Back to Journals » Clinical Interventions in Aging » Volume 21
Development and Validation of a Risk Screening Model for Depressive Symptoms in Older Inpatients: A Cross-Sectional Study
Authors Wang L, Zhang X, Cheng S, Deng K
Received 26 January 2026
Accepted for publication 6 May 2026
Published 15 May 2026 Volume 2026:21 599044
DOI https://doi.org/10.2147/CIA.S599044
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Lu Wang,1 Xin Zhang,2 Shaoping Cheng,3 Kaiqin Deng4
1Department of Science and Education, The First Affiliated Hospital of Yangtze University, Jingzhou, People’s Republic of China; 2Department of Medical Record Statistics, The First Affiliated Hospital of Yangtze University, Jingzhou, People’s Republic of China; 3Department of Surgery, The First Affiliated Hospital of Yangtze University, Jingzhou, People’s Republic of China; 4Department of Mental Health, The First Affiliated Hospital of Yangtze University, Jingzhou, People’s Republic of China
Correspondence: Kaiqin Deng, Department of Mental Health, The First Affiliated Hospital of Yangtze University, Jingzhou, People’s Republic of China, Email [email protected]
Purpose: Depression is common among the elderly and linked to higher morbidity, mortality, and healthcare costs. Hospitalized elderly patients are especially vulnerable. This study aimed to develop a novel, convenient, and validated tool for preliminary screening of depression symptoms in older inpatients.
Patients and Methods: This study utilized clinical data from 11,269 hospitalized geriatric patients aged ≥ 60 years, collected from January 2023 to December 2024. Data sources included medical record systems,health information management system and inpatient psychological assessment scale information system. Multivariate logistic regression analysis was performed to determine the predictors and further construct a nomogram based on the predictors. Bootstrap with 5000 resamples was used for internal validation of nomogram. Model performance was evaluated using the area under the receiver operating characteristic curve (AUC), calibration curves and decision curve analysis (DCA).
Results: The prevalence of depressive symptoms in older inpatients was 28.64%. Eight independent influencing factors were identified: gender, age, marital status, income source, sleep disturbance, chronic diseases, pain, and self-rated health. The development set AUC was 0.930, and the corrected AUC after internal validation was 0.832. The Hosmer-Lemeshow test (P = 0.126) and calibration curves indicated favorable calibration. DCA confirmed clinical net benefit across a range of threshold probabilities.
Conclusion: An easy-to-use nomogram was developed for identifying depressive symptoms in older inpatients with satisfactory screening ability based on simple and easily accessible clinical features. The nomogram can identify older inpatients at high risk for depressive symptoms and may be a useful preliminary screening tool in clinical.
Keywords: aged, inpatients, depressive symptoms, prognostic factors, risk assessment
Introduction
Depression is a common mental health problem in older adults and has become one of the most important factors affecting the health of the elderly population, which can directly cause disability, trigger self-harm and suicidal tendencies,1,2 and indirectly lead to other physical health problems and care complications, placing a significant burden on healthcare and social care systems.3 The global burden of depression is rising sharply. According to the World Health Organization and the Global Burden of Disease Study, major depressive disorder is projected to become the leading cause of disease burden worldwide by 2030.4 The Global Health Assessment Report shows that the prevalence of depression in older adults has peaked, with more than 10% of older adults worldwide suffering from depression.5
In China, the situation is particularly concerning. Based on the Global Burden of Disease (GBD) database statistics, in 2019 there were about 15 million patients with depression in the elderly in China, with a prevalence rate as high as 5.97%, which is significantly higher than the 3.67% prevalence in the 20–55 age group.6 Depression has become the fourth leading cause of disability in China and older adults with depression are more likely to experience unintentional disability and have an increased risk of death compared with normal people.7–9
For hospitalized older patients, the compounded consequences of comorbid depression are even more severe. With the accelerated aging of the population, the number of older patients is increasing year by year, and the negative emotional experiences of patients intensify during the period of illness, which becomes a main trigger of depression.10 Older inpatients have a significantly higher depression than younger inpatients, and their disease prognosis is poorer than that of the younger population.11,12 More importantly, comorbid depression in older inpatients exacerbates chronic disease prognosis, prolongs hospital stays, increases healthcare expenditures, and elevates mortality risk. Therefore, identifying high-risk patients earlier, before typical clinical symptoms appear and providing early intervention is crucial to controlling this condition.
