Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Development and Validation of the TCAP Nomogram for Predicting Hepatotoxicity Risk in Hepatocellular Carcinoma Patients Receiving TACE Combined with Systemic Therapy
Authors Ma S, Shi C, Chen J, Song J, Li J
Received 14 February 2026
Accepted for publication 17 March 2026
Published 25 March 2026 Volume 2026:13 600757
DOI https://doi.org/10.2147/JHC.S600757
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mohamed Shaker
Shuangshuang Ma,1,* Congcong Shi,2,* Jiao Chen,3 Jinlong Song,3 Jinpeng Li3
1Department of Oncologic Anesthesiology, Shandong Cancer Hospital and Institute, Shandong First Medical University and Shandong Academy of Medical Sciences, Jinan, Shandong, People’s Republic of China; 2Depression Disorder Diagnosis and Treatment Center, Shandong Mental Health Center, Jinan, Shandong, 250014, People’s Republic of China; 3Department of Interventional Therapy I, Shandong Cancer Hospital and Institute, Shandong First Medical University and Shandong Academy of Medical Sciences, Jinan, Shandong, 250117, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jinpeng Li, Department of Interventional Therapy I, Shandong Cancer Hospital and Institute, Shandong First Medical University and Shandong Academy of Medical Sciences, Jinan, Shandong, 250117, People’s Republic of China, Email [email protected]
Background and Aims: The combination of transarterial chemoembolization (TACE) with molecular targeted therapy and/or immune checkpoint inhibitors (ICIs) has emerged as a cornerstone treatment for intermediate-to-advanced hepatocellular carcinoma (HCC). However, the risk of hepatotoxicity associated with these multimodal regimens remains inadequately characterized. This study aimed to evaluate the incidence, severity, and independent predictors of hepatotoxicity, and to develop a clinically practical prediction model.
Materials and Methods: This retrospective study analyzed data from 200 HCC patients treated at Shandong First Medical University Affiliated Cancer Hospital between October 2021 and July 2024. Patients received either TACE plus tyrosine kinase inhibitors (TKIs) (n=120) or TACE plus TKIs and ICIs (n=80). Hepatotoxicity was graded according to CTCAE v5.0 criteria. Multivariate logistic regression was employed to identify independent risk factors and construct a predictive nomogram.
Results: The overall hepatotoxicity incidence was 38.00%, predominantly mild-to-moderate (Grade 1: 63.16%; Grade 2: 23.68%; Grade 3: 13.16%). No Grade 4 events occurred, and no significant difference was observed between treatment groups (P=0.637). Multivariate analysis identified four independent predictors: liver cirrhosis (OR=1.684), ALBI Grade 2/3 (OR=6.436), elevated total bilirubin (OR=1.040), and decreased prothrombin activity (OR=0.968). The resulting TCAP (Total bilirubin, Cirrhosis, ALBI grade, Prothrombin activity) nomogram demonstrated robust discriminatory performance (AUC=0.855) with a sensitivity of 82.00% and specificity of 79.10% at the optimal cut-off value of 0.419.
Conclusion: The TCAP nomogram provides a reliable, evidence-based tool for individualized hepatotoxicity risk stratification in HCC patients undergoing TACE-based combination therapy.
Keywords: hepatocellular carcinoma, transarterial chemoembolization, tyrosine kinase inhibitors, immune checkpoint inhibitors, hepatotoxicity, nomogram
Introduction
Hepatocellular carcinoma (HCC) represents a major global health burden, ranking as the sixth most common malignancy and the third leading cause of cancer-related mortality worldwide.1 In China, the disease poses an even greater challenge, with approximately 410,000 new cases and 390,000 deaths reported in 2020 alone, accounting for approximately 45% of the global HCC burden.2 The overwhelming majority of HCC cases (85%~90%) arise in the context of chronic liver disease, predominantly hepatitis B virus (HBV) infection and cirrhosis in endemic regions. Owing to the insidious nature of the disease and inadequate surveillance programs, the majority of patients present with intermediate-to-advanced stage disease, precluding potentially curative surgical interventions and resulting in historically poor 5-year survival rates below 20%.3
The therapeutic landscape for HCC has undergone a paradigm shift in recent years. Transarterial chemoembolization (TACE) has long served as the standard-of-care locoregional therapy for intermediate-stage HCC, functioning through dual mechanisms of tumor-feeding artery embolization and localized chemotherapeutic delivery.4 However, the efficacy of TACE monotherapy is often constrained by tumor heterogeneity, the development of collateral circulation, and progressive deterioration of hepatic functional reserve. The landmark IMbrave150 trial established the combination of atezolizumab and bevacizumab as a new first-line standard for advanced HCC, demonstrating superior overall survival compared with sorafenib (median OS: 19.2 vs. 13.4 months; HR=0.58).5 Subsequently, the HIMALAYA trial validated the efficacy of tremelimumab plus durvalumab (STRIDE regimen), further expanding the therapeutic armamentarium.6 In parallel, recent reviews have highlighted both the therapeutic potential and the safety concerns of immunotherapy in HCC, particularly with respect to liver-related adverse events and patient selection in complex clinical settings.7,8 The TACTICS trial demonstrated that combining TACE with sorafenib significantly improved progression-free survival compared with TACE alone, establishing a rationale for multimodal approaches.9
These advances notwithstanding, the synergistic efficacy of combination regimens is accompanied by compounded hepatotoxicity risks. The ischemia-reperfusion injury inherent to TACE procedures, the metabolic hepatotoxicity of tyrosine kinase inhibitors (TKIs), and immune-mediated hepatitis associated with ICIs represent distinct but potentially overlapping mechanisms of liver injury.10,11 Recent literature has further emphasized the expanding role of immunotherapy in HCC while also underscoring the need for careful evaluation of hepatic safety and treatment tolerance in patients with impaired underlying liver reserve.12,13 Importantly, these mechanisms may differ in their temporal patterns and pathophysiological characteristics. Acute liver injury following TACE is primarily related to ischemia–reperfusion damage and embolization-induced hypoxia in the surrounding liver parenchyma, which typically manifests within several days after the procedure. In contrast, immune-related hepatitis induced by ICIs is mediated by immune activation and inflammatory infiltration of hepatic tissue and may present later during systemic therapy. Recognizing these mechanistic and temporal differences is important when interpreting early hepatotoxicity events and provides a rationale for the short-term liver function monitoring window adopted in this study. Previous studies have reported hepatotoxicity incidence rates ranging from 15% to 50% in patients receiving systemic therapy for HCC, with the risk further amplified when combined with locoregional interventions.14,15 Severe hepatotoxicity necessitating treatment interruption or discontinuation can significantly compromise therapeutic efficacy and overall survival, underscoring the critical importance of hepatic functional reserve preservation in treatment planning.
