Back to Journals » Infection and Drug Resistance » Volume 16
Development of a Nomogram for Predicting Massive Necrotizing Pneumonia in Children
Received 11 February 2023
Accepted for publication 17 March 2023
Published 29 March 2023 Volume 2023:16 Pages 1829—1838
DOI https://doi.org/10.2147/IDR.S408198
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Yonghan Luo, Yanchun Wang
Second Department of Infectious Disease, Kunming Children’s Hospital, Kunming, Yunnan, People’s Republic of China
Correspondence: Yanchun Wang, Second Department of Infectious Disease, Kunming Children’s Hospital, Kunming, Yunnan, 650000, People’s Republic of China, Email [email protected]
Objective: This study aimed to develop a nomogram model for predicting massive necrotizing pneumonia (NP) in children.
Methods: A total of 282 children with NP admitted to Kunming Children’s Hospital from January 2014 to November 2022 were enrolled. The children with NP were divided into massive necrotizing pneumonia (MNP) group and non-MNP group according to the severity of the lung necrosis. The clinical data of the children were collected, and least absolute shrinkage and selection operator (LASSO) regression and multivariate logistic regression models were used to analyze the influencing factors of MNP. A nomogram model was constructed, and its predictive efficacy was evaluated.
Results: The predictors selected by LASSO regression analysis were: haematogenous spread, white blood cell (WBC), hemoglobin (Hb), C-reactive protein (CRP), lactate dehydrogenase (LDH), and activated partial thromboplastin time (APTT) (P < 0.05). Based on the above independent influencing factors, a nomogram model for MNP was constructed. The bootstrap method was used to repeat sampling 1000 times. The results showed that the consistency index of the nomogram model in predicting MNP was 0.833 in the training set and 0.810 in the validation set. The results of ROC curve analysis showed that the area under the receiver-operating-characteristic curve (AUC) of the nomogram model for predicting MNP was 0.889 [95% CI (0.818, 0.959)] in the training set and 0.814 [95% CI (0.754, 0.874)] in the validation set. The calibration curve of the nomogram predicting MNP was basically close to the actual curve. The decision curve showed that the nomogram had good clinical utility.
Conclusion: We developed a nomogram for predicting MNP, which can help clinicians identify the severity of lung necrosis early.
Keywords: nomogram, children, necrotizing pneumonia, LASSO
Introduction
Necrotizing pneumonia (NP), also known as cavitary pneumonia or cavitary necrosis, is the liquefaction and necrosis of lung tissue on the basis of lung tissue consolidation.1 The clinical diagnosis is mainly based on imaging examination. NP is a rare and serious complication of community-acquired pneumonia (CAP) in children,2,3 which can occur in people of all ages. The incidence of NP in children has been increasing year by year since the beginning of this century.4,5 Mycoplasma pneumoniae, Streptococcus pneumoniae, Staphylococcus aureus, and other infections can lead to the occurrence of NP.6–9 The pathogenesis of pulmonary necrosis caused by different pathogens differs, as does the severity of lung damage.9,10 Mild pulmonary necrosis can be cured by anti-infection and anti-inflammatory treatment, while massive necrotizing pneumonia (MNP) requires surgical intervention, and more severe cases can eventually die.11–15 As a result, Li et al11 investigated the early warning indicators of massive lung necrosis in children with CAP in order to detect it early. However, this study’s sample size was small, and it is not clinically useful to predict the severity of NP using just one predictor. Considering the above reasons, we retrospectively analyzed the characteristics of all children with NP since the establishment of an electronic medical record system in our hospital. We tried to find out the early predictors of massive lung necrosis, establish a simple and practical prediction model, and provide a theoretical basis for the development of targeted diagnosis and treatment plans.
Methods
Data Source
The retrospective study was conducted at the Children’s Hospital affiliated with Kunming Medical University. The hospitalized children with NP from January 2014 to November 2022 were analyzed retrospectively. This study complied with the Declaration of Helsinki and was approved by the Ethics Review Committee of the Children’s Hospital affiliated with Kunming Medical University. Written informed consent was obtained from the guardian of each patient.