Despite this urgent need, existing models have notable gaps. Currently, numerous models have been used to analyze the risk of depression in populations, primarily based on sociodemographic factors, lifestyle variables, health indicators, environmental influences, genetic information, as well as blood biomarkers and brain imaging techniques.13–21 Many studies have explored the application of machine learning in predicting the severity of depression, often using different data sources, such as biomarkers, functional brain activity metrics, and behavioural data.22,23 However, most prior models focused on only one category of predictors, either biological markers (eg., neuroimaging, genetic data) or sociodemographic/lifestyle variables alone. Few models integrated multiple domains simultaneously (eg., health status, lifestyle, demographic, and socioeconomic indicators), lacking a comprehensive, multi-dimensional screening tool. Many models relied on costly or inaccessible predictors, such as brain CT, MRI, PET-CT scans, or specialized blood biomarkers,which cannot be performed in many hospitals or clinics due to limited equipment or high expense. Additionally, many models were developed from department-specific samples (eg., neurology, oncology, psychiatry), severely limiting their generalizability to general older inpatient populations. Consequently, there existed a clear gap between “predictive accuracy” and “clinical practicality.”
To address these gaps, the study aimed to develop an easy-to-use, practical screening tool for depressive symptoms in older inpatients. Specifically, it utilized only routinely collected, mandatory clinical data from medical record systems and health information management systems, no additional costly tests or specialized equipment were required. The study incorporated multiple predictor domains (demographic, health status, lifestyle, and socioeconomic indicators) to capture the complexity of depression risk. It developed and validated the model based on a large, cross-departmental sample of older inpatients, not restricted to a single specialty. By balancing predictive accuracy with clinical feasibility, the model can rapidly identify high-risk older inpatients at admission while minimizing additional burden on clinical staff.
Methods
Study Participants
We retrospectively collected clinical data from older inpatients from January 2023 to December 2024 in the hospital. Inclusion criteria: Hospitalized patients aged ≥60 years. Exclusion criteria: Cases with missing data. A total of 11,813 eligible cases were initially identified. Missing data were observed in the PHQ-9 score, with 544 cases missing (missing rate = 4.6%). No missing values were found for the independent variables, as these variables were derived from mandatory entry fields in the system. To verify the missing data mechanism, we compared the baseline characteristics between excluded patients (n=544) and included participants (n=11,269), as presented in Supplementary Table 1. No significant differences were observed between the two groups (all P > 0.05), which verified that the missing data were consistent with the missing completely at random(MCAR) mechanism.24 Given the low overall missing rate (< 5%) and MCAR property, complete case analysis (CCA) was adopted. For sensitivity analysis, multiple imputation (MI) with 10 imputed datasets was further conducted. Comparisons of OR values, AUC, calibration curves and decision curve analysis showed consistency between CCA and MI results, verifying the robustness of the main findings against different missing data strategies. Finally, a total of 11,269 participants were included in the subsequent model construction. The study was reviewed and approved by the Ethics Committee of the hospital (Approval No. KY202563). The study was conducted in accordance with the principles of the Declaration of Helsinki.
Variable Definitions and Data Collection
Candidate variables were selected based on literature review and clinical relevance. These variables were assorted into four categories: (1) Demographic variables include gender, age, ethnicity, marital status, education, residential area, etc. (2) Health status variables include admission route (outpatient or emergency), self-rated health status, presence of chronic diseases, injuries,pain, falls in the past two years, medication allergies, etc. (3) Lifestyle variables include sleep status, smoking, drinking, etc. (4) Socioeconomic variables include health care payment method, sources of income, occupation etc. Some of the variable definitions and codes are shown in Supplementary Table 2.
In this study, the operational definition of chronic diseases was formulated according to the China’s Medium-to-Long Term Plan for the Prevention and Treatment of Chronic Diseases (2017–2025) and ICD-10 coding standards. Chronic diseases included but were not limited to cardiovascular diseases (hypertension, coronary artery disease, chronic heart failure,stroke), chronic respiratory diseases (chronic obstructive pulmonary disease, asthma), type 1 and type 2 diabetes mellitus, chronic kidney disease, chronic liver disease, chronic neurological (dementia, Parkinson’s disease), malignant tumors, and major musculoskeletal and arthritic disturbance. Only formally diagnosed and documented conditions in the medical record systems. Symptoms, risk factors (eg., pre-hypertension), or conditions managed solely outside our hospital system without a formal transfer note were excluded. The diagnostic information was extracted from structured “Medical History” and “Admission Diagnosis”, routinely completed by attending physicians, and categorized based on standardized ICD-10 codes.
