")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Development and Validation of a Sexual Health Literacy Measurement Tool for Pregnancy Prevention Among Adolescents (SHL-PPA)
Authors Thongnopakun S, Manwong M, Visanuyothin S , Wattanaburanon A, Suwannarat W , Magteppong W
Received 9 May 2023
Accepted for publication 15 August 2023
Published 23 August 2023 Volume 2023:16 Pages 2417—2430
DOI https://doi.org/10.2147/JMDH.S420640
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Saowanee Thongnopakun,1,* Mereerat Manwong,2,* Sawitree Visanuyothin,3 Aimutcha Wattanaburanon,1 Wasimon Suwannarat,4 Worarat Magteppong5
1Faculty of Public Health, Burapha University, Chon Buri, Thailand; 2College of Medicine and Public Health, Ubon Ratchathani University, Ubon Ratchathani, Thailand; 3National Health Security Office (NHSO), Nakhon Ratchasima, Thailand; 4Chanthaburi Provincial Health Office, Chanthaburi, Thailand; 5Faculty of Nursing, Rajamangala University of Technology, Pathumthani, Thailand
*These authors contributed equally to this work
Correspondence: Mereerat Manwong, College of Medicine and Public Health, Ubon Ratchathani University, Ubon Ratchathani, 34190, Thailand, Tel +66 45-353-900, Email [email protected]
Purpose: Several measurement tools have been developed for health literacy. However, little emphasis has been placed on the development of sexual health literacy (SHL) in adolescents. This paper describes the development and validation of an SHL measurement tool for pregnancy prevention among adolescents (SHL-PPA).
Methodology: This study explores research and development (R&D) and presents three stages of R&D, including a literature review, the Delphi approach, and a valid and reliable questionnaire. Three groups were used for the population and sampling: 18 experts, five competent people, and 654 adolescents. An online self-assessment tool was used. The data analysis methods used were median, interquartile range, content validity index, Cronbach’s alpha coefficient, and exploratory factor analysis.
Results: The results show that the definition of SHL for adolescents was “cognitive, social, and cultural skills that determine the motivation and ability of an adolescent to access and sufficiently understand sexual health information and services, which results in them being capable of sexual health assessment and making decisions to prevent pregnancy”. The final devised SHL-PPA included 33 items and the three following components: 1) accessibility to sexual health information and services, 2) an understanding of sexual health information and services and appraisal of sexual health to prevent pregnancy, and 3) applying the obtained sexual health information and skills to prevent pregnancy.
Conclusion: This study proves that the SHL-PPA is appropriate for Generation Z teenagers, particularly for online self-assessment of SHL. An online self-evaluation using the SHL-PPA demonstrated that related organizations should develop online activities or programs to improve teenage girls’ pregnancy-prevention behavior.
Keywords: sexual health literacy, instrument, pregnancy, school health, student, youth
Introduction
In 2022, according to the United Nations International Children’s Emergency Fund, the number of adolescents globally was 1.3 billion, which was 16% of the global population.1 Adolescents face sexual risk behaviors, including unwanted pregnancy.2,3 Adolescent pregnancy is an important problem in low- and middle-income countries, with half of unintended pregnancies resulting in pregnancy-related morbidity and mortality, such as preterm birth, low birth weight, and severe neonatal condition.4–6 Today’s adolescents are part of Generation Z (Gen Z), which has the following characteristics:
High consumers of technology and cravers of the digital world, individualistic, underdeveloped social and relationship skills, increased risk for mental health concerns, lack of attention span, desiring convenience and immediacy, pragmatic, cautious and concerned with emotional, physical and financial safety, sedentary activism, open-minded, diverse and comfortable with differences.7
In addition, Gen Z has higher levels of sexual risk behaviors than millennials, the preceding generation.8 Some studies have pointed out that adolescents with higher sexual health literacy (SHL) are more likely to have preventive sexual behavior than those with lower SHL.9,10 Moreover, SHL is imperative for decreasing adolescent pregnancy.11–13 However, various definitions of SHL and different numbers of SHL components have been presented.13–27 Additionally, there are few sexual health literacy measurement tools for preventing adolescent pregnancy.18,28,29 Therefore, this study aimed to define the definition and components of SHL for preventing pregnancy for adolescents. Additionally, a qualified SHL measurement tool for pregnancy prevention among adolescents (SHL-PPA) was developed. This tool can be used to assess adolescents’ levels of SHL for pregnancy prevention so that individual groups and related organizations can improve existing SHL-PPAs.
