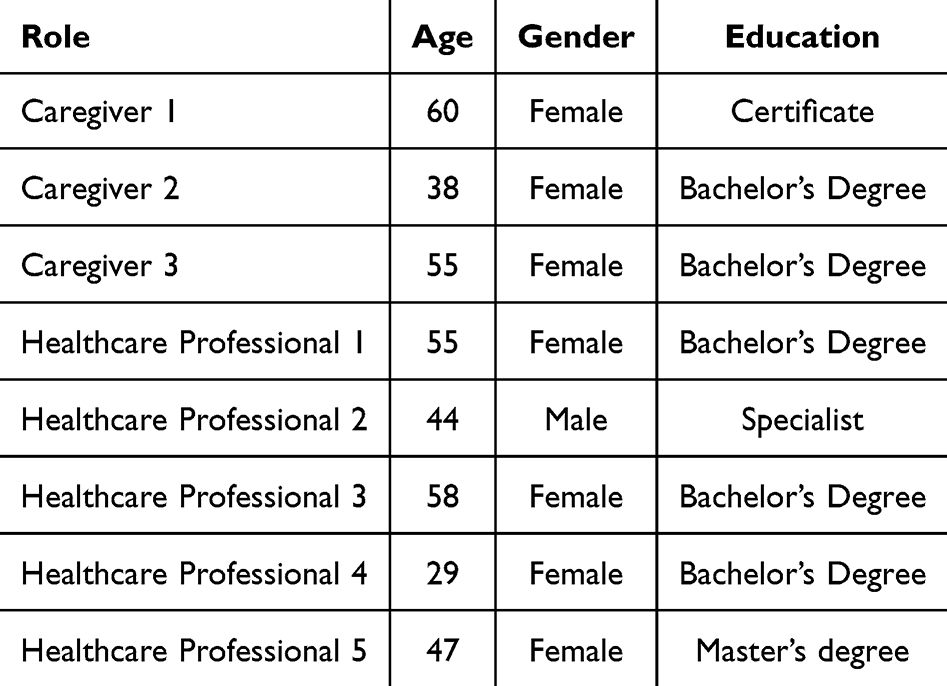 |
Table 1 Demographic Characteristics of Participants |
Document Review
Besides the in-depth interviews, a document study was also done through the utilization of two main data sources: (1) transcripts of chat from the WhatsApp consultation service (KJOL) from mid-2022 through mid-2025, and (2) discharge notes represented by Information and Education Note Sheets from inpatient case notes. The querying of the WhatsApp chat data utilized the keywords of “pasca rawat”, “pulang rawat inap”, “dirawat”, and “kontrol.” Table 2 specifies the number and classification of documents encompassed in the analysis.
 |
Table 2 Results of Document Classification Included in the Analysis |
Of the content analysis of documents surveyed, 67 WhatsApp numbers were investigated with a yield of 98 reference quotes. Similarly, the discharge note forms comprising 5 documents generated 19 references. These results augment information obtained from interview data and yield more evidence of the persistent information needs generally captured by caregivers upon discharging patients.
Thematic Findings
The results of the thematic analysis in Tables 3–4 identified two main topics: Knowledge and Skills, and Digital Media. From the overall data, a total of 94 codes, 25 categories, and 9 themes were obtained. The Knowledge and Skills topic comprised 71 codes, 17 categories, and 6 themes, while the Digital Media topic comprised 23 codes, 8 categories, and 3 themes. The identified nine domains of caregiver needs: Treatment, Supporting Information Services, Caregiver-Related Issues, Community Support, Patient Condition, Home Care for Patients, Barriers in Online Mental Health Consultation (KJOL), Future Challenges in Chatbot Implementation, Expected Digital Media (Chatbot). Expectations for a chatbot clustered into three themes: usability, integration with existing systems, and value for health promotion.
