Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Artificial Intelligence and Mental Health Services in Somalia: Opportunities and Health-System Considerations
Authors Hussein AM ![]() , Yusuf FY
, Yusuf FY ![]()
Received 7 May 2026
Accepted for publication 4 July 2026
Published 10 July 2026 Volume 2026:19 622655
DOI https://doi.org/10.2147/JMDH.S622655
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Abdiwali Mohamed Hussein,1 Fathi Yasin Yusuf1,2
1Department of Psychiatry, Dr. Sumait Hospital, SIMAD University, Mogadishu, Somalia; 2Department of Public Health, Faculty of Medicine and Health Science, SIMAD University, Mogadishu, Somalia
Correspondence: Abdiwali Mohamed Hussein, Email [email protected]
Abstract: Somalia faces a substantial mental health treatment gap driven by severe workforce shortages, limited specialist services, and weak health-system infrastructure. Artificial intelligence (AI) is increasingly promoted as a tool to strengthen health systems, yet its application in low-resource and conflict-affected settings requires careful consideration of feasibility, governance, and equity. This commentary examines realistic opportunities for integrating AI into mental health research and service delivery in Somalia. It requires AI to be viewed as a system-support tool rather than a substitute for clinicians, with potential to strengthen task-shared primary care, supervision, referral pathways, and routine data use within the District Health Information Software 2 (DHIS2) platform. Examples of potential applications include WHO Mental Health Gap Action Programme (mhGAP)-aligned decision-support tools, automated data-quality checks, supervision dashboards, and mobile-based appointment reminders with privacy safeguards. Key constraints include uneven digital connectivity, affordability barriers, limited regulatory capacity, and evolving data protection frameworks under Somalia’s 2023 Data Protection Act. Ethical considerations such as confidentiality, stigma, algorithmic bias, and digital exclusion are highlighted, alongside the need for human in the-loop oversight and monitoring of performance across vulnerable groups. In low-resource settings such as Somalia, responsible AI integration requires feasibility, equity, and accountability. Successful implementation also requires alignment with existing health-system platforms, strong governance safeguards, measurable outcomes, and sustained investment in workforce capacity. When carefully deployed, AI can support but not replace mental health system strengthening in Somalia.
Keywords: artificial intelligence, mental health, Somalia, task-sharing, mhGAP, digital health, low-resource settings, health-system strengthening
Introduction
Artificial intelligence (AI) is increasingly being integrated into mental health care to support clinical decision-making, improve service delivery, strengthen health information systems, and enable data-driven planning. Applications such as clinical decision-support tools, automated symptom screening, predictive analytics, and digital mental health interventions have demonstrated potential to improve access, efficiency, and quality of care. However, their implementation also raises important ethical, legal, and governance challenges, including privacy, algorithmic bias, transparency, accountability, and equitable access, particularly in settings with limited digital infrastructure and regulatory capacity.1–6
In low-resource including Somalia, AI is increasingly viewed as a means of strengthening rather than replacing existing mental health services.1–5
Somalia’s mental health needs are substantial, yet service availability and specialist capacity remain constrained, creating a treatment gap. In this context, AI can support task-shared care by assisting non-specialist health workers through decision support, supervision, referral coordination, and improved use of routine health data, complementing clinicians and health-system investment.7,8
Additionally, public-sector specialist workforce is limited; national strategy documents and reviews have reported only three psychiatrists working in public facilities, with general practitioners often filling psychiatric roles. A recent study suggests that WHO Mental Health Gap Action Programme (mhGAP)-based training for front-line health workers can improve knowledge, skills, and readiness to manage mental, neurological, and substance use (MNS) conditions in primary care settings.7–10 These realities imply that the most feasible near-term AI applications are those that strengthen task-sharing, supervision, referral pathways, and continuity of care within primary care while keeping clinical decision-making accountable to trained providers.1,4,7–10
The major opportunities, associated risks, and implementation priorities are summarized in Table 1.
