Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Development of a PERMA-Based Intervention Program to Address Fear of Disease Progression in Systemic Lupus Erythematosus: A Delphi Consensus Study
Authors Wu W ![]() , Qu Z, Wang X, Xie X, Qiu X, Yang J
, Qu Z, Wang X, Xie X, Qiu X, Yang J
Received 26 November 2025
Accepted for publication 24 February 2026
Published 7 March 2026 Volume 2026:19 584552
DOI https://doi.org/10.2147/JMDH.S584552
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Charles V Pollack
Wenyan Wu,1 Zhixin Qu,2 Xiuli Wang,1 Xiaojuan Xie,1 Xiaomei Qiu,1 Jing Yang1
1Department of Rheumatology and Immunology, The Second Hospital of Shanxi Medical University, Taiyuan, 030001, People’s Republic of China; 2School of Nursing, Shanxi Medical University, Taiyuan, 030001, People’s Republic of China
Correspondence: Wenyan Wu, Department of Rheumatology and Immunology, The Second Hospital of Shanxi Medical University, No. 382 Wuyi Road, Taiyuan, Shanxi, 030001, People’s Republic of China, Email [email protected]
Purpose: To construct an intervention program based on the PERMA model to address fear of disease progression (FoP) among patients with systemic lupus erythematosus (SLE), aiming to develop a structured, consensus-based intervention protocol for future clinical testing and implementation.
Methods: This study established a multidisciplinary research team comprising twelve members. Drawing upon the PERMA model within positive psychology and incorporating a comprehensive literature review, the team formulated a preliminary intervention programme. Subsequently, through purposive sampling, sixteen external experts from relevant fields—including rheumatology, nursing, psychology, and healthcare management—were invited to participate in a Delphi consensus consultation. Following statistical analysis of their feedback, the intervention programme underwent optimisation and refinement before being finalised.
Results: The expert consultation achieved a high consensus (Kendall’s W = 0.56). The finalized intervention is an 8-week, multi-modal program structured around the five PERMA pillars. It comprises eight core themes, including psychoeducation on positive emotions, strengths identification, mindfulness-based engagement exercises, communication skills training for relationship enhancement, and meaning-making through narrative and film. Key weekly activities involve group discussions, the “Three Good Things” journaling, and role-playing. The program will be delivered via a combination of face-to-face sessions and WeChat-based support.
Conclusion: Through a structured Delphi consensus process, this study developed a PERMA-based intervention program designed to address fear of disease progression in patients with systemic lupus erythematosus. The program demonstrates strong expert endorsement, theoretical coherence, and practical relevance. It provides a systematically developed, consensus‑informed framework to guide future feasibility testing and clinical implementation. The actual effectiveness and feasibility of the intervention in reducing fear of progression await empirical evaluation in subsequent pilot and controlled studies.
Keywords: Delphi method, fear of progression, PERMA model, systemic lupus erythematosus
Introduction
Systemic lupus erythematosus (SLE) is a chronic, recurrent, and highly heterogeneous autoimmune disease that affects multiple organ systems. As a chronic systemic autoimmune disorder, SLE does not typically result in mortality directly from the disease itself, but rather from complications arising from disease activity or treatment-related factors. Existing research clearly indicates that mortality in SLE patients follows a “bimodal pattern”: the early mortality peak is primarily attributable to infections and disease activity, whilst the late mortality peak is predominantly driven by cardiovascular disease (CVD) stemming from atherosclerosis.1,2 SLE imposes a significant global burden characterized by high morbidity, increased mortality (particularly among young women), and substantial economic costs to healthcare systems and individuals.3,4 For instance, a nationwide study in China highlighted the considerable economic impact, with the average annual cost per patient being substantial.5 More critically than these aggregate burdens, the unpredictable, fluctuating nature of SLE, combined with its high recurrence rate and potential for cumulative organ damage, places a heavy and persistent physical and psychological burden on patients, who must constantly cope with the threat of disease relapse and its impact on daily life.6–8
Amid these challenges, negative emotions such as anxiety and depression are highly prevalent among patients with SLE, with fear of disease progression (FoP) being particularly prominent. FoP refers to patients’ fear and worry about the worsening of their disease or the emergence of new severe symptoms. It is a common psychological concern among individuals with chronic illnesses and often persists throughout the entire course of the disease.9 At present, there are no standardised clinical diagnostic criteria for fear of disease that possess clear diagnostic items and thresholds, as exist for depression or anxiety disorders. In research and clinical practice, it is primarily conceptualised as a continuous psychological construct and assessed using validated self-report scales. Among these, the Fear of Progression Questionnaire (FoP-Q) and its short form (FoP-Q-SF) are the most widely used assessment tools internationally.10,11 This scale quantifies the severity of fear by calculating a total score. Patients’ FoP levels are typically categorised as “mild”, “moderate”, or “severe” based on predefined cut-off values or percentile rankings, thereby enabling a graded assessment of severity. Among patients with SLE, FoP is not only a common psychological response but also exhibits particular clinical and humanistic significance due to its deep intertwining with disease uncertainty, multisystem involvement, and sociocultural contexts. The highly unpredictable course of SLE, characterised by symptom fluctuations, recurrence risks, and organ involvement uncertainty, significantly exacerbates patients’ anxiety about the future.12 Qualitative research further reveals that patients describe their disease experience as “permeated by sadness, fear, and suffering”, with societal lack of awareness amplifying their psychological burden.13 Moreover, FoP does not exist in isolation; it forms a vicious cycle with anxiety and depression, potentially adversely affecting SLE disease management.14,15 Prolonged and excessive FoP can lead to functional impairment, heightened negative emotions, reduced treatment adherence, and diminished quality of life (QoL), thereby adversely affecting disease management and prognosis. Consequently, FoP has been recognized as a major psychological stressor among patients with chronic diseases.16 For patients with SLE, FoP often extends beyond a rational level of concern and may evolve into a debilitating psychological distress, exerting significant negative effects on treatment compliance, functional status, and overall QoL.17–19 Without timely and effective intervention, excessive fear may create a vicious cycle in which psychological distress amplifies the perception of physical symptoms, potentially leading to poorer health outcomes.