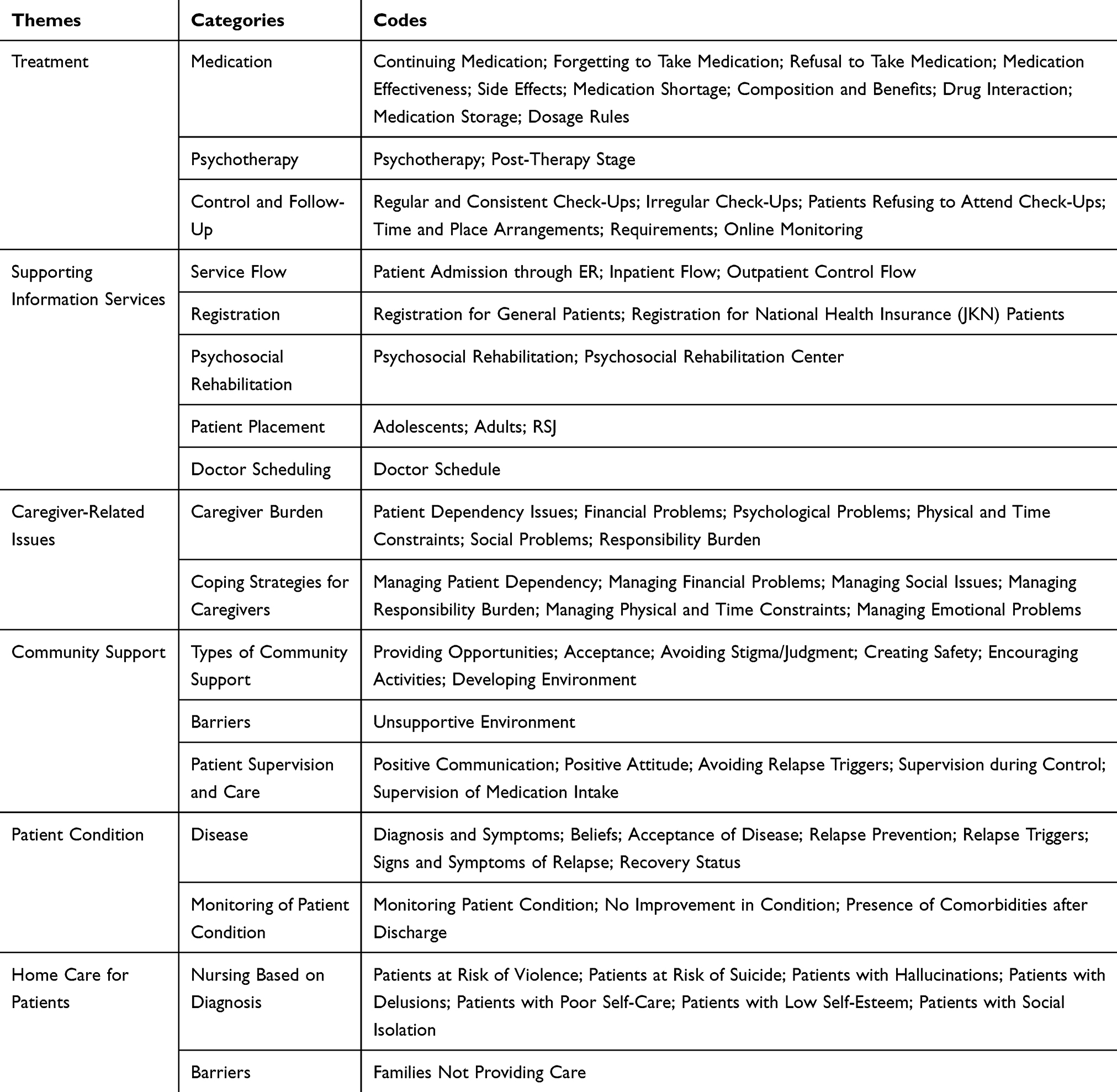 |
Table 3 Themes, Categories, and Codes from Caregiver Interviews and Document Review: Caregiver Knowledge and Skills |
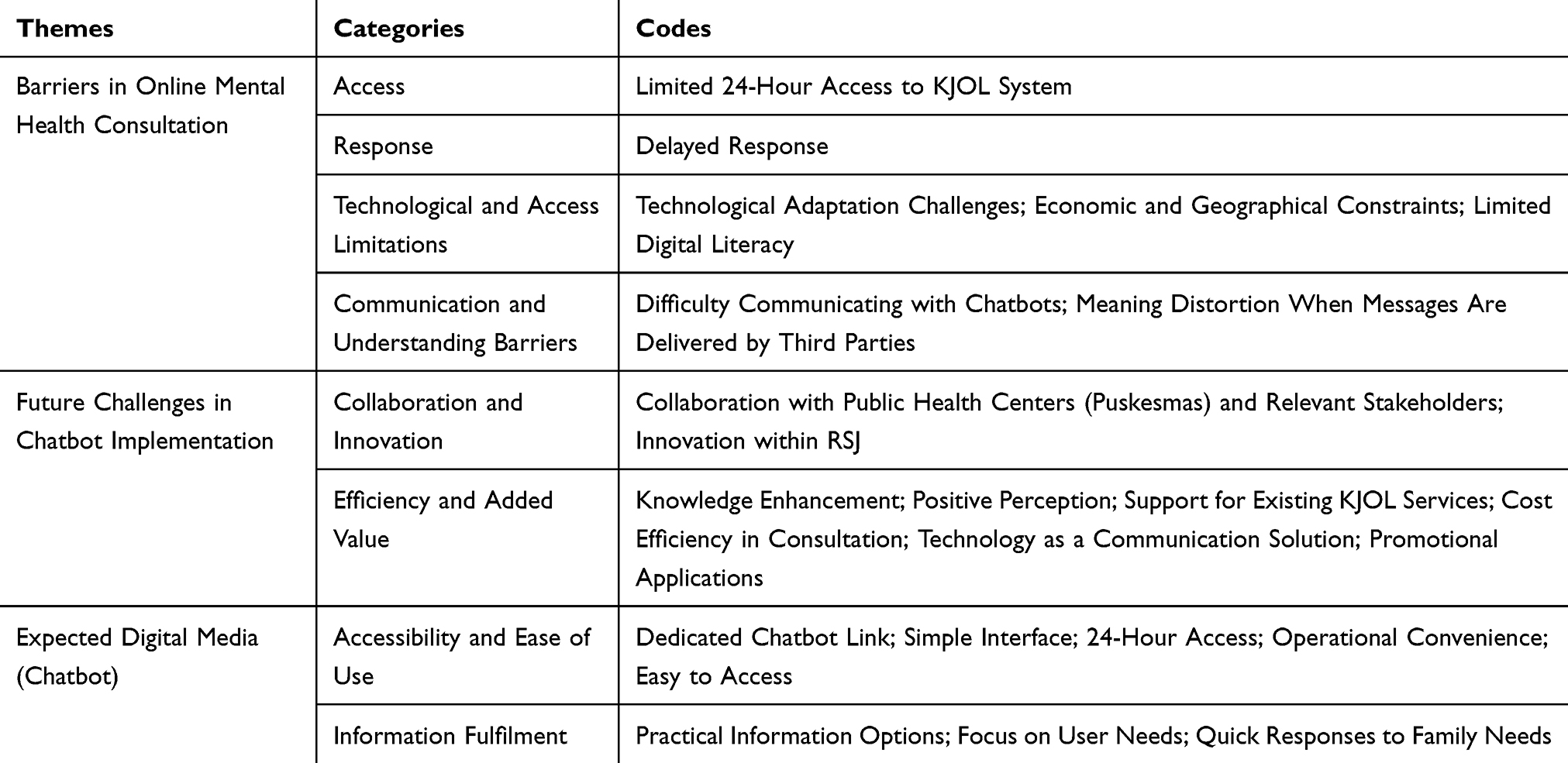 |
Table 4 Themes, Categories, and Codes from Caregiver Interviews and Document Review: Media Digital |
Narrative Findings by Theme
Patient Condition
Two categories were identified: disease understanding and patient monitoring. Participants frequently sought clear explanations about diagnosis, relapse signs, and prognosis. “If I want to ask questions related to patients diagnosed with schizophrenia, is that okay?” caregiver O47, WhatsApp.
Caregivers described early relapse indicators, including talking to oneself and emotional instability.
Symptoms also reappeared, such as spitting indiscriminately, talking and laughing to oneself, and emotional ups and downs. caregiver O21, WhatsApp.
Clinicians confirmed that families often requested information on relapse triggers and prevention. “For patients who frequently visit the hospital. what is the problem?” Healthcare Professional 3, interview.
Families also expressed uncertainty about recovery possibilities. “Is it possible that my child will recover within the next year or two?” caregiver O64, WhatsApp.
Monitoring after discharge remained a persistent concern. Families requested continued communication from hospital staff. “If it’s not too much trouble, is there someone specific I can contact to find out how the patient is doing?” Caregiver 3, interview.
These findings highlight that caregivers require ongoing education and structured follow-up systems to detect changes early and manage recovery.
Treatment
This theme consisted of medication, control and follow-up, and psychotherapy. Caregivers sought detailed information about medication composition, dosage, side effects, and interactions. “Perhaps in its contents, what is this medicine for, what are its benefits?” Healthcare Professional 3.
Some families expressed fear of side effects or dependency. His body was shaking, his hands were stiff like a robot’s. was the medicine too strong? Caregiver O28, WhatsApp.
Clinicians emphasized that medication should not be stopped abruptly. It is recommended not to stop. If you feel better, consult your doctor first. Caregiver 2.
Barriers to control included patients refusing to attend due to trauma or fear of being re-hospitalized.
