Back to Journals » International Journal of Women's Health » Volume 18
Development of a Nomogram for Predicting 6-Month HPV Persistence After Cold Knife Conization in Chinese Women with High-Grade Squamous Intraepithelial Lesions
Received 2 July 2025
Accepted for publication 22 December 2025
Published 29 January 2026 Volume 2026:18 551082
DOI https://doi.org/10.2147/IJWH.S551082
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Qian Zhang, Xiaomei Tai, Lihua Jia
Department of Obstetrics and Gynecology, Maternal and Child Health Hospital of Tongzhou, Beijing, People’s Republic of China
Correspondence: Lihua Jia, Department of Obstetrics and Gynecology, Maternal and Child Health Hospital of Tongzhou, No. 124, Yuqiao Middle Road, Tongzhou District, Beijing, 010110, People’s Republic of China, Tel +86 18611998768, Email [email protected]
Purpose: This study aimed to develop and validate a nomogram to predict the risk of persistent human papillomavirus (HPV) infection after cold knife conization (CKC) in Chinese women with high-grade squamous intraepithelial lesions (HSIL).
Methods: A single-center retrospective study included 476 HPV-positive patients with HSIL who underwent CKC between January 1 2020 and December 31 2023. Patients were randomly divided into a training cohort (n=333) and a validation cohort (n=143) in a 7:3 ratio. Univariate and multivariate logistic regression analyses were used to identify predictors of HPV persistence after CKC, which was defined as the presence of the same HPV genotype both before and 6 months after surgical intervention. A nomogram was constructed using the independent risk factors. The validation of the prognostic model was evaluated by concordance index (C-index), calibration curves, and decision curve analyses (DCAs).
Results: HPV persistence was detected in 120 patients (25.21%) at 6 months post-CKC. Multivariate analysis revealed that the factors associated with HPV persistence after CKC were age, menopausal status, and number of types of HPV infections. The nomogram was constructed based on the above 3 factors. The nomogram demonstrated moderate and acceptable discrimination (AUC=0.700; 95% CI: 0.606– 0.794, Youden index = 0.30, sensitivity = 0.636, specificity = 0.664), good calibration, and positive net benefit in the validation cohort.
Conclusion: We successfully developed the first nomogram to predict the risk of HPV persistence at 6 months after CKC in Chinese women with HSIL using risk factors of age, menopausal status, and number of types of HPV infections, with HPV multiplicity being a novel and key predictor.
Keywords: HPV persistence, nomogram, cold knife conization, risk, high-grade squamous intraepithelial lesions
Introduction
Cervical cancer remains a global health burden, with persistent infection by high-risk human papillomavirus (HR-HPV) as its principal etiological agent.1 Fortunately, the well-characterized precancerous stages, collectively termed high-grade squamous intraepithelial lesions (HSIL) or cervical intraepithelial neoplasia grade 2/3 (CIN2/3), offer a critical window for intervention to prevent progression to invasive carcinoma. Among the established treatment modalities for HSIL/CIN2+, cold knife conization (CKC), which can effectively remove precancerous tissue, stands as a cornerstone surgical procedure.2
However, persistent HPV infection after CKC has been identified as a major risk factor of treatment failure and lesion recurrence. A 10-year retrospective cohort study found that the risk of residual or recurrent HSIL+ was higher in patients with HPV persistence after CKC.3 A cohort study by Byun et al4 similarly identified persistent HPV infection following CKC as a predictor of high-grade CIN recurrence. Understanding the factors influencing post-treatment HPV clearance is therefore paramount for optimizing patient management, risk stratification, and long-term outcomes.
Previously, Baser et al5 investigated risk factors for high-risk HPV persistence in women undergoing CKC for high-grade CIN, identifying patient age and cone depth as significant independent predictors. Zhang et al6 demonstrated that vaginal microecological imbalance (flora density, flora diversity, and dominant bacteria) was an independent risk factor for persistent HPV infection after CKC treatment in patients with HSIL. Gao et al7 conducted a retrospective study enrolled 334 patients with CIN2/3 and found that age was an important risk factor for the recovery of HPV infection after CKC surgery. Similarly, Zhang et al8 identified that age above 55 years was a prognostic factor for post-operative high-risk HPV infection clearance.
A prediction model which can predict the risk of HPV persistence after CKC could help women receive appropriate post-operative surveillance strategies. Failure to identify women at high risk for HPV persistence may lead to delayed intervention and an increased risk of lesion recurrence and progression to cervical cancer. To the best of our knowledge, no straightforward prediction model of HPV persistence after CKC has been constructed using the data from Chinese women. The nomogram is a simple-to-implement visualization tool for implementation of individual predictions. This study aims to develop a nomogram to predict HPV persistence after CKC, thereby improving risk assessment and ultimately enhancing long-term preventive management for women treated for cervical precancer.