In China, psychological interventions for patients with chronic diseases such as SLE have traditionally focused on alleviating pathological symptoms such as anxiety and depression. Although such interventions are essential, this deficit-oriented approach may be insufficient in cultivating patients’ positive psychological resources and resilience. In recent years, positive psychology has offered a valuable complementary perspective by shifting the focus of interventions toward the enhancement of individual strengths and well-being. The application of positive psychology aims to help individuals discover and develop internal positive resources—such as optimism, hope, resilience, and gratitude—to improve psychological adaptability and overall well-being.12
The PERMA model, proposed by Martin Seligman, provides an integrated framework for promoting human flourishing. It encompasses five core components: Positive Emotion, Engagement, Relationships, Meaning, and Accomplishment.11 Each of these elements contributes to well-being and can be independently pursued, defined, and measured.20 The model posits that by enhancing these key components, individuals can achieve positive psychological growth even in the face of adversity. In recent years, the PERMA framework has demonstrated its effectiveness in improving well-being and alleviating psychological distress among patients with cancer and other chronic illnesses.21–23 The PERMA framework was selected over other psychological models (eg, generic cognitive-behavioral therapy) for its proactive, strength-based approach. It directly counteracts the deficits-focused experience of FoP by systematically building positive resources: fostering Positive Emotion to counteract the affective component of fear;24 promoting Engagement to disrupt rumination on illness;25 strengthening Relationships to buffer against isolation;26 cultivating Meaning to reframe the illness narrative;27 and enhancing Accomplishment to rebuild self-efficacy undermined by disease uncertainty.24 This makes PERMA uniquely suited to not just reduce fear, but to promote flourishing amidst a chronic, unpredictable illness like SLE. Despite its potential, the structured application of the PERMA model as an intervention framework for SLE patients—particularly in addressing fear of disease progression (FoP)—remains largely unexplored.
Therefore, to bridge this critical gap in research and clinical practice, the present study aimed to systematically develop an evidence-based and targeted psychological intervention program grounded in the PERMA model. The primary goal was to establish a feasible and acceptable procedure to effectively alleviate FoP among SLE patients. It is anticipated that this program will enhance patients’ psychological adaptability, foster resilience, and ultimately improve their overall quality of life, providing a novel and positive approach to the comprehensive management of SLE.
Materials and Methods
Phase 1
Formation of the Research Team
A multidisciplinary research team was established, consisting of twelve members: one head nurse from the Department of Rheumatology and Immunology, seven rheumatology nurses, one rheumatologist, one psychotherapist, one data analyst, and one nursing postgraduate student. The principal investigator was responsible for expert selection, the design of the Delphi questionnaires, and overall project coordination. Other team members contributed according to their professional expertise, including drafting the preliminary intervention framework, distributing and collecting questionnaires, conducting statistical analyses, and summarizing the results.
This study was approved by the Ethics Committee of the Second Hospital of Shanxi Medical University (Approval No. [2024] YX-164).
Literature Review
A comprehensive literature search was conducted across eight Chinese and English databases, including PubMed, Web of Science, Embase, CINAHL (EBSCO), Chinese Biomedical Literature Database (CBM), China National Knowledge Infrastructure (CNKI), Wanfang Data, and VIP Database for Chinese Technical Periodicals.
The search terms included: systemic lupus erythematosus/lupus erythematosus, systemic/SLE/lupus erythematosus disseminates, PERMA/PERMA model/positive psychology/positive psychology Intervention, fear/fear of progression/fear of recurrence (the complete search strategies for all databases are provided in Supplementary Material 1). The search period extended from the inception of each database to May 2024.
Inclusion criteria were as follows:
- Studies focusing on psychological interventions based on the PERMA model;
- Intervention studies or descriptive studies on the design of positive psychology-based programs.
Exclusion criteria were:
- Duplicate publications;
- Full text unavailable;
- Non-Chinese or non-English articles.
Two reviewers independently screened and cross-checked all retrieved records according to the above criteria. Any disagreements were resolved through discussion with a third reviewer. This process was documented using a PRISMA-style flowchart (Figure 1), illustrating the study selection process from identification to final inclusion. A total of 48 studies published between 2010 and 2024 were included, comprising 10 English and 36 Chinese articles (Figure 1).