His child did not want to go with him because he was afraid of being hospitalized again. Caregiver O51, WhatsApp.
Families also reported logistical and administrative challenges (JKN referrals, scheduling) and expressed interest in online consultation systems for easier access. Psychotherapy and psychoeducation were identified as important complementary approaches for both patients and families to reinforce medication adherence and emotional stability.
Home Care
Families described challenges and needs related to home-based care after discharge. They required guidance specific to the patient’s condition such as managing risk of violence, suicide, hallucination, delusion, or social isolation. “There are seven diagnoses, the most common being violent behaviour and hallucinations.” Healthcare Professional 3.
Practical instructions helped families handle emotions and encourage independence. When you’re angry, take a deep breath or hit a pillow, not a wall. Healthcare Professional 3.
Routine structuring and activity reinforcement were emphasized. After eating, wash your own dishes, sweep, mop, cook noodles, so you can be independent.” Healthcare Professional 3.
Caregivers also stressed the importance of communication, empathy, and creating a safe home environment. Caring must be prioritized. once you are close, patients will surely obey. Healthcare Professional 5.
This theme reflects the integration of nursing education and behavioural therapy within the family setting.
Community Support
Two categories emerged: forms of community support and barriers. Families valued acceptance, safety, and opportunity for social reintegration. “Praise be to God, everyone accepted it.” Caregiver 3.
Conversely, stigma and rejection were recurring barriers. When I arrived, they said, ‘Nugelo is here again. Healthcare Professional 3.
Collaboration with local institutions such as Puskesmas, RT/RW, and village leaders was described as essential for sustainable recovery. It’s not just hospitals, this is cross-sectoral, there is a role for community health centers and RT/RW. Healthcare Professional 5.
This theme highlights that community empathy and structural collaboration are therapeutic elements in long-term rehabilitation.
Caregiver Burden and Coping
Caregivers reported multidimensional strain physical, emotional, economic, and social. “Since spending a week at home, I haven’t been able to sleep or eat because of my child.” Caregiver O35.