Since 2020, the hospital has implemented an “Inpatient Psychological Assessment Scale” information system. This system routinely screens for depressive symptoms among all inpatients, with a specific focus on older inpatients, using the Patient Health Questionnaire-9 (PHQ-9). The PHQ-9 comprises nine items, each scored on a four-point scale ranging from 0 (Not at all) to 3 (Nearly every day). The overall score ranges from 0 to 27; thresholds for levels of severity are as follows: 0–4, none; 5–9, mild; 10–14, moderate; 15–19, moderately severe; and 20–27, severe.25 A score of ≥ 5 indicates depressive symptoms, with higher scores reflecting greater severity. The Cronbach’s alpha coefficient for the scale in this study was 0.818, indicating good internal consistency reliability.
Sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI) in the mobile nursing information system. It consisting of 19 items covering seven domains: subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction, with a total score ranging from 0 to 21 points. Higher scores indicate more severe sleep disturbances.26 The total score (0–21) can be categorized into four levels: 0–5(normal/good sleep quality), 6–10 (mild sleep disturbance), 11–15 (moderate sleep disturbance), and 16–21 (severe sleep disturbance). For analytical simplicity, we combined the mild and moderate disturbance groups into a single category of 6–15 (mild/moderate disturbance).
Self-rated health was assessed by a single question, “How would you rate your overall health?”, with five response options: very good, good, fair, poor, and very poor. This information was recorded in the medical record system by the attending physician upon admission.
The hospital organized specialized training for all clinical nurses to ensure standardization of assessments. The inpatient psychological assessment scale assessment became an institutionalized and systematic component of the inpatient admission nursing assessment, thereby minimizing inter-rater variability at its source. The PHQ-9 scores, and sleep quality were collected by the primary nurse via face-to-face interviews after patient admission, during clinically stable periods. Questions were posed using standardized prompts, with responses entered in real-time into the mobile nursing information system integrated with a standardized module.
Data Analysis
All statistical analyses were performed using SPSS 26.0 and R software (version 4.4.2). Continuous data following a normal distribution were presented as mean ± standard deviation (SD) and compared using the independent samples t-test. Non-normal continuous data were presented as medians with interquartile ranges (IQRs) M (Q1, Q3) and compared using the Mann–Whitney U-test. Categorical data were presented as frequency (percentage) n (%) and compared using the Chi-squared test (or Pearson’s Chi-squared test).