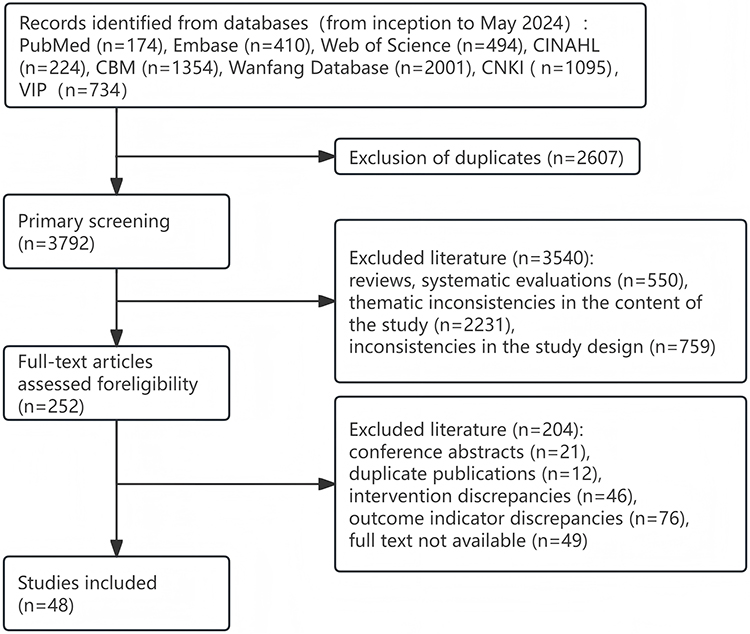 |
Figure 1 Literature screening process. |
Focus Group Interviews
Following the preliminary literature review, we conducted focus group interviews to ground the intervention content in patient experiences and needs. A convenience sample of 15 SLE patients was recruited from the outpatient clinic of our department. Eligible participants were adults (≥18 years) with a confirmed SLE diagnosis, able to communicate in Mandarin, and willing to provide informed consent. Each focus group comprised 6–8 patients and was facilitated by two trained researchers (one moderator, one note-taker) using a semi-structured interview guide designed to explore patients’ perceptions of disease-related fear, coping strategies, and their views on potential intervention components. Sessions lasted approximately 60–90 minutes, were audio-recorded with permission, and transcribed verbatim. Transcripts were analyzed using thematic analysis to identify key themes and concerns, which directly informed the initial draft of the intervention program. All participants provided written informed consentThis patient-engagement phase was instrumental in ensuring the intervention was grounded in the lived experience of the target population before proceeding to the formal expert consultation via the Delphi method. This process led to the preliminary development of the “PERMA-Based Intervention Program to Address Fear of Disease Progression Among Patients with Systemic Lupus Erythematosus”.
The preliminary draft consisted of eight core weekly themes (eg, psychoeducation on positive emotions, strength identification, mindfulness-based engagement, communication skills training, and meaning-making) and employed specific, standardized activities such as the “Three Good Things” journal, group discussions, and role-playing. The complete preliminary draft is available as Supplementary Material 2.
Phase 2: Selection of Delphi Panel
In accordance with the Delphi method procedure, a panel of 15–20 experts was selected. The inclusion criteria for experts were as follows:
- Research or work experience in psychology, nursing, management, or systemic lupus erythematosus (SLE);
- Bachelor’s degree or higher;
- Senior professional title;
- At least one previous experience in participating in a Delphi consultation.
A total of 16 experts were selected from Sichuan, Henan, Jiangxi, Zhejiang, Guangdong, Guizhou, and Shanxi provinces as the consultation panel for the Delphi process.
Round 1 of the Delphi Survey
From February to May 2024, the first round of the Delphi survey was conducted by sending the survey questionnaire to experts via WeChat documents or email. The questionnaire included three sections:
- Letter to Experts: This section explained the background, objectives, research methods, instructions for completing the questionnaire, the deadline for responses, and contact information.
- Indicator Content Consultation Form: This form included ratings of the importance of each indicator and space for suggested revisions. Experts were invited to evaluate each level and indicator individually. The importance and feasibility of each indicator were scored using a Likert 5-point scale ranging from “worst” to “best” (scores of 1 to 5). Experts were also asked to provide reasons for adding, removing, or modifying any indicators in the comment section.
- Expert Information Survey: This section collected demographic information and assessed the expert’s familiarity with the indicators and their judgment criteria. The demographic information included: age, education level, gender, professional title, and years of work experience. The level of familiarity of the experts was rated on a scale from “familiar” to “not familiar”, with values assigned as follows: 0.9 for familiar, 0.7 for somewhat familiar, 0.5 for neutral, 0.3 for not very familiar, and 0.1 for unfamiliar. The influence of the experts’ judgment was categorized into three levels: high, medium, and low, with corresponding values assigned for each. The weights were assigned as follows: practical experience (0.5, 0.4, 0.3), theoretical analysis (0.3, 0.2, 0.1), knowledge of domestic and international practices (0.1, 0.1, 0.1), and intuition (0.1, 0.1, 0.1).14
Round 2 of the Delphi Survey
After completing Round 1 of the Delphi survey, the research team collected the expert questionnaires and summarized the feedback. The analysis of the first-round expert responses and their opinions served as the basis for the second-round survey. Indicators with an importance score <3.5 or a coefficient of variation >0.3 were removed, and the second-round consultation questionnaire was revised according to the expert feedback. The second-round questionnaire was then sent to the experts using the same method. Based on the expert opinions collected in Round 2, the intervention program was adjusted and revised until a consensus was reached among the experts.
Statistical Methods
Data were entered and organized using Excel 2021, and statistical analysis was performed using SPSS 23.0 software. Continuous data were found to follow a normal distribution and are presented as mean ± standard deviation. Categorical data are expressed as frequency and percentage (%). The expert authority coefficient was expressed as the effective response rate of the questionnaire (%). The degree of consensus among expert opinions was assessed using the coefficient of variation and Kendall’s coefficient of concordance (Kendall’s W), with values ranging from 0 to 1. A higher value indicates a higher level of expert consensus. The degree of concentration of expert opinions was represented by the mean score and coefficient of variation of indicator importance. The expert authority coefficient (Cr) was calculated as the average of the judgment basis coefficient (Ca) and familiarity coefficient (Cs). A Cr value greater than 0.70 indicates high expert authority. A P-value of <0.05 was considered statistically significant.
Results
Demographics of the Expert Panel
A total of 16 experts were selected for the Delphi consultation in this study. The basic demographics of the expert panel are shown in Table 1.