Methods
Patients
This single-center retrospective study was approved by the ethics committee of our hospital in accordance with Declaration of Helsinki. Written informed consent was obtained from all patients.
In this retrospective study, we collected data from patients who underwent CKC at our hospital from January 1 2020 to December 31 2023 due to pathological results of colposcopy biopsy CIN2-CIN3. Inclusion criteria were as followed: (1) patients aged 18 years or older; (2) patients with pathological confirmation of HSIL (CIN2/3) under colposcopy; (3) preoperative HPV positive and clear typing results. (4) the patient underwent CKC; (5) informed consent of the patient. Exclusion criteria included: prior hysterectomy for any reason, concomitant malignancy, pregnancy, or incomplete follow-up data.
The enrolled patients were randomly separated into the training and validation sets in a 7:3 ratio. The training set was applied to construct the nomogram and the validation set was used to validate the nomogram.
Data Collection
HPV test results from all patients who met the standards at 6 months after surgery were collected. Persistent HPV infection was defined as the presence of the same HPV genotype both before and after surgical intervention.4 Patients with persistent HPV infection were included in the experimental group, while women without persistent HPV infection were included in the control group.
HPV testing was performed as follows: Cervical scrape specimens were collected from the squamocolumnar junction using a sampling brush. HPV genotyping was conducted using the 23-HPV Genotyping Real-time PCR Kit (Hybribio, China) according to the manufacturer’s instructions.
The selected factors for analysis, which were the potential confounders of HPV persistence after CKC, were identified in previous studies.5–8 The selected factors for analysis included age, gravidity, parity, preoperative HPV results, ThinPrep cytologic test (TCT) results, diameter and cone height of the cervical resection section and pathological status of surgical specimen edge. The data of above factors were obtained from the medical records in our hospital.
Statistical Analysis
Statistical analyses were performed using R software (version 3.6.2) and SPSS (version 23.0). The training set was used to develop a nomogram based on logistic regression analysis. Univariate analysis identified potential predictors of HPV persistence after CKC (p < 0.10). These selected factors were subsequently analyzed in a multivariable logistic regression model. The nomogram was constructed using the independent predictors identified in the final multivariable model. The validation set was then employed to assess the nomogram’s performance. Predictive accuracy was evaluated using calibration curves, while discrimination was assessed using receiver operating characteristic (ROC) curves. Decision curve analysis (DCA) evaluated the nomogram’s clinical utility. Results are presented as odds ratios (ORs) with corresponding 95% confidence intervals (CIs). Statistical significance was defined as p < 0.05. For nomogram development studies, sample size depends critically on the number of outcome events; at least 10 events per variable (EPV) are required.9
For greater transparency and replicability, the following specifics are noted: The continuous variable “age” was categorized into three groups (<35, 35–45, >45 years) based on both clinical relevance (reflecting reproductive stages and menopausal transition) and the distribution of our patient data to ensure sufficient sample size in each category for stable statistical estimation. The nomogram was constructed using the rms package in R software. The points assigned to each variable in the nomogram were derived directly from the scaled coefficients (beta values) of the final multivariable logistic regression model.
Results
During the study period, a total of 476 patients with HSIL who underwent CKC in our hospital were included in this study. Of these patients, 312 (65.55%) had CIN 2 and 164 (34.45%) had CIN 3. Mean patient age was 39.32 ± 9.46 years (range 22–70 years). 394 (82.77%) women were premenopausal and 82 (17.23%) were postmenopausal. Median gravidity and parity were 2 (range 0–8) and 1 (range 0–4), respectively. 72 (15.13%) patients were nulliparous and 404 (84.87%) had at least 1 prior delivery. In 73 (15.34%) patients, surgical margins were positive after the CKC procedure. HPV persistence after CKC was detected in 120 (25.21%) patients at 6 months after surgery. The enrolled patients were randomly divided into a training cohort (n = 333) and a validation cohort (n = 143) at a ratio of 7:3. The baseline characteristics of the two cohorts are shown in Table 1. The chi-square test results showed that the baseline characteristics in the training and validation cohorts were balanced (all p > 0.05). The proportion of patients with HPV persistence in the training and validation datasets was 26.13% and 23.08%, respectively.