Despite the clinical significance of this issue, there remains a paucity of validated predictive tools specifically designed to assess hepatotoxicity risk in patients undergoing TACE combined with systemic therapy. The albumin-bilirubin (ALBI) grade, developed by Johnson et al as an objective measure of liver function in HCC patients, has demonstrated superior prognostic performance compared with the traditional Child-Pugh classification.16 Building upon this foundation, the modified ALBI (mALBI) grading system has shown enhanced sensitivity in detecting subtle deteriorations in liver function.17 However, comprehensive risk prediction models incorporating multiple clinical parameters for hepatotoxicity assessment in the context of combination therapy remain lacking.
To address this knowledge gap, the present study retrospectively analyzed clinical data from 200 HCC patients who underwent TACE combined with TKIs and/or ICIs at our institution. Our primary objectives were to: (1) characterize the incidence and severity profile of hepatotoxicity; (2) identify independent risk factors through multivariate analysis; and (3) develop and validate a clinically practical nomogram prediction model to facilitate individualized risk stratification and guide clinical decision-making in this era of multimodal HCC therapy.
Materials and Methods
Study Design and Patient Selection
This retrospective cohort study analyzed clinical data from patients with HCC treated at Shandong First Medical University Affiliated Cancer Hospital between October 2021 and July 2024. The study protocol was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Institutional Ethics Committee. Given the retrospective nature of the analysis, the requirement for written informed consent was waived.
Inclusion Criteria: ① Age ≥18 years; ② Histologically or radiologically confirmed HCC diagnosis according to the 2022 Chinese Guidelines for the Diagnosis and Treatment of Primary Liver Cancer;18 ③ Barcelona Clinic Liver Cancer (BCLC) stage B or C, or CNLC stage Ib-IIIb; ④ Eastern Cooperative Oncology Group (ECOG) performance status 0–1; ⑤ Child-Pugh class A or B liver function; ⑥ Treatment with TACE combined with TKIs for ≥2 months and/or ICIs for ≥3 cycles; ⑦ Complete baseline and follow-up laboratory data.
Exclusion Criteria: ① ECOG performance status ≥2; ② Complete main portal vein thrombosis with inadequate collateral circulation; ③ Severe cardiac, pulmonary, or renal dysfunction; ④ Incomplete clinical data or loss to follow-up.
Data Collection and Assessments
Demographic and clinical variables collected included age, sex, viral etiology, cirrhosis status, tumor characteristics (size, number, vascular invasion, extrahepatic metastasis), and tumor staging according to the China Liver Cancer (CNLC) staging system.18 Laboratory parameters assessed included complete blood count, liver function tests (albumin [Alb], total bilirubin [TBil], alanine aminotransferase [ALT], aspartate aminotransferase [AST]), coagulation profile (prothrombin time [PT], prothrombin activity [PTA]), and alpha-fetoprotein (AFP).
All laboratory assessments were performed within one week prior to treatment initiation and 3–7 days following each treatment cycle using standardized automated analyzers. The upper limits of normal (ULN) for transaminases were defined as ALT 50 U/L and AST 40 U/L for males, and ALT 40 U/L and AST 35 U/L for females, in accordance with institutional reference ranges.
The modified albumin-bilirubin (mALBI) grade was calculated using the formula: ALBI score = 0.66 × log10 (TBil, μmol/L) − 0.085 × (Alb, g/L). All total bilirubin measurements were standardized and recorded in μmol/L, and albumin levels were reported in g/L, consistent with the conventional ALBI calculation method. Patients were subsequently stratified into four grades: Grade 1 (≤−2.60), Grade 2a (>−2.60 to −2.27), Grade 2b (>−2.27 to −1.39), and Grade 3 (>−1.39).14
Treatment Protocols
TKI Administration
All TKIs were administered orally according to standard dosing regimens. Lenvatinib (n=130) was administered at 8–12 mg once daily (body weight-adjusted dosing), donafenib (n=55) at 200 mg twice daily, and apatinib (n=15) at 250 mg once daily. Dose modifications were implemented according to manufacturer guidelines based on individual tolerability.
ICI Administration
ICIs were administered via intravenous infusion every three weeks. The agents utilized included camrelizumab (n=115, 200 mg/cycle), sintilimab (n=38, 200 mg/cycle), tislelizumab (n=35, 200 mg/cycle), and atezolizumab (n=12, 1200 mg/cycle).
TACE Procedure
TACE procedures were performed in accordance with the Chinese Clinical Practice Guidelines for Transarterial Chemoembolization in Hepatocellular Carcinoma (2021 Edition).19 Under local anesthesia, femoral artery access was established using the Seldinger technique. Following diagnostic angiography to assess portal vein patency and identify tumor-feeding arteries, superselective catheterization of the tumor-feeding vessels was achieved using a coaxial microcatheter system. Embolization was performed using a mixture of iodized oil (Lipiodol) and chemotherapeutic agents (epirubicin, cisplatin, or their combination) or drug-eluting beads, with the endpoint being complete cessation of arterial flow to the tumor.
Assessment of Hepatotoxicity
Hepatotoxicity was evaluated and graded in accordance with the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0.20 The primary assessment timepoint was 3–7 days following combination therapy initiation. Hepatotoxicity was defined as: (1) new-onset elevation of liver function parameters above ULN in patients with normal baseline values, or (2) significant worsening of pre-existing hepatic dysfunction (≥1 grade increase from baseline) following treatment.