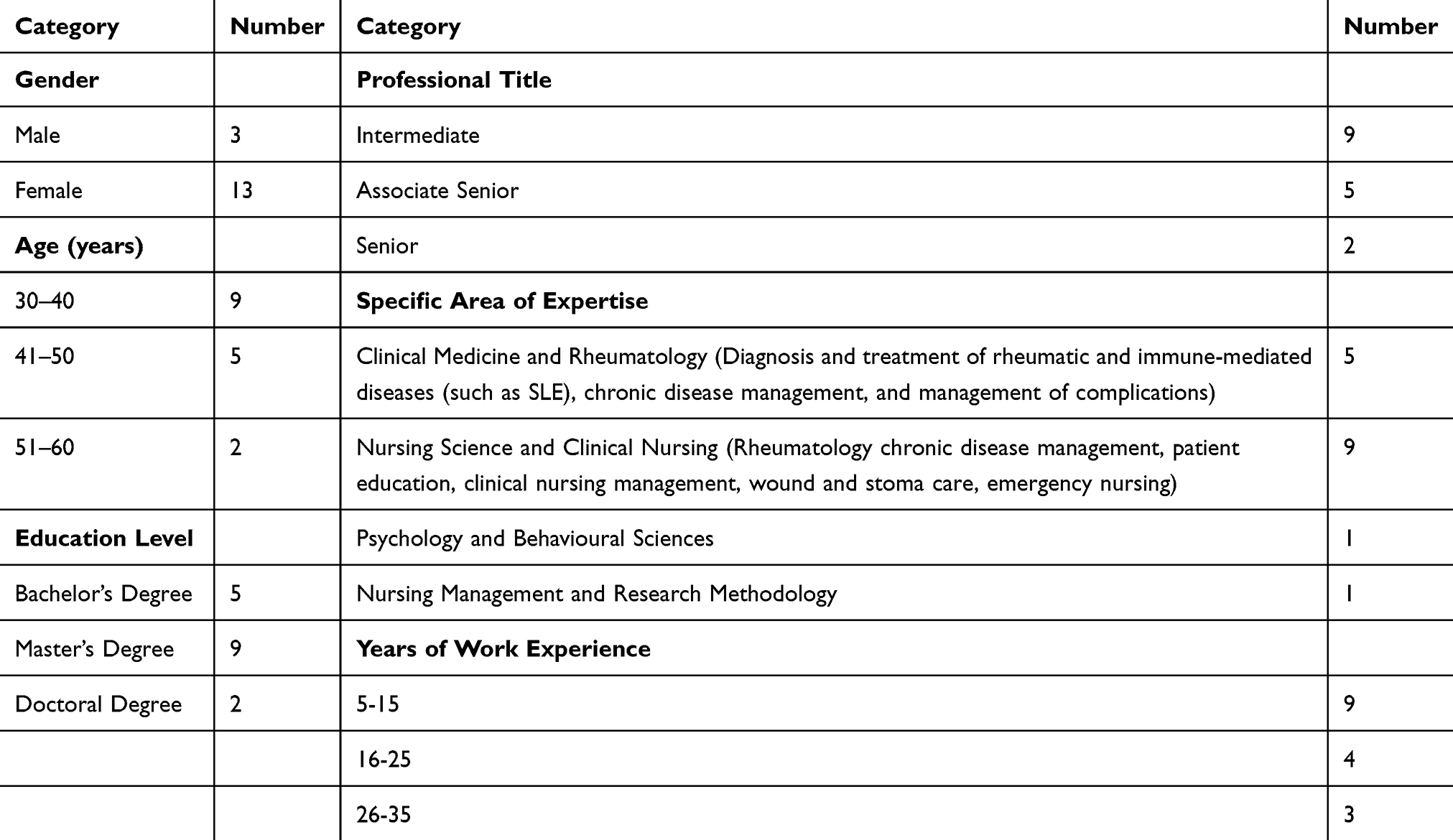 |
Table 1 Demographic Information of the 16 Delphi Experts |
Expert Consultation Results
Both rounds of the expert consultation achieved a 100% response rate (16 questionnaires distributed and returned in each round). The experts’ judgment coefficient (Ca) was 0.93, the familiarity coefficient (Cs) was 0.68, and the expert authority coefficient (Cr) was 0.81.
Round 1 Consultation: All 16 invited experts completed and returned the questionnaire. Among them, 14 experts (87.5%) provided specific qualitative feedback and suggestions for revision. The research team reviewed and summarized all comments and revised the items accordingly. The modifications primarily included three categories: (1) Addition of new items: Twelve items were added based on expert suggestions, such as incorporating a symbolic “flower seed distribution” activity in Week 1 and expanding emotion regulation techniques (eg, deep breathing, aromatherapy, expressive writing) in Week 2. (2) Revision of existing items: Six items were substantially revised, including adjusting the intervention frequency (one theme per week, with two sessions in Week 3) and extending the assessment schedule to include follow-ups at 1, 3, and 6 months after the intervention. (3) Item integration: One item was merged by combining the inclusion criteria for “research team members” and “rheumatology nurses.” Furthermore, based on quantitative ratings (importance score <3.5 or coefficient of variation >0.3), 5 items were deleted from the initial draft. The revised questionnaire containing 34 items was used for the second-round consultation. In this round, the Kendall’s coefficient of concordance (W) was 0.54 (P < 0.001) for item importance ratings and 0.33 (P < 0.001) for feasibility ratings.
Round 2 Consultation: All 16 questionnaires were returned again. The importance scores for all items ranged from 3.50 to 4.63, with coefficients of variation (CV) between 0.11 and 0.21. The feasibility scores ranged from 3.44 to 4.31, with CVs between 0.14 and 0.18. The Kendall’s coefficient of concordance (W) was 0.56 (P < 0.001) for importance ratings and 0.30 (P < 0.001) for feasibility ratings, indicating statistically significant consensus among the experts. Detailed scores for each item are provided in Table 2.