Study Population
The inclusion criteria were as follows: (a) hospitalized children under 18 years of age; (b) meet the clinical diagnostic criteria of pneumonia;16 and (c) chest CT showed segmental or lobular consolidation with enhanced hypodensity areas and/or necrotic cysts.
The exclusion criteria included any of the following: 1) patients with a history of chronic lung disease, immunodeficiency disease, connective tissue disease, or hematological disease; 2) cavitary lung diseases, including congenital lung diseases with infection, tuberculosis, lung cyst, etc.
The severity of pulmonary necrosis was determined by analyzing the chest CT with the largest relative ratio of necrotic tissue to the total lung area during hospitalization. More than 30% necrosis was included in the MNP group, and no more than 30% necrosis was included in the non-MNP group.11
Study Variables and Data Extraction
All clinical data were collected through the medical case system of the Children’s Hospital of Kunming Medical University. 1) General information, including sex, weight, and age. (2) Clinical features, including cough, hemoptysis, chest pain, wheezing, shortness of breath, rales, duration of fever, peak body temperature, haematogenous spread (3) radiological features, including pulmonary consolidation, atelectasis, and pleural effusion. (4) complications, including digestive system, nervous system, urinary system, circulatory system, blood system, and endocrine system. (5) Laboratory tests, including white blood cell (WBC), hemoglobin (Hb), neutrophil percentage, lymphocyte percentage, platelet (PLT), C-reactive protein (CRP), procalcitonin (PCT), alanine aminotransferase (AST), alanine aminotransferase (ALT), lactate dehydrogenase (LDH), albumin (Alb), prothrombin time (PT), activated partial thromboplastin time (APTT), Fibrinogen (FG), mycoplasma infection, viral infection, bacterial infection, co-infection. (6) treatment, including glucocorticoids, intravenous immune globulin (IVIG), intensive care unit (ICU) admission, thoracic close drainage, surgery, length of hospital stays, and hospitalization expenses.
Definition
Hematogenous spread is defined as the pathogen that causes NP not through direct respiratory infection but through blood flow from other parts of the body to the lungs. Patients who complain not of respiratory symptoms but of other systemic symptoms such as bone headaches and have specific pathogenic bacteria in their blood cultures will be considered to have hematogenous spread. Co-infection was defined as the detection of two or more of the three pathogens (bacteria, virus, or mycoplasma) in children with NP.
Statistical Analysis
SPSS 25.0 statistical software was employed for data processing. The continuous variables of a normal distribution were compared by t-test and expressed as X ± standard deviation, while the continuous variables of a non-normal distribution were compared by the Mann–Whitney test and expressed as the median of a quartile [M (P25, p75)]. Categorical variables were analyzed by χ2 test or Fisher’s exact test and expressed as numbers (n) and percentages (%). All samples were randomly divided into training and validation sets at a ratio of 7:3 using the “caret” package of R software. Least absolute shrinkage and selection operator (LASSO) regression of the “glmnet” package in R software was used to select variables, and multivariate logistic regression analysis was used to construct the nomogram model in training sets. The bootstrap method with 1000 repeated sampling, receiver-operating-characteristic (ROC) curve, the calibration curve, and the decision curve were used to evaluate the predictive ability of the nomogram model.
Outcome
Clinical Characteristics
Among 282 children with NP, 89 (33%) were MNP. Bacteria are the most common pathogens causing NP. They were Streptococcus pneumoniae (53 cases), Staphylococcus aureus (27 cases), Haemophilus influenzae (26 cases), and Acinetobacter Baumannii(7 cases). Other pathogens included Legionella pneumophila (3 cases), Klebsiella pneumoniae (2 cases), Pseudomonas aeruginosa (1 case), Staphylococcus epidermidis (1 case), and Moraxella catarrhalis (1 case). There were significant differences between the two groups in haematogenous spread, digestive systemomplications, WBC, Hb, neutrophil percentage, lymphocyte percentage, CRP, PCT, AST, ALT, LDH, Alb, APTT, co-infection, closed thoracic drainage, surgery, hospitalization duration, and hospitalization expenses (P < 0.05). The remaining indicators were not statistically significant between the two groups (P > 0.05) (See Table 1).