For this analysis, patients were categorized into two outcome groups: those with any hepatotoxicity (CTCAE Grade ≥1) and those without hepatotoxicity.
Statistical Analysis
Statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA) and R software version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria). Continuous variables were assessed for normality using the Shapiro-Wilk test and expressed as mean ± standard deviation (SD) or median (interquartile range [IQR]) as appropriate. Categorical variables were reported as frequencies (percentages).
Comparisons between groups were performed using the Student’s t-test or Mann-Whitney U test for continuous variables and the chi-square test or Fisher’s exact test for categorical variables, as appropriate. Univariate and multivariate logistic regression analyses were conducted to identify independent risk factors for hepatotoxicity. Variables with P<0.10 in univariate analysis were entered into the multivariate model using a forward stepwise selection procedure.
Based on the identified independent predictors, a nomogram was constructed using the “rms” package (version 6.2–0) in R software version 4.0.3. Model discrimination was evaluated using the area under the receiver operating characteristic (ROC) curve (AUC) with 95% confidence intervals (CI). The optimal cut-off value was determined using the maximum Youden index. Model calibration was assessed using the Hosmer-Lemeshow goodness-of-fit test and calibration curves. Internal validation was performed using bootstrap resampling with 1000 iterations. Decision curve analysis (DCA) was conducted to evaluate the clinical utility of the model. All statistical tests were two-sided, and P<0.05 was considered statistically significant.
Results
Patient Demographics and Baseline Characteristics
A total of 200 eligible HCC patients were enrolled in this study. The mean age was 59.6 ± 9.3 years, with a male predominance (n=169, 84.50%). Chronic HBV infection was the predominant etiology (n=178, 89.00%). Liver cirrhosis was present in 200 patients, with compensated cirrhosis in 105 (52.50%) and decompensated cirrhosis in 95 (47.50%).
According to the CNLC staging system, patients were distributed as follows: stage Ib (n=74, 37.00%), stage IIa (n=21, 10.50%), stage IIb (n=55, 27.50%), stage IIIa (n=27, 13.50%), and stage IIIb (n=23, 11.50%). Portal vein tumor thrombosis was present in 42 patients (21.00%), and extrahepatic metastases were identified in 23 patients (11.50%).
Regarding treatment stratification, 120 patients (60.00%) received TACE combined with TKIs (Targeted Therapy group), while 80 patients (40.00%) underwent TACE combined with TKIs and ICIs (Combination group). The baseline mALBI grade distribution was as follows: Grade 1 (n=44, 22.00%), Grade 2a (n=49, 24.50%), Grade 2b (n=97, 48.50%), and Grade 3 (n=10, 5.00%). Detailed baseline characteristics are summarized in Table 1.
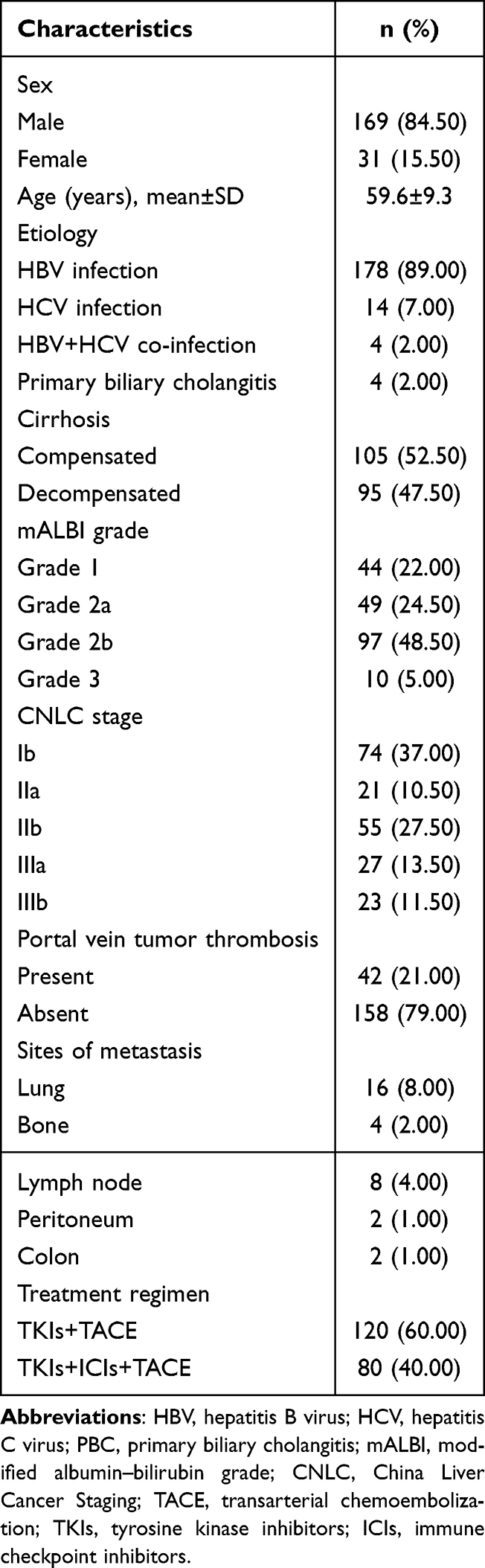 |
Table 1 Baseline Clinical Characteristics of 200 Patients with Primary Liver Cancer |
Incidence and Severity of Hepatotoxicity
Based on CTCAE v5.0 assessment criteria, the overall incidence of hepatotoxicity was 38.00% (n=76). The severity distribution demonstrated a predominance of mild hepatotoxicity, with Grade 1 accounting for 48 cases (63.16%), Grade 2 for 18 cases (23.68%), and Grade 3 for 10 cases (13.16%). Notably, no Grade 4 (life-threatening) hepatotoxicity events were observed in the study cohort. Temporal assessment indicated that the majority of hepatotoxicity events occurred within the early 3–7 day post-treatment window, while a smaller proportion of patients exhibited delayed biochemical abnormalities during subsequent follow-up evaluations.