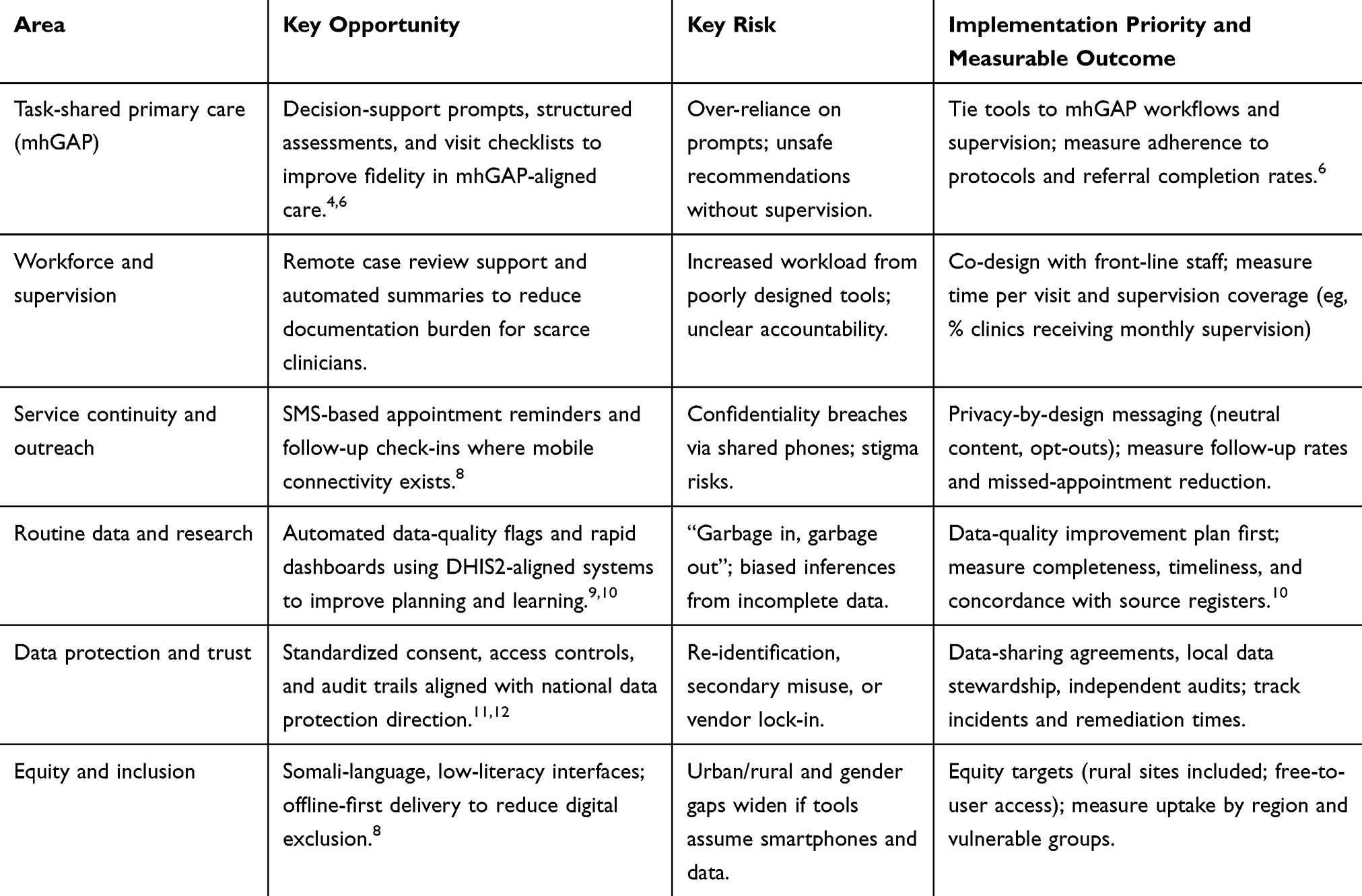 |
Table 1 AI for Mental Health Services in Somalia; Opportunities, Risks, and Implementation Priorities |
This commentary provides an evidence-informed conceptual analysis of the opportunities, risks, and implementation considerations for integrating artificial intelligence into mental health services in Somalia, drawing on existing literature and policy sources rather than primary empirical data. It does not present primary data or empirical results; rather, it synthesizes these sources into thematic and context-specific insights to inform policy and practice in Somalia.
Digital and Data Foundations
Somalia’s digital landscape is mobile-first; recent national digital profiles report growth in mobile connections and estimate that roughly three-quarters of connections are “broadband” (3G/4G/5G), which matters for app-based tools but does not guarantee reliable coverage or affordability for the poorest households. On the health-system side, Somalia has been implementing DHIS2 and related digital health initiatives, with explicit concern that coordination is needed to avoid fragmentation and duplication of electronic information systems. WHO’s assessment of Somalia’s health information system describes DHIS2 roll-out and notes that HIV, tuberculosis, and logistics data have been added as part of integrated disease surveillance and response efforts—an important signal that routine platforms exist, even if completeness and quality remain variable.8,10
For mental health research and service planning, the practical opportunity is not “big data”, but better use of small, routine data: AI-assisted data quality checks (missingness, implausible values), automated aggregation, and rapid-cycle dashboards for supervision and outreach—embedded within DHIS2-aligned workflows. Where patient-level AI tools are considered (eg, triage prompts, symptom check-ins), offline-first design (on-device processing, intermittent sync) and SMS/USSD fallbacks can reduce exclusion when smartphones, data bundles, or electricity are unreliable.9,10
Governance, Ethics, and Regulation
Somalia’s data governance capacity is evolving: the 2023 Data Protection Act establishes a national data protection authority and sets out its mandate and functions. Secondary commentary on implementation notes the authority’s formal launch in February 2024, indicating an emerging institutional home for privacy oversight—though practical enforcement capacity will take time to mature.11,13
Given the sensitivity and stigma often associated with mental health, Somalia should adopt a “minimum safe governance package” for any AI-enabled mental health tool: clear purpose limitation, data minimization, explicit consent where feasible, defined retention periods, and auditable access controls. These measures align with WHO’s guidance on ethics and governance of AI for health, including principles on autonomy, safety and public interest, transparency, accountability, equity, and sustainability. In fragile settings, ethical safeguards should also include: (1) explicit “do-no-harm” pathways for crisis content (self-harm, violence, abuse), (2) human-in-the-loop escalation to trained staff, and (3) model performance monitoring by sex, age, displacement status, literacy, and geography to detect systematic exclusion.13
Regulatory capacity is a binding constraint: procurement, certification, and post-market surveillance for software-based tools are often underdeveloped in low-resource systems. WHO’s AI governance guidance underscores the need for accountability across developers, implementers, and health authorities; in Somalia, that translates into simple, enforceable requirements—model cards, data sheets, version control, incident reporting, and independent evaluation—before scale-up.13
Abbreviations
AI, Artificial Intelligence; DHIS2, District Health Information Software 2; FMoH, Federal Ministry of Health; LMICs, Low- and Middle-Income Countries; MNS, Mental, Neurological and Substance use disorders; mhGAP, Mental Health Gap Action Programme; SMS, Short Message Service; USSD, Unstructured Supplementary Service Data; WHO, World Health Organization.