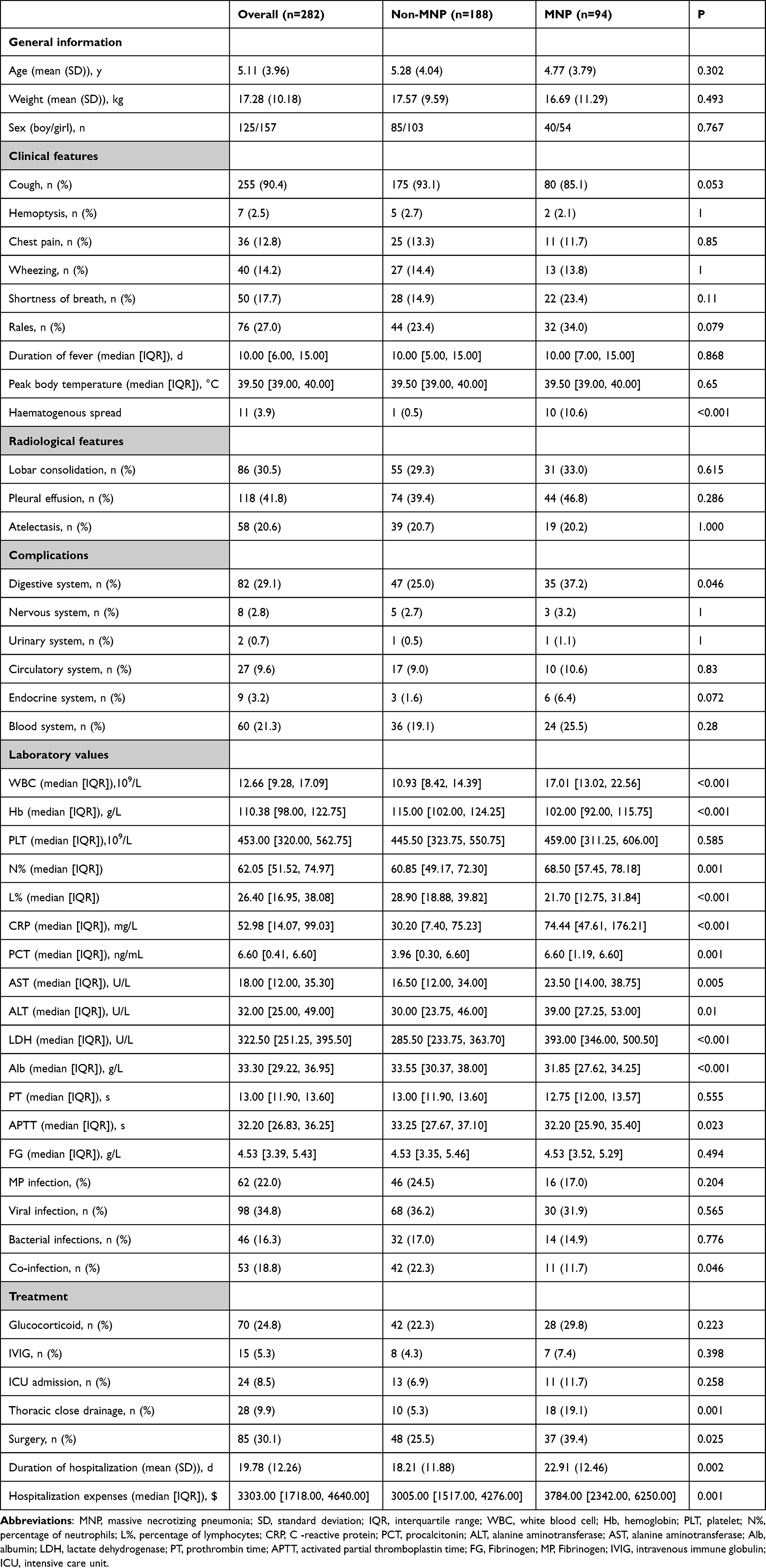 |
Table 1 The Clinical Characteristic and Laboratory Tests in MNP and Non-MNP |
Variable Selection
Since the aim of this study was to construct a model for early prediction of MNP, four variables (closed thoracic drainage, surgery, duration of hospitalization, and hospitalization expenses) representing the severity of the disease were excluded. Finally, 14 variables were chosen as candidate predictors, including haematogenous spread, digestive systemomplications, WBC, Hb, neutrophil percentage, lymphocyte percentage, CRP, PCT, AST, ALT, LDH, Alb, APTT and co-infection. Finally, haematogenous spread, WBC, Hb, CRP, APTT, and LDH were identified as risk factors for MNP using Lasso regression (see Figure 1).