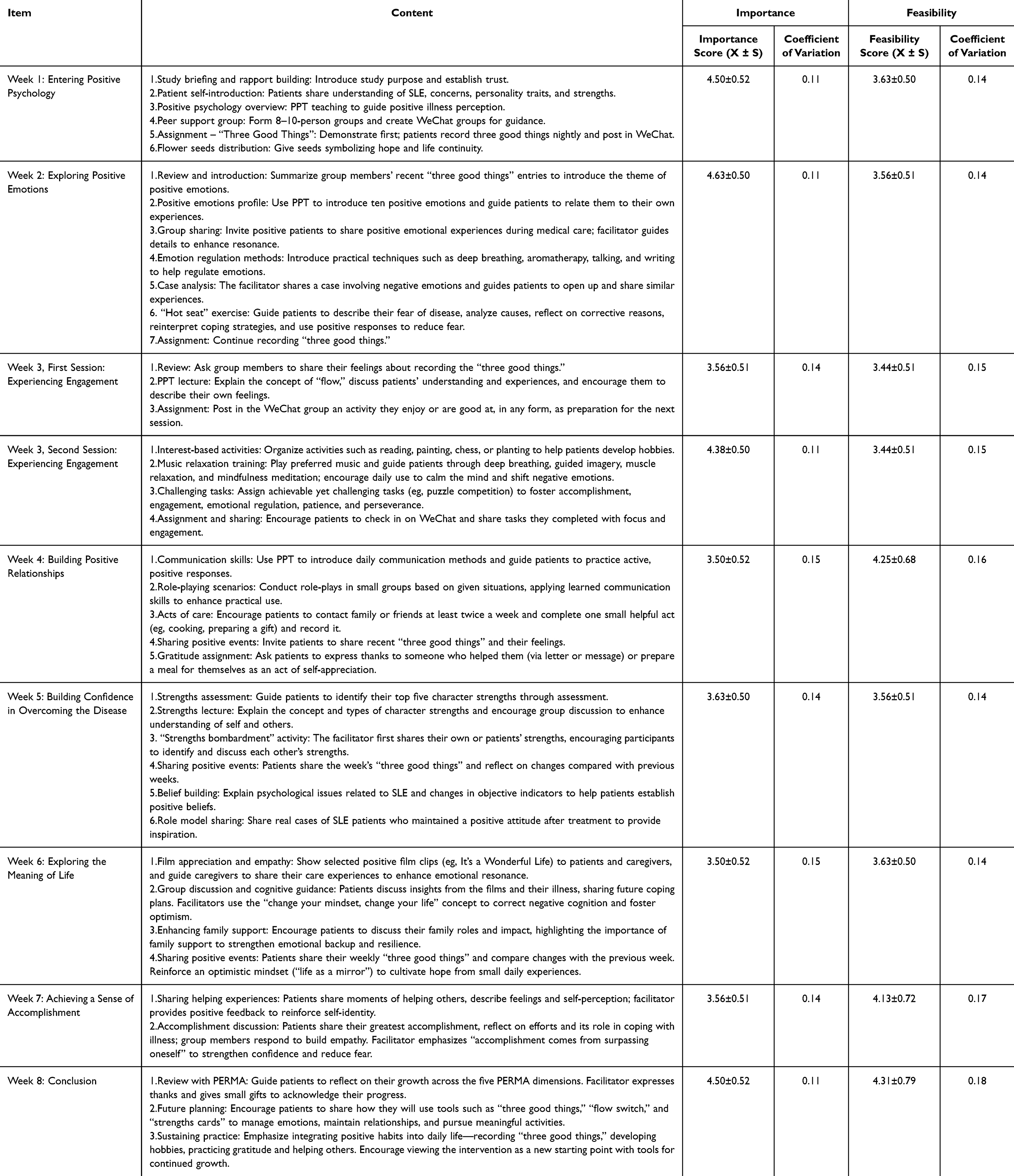 |
Table 2 Intervention Program |
Final Consensus and Program Finalization: Consensus was achieved on all items after two rounds. All items included in the final intervention program (Table 2) met the consensus criterion of an importance score ≥3.5, confirming their perceived value in addressing fear of progression. For a subset of these items, the feasibility score was below 3.5. These items were retained based on their theoretical criticality to the integrity of the PERMA model and the intervention’s active components. Expert qualitative feedback during the Delphi process emphasized that the clinical relevance and potential impact of these activities outweighed the anticipated practical challenges in delivery. It was acknowledged that the successful implementation of these specific components would require particular attention during facilitator training and might necessitate flexible adaptation in clinical practice. Ultimately, the finalized program comprised 8 themes and 28 specific intervention measures.
The details of the intervention program are as follows:
- Intervention Duration:
The intervention lasts 8 weeks, with one thematic module per week. Week 3 includes two sessions, while all other weeks include one session, resulting in a total of nine sessions. Each session lasts 60–90 minutes, during which patients are guided to complete related psychological exercises.
Researchers added patients as WeChat contacts and maintained communication after discharge through WeChat voice messages, texts, or phone calls, ensuring continuity of the intervention.
- Intervention Setting:
Sessions were conducted in the Rheumatology and Immunology Department office, which provides a quiet, comfortable, and distraction-free environment equipped with a projector.
- Intervention Format:
This study adopted an integrated blended model of intervention, combining structured face-to-face group sessions, individualized face-to-face counseling, WeChat-based educational content delivery, and online meeting support. All participants received the same core intervention protocol; no separate “online-only” or “offline-only” comparison groups were established.
