Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Development of a Patient-Centered Daily Foot Self-Care Protocol for High-Risk Diabetic Foot Patients Based on Checklist Management Model: A Delphi Study
Authors Lin X, Chen X, Li Y, He S, Xie H, Zhuo Y, Zhang L, Zhou X
Received 22 July 2025
Accepted for publication 15 December 2025
Published 3 February 2026 Volume 2026:19 545241
DOI https://doi.org/10.2147/DMSO.S545241
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ernesto Maddaloni
Xiaodan Lin,1 Xianghao Chen,1 Yuantian Li,2 Shumin He,3 Haidan Xie,1 Yiting Zhuo,1 Leting Zhang,1 Xiaozhou Zhou4
1School of Nursing, Guangdong Pharmaceutical University, Guangzhou, Guangdong, 510315, People’s Republic of China; 2Department of Endocrinology, The First Affiliated Hospital of Guangdong Pharmaceutical University, Guangzhou, Guangdong, 510080, People’s Republic of China; 3Wound and Ostomy Center, The First Affiliated Hospital of Guangdong Pharmaceutical University, Guangzhou, Guangdong, 510080, People’s Republic of China; 4Department of Nursing, The First Affiliated Hospital of Guangdong Pharmaceutical University, Guangzhou, Guangdong, 510080, People’s Republic of China
Correspondence: Xiaozhou Zhou, Department of Nursing, The First Affiliated Hospital of Guangdong Pharmaceutical University, No. 19, Nonglinxia Road, Yuexiu District, Guangzhou, Guangdong Province, 510080, People’s Republic of China, Tel +86-13622268608, Email [email protected]
Background: The International Diabetic Foot Working Group emphasizes that daily foot self-care is a critical measure for preventing diabetic foot ulcers, with patients serving as the primary implementers. However, there is a notable lack of patient-centered, specific, and actionable care management plans. This study aims to develop a scientifically sound, standardized, and practical daily foot self-care protocol for high-risk diabetic foot patients based on the checklist management model.
Methods: This study was conducted in two sequential phases. First,a preliminary draft of the foot self-care program was developed through a comprehensive literature review and semi-structured interviews with healthcare professionals and patients. Subsequently, from December 2024 to January 2025, the Delphi method was employed to conduct two rounds of expert consultation with 17 specialists, during which the indicators were screened and refined based on predefined criteria.
Results: In the first and second rounds of expert consultations, 18 and 17 questionnaires were distributed, respectively, with 17 valid responses returned each round, yielding effective response rates of 94.44% and 100%. The expert authority coefficient was 0.93, indicating high credibility. The Kendall’s harmony coefficients were 0.168 and 0.272 (p< 0.001), reflecting improved consensus across rounds. In the second round, the coefficient of variation ranged from 0 to 0.16, with all items below the 0.25 threshold. The final self-care plan comprises 5 primary indicators (self-foot examination, foot hygiene care, shoe and sock selection, daily precautions, and daily foot self-care flowchart) and 27 secondary indicators.
Conclusion: The self-care plan developed using the checklist management model is scientifically grounded, targeted, and feasible. It provides a structured basis for effective and standardized self-care among high-risk diabetic foot patients, However, it is essential to note that this protocol is still in the developmental stage and requires further clinical validation to assess its practical effectiveness and implementation feasibility.
Keywords: diabetes high-risk feet, self-care, checklist management model, Delphi method
Introduction
Diabetic foot (DF) represents one of the most severe and costly chronic complications of diabetes,1 with diabetic foot ulcers (DFUs) being its most common manifestation.2,3 Against the backdrop of rising global diabetes prevalence, the number of DF cases is increasing accordingly.4 Statistics indicate that the annual mortality rate for patients with diabetic foot ulcers is as high as 11%, escalating to 22% for those requiring amputations.1,5 The International Working Group on the Diabetic Foot (IWGDF) has emphasizes that with effective prevention, early detection, and proactive management, over 90% of amputations could be avoided.6 This highlights the paramount importance of preventative foot self-care, for which patients themselves are the primary actors.7,8
However, a significant gap exists between this recognized importance and the reality of patient self-care.9,10 The overall level of foot self-care among at-risk patients remains suboptimal.11,12 The core scientific problem we identify is that current management approaches often fail to translate guideline recommendations into sustained, correct self-care behaviors by patients.11–13
Several limitations persist in existing diabetic foot management plans. Firstly, many protocols are predominantly designed from the healthcare provider’s perspective, overlooking patient autonomy and the cultivation of self-management capabilities.11,12,14 This top-down approach has resulted in insufficient verification of patient compliance and the generalizability of plan effectiveness.15,16 Secondly, while traditional health education interventions are somewhat effective in knowledge dissemination, they demonstrate limited success in fostering long-term behavioral change and adherence.17,18 Furthermore, international guidelines like those from the IWGDF,6,19 while comprehensive, often present principle-based recommendations rather than specific, actionable, step-by-step instructions that are easy for patients to follow and integrate into daily life.20 Consequently, nurses and patients alike lack a standardized, patient-centric, and highly operational tool to bridge the gap between knowledge and practice.
In recent years, the patient-centered care philosophy has gained well-deserved attention. This concept prioritizes the patient’s perspective, addressing their needs, decision preferences, and treatment goals to optimize care processes and outcomes.21 Simultaneously, the checklist management model has emerged as a powerful, structured tool in healthcare. It ensures all critical items are considered and completed, showing distinct advantages in improving compliance and reducing errors across various medical fields.22,23 Its application in diabetic foot care holds the potential to simplify complex procedures into manageable, executable steps.
Therefore, this study aims to develop a patient-centered, standardized daily foot self-care protocol for high-risk diabetic foot patients based on the checklist management model. Our research focuses explicitly on the development and consensus-building phase. By systematically integrating evidence, patient insights, and expert opinion via the Delphi method, we seek to create a foundational protocol that is not only scientifically sound but also practical and acceptable The ultimate goal is to provide a clear, structured reference for patients and nurses, thereby enhancing self-care behaviors, delaying the progression of foot lesions, reduceing amputation risk, and improving patients’ quality of life.24,25
Method
Study Design
This study used an improved Delphi method to collect expert opinions on daily foot self-care plans for patients with high-risk diabetic feet.26,27 The study was divided into two distinct phases: the first phase was the preparation phase, where the initial draft of the daily foot self-care plan for high-risk diabetic feet patients was developed through a combination of literature review and semi-structured interviews; the second phase was the Delphi survey phase, where a Delphi questionnaire was designed based on the initial draft framework, and two rounds of expert consultations were conducted to reach a consensus. The Delphi method, as a systematic expert consultation approach, typically collects opinions from recognized experts in the field through multiple rounds of questionnaire surveys to determine best practice solutions.28 This stepwise approach ensured the systematic and rigorous development of the protocol.