They described fatigue, lack of rest, and financial strain due to increased daily costs. Being tired of money is definitely tiring. Caregiver 1.
Coping strategies included family task-sharing, spiritual acceptance, WhatsApp peer groups, and counselling sessions. “The WhatsApp group is helpful, supporting each other.” Caregiver 3.
Clinicians provided supportive psychotherapy and psychoeducation. Supportive psychotherapy for patients and families. Healthcare Professional 2.
This theme reinforces that emotional resilience and institutional support are crucial for sustaining caregiving roles.
Supporting Health Services
Families expressed confusion about the hospital’s administrative flow. They sought information about service procedures, doctor schedules, registration, rehabilitation programs, and emergency pickup. “If I bring an emergency patient to the emergency room today, do I need to bring a referral letter?” Caregiver O36.
Transparent information flow was perceived as essential to reduce anxiety and delays in accessing care. Her Instagram account likes to follow her doctor’s practice. Caregiver 3.
This finding indicates the need for better communication systems and health information literacy among caregivers.
Barriers in Online Mental Health Consultation (KJOL)
Participants reported that KJOL services lacked real-time responsiveness and 24-hour availability. “I have, but there was no response. I’d like it to be 24 hours.” Caregiver 3.
These limitations affected satisfaction, especially during urgent episodes. Currently, KJOL is not online 24 hours a day. Healthcare Professional 2.
The findings highlight the gap between technological availability and actual usability in clinical practice.
Expected Digital Media (Chatbot)
Caregivers and clinicians envisioned a 24-hour chatbot with simple, accessible features and a dedicated link. “Ideally, there should be a chatbot for KJOL.” Healthcare Professional 2.
There should be someone who’s available and easy to reach whenever we need help. Caregiver 3.
They expected the chatbot to deliver practical health information and promote efficiency and knowledge gain. It’s educational, so it’s useful. Caregiver 3.
Clinicians added that chatbots could complement existing online services and act as tools for mental health promotion. It can also be used for health promotion. Healthcare Professional 2.
Future Challenges in Chatbot Implementation
Predicted challenges involved technological literacy gaps, economic and geographic inequalities, and communication limitations in conveying empathy through automated systems. “Our patients come from lower-middle-class families and remote areas.” Healthcare Professional 1.
It’s a bit difficult for the soul, because it requires the art of medicine. Healthcare Professional 2.
Participants cautioned that misinterpretation could occur when messages were relayed indirectly. “If information is conveyed through other people, there is a concern that perceptions may differ.” Healthcare Professional 1. This indicates the necessity for user-centered and empathetic AI design in mental health contexts.
Across themes, caregiver needs were interconnected, with knowledge gaps contributing to emotional burden and challenges in accessing healthcare services. These findings highlight the need for integrated and continuous caregiver support following hospital discharge.
Translation of Qualitative Findings into Chatbot Features
Qualitative findings from caregiver interviews, healthcare professionals, and WhatsApp consultation records informed the development of the chatbot prototype. Themes related to medication management, relapse prevention, caregiving burden, communication difficulties, and limited access to mental health services were translated into chatbot features including psychoeducation, caregiving guidance, relapse support, coping information, and referral navigation pathways. These themes informed the structure of chatbot decision nodes, where each caregiving issue corresponded to specific response pathways within the system. The chatbot was conceptually designed as a caregiver-centered informational and supportive tool to address commonly reported post-discharge caregiving needs.
Prototype KJOL-ITEUNGBOT
These thematic results were then converted to the development of a prototype chat assistant, called KJOL-ITEUNGBOT (“Informasi, Teman, Edukasi Untuk Ngerawat Gangguan Jiwa” - Information, Companion, and Education for Mental Health Care). It is a chatbot-based online mental health consultation service developed to provide continuous support for patients and their families after hospital discharge. The system was built as an internet-based application so that it can be broadly usable and always available 24/7 to caregivers. The chatbot architecture was organized using a rule-based decision tree, enabling structured navigation of caregiver queries and providing appropriate responses based on predefined caregiving scenarios.
System Features
It has (1) information dissemination modules on mental health, (2) medication and daily care regimen management, (3) emotional coping assistance to aid caregiver coping, and (4) integrated referral links to Online Mental Health Consultation (KJOL). There is also an IP address-based use counter implemented to monitor utilization of the system and determine user activity.
User Interface
The interface designs and prototypes Figure 1 illustrates the interface of the prototype, which showcases two primary functionalities. To the left, users are able to navigate a series of structured inquiries pertinent to medication management (for instance, “Do we really have to keep taking the medicine every day?”, “What if the medicine dose feels too low?”, “What could happen if we suddenly stop the medication?”). These alternatives mirror the concerns of caregivers highlighted in the thematic analysis, particularly uncertainties regarding adherence and potential side effects. On the right, the chatbot delivers explicit, contextually relevant responses, stressing the importance of consistent medication use while providing advice for follow-up actions. Significantly, the chatbot also incorporates direct referral details, facilitating caregivers’ access to the hospital’s online consultation service (WA KJOL: 081221292020) for urgent or complex situations.