 |
Figure 1 Predictors’ selection using LASSO (least absolute shrinkage and selection operator) regression method. (A) LASSO coefficient profiles of the 14 variables. The coefficient profile plot was produced against the log (λ) sequence. (B) The best penalty coefficient lambda was selected using a tenfold cross-validation and minimization criterion. By verifying the optimal parameter (λ) in the LASSO model, the binomial deviance curve was plotted versus log (λ) and dotted vertical lines were drawn. 6 variables with nonzero coefficients were selected by optimal lambda. |
Development of a Nomogram
A predictive nomogram containing six independent predictors (haematogenous spread, WBC, Hb, CRP, LDH, and APTT) was established by logistic regression (Figure 2). A patient with MNP who had haematogenous spread, for example, had a WBC of 15.5*109/L, Hb of 122 g/L, CRP of 200 mg/L, LDH of 590 U/L, and an APTT of 34s, totaling 262 (87 + 31 + 27 + 48 + 41 +28). The predicted risk is 0.942 (Figure 2).
 |
Figure 2 Nomogram was plotted based on six optimal predictors for massive necrotizing pneumonia in children. Abbreviations: WBC, white blood cell; Hb, hemoglobin; CRP, C-reactive protein; LDH, lactate dehydrogenase; APTT, activated partial thromboplastin time. |
Validation and Evaluation of the Nomogram
The bootstrap method was used for repeated sampling 1000 times. The results showed that the consistency index of the nomogram model in predicting MNP was 0.833 in the training set and 0.810 in the validation set. The results of ROC curve analysis showed that the AUC of the nomogram model predicting MNP was 0.889 [95% CI (0.818, 0.959)] in the training set and 0.814 [95% CI (0.754, 0.874)] in the validation set, respectively (Figure 3). Figure 4 shows that the calibration curve of the nomogram model predicting MNP was basically close to the actual curve. The Hosmer‐Lemeshow test showed good probability consistency between the predicted and actual probability in the training set and validation set (P = 0.211 and P = 0.792, respectively). The results of the decision curve analysis showed that when the threshold probability was between 0.10 and 0.70, the net benefit rate of the nomogram model in predicting MNP was greater than 0 in both the training set and the validation set, as shown in Figure 5. When the high-risk threshold was greater than 0.2 and 1000 patients were used for prediction, the clinical impact curve analysis revealed that the predicted number of patients was close to the actual number of patients (Figure 6).