The implementation process consisted of three sequential phases:
① Core In-Person Intervention Phase (Weeks 1–8): During hospitalization or outpatient visits, participants were divided into 7–8 groups, each comprising 8–10 patients and staffed with one physician and four nurses. Each group attended a structured, face-to-face session once per week in a quiet rheumatology and immunology department office, following the eight weekly themes (with two sessions in Week 3, totaling nine sessions). Each session lasted 60–90 minutes and included group discussions, simulation exercises, and individualized counseling.
② Extended Online Support Phase (Following the Core Weeks 1–8): After completing the core in-person phase, patients who chose to continue participation were invited to join a dedicated WeChat group corresponding to their original assigned small group. WeChat was selected as the primary online platform for the following reasons: its near-universal adoption in China ensures high accessibility and low technical barriers; its flexibility supports the sustained, long-term management crucial for a fluctuating chronic condition like SLE; and its integrated features (eg, group chats, push notifications) directly facilitate key intervention components. Specific online support included: (a) facilitating communication through WeChat group chats (each still moderated by one physician and four nurses); (b) delivering weekly summaries of intervention themes and detailed educational content via push notifications; and (c) assigning online tasks (eg, the “Three Good Things” journal) and providing incentives to enhance engagement and skill maintenance.
③ Sustained Individual Contact: Throughout the entire intervention process and beyond, researchers maintained contact with all participants via WeChat (voice messages, text) or phone calls. This ensured continuity of care, provided personalized feedback and encouragement, addressed ad-hoc questions, and thereby reinforced the intervention principles in daily life.
The online component (WeChat) was designed as a supplement and extension tool, not a replacement, aiming to consolidate learning outcomes, foster peer connectivity, and support the long-term application of positive psychology skills by patients between and after the formal face-to-face sessions.
- Qualifications of Intervention Providers:
1) Professional background in psychology, nursing, or management, or possession of recognized certification in psychological counseling, or research/clinical experience in SLE nursing. 2) ≥5 years of clinical experience in the rheumatology and immunology department. 3) Completion of standardized pre-intervention training conducted by the project leader, followed by a competency assessment to ensure consistency across providers.
- Assessment Time Points:
Assessments were conducted at five time points: Before the intervention, immediately after completion, 1 month, 3 months, and 6 months post-intervention.
- Evaluation Indicators:
Psychological: Fear of Progression scale; Subjective Well-Being scale; Brief Coping Inventory. Objective psychological: SAS, SDS, Quality of Life Assessment Scale. Physiological: SLEDAI score, complete blood count, urinalysis, ESR, complement C3, complement C4, and anti-dsDNA antibody levels.
The specific weekly intervention activities are detailed in Table 2.
Discussion
Importance and Holistic Nature of Developing a Fear-of-Progression Intervention for Systemic Lupus Erythematosus Patients Based on the PERMA Model
With continuous economic development and the improvement of living standards, people have increasingly emphasized not only physical health but also mental well-being. Both the Healthy China Action (2019–2030) and the “Healthy China 2030” Planning Outline call for strengthening humanistic care in medical services and enhancing the focus on mental health,28 with the goal of improving the psychological health literacy of the entire population. SLE patients are required to endure not only the physical pain and discomfort caused by the disease but also the psychological stress arising from its uncertainty and the potential for adverse outcomes. These related psychological issues must be given high priority.
The development of an intervention addressing fear of progression (FoP) in SLE patients is timely, aligning with broader calls for integrated biopsychosocial care. The PERMA model offers a structured, strengths‑based framework that may help counter the uncertainty and threat perception central to FoP. Its five components provide distinct, complementary pathways through which psychological resilience might be cultivated.
First, fostering Positive Emotion could serve as a counterweight to fear‑based preoccupations. While not directly tested here, prior theory suggests that cultivating positive affect may broaden cognitive‑behavioral repertoires and build psychological resources, which could, in turn, improve adaptation to chronic illness.29,30 Second, promoting Engagement in meaningful activities might help patients temporarily shift attention away from illness‑related rumination. The concept of “flow” provides a theoretical basis for this approach, though its direct impact on SLE‑specific distress requires empirical confirmation. Claims regarding potential neuroimmune modulation through engagement remain speculative and should be interpreted with caution until supported by direct evidence.31
Third, strengthening Relationships and social support is widely recognized as a buffer against illness‑related distress. For SLE patients, perceived support may mitigate feelings of isolation and helplessness that often fuel FoP.32,33 Fourth, exploring Meaning can facilitate cognitive reframing, allowing patients to integrate the illness experience into a broader, more coherent life narrative. This process may help reduce the threat salience of SLE.34 Finally, supporting experiences of Accomplishment—even small, personalized successes—could enhance self‑efficacy, a key psychological resource for managing chronic disease.35
Scientific Rigor and Reliability of the PERMA-Based Intervention for Reducing Fear of Disease Progression in Patients with Systemic Lupus Erythematosus
The development process adhered to established Delphi methodology. On one hand, the study employed purposive sampling to strictly select 16 qualified experts from tertiary hospitals across seven provinces and autonomous regions in China. All selected experts held intermediate or higher professional titles and had over 5 years of clinical or academic experience. Their professional backgrounds spanned nursing psychology, clinical nursing, clinical medicine, and other related fields. This selection strategy not only ensured a broad geographical distribution of experts but also provided diversity in professional fields, guaranteeing the authority and representativeness of expert opinions while minimizing the limitations of a single disciplinary perspective.