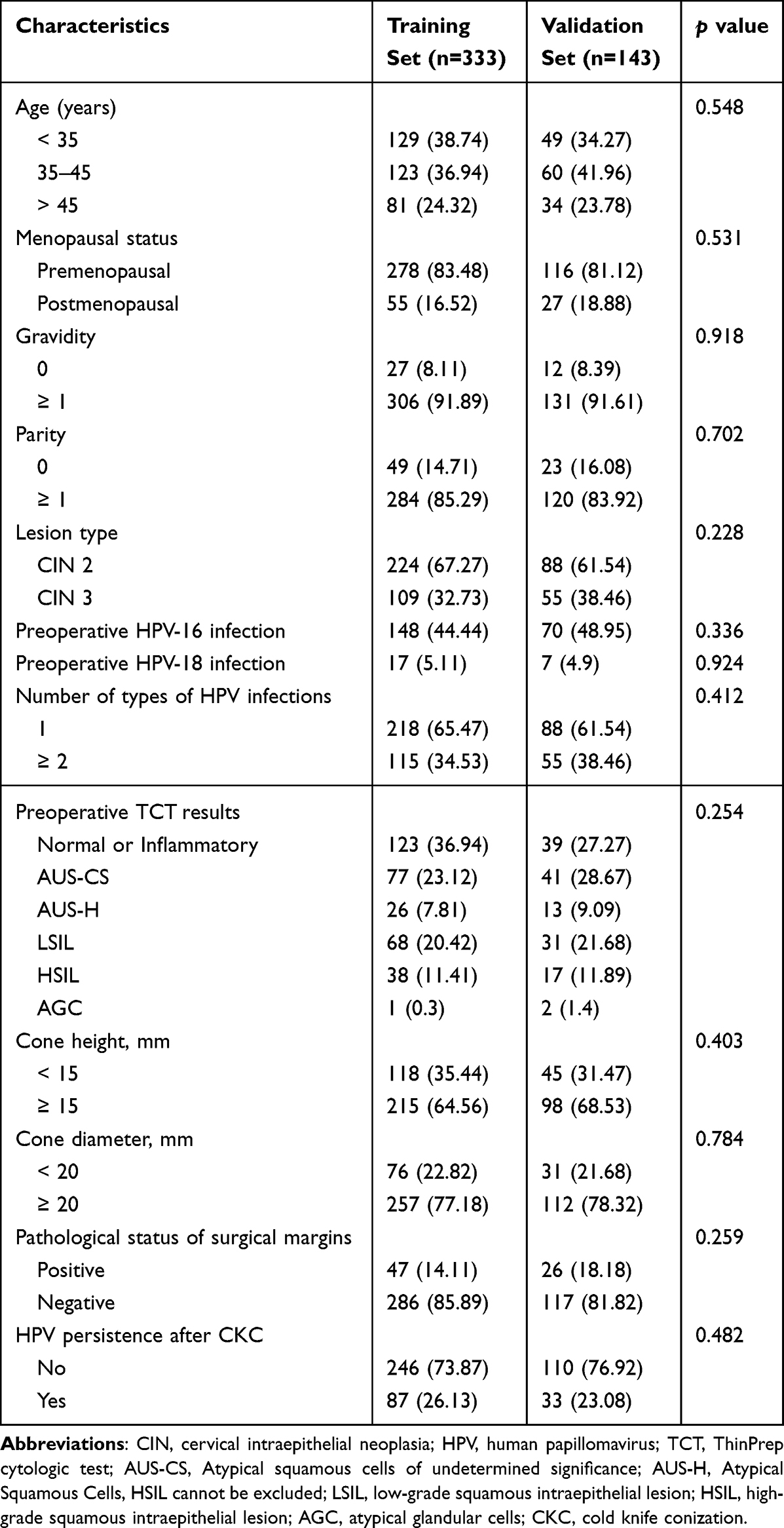 |
Table 1 The Demographic Data for the Enrolled Patients, n (%) |
We used univariate logistic regression to determine the risk factors associated with HPV persistence after CKC using the training set. The results showed that age (35–45 years vs < 35 years, p = 0.003; > 35 years vs.< 35 years, p < 0.001), menopausal status (postmenopausal status vs premenopausal status, p < 0.001) and number of types of HPV infections (≥ 2 vs 1, p = 0.007) were potential risk factors. Then, the selected factors obtained from the univariate analysis were analyzed in the multivariate logistic regression model. At the multivariate level, the factors associated with HPV persistence after CKC were age (35–45 years vs < 35 years, OR = 2.843, 95% CI = 1.398–5.781, p = 0.004; > 35 years vs.< 35 years, OR = 4.469, 95% CI = 1.644–12.146, p = 0.003), menopausal status (postmenopausal status vs premenopausal status, OR = 3.149, 95% CI = 1.175–8.440, p = 0.023) and number of types of HPV infections (≥ 2 vs 1, OR = 1.868, 95% CI = 1.076–3.243, p = 0.026). The results of the univariate and multivariate analyses are shown in Table 2.