Development of the Preliminary Daily Foot Self-Care Plan
Literature Review
A comprehensive and systematic search was conducted on PubMed, Embase, Cochrane Library, Web of Science, China National Knowledge Infrastructure (CNKI), China Biomedical Database (CBM), WanFang Data, and the VIP Journal Resource Integration Service Platform (VIP), retrieving clinical practice guidelines, randomized controlled trials, quasi-experimental studies, and qualitative research related to foot self-management behavior from the past decade. The main search terms are “Diabetic Foot OR Foot Diabetic OR Diabetic Feet OR Feet Diabetic OR Foot Ulcer Diabetic OR Foot ulcers at-risk patients with diabetes OR Foot ulcers Diabetes foot ulcer OR Diabetic foot disease OR Diabetic foot ulcers”; “Foot self-examination OR Foot care OR Foot screening”; “Self Care OR Care Self OR Self-Care OR Self-management OR Self-care behaviors OR Self-care practices OR Self-management”. To ensure the reliability and accuracy of the daily foot self-care plan for patients at high risk of diabetic foot, the plan content was derived from scales with good reliability and validity, as well as published articles. This study first screened the foot care behaviors and knowledge scales for diabetic foot patients, ultimately selecting two mature scales as the framework for the plan: the Chinese version of the Nottingham Foot Care Assessment Scale and the Foot Care Knowledge Scale for Diabetic Patients.29,30 The remaining content was sourced from relevant studies on preventive behaviors for diabetic ulcers.19,31,32 To enhance clarity for end-users regarding correct nail trimming, a visual reference (Figure 1) was added to Item 7 (“Nail Trimming”) within the foot inspection dimension of the plan. Furthermore, to clearly illustrate the plantar temperature measurement areas, a corresponding diagram (Figure 2) was incorporated into Item 10 (“Plantar Temperature Measurement”) of the same dimension. Through literature reviews and team discussions,19,32,33 a preliminary list of daily foot self-care measures for patients with high-risk diabetic feet has been developed, comprising four dimensions and 20 items, as detailed in Supplementary Material S1, Part A.
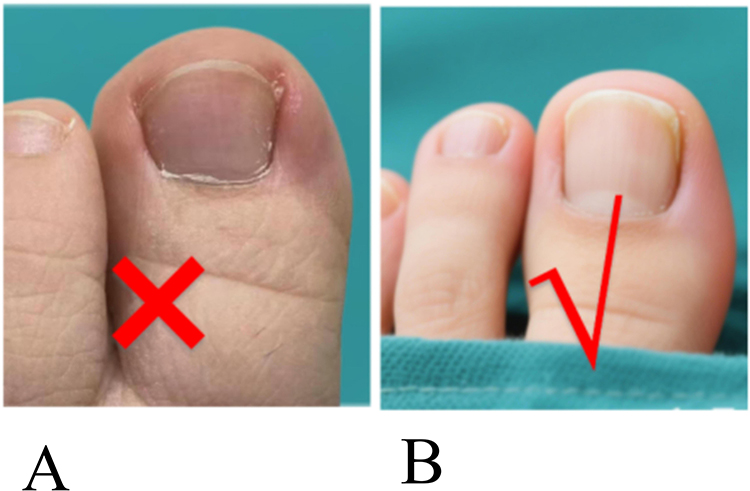 |
Figure 1 Schematic diagram of toenail trimming status for patients with diabetic high-risk feet. (A) Rounded toenails. (B) Toenails properly trimmed. |
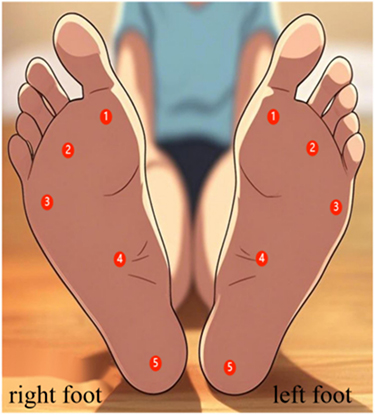 |
Figure 2 Schematic diagram of foot skin temperature measurement areas for patients with diabetic high-risk feet. |
Semi-Structured Interview
Purposeful sampling was adopted, and interviews were conducted until data saturation was reached.34 In-depth interviews were carried out with 2 chief physicians, 2 associate chief physicians, 3 attending physicians, 1 resident physician, 2 senior nurses, 3 nurses, and 6 patients from the endocrinology department and the wound and ostomy outpatient clinic of a Grade III Class A hospital in Guangzhou, China. Data saturation was determined when subsequent interviews no longer yielded new themes and information repetition reached a stable state, at which point the inclusion of new participants was ceased. The goal was to understand the cognition and needs of diabetic foot patients in developing daily self-care behaviors for their feet. The interview outline was determined through literature review35 and multiple internal discussions within the research team. The interview outline for healthcare professionals included the following questions: (1) What common foot self-care problems or difficulties have you observed in patients you encounter? (2) In your daily work, what common misconceptions have you noticed among patients when performing foot self-care? (3) What urgent educational needs do you think patients have regarding foot self-care? (4) Based on your observations, if you give patients the self-care instructions for their feet, do they generally follow these suggestions for foot self-care? Why? (5) What areas do you think need to be added or modified in the foot self-care content? The interview outline for patients included: (1) Do you know what foot self-care is? (2) How do you usually perform foot self-care? (3) What difficulties or challenges have you encountered during the self-care of your feet? (4) How do you think foot self-care content helps in taking care of your feet? (5) Within the self-care content for feet, which aspects do you find particularly useful, less practical, or difficult to implement? What are the reasons? (6) Do you have any suggestions for improving self-care content for diabetic foot patients? The recorded interview were transcribed within 24 hours after the interview ended, and based on the extracted themes, the first draft of the daily foot self-care plan was refined. During the semi-structured interviews, some patients reported an inability to identify diabetes-related foot problems. Concurrently, some healthcare professionals suggested incorporating images to clearly illustrate these conditions for patients. They also recommended establishing a time-based foot care routine: “check shoes and socks before going out → check for wounds after returning home → check between toes before sleep.” Additionally, the professionals highlighted that improper nail trimming includes not only cutting “too rounded” but also cutting “too short”. Following literature reviews and team discussions,36–38 the plan was subsequently modified. Images of diabetes-related foot problems were added to Item 7 (“Foot Inspection”) under the “Foot Inspection” dimension (see Figure 3), and the illustration for nail trimming was updated in Item 16 (“Other”) under the “Other” dimension (see Figure 4). Furthermore, a new dimension, “Foot Self-examination Flowchart,” was introduced, with the detailed flowchart presented in Figure 5. Other refinements included adding indicators such as blood sugar monitoring, modifying methods for keeping toe spaces dry, reasons for behaviors, ways of warming feet, and other content. A preliminary plan for daily foot self-care for high-risk diabetic foot patients has been formed, consisting of 5 primary indicators and 21 secondary indicators (see Supplementary Material S1, Part B).