Multivariate logistic regression analyses (using a stepwise forward selection procedure with entry P < 0.05 and removal P > 0.10) were performed to identify independent predictors among those with univariate P < 0.05. The final screening model was presented as a nomogram. The bootstrap resampling method (5000 bootstrap resamples) was used for internal evaluation. Model performance was evaluated by the area under the receiver operating characteristic curve (AUC), calibration curves, and decision curve analysis (DCA).27 All statistical tests were two-sided and P<0.05 was regarded as statistically significant.
Results
Characteristics of Participants
Of the 11,269 older inpatients included in this study, 3,228 were assessed as having depressive symptoms. The majority of inpatients were aged between 60 and 79 years, accounting for 83.56%. Additionally, 53.3% were male, 91.52% reported having a spouse or partner, 55.98% were diagnosed with chronic diseases.More details were presented in Table 1.
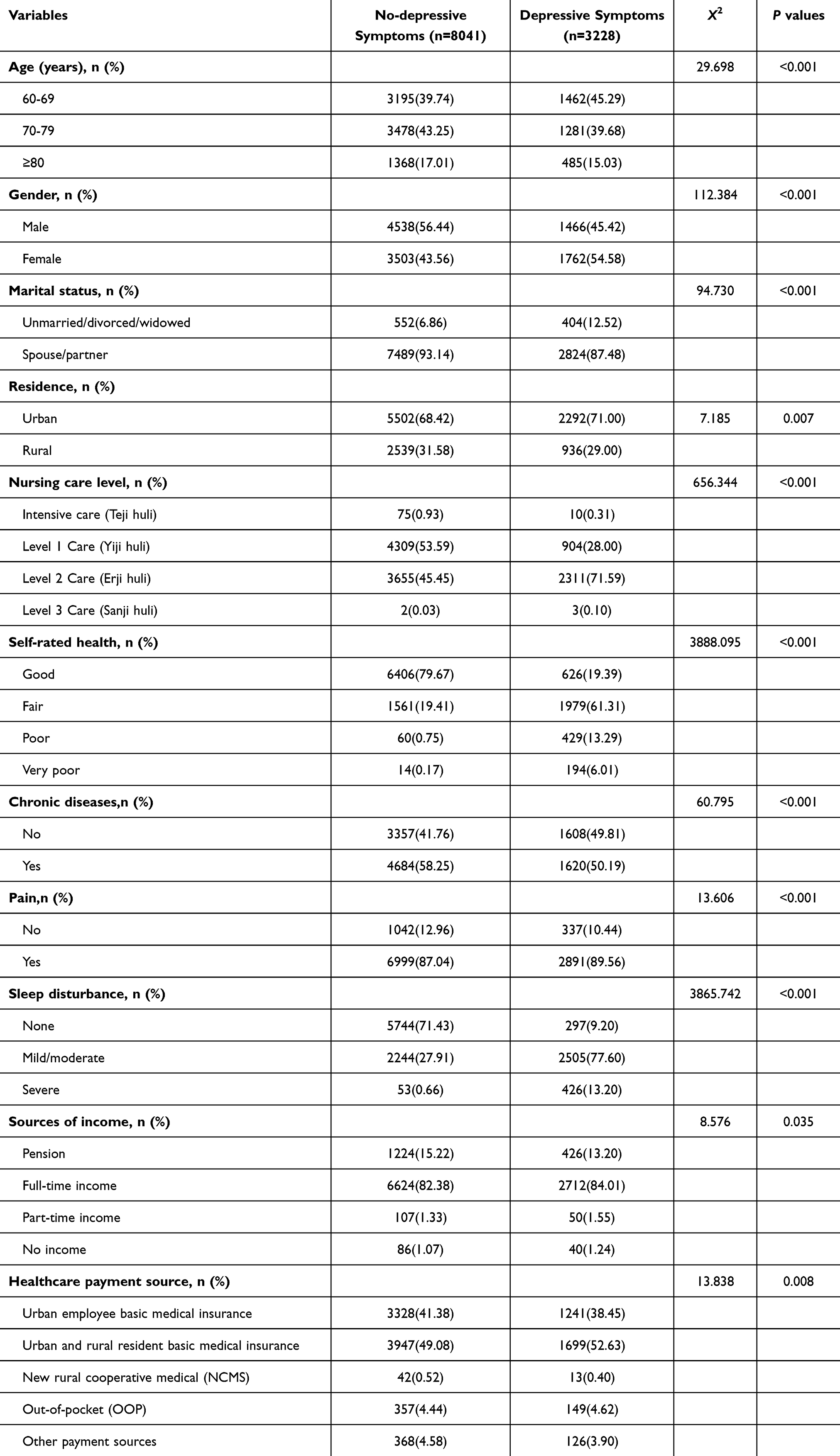 |
Table 1 The Univariate Analyses |
Univariate Analysis and Multivariate Logistic Regression Analysis
As shown in Table 1, the univariate analysis identified that a total of 11 factors were associated with depressive symptoms among older inpatients. We performed multicollinearity diagnostics for all independent variables. The results indicated that the variance inflation factors (VIFs) for all variables were less than 5, which stated that there was no collinearity among the independent variables. Therefore, all variables included in the regression analysis were not mutually related.
The detailed results of the multivariate logistic regression analysis were presented in Table 2. Gender, age, marital status, self-health, chronic diseases, pain, sleep disturbance, sources of income were included in a multivariate logistic regression model. Compared with male patients, female gender was associated with higher odds (OR = 1.319). Compared with ages 60–69, ages 70–79 (OR=2.897) and ≥80 (OR=1.621) showed increased odds. Unmarried/ divorced/ widowed status had higher odds than being married/partnered (OR = 3.020). Worse self-rated health was linked to greater odds, versus “good”, fair (OR=2.251), poor (OR=3.621), and very poor (OR=4.531). Chronic diseases (OR=2.476) and pain (OR=2.114) were significant risk factors. Compared with no sleep disturbance, mild/moderate disturbance (OR=3.614) and severe disturbance (OR=6.624) showed strong associations. For income sources, versus pension, full-time income had borderline significance (OR=1.414), no income had higher odds (OR=4.488), and part-time income was not significant (OR=1.057).