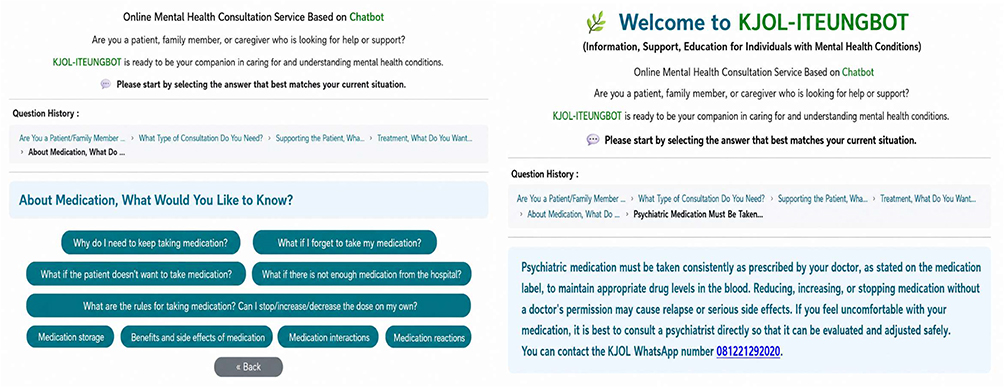 |
Figure 1 Illustrates the prototype interface of the ITEUNG chatbot, consisting of two main panels. The left panel presents a structured menu of frequently asked questions (FAQs) related to medication management, displayed as selectable buttons that allow users to navigate caregiving topics through a hierarchical pathway, as indicated by the navigation trail (“Riwayat Pertanyaan”). The right panel displays the chatbot’s response interface, where selected queries generate context-specific textual responses presented in a highlighted message box. The response emphasizes medication adherence and includes actionable guidance, along with integrated referral information (e.g., WhatsApp contact for the KJOL consultation service) to support follow-up in complex situations. The interface is presented in Bahasa Indonesia, as the application is specifically designed for Indonesian users, ensuring accessibility and contextual relevance for the target population. This figure demonstrates the interaction flow from user-selected queries to automated responses with embedded referral pathways. |
Decision Tree Structure
The chatbot responses were organized using a rule-based decision tree framework, as illustrated in Supplementary Figures S1–S11. The detailed structure of the decision logic, including question codes and chatbot response mappings, is provided in Supplementary Tables 1 and 2. The decision tree begins with general caregiver inquiries regarding psychiatric illness and guides users through several thematic pathways, including disease understanding, diagnosis, recovery, causes of relapse, and warning signs of relapse. Each node represents a caregiver query or caregiving situation, while the branches define structured response pathways that guide caregivers toward relevant information or recommended actions. When caregiver responses indicate complex or potentially severe conditions, the chatbot redirects users to professional mental health consultation services. This rule-based structure allows transparent and interpretable decision pathways while ensuring that caregivers receive appropriate guidance during the post-discharge care process.
Expert Validation
The expert validation process generated several recommendations to improve the chatbot prototype. Clinical experts suggested simplifying diagnostic categories, integrating relapse management with patient condition monitoring, and ensuring that medication information includes both therapeutic effects and possible side effects. Experts also recommended using language that is easily understood by caregivers and directing complex cases to professional consultation services.
The medical social worker recommended incorporating referral pathways to nearby health services and crisis response systems, while the pharmacist suggested revisions related to medication storage and safety information. The public relations expert recommended including clear information about hospital services and health insurance access. The information technology expert confirmed the feasibility of implementing the chatbot and suggested several design improvements, including avoiding unnecessary personal data collection, enabling conversation history tracking, and integrating the chatbot into the KJOL web platform and WhatsApp consultation service.
Discussion
This pilot study investigated the neglected needs of family caregivers of psychiatric patients post-discharge and the promise of a consultation service using a hospital-based chatbot.10,25,26 The thematic analysis identified four key areas of caregiver needs: Treatment, Supporting Information Services, Caregiver-Related Issues, Community Support, Patient Condition, Home Care for Patients, Barriers in Online Mental Health Consultation (KJOL), Future Challenges in Chatbot Implementation, Expected Digital Media (Chatbot).27,28 Furthermore, both healthcare professionals and caregivers prioritized the design of a user-friendly but responsive and always-on 24/7 hospital-based chatbot that is seamlessly integrated into hospital services.10,25,28 These results add to the present literature on caregiver challenges in Indonesia27,28 and add to the burgeoning literature on digital mental health programs.10,26,27
It is remarkable that the PsyBot study12 demonstrated significant reductions in loneliness and improvements in well-being. The present study extends these findings by focusing on online interventions based on caregivers within the post-discharge setting. Differing from PsyBot, which primarily tackled individual users’ affective wellbeing, the KJOL-ITEUNG chatbot focuses on empowering knowledge, increasing caregiving skills, and up keeping hospital-associated care. This distinction highlights that the role of chatbots for mental health support could shift out from providing brief immediate emotional support alone towards enabling a broader family-centered and systemic extension of care.