Subgroup analysis stratified by treatment regimen revealed comparable hepatotoxicity profiles between groups. In the TKI + TACE group, the incidence rates of Grade 1, 2, and 3 hepatotoxicity were 23.33%, 8.33%, and 5.00%, respectively. Similarly, in the TKI + ICI + TACE group, the corresponding rates were 25.00%, 10.00%, and 5.00%. Statistical analysis demonstrated no significant difference between the two treatment groups with respect to either the overall incidence or severity distribution of hepatotoxicity (χ2=1.299, P=0.637). Detailed results are presented in Table 2.
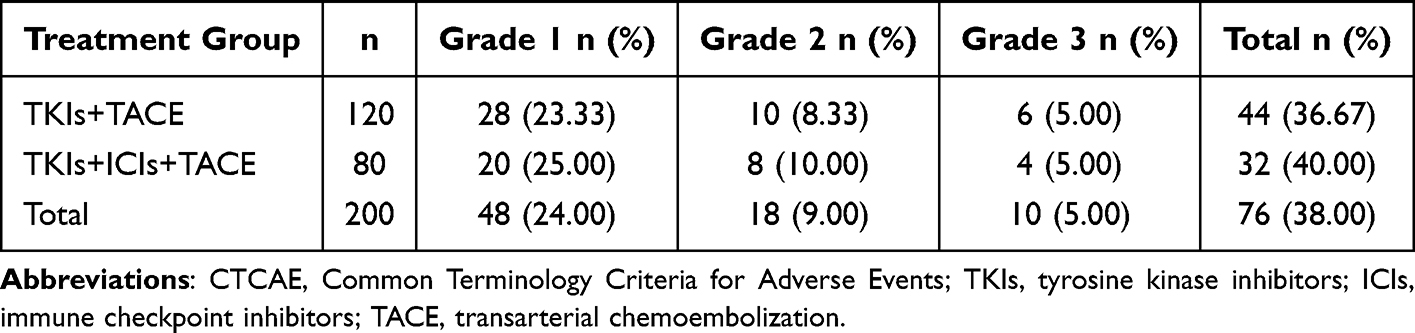 |
Table 2 Incidence of Early Liver Injury by Treatment Regimen and CTCAE Grade |
Risk Factor Analysis
Univariate analysis identified several clinical variables significantly associated with hepatotoxicity occurrence (P<0.05), including advanced age (>65 years), elevated baseline TBil (>17 μmol/L), presence of cirrhosis, poor mALBI grade (Grade 2b/3), decreased PTA (<75%), and history of multiple TACE sessions (>2). Conversely, sex, tumor burden parameters (tumor size and number), and baseline ALT, AST, and albumin levels showed no significant association with hepatotoxicity risk.
A significant dose-response relationship was observed between hepatotoxicity severity and baseline biochemical markers. Progressive elevation of baseline TBil and deterioration of PTA were significantly correlated with increasing hepatotoxicity grade (both P<0.01). Additionally, higher mALBI grades were significantly associated with a greater proportion of moderate-to-severe hepatotoxicity (P=0.005). The detailed baseline characteristics stratified by hepatotoxicity severity are presented in Table 3.
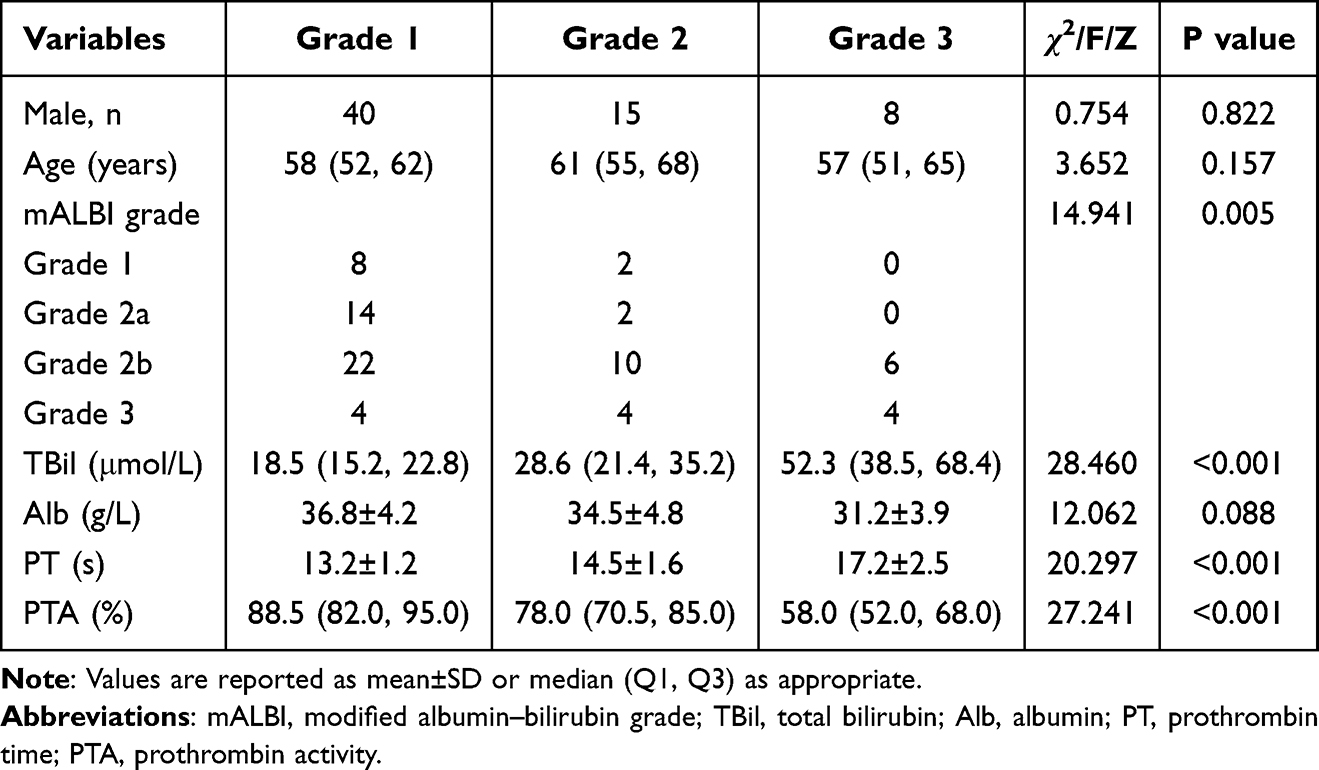 |
Table 3 Baseline Factors Associated with Liver Injury Severity Among Patients with Liver Injury (n=76) |
Construction and Validation of the TCAP Prediction Model
Multivariate logistic regression analysis identified four independent predictors significantly associated with hepatotoxicity: pre-treatment cirrhosis status (OR=1.684, 95% CI: 1.006~2.817, P=0.047), ALBI Grade 2/3 (OR=6.436, 95% CI: 3.730~11.103, P<0.001), total bilirubin level (OR=1.040, 95%CI:1.011~1.069, P=0.007), and prothrombin activity (OR=0.968, 95% CI: 0.952~0.984, P<0.001). The detailed regression results are summarized in Table 4.
