Back to Journals » Journal of Inflammation Research » Volume 18
Development of a Nomogram for Predicting Multiple Organ Dysfunction in Acute Pancreatitis
Authors Che Z ![]() , Zhao X
, Zhao X ![]() , Xue W, Wang Z
, Xue W, Wang Z ![]() , Hu C
, Hu C ![]() , Feng Y
, Feng Y ![]() , Ru R, Tian Y, Mo S
, Ru R, Tian Y, Mo S
Received 8 November 2025
Accepted for publication 11 December 2025
Published 24 December 2025 Volume 2025:18 Pages 18025—18037
DOI https://doi.org/10.2147/JIR.S577488
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Nadia Andrea Andreani
Zongyuan Che,* Xuchen Zhao,* Wei Xue, Zhiyao Wang, Congzhong Hu, Yulin Feng, Ruijun Ru, Yanzhang Tian, Shaojian Mo
Third Hospital of Shanxi Medical University, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Taiyuan, 030032, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanzhang Tian, Third Hospital of Shanxi Medical University, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Taiyuan, 030032, People’s Republic of China, Tel +86-13903512030, Email [email protected] Shaojian Mo, Third Hospital of Shanxi Medical University, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Taiyuan, 030032, People’s Republic of China, Tel +86-19834514208, Email [email protected]
Background: Multiple Organ Dysfunction Syndrome (MODS) is a lethal complication of acute pancreatitis (AP), making early identification of high-risk patients crucial for improving outcomes.
Aim: To develop and validate a clinically applicable nomogram for predicting MODS risk in acute pancreatitis patients based on clinical and laboratory variables collected within the first 24 hours of admission.
Methods: We conducted a single-center retrospective cohort study using routinely collected electronic health records from Shanxi Bethune Hospital (Taiyuan, China), including 693 adult patients with acute pancreatitis admitted between January 1, 2019 and December 31, 2021. From 29 candidate indicators obtained within 24 hours of admission, key predictors were selected via LASSO regression, and three machine-learning models – generalized linear model (GLM), random forest (RF), and support vector machine (SVM) – were constructed and compared.
Results: Among the candidate models, the GLM-based nomogram showed the best overall performance. Using a parsimonious variable selection strategy, we derived a final 7-variable model. This model demonstrated good discrimination, with areas under the curve of 0.829 in the training cohort and 0.846 in the validation cohort, and showed satisfactory calibration, a high negative predictive value, and clinical net benefit.
Conclusion: Our internally validated 7-variable nomogram, based on a generalized linear model, showed good discrimination and a high negative predictive value for early prediction of multiple organ dysfunction syndrome in patients with acute pancreatitis, and may assist clinicians in early risk stratification and resource allocation. Further external validation and prospective studies are warranted to confirm its generalizability and clarify its impact on clinical decision-making and patient outcomes.
Keywords: acute pancreatitis, multiple organ dysfunction syndrome, risk stratification, electronic health records, machine learning
Introduction
Acute pancreatitis (AP) is a common digestive emergency in which aberrant activation of pancreatic enzymes leads to autodigestion and inflammation.1 In 20–30% of patients with severe acute pancreatitis (SAP), the disease progresses to multiple organ dysfunction syndrome (MODS), which carries a mortality rate of 30–50%.2 MODS, defined as failure of two or more organ systems, is closely associated with high mortality and prolonged intensive care unit (ICU) stays.3 Notably, organ failure persisting beyond 48 hours is linked to a marked increase in mortality (>50%).4
According to the latest clinical classification standards, the duration of organ dysfunction is the key criterion for distinguishing mild (MAP), moderately severe (MSAP), and severe AP (SAP). Clinical data indicate that organ failure occurs in approximately 20% of patients with AP, and mortality can surge to 30% once persistent organ dysfunction is established.5 In the temporal evolution of organ failure, the respiratory and circulatory systems are often affected early, manifesting as acute respiratory distress syndrome (ARDS, mortality ~37%) and refractory hypotension.4,6,7 As the disease progresses, it can further involve the kidneys (evidenced by rapidly rising creatinine levels and oliguria), liver, and central nervous system, creating a vicious cycle of mutually aggravating multiorgan dysfunction and markedly increasing the risk of severe complications such as infected pancreatic necrosis.8 From a therapeutic perspective, early fluid resuscitation using balanced crystalloids (eg, lactated Ringer’s solution) can improve microcirculation and reduce the risk of MODS, whereas high-volume hemofiltration (HVHF) can effectively clear inflammatory mediators and promote recovery of organ function.9 Therefore, early identification of AP-associated organ failure and timely intervention are crucial for improving prognosis and survival.10
Currently, the emergency management of AP complicated by organ failure faces numerous challenges, including the insufficient sensitivity of early warning indicators and difficulty in determining the optimal timing for intervention. Traditional scoring systems (eg, SOFA) have limited early predictive power for progression from AP to MODS because they rely on static parameters and do not incorporate dynamic changes in biomarkers. In-depth exploration of the pathophysiological mechanisms underlying progression from AP to MODS and the development of diagnosis and treatment strategies based on organ failure risk assessment have become key research priorities in the emergency care of AP. Therefore, in this study we aimed to develop and internally validate an early prediction model for MODS in patients with AP, using routinely collected clinical and laboratory indicators and existing scoring tools to support early risk stratification and targeted intervention.
Materials and Methods
Data Source
This was a single-center retrospective cohort study at Shanxi Bethune Hospital. We collected clinical data from 784 patients diagnosed with Acute Pancreatitis at Shanxi Bethune Hospital between January 1, 2019, and December 31, 2021. Based on the inclusion and exclusion criteria, clinical data from 693 patients were included in this study. Given the retrospective nature of the research, patient data were kept strictly confidential, and all data were anonymized to protect patient privacy.