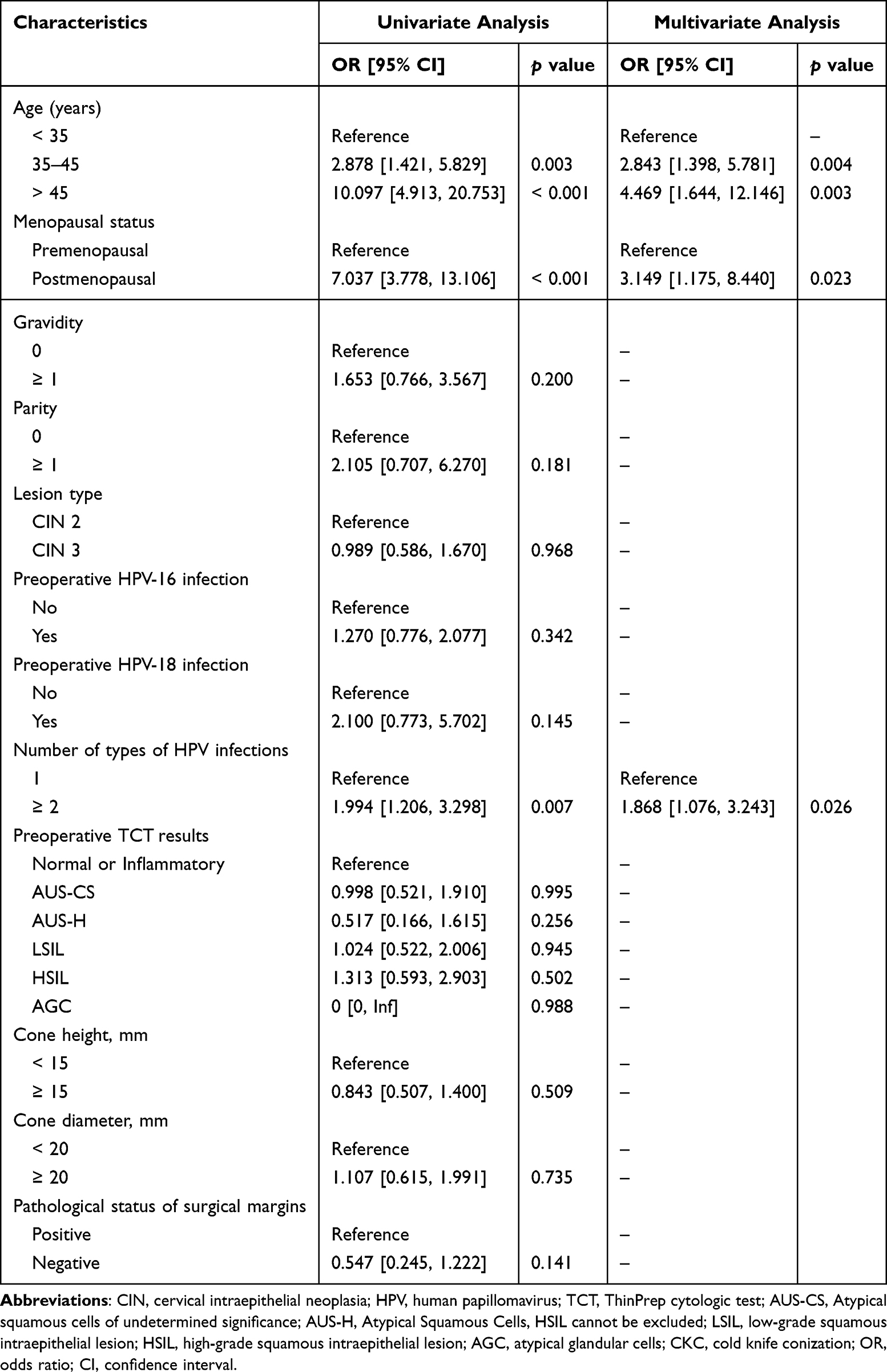 |
Table 2 Univariate and Multivariate Logistic Regression Analysis of Study Variables |
After variable selection, 3 risk factors were identified in the final multivariable model, including age, menopausal status and number of types of HPV infections. A nomogram for predicting risk of HPV persistence after CKC that integrated the above 3 independent prognostic factors is shown in Figure 1.