Materials and Methods
Study Design
The development and validation of an SHL-PPA was a research and development (R&D) study conducted from August to November 2022.
Development of a Tool for Pregnancy Prevention Among Adolescents
The three steps involved in developing the SHL-PPA are as follows:
Step 1: After a literature review,10,13–27,30,31 a definition and the components of SHL among adolescents were developed and sent to six policy experts, six academic experts, and six practice experts for their opinion and suggestions regarding the appropriate definition and components of SHL for pregnancy prevention among adolescents.
Step 2: The Delphi technique was applied in this step. Based on 18 experts’ opinions and suggestions, the researchers produced an outline draft of the SHL-PPA questionnaire. The questionnaire was sent to 18 experts to review and provide comments on improving the questionnaire, which took place in three rounds. Then, the questionnaire was tested for its Content Validity Index (CVI) score based on the 18 experts. The five competent people in measurement and evaluation who work as biostatistician, public health worker, and adolescent sexual health worker evaluated the item objective congruence (IOC), which total was greater than 0.5. The reliability based on 60 adolescents with qualifications similar to those of the 654 samples in this study.
Step 3: The questionnaire, which was found to be valid and reliable, comprised 33 questions and was tested among 654 adolescents using exploratory factor analysis (EFA).
Population Sample and Sampling Technique
The samples were divided into two groups.
Group 1: Based on the Delphi technique, the number of experts was determined by the researchers to be 18. A purposive sampling technique was used to recruit experts. The inclusion criteria for the 18 experts32,33 were health-related experts with at least five years’ experience in the designated field of interest. The selective inclusion criteria for each group were 1) six policy-making experts from the Department of Health, Regional Health Promotion Center Office, Provincial Health Office, or Regional Health Security Office; 2) six academic experts from university staff working with adolescents or in health literacy teaching and research; and 3) six members from among high school teachers working with adolescents and the sexual health field and frontline health workers in government organizations, non-governmental organizations, and local government organizations.
Group 2: The appropriate sample size for EFA should be 10 times the number of question items or more than 500 samples.34 The number of respondents in this study was 654, which included both male and female adolescents who were students in junior school, high school, or university or who were studying for their vocational or high vocational certificate in the 2022 school year. In this study, three steps of multi-stage sampling were applied to recruit the respondents who were 13–19 years old as following: 1) purposive sampling for a province with high incidence of sexual transmitted diseases and adolescence pregnancy, 2) simple random sampling by computer software for educational institutes at provincial level, 3) simple random sampling by computer software for classrooms at educational institutes level. Respondents were required to be capable of interacting with an online questionnaire. Pregnant female adolescents were excluded from this study. The number of respondents from junior school was 123, from high school was 125, studying for vocational certificate was 114, studying for high vocational certificate was 107, and from university was 185.
Data Collection and Data Analysis
Step 1: The online questionnaire regarding expert opinions on the definition and components of SHL was produced and distributed to 18 experts in the first round. The questionnaire included three parts: 1) expert demographic, 2) expert opinion on the definition of SHL for pregnancy prevention among adolescents, and 3) expert opinion on the components of SHL for pregnancy prevention among adolescents. They had to agree or disagree with the given definition and components of SHL for pregnancy prevention among adolescents provided by the researchers. If experts did not agree with the researchers, they needed to give their opinion on what the definition and components of SHL for pregnancy prevention among adolescents should be. Descriptive statistics were used for analyzing the experts’ comments.