Exclusion criteria were as follows: (1) Incomplete clinical data or missing medical records; (2) Non-first hospitalization; (3) Chronic pancreatitis, trauma-related pancreatitis, or pregnancy-associated pancreatitis; (4) Patients with tumors; (5) Patients diagnosed with severe cardiac, cerebral, pulmonary, renal, or other organ dysfunction prior to the onset of AP; (6) Patients who were tertiary referrals and had received prior medication or invasive interventions.
Sample size adequacy was evaluated using the events-per-variable (EPV) principle for logistic regression, which recommends ≥10 outcome events per predictor. We planned to include seven candidate predictors in the final model. Given the observed MODS incidence of 34.6% in the training cohort, the minimum required sample size was calculated as N ≥ (10 × 7) / 0.346 ≈ 203 patients, corresponding to at least 70 MODS events. Our training cohort (n = 486) contained 168 MODS events, which comfortably exceeded this threshold and was therefore considered sufficient to ensure stable coefficient estimates and to reduce the risk of overfitting.
Data Collection
General Information: Gender, age, Body mass index (BMI), smoking history, alcohol history, diabetes, hypertension, hyperlipidemia, other chronic diseases.
Laboratory Parameters within 24 hours of admission: Total cholesterol, triglycerides, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), serum magnesium, serum calcium, prothrombin time (PT), white blood cell count (WBC), neutrophil count, lymphocyte count, monocyte count, red blood cell count (RBC), hemoglobin (Hb), platelet count (PLT), C-reactive protein (CRP).
Inflammatory Indices and Clinical Scoring Parameters for AP: Modified Computed Tomography Severity Index (MCTSI), Bedside Index for Severity in Acute Pancreatitis (BISAP), Early Warning Score for Acute Pancreatitis (ERAP), Hemoglobin to Red cell distribution width Ratio (HRR), Neutrophil-to-Lymphocyte Ratio (NLR), Hemoglobin-Albumin-Lymphocyte-Platelet (HALP) score, C-reactive protein to Albumin Ratio (CAR), D-dimer to serum Calcium ratio (DDCa), Serum Creatinine to Total Bilirubin ratio (SCTB).
We performed deduplication, date/logic checks, and physiologic range checks; implausible values were set to missing a priori. No linkage across separate databases was performed.
Definitions
Diagnosis of Acute Pancreatitis
The diagnosis of AP was consistent with the revised 2012 Atlanta classification, requiring at least two of the following three criteria: (1) typical acute upper abdominal pain; (2) serum amylase and/or lipase levels at least three times the upper limit of normal; and (3) characteristic findings of AP on abdominal imaging.11
Multiple Organ Dysfunction Syndrome (MODS)
The Sequential Organ Failure Assessment (SOFA) score is one of the most commonly used tools for assessing organ failure. It includes six organ systems: respiratory, coagulation, liver, cardiovascular, renal, and neurological, each scored from 0 (normal) to 4 (most severe dysfunction). An SOFA score ≥2 in a given organ system indicates organ dysfunction, and MODS is considered when at least two organ systems are involved.12 In this study, MODS was defined as dysfunction (SOFA ≥2) in two or more organ systems during hospitalization.12
Laboratory Parameters
All laboratory parameters described in this section were obtained from venous blood samples collected within 24 hours of admission and analyzed using automated biochemical and hematology analyzers.
Modified Computed Tomography Severity Index (MCTSI)
The MCTSI comprises three components: (1) pancreatic inflammation, (2) pancreatic necrosis, and (3) extrapancreatic complications. The total MCTSI score is calculated as the sum of the inflammation score, necrosis score, and extrapancreatic complications score. All patients with AP underwent abdominal and pelvic CT scanning within 48 hours of symptom onset. Two experienced radiologists independently assessed pancreatic morphology, local complications, and extrapancreatic complications while remaining blinded to patient identity.13
BISAP Score
Introduced in 2008, the Bedside Index for Severity in Acute Pancreatitis (BISAP) score includes five clinical parameters: (1) blood urea nitrogen (BUN) >25 mg/dL; (2) impaired mental status (Glasgow Coma Scale score <15); (3) presence of systemic inflammatory response syndrome (SIRS); (4) age >60 years; and (5) presence of pleural effusion. Each parameter contributes 1 point, yielding a total score ranging from 0 to 5.14
Emergency Room Assessment for Acute Pancreatitis (ERAP) Score
The ERAP score ranges from 0 to 4 points and is calculated based on four binary indicators, each contributing 1 point if present: respiratory rate (RR) ≥22 breaths/minute, Glasgow Coma Scale (GCS) score <15, blood urea nitrogen (BUN) ≥25 mg/dL, and C-reactive protein (CRP) >150 mg/L.15,16
Hemoglobin-to-Red Cell Distribution Width Ratio (HRR)
HRR was calculated as hemoglobin divided by red cell distribution width (RDW), both obtained from the same complete blood count. Previous studies have shown that incorporating HRR can significantly improve the predictive performance of the SOFA score (C-index = 0.736) and BISAP score (C-index = 0.704) for 30-day mortality in AP. A higher HRR level is associated with a reduced 30-day mortality risk and may enhance the predictive ability of existing scoring tools.17
HALP Score
The HALP score is a comprehensive scoring system composed of four parameters: Hemoglobin, Albumin, Lymphocyte count, and Platelet count. These parameters are readily available in clinical practice and are closely related to the patient’s nutritional status, immune function, and inflammatory response, thus holding potential as a prognostic tool for critically ill patients. Studies have also found that the HALP score can improve the predictive ability of the SOFA score for short-term mortality.18,19
In this study, all clinical and laboratory variables used to calculate the BISAP, ERAP, HRR, and HALP scores were obtained within the first 24 hours of admission. This uniform time window ensured that all severity scores reflected early disease status for the purpose of early risk prediction.