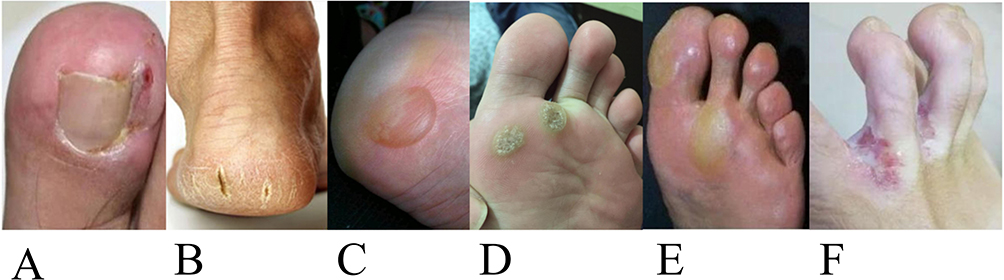 |
Figure 3 Schematic diagram of common foot abnormalities in diabetic high-risk feet. (A) Ingrown toenail; (B) Crack; (C) Blisters; (D) Corns; (E) Calluses; (F) Athlete’s foot. |
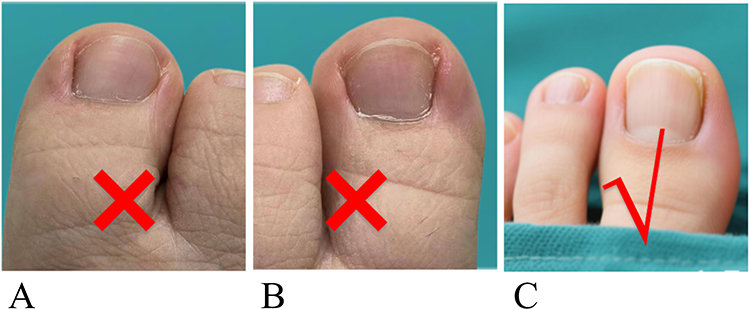 |
Figure 4 Schematic diagram of toenail trimming status for patients with diabetic high-risk feet. (A) Short toenails. (B) Rounded toenails. (C) Toenails properly trimmed. |
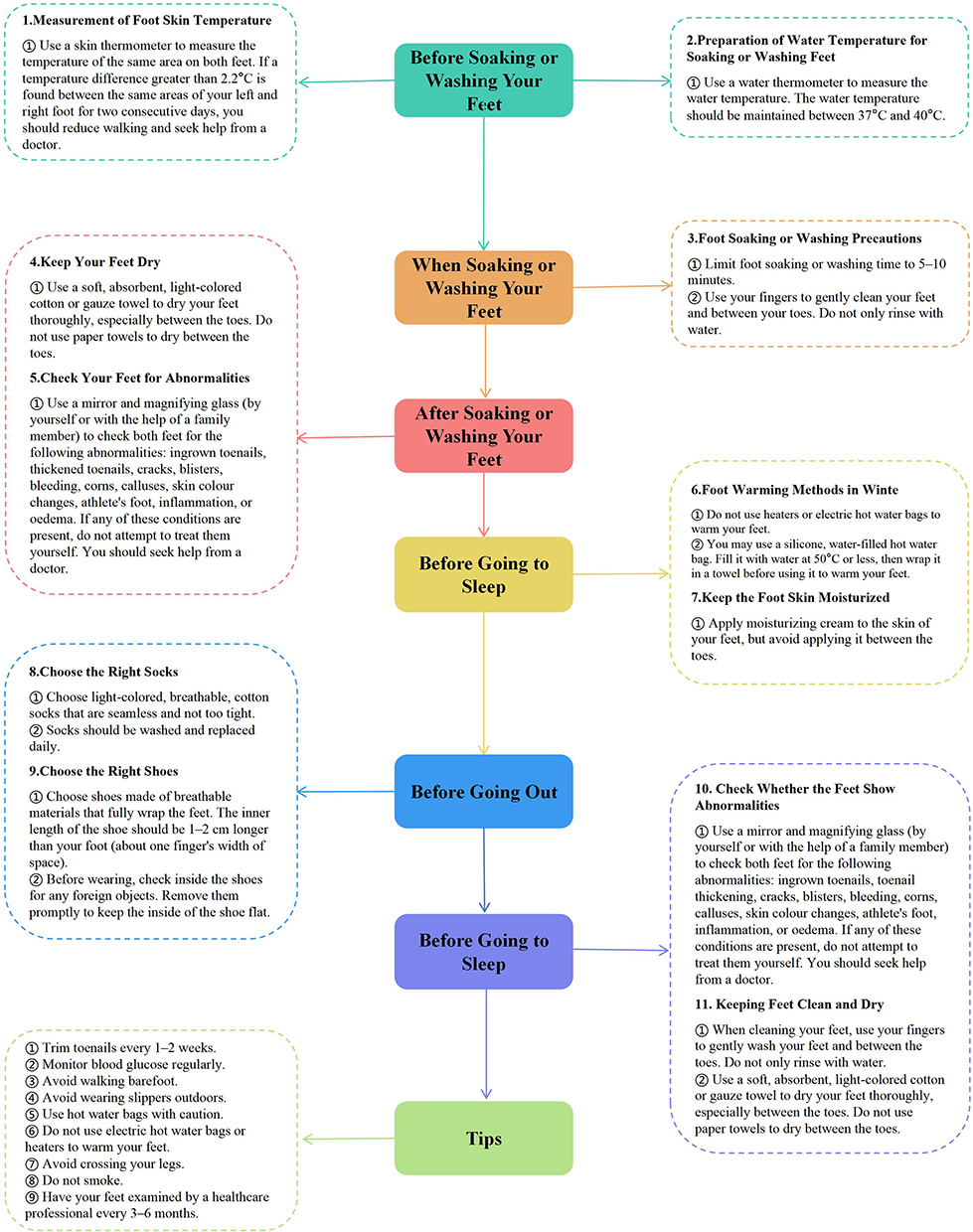 |
Figure 5 Foot self-care flowchart for patients with diabetic high-risk feet (semi-structured interviews version). |
Delphi Method
Expert Panel
The experts participating in the Delphi survey come from hospitals of different levels across China, with the inclusion criteria as follows: Exclusion criteria included: (1) having less than 10 years of nursing experience; (2) having less than 3 years of experience in diabetes/diabetic foot care; (3) unwillingness to participate in two rounds of consultation. A total of 17 experts completed two rounds of Delphi inquiries. The experts came from 12 tertiary grade A hospitals, 1 tertiary grade B hospital, and 2 secondary grade A hospitals in Guangdong Province, 1 tertiary grade A hospital in Sichuan Province, and 1 township health center in Shandong Province. The average age of the experts was 45.65±7.58 years, with an average of 25.41±8.56 years of nursing experience, and an average of 12.88±7.61 years of experience in diabetes/diabetic foot care. The general information of the experts is shown in Table 1.