These complementing findings suggest that the integration of hospital-centered chatbot systems such as KJOL-ITEUNG with user-centered frameworks such as PsyBot is likely to achieve a holistic online framework for both users and caregivers within the mental health context of Indonesia. This low awareness of relapse prevention is reflected by earlier literature indicating that inadequate knowledge about psychiatric illness amplifies anxiety and prolongs recognition of relapse.25,28 The international literature again and again demonstrates an outcome where families lacking definitive guidance are less confident to support at home and report higher readmission.28 Our results again emphasize ongoing education delivery and avoiding restricting it to short sessions at the time of discharge. An online medium has an important part to play in maintaining education through the duration of hospital stay.25–27
Medication administration and delivery of daily care presented critical challenges. Gaps in medication scheduling adherence, side effect observation, and management of patient activities were repeatedly cited by respondents.29,30 These results are in alignment with global literature indicating suboptimal medication adherence is usually related to inadequate caregiver preparation.29,30 Communication barriers otherwise compounded caregiving experiences with family members indicating confusion in de-escalation approaches of hostility or increasing participation.27,28 These themes in combination each emphasize the concept that caregiving effectively necessitates not only knowledge of medicine but interpersonal and practical competency something usually deficient in formal discharge education.26–28
The findings also showed the steep emotional and economic burden faced by caregivers.31,32 Most frequent were reports of stress, fatigue, and social isolation, in keeping with findings in low- and middle-income countries where caregiving is often unsupported at the family level.32,33 Financial pressure, and in particular costs related to medication and transportation, was made worse by confusing processes of referral.32,33 These interconnected strains show how the needs of caregivers cannot be addressed in isolation: the mental health support, the provision of money, and steering through systems are all closely interconnected.32
Access to healthcare services, particularly in emergencies, was a key issue.34 Caregivers tended to express ambiguity about how to approach or where to seek help when patients displayed behaviour consistent with relapse or aggression.34 The need for direct referral procedures is commensurate with evidence identified in overseas mental health literature pointing to the essentiality of timely crisis intervention.4 Accordingly, the addition of direct referral information to the prototype of a chatbot addresses an operational and urgent need with the prospect of preventing delays in accessing professional assistance.4
Notably, the requirements of the conversation-based bot overwhelmingly emphasized usability and integration.35 The caregivers favoured a tool that would be easily retrievable at all times, required low digital literacy levels, and provided responsive feedback.35 The clinicians emphasized having the chatbot linked with KJOL to support continuity of care.4 This highlights the evidence reviewed demonstrating digital health interventions are their best when integrated into established health systems and not running in isolation.35
Together, these outcomes suggest that caregiver needs are multifaceted and interrelated.31,32,36 Knowledge gaps widen levels of stress, communication challenges increase feelings of burden, and financing limitations escalate barriers to accessing health services.31–33 The design of a decision tree based chatbot addressed these overlapping requirements effectively by providing structured frequent questions, coping strategies with regard to stress reduction, and combined-referral contact.36,37 Translating thematic findings into design elements with a tangible action agenda, this study highlights the critical need to balance digital innovation with user experiences.36,37
Theoretically, the current study application of Social Cognitive Theory in Chatbot Design.38 The findings demonstrated substantial caregiver uncertainty regarding medication management, relapse recognition, and home-based psychiatric care. Within SCT, these findings reflect low caregiving self-efficacy.38 The chatbot was therefore designed to support caregiver confidence through structured guidance and accessible psychoeducation.38 Caregivers expressed substantial needs for practical knowledge and caregiving skills, including medication management, symptom monitoring, and positive communication. These findings align with the SCT construct of behavioral capability.39 The chatbot’s 24-hour accessibility may function as a reinforcement mechanism by repeatedly exposing caregivers to caregiving guidance, relapse prevention information, and service navigation support. This implies digital interventions are in a position to be sources of information and even systems providing behavioural support. These constructs were operationalized within the chatbot design to support caregiver behavior and decision-making.
Long term, although this trial has significant findings, it simultaneously presents questions to be addressed by subsequent research.36,39 The prototype has neither been assessed in usability terms nor by clinical significance and how much it lowers relapse rates or alleviates caregiver burden is unknown.36 There are infrastructure and digital literacy issues likely to constrain delivery in low-resource environments.32,38 Referring to these in pilot and multi-centre investigations will be important to clarifying the value of chatbot-assisted support to mental health services’ caregivers.36
Limitation
Some limitations need to be acknowledged. First, this study was an exploratory qualitative single site study, thus limiting generalizability to other geographical locations. Secondly, although thematic saturation was achieved, the sample size remained small and only covered a minority of caregiver experiences. Thirdly, the prototype nature of it means it has never been subjected to usability or effectiveness testing and so is uncertain in its practical effect. Fourthly, the current version utilizes a decision-tree approach, and this might limit adaptability to the diverse linguistic and practical needs of caregivers compared to AI-based systems. Lastly, caregiver digital literacy levels were not systematically assessed, though it has the possibility of having a profound impact on adoption levels.
Conclusion
The study provides an exploratory understanding of the needs of the caregivers of patients with mental illness after their discharge from psychiatric hospitals in Indonesia. Through these findings, the need for caregiver-focused intervention can be clearly seen in several aspects, including caregiving knowledge and skills, emotional burden, and availability of mental health care services. In addition, these needs are further transformed into a decision tree-based chatbot application prototype, representing a conceptual framework on how digital health could improve the availability of information and guidance for caregivers after patient discharge, especially in resource-constrained environments.