Data Processing and Statistical Analysis
All data processing and statistical analyses were performed using R software (version 4.5.1). Continuous variables were first assessed for normality using the Shapiro–Wilk test; for normally distributed data, homogeneity of variances was then evaluated using Levene’s test. Between-group comparisons were conducted using the independent-samples t-test when variances were equal and Welch’s t-test when they were unequal, with results presented as mean ± standard deviation. Non-normally distributed data were summarized as median (interquartile range) and compared using the Mann–Whitney U-test. Categorical variables were summarized as counts and percentages, and between-group comparisons were performed using Pearson’s chi-square test or Fisher’s exact test, as appropriate.
Missing data were addressed using multiple imputation (MICE, R package mice, m = 5). All candidate predictors and the outcome were included in the imputation model, and pooled estimates were obtained using Rubin’s rules.
Subsequently, a machine learning workflow was employed to select predictive variables from the high-dimensional baseline data and to construct the prediction model: The dataset was randomly split into a training set (70%, n=486) and a validation set (30%, n=207) at a 7:3 ratio. The Least Absolute Shrinkage and Selection Operator (LASSO) regression was applied exclusively to the training set for variable selection to identify key predictors. Based on these predictors, three machine learning models-Generalized Linear Model (GLM), Random Forest (RF), and Support Vector Machine (SVM)-were constructed and compared. The final model was chosen according to a predefined strategy balancing predictive accuracy, calibration performance, and clinical interpretability. Predictors with negligible contribution were removed using backward elimination to improve model parsimony. Model performance was evaluated on the independent validation set, assessing discrimination via the Area Under the Receiver Operating Characteristic curve (AUC), calibration via calibration curves, and clinical utility via Decision Curve Analysis (DCA). Furthermore, internal validation was performed using 1000 Bootstrap resamples and 10-fold cross-validation to ensure model robustness.
Result
A total of 784 patients with acute pancreatitis were screened during the study period. Of these, 91 were excluded according to the predefined criteria, and 693 patients were included in the final analysis (Figure 1A). Missing baseline data for candidate predictors were handled using multiple imputation by chained equations (MICE; m = 5) including all candidate predictors and the outcome, and results across the imputed datasets were combined using Rubin’s rules. The pattern and proportion of missing data are presented in Supplementary Figure 1.
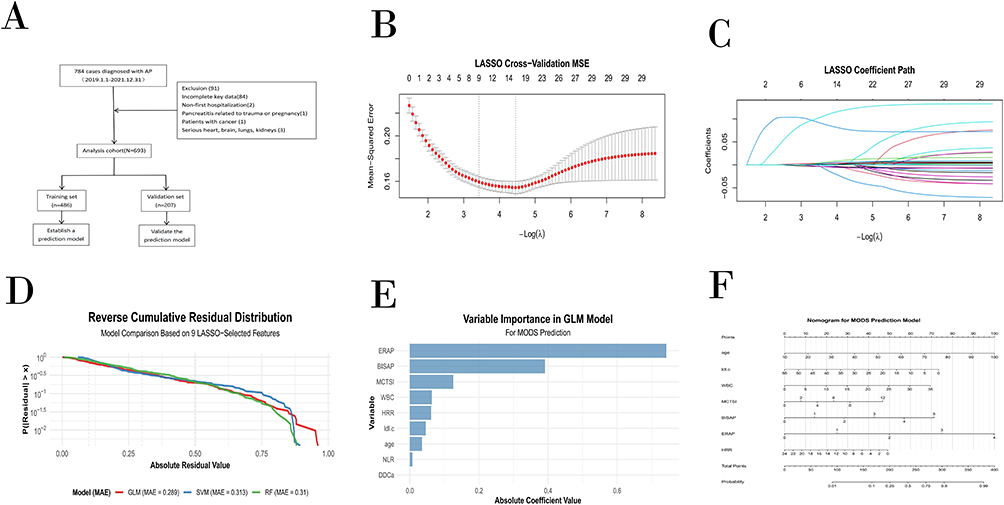 |
Figure 1 Development of the 7-variable nomogram for predicting multiple organ dysfunction syndrome (MODS) in acute pancreatitis. (A) Flowchart of patient selection and cohort allocation. (B–C) Least absolute shrinkage and selection operator (LASSO) regression for variable selection from 29 candidate predictors, identifying 9 key variables. (D) Comparison of residual distributions for generalized linear model (GLM), random forest (RF), and support vector machine (SVM) models built on the 9-predictor set. (E) Regression coefficients of the multivariable GLM. (F) Final 7-variable nomogram for predicting individual MODS risk. Abbreviations: MODS, multiple organ dysfunction syndrome; LASSO, least absolute shrinkage and selection operator; GLM, generalized linear mo RF, random forest; SVM, support vector machine; MSE, mean squared error; MAE, mean absolute error; AUC, area under the curve; BISAP, bedside index for severity in acute pancreatitis; MCTSI, modified computed tomography severity index; LDL-C (LDLC), low-density lipoprotein cholesterol; WBC, white blood cell count; ERAP, early risk assessment of acute pancreatitis; HRR, hemoglobin-to-red cell distribution width ratio; NLR, neutrophil-to-lymphocyte ratio; DDCa, D-dimer-to-calcium ratio. |
Patient Baseline Characteristics
This study included 693 patients with acute pancreatitis, of whom 240 (34.6%) developed MODS and 453 (65.4%) did not. As summarized in Table 1, baseline characteristics differed markedly between the two groups. Patients who developed MODS were older than those who did not (56.50 [44.00–69.00] vs 42.00 [33.00–56.00] years, P < 0.001) and had higher MCTSI, BISAP, and ERAP scores (all P < 0.001).