On the other hand, both rounds achieved a 100% response rate. The authority coefficient (Cr=0.81) exceeded the recommended threshold of 0.70, indicating satisfactory expert credibility. Consensus was statistically significant for importance ratings across rounds (Kendall’s W=0.54 in Round 1, 0.56 in Round 2; both p<0.001). These metrics support the rigor of the consensus‑building process and the content validity of the resulting framework.
Limitations
This study has several limitations that should be acknowledged. First, the primary outcome is a theoretically and expert-informed intervention protocol, not its empirical evaluation. While developed through a rigorous Delphi process, the clinical efficacy and effectiveness of this PERMA-based program in reducing fear of progression among SLE patients remain to be tested in future feasibility studies and randomized controlled trials.
Second, potential biases exist in the expert selection process. Although we aimed for diversity, all experts were from Chinese tertiary hospitals, which may limit the generalizability of the findings to other healthcare settings or cultural contexts. Furthermore, the panel’s composition, heavily weighted towards nursing (11/16), while ensuring practical relevance, might have introduced a perspective bias that prioritized nursing care models over, for instance, purely psychological or patient-led approaches.
Third, limitations inherent to the Delphi method itself should be considered. The consensus achieved does not necessarily equate to objective correctness, and the process may sometimes suppress divergent or innovative minority opinions. Additionally, the structured feedback rounds, while improving convergence, rely on the subjective judgment of the selected experts.
Despite these limitations, this study provides an essential, consensus-based foundational step by developing a structured, theory-driven intervention. The clear limitations outlined here directly inform the necessary next steps: pilot testing and rigorous empirical validation.
Conclusion
This study provides a systematically developed, expert‑endorsed framework for a PERMA‑based intervention targeting FoP in SLE. Its value lies in offering a structured, theory‑informed starting point for subsequent empirical research. Future work should focus on pilot testing, adaptation, and rigorous evaluation of the program’s feasibility, acceptability, and preliminary effects.
Data Sharing Statement
The data used and/or analyzed during the current study are available from the corresponding author.
Ethics Statement
This study was approved by the Ethics Committee of the Second Hospital of Shanxi Medical University (Approval No. [2024] YX-164). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Funding
This study was supported by the Hospital Fund Project of the Second Hospital of Shanxi Medical University (Grant No. 202403-3).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Liu X, Wang C, Guan X. Mitochondrial dysfunction is a potential key mechanism for atherosclerosis predisposition in patients with systemic lupus erythematosus. J Autoimmun. 2025;157:103488. doi:10.1016/j.jaut.2025.103488
2. Yennemadi AS, Jordan N, Diong S, Keane J, Leisching G. The link between dysregulated immunometabolism and vascular damage: implications for the development of atherosclerosis in systemic lupus erythematosus and other rheumatic diseases. J Rheumatol. 2024;51(3):234–13. doi:10.3899/jrheum.2023-0833
3. Tian J, Zhang D, Yao X, et al. Global epidemiology of systemic lupus erythematosus: a comprehensive systematic analysis and modelling study. Ann Rheumatic Dis. 2023;82(3):351–356. doi:10.1136/ard-2022-223035
4. Etchegaray-Morales I, Mendoza-Pinto C, Munguía-Realpozo P, et al. Systemic lupus erythematosus, a leading cause of death in young Mexican females: a nationwide population-based study, 2000–2020. Rheumatol Int. 2022;42(10):1715–1720. doi:10.1007/s00296-022-05154-9
5. Li M, Li C, Cao M, et al. Incidence and prevalence of systemic lupus erythematosus in urban China, 2013–2017: a nationwide population-based study. Sci Bull. 2024;69(19):3089–3097. doi:10.1016/j.scib.2024.04.075
6. Frade-Sosa B, Sarmiento-Monroy JC, Bruce IN, et al. Dual B-cell targeting in systemic lupus erythematosus: the role of combined and sequential therapy with rituximab and Belimumab. Autoimmunity Rev. 2025:103837. doi:10.1016/j.autrev.2025.103837
7. Parodis I, Lindblom J, Levy RA, et al. Attainment of remission and low disease activity after treatment with belimumab in patients with systemic lupus erythematosus: a post-hoc analysis of pooled data from five randomised clinical trials. Lancet Rheumatol. 2024;6(11):e751–e761. doi:10.1016/S2665-9913(24)00162-0
8. Todd J, Pickup B, Coutts-Bain D. Fear of progression, imagery, interpretation bias, and their relationship with endometriosis pain. Pain. 2023;164(12):2839–2844. doi:10.1097/j.pain.0000000000003003
9. Meissner VH, Olze L, Schiele S, et al. Fear of cancer recurrence and disease progression in long-term prostate cancer survivors after radical prostatectomy: a longitudinal study. Cancer. 2021;127(22):4287–4295. doi:10.1002/cncr.33836
10. Mazhariazad F, Dianati M, Taghadosi M, Zamani B. Uncertainty and its related coping strategies in systemic lupus erythematosus. Life in the fog. J Educ Health Promot. 2023;12:233. doi:10.4103/jehp.jehp_1080_22
11. Souza RR, Marcon SS, Teston EF, et al. From diagnosis to complications: experiences of those who live with systemic lupus erythematosus. Rev Bras Enferm. 2022;75(4):e20200847. doi:10.1590/0034-7167-2020-0847