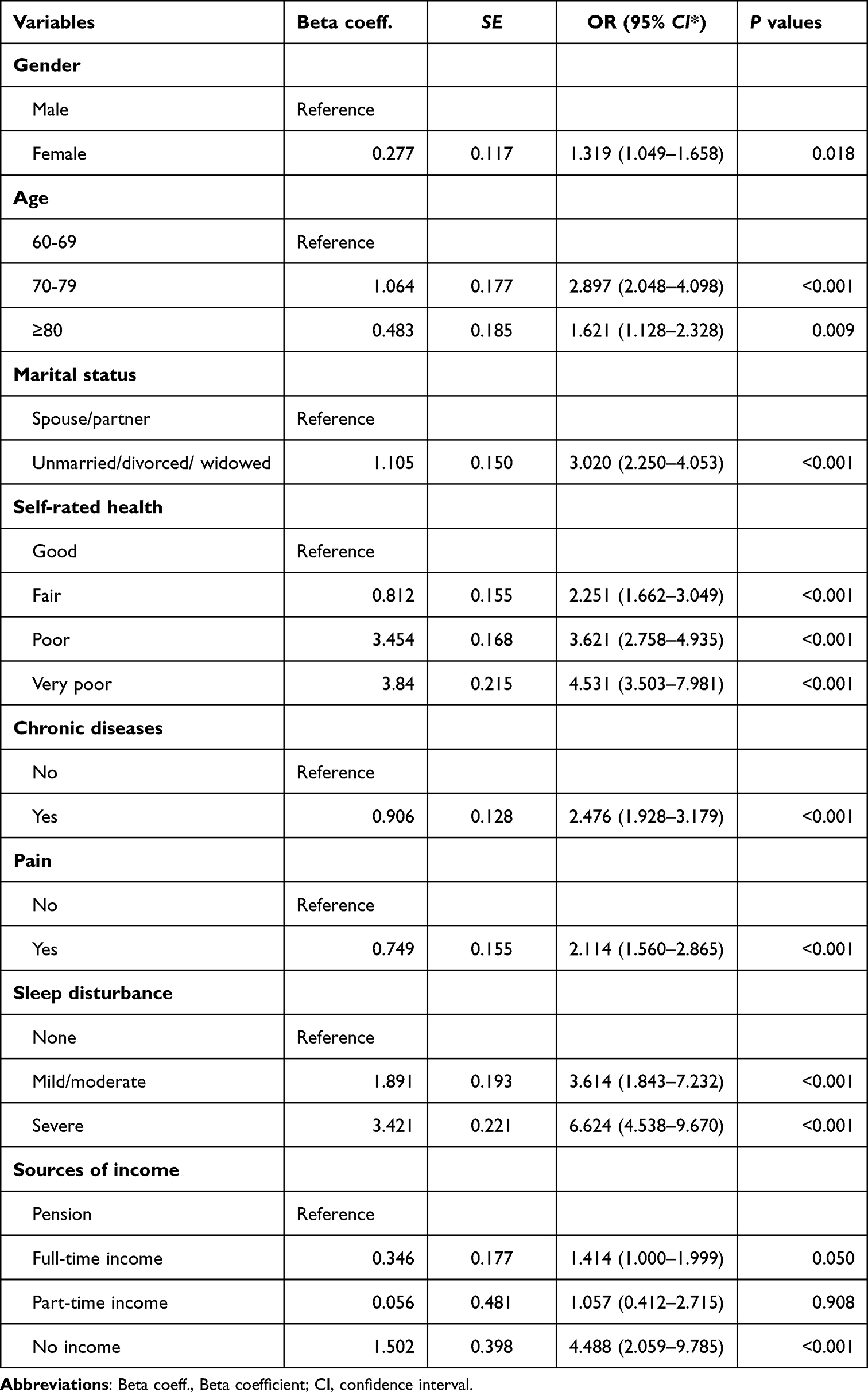 |
Table 2 The Multivariate Logistic Regression Analysis for Depressive Symptoms Among Older Inpatients |
Construction of the Nomogram Model
On the basis of the multivariate logistic regression analysis, a nomogram was constructed to quantitatively asses the risk probability of depressive symptoms among older inpatients (Figure 1). The value of each of these factors gives a score on the point scale axis. By summing each score and projecting the total score onto the bottom risk scale axis, we can easily calculate the total score and estimate the likelihood of depressive symptoms in older inpatients. Suppose a 65-year-old female patient who lived alone, had chronic diseases and mild sleep disturbances, received a pension, had good self-rated health, and had no pain. Based on this information, the corresponding scores in the nomogram are derived, and the sum of the scores for the variables is 157.5. The nomogram assessed a probability of approximately 15% that the patient would develop depressive symptoms.