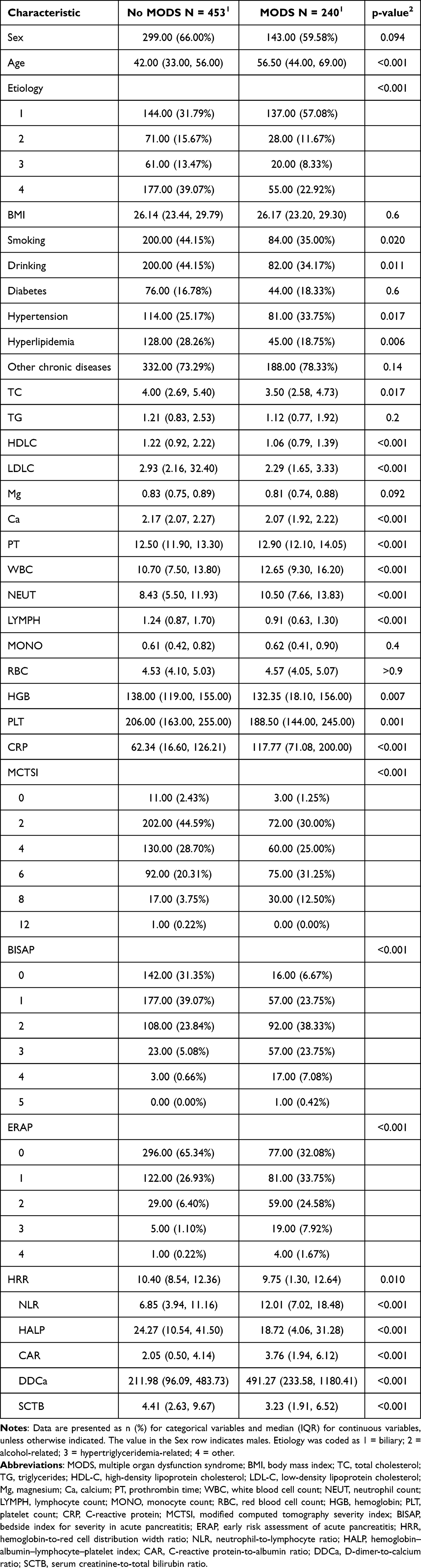 |
Table 1 Baseline Characteristics of Patients with Acute Pancreatitis Stratified by MODS |
The distribution of etiologies also differed significantly. Biliary pancreatitis was more common in the MODS group, whereas hyperlipidemic, alcoholic, and other etiologies were relatively more frequent in the non-MODS group (P < 0.001). In terms of laboratory findings, patients with MODS showed a more pronounced systemic inflammatory response, with higher white blood cell count (WBC), neutrophil-to-lymphocyte ratio (NLR), C-reactive protein-to-albumin ratio (CAR), and D-dimer-to-serum calcium ratio (DDCa) (all P < 0.001), together with lower lymphocyte count, hemoglobin-to-red cell distribution width ratio (HRR), and hemoglobin–albumin–lymphocyte–platelet (HALP) score (P = 0.010, P < 0.001, and P < 0.001, respectively).
Disturbances in lipid metabolism were also more evident in the MODS group: both low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C) levels were lower than those in the non-MODS group (both P < 0.001). Regarding comorbidities, hypertension was more prevalent in patients with MODS (33.8% vs 25.2%, P = 0.017), whereas hyperlipidemia was less frequent (18.8% vs 28.3%, P = 0.006). Taken together, these differences in etiology, disease severity, inflammatory burden, and metabolic status highlight substantial baseline heterogeneity between patients with and without MODS and provide a rationale for developing a prediction model for MODS in acute pancreatitis (Table 1).
Variable Selection
Baseline characteristics were broadly comparable between the training and validation sets, with no statistically significant differences for most clinical and laboratory variables (Supplementary Table 1). A slight difference was observed only for C-reactive protein (CRP), whereas all other key predictors remained well balanced between the two groups, indicating that the random split achieved an adequate distribution of patient features and provided a reasonable basis for subsequent variable selection and model development.
To identify the most informative predictors and reduce dimensionality, least absolute shrinkage and selection operator (LASSO) regression was applied to the training set. Starting from 29 candidate clinical variables, LASSO selected nine predictors associated with the development of MODS: age, low-density lipoprotein cholesterol (LDL-C), white blood cell count (WBC), modified CT severity index (MCTSI), BISAP score, ERAP score, hemoglobin-to-red cell distribution width ratio (HRR), neutrophil-to-lymphocyte ratio (NLR), and D-dimer-to-calcium ratio (DDCa) (Figure 1B and C). The optimal penalty parameter λ identified by cross-validation was 0.0325. Among the selected variables, LDL-C and HRR had negative regression coefficients, suggesting that higher levels of these markers may be associated with a lower risk of MODS.
Model Construction and Comparison
Based on the nine predictive variables selected by LASSO regression, we constructed three machine learning models—a generalized linear model (GLM), a random forest (RF), and a support vector machine (SVM)—to evaluate their performance in predicting MODS. When assessed using mean absolute error (MAE), the GLM performed best (MAE = 0.289), followed by the RF (MAE = 0.310) and SVM (MAE = 0.313). The mean residuals of all three models were close to zero (GLM: 0.028; SVM: 0.025; RF: 0.006), and the standard deviations of the residuals were similar (GLM: 0.376; SVM: 0.395; RF: 0.385). These findings indicate that none of the models showed obvious systematic bias and that the more complex RF and SVM models did not provide a meaningful improvement in predictive accuracy over the GLM. Overall, among the models built using the same set of predictors, the GLM provided the best balance between adequate accuracy and clinical interpretability and was therefore selected as the final modeling framework for subsequent nomogram construction (Figure 1D).