Step 2: The researchers used the results from the first round to construct a questionnaire framework and drafted 36 close-ended question items. CVI analysis was applied in this step. In the second round, the online questionnaire was sent to the 18 experts to provide scores on a five-point Likert scale for their opinion on the level of relevancy that each question had to the item objective. The scale was as follows: 1 = highly irrelevant, 2 = irrelevant, 3 = somewhat relevant, 4 = quite relevant, and 5 = highly relevant. The proportion of expert scores or 4–5 was analyzed for each question item. If the proportion was less than 0.83, the item needed to be improved. However, the total proportion of the questionnaire based on CVI should not be less than 0.8. All experts’ opinions were analyzed for median and interquartile range (IQR) for each item; a median score of at least 4.5 meant that experts gave the highest relevancy level for this item. A median score of 3.50–4.49 meant that this question had a high relevancy level. To determine the accordance of the experts’ opinions with both the high and highest relevancy levels, the IQR should not exceed 1.5. An improved questionnaire was sent in the third round to the 18 experts to determine the CVI, as was done in the second round. If there were any unclear comments, the researchers directly contacted that expert to comprehend and correct the questionnaire. The final online questionnaire had 33 items and was conducted and randomly tested on 60 adolescents. Cronbach’s alpha was calculated to determine the reliability of the questionnaire.
Step 3: Based on factor analysis, the Kaiser-Meyer-Olkin measure (KMO) was used to determine whether each question item met the assumption (the result should be at least 0.6). The maximum likelihood was used to extract the factor analysis through the rotation of the varimax. To decide the number of components were determined by eigenvalue which was greater than 1. IBM SPSS Statistics version 23×86 (through the Burapha University license) was used for the data analysis.
Informed Consent Statement
Ethical approval for this study under the Helsinki Declaration was approved by Ubon Ratchathani University (certification code: UBU-REC-106/2565) and Burapha University (certification code: HU 098/2565). The participants were informed of the details of this research, and their privacy was protected via confidentiality. Then participants signed informed consent.
Results
The findings were divided into three steps based on the research objectives.
Step 1: Definition and Components of SHL
The 18 experts who gave their opinions on the definition and components of SHL for pregnancy prevention among adolescents had an average age of 46.83 years (SD = 11.03) and had an average 10.50 years (SD = 8.50) of SHL-related experience. All agreed with the proposed definition and components of SHL for pregnancy prevention among adolescents. However, 13 experts provided recommendations for defining the definition. In terms of components, they provided suggestions to improve 1) accessibility to sexual health information and services (8 experts), 2) understanding of sexual health and services (13 experts), 3) appraising sexual health to prevent pregnancy (13 experts), and 4) applying the obtained sexual health information and skills to prevent pregnancy (11 experts).
Eventually, the definition of SHL for pregnancy prevention among adolescents was drafted as
Cognitive, social, and cultural skills that determine the motivation and ability of adolescents to access and sufficiently understand sexual health information and services, which results in them being capable of sexual health assessment and making decisions to prevent pregnancy.
Four components were determined: 1) accessibility to sexual health information and services, 2) understanding sexual health information and services, 3) appraising sexual health to prevent pregnancy, and 4) applying the obtained sexual health information and skills to prevent pregnancy. Overall, experts suggested revising the Thai language to be more easily comprehended by adolescents. Additionally, three of the experts recommended that interpretation and spreading the word should be included in Component 2.
Step 2: Results of the Content Validity Index (CVI) Analysis
The total number of items drafted for the SHL-PPA questionnaire was 36, comprising 12 items on accessibility to sexual health information and services, six items on understanding sexual health information and services, six items on appraising sexual health to prevent pregnancy, and 12 items on applying the obtained sexual health information and skills to prevent pregnancy. The results of a CVI analysis after three rounds of Delphi technique approval were at least 0.83 for all questions with the highest relevancy level. The CVI for scale (S-CVI) was 0.97, but two questions were deemed unclear, so both were deleted (Q3 and Q16). Furthermore, Q8 was similar to Q9; therefore, Q9 was also deleted.