Further studies are needed to determine the feasibility, efficacy, and generalizability of the chatbot intervention. Issues related to digital literacy and cybersecurity should also be addressed when applying the chatbot intervention. The chatbot application, if improved and validated, would be a useful platform for mental health care provision in Indonesia and similar contexts.
Acknowledgments
This publication charge is funded by Unpad through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/ B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025). This paper and the research behind it would not have been possible without the exceptional support of IT programmer Rifaz Muhammad Sukma.
Disclosure
Mr Fajar Hermansyah reports a patent SIPAPAP MACO (Sistem Informasi Pendaftaran Penjadwalan Praktikan Mahasiswa Dan Co-Ass) licensed to EC002024208923/000781355. The authors report no other conflicts of interest in this work.
References
1. Prescott J. Digital technology to support mental health: a brief introduction to what it is and why it is important? Mental Health Social Inclusion. 2022;26(2):103–15. doi:10.1108/mhsi-02-2022-0010
2. Lim CT, Fuchs C, Torous J. Integrated digital mental health care: a vision for addressing population mental health needs. Int J Gen Med. 2024;Volume 17:359–365. doi:10.2147/ijgm.s449474
3. Ellis LA, Augustsson H, Grødahl AI, et al. Implementation of E-mental health for depression and anxiety: a critical scoping review. J Community Psychol. 2020;48:904–920. doi:10.1002/jcop.22309
4. Dowrick C, Kassai R, Lam CL, et al. The APEC digital hub-wonca collaborative framework on integration of mental health into primary care in the Asia Pacific. J Multidiscip Healthc. 2020. doi:10.2147/jmdh.s271070
5. Álvarez-jiménez M, Rice S, D’Alfonso S, et al. A novel multimodal digital service (moderated online social therapy+) for help-seeking young people experiencing mental ill-health: pilot evaluation within a national youth E-mental health service. J Med Internet Res. 2020. doi:10.2196/17155
6. Strudwick G, Kassam I, Torous J, Patenaude S. Building the infrastructure for sustainable digital mental health: it is “prime time” for implementation science. JMIR Ment Health. 2025;12:e78791–e78791. doi:10.2196/78791
7. McShane D, Madden AP, Kinsey L, Bífárìn O. Navigating challenges and shaping futures through mental health nursing in the United Kingdom. J Psychiatr Ment Health Nurs. 2024. doi:10.1111/jpm.13092
8. Torous J, Bucci S, Bell IH, et al. The growing field of digital psychiatry: current evidence and the future of apps, social media, chatbots, and virtual reality. World Psychiatry. 2021;20(3):318–335. doi:10.1002/wps.20883
9. Camacho E, Cohen A, Torous J. Assessment of mental health services available through smartphone apps. JAMA Netw Open. 2022;5(12):e2248784. doi:10.1001/jamanetworkopen.2022.48784
10. Shen N, Kassam I, Chen S, et al. Canadian perspectives of digital mental health supports: findings from a national survey conducted during the COVID-19 pandemic. Digit Health. 2022;8:205520762211022. doi:10.1177/20552076221102253
11. Ogugua JO, Okongwu CC, Akomolafe OO, Anyanwu EC, Daraojimba OD. Mental Health and digital technology: a public health review of current trends and responses. Int Med Sci Res J. 2024. doi:10.51594/imsrj.v4i2.754
12. Indrayanti I, Salsabila AK, Amrita V, Alhaddad MM, Saskia AB, Ramadhani DP. PsyBot: a randomized controlled trial of WhatsApp-based psychological first aid to reduce loneliness among 18–22-year-old students in Yogyakarta, Indonesia. SSM Mental Health. 2025;8. doi:10.1016/j.ssmmh.2025.100504
13. Rackoff GN, Zhang ZZ, Newman MG. Chatbot-delivered mental health support: attitudes and utilization in a sample of U.S. College students. Digit Health. 2025. doi:10.1177/20552076241313401
14. Abd-Alrazaq A, Alajlani M, Ali N, Denecke K, Bewick BM, Househ M. Perceptions and opinions of patients about mental health chatbots: scoping review. J Med Internet Res. 2021;23:e17828. doi:10.2196/17828
15. Glanz K, Rimer BK, Viswanath K. Health behavior theory, research and practice. Euro Univ Instit. 2015;2–5.
16. Mujahidah N, Yusdiana A. of Albert Bandura’s social-cognitive theories in teaching and learning. Edukasi Islam J Pendidik Islam. 2023;12(2):2131–2146.