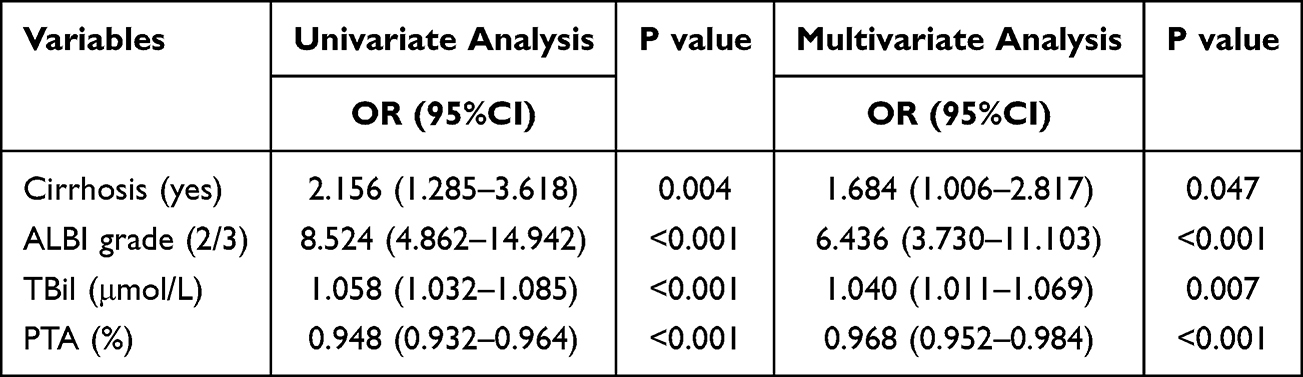 |
Table 4 Logistic Regression Analyses for Predictors of Early Liver Injury (CTCAE ≥1) |
Based on these four independent risk factors, a nomogram prediction model (designated TCAP: Total bilirubin, Cirrhosis, ALBI grade, Prothrombin activity) was constructed (Figure 1).
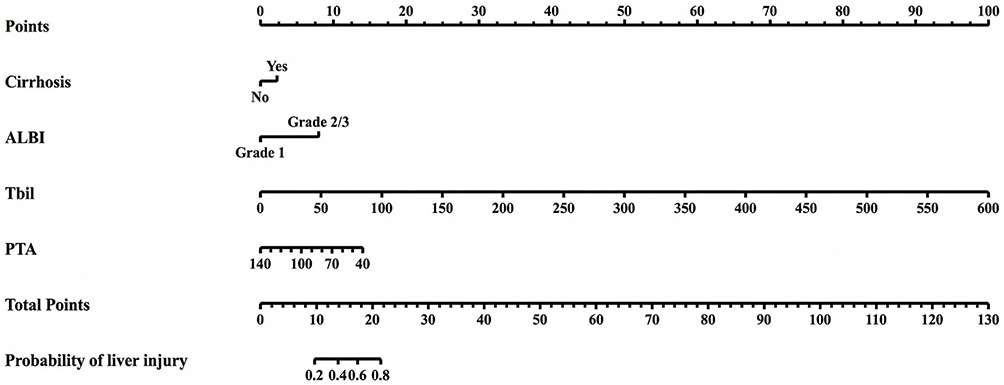 |
Figure 1 Nomogram for predicting hepatotoxicity risk in hepatocellular carcinoma patients receiving TACE combined with systemic therapy. The TCAP model incorporates four independent predictors: Total bilirubin (TBil), Cirrhosis status, ALBI grade, and Prothrombin activity (PTA). To calculate the predicted probability, identify the value for each predictor on its respective axis, draw a vertical line to the “Points” axis to determine the points contribution, sum all points, and locate this total on the “Total Points” axis to read the corresponding “Risk of Hepatotoxicity” probability. |
The prediction equation is expressed as:

Model Performance Evaluation
The TCAP nomogram demonstrated excellent discriminatory performance, with an AUC of 0.855 (95% CI: 0.812–0.898) (Figure 2A). At the optimal cut-off value of 0.419, determined by the maximum Youden index, the model achieved a sensitivity of 82.00% and a specificity of 79.10%. Calibration analysis demonstrated excellent agreement between predicted and observed probabilities of hepatotoxicity (Figure 2B). The Hosmer-Lemeshow goodness-of-fit test indicated adequate calibration (P=0.1145). Internal validation using 1000 bootstrap resamples confirmed the model’s stability, with a bias-corrected AUC of 0.843 and a mean absolute error (MAE) of only 0.008, indicating minimal optimism and robust internal validity.