The final draft of the SHL-PPA had 33 items: 10 items on accessibility to sexual health information and services, five items on understanding sexual health information and services, six items on appraising sexual health to prevent pregnancy, and 12 items on applying the obtained sexual health information and skills to prevent pregnancy (Table 1). The range of IOC from five competent people approval was between 0.6–1.0. Then, the reliability of this questionnaire was tested in 60 adolescents, resulting in a Cronbach’s alpha of 0.97.
 |
Table 1 Experts’ Evaluation Based on CVI for Item Development of a Sexual Health Literacy Measurement Tool for Pregnancy Prevention Among Adolescents in Rounds 2 and 3 |
Step 3: Results of the Exploratory Factor Analysis (EFA)
The total sample size for the EFA was 654. All assumptions of the EFA were met. The correlation of items was between 0.30 and 0.84 (Table 2). The KMO revealed that the statistical value was 0.98, which was more than 0.6. Based on Bartlett’s test, p < 0.001. Using maximum likelihood for the extraction of factor analysis with varimax rotation, the 33 SHL-PPA items were determined to have sufficient relationships for according to EFA by using maximum likelihood for extraction of factor analysis with varimax rotation. After that, the eigenvalue and scree plot were used to determine the number of components. The analysis found that the eigenvalue of components from one to three were 19.938, 2.334, and 1.292, respectively, which all three values were greater than one.35 Additionally, the scree plot presented eigenvalue which started at almost twenty for component one, then it dramatically dropped to slightly greater than one for component three. However, there were a few changes of eigenvalue for factor four to thirty-three. According to the result of Table 3 and Figure 1, the appropriate number of components for SHL-PPA was three. Component 1 had 12 items on applying the obtained sexual health information and skills to prevent pregnancy (Q22–Q33), with a 0.56–0.81 correlation; Component 2 comprised 10 items on accessibility to sexual health information and services (Q1–Q10), with a 0.50–0.78 correlation; and Component 3 comprised five items on understanding sexual health information and services (Q11–Q15) and six items on appraising sexual health to prevent pregnancy (Q16–Q21), with a 0.53–0.75 correlation (Table 4). The variance of the three components for use in predicting SHL in adolescents was 28.38%, 20.94%, and 19.16%, respectively. All three component variances can predict SHL in adolescents at a rate of 68.48%.
 |
Table 2 Rotated Factors Matrix |
 |
Table 3 The Statistics of Each Component |
 |
Table 4 The Relationship of Exploratory Factor Analysis |
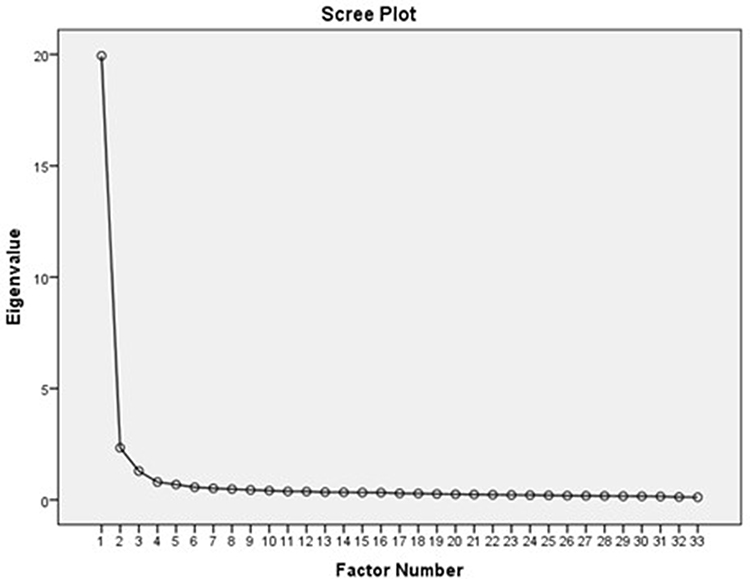 |
Figure 1 Scree plot of eigenvalue. |
Discussion
This was an R&D study that had three main steps.