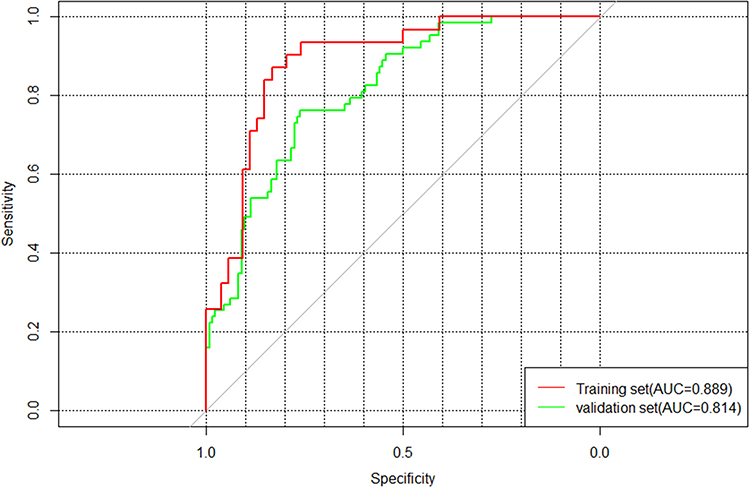 |
Figure 3 Receiver-operating-characteristic (ROC) curve of predictive nomogram in the training set and the validating set. |
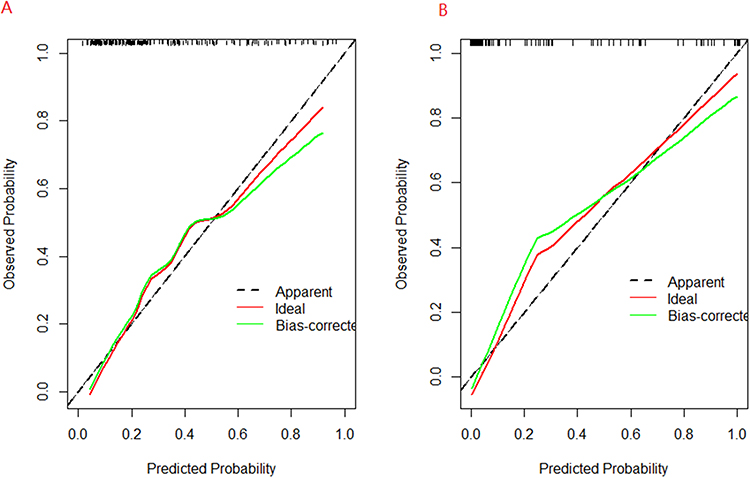 |
Figure 4 Calibration plots of the nomogram in (A) the training set and (B) the validating set. |
 |
Figure 5 Decision curve analysis (DCA) for the predictive model. (A) the training set. (B) the validating set. |
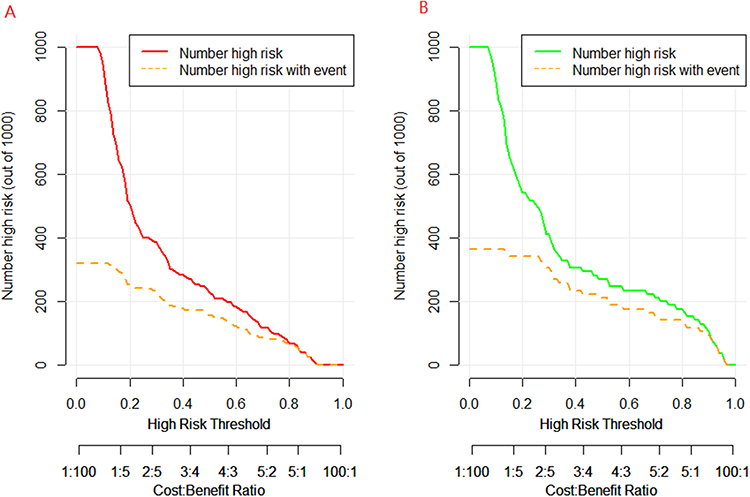 |
Figure 6 Clinical impact curves for the predictive model. (A) the training set. (B) the validating set. |
Discussion
NP belongs to severe pneumonia, which is a serious complication of CAP. It has been reported that the proportion of NP in CAP can reach 7%, which seriously affects the health of children. The average hospitalization cost for each child with NP in this study was US $3303, a substantial financial burden for most families. Therefore, if an effective method can be explored to predict the occurrence of MNP, it is likely to be of important guiding value for clinicians to judge the condition of children with CAP and make reasonable treatment plans. However, there are many risk factors for MNP. How to select predictive indicators and establish a good predictive model has become one of the most urgent clinical problems to be solved. The nomogram model can screen risk factors using a multivariate logistic regression model and transform complex regression equations and related risk factors into visual graphs that can be used as an endpoint event prediction tool.17 Because of its advantages of being intuitive and simple to understand, it has been widely used in disease prediction. In this study, a nomogram was developed based on six predictors, including haematogenous spread, WBC, Hb, CRP, LDH, and APTT. The validation of the model showed good prediction accuracy, calibration, and clinical practicability.