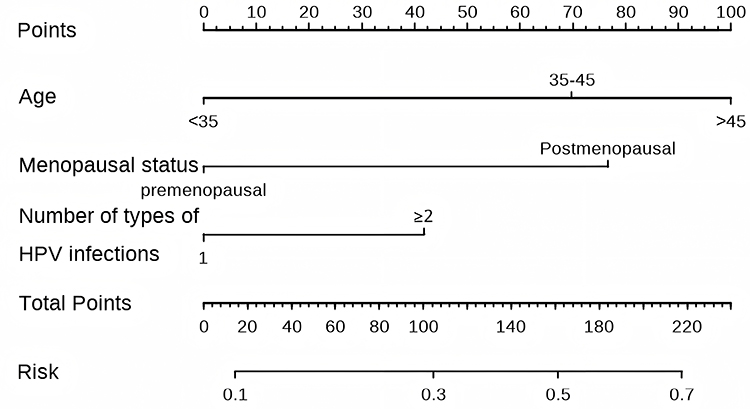 |
Figure 1 The nomogram for predicting HPV persistence after cold knife conization (CKC) in Chinese women with high-grade squamous intraepithelial lesions (HSIL). |
The nomogram’s performance was evaluated using the validation cohort. The area under the ROC curve (AUC) was 0.700 (95% CI: 0.606–0.794, p < 0.001), indicating good discriminative ability (Figure 2). The Youden index of the model was 0.30, with a sensitivity of 0.636 and a specificity of 0.664. Calibration plots demonstrated good agreement between the nomogram’s predicted risk of HPV persistence after CKC and actual observations (Figure 3). Decision curve analysis (DCA) further indicated that the nomogram provided substantial positive net clinical benefit for predicting HPV persistence risk (Figure 4).
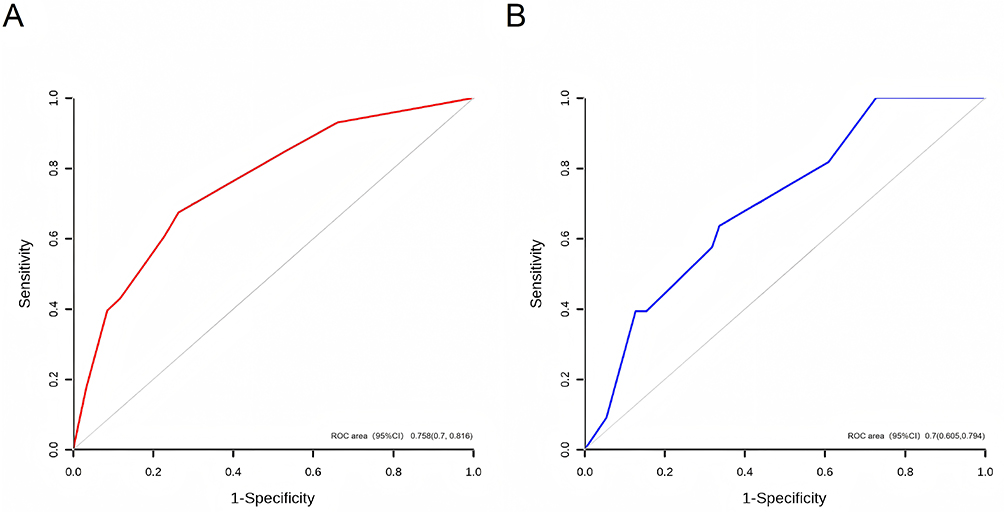 |
Figure 2 ROC curves of the established model for predicting risk of HPV persistence after cold knife conization. (A) training cohort, (B) validation cohort. Red curve (A): Represents the model’s performance in the training cohort (n=333), used to develop the nomogram. Blue curve (B): Represents the model’s performance in the validation cohort (n=143), used to independently test the nomogram’s predictive accuracy. Abbreviations: ROC, receiver operating characteristic; AUC, area under the curve. |
 |
Figure 3 Calibration curve of the model in the validation set. |
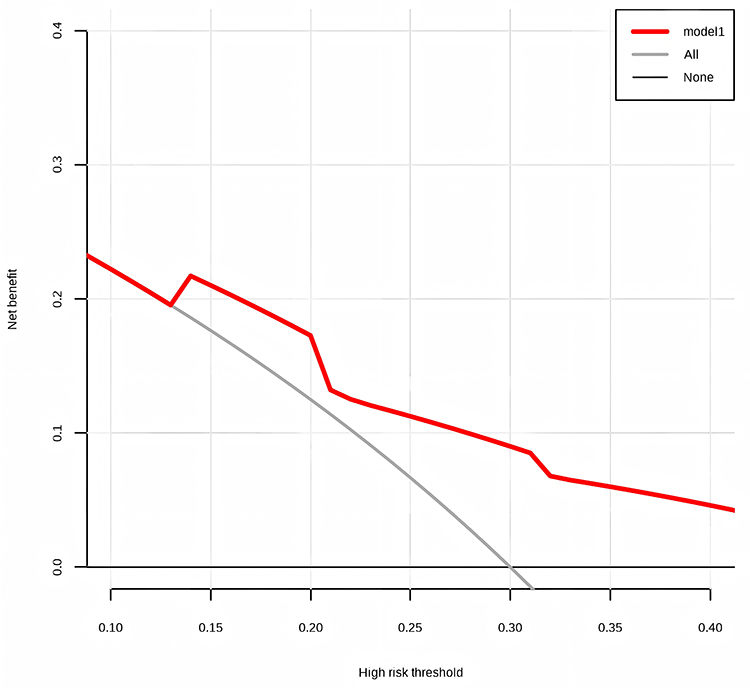 |
Figure 4 Decision curve analysis of the nomogram for predicting risk of HPV persistence after cold knife conization. |
Discussion
This study developed and validated a clinical prediction tool for a well-defined clinical scenario. While the identified predictors (age, menopausal status, HPV multiplicity) are not novel in themselves, the primary contribution of this work lies in their integration into the first nomogram for predicting HPV persistence after CKC specifically in Chinese women with HSIL. This addresses a gap in tailored risk assessment for this population.