Regression Coefficient Analysis of Predictive Variables
Based on the nine variables selected by LASSO regression, we further examined their effects in a multivariable generalized linear model (logistic regression). The ERAP score had the largest positive regression coefficient (β = 0.755, P < 0.001), indicating a strong association with the development of MODS. Other variables with positive coefficients included BISAP score (β = 0.183, P = 0.281), modified CT severity index (MCTSI; β = 0.087, P = 0.159), white blood cell count (WBC; β = 0.053, P = 0.062), and age (β = 0.036, P < 0.001). In contrast, low-density lipoprotein cholesterol (LDL-C; β = −0.039, P < 0.001) and hemoglobin-to-red cell distribution width ratio (HRR; β = −0.073, P = 0.003) showed negative coefficients, suggesting that higher levels of these markers are associated with a lower risk of MODS. The D-dimer-to-calcium ratio (DDCa; β = 0.00021, P = 0.039) also reached statistical significance, although its effect size was very small. The neutrophil-to-lymphocyte ratio (NLR; β = 0.022, P = 0.129) did not achieve statistical significance in the multivariable model (Figure 1E).
Construction of the Predictive Nomogram
To develop a predictive tool that balanced parsimony with clinical utility, we further optimized the initial multivariable generalized linear model. Starting from the nine LASSO-selected predictors, we applied backward elimination in the multivariable logistic regression model. The neutrophil-to-lymphocyte ratio (NLR) was removed because it did not achieve statistical significance in the multivariable analysis (β = 0.022, P = 0.129) and contributed little to overall model performance. In contrast, the D-dimer-to-calcium ratio (DDCa) remained statistically significant (β = 0.00021, P = 0.039), but its regression coefficient was extremely small, indicating only a minimal effect on the predicted log-odds of MODS. In line with the principle of parsimony, DDCa was therefore also excluded to avoid unnecessary model complexity. The remaining seven core variables—age, LDL-C, WBC, MCTSI, BISAP, ERAP, and HRR—were incorporated into the final nomogram for individualized risk prediction (Figure 1F).
Performance Verification and Evaluation of the Final Model
The final 7-variable logistic regression model demonstrated strong predictive performance for MODS. In the training cohort (n = 486), the model achieved an AUC of 0.829, which was slightly higher in the independent validation cohort (AUC = 0.846). Using the optimal cutoff probability determined by the Youden index (0.28), the model yielded an accuracy of 0.773, sensitivity of 0.819, specificity of 0.748, positive predictive value of 0.634, and negative predictive value of 0.886 in the validation cohort, indicating good overall discriminative ability and particularly strong ruling-out capacity (Figure 2A).
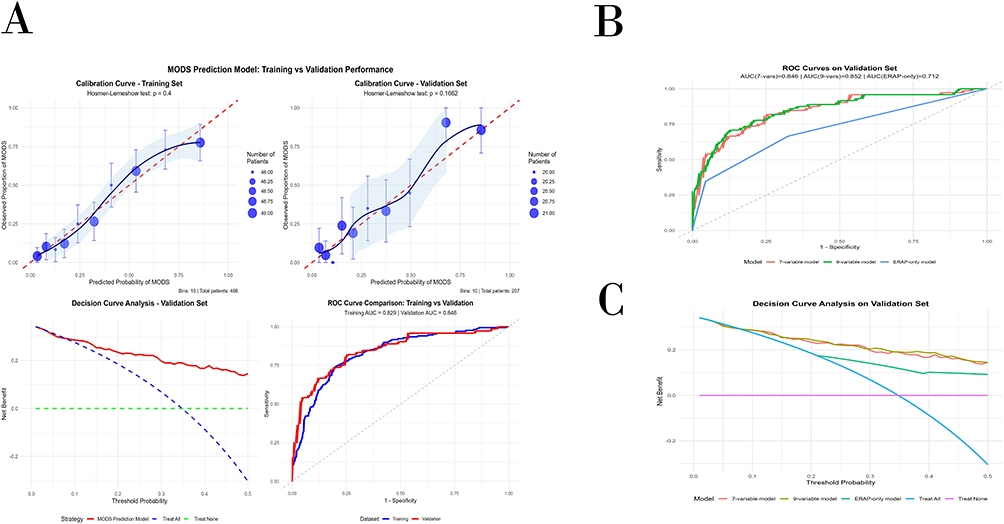 |
Figure 2 Comprehensive performance evaluation of the final 7-variable prediction model for multiple organ dysfunction syndrome (MODS). (A) Calibration curves in the training and validation cohorts. (B) Receiver operating characteristic (ROC) curves in the training and validation cohorts. (C) Decision curve analysis in the validation cohort. Abbreviations: MODS, multiple organ dysfunction syndrome; ROC, receiver operating characteristic; AUC, area under the curve; ERAP, early risk assessment of acute pancreatitis. |
Comparison with alternative models further highlighted the efficiency of the simplified approach. The 7-variable model retained nearly all the discriminative ability of the full 9-variable model (validation AUC: 0.846 vs 0.852), while markedly outperforming the ERAP-only model (AUC: 0.712). These findings underscore the incremental predictive value of combining ERAP with age, LDL-C, WBC, MCTSI, BISAP, and HRR in a unified framework (Figure 2B).
Subgroup analyses stratified by the etiology of acute pancreatitis demonstrated consistent performance across the major etiologic categories. In the validation cohort, the model achieved AUCs of 0.845 for biliary AP, 0.829 for alcoholic AP, and 0.864 for AP due to other causes. Corresponding sensitivity and negative predictive value remained high when applying the global cutoff of 0.28—for instance, 0.914/0.885 in biliary AP, 0.800/0.895 in alcoholic AP, and 0.800/0.922 in other etiologies. Performance was lower in hypertriglyceridemia-associated AP (AUC = 0.669; sensitivity/NPV = 0.429/0.778), likely reflecting both the small sample size and etiologic heterogeneity in this subgroup (Supplementary Table 2).
Calibration analyses further confirmed the reliability of the model. Calibration curves in both the training and validation cohorts showed close agreement between predicted and observed MODS probabilities, supported by non-significant Hosmer–Lemeshow tests (P > 0.05) and low Brier scores of 0.157 and 0.144, respectively.