Acknowledgments
We express our sincere gratitude and deep appreciation to the Center of Research and Development, SIMAD University, for their guidance and recommendations.
Funding
The authors received Institutional Support from SIMAD University.
Disclosure
The authors declare no conflicts of interest in this case report.
References
1. World Health Organization. Ethics and Governance of Artificial Intelligence for Health. Geneva: World Health Organization; 2021.
2. Graham S, Depp C, Lee EE, et al. Artificial intelligence for mental health and mental illnesses: an overview. Curr Psychiatry Rep. 2019;21(11):116. doi:10.1007/s11920-019-1094-0
3. Shatte ABR, Hutchinson DM, Teague SJ. Machine learning in mental health: a scoping review of methods and applications. Psychol Med. 2019;49(9):1426–4. doi:10.1017/S0033291719001644
4. Torous J, Bucci S, Bell IH, et al. The growing field of digital psychiatry: current evidence and future directions. World Psychiatry. 2021;20(3):318–335. doi:10.1002/wps.20883
5. World Health Organization. Ethics and Governance of Artificial Intelligence for Health: Guidance on Large Multimodal Models. Geneva: World Health Organization; 2024.
6. Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med. 2019;25(1):44–56. doi:10.1038/s41591-018-0300-7
7. Ibrahim M, Rizwan H, Afzal M, Malik MR. Mental health crisis in Somalia: a review and a way forward. Int J Ment Health Syst. 2022;16. doi:10.1186/s13033-022-00525-y
8. Federal Ministry of Health Somalia. Somali Mental Health Strategy 2019–2022. Mogadishu: FMoH; 2019.
9. DIVA Portal. Training of front-line health workers in Somalia on mental health (mhGAP): effectiveness findings. 2025.
10. CHW Central. mhGAP training introduced in Somalia (2020) and outcomes summary. 2025.
11. Kemp S. Digital 2026: somalia. DataReportal; 2026. Available from: https://datareportal.com/reports/digital-2026-somalia.
12. World Health Organization Regional Office for the Eastern Mediterranean. Comprehensive Assessment of Somalia’s Health Information System. Cairo: WHO EMRO; 2024.
13. Federal Government of Somalia. Data Protection Act (Law No. 005 of 2023). Mogadishu: Federal Government of Somalia; 2023.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Adapting Artificial Intelligence Concepts to Enhance Clinical Decision-Making: A Hybrid Intelligence Framework
Hirosawa T, Suzuki T, Shiraishi T, Hayashi A, Fujii Y, Harada T, Shimizu T
International Journal of General Medicine 2024, 17:5417-5422
Published Date: 19 November 2024
Exploring Melasma Patients’ Needs Through Social Media: A Qualitative Study
Liu X, Liu X, Han Y, Cheng Y, Luo H, Liu Y, Li D, Guo W, Jiang H, Guo L, Jiang X
Patient Preference and Adherence 2025, 19:2333-2341
Published Date: 4 August 2025
Reimagining Mental Health with Artificial Intelligence: Early Detection, Personalized Care, and a Preventive Ecosystem
Mikaeili N, Naeim M, Narimani M
Journal of Multidisciplinary Healthcare 2025, 18:7355-7373
Published Date: 7 November 2025
Prostate Cancer Screening in Somalia: A Perspective on Addressing a Critical Gap in Early Detection
Serar Yusuf M, Mohamed Ali R
Research and Reports in Urology 2026, 18:602286
Published Date: 16 April 2026
The AI Health Arms Race: A Critical Perspective on Big Tech and the Widening Global Health Equity Gap
Ahmed MM, Othman ZK
Journal of Multidisciplinary Healthcare 2026, 19:610208
Published Date: 21 April 2026