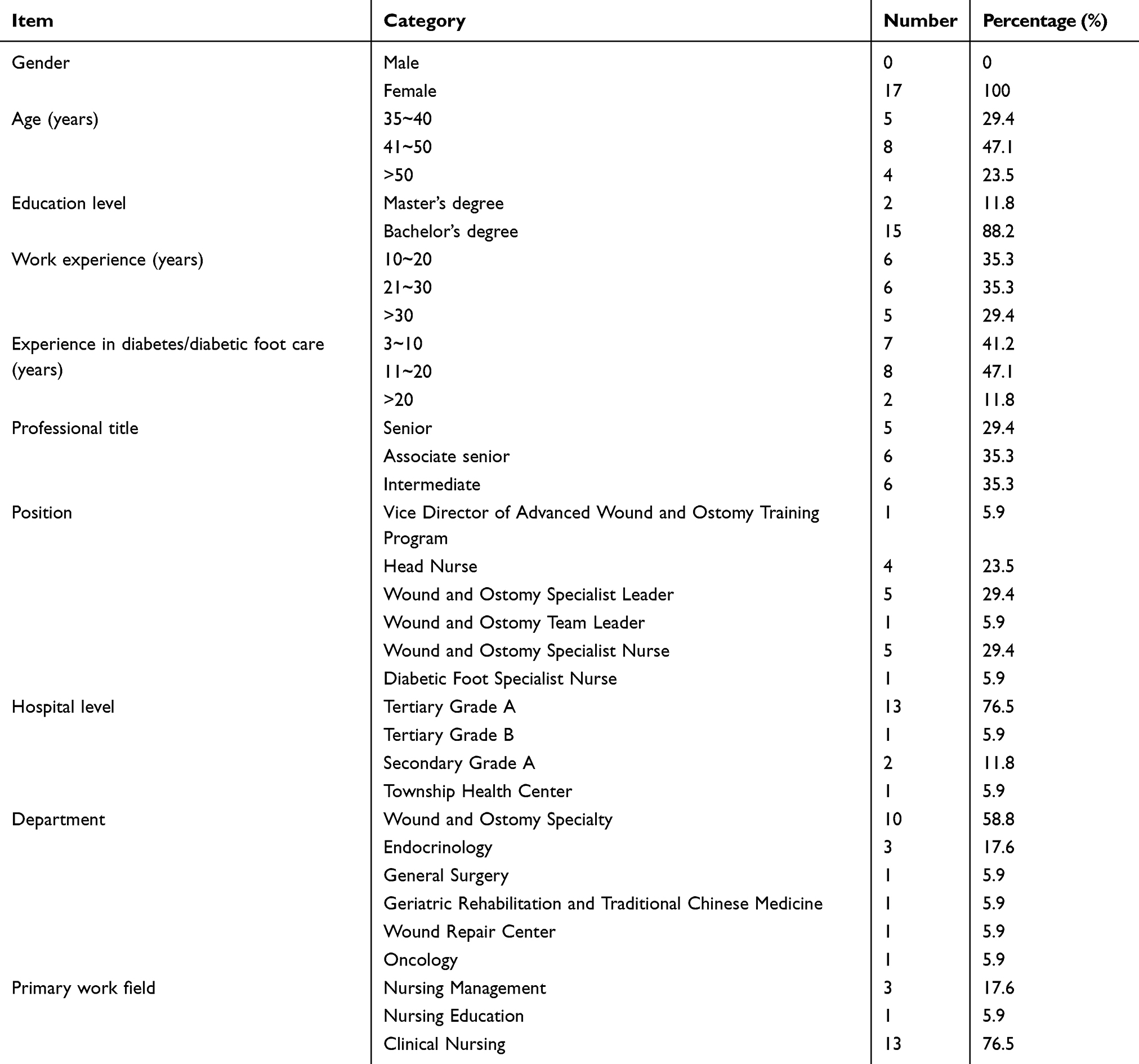 |
Table 1 General Characteristics of the Experts (n=17) |
Data Collection
According to the initial draft of the plan, a questionnaire for expert consultation on the daily foot self-care plan for diabetic high-risk foot patients was designed, including three parts: (1) Introduction, summary, research objectives, and instructions for filling out the questionnaire, etc. (2) Main part of the questionnaire, including the expert opinion form on the daily foot self-care plan for diabetic high-risk foot patients. Experts are asked to judge the importance of each indicator, using the Likert 5-point scale, ranging from “very important” to “very unimportant”, assigned 5 to 1 points respectively. A comments section is provided after each item, and a section for adding or removing items is placed at the end of the table to facilitate experts’ open-ended feedback; also includes a survey on the expert’s familiarity with the consultation content and the basis for their judgments. (3) Expert basic information survey form. The first round of consultations was conducted in December 2024, with the consultation questionnaire sent via Email and WeChat, to be replied to within one week. For each completed questionnaire received, promptly check for any missing fields, and if any are found, return it for completion. Items were selected based on the mean importance score and the coefficient of variation. If the mean importance score is ≥ 4 points and the coefficient of variation is < 0.25, the item was retained.39 The results of the consultation indicate that there were disagreements among the experts. After discussions within the project team and combining the principles for literature and indicator selection,40 the importance scores and modification suggestions were organized and analyzed, leading to revisions of the self-care plan. In January 2025, a second round of consultation was conducted, following the same approach as the first round. The Delphi consultation was concluded after the second round, as the results demonstrated a significant convergence of expert opinions, evidenced by an increase in Kendall’s coefficient of concordance (W) from 0.168 to 0.272 and all items achieving a coefficient of variation (CV) below the 0.25 threshold.26 Finally, through two rounds of Delphi expert surveys, a list of daily foot self-care measures for patients with high-risk feet due to diabetes was compiled, as detailed in Supplementary Material S1, Part C.
Data Analysis
The results of the inquiry were processed using SPSS 25.0 software. Categorical data were described using frequencies and percentages, while continuous data were described using mean ± standard deviation. The response rate of the questionnaires and the proportion of experts providing feedback were used to reflect expert engagement; the higher the response rate and the proportion of experts offering feedback, the higher the expert engagement. The authority coefficient of the experts was evaluated based on their judgment coefficient, academic level, and familiarity, while the degree of coordination of expert opinions was represented by the Kendall concordance coefficient.26
Ethical Approval
This study was conducted under the guidance of the Helsinki Declaration, and all research methods were carried out by relevant guidelines and regulations. The study was approved by the Ethics Committee of the First Affiliated Hospital of Guangdong Pharmaceutical University (No: 2024-IIT-62 and 2024-IIT-62 (01)). In the semi-structured interview section, written consent was obtained from all participants, and in the Delphi expert consultation section, all participants gave oral informed consent to participate in the study. During the investigation process, all participants were free to withdraw from the study at any time. The Ethics Committee of the First Affiliated Hospital of Guangdong Pharmaceutical University approved the procedures for obtaining both written and oral informed consent.
Result
Reliability of the Delphi Expert Consultation Results
Expert Engagement Level
In the first and second rounds of expert consultations for this study, 18 and 17 questionnaires were distributed, respectively with 17 questionnaires returned in each round, resulting in effective response rates of 94.44% and 100%. In the first round, 15 experts (83.33%) provided suggestions, while in the second round, 4 experts (23.52%) provided suggestions, indicating a high level of expert engagement.