Step 1: Definition and Components of SHL
The 18 multidisciplinary experts were composed of three groups comprising policy makers, academic staff, and healthcare workers. They had longtime experience in working with adolescents and health literacy. Therefore, the experts provided reliable opinions for the researchers to determine the definition and components of SHL in order to create an SHL-PPA questionnaire. In addition, there was a sufficient number of experts, which decreased error by 0.0232,33 for the Delphi technique. There were four components of SHL-PPA. In contrast, Thai studies have 5–7 components.16,18,19,22,23,27 However, non-Thai studies have two components,20,24,25 three components,14,30 four components,10,15,17,21,26,31 or five components.13 Whether the component was four or not, the definitions in other studies were nearly similar to the definition in this study.10,15–17,21,22,27 However, the abovementioned studies were about SHL and reproductive health literacy, while this study specifically focused on SHL for pregnancy prevention among adolescents. EFA was used to define the number needed for components of SHL for pregnancy prevention among adolescents.
Step 2: Results of the Content Validity Index (CVI) Analysis
The results revealed that, using the Delphi technique, the Item content Validity Index (I-CVI) had three values (4 items = 0.89, 7 items = 0.94, and 22 items = 1.00), with all I-CVI values for each item meeting the acceptable standard of 0.83.36 Furthermore, the S-CVI of this study was 0.97, which shows excellent validity. Generally, the acceptable value of opinion agreement should not be less than 0.80.36 Although Q3, Q16, Q8, and Q9 had a CVI value of 0.94, three experts suggested deleting Q3 and Q16 because they were unclear. Since Q8 had a meaning similar to Q9, two experts recommended deleting one of them. According to multidisciplinary experts and the highest relevancy levels for both I-CVI and S-CVI, the SHL-PPA was found to be excellently valid and suitable in terms of content for adolescents to do self-assessment.
Step 3: Results of the Exploratory Factor Analysis (EFA)
The EFA resulted in three components relevant to the definitions of this study. In Component 2, understanding and appraising were merged. Three of the 18 experts recommended three components at the beginning as well. The 654 samples were from Gen Z, who have grown up with access to the internet and portable digital technology.37 Moreover, they have a smaller attention period and a desire for convenience and instantaneity.7 Thus, the 33 questions with three components from the EFA analysis may be appropriate for Gen Z. Although the SHL-PPA is not the gold standard tool for measuring SHL among adolescents, adolescents themselves, schools, universities, and organizations may use this tool for primary assessment and follow-up of the sexual health prevention pregnancy behavior of adolescents.7
Conclusion
This study defined the definition of SHL, and three components of SHL to prevent pregnancy for adolescents were found (accessibility, understanding and apprising, applying). To develop SHL-PPA, three steps were taken: 1) determining the definition and components of SHL, 2) deriving the results of the CVI analysis, and 3) deriving the results of the EFA. The SHA-PPA in this study comprised 33 items, and this tool was found to be appropriate for adolescents, especially Gen Z, to perform an online self-assessment of SHL for pregnancy prevention. Moreover, educational institutions may provide this tool to evaluate SHL for pregnancy prevention, and to design the appropriate intervention for decrease of pregnancy rate among adolescents.
Strengths and Limitations
This study provided quality expert opinion in terms of their number and multidisciplinary professionalism; consequently, the SHL-PPA was valid, reliable, relevant, and suitable for adolescents. This tool can be useful in determining SHL to prevent pregnancy for Gen Z. In addition, the tool can be used in both normal circumstances and crisis events, such as the COVID-19 pandemic, because it is an online self-assessment tool. However, those who do not have a mobile phone or who cannot access the internet are limited in performing the self-assessment. This tool may not be appropriate for another generation.
Suggestions
The SHL-PPA should be explored using EFA and should be used to widely survey SHL to prevent pregnancy. Then, an appropriate SHL intervention should be created, and its effectiveness tested to improve the SHL level in the target adolescents.
Abbreviations
CVI, Content Validity Index; EFA, Exploratory Factor Analysis; IOC, Index of Item-Objective Congruence; IQR, Interquartile Range; KMO, Kaiser-Meyer-Olkin measure; R&D, Research and Development; S-CVI, Content Validity Index for Scale; I-CVI, Item Content Validity Index; SHL, Sexual Health Literacy; SHL-PPA, Sexual Health Literacy measurement tool for Pregnancy Prevention among Adolescents.
Ethics
Ethical approval for this study under the Helsinki Declaration was approved by Ubon Ratchathani University (certification code: UBU-REC-106/2565) and Burapha University (certification code: HU 098/2565). The participants were informed of the details of this research, and their privacy was protected via confidentiality. Then participants signed informed consent.