Persistent infection with high-risk HPV genotypes has been described as the most common non-systemic biological risk factor for the development of cervical cancer.10,11 To better understand the factors influencing post-treatment HPV clearance, we conducted this study. The identified predictors in our final model align with the established literature on factors influencing HPV clearance post-treatment. The significant association of increasing age with higher risk of HPV persistence strongly corroborates previous studies. For instance, Baser et al5 identified age as a significant independent predictor of HPV persistence following CKC for high-grade CIN. Similarly, Gao et al7 in their retrospective study of CIN2/3 patients, found age to be an important risk factor for delayed HPV clearance post-CKC. Furthermore, Zhang et al8 specifically highlighted age ≥ 55 years as a poor prognostic factor for HPV clearance after CKC in CIN3 patients. Our study found a stepwise increase in risk of post-CKC HPV persistence across age groups (< 35, 35–45, > 45 years), particularly among women > 45 years, confirming that older age impairs post-treatment viral clearance. Studies indicate that immunosuppressive responses may facilitate HPV immune evasion, leading to persistent infection.10 In advanced age, immune changes due to “immune-senescence” could affect the acquisition and reactivation of HPV infections.12,13 Consequently, older patients exhibit increased risk of HPV persistence following CKC.
Our finding indicated that postmenopausal status was an independent predictor of HPV persistence after CKC, further supporting the role of age and hormonal milieu in HPV persistence. While not all prior studies explicitly separated menopausal status from chronological age, the hormonal changes associated with menopause, including alterations in local immunity and cervical epithelial characteristics, are biologically plausible contributors to reduced viral clearance efficiency.5 This aligns with the broader understanding that older age groups, predominantly including postmenopausal women, face higher HPV persistence risks.
A previous study enrolled 7372 Chinese women aged 18–45 years revealed that multiple HPV infections were observed in 25.2% of HPV-positive women, which increased the risk of cervical disease.14 In the present study, we found that multiple HPV type infections was another risk factor for HPV persistence after CKC. The inclusion of multiple HPV type infections (≥ 2 types) as a significant predictor of HPV persistence adds another dimension consistent with immunological principles. Co-infection with multiple HPV types implies either higher viral loads or inadequate immune control, resulting the impaired HPV clearance.15–17 While not directly replicated in every previous model, the association between HPV multiplicity and persistence risk is mechanistically sound. To our knowledge, this study presents the first nomogram developed specifically for predicting HPV persistence after CKC in Chinese women with HSIL. Its modest novelty and primary contribution lie in the incorporation of HPV multiplicity as a key, readily available predictor, alongside age and menopausal status, thereby offering a practical tool for initial individualized risk stratification in clinical practice.
Based on the risk factors of age, menopausal status, and the number of HPV types infected, we successfully developed a nomogram to predicate the risk of post-CKC HPV persistence in Chinese women. Our model has 3 predictor variables, so the number of positive events should be a minimum of 30.9,18 The actual number of positive events in the training cohort in the present study was 87, which was within the acceptable range. The discriminative performance of our nomogram (C-index = 0.700) is comparable to some existing models predicting related outcomes in cervical precancer management.19,20 While models incorporating more complex biomarkers might achieve higher AUCs. The calibration curve showing good agreement between predicted and observed risks, along with the positive net benefit demonstrated by DCA, further supports the model’s potential clinical applicability in risk stratification.