Expert Authority Level
The expert authority coefficient (Cr) is determined by the judgment coefficient (Ca), the expert’s academic level (C), and the expert’s familiarity coefficient (Cs). The formula for calculating Cr is as follows: Cr = (Ca + C + Cs) / 3. In this study, the judgment coefficient (Ca) from two rounds of Delphi expert consultations was 0.99, the expert academic level (C) was 0.86, and the expert familiarity coefficient (Cs) was 0.93. Therefore, the expert authority coefficient (Cr) is 0.93 indicating that the experts possess high authority in this field.41
Degree of Coordination of Expert Opinions
The degree of expert opinion coordination is represented by the coefficient of variation (CV) and the coordination coefficient. In this study, the CV range for both rounds was 0 to 0.16.42 The coordination coefficient was evaluated using Kendall’s concordance coefficient. In the first round of expert consultation, the coordination coefficient for the first-level indicators was 0.413, and for the second-level indicators, it was 0.105. In the second round of expert consultation, the coordination coefficient for the first-level indicators was 0.466, and for the second-level indicators, it increased to 0.225. The P-values for the first and second-level indicators of the two rounds of Delphi expert consultation, tested by Kendall’s concordance coefficient, were both <0.05, indicating statistically significant differences. Therefore, the degree of opinion coordination in the Delphi expert consultation is considered good (see Table 2).In the final protocol, the majority of indicators demonstrated strong consensus (CV < 0.10). However, a few items, such as “foot skin temperature monitoring” (CV=0.16) and “daily foot self-care flowchart” (CV=0.16), had CVs approaching the 0.25 threshold. These items were retained after deliberation within the research group due to their clinical importance and strong supporting evidence for their value in preventing diabetic foot ulcers.19,43
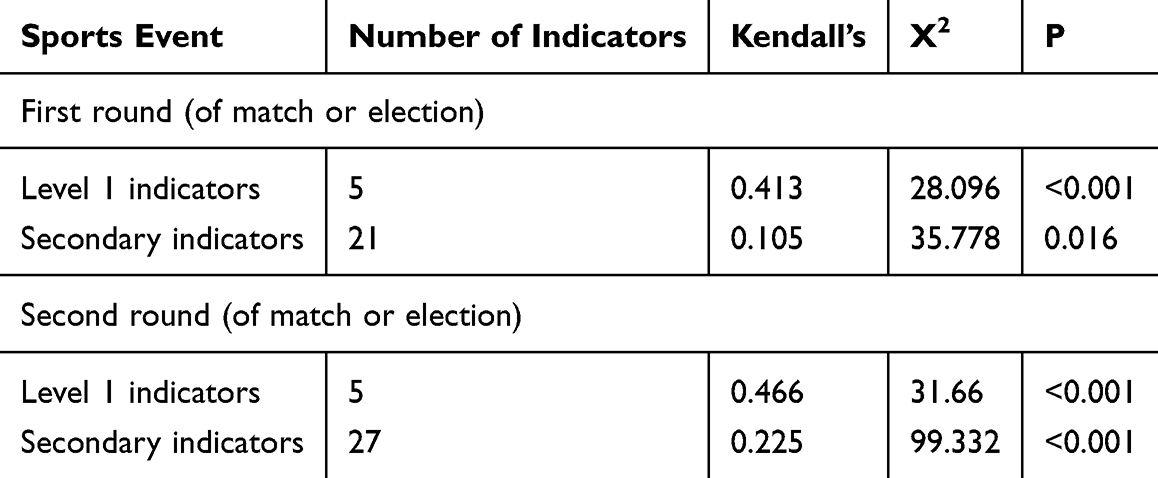 |
Table 2 Coordination Coefficients of Delphi Expert Consultation |
Results of the Expert Inquiry
Results of the First Round of Expert Consultations
In the first round of Delphi expert consultation, experts evaluated the draft of the daily foot self-care plan for patients at high risk of diabetic foot. This evaluation included 5 primary items and 21 secondary items, as detailed in Supplementary Material S1, Part D. A total of 48 comments were made, which, after combining similar ones, resulted in 12 revision suggestions, 7 additional suggestions, and no deletion suggestions. After discussion among the group members, all 7 additional suggestions, which were closely related to foot self-care behaviors, were adopted.Based on these consolidated expert opinions, a revised foot self-care flowchart was developed (see Figure 6). Items that did not reach a 75% full score rate were discussed by the research group, and relevant literature was reviewed.19 It was determined that these items are of significant importance in preventing foot ulcers, and thus were not deleted.19,43
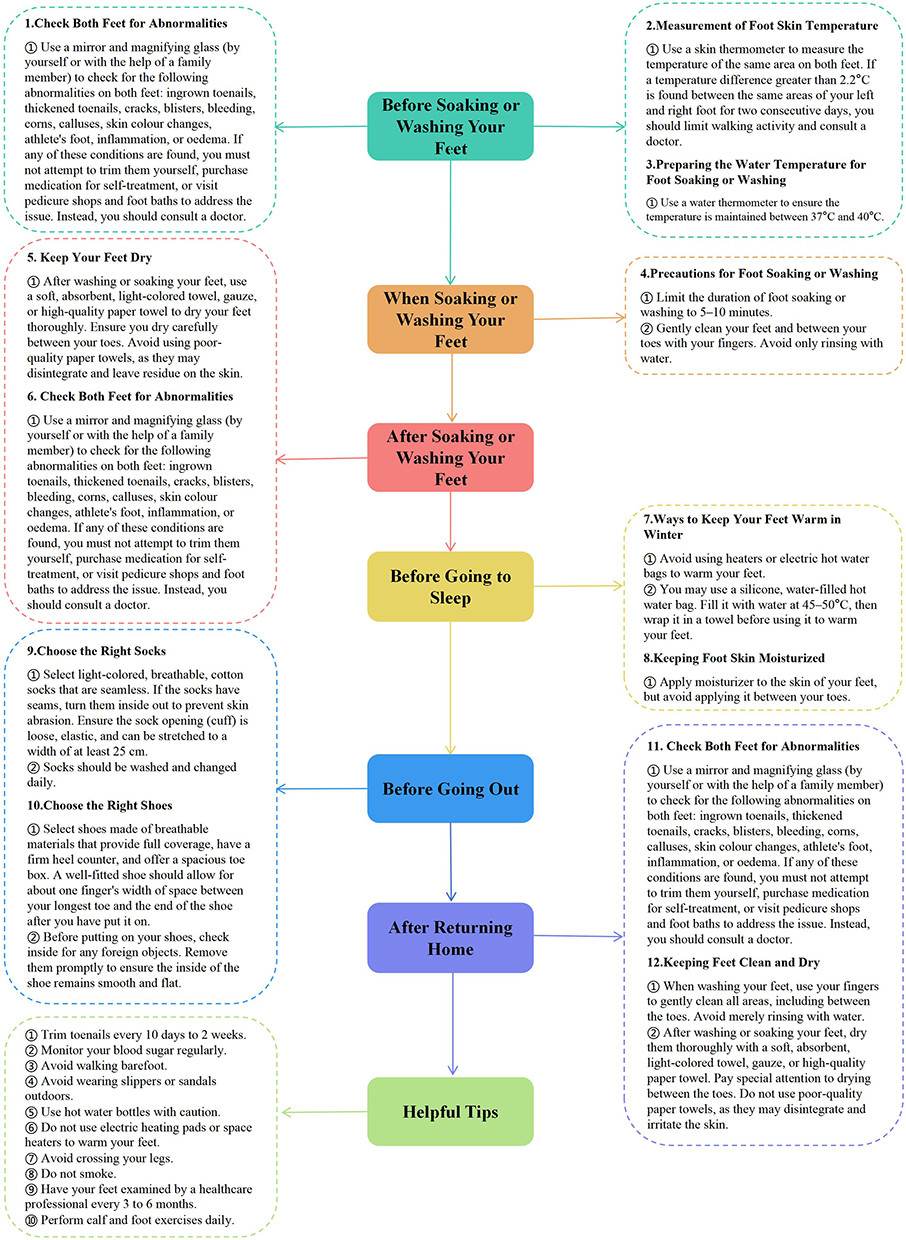 |
Figure 6 Foot self-care flowchart for patients with diabetic high-risk feet (post first-round Delphi expert consultation version). |
Results of the second Round of Expert Inquiries
In the second round of expert consultation, under the guidance of predefined standards, a consensus was reached on all proposals, with only minor adjustments made to the wording, without adding or deleting any suggestions. As a result, five first-level indicators were finalized (self-foot inspection, foot hygiene care, shoe and sock selection, daily precautions, and daily foot self-care flowchart), along with 27 second-level indicators, as detailed in Table 3.Compared with the first round, the number of secondary indicators increased from 21 to 27, reflecting further refinement and improvement based on expert opinions. The increase in the coordination coefficient indicates a significant enhancement in expert consensus.