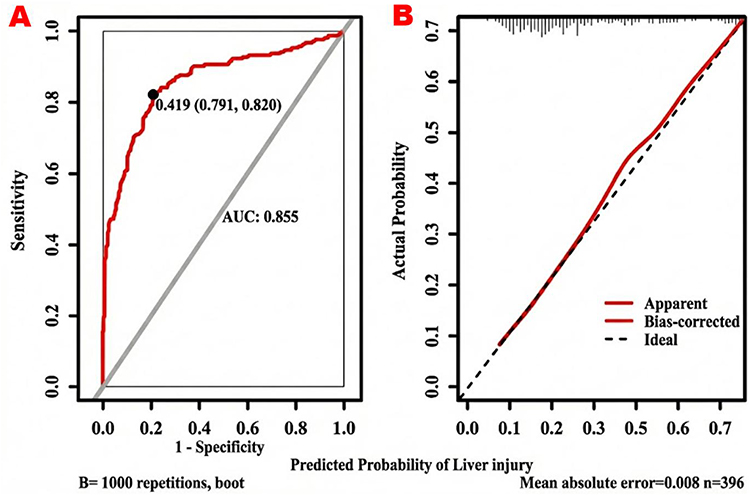 |
Figure 2 Performance evaluation of the TCAP hepatotoxicity risk prediction model. (A) Receiver operating characteristic (ROC) curve demonstrating the discriminatory performance of the model. The area under the curve (AUC) was 0.855 (95% CI: 0.812–0.898). At the optimal cut-off value of 0.419, the model achieved a sensitivity of 82.00% and a specificity of 79.10%. (B) Calibration curve demonstrating the agreement between predicted and observed probabilities of hepatotoxicity. The apparent and bias-corrected curves closely approximate the ideal diagonal line, indicating excellent calibration. Internal validation using 1000 bootstrap resamples confirmed model stability with a mean absolute error (MAE) of 0.008. |
Discussion
This study provides a comprehensive characterization of hepatotoxicity patterns in HCC patients undergoing TACE combined with contemporary systemic therapies. Our findings demonstrate that while hepatotoxicity remains a common treatment-related adverse event (overall incidence: 38.00%), the clinical presentation is predominantly mild-to-moderate, with severe (Grade 3) hepatotoxicity occurring in only 13.16% of patients and no Grade 4 events observed. Importantly, the addition of ICIs to the targeted therapy-TACE regimen did not significantly increase the hepatotoxicity risk, supporting the overall safety of triplet combination approaches when properly managed.
The observed hepatotoxicity incidence in our cohort aligns with previously published data. Li et al reported a 47.62% hepatotoxicity rate in patients receiving similar combination regimens,21 while other studies have documented rates ranging from 15% to 50% depending on the specific agents used and patient population characteristics.22 The absence of a significant difference in hepatotoxicity between dual and triplet therapy groups corroborates findings from systematic reviews by Sangro et al23 regarding the hepatic safety profile of ICIs in patients with underlying liver disease. These observations suggest that with careful patient selection and vigilant monitoring, the safety profile of combination therapy remains clinically manageable.
Our multivariate analysis identified ALBI Grade 2/3 as the most potent independent predictor of hepatotoxicity (OR=6.436). The ALBI grade, developed by Johnson et al16 represents a significant advancement over the traditional Child-Pugh classification by eliminating subjective parameters (ascites, encephalopathy) and relying solely on objective biochemical markers (albumin, bilirubin). This objectivity enhances reproducibility and facilitates standardized assessment across different clinical settings. Multiple studies have validated the superior prognostic performance of the ALBI grade in various HCC treatment contexts, including surgical resection, ablation, TACE, and systemic therapy.24,25 The mALBI grading system, which further subdivides ALBI Grade 2 into 2a and 2b categories, has demonstrated enhanced sensitivity in detecting subtle functional deteriorations following locoregional interventions.26,27 Our data strongly support prioritizing the ALBI grade-either as a replacement for or supplement to the Child-Pugh score-when formulating treatment strategies for HCC patients.
The identification of underlying liver cirrhosis as an independent risk factor (OR=1.684) underscores the mechanistic complexity of hepatotoxicity in this patient population. Cirrhosis-associated pathophysiological changes-including hepatic sinusoidal capillarization, portal hypertension, and microcirculatory dysfunction-may amplify the ischemia-reperfusion injury induced by TACE beyond what is radiographically apparent.28 Furthermore, the diminished regenerative capacity of cirrhotic hepatocytes compromises the liver’s ability to compensate for drug-induced cytotoxicity and procedural injury, potentially accelerating the progression from transient biochemical abnormalities to clinically significant hepatic decompensation.29
Total bilirubin and prothrombin activity serve as complementary biomarkers reflecting distinct aspects of hepatic parenchymal function-metabolic clearance capacity and synthetic reserve, respectively. The inclusion of both parameters in our TCAP model provides a multidimensional assessment of hepatic functional integrity. Mechanistically, elevated TBil indicates compromised bilirubin conjugation and excretion, signaling the transition from compensated to decompensated liver function, while declining PTA reflects exhaustion of coagulation factor synthesis capacity.30,31 The integration of these parameters with cirrhosis status and ALBI grade creates a comprehensive risk assessment framework.
In addition, because TBil and PTA are laboratory-based variables, the potential influence of assay variability should be considered when interpreting the model’s broader applicability. In the present study, all biochemical and coagulation measurements were performed in a single institutional laboratory using standardized automated analyzers under routine internal quality-control procedures, which likely minimized inter-assay variability and contributed to the internal consistency of the TCAP model. Nevertheless, differences in assay platforms, calibration standards, reagent systems, and pre-analytical sample handling across institutions may introduce measurement heterogeneity, potentially affecting the reproducibility of absolute threshold-based risk stratification. Therefore, standardized laboratory testing and cross-platform validation will be important for confirming the generalizability and clinical utility of this model in external cohorts.