Acknowledgments
The researchers would like to express gratitude to all of their informants, including experts, knowledgeable individuals, adolescents, and educational institution administrators. Furthermore, we would like to express our gratitude to the Faculty of Public Health at Burapha University in Thailand for all of their assistance including funding support.
Disclosure
The authors declare that there are no conflicts of interest in this research.
References
1. UNICEF. Adolescents. New Yor: United state of America: UNICEF; 2022. Available from: https://data.unicef.org/topic/adolescents/overview/.
2. Widman L, Evans R, Javidi H, Choukas-Bradley S. Assessment of parent-based interventions for adolescent sexual health: a systematic review and meta-analysis. JAMA Pediatr. 2019;173:866–877. doi:10.1001/jamapediatrics.2019.2324
3. World Health Organization. Adolescent sexual reproductive health; 2022. Available from: https://bit.ly/3leXrxA.
4. Darroch JE, Woog V, Bankole A, Ashford LS. Adding it up: costs and benefits of meeting the contraceptive needs of adolescents; 2016.
5. World Health Organization. Adolescent pregnancy. Switzerland World Health Organization; 2019. Available from: https://www.who.int/publications/i/item/WHO-RHR-19.15.
6. Sully EA, Biddlecom A, Darroch JE, et al. Adding it up: investing in sexual and reproductive health 2019; 2020.
7. Chicca J, Shellenbarger T. Connecting with generation Z: approaches in nursing education. Teach Learn Nurs. 2018;13:180–184. doi:10.1016/j.teln.2018.03.008
8. Dhanoa A, Ehsan F, Huxter K, Moller CL, Nolet-Mulholland L, Dahal R. Young and risky: sexual behaviours among generation Z and millennials. Eureka. 2020;2020:5.
9. Manwong M, Thongnopakun S, Rodjarkpai Y, Wattanaburanon A, Visanuyothin S. Sexual health literacy and preventive behaviors among middle-school students in a rural area during the COVID-19 situation: a mixed methods study. Health Promot Perspect. 2022;12:178–185. doi:10.34172/hpp.2022.22
10. Vongxay V, Albers F, Thongmixay S, et al. Sexual and reproductive health literacy of school adolescents in Lao PDR. PLoS One. 2019;14:e0209675. doi:10.1371/journal.pone.0209675
11. Thongnopakun S, Pumpaibool T, Somrongthong R. The effects of an educational program on knowledge, attitudes and intentions regarding condom and emergency contraceptive pill use among Thai female university students. J Health Res. 2018;32:270–278. doi:10.1108/JHR-05-2018-033
12. Porter AW, Cooper SC, Palmedo PC, Wojtowicz N, Chong J, Maddalon M. Podcasts and their potential to improve sexual health literacy in adolescents and young adults. Am J Sex Educ. 2021;1–12. doi:10.1080/15546128.2021.1987365
13. McDaid L, Flowers P, Ferlatte O, Young I, Patterson S, Gilbert M. Sexual health literacy among gay, bisexual and other men who have sex with men: a conceptual framework for future research. Cult Health Sex. 2021;23:207–223. doi:10.1080/13691058.2019.1700307
14. Guzzo KB, Hayford S. Race-ethnic differences in sexual health knowledge. Race Soc Probl. 2012;4:158–170. doi:10.1007/s12552-012-9076-4
15. Maasoumi R, Lamyian M, Montazeri A, Azin SA, Aguilar-Vafaie ME, Hajizadeh E. The sexual quality of life-female (SQOL-F) questionnaire: translation and psychometric properties of the Iranian version. Reprod Health. 2013;10:1–6. doi:10.1186/1742-4755-10-25
16. Ministry of Public Health. Health Literacy Scale for Unwanted Pregnancy Prevention of Thai Female Adolescents. Nonthaburi: Ministry of Public Health; 2014.