Decision curve analysis showed that the 7-variable and 9-variable models provided substantially greater net clinical benefit across a wide range of threshold probabilities than the ERAP-only, treat-all, and treat-none strategies, with nearly overlapping net-benefit curves for the two multivariable models (Figure 2C).
Internal validation using 1000 bootstrap resamples and 10-fold cross-validation demonstrated good robustness, yielding an optimism-corrected C-index of approximately 0.839 (Figure 3). Taken together, these results support the 7-variable model as a well-calibrated, discriminative, and clinically practical tool for early MODS risk stratification in patients with acute pancreatitis.
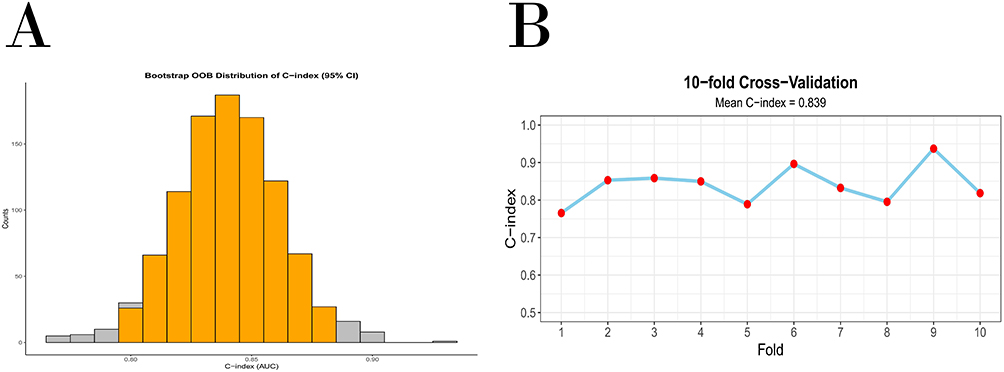 |
Figure 3 Internal validation of the 7-variable nomogram. (A) Bootstrap validation of the final model based on 1000 resamples. (B) Ten-fold cross-validation of the final model. Abbreviations: OOB, out-of-bag; C-index, concordance index; CI, confidence interval; AUC, area under the curve. |
Discussion
In this retrospective cohort of 693 patients with acute pancreatitis, we developed and internally validated a parsimonious 7-variable nomogram to predict the risk of multiple organ dysfunction syndrome (MODS) using clinical and laboratory data collected within the first 24 hours of admission. The model demonstrated good discrimination in both the training (AUC = 0.829) and validation cohorts (AUC = 0.846), together with favorable calibration and decision curve performance. At a pragmatic cutoff probability of 0.28, the nomogram achieved a high negative predictive value (0.886), supporting its primary role as an early rule-out tool for MODS. Importantly, the simplified 7-variable model retained almost all of the discriminative ability of the original 9-variable model, while clearly outperforming the ERAP score alone, and showed generally consistent performance across major etiological subgroups of acute pancreatitis.
Compared with existing prognostic tools in acute pancreatitis, our approach has several distinctive features. Traditional scoring systems such as SOFA, BISAP and the modified CT severity index (MCTSI) were not specifically designed to predict MODS as an independent outcome, but rather overall disease severity or mortality. SOFA is widely used to quantify established organ dysfunction and has been repeatedly associated with mortality in critically ill patients.12 BISAP and MCTSI have been validated for early risk stratification in acute pancreatitis, but they provide only a coarse categorization of severity and do not integrate newer dynamic inflammatory and metabolic markers.10,12 More recently, the ERAP score has been proposed as an easy-to-use emergency triage tool that combines respiratory rate, mental status, blood urea nitrogen and C-reactive protein to predict adverse outcomes in acute pancreatitis. Our findings confirm ERAP as the single strongest predictor within the multivariable model, but also show that combining ERAP with age, MCTSI, BISAP, white blood cell count, low-density lipoprotein cholesterol (LDL-C) and the hemoglobin-to-red cell distribution width ratio (HRR) yields substantially better discrimination than ERAP alone, without sacrificing bedside feasibility. Thus, the present nomogram can be viewed as an ERAP-anchored, MODS-focused extension of existing scoring systems.
The individual predictors included in the final model are biologically plausible and align with current understanding of MODS pathophysiology in acute pancreatitis. ERAP, BISAP and MCTSI collectively capture the global burden of systemic inflammatory response, early organ dysfunction and local pancreatic injury, which have all been strongly linked to persistent organ failure. Age and white blood cell count reflect baseline vulnerability and systemic inflammatory load, respectively, both of which predispose patients to progression from transient to persistent organ dysfunction. Of particular interest, LDL-C and HRR entered the model with negative coefficients, indicating that lower values are associated with increased MODS risk. Generally, low-density lipoprotein cholesterol (LDL-C) is considered a detrimental factor; however, our findings suggest that higher LDL-C may serve as a marker of lower risk against MODS in AP, whereas low LDL-C is associated with increased risk. A plausible explanation is that during the pathological process of AP, activated inflammatory cells (such as macrophages) extensively uptake and metabolize LDL-C via scavenger receptors to synthesize pro-inflammatory cytokines and reactive oxygen species, leading to a marked reduction in circulating LDL-C and indirectly reflecting the intensity of the inflammatory response.20 Clinical studies further indicate that low LDL-C levels are closely associated with the occurrence of persistent organ failure (POF), a core clinical phenotype of MODS, possibly through mechanisms involving lipid metabolism disorders, endothelial dysfunction and impaired microcirculatory perfusion.21 Notably, LDL-C levels have been reported to exhibit a U-shaped relationship with AP severity, whereby both excessively high and excessively low LDL-C concentrations are associated with a higher risk of severe acute pancreatitis; our results extend these observations by demonstrating that LDL-C behaves as an independent inverse predictor of MODS in this cohort.22 Several studies have also reported that reduced levels of LDL-C and high-density lipoprotein cholesterol are associated with necrotizing pancreatitis and worse outcomes in acute pancreatitis or critical illness, which is consistent with this mechanistic framework.