The TCAP nomogram demonstrated robust predictive performance with an AUC of 0.855, indicating excellent discrimination between patients who will and will not develop hepatotoxicity. The calibration analysis confirmed good agreement between predicted probabilities and observed outcomes, supporting the model’s reliability for clinical application. A distinctive strength of this model lies in its exclusive reliance on readily available clinical parameters; by obviating the need for sophisticated or costly diagnostic tests, it ensures high health-economic viability and facilitates seamless implementation across diverse healthcare settings.
The clinical utility of the TCAP model extends beyond passive risk prediction to active treatment optimization. For patients identified as high-risk (predicted probability >0.419), clinicians may consider implementing a more conservative intervention strategy, including: (1) limiting the extent of single-session embolization; (2) extending the interval between TACE procedures; (3) intensifying hepatoprotective and antiviral therapies; (4) increasing the frequency of liver function monitoring; and (5) establishing lower thresholds for treatment modification or discontinuation. Conversely, patients classified as low-risk may proceed with standard combination therapy protocols with routine monitoring. This risk-stratified approach aligns with the principles of prioritizing hepatic reserve and dynamically monitoring liver function advocated in current treatment guidelines.32
Several limitations merit consideration. First, the retrospective design and single-center cohort of 200 patients may introduce selection bias and limit generalizability, although bootstrap internal validation mitigated overfitting risks. Second, the heterogeneity of systemic agents employed-encompassing various tyrosine kinase inhibitors (eg., sorafenib, lenvatinib) and immune checkpoint inhibitors (eg., atezolizumab, durvalumab)-could influence hepatotoxicity profiles, as different combinations may exhibit varying pharmacokinetic interactions and toxicity spectra. For instance, anti-angiogenic TKIs may exacerbate ischemic effects post-TACE, while ICIs could potentiate immune-mediated liver injury, though our analysis did not detect significant differences between treatment groups (P=0.637). Future studies should stratify by specific regimens to refine risk predictions. Third, while the TCAP nomogram demonstrated robust internal performance (AUC=0.855), reliance on bootstrap resampling underscores the need for external validation in multicenter, prospective cohorts to confirm its accuracy and calibration across diverse populations before broad clinical adoption. Additionally, unmeasured confounders such as genetic polymorphisms in drug metabolism (eg., UGT1A1 variants affecting bilirubin handling) were not assessed and warrant exploration in larger datasets.
Conclusion
In conclusion, the combination of TACE with targeted therapy alone or with targeted-immune combination therapy demonstrates a manageable hepatic safety profile in patients with hepatocellular carcinoma, with the majority of hepatotoxic events being mild-to-moderate and self-limiting. Underlying liver cirrhosis, poor ALBI grade (Grade 2/3), elevated total bilirubin, and decreased prothrombin activity were identified as independent risk factors for hepatotoxicity. Based on these factors, the TCAP nomogram provides a quantitative approach for individualized hepatotoxicity risk assessment in patients undergoing TACE-based combination therapy. However, the predictive performance of the model was evaluated using internal bootstrap validation within a single-center retrospective cohort. Therefore, prospective studies and external validation in independent populations are required to further confirm the generalizability and clinical applicability of the model.
Abbreviations
AFP, Alpha-fetoprotein; Alb, Albumin; ALBI, Albumin-bilirubin; ALT, Alanine aminotransferase; AST, Aspartate aminotransferase; AUC, Area under the curve; BCLC, Barcelona Clinic Liver Cancer; CI, Confidence intervals; CNLC, China Liver Cancer; CTCAE, Common Terminology Criteria for Adverse Events; DCA, Decision curve analysis; ECOG, Eastern Cooperative Oncology Group; HBV, Hepatitis B virus; HCC, Hepatocellular carcinoma; HR, Hazard ratio; ICIs, Immune checkpoint inhibitors; IQR, Interquartile range; MAE, Mean absolute error; mALBI, Modified ALBI; OR, Odds ratio; OS, Overall survival; PT, Prothrombin time; PTA, Prothrombin activity; ROC, Receiver operating characteristic; SD, Standard deviation; TACE, Transarterial chemoembolization; TBil, Total bilirubin; TCAP, Total bilirubin, Cirrhosis, ALBI grade, Prothrombin activity; TKIs, Tyrosine kinase inhibitors; ULN, Upper limits of normal.
Data Sharing Statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
Ethics Approval and Informed Consent
The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of the Shandong Cancer Hospital and Institute, affiliated with Shandong First Medical University (Jinan, Shandong Province, China. Given that this was a retrospective study of patient clinical data, a waiver of written informed consent was approved. All patient data were strictly confidential and used solely for the purpose of this study. During the data usage process, patient personal information was anonymized, in compliance with relevant privacy protection regulations.
Acknowledgments
We aregrateful to all patients and their families and all members of thecollaborative group.