The variable haematogenous spread was selected as a predictor in this nomogram. Hematogenous infection is defined as the pathogen that causes NP not through direct respiratory infection but through blood flow from other parts of the body to the lungs. Only 11 patients (3%) developed NP as a result of haematogenous infection in our study, indicating that haematogenous spread is not the primary route of NP transmission. Of the 11 patients, 8 cases had pyogenic osteomyelitis or arthritis, and the causative bacteria in these cases were all Staphylococcus aureus (SA). The mechanism of NP caused by SA is mainly by adhering to and destroying respiratory cells. The inflammatory storm caused by SA will lead to apoptosis of tissue cells and necrosis of the alveolar membrane. Due to the widespread use of antibiotics in recent years, NP caused by methicillin-resistant Staphylococcus aureus (MRSA) has been widely reported. Li et al6 described a case of MRSA-caused community-acquired necrotizing pneumonia in which the child developed severe encephalitis as a result of a haematogenous infection. Our study confirmed that SA is more likely to cause MNP than other pathogens, and NP caused by SA requires a longer hospital stay and a higher proportion of surgery. It is suggested that we should always be alert to the possibility of systemic dissemination of SA infection, especially in the lungs, in the diagnosis and treatment of SA sepsis in children.
WBC and CRP are common markers of inflammation and are often used to predict the severity of pneumonia. As an important enzyme in the glycolytic pathway, LDH is widely distributed in all tissues of the body and is released into the blood in large quantities during inflammatory response. Therefore, LDH is also often used as a predictor of severe pneumonia.18,19 A retrospective analysis of NP by Li et al11 found that CRP is an independent predictor of the degree of lung necrosis. CRP > 48.35 mg/L had a high predictive value for the diagnosis of NP, according to Qian et al.7 Zhou et al20 found that WBC and CRP in the NP group caused by Mycoplasma pneumoniae were significantly higher than those in non-NP group. WBC > 12.3×10 9/L was found to be a predictor of lung necrosis by Zheng et al.21 WBC, CRP, and LDH were also selected as predictors in our prediction model, which was consistent with the conclusions of previous studies.
Although hemoglobin was frequently overlooked in NP research, secondary hemophagocytic lymphohistiocytosis (HLH) caused by severe pneumonia in children has been widely reported.22,23 The decrease of Hb is an important clinical manifestation of HLH. Therefore, we also analyzed the differences in Hb between the non-MNP and the MNP group, and found that Hb was an important correlation index of MNP. The occurrence of secondary HLH is related to the excessive activation of the systemic immune response, and the excessive immune response is an important pathogenesis of NP. The attention we pay to Hb will help us predict the occurrence of MNP in the early stages so as to carry out anti-inflammatory treatment as soon as possible.
The development of NP is not independently affected by a single factor, but is the comprehensive result of a variety of confounding factors. Therefore, the prediction of disease by a single indicator in previous studies is not clinically practical. Our model selected the optimal predictors from a wide range of confounders, and we were able to directly calculate the probability of MNP in a case of pneumonia with the visual nomogram. This greatly improves prediction accuracy and utility.
Our study still has some limitations. First, prediction models are best developed by validation in multiple centers, but multicenter data on NP are lacking. Second, due to the high absence rate, some predictors, such as D-dimer and INF-γ, were considered to be important predictors of the severity of NP but were excluded. Finally, as this study is retrospective, there are inevitably some selection biases.