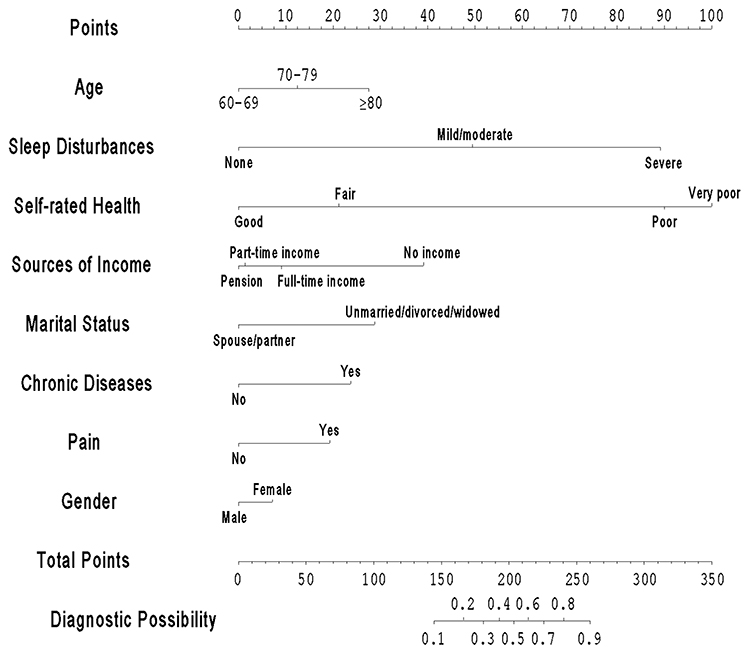 |
Figure 1 Nomogram predicting the probability of depression. |
Evaluation of the Nomogram
For the nomogram, the AUC was 0.930 (95% CI: 0.919–0.941, P <0.001) (Figure 2). The Hosmer-Lemeshow goodness of fit test was used to calibrate the model of depressive symptoms among older inpatients. The Hosmer-Lemeshow goodness of fit test indicated that the model was well calibrated (ꭓ2=12.617, P = 0.126). The calibration curve for the model shown overall good agreement between the assessed and observed values (Figure 3). According to the data from the modeling datasets, the curves for most of the predicted threshold probabilities were above the two extreme lines in the 0–1 threshold probability range, suggesting that the model has some clinical validity (Figure 4). The accuracy of the nomogram was internally validated by the bootstrap resampling method (5000 bootstrap resamples), and as shown by the calibration curve, the model shown that the predicted and actual probabilities were highly consistent (Figure 5). The bootstrap-corrected concordance index (C-index) of the nomogram was 0.832 (95% CI: 0.825–0.839).
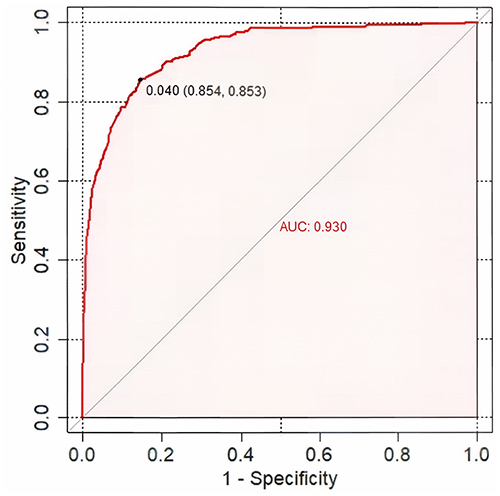 |
Figure 2 The ROC curve of the nomogram predictive model. |
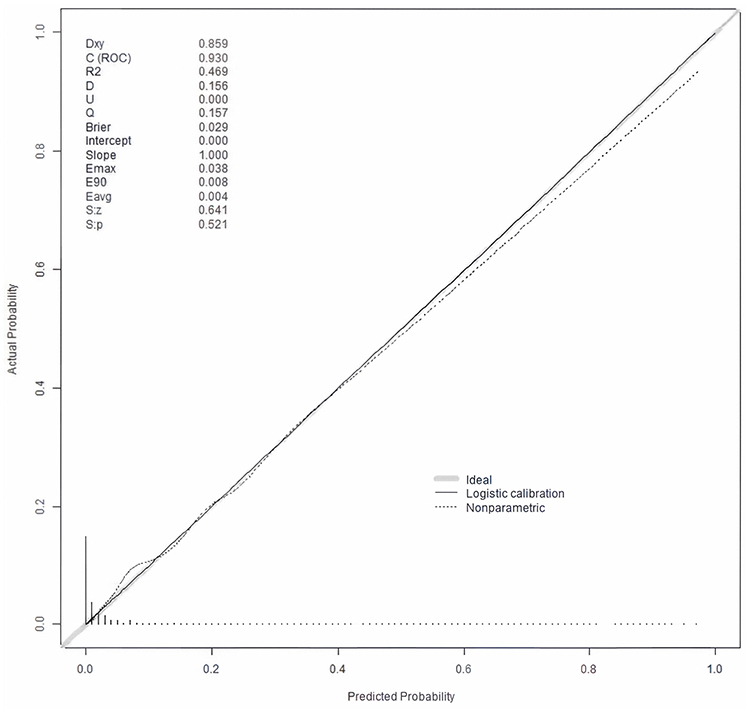 |
Figure 3 The calibration curve of the nomogram prediction model. |
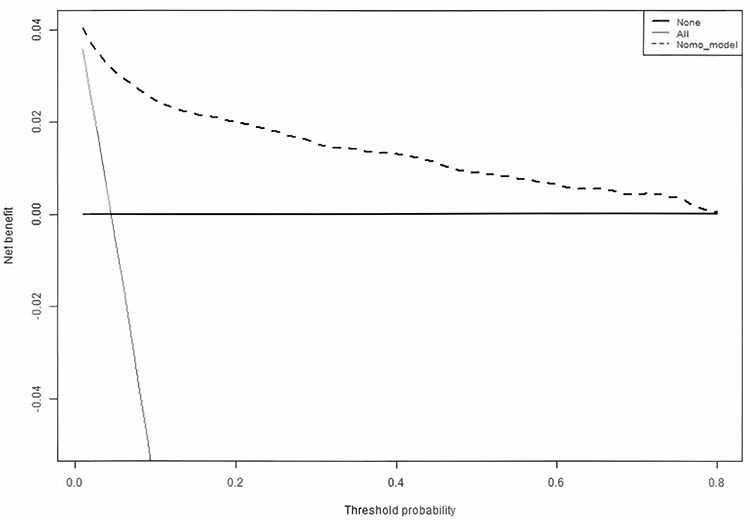 |
Figure 4 Decision curve analysis of the nomogram prediction model. |
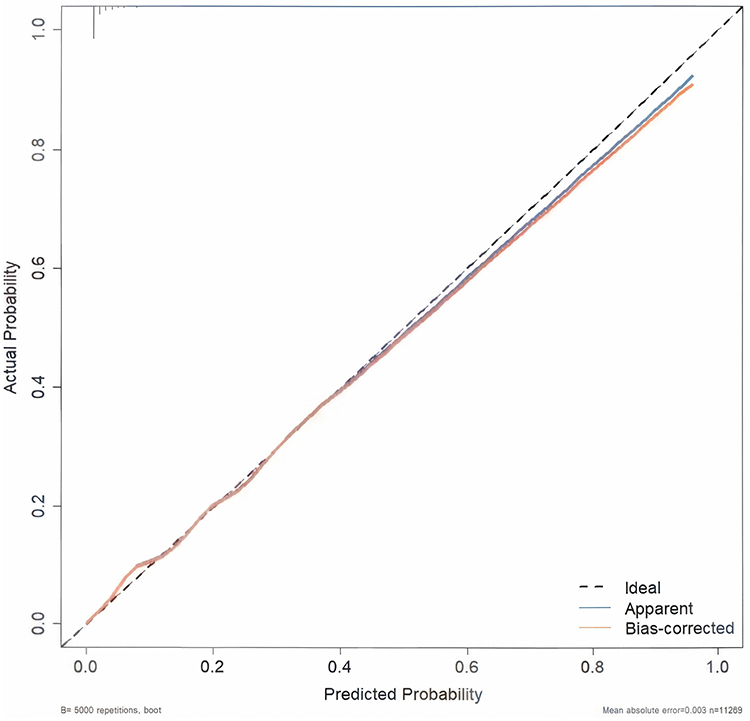 |
Figure 5 Bootstrap method for internal validation of calibration curves for the nomogram. |
Discussion
In this study, a simple nomogram for screening older inpatients at risk of depressive symptoms was developed. The results suggested that the model has potential due to its discrimination and calibration ability to assess the occurrence of depressive symptoms. In addition, the model has good clinical utility and can be used as a reference tool for clinicians screening for depressive symptoms.