Funding
This research was supported by the Shanghai YRD Foundation for Innovation in Health Industry (2025-YRDFHI-012) and Project YXH2025YS059 supported by ShanDong Provincial Medical Association Natural Science.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–12. doi:10.3322/caac.21660
2. Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China, 2022. J Natl Cancer Cent. 2024;4(1):47–53. doi:10.1016/j.jncc.2024.01.006
3. Ganesan P, Kulik LM. Hepatocellular carcinoma: new developments. Clin Liver Dis. 2023;27(1):85–102. doi:10.1016/j.cld.2022.08.004
4. Lencioni R, de Baere T, Soulen MC, Rilling WS, Geschwind JH. Lipiodol transarterial chemoembolization for hepatocellular carcinoma: a systematic review of efficacy and safety data. Hepatology. 2016;64(1):106–116. doi:10.1002/hep.28453
5. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
6. Abou-Alfa GK, Lau G, Kudo M, et al. Tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. NEJM Evid. 2022;1(8):EVIDoa2100070. doi:10.1056/EVIDoa2100070
7. Berber I, Aydın Köker S, Köker C, et al. Immune checkpoint inhibitors in the treatment of hepatocellular carcinoma. Front Immunol. 2024;15:1379622. doi:10.3389/fimmu.2024.1379622
8. Celsa C, Cabibbo G, Fulgenzi CAM, et al. Characteristics and outcomes of immunotherapy-related liver injury in patients with hepatocellular carcinoma versus other advanced solid tumours. J Hepatol. 2024;80(3):431–442. doi:10.1016/j.jhep.2023.10.040
9. Kudo M, Ueshima K, Ikeda M, et al. Randomised, multicentre prospective trial of transarterial chemoembolisation (TACE) plus sorafenib as compared with TACE alone in patients with hepatocellular carcinoma: tactics trial. Gut. 2020;69(8):1492–1501. doi:10.1136/gutjnl-2019-318934
10. Zhu AX, Kang Y, Yen C, et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (reach-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(2):282–296. doi:10.1016/S1470-2045(18)30937-9
11. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. doi:10.1016/S0140-6736(18)30207-1
12. Cabibbo G, Rimassa L, Lamarca A, et al. The present and the future of immunotherapy in hepatocellular carcinoma and biliary tract cancers. Cancer Treat Rev. 2025. doi:10.1016/j.ctrv.2025.102896
13. Cabibbo G, Celsa C, Alimenti E, Iavarone M. Evaluating the risk-benefit ratio of immunotherapy according to liver-functional reserve in advanced HCC: the dark side of the moon. Hepatology. 2023;77(4):1074–1077. doi:10.1097/HEP.0000000000000205
14. Bruix J, Chan SL, Galle PR, Rimassa L, Sangro B. Systemic treatment of hepatocellular carcinoma: an EASL position paper. J Hepatol. 2021;75(4):960–974. doi:10.1016/j.jhep.2021.07.004
15. Duran SR, Jaquiss RDB Hepatocellular Carcinoma. N Engl J Med. 2019;381(1):e2. doi:10.1056/NEJMc1906565
16. Johnson PJ, Berhane S, Kagebayashi C, et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach-the ALBI grade. J Clin Oncol. 2015;33(6):550–558. doi:10.1200/JCO.2014.57.9151
17. Hiraoka A, Kumada T, Michitaka K, et al. Usefulness of albumin-bilirubin grade for evaluation of prognosis of 2584 japanese patients with hepatocellular carcinoma. J Gastroenterol Hepatol. 2016;31(5):1031–1036. doi:10.1111/jgh.13250
18. National HCOT. National guidelines for diagnosis and treatment of cervical cancer 2022 in China (English version). Chin J Cancer Res. 2022;34(3):256–269. doi:10.21147/j.issn.1000-9604.2022.03.06
19. Hepatology CSO, Association CM. [Chinese clinical practice guidelines for transarterial chemoembolization of hepatocellular carcinoma (2023 edition)]. Zhonghua Yi Xue Za Zhi. 2023;103(34):2674–2694. doi:10.3760/cma.j.cn112137-20230630-01114
20. Freites-Martinez A, Santana N, Arias-Santiago S, et al. Using the Common Terminology Criteria for Adverse Events (CTCAE - Version 5.0) to Evaluate the Severity of Adverse Events of Anticancer Therapies. CTCAE versión 5.0. Evaluación de la gravedad de los eventos adversos dermatológicos de las terapias antineoplásicas. Actas Dermosifiliogr. 2021;112(1):90–92. doi:10.1016/j.ad.2019.05.009
21. Li M, Zhang K, He J, et al. Hepatic arterial infusion chemotherapy in hepatocellular carcinoma: a bibliometric and knowledge-map analysis. Front Oncol. 2022;12:1071860. doi:10.3389/fonc.2022.1071860
22. Cheng A, Hsu C, Chan SL, Choo S, Kudo M. Challenges of combination therapy with immune checkpoint inhibitors for hepatocellular carcinoma. J Hepatol. 2020;72(2):307–319. doi:10.1016/j.jhep.2019.09.025
23. Sangro B, Chan SL, Meyer T, Reig M, El-Khoueiry A, Galle PR. Diagnosis and management of toxicities of immune checkpoint inhibitors in hepatocellular carcinoma. J Hepatol. 2020;72(2):320–341. doi:10.1016/j.jhep.2019.10.021
24. Chan AWH, Chong CCN, Mo FKF, et al. Applicability of albumin-bilirubin-based Japan integrated staging score in hepatitis b-associated hepatocellular carcinoma. J Gastroenterol Hepatol. 2016;31(10):1766–1772. doi:10.1111/jgh.13339
25. Hiraoka A, Michitaka K, Kumada T, et al. Validation and potential of albumin-bilirubin grade and prognostication in a nationwide survey of 46,681 hepatocellular carcinoma patients in Japan: the need for a more detailed evaluation of hepatic function. Liver Cancer. 2017;6(4):325–336. doi:10.1159/000479984
26. Kudo M. Newly developed modified ALBI grade shows better prognostic and predictive value for hepatocellular carcinoma. Liver Cancer. 2022;11(1):1–8. doi:10.1159/000521374
27. Hiraoka A, Kumada T, Kudo M, et al. Hepatic function during repeated TACE procedures and prognosis after introducing sorafenib in patients with unresectable hepatocellular carcinoma: multicenter analysis. Dig Dis. 2017;35(6):602–610. doi:10.1159/000480256
28. Vollmar B, Menger MD. The hepatic microcirculation: mechanistic contributions and therapeutic targets in liver injury and repair. Physiol Rev. 2009;89(4):1269–1339. doi:10.1152/physrev.00027.2008
29. So J, Kim A, Lee S, Shin D. Liver progenitor cell-driven liver regeneration. Exp Mol Med. 2020;52(8):1230–1238. doi:10.1038/s12276-020-0483-0
30. Sticova E, Jirsa M. New insights in bilirubin metabolism and their clinical implications. World J Gastroenterol. 2013;19(38):6398–6407. doi:10.3748/wjg.v19.i38.6398
31. Barnhart MI. Prothrombin synthesis: an example of hepatic function. J Histochem Cytochem. 1965;13(8):740–751. doi:10.1177/13.8.740
32. Heimbach JK, Kulik LM, Finn RS, et al. Aasld guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380. doi:10.1002/hep.29086
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.