Conclusions
We developed a nomogram for predicting MNP, which can help clinicians identify the severity of lung necrosis early.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chatha N, Fortin D, Bosma KJ. Management of necrotizing pneumonia and pulmonary gangrene: a case series and review of the literature. Can Respir J. 2014;21(4):239–245. doi:10.1155/2014/864159
2. Shi T, McAllister DA, O’Brien KL, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet. 2017;390(10098):946–958. doi:10.1016/S0140-6736(17)30938-8
3. Sawicki GS, Lu FL, Valim C, Cleveland RH, Colin AA. Necrotising pneumonia is an increasingly detected complication of pneumonia in children. Eur Respir J. 2008;31(6):1285–1291. doi:10.1183/09031936.00099807
4. Lemaître C, Angoulvant F, Gabor F, et al. Necrotizing pneumonia in children: report of 41 cases between 2006 and 2011 in a French tertiary care center. Pediatr Infect Dis J. 2013;32(10):1146–1149. doi:10.1097/INF.0b013e31829be1bb
5. Bender JM, Ampofo K, Korgenski K, et al. Pneumococcal necrotizing pneumonia in Utah: does serotype matter? Clin Infect Dis. 2008;46(9):1346–1352. doi:10.1086/586747
6. Li P, Dai L, Yuan K, et al. Necrotizing pneumonia and purulent meningitis caused by bloodstream infection of CA-MRSA in a child: a rare case report. Front Pediatr. 2022;10:1045774. doi:10.3389/fped.2022.1045774
7. Qian J, Wei YJ, Cheng YJ, Zhang Y, Peng B, Zhu CM. 儿童坏死性肺炎临床特征及危险因素分析 [Analysis of clinical features and risk factors of necrotizing pneumonia in children]. Beijing Da Xue Xue Bao Yi Xue Ban. 2022;54(3):541–547. Chinese. doi:10.19723/j.issn.1671-167X.2022.03.021
8. Surve RM, Das BP, Venkateswaran P, Kulanthaivelu K. Community acquired staphylococcus aureus necrotizing pneumonia and guillain barre syndrome: an unusual presentation in an adolescent patient. Neurol India. 2022;70(3):1200–1202. doi:10.4103/0028-3886.349608
9. Ness-Cochinwala M, Kobaitri K, Totapally BR. Characteristics and outcomes of children with necrotizing pneumonia. Pediatr Crit Care Med. 2021;22(12):e640–e643. doi:10.1097/PCC.0000000000002793
10. Yang B, Zhang W, Gu W, et al. Differences of clinical features and prognosis between Mycoplasma pneumoniae necrotizing pneumonia and non-Mycoplasma pneumoniae necrotizing pneumonia in children. BMC Infect Dis. 2021;21(1):797. doi:10.1186/s12879-021-06469-x
11. Li Q, Zhang X, Chen B, et al. Early predictors of lung necrosis severity in children with community-acquired necrotizing pneumonia. Pediatr Pulmonol. 2022;57(9):2172–2179. doi:10.1002/ppul.26020
12. Hsieh YC, Chi H, Chang KY, et al. Increase in fitness of Streptococcus pneumoniae is associated with the severity of necrotizing pneumonia. Pediatr Infect Dis J. 2015;34(5):499–505. doi:10.1097/INF.0000000000000631
13. Lai SH, Wong KS, Liao SL. Value of lung ultrasonography in the diagnosis and outcome prediction of pediatric community-acquired pneumonia with necrotizing change. PLoS One. 2015;10(6):e0130082. doi:10.1371/journal.pone.0130082
14. Khanafer N, Sicot N, Vanhems P, et al. Severe leukopenia in Staphylococcus aureus-necrotizing, community-acquired pneumonia: risk factors and impact on survival. BMC Infect Dis. 2013;13:359. doi:10.1186/1471-2334-13-359
15. Demirel N, Quizon A. Beltetón De Leon EL, Reiter J. On the nature of pleural involvement in necrotizing pneumonia: a report of two cases of life threatening late complications. Pediatr Pulmonol. 2014;49(3):E90–95. doi:10.1002/ppul.22943
16. Board E. 儿童社区获得性肺炎管理指南 (2013修订) [Guidelines for management of community acquired pneumonia in children (the revised edition of 2013) (I)]. Zhonghua Er Ke Za Zhi. 2013;51(10):745–752. Chinese.