Age, Gender and Depressive Symptoms
Current research identifies both gender and age as significant predictors of depressive symptoms in elderly patients.28 These findings align with previous studies, demonstrating that ageing in this population was associated with physiological decline, functional dysregulation, or deterioration across multiple bodily systems. Neuroendocrine system dysfunction, such as thyroid abnormalities, was frequently implicated.29,30 Extant evidence indicated that advancing age heightens vulnerability to physiological decline, chronic disease-related functional impairment, diminished social engagement, reduced social support, and increases susceptibility to loneliness. Elderly individuals also exhibit heightened sensitivity to changes in their health status. Collectively, these factors constitute major contributors to elevated depression risk.31–33
Concurrently, the oldest-old (typically defined as ≥80 years) exhibit a higher prevalence of living alone and frailty status,34 further augmenting their susceptibility to depression. Research demonstrates a significantly higher incidence of depression in this advanced-age cohort compared to younger elderly individuals (aged 60–79 years).35
The results further revealed a marked gender disparity: women exhibited a substantially greater propensity for developing depression, with a risk approximately twice that of men.36,37 This heightened vulnerability in females may stem from hormonal fluctuations, social stressors, and sex-related neurohormonal and psychological differences.38 Additionally, elderly women face a greater likelihood of widowhood and solitary living, compounding depression risk.39 Studies indicated that female older patients manifest a greater inclination toward low mood and depressive symptoms when confronting chronic illness or somatic discomfort.