Similarly, HRR integrates information on anemia and red cell size heterogeneity, linking impaired oxygen-carrying capacity and heightened inflammatory stress.23,24 A lower HRR may therefore reflect both tissue hypoxia and a pro-inflammatory milieu, which jointly amplify the risk of multi-organ injury. Several recent studies have highlighted HRR and related hemoglobin-based composite indices (such as the HALP score) as prognostic markers in cardiovascular disease, critical illness and acute pancreatitis, with lower HRR consistently associated with higher short-term and long-term mortality.25,26 Our results are consistent with this mechanistic framework and extend previous observations by demonstrating that LDL-C and HRR preserve independent prognostic value for MODS even after adjustment for established severity scores.
From a clinical perspective, the main utility of our nomogram lies in early, individualized risk stratification during the first 24 hours of hospitalization. Because all seven predictors are routinely measured in standard care, the model can be readily implemented at the bedside or embedded within electronic health record systems. In practice, patients with a low predicted probability of MODS—for example, below the 0.28 cutoff used in this study—could be managed with close observation on a general ward, whereas those with intermediate or high predicted risk might warrant early admission to a monitored unit, more frequent reassessment of organ function or escalation of supportive therapies. The high negative predictive value observed across major etiologic subgroups (biliary, alcoholic and other causes) suggests that the nomogram is particularly well suited for ruling out MODS in a broad spectrum of patients, thereby helping clinicians prioritize intensive care resources for those at greatest risk. At the same time, performance was more modest in hypertriglyceridemia-associated acute pancreatitis, underscoring the need for cautious interpretation in this subgroup and for further refinement of the model in etiologically heterogeneous cohorts.9
This study has several limitations. First, it was a single-center, retrospective analysis based on routinely collected electronic health records from Shanxi Bethune Hospital; selection and information bias cannot be completely ruled out, and patterns of care in our institution may limit the generalizability of the findings to other settings. Second, although we attempted to minimize overfitting by adhering to an events-per-variable rule for sample size planning, using LASSO for variable selection, and performing bootstrap resampling and cross-validation, the nomogram underwent only internal validation. External validation in independent cohorts and prospective impact studies are required before it can be recommended for routine clinical use. Third, several potentially relevant variables—such as dynamic changes in laboratory parameters, detailed imaging-based severity scores, and novel inflammatory or lipid biomarkers—were unavailable or had excessive missingness and thus were not incorporated into the model, which may have resulted in residual confounding. Fourth, missing data were handled using multiple imputation under a missing-at-random assumption; we did not perform additional sensitivity analyses, such as complete-case analysis or varying prediction thresholds, so the robustness of our findings under different missing-data mechanisms and decision thresholds remains uncertain. Finally, the model was developed using variables collected within the first 24 hours of admission and was designed to predict early in-hospital MODS; its applicability to patients with late-onset organ dysfunction, recurrent acute pancreatitis, or different etiologic spectra should be explored in future studies.
Future prospective studies should therefore focus on validating and, if necessary, recalibrating this model in diverse populations, integrating it into real-time electronic decision-support systems, and evaluating whether its use can improve patient-centered outcomes such as MODS incidence, ICU utilization, and mortality.
Conclusion
Our internally validated 7-variable nomogram, based on a generalized linear model, showed good discrimination and a high negative predictive value for early prediction of multiple organ dysfunction syndrome in patients with acute pancreatitis. It may assist clinicians in early risk stratification and resource allocation, but external validation and prospective impact studies are needed before it can be routinely implemented in clinical practice.
Data Sharing Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to privacy and ethical restrictions regarding patient data. However, de-identified participant data may be made available after signing a data use agreement and upon approval from the relevant ethics committee.
Ethics Statement and Data Source
This study was reviewed and approved by the Ethics Committee of Shanxi Bethune Hospital (Approval No. YXLL-2023-237). Due to the retrospective nature of the research and the fact that all data were anonymized prior to analysis, posing no risk to patient privacy, the requirement for informed consent was waived by the ethics committee. This study was conducted in strict accordance with the ethical principles of the Declaration of Helsinki. The data for this study were derived from the clinical records of 784 patients diagnosed with acute pancreatitis at Shanxi Bethune Hospital between January 1, 2019, and December 31, 2021. All data were anonymized to protect patient privacy.
Author Contributions
All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Zongyuan Che: Conceptualization, Methodology, Software, Formal analysis, Data curation, Visualization, Writing – original draft.
Xuchen Zhao: Conceptualization, Methodology, Software, Formal analysis, Data curation, Writing – review & editing.
Wei Xue: Investigation, Validation, Writing – review & editing.
Zhiyao Wang: Data curation, Writing – review & editing.
Congzhong Hu: Conceptualization, Resources, Writing – review & editing.
Yulin Feng: Formal Analysis, Investigation, Validation, Writing – review & editing.
Ruijun Ru: Data curation, Validation, Visualization, Writing – review & editing.
Yanzhang Tian: Supervision, Project administration, Funding acquisition, Writing – review & editing.
Shaojian Mo: Conceptualization, Data Curation, Methodology, Funding acquisition, Writing – review & editing, Software, Resources.
Funding
This work was supported by the Science and Technology Cooperation and Exchange Project of Shanxi Province (202104041101024) and the Central Guidance on Local Science and Technology Development Fund (YDZJSX2025075).
Disclosure
The author(s) report no conflicts of interest in this work. During the preparation of this work, the author(s) used Gemini (Google) in order to polish and revise the paper for language clarity and to receive assistance with formatting. After using this tool/service, the author(s) reviewed and edited the content as needed and take full responsibility for the content of the paper.
References
1. Zheng Z, Ding YX, Qu YX, et al. A narrative review of the mechanism of acute pancreatitis and recent advances in its clinical management. Am J Transl Res. 2021;13(3):833–852.
2. Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62(1):102–111. doi:10.1136/gutjnl-2012-302779
3. Marshall JC. The multiple organ dysfunction syndrome. Surgical Treatment: Evidence-Based and Problem-Oriented. Zuckschwerdt; 2001. Available from https://www.ncbi.nlm.nih.gov/books/NBK6868/.
4. Petrov MS, Shanbhag S, Chakraborty M, et al. Organ failure and infection of pancreatic necrosis as determinants of mortality in patients with acute pancreatitis. Gastroenterology. 2010;139(3):813–820. doi:10.1053/j.gastro.2010.06.010
5. Schepers NJ, Bakker OJ, Besselink MG, et al. Impact of characteristics of organ failure and infected necrosis on mortality in necrotising pancreatitis. Gut. 2019;68(6):1044–1051. doi:10.1136/gutjnl-2017-314657
6. Asim M, Amin F, El-Menyar A. Multiple organ dysfunction syndrome: contemporary insights on the clinicopathological spectrum. Qatar Med J. 2020;2020(1):22. doi:10.5339/qmj.2020.22
7. Beger HG, Rau BM. Severe acute pancreatitis: clinical course and management. World J Gastroenterol. 2007;13(38):5043–5051. doi:10.3748/wjg.v13.i38.5043
8. Pathophysiology of septic shock | intechOpen. Available from: https://www.intechopen.com/chapters/1192748.
9. de-Madaria E, Buxbaum JL, Maisonneuve P, et al. Aggressive or moderate fluid resuscitation in acute pancreatitis. N Engl J Med. 2022;387(11):989–1000. doi:10.1056/NEJMoa2202884
10. Fei Y, Gao K, Li WQ. Prediction and evaluation of the severity of acute respiratory distress syndrome following severe acute pancreatitis using an artificial neural network algorithm model. HPB. 2019;21(7):891–897. doi:10.1016/j.hpb.2018.11.009
11. Szatmary P, Grammatikopoulos T, Cai W, et al. Acute pancreatitis: diagnosis and treatment. Drugs. 2022;82(12):1251–1276. doi:10.1007/s40265-022-01766-4
12. Pölkki A, Pekkarinen PT, Takala J, et al. Association of sequential organ failure assessment (SOFA) components with mortality. Acta Anaesthesiol Scand. 2022;66(6):731–741. doi:10.1111/aas.14067
13. Dalal AD, Dalal YD, Rana DA. Modified computed tomography severity index in evaluation of acute pancreatitis and its correlation with clinical outcome: a prospective observational study from a tertiary care teaching hospital, India. Ann Afr Med. 2023;22(3):340–346. doi:10.4103/aam.aam_79_22
14. Wu B, Yang J, Dai Y, Xiong L. Combination of the BISAP score and miR-155 is applied in predicting the severity of acute pancreatitis. Int J Gen Med. 2022;15:7467–7474. doi:10.2147/IJGM.S384068
15. Rasch S, Pichlmeier EM, Phillip V, et al. Prediction of outcome in acute pancreatitis by the qSOFA and the new ERAP score. Dig Dis Sci. 2022;67(4):1371–1378. doi:10.1007/s10620-021-06945-z
16. Phan NT, Vo DM, Huynh TM, et al. Evaluating the prognostic performance of the novel ERAP score in Vietnamese acute pancreatitis patients. Medicine. 2024;103(38):e39738.
17. Li Y, Xu C, Qin Z, Ge L. Relationship between the hemoglobin-to-red cell distribution width ratio and in-hospital mortality in patients with chronic heart failure. Vasc Health Risk Manag. 2024;20:553–565. doi:10.2147/VHRM.S486075
18. Zhang C, Peng W, Ning M, et al. Correlation between hemoglobin, albumin, lymphocyte, and platelet score and short-term mortality in critically ill patients. J Health Popul Nutr. 2025;44(1):36. doi:10.1186/s41043-025-00759-9
19. Antar R, Farag C, Xu V, Drouaud A, Gordon O, Whalen MJ. Evaluating the baseline hemoglobin, albumin, lymphocyte, and platelet (HALP) score in the United States adult population and comorbidities: an analysis of the NHANES. Front Nutr. 2023;10:1206958. doi:10.3389/fnut.2023.1206958
20. Hong W, Zimmer V, Stock S, et al. Relationship between low-density lipoprotein cholesterol and severe acute pancreatitis (“the lipid paradox”). Ther Clin Risk Manag. 2018;14:981–989. doi:10.2147/TCRM.S159387
21. Zhang Y, Guo F, Li S, et al. Decreased high density lipoprotein cholesterol is an independent predictor for persistent organ failure, pancreatic necrosis and mortality in acute pancreatitis. Sci Rep. 2017;7(1):8064. doi:10.1038/s41598-017-06618-w
22. Xanthomas: clinical and pathophysiological relations - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/24781043/.
23. Cai YL, Wang SQ, Zhong HJ, He XX. The effect of anemia on the severity and prognosis of patients with acute pancreatitis: a single-center retrospective study. Medicine. 2022;101(52):e32501. doi:10.1097/MD.0000000000032501
24. Khan NA, Haider Kazmi SJ, Asghar MS, et al. Hematological indices predicting the severity of acute pancreatitis presenting to the emergency department: a retrospective analysis. Cureus. 2021;13(7):e16752. doi:10.7759/cureus.16752
25. Rahamim E, Zwas DR, Keren A, et al. The ratio of hemoglobin to red cell distribution width: a strong predictor of clinical outcome in patients with heart failure. J Clin Med. 2022;11(3):886. doi:10.3390/jcm11030886
26. Xiong J, Tan H, Mao S, Ma L, Ma K. Association between hemoglobin-to-red blood cell distribution width ratio and 30-day mortality in patients with acute pancreatitis: data from MIMIC-III and MIMIC-IV. Turk J Gastroenterol. 2024;35(8):651–664. doi:10.5152/tjg.2024.24067
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.