The present study has several limitations. Firstly, the single-center, retrospective design is a primary limitation of our study. The patient population from a single institution may not be fully representative of the broader Chinese population with HSIL, introducing potential selection bias. This limits the immediate generalizability of our findings and the nomogram’s applicability to other clinical settings. Secondly, the follow-up period was restricted to 6 months post-CKC. While this timeframe is clinically relevant for identifying early persistence and guiding initial post-operative management, it is insufficient to establish a definitive link between the predicted HPV persistence and the long-term risk of histologically confirmed lesion recurrence. Future studies with extended follow-up are needed to validate the nomogram’s prognostic value for predicting clinically significant endpoints like disease recurrence. Thirdly, the retrospective nature of our study limited the breadth of variables available for analysis. Several factors with known biological plausibility for influencing HPV persistence, such as vaginal microbiota composition, HPV viral load, and specific cellular immune responses, were not routinely tested or documented in the medical records and thus could not be included in our univariate analysis. This omission may mean our model does not capture the full spectrum of predictors. Additionally, key surgical variables such as the precise volume of the cone specimen, which is a function of both height and base dimensions, could not be accurately calculated or analyzed due to inconsistencies in retrospective documentation. The inclusion of cone volume might have improved the predictive accuracy of the model. Most importantly, our nomogram has only undergone internal validation. External validation using prospective, multi-center datasets is essential to confirm the model’s stability, calibrate its performance across different populations and clinical practices, and ultimately confirm its clinical utility before widespread adoption can be recommended.
Collectively, these limitations define clear pathways for future research and highlight that our model should be viewed as a foundational step. Its real-world applicability and potential to improve patient outcomes will be determined by successfully addressing these gaps, particularly through rigorous external validation and long-term outcome assessment.
The potential clinical utility of this nomogram lies in stratifying post-CKC surveillance intensity. For instance, based on the Youden index-derived probability threshold in our cohort, patients identified as “high-risk” (eg, with a predicted probability exceeding a certain value) could be considered for more frequent follow-up, such as co-testing (HPV and cytology) at shorter intervals (eg, 6–12 months) as per clinician judgment, or more intensive counseling regarding adherence to follow-up. Conversely, “low-risk” patients might adhere to standard follow-up protocols. However, the determination of an optimal, universally applicable risk threshold requires further prospective validation and cost-effectiveness analysis. This model provides a quantitative starting point for such personalized management discussions.
Conclusion
In conclusion, we have developed and internally validated a nomogram incorporating age, menopausal status, and HPV multiplicity to predict the risk of 6-month HPV persistence after CKC in Chinese women with HSIL. The model demonstrated moderate discriminative ability (AUC=0.700) and good calibration. While this tool represents a practical first step towards individualized risk assessment, its current utility is preliminary. The model’s performance warrants confirmation through external validation in independent, multi-center cohorts. Its generalizability is unproven and must be established through external validation in diverse settings before broader clinical implementation can be recommended. Future research should focus on this validation and on linking the predicted short-term persistence to long-term recurrence risks. Furthermore, future studies with longer follow-up are essential to establish the critical link between the predicted HPV persistence and the long-term risk of disease recurrence, which is the ultimate clinical endpoint.
Artificial Intelligence (AI)
The authors did not use generative AI or AI-assisted technologies in the development of this manuscript.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Maternal and Child Health Hospital of Tongzhou. Written informed consent was obtained from all participants.
Funding
This study did not receive any funding in any form.
Disclosure
All of the authors had no any personal, financial, commercial, or academic conflicts of interest separately.
References
1. Mayadev JS, Ke G, Mahantshetty U, et al. Global challenges of radiotherapy for the treatment of locally advanced cervical cancer. Int J Gynecol Cancer. 2022;32:436–10. doi:10.1136/ijgc-2021-003001
2. Li X, Liu M, Ji Y, Qu P. The effectiveness of cold-knife conization (CKC) for post-menopausal women with cervical high-grade squamous intraepithelial lesion: a retrospective study. BMC Surg. 2021;21:241. doi:10.1186/s12893-021-01238-8
3. Fu K, Yangzom K, Li L, Wu L, Zhang Y. Optimizing the follow-up interval after successful cold knife conization of CIN3: a 10-year retrospective cohort study. Cancer Med. 2025;14:e70825. doi:10.1002/cam4.70825
4. Byun JM, Jeong DH, Kim YN, et al. Persistent HPV-16 infection leads to recurrence of high-grade cervical intraepithelial neoplasia. Medicine. 2018;97:e13606. doi:10.1097/md.0000000000013606
5. Baser E, Ozgu E, Erkilinc S, et al. Risk factors for human papillomavirus persistence among women undergoing cold-knife conization for treatment of high-grade cervical intraepithelial neoplasia. Int J Obstet Gynaecol. 2014;125:275–278. doi:10.1016/j.ijgo.2013.12.012
6. Zhang S, Cao Y, Hu Y, Li G, Lan H. Correlation between persistent HPV infection and vaginal microecological imbalance after treatment of cervical high-grade squamous intraepithelial lesion. Altern Ther Health Med. 2024;30:414–418.