17. Islam KF, Awal A, Mazumder H, et al. Social cognitive theory-based health promotion in primary care practice: a scoping review. Heliyon. 2023;9(4):e14889. doi:10.1016/j.heliyon.2023.e14889
18. Nadarzynski T, Miles O, Cowie A, Ridge D. Acceptability of Artificial Intelligence (AI)-led Chatbot services in healthcare: a mixed-methods study. Digit Health. 2019;5. doi:10.1177/2055207619871808
19. Abd-Alrazaq A, Alajlani M, Alalwan AA, Bewick BM, Gardner P, Househ M. An overview of the features of Chatbots in mental health: a scoping review. Int J Med Inform. 2019;132:103978. doi:10.1016/j.ijmedinf.2019.103978
20. Chauke TA, Obadire OS. The impact of school closures on learners. mental health in the context of COVID-19 in the city of cape town. Res Soci Sci Technol. 2024. doi:10.46303/ressat.2024.5
21. Syla LB. Perspectives of primary teachers, students, and parents on homework. Educ Res Int. 2023. doi:10.1155/2023/7669108
22. Clarke V, Braun V. Thematic analysis. J Positive Psychol. 2017;12(3):297–298. doi:10.1080/17439760.2016.1262613
23. Dossett LA, Kaji AH, Cochran A. SRQR and COREQ reporting guidelines for qualitative studies. JAMA Surg. 2021;156(9):875–876. doi:10.1001/jamasurg.2021.0525
24. Riduwan MB. Skala Pengukuran Variabel-Variabel Penelitian. Alfabeta; 2013.
25. Zhang J, Oh YJ, Lange P, Yu Z, Fukuoka Y. Artificial intelligence Chatbot behavior change model for designing artificial intelligence chatbots to promote physical activity and a healthy diet: viewpoint. J Med Internet Res. 2020;22:e22845. doi:10.2196/22845
26. Maenhout L, Peuters C, Cardon G, Compernolle S, Crombez G, DeSmet A. Participatory development and pilot testing of an adolescent health promotion Chatbot. Front Public Health. 2021;9. doi:10.3389/fpubh.2021.724779
27. Anderson JG, Summers AJ, Ahn S, et al. Digital health and caregiving resources used by family caregivers of older adults during the COVID-19 pandemic. J Fam Nurs. 2024. doi:10.1177/10748407241275897
28. Borghouts J, Eikey EV, Mark G, et al. Barriers to and facilitators of user engagement with digital mental health interventions: systematic review. J Med Internet Res. 2021. doi:10.2196/24387
29. Li N, Look KA. The association of caregiver characteristics and caregivers’ perceived difficulty in medication management tasks. Innov Pharm. 2022;13:16. doi:10.24926/iip.v13i1.4523
30. Oh YJ, Zhang J, Fang M-L, Fukuoka Y. A systematic review of artificial intelligence chatbots for promoting physical activity, healthy diet, and weight loss. Int J Behav Nutrit Physical Activity. 2021;18(1). doi:10.1186/s12966-021-01224-6
31. Litzelman K, Harnish A. Caregiver eligibility for support services: correlates and consequences for resource utilization. J Appl Gerontol. 2020. doi:10.1177/0733464820971134
32. Docrat S, Besada D, Cleary S, Daviaud E, Lund C. Mental health system costs, resources and constraints in South Africa: a national survey. Health Policy Plan. 2019. doi:10.1093/heapol/czz085
33. Ahmed T, Dumka N, Bhagat D, Hannah E, Kotwal A. Effect on essential health services during COVID-19 at the primary level in India. J Family Med Prim Care. 2022;11:5423–5429. doi:10.4103/jfmpc.jfmpc_390_22
34. Sheron VA, Shanmugathas S, Gooden TE, et al. Healthcare provider and patient perspectives on access to and management of atrial fibrillation in the northern province, Sri Lanka: a rapid evaluation of barriers and facilitators to care. BMC Health Serv Res. 2022;22. doi:10.1186/s12913-022-08440-1
35. Sasseville M, LeBlanc A, Tchuente J, et al. The impact of technology systems and level of support in digital mental health interventions: a secondary meta-analysis. Syst Rev. 2023;12. doi:10.1186/s13643-023-02241-1
36. Potts C, Lindström F, Bond R, et al. A multilingual digital mental health and well-being Chatbot (ChatPal): pre-post multicenter intervention study. J Med Internet Res. 2023;25:e43051. doi:10.2196/43051
37. Gaffney H, Mansell W, Tai S. conversational agents in the treatment of mental health problems: mixed-method systematic review. JMIR Ment Health. 2019;6:e14166. doi:10.2196/14166
38. Xu L, Sanders L, Li K, Chow JC. Chatbot for health care and oncology applications using artificial intelligence and machine learning: systematic review. JMIR Cancer. 2021;7:e27850. doi:10.2196/27850
39. Vaidyam A, Wisniewski H, Halamka J, Kashavan MS, Torous J. Chatbots and conversational agents in mental health: a review of the psychiatric landscape. Canadian J Psychiatry. 2019;(7):456–464. doi:10.1177/0706743719828977
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Potential Mobile Health Applications for Improving the Mental Health of the Elderly: A Systematic Review
Chou YH, Lin C, Lee SH, Chang Chien YW, Cheng LC
Clinical Interventions in Aging 2023, 18:1523-1534
Published Date: 14 September 2023
Telehealth in Cancer Care: A Qualitative Study of Nurses’ and Healthcare Professionals’ Perspectives in Indonesia
Kosasih CE, Fitri SUR, Sari EA, Platini H
Journal of Multidisciplinary Healthcare 2026, 19:597784
Published Date: 21 May 2026
Artificial Intelligence and Mental Health Services in Somalia: Opportunities and Health-System Considerations
Hussein AM, Yusuf FY
Journal of Multidisciplinary Healthcare 2026, 19:622655
Published Date: 10 July 2026