 |
Table 3 Foot Self-Care Program for Patients with Diabetic High-Risk Feet (Round 2) |
Discussion
Scientific Rigor and Development Process of the Protocol
The daily foot self-care protocol developed in this study demonstrates strong scientific rigor, which is underpinned by its systematic development process. We constructed the initial framework through a comprehensive literature review, integrating findings from reliable scales and high-quality studies. Crucially, the adoption of a modified Delphi method enhanced the efficiency and foundational strength of our study. The two-round consultation process involved a panel of 17 experts with high authority (Cr=0.93), resulting in significantly improved coordination coefficients from the first to the second round. This indicates that the final consensus we achieved is both reliable and robust.26,44 The entire process, from initial item generation based on patient and professional input to iterative expert refinement, ensures that the protocol is not only evidence-based but also clinically relevant and practical.45
Advantages Over International Guidelines and Patient-Centered Innovation
When compared to internationally recognized guidelines such as those from the IWGDF,19 our protocol offers distinctive advantages in translating evidence into practice.46 While the IWGDF guidelines provide comprehensive, principle-based recommendations, they often lack the specificity required for direct patient implementation. Our protocol addresses this gap by leveraging the checklist management model to deconstruct complex guidelines into 27 specific, actionable secondary indicators.23 For instance, regarding skin temperature monitoring—a known predictor of ulceration43 — our protocol provides clear, patient-friendly operational criteria (eg, “a temperature difference >2.2°C for two consecutive days”), which aligns with the evidence but presents it in a more executable format. This structured, patient-centered approach fundamentally shifts the focus from knowledge dissemination to behavioral facilitation, potentially bridging the critical gap between guideline recommendations and sustained self-care behaviors.47
In-Depth Interpretation of the Protocol’s Components
The finalized protocol encompasses five core domains, each designed to address key risk factors for diabetic foot ulcers.19 Daily self-foot examination is the cornerstone of prevention.48 Our protocol not only specifies the methodology (eg, using mirrors in good light) but also emphasizes the role of caregivers and provides visual aids to enhance early problem identification.36,49 The inclusion of foot skin temperature monitoring with explicit thresholds is a significant step towards proactive ulcer prevention, empowering patients to recognize pre-ulcerative signs.50 Foot hygiene care details critical steps like water temperature control and interdental drying, directly targeting common causes of skin breakdown and infection.32,51 Furthermore, the guidelines on shoe and sock selection extend beyond basic advice to include break-in procedures for new footwear, a frequent oversight that can lead to preventable trauma.32 By consolidating these evidence-based components into a coherent checklist, the protocol provides a comprehensive yet practical framework for daily self-management.
Clinical Significance and Application Value
The development of this patient-centered, checklist-based protocol holds considerable clinical and practical significance.9 It provides a standardized and structured tool that bridges a critical gap in current diabetic foot prevention. For nurses, it offers a clear framework for delivering consistent and comprehensive patient education, moving beyond ad-hoc advice.52 For high-risk patients, it translates complex self-care principles into manageable daily actions, thereby potentially enhancing adherence, reducing the incidence of DFUs, and lowering the associated risk of amputations.47
Limitations
Notwithstanding its potential value, this study has several limitations. First, the expert panel, though highly authoritative, was exclusively composed of Chinese nursing specialists. The gender homogeneity (all female) reflects the demographic reality of the nursing workforce in China but may limit the diversity of perspectives. Second, as most experts were from more developed provinces, a regional bias exists, which may affect the generalizability of the findings across all regions of China. Finally, it is crucial to emphasize that this protocol is a consensus-based tool whose efficacy in improving clinical outcomes remains to be empirically tested.
Conclusions
In conclusion, this study successfully constructed a standardized, patient-centered daily foot self-care protocol for high-risk diabetic foot patients by integrating the checklist management model with a modified Delphi expert consensus approach. The final protocol, comprising 5 primary indicators and 27 secondary indicators, provides a structured and actionable tool intended to bridge the gap between clinical guidelines and patients’ daily self-care practices. While this study establishes a foundational, consensus-based framework, it is crucial to emphasize that this protocol represents the development phase. Its practical effectiveness and ability to improve clinical outcomes must be rigorously evaluated through future implementation science and randomized controlled trials.
Future Directions for Research and Implementation
The limitations noted above point directly to clear priorities for future work. The next essential step is to move beyond protocol development to clinical validation. This should begin with pilot studies to assess feasibility and acceptability in real-world settings. Subsequently, well-designed randomized controlled trials (RCTs) are imperative to definitively establish the protocol’s efficacy in reducing ulcer incidence and amputation rates, and in improving patients’ quality of life. Furthermore, given its development within a specific cultural context, cross-cultural adaptation followed by validation is recommended before any international application.
Abbreviations
DF, Diabetic Foot; IWGDF, International Working Group on the Diabetic Foot; DFUs, Diabetic Foot Ulcers; CNKI, China National Knowledge Infrastructure; CBM, China Biomedical Database; CV, coefficient of variation. Note: These are methodological abbreviations used in this article.
Data Sharing Statement
Data is provided within the article or supplementary information files.
Ethics and Consent Statement
Written informed consent was obtained from all participants in the semi-structured interviews prior to the commencement of the study. The study protocol was approved by the Ethics Committee of the First Affiliated Hospital of Guangdong Pharmaceutical University (Approval No.: 2024-IIT-62 and 2024-IIT-62(01)). Due to the broad geographic distribution of experts participating in the Delphi consultation, verbal informed consent was obtained from participants and formally documented via WeChat and email. This procedure was approved by the Ethics Committee of the First Affiliated Hospital of Guangdong Pharmaceutical University (Approval No.: 2024-IIT-62 and 2024-IIT-62(01)). Participants provided written consent for the publication of de-identified images of their feet and associated case details.
Acknowledgments
The author extends sincere gratitude to all participants involved in this study, appreciating their valuable time and insights. We also thank the experts who contributed through the Delphi consultation.