7. Gao S, Huang L, Wang T, Wang J. The effect of cervical Cold-Knife Conization (CKC) on HPV infection in patients with high-grade cervical intraepithelial neoplasia: a retrospective study. Int J Womens Health. 2023;15:1681–1691. doi:10.2147/ijwh.s429749
8. Zhang G, Lang J, Shen K, Zhu L, Xiang Y. High-risk human papillomavirus infection clearance following conization among patients with cervical intraepithelial neoplasm grade 3 aged at least 45 years. Int J Obstet Gynaecol. 2017;136:47–52. doi:10.1002/ijgo.12000
9. Riley RD, Ensor J, Snell KIE, et al. Calculating the sample size required for developing a clinical prediction model. BMJ. 2020;368:m441. doi:10.1136/bmj.m441
10. Ntuli L, Mtshali A, Mzobe G, Liebenberg LJ, Ngcapu S. Role of Immunity and Vaginal Microbiome in Clearance and Persistence of Human Papillomavirus Infection. Front Cell Infect Microbiol. 2022;12:927131. doi:10.3389/fcimb.2022.927131
11. Li W, Meng Y, Wang Y, et al. Association of age and viral factors with high-risk HPV persistence: a retrospective follow-up study. Gynecol Oncol. 2019;154:345–353. doi:10.1016/j.ygyno.2019.05.026
12. Giannella L, Rossi PG, Carpini GD, et al. Age-related distribution of uncommon HPV genotypes in cervical intraepithelial neoplasia grade 3. Gynecol Oncol. 2021;161:741–747. doi:10.1016/j.ygyno.2021.03.025
13. Burger EA, Kim JJ, Sy S, Castle PE. Age of acquiring causal Human Papillomavirus (HPV) Infections: leveraging simulation models to explore the natural history of HPV-induced cervical cancer. Clinl Infect Dis. 2017;65:893–899. doi:10.1093/cid/cix475
14. Su Y, Zheng T, Bi Z, et al. Pattern of multiple human papillomavirus infection and type competition: an analysis in healthy Chinese women aged 18–45 years. Hum Vaccines Immunother. 2024;20:2334474. doi:10.1080/21645515.2024.2334474
15. Gong P, Shi B, Cong X, et al. Multiple infections containing the top five prevalent HPV genotypes and their impact on cervical lesions in Changzhou, China. Hum Vaccines Immunother. 2023;19:2245723. doi:10.1080/21645515.2023.2245723
16. Oyervides-Muñoz MA, Pérez-Maya AA, Sánchez-Domínguez CN, et al. Multiple HPV infections and viral load association in persistent cervical lesions in Mexican women. Viruses. 2020;12:380. doi:10.3390/v12040380
17. Della Fera AN, Warburton A, Coursey TL, Khurana S, McBride AA. Persistent human papillomavirus infection. Viruses. 2021;13:321. doi:10.3390/v13020321
18. Riley RD, Debray TPA, Collins GS, et al. Minimum sample size for external validation of a clinical prediction model with a binary outcome. Stat Med. 2021;40:4230–4251. doi:10.1002/sim.9025
19. Liu Q, Yang J, Cheng H, et al. A clinical prediction model for pathologic upgrade to invasive carcinoma following conization of cervical high-grade squamous intraepithelial lesions. Cancer Med. 2025;14:e70540. doi:10.1002/cam4.70540
20. Bogani G, Tagliabue E, Ferla S, et al. Nomogram-based prediction of cervical dysplasia persistence/recurrence. Eur J Cancer Prev. 2019;28:435–440. doi:10.1097/cej.0000000000000475
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The m7G Modification Level and Immune Infiltration Characteristics in Patients with COVID-19
Lu L, Zheng J, Liu B, Wu H, Huang J, Wu L, Li D
Journal of Multidisciplinary Healthcare 2022, 15:2461-2472
Published Date: 26 October 2022
Establishment and Validation of a Risk Prediction Model for Sepsis-Associated Liver Injury in ICU Patients: A Retrospective Cohort Study
Li C, Ji J, Shi T, Pan S, Jiang K, Jiang Y, Wang K
Infection and Drug Resistance 2025, 18:1-13
Published Date: 1 January 2025