17. Hu X, Yang B, Li J, et al. Individualized prediction of acute pancreatitis recurrence using a nomogram. Pancreas. 2021;50(6):873–878. doi:10.1097/MPA.0000000000001839
18. Zhang H, Yang J, Zhao W, et al. Clinical features and risk factors of plastic bronchitis caused by refractory Mycoplasma pneumoniae pneumonia in children: a practical nomogram prediction model. Eur J Pediatr. 2023;182(3):1239–1249. doi:10.1007/s00431-022-04761-9
19. Xie Q, Zhang X, Cui W, Pang Y. Construction of a nomogram for identifying refractory mycoplasma pneumoniae pneumonia among macrolide-unresponsive mycoplasma pneumoniae pneumonia in children. J Inflamm Res. 2022;15:6495–6504. doi:10.2147/JIR.S387809
20. Zhou Y, Hu M, Ye B, Chen Z, Zhang Y. Early prediction of necrotizing pneumonia from mycoplasma pneumoniae pneumonia with large pulmonary lesions in children. Sci Rep. 2020;10(1):19061. doi:10.1038/s41598-020-76083-5
21. Zheng B, Zhao J, Cao L. The clinical characteristics and risk factors for necrotizing pneumonia caused by Mycoplasma pneumoniae in children. BMC Infect Dis. 2020;20(1):391. doi:10.1186/s12879-020-05110-7
22. Gualdoni GA, Hofmann GA, Wohlfarth P, et al. Prevalence and outcome of secondary hemophagocytic lymphohistiocytosis among SIRS patients: results from a prospective cohort study. J Clin Med. 2019;8:4. doi:10.3390/jcm8040541
23. Yasutomi M, Okazaki S, Hata I, et al. Cytokine profiles in Mycoplasma pneumoniae infection-associated hemophagocytic lymphohistiocytosis. J Microbiol Immunol Infect. 2016;49(5):813–816. doi:10.1016/j.jmii.2014.11.015
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Characteristics of Necrotizing Pneumonia Caused by Different Pathogens
Luo Y, Wang Y
Infection and Drug Resistance 2023, 16:3777-3786
Published Date: 14 June 2023
Diagnosis of Early Bacterial Pneumonia and Sepsis After Cardiovascular Surgery: A Diagnostic Prediction Model Based on LASSO Logistic Regression
Zhang HT, Wang K, Li ZS, Wang CS, Han XK, Chen W, Fan FD, Pan J, Zhou Q, Cao HL, Pan HD, Hafu X, Li C, Fan GL, Pan T, Wang DJ, Wang W
Journal of Inflammation Research 2023, 16:3983-3996
Published Date: 11 September 2023
Dynamic Nomogram for Subsyndromal Delirium in Adult Intensive Care Unit: A Prospective Cohort Study
Cheng J, Lao Y, Chen X, Qiao X, Sui W, Gong X, Zhuang Y
Neuropsychiatric Disease and Treatment 2023, 19:2535-2548
Published Date: 22 November 2023
Development and Validation of a Risk Prediction Model for NAFLD: A Study Based on a Physical Examination Population
Yang C, Du T, Zhao Y, Qian Y, Tang J, Li X, Ma L
Diabetes, Metabolic Syndrome and Obesity 2024, 17:143-155
Published Date: 8 January 2024
Development and Validation of a Nomogram for Predicting Suicidal Ideation Among Rural Adolescents in China
Luo Y, Wang Y, Wang Y, Wang Y, Yan N, Shiferaw BD, Mackay LE, Zhang Z, Zhang C, Wang W
Psychology Research and Behavior Management 2024, 17:4413-4429
Published Date: 25 December 2024