Author Contributions
Xiaodan Lin: Conceptualization, Investigation, Software, Supervision, Writing – Original Draft; Xianghao Chen: Conceptualization, Investigation, Software, Visualization, Writing – Original Draft; Xiaozhou Zhou: Data Curation, Formal Analysis, Methodology, Project Administration, Resources, Supervision, Writing – Review & Editing; Yuantian Li: Data Curation, Formal Analysis, Project Administration, Resources, Supervision, Writing – Review & Editing; Shumin He: Data Curation, Formal Analysis, Project Administration, Resources, Supervision, Writing – Review & Editing; Haidan Xie: Investigation, Writing – Original Draft; Yiting Zhuo: Formal Analysis,Writing – Original Draft; Leting Zhang: Conceptualization,Writing – Original Draft; All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The author(s) received no specific funding for this work. This study was completed using existing resources.
Disclosure
The authors declare no competing interests.
References
1. Federation ID. Diabetes global report 2000 — 2050. Available from: https://diabetesatlas.org/data-by-location/global/.
2. Society CD. Chinese Guidelines for the Prevention and Control of Type 2 Diabetes Mellitus (2020 Edition) (below). Chin J Pract Interal Med. 2021;41(9):757–16. doi:10.19538/j.nk2021090106
3. Zhang Y, Liu H, Yang Y, Feng C, Cui L. Incidence and risk factors for amputation in Chinese patients with diabetic foot ulcers: a systematic review and meta-analysis. Front Endocrinol. 2024;15:1405301. doi:10.3389/fendo.2024.1405301
4. Sun H, Saeedi P, Karuranga S, et al. IDF Diabetes Atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabet Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
5. Yin Jingxia YL, Danlan P, Xiaoli X, Yong L. Interpretation of the China Guidelines for the Prevention and Treatment ofDiabetes (2024 Edition). J Chongqing Med Univ. 2025;1–8. doi:10.13406/j.cnki.cyxb.003749
6. Schaper NC, van Netten JJ, Apelqvist J, et al. Practical guidelines on the prevention and management of diabetes-related foot disease (IWGDF 2023 update). Diabetes Metab Res Rev. 2024;40(3):e3657. doi:10.1002/dmrr.3657
7. Kumbhar S, Bhatia M. Advancements and best practices in diabetic foot Care: a comprehensive review of global progress. Diabet Res Clin Pract. 2024;217:111845. doi:10.1016/j.diabres.2024.111845
8. Alrashed FA, Iqbal M, Al-Regaiey KA, et al. Evaluating diabetic foot care knowledge and practices at education level. Medicine. 2024;103(34):e39449. doi:10.1097/md.0000000000039449
9. Lin X, Chen X, Li Y, He S, Xie H, Zhou X. Cognitive gaps and educational needs in foot self-care among patients with diabetic foot from a health literacy perspective: a qualitative study. J Tissue Viability. 2025;34(4):100960. doi:10.1016/j.jtv.2025.100960
10. Kosaji D, Awad MI, Katmah R, et al. Diabetic foot prevention, assessment, and management using innovative smart wearable technology: a systematic review. J Neuroeng Rehabil. 2025;22(1):168. doi:10.1186/s12984-025-01695-9
11. Bonner T, Guidry J, Jackson Z. Association between Foot Care Knowledge and Practices among African Americans with Type 2 Diabetes: an Exploratory Pilot Study. J Natl Med Assoc. 2019;111(3):256–261. doi:10.1016/j.jnma.2018.10.004
12. Xinyi L, Wenjing L, Nan Z, et al. The Status Quo and Influencing Factors of Foot Skin Problems among Patients with Diabetes. Military Nursing. 2020;37(10):5–9. doi:10.3969/i.issn1008-9993.2020.10.002
13. Ahlberg M, Tang UH, Petersson C. Enhancing Clinical Guideline Adherence in Diabetic Foot Ulcer Prevention: a Case Study on Quality Improvement Interventions. Jt Comm J Qual Patient Saf. 2025;51(10):642–651. doi:10.1016/j.jcjq.2025.06.011
14. Ma L, Chen J, Sun Y, Feng Y, Yuan L, Ran X. The perceptions of living with diabetic foot ulcers: a systematic review and meta-synthesis of qualitative studies. J Tissue Viability. 2023;32(1):39–50. doi:10.1016/j.jtv.2022.11.005
15. Wu Y, Zhang J, Ge P, et al. Application of Chatbots to Help Patients Self-Manage Diabetes: systematic Review and Meta-Analysis. J Med Internet Res. 2024;26:e60380. doi:10.2196/60380
16. Oni D. Foot Self-Care Experiences Among Patients With Diabetes: a Systematic Review of Qualitative Studies. Wound Manag Prev. 2020;66(4):16–25. doi:10.25270/wmp.2020.4.1625
17. Xuejing L, Lifiao Y, Xiaoyan Z, Jingya M, Wang Jinfang WD, Yufang H. Interpretation of the best practice guideline by Registered Nurses Association of Ontario--Evaluation and Management of Diabetic Foot Ulcer Patients, 2nd edition, 2013. Chin J Modern Nurs. 2018;24(27):2. doi:10.3760/cma.j.issn.1674-2907.2018.27.002
18. Sajith R, Ackers L, Ackers-Johnson S, Parker DJ, Stephens M. The practice, nature, and impact of nurse-led type 2 diabetic foot prevention services and educational programs in Sub-Saharan Africa: a scoping review. Front Public Health. 2024;12:1465750. doi:10.3389/fpubh.2024.1465750
19. Bus SA, Sacco ICN, Monteiro-Soares M, et al. Guidelines on the prevention of foot ulcers in persons with diabetes (IWGDF 2023 update). Diabetes Metab Res Rev. 2024;40(3):e3651. doi:10.1002/dmrr.3651
20. Shiffman RN, Michel G, Essaihi A, Thornquist E. Bridging the guideline implementation gap: a systematic, document-centered approach to guideline implementation. J Am Med Inform Assoc. 2004;11(5):418–426. doi:10.1197/jamia.M1444
21. Bodolica V, Spraggon M. Toward patient-centered care and inclusive health-care governance: a review of patient empowerment in the UAE. Public Health. 2019;169:114–124. doi:10.1016/j.puhe.2019.01.017
22. Hales BM, Pronovost PJ. The checklist--a tool for error management and performance improvement. J Crit Care. 2006;21(3):231–235. doi:10.1016/j.jcrc.2006.06.002
23. Pugel AE, Simianu VV, Flum DR, Patchen DE. Use of the surgical safety checklist to improve communication and reduce complications. J Infect Public Health. 2015;8(3):219–225. doi:10.1016/j.jiph.2015.01.001
24. Lydecker AD, Kim JJ, Robinson GL, et al. Chlorhexidine vs Routine Foot Washing to Prevent Diabetic Foot Ulcers: a Randomized Clinical Trial. JAMA Netw Open. 2025;8(2):e2460087. doi:10.1001/jamanetworkopen.2024.60087
25. Pouwer F, Perrin B, Lavender A, Najafi B, Ismail K, Vileikyte L. The quest for wellness: how to optimise self-care strategies for diabetic foot management? Diabetes Metab Res Rev. 2024;40(3):e3751. doi:10.1002/dmrr.3751