12. Addis SG, Dires A, Goshiye D, et al. Fear of disease progression and related factors among chronic disease patients attending South Wollo zone government hospitals. Sci Rep. 2025;16(1):140. doi:10.1038/s41598-025-28868-9
13. Lew D, Huang X, Kellahan SR, Xian H, Eisen S, Kim AHJ. Anxiety symptoms among patients with systemic lupus erythematosus persist over time and are independent of SLE disease activity. ACR Open Rheumatol. 2022;4(5):432–440. doi:10.1002/acr2.11417
14. Zen M, Salmaso L, Amidei CB, et al. Mortality and causes of death in systemic lupus erythematosus over the last decade: data from a large population-based study. Eur J Internal Med. 2023;112:45–51. doi:10.1016/j.ejim.2023.02.004
15. Lebel S, Mutsaers B, Tomei C, et al. Health anxiety and illness-related fears across diverse chronic illnesses: a systematic review on conceptualization, measurement, prevalence, course, and correlates. PLoS One. 2020;15(7):e0234124. doi:10.1371/journal.pone.0234124
16. Ocalewski J, Michalska P, Izdebski P, et al. Fear of cancer progression and health behaviors in patients with colorectal cancer. Am J Health Behav. 2021;45(1):138–151. doi:10.5993/AJHB.45.1.11
17. Coutts-Bain D, Sharpe L, Techakesari P, et al. A mixed-methods review and meta-synthesis of fears of recurrence and progression in people with mental health conditions. Clinic Psychol Rev. 2023;105:102342. doi:10.1016/j.cpr.2023.102342
18. Wang X, Jiang N, Chen S, et al. Fear of progression in patients with acute myocardial infarction: a cross-sectional study. BMC Nurs. 2024;23(1):866. doi:10.1186/s12912-024-02552-1
19. Sharpe L, Menzies RE, Boyse J, et al. Mediators and moderators of two online interventions for managing pain, fear of progression and functional ability in rheumatoid arthritis. Behav Res Ther. 2025;185:104676. doi:10.1016/j.brat.2024.104676
20. Moustafa AT, Moazzami M, Engel L, et al. Prevalence and metric of depression and anxiety in systemic lupus erythematosus: a systematic review and meta-analysis. In Seminars in Arthritis and Rheumatism: 2020. Elsevier; 2020:84–94.
21. Tisseverasinghe A, Peschken C, Hitchon C. Anxiety and mood disorders in systemic lupus erythematosus: current insights and future directions. Curr Rheumatol Rep. 2018;20(12):85. doi:10.1007/s11926-018-0797-2
22. Seligman MEP, Csikszentmihalyi M. Positive psychology: an introduction. In: Flow and the Foundations of Positive Psychology: The Collected Works of Mihaly Csikszentmihalyi. edn: Springer; 2014:279–298.
23. Qu SM, Qi XX, Li Q, et al. Effects of positive psychological intervention in patients with permanent enterostomy. Chin J Nurs. 2024;59(12):1422–1428. doi:10.3761/j.issn.0254-1769.2024.12.002
24. Schlebusch L, Chambers N, Rosenstein D, et al. Supporting caregivers of children with developmental disabilities: findings from a brief caregiver well-being programme in South Africa. Autism. 2024;28(1):199–214. doi:10.1177/13623613221133182
25. Luo L, Li Y, Zhou Z, et al. Study on the effect of positive psychological intervention based on PERMA model on perioperative patients with AIDS complicated with breast cancer. Comput Math Methods Med. 2022;2022(1):9788122. doi:10.1155/2022/9788122
26. Salsman JM, McLouth LE, Cohn M, et al. A web-based, positive emotion skills intervention for enhancing posttreatment psychological well-being in young adult cancer survivors (EMPOWER): protocol for a single-arm feasibility trial. JMIR Res Protocol. 2020;9(5):e17078. doi:10.2196/17078
27. Tu M, Wang F, Shen S, et al. Influences of psychological intervention on negative emotion, cancer-related fatigue and level of hope in lung cancer chemotherapy patients based on the PERMA framework. Iran J Public Health. 2021;50(4):728. doi:10.18502/ijph.v50i4.5997
28. Wang N, Li YX, Jiao H, et al. Visual analysis of mental health research on Covid-19 based on CiteSpace. Proceed Clin Med. 2021;30(10):736–740. doi:10.16047/j.cnki.cn14-1300/r.2021.10.004
29. Silva-Ribeiro S, Godinho CA, Camilo C, et al. Psychological, social and behavioural factors associated with disease/illness activity and adjustment to lupus: a systematic review and meta-analysis. Health Psychol Rev. 2025:1–35. doi:10.1080/17437199.2025.2478877
30. Wang Y, Yu ZY. Chain mediating role of psychological resilience and emotional balance between daily stress and depression in adolescents. Chin J Child Health Care. 2023;31(09):1033–1037. doi:10.11852/zgetbjzz2023-0098
31. Abernathy-Close L, Lazar S, Stannard J, et al. B cell signatures distinguish cutaneous lupus erythematosus subtypes and the presence of systemic disease activity. Front Immunol. 2021;12:775353. doi:10.3389/fimmu.2021.775353
32. Zheng W, Hu M, Liu Y. Social support can alleviate the fear of cancer recurrence in postoperative patients with lung carcinoma. Am J Transl Res. 2022;14(7):4804.
33. Ban Y, Li M, Yu M, et al. The effect of fear of progression on quality of life among breast cancer patients: the mediating role of social support. Health Qual Life Outcomes. 2021;19(1):178. doi:10.1186/s12955-021-01816-7
34. Moroni L, Mazzetti M, Ramirez GA, et al. Beyond neuropsychiatric manifestations of systemic lupus erythematosus: focus on post-traumatic stress disorder and alexithymia. Curr Rheumatol Rep. 2021;23(7):52. doi:10.1007/s11926-021-01019-5
35. Geertsema-Hoeve BC, Sickinghe AA, van Schaik-Mast SJ, et al. The effects of lifestyle interventions on disease activity and quality of life in patients with systemic lupus erythematosus: a systematic review. Autoimmunity Rev. 2024;23(10):103609. doi:10.1016/j.autrev.2024.103609
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.