17. Graf AS, Patrick JH. Foundations of life-long sexual health literacy. Health Educ. 2015. doi:10.1108/HE-12-2013-0073
18. Nomsiri A, Srisiri S, Virutsetazin K, Malarat A. Development of sexual health literacy indicators for early adolescent. Thammasat Med J. 2015;15:609–621.
19. Boonthanom C, Jamjuree D, Yoonaisil W. Puntip Sirivunnabood, Nikorn Dusitsin. Qualitative study: 1 stage of sexual literacy indicators development. J Educ Meas. 2015;21:37–50.
20. World Health Organization. Sexual and reproductive health literacy and the SDGs; 2016. Available from: http://www.who.int/healthpromotion/conferences/9gchp/sexual-reproductive-health-literacy/en/.
21. Martin SP. Young People’s Sexual Health Literacy: Seeking, Understanding, and Evaluating Online Sexual Health Information. University of Glasgow; 2017.
22. Kiddee K. Factors and indicators in the sexual literacy of Thai adolescents Veridian E-Journal, silpakorn university (humanities, social sciences and arts). J Silpakorn Univer. 2019;12:588–602.
23. Narkbubpha R, Deoisares W, Pongjaturawit Y, Graham M, Whitfield C. Experiences of sexual health literacy in sexual relationship among female adolescent students with unplanned pregnancy: a qualitative study. Thai Pharmaceut Health Sci J. 2020;15:106–115.
24. Vamos CA, Thompson EL, Logan RG, et al. Exploring college students’ sexual and reproductive health literacy. J Am Coll Health. 2020;68:79–88. doi:10.1080/07448481.2018.1515757
25. Rakhshaee Z, Maasoumi R, Nedjat S, Khakbazan Z. Sexual health literacy, a strategy for the challenges of sexual life of infertile women: a qualitative study. Galen Med J. 2020;9:e1862–e. doi:10.31661/gmj.v9i0.1862
26. Wong JY-H, Zhang W, Wu Y, et al. An interactive web-based sexual health literacy program for safe sex practice for female Chinese university students: multicenter randomized controlled trial. J Med Internet Res. 2021;23:e22564–e. doi:10.2196/22564
27. Prongprommarat J, Hongkhuntod A, Talas W. The development of sexual literacy scale and norm of secondary school students. J Educ. 2021;8:23–35.
28. Panahi R, Dehghankar L, Amjadian M. Investigating the structural validity and reliability of the sexual health literacy for adults (SHELA) questionnaire among a sample of women in Qazvin, Iran. BMC Women’s Health. 2022;22:524. doi:10.1186/s12905-022-02112-2
29. Rashidi K, Watson P, Farahani H, Chesli RR, Abiri FA. Developing and validating the sexual health literacy scale in an Iranian adult sample. Humanit Soc Sci. 2023;10:1–9. doi:10.1057/s41599-023-01669-z
30. Alvarez-Nieto C, Pastor-Moreno G, Grande-Gascón ML, Linares-Abad M. Sexual and reproductive health beliefs and practices of female immigrants in Spain: a qualitative study. Reprod Health. 2015;12:1–10. doi:10.1186/s12978-015-0071-2
31. Vongxay V, Thongmixay S, Stoltenborg L, et al. Validation of the questionnaire on sexual and reproductive health literacy for adolescents age 15 to 19 years in lao people’s democratic republic. HLRP. 2022;6:e37–e50. doi:10.3928/24748307-20220207-01
32. Lilja KK, Laakso K, Palomäki J. Using the Delphi method.
33. Macmillan TT. The delphi technique annual meeting of the California junior college associations committee on research and development. Monterey, California; 1971.
34. DeVellis RF, Thorpe CT. Scale Development: Theory and Applications. Sage publications; 2021.
35. Sarmento R, Costa V. Comparative Approaches to Using R and Python for Statistical Data Analysis. IGI Global; 2017.
36. Polit DF, Beck CT. The content validity index: are you sure you know what’s being reported? Critique and recommendations. Res Nurs Health. 2006;29:489–497. doi:10.1002/nur.20147
37. Shatto B, Erwin K. Moving on from millennials: preparing for generation Z. J Contin Educ Nurs. 2016;47:253–254. doi:10.3928/00220124-20160518-05
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.