26. He F, Zhang X, Liu J, et al. Construction of a nursing management program for early fluid resuscitation in patients with acute pancreatitis: a Delphi study in China. BMC Nurs. 2025;24(1):28. doi:10.1186/s12912-025-02689-7
27. Sun X, Yuan J, Xu M, et al. Development of a graded management program for patients with diabetic foot ulcers based on the triangle model: a Delphi study. J Tissue Viability. 2025;34(2):100868. doi:10.1016/j.jtv.2025.100868
28. Makhmutov R. The Delphi method at a glance. Pflege. 2021;34(4):221. doi:10.1024/1012-5302/a000812
29. Speight J, Bradley C. The ADKnowl: identifying knowledge deficits in diabetes care. Diabet Med. 2001;18(8):626–633. doi:10.1046/j.1464-5491.2001.00537.x
30. Jing L, Qiuling X. Study on the reliability and validity of the Chinese version of the Nottingham Assessment of Functional Footcare. Chin J Practical Nurs. 2015;31(6):450–453. doi:10.3760/cma.j.issn.1672-7088.2015.06.021
31. Lopes GSG, Landeiro MJL, Maciel T, Sousa M. Clinical practice guidelines of foot care practice for patients with type 2 diabetes: a scoping review using self-care model. Contemp Nurse. 2024;60(5):516–536. doi:10.1080/10376178.2024.2362289
32. Untari EK, Andayani TM, Yasin NM, Asdie RH. A Review of Patient’s Knowledge and Practice of Diabetic Foot Self-Care. Malays J Med Sci. 2024;31(1):33–50. doi:10.21315/mjms2024.31.1.3
33. Mirzaei-Alavijeh M, Yarmoradi S, Khashij S, Jalilian F. Application of the information-motivation-behavioral skills model to improve medication adherence among older adults with type 2 diabetes: findings from a quasi-experimental study in Kermanshah, Iran. BMC Geriatr. 2025;25(1):328. doi:10.1186/s12877-025-06000-w
34. Liping Y, Lidong Q, Bo Z. Concepts and evaluation of saturation in qualitative research. Adv Psychol Sci. 2022;30(3):511–521. doi:10.3724/SP.J.1042.2022.00511
35. Hellstrand Tang U, Scandurra I, Sundberg L, Annersten Gershater M, Patients’ ZR. Expectations of Evidence-Based Service at the Pharmacy Regarding Information on Self-Care of the Feet for Persons with Diabetes at Risk of Developing Foot Ulcers - A Cross-Sectional Observational Study in Sweden. Patient Prefer Adherence. 2023;17:3557–3576. doi:10.2147/ppa.S435632
36. Bus SA, Lavery LA, Monteiro-Soares M, et al. Guidelines on the prevention of foot ulcers in persons with diabetes (IWGDF 2019 update). Diabetes Metab Res Rev. 2020;36(1):e3269. doi:10.1002/dmrr.3269
37. Bonilla-Carrasco MI, Rasero-Fernández E, Aguayo-González M, Rafael-Gutiérrez SS. Self-care of the feet in people with type 2 diabetes. A qualitative study. Enferm Clin. 2023;33(3):223–233. doi:10.1016/j.enfcle.2023.01.002
38. Ricci L, Villegente J, Loyal D, Ayav C, Kivits J, Rat AC. Tailored patient therapeutic educational interventions: a patient-centred communication model. Health Expect. 2022;25(1):276–289. doi:10.1111/hex.13377
39. Chen L, Wu Y, Wang S, Zhao H, Zhou C. Construction of evidence-based practice competencies for nurses in China: a modified Delphi study. Nurse Educ Today. 2021;102:104927. doi:10.1016/j.nedt.2021.104927
40. Keeney S, Hasson F, McKenna H. Consulting the oracle: ten lessons from using the Delphi technique in nursing research. J Adv Nurs. 2006;53(2):205–212. doi:10.1111/j.1365-2648.2006.03716.x
41. Liu X, Liu L, Zhang J, Meng X, Huang C, Zhang M. Construction and evaluation of nursing-sensitive quality indicators for vaginal birth after cesarean: a Delphi study based on Chinese population. Heliyon. 2023;9(11):e21389. doi:10.1016/j.heliyon.2023.e21389
42. Wan F, Yang L, Zhou N, He Y. Construction of learning objectives and content for newly graduated nurses in tertiary teaching hospitals: a Delphi study. Nurse Educ Today. 2023;121:105716. doi:10.1016/j.nedt.2023.105716
43. Bus SA, Aan de Stegge WB, van Baal JG, Busch-Westbroek TE, Nollet F, van Netten JJ. Effectiveness of at-home skin temperature monitoring in reducing the incidence of foot ulcer recurrence in people with diabetes: a multicenter randomized controlled trial (DIATEMP). BMJ Open Diabetes Res Care. 2021;9(1):1. doi:10.1136/bmjdrc-2021-002392
44. Klompstra L, Liljeroos M, Lundgren J, Ingadottir B. A Clinical Tool (CUE-tool) for Health Care Professionals to Assess the Usability and Quality of the Content of Medical Information Websites: electronic Delphi Study. J Med Internet Res. 2021;23(2):e22668. doi:10.2196/22668
45. Ji Y, Li Y, Peng F, Yin J. Construction of competency evaluation index system for infection control link nurses based on iceberg model. Occupation Health. 2025;41(21):2960–2965. doi:10.13329/j.cnki.zyyjk.2025.0537
46. Montoya L, Liddy C, Hogg W, et al. Development of the Champlain primary care cardiovascular disease prevention and management guideline: tailoring evidence to community practice. Can Fam Physician. 2011;57(6):e202–7.
47. Paton J, Abey S, Hendy P, Williams J, Collings R, Callaghan L. Behaviour change approaches for individuals with diabetes to improve foot self-management: a scoping review. J Foot Ankle Res. 2021;14(1):1. doi:10.1186/s13047-020-00440-w
48. Dogan DA, Enç N. The effect of using a reminder diabetic foot mirror on foot checking frequency and development of diabetic foot in people with diabetes. Int J Diabetes Dev Countries. 2022;42(2):321–330. doi:10.1007/s13410-021-00985-x
49. Ang CS, Goh KFI, Lodh N, et al. Foot care behaviours and associated factors among patients with type 2 diabetes: a cross-sectional study. J Glob Health. 2024;14:04145. doi:10.7189/jogh.14.04145
50. Manickum P, Mashamba-Thompson T, Naidoo R, Ramklass S, Madiba T. Knowledge and practice of diabetic foot care - A scoping review. Diabetes Metab Syndr. 2021;15(3):783–793. doi:10.1016/j.dsx.2021.03.030
51. Binyao Q. Analysis of Preventive Effect of “Five steps” Health Education on Diabetic Foot Nursing. Guide Chin Med. 2021;19(16):147–148. doi:10.15912/j.cnki.gocm.2021.16.066
52. Orestes LP, Meneguin S, de Leo A, Patini MSG, Santos BP, de Oliveira C. COVID-19: protocol and Checklist for Nursing Care Management at Urgent Care Units. Int J Environ Res Public Health. 2023;20(3):2169. doi:10.3390/ijerph20032169
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.