Marital Status and Depressive Symptoms
Widowed or unmarried elderly individuals exhibited a higher risk of depression. The absence of companionship and support from a partner may contribute to feelings of isolation, lack of validation, diminished self-confidence, reduced social engagement, and lead to insufficient emotional and material support, potentially increasing vulnerability to psychological stress and distress.40,41
This study found that widowed or unmarried older adults had 3.020-fold higher odds in exhibiting depressive symptoms compared to married and cohabiting older adults, consistent with previous research findings.42
Marriage provided unique social, psychological, and economic resources not typically found in other relationship types. These resources, as protective factors, were more likely to promote health and longevity among older adults with spouses.43 Due to the spousal role in providing care and support, marriage can broaden the scope of social support older adults receive from their families.44 Advancing age often restricts the living environment of older adults and reduces their sources of social support, making spousal support a crucial component of their social network. For widowed older adults, the loss of spousal companionship and support can lead to psychological distress and emptiness, even triggering depressive symptoms.45,46 This effect was particularly relevant for widowed elderly patients living alone, who may additionally face challenges such as a lack of family care, poor self-management abilities, and reduced initiative in seeking treatment.47,48
Sleep Disturbances and Depressive Symptoms
Sleep is a vital physiological process essential for self-regulation and maintaining internal homeostasis. It plays crucial roles in memory consolidation, brain function protection, and immune system modulation.49 Adequate sleep supports normal cognitive functions, including decision-making, language processing, information handling, and memory storage.50
Sleep disturbances encompass disturbance characterised by excessive sleep, insufficient sleep, disruptions in the sleep-wake cycle, or abnormal behaviours during sleep.51
Ageing is associated with alterations in sleep architecture. Compared to younger adults, older adults exhibit reduced proportions of deep (slow-wave) sleep and rapid eye movement (REM) sleep, decreased sleep efficiency, and prolonged sleep latency. Concurrently, the high prevalence of underlying comorbidities among the elderly further predisposes them to sleep problems.52,53
Sleep disturbances are highly prevalent in this population,54,55 affecting nearly half of older adults, with at least one-fifth meeting diagnostic criteria for insomnia.56 Chronic and recurrent sleep disturbances imposed significant physiological and psychological burdens on older adults.
A significant association exists between sleep disturbances and depression,57,58 a finding corroborated by this study. Elderly inpatients with sleep problems demonstrated a significantly higher incidence of depression compared to those with good sleep quality. Research indicated a bidirectional relationship between sleep disturbances and depression.59,60 Disturbances such as insomnia and sleep fragmentation are common symptoms of depression but may also acted as contributing factors or triggers. Poor sleep quality can induce anxiety and depressive mood, while depression, in turn,disrupts sleep patterns.61,62 In elderly patients, sleep disturbances often stem from chronic diseases, medication side effects, or environmental factors, thereby elevating depression risk. Studies suggested that sleep disturbances may increase vulnerability to depression by impairing activities of daily living and emotional regulation.63 Furthermore, sleep quality not only impacted the presence of depression in the elderly but also influenced the risk of relapse following a depressive episode remission.63 The often “invisible” nature of sleep disturbances, coupled with their frequent underdiagnosis and undertreatment,64 represents a critical vulnerability in elderly patient health management. Research indicated that comorbid sleep disturbances, depression, and anxiety present greater treatment challenges and impose a heavier disease burden on elderly patients.65
Chronic Diseases and Depressive Symptoms
Geriatric depression is frequently associated with chronic diseases, including cardiovascular disease, chronic obstructive pulmonary disease (COPD), diabetes, and Parkinson’s disease.66–71 Consistent with these previous findings, the present study demonstrates that older adults with chronic diseases have a 2.476-fold higher risk of developing depression compared with those without chronic diseases. Accumulating evidence suggests that chronic diseases are risk factors for depressive states, and this relationship is bidirectional, as each condition may act as both a cause and an effect.72–74 Chronic diseases often entail prolonged courses and incomplete recovery, which can induce negative emotions and lead to depressive symptoms. Furthermore, the long-term medication regimens typically required for chronic disease management significantly compromise the quality of life for older adults. This impaired quality of life, coupled with the cumulative burden of adverse drug effects(ADEs), exacerbates depressive symptoms. Ongoing medical expenses not only increase the financial burden on families but also heighten psychological distress for the elderly, ultimately precipitating the onset or exacerbation of depressive symptoms over time.75
This relationship is a matter of significant concern, as growing evidence highlights their complex interplay and combined impact on overall health and well-being.76,77 Substantial research has indicated that depression worsens disease prognosis, increases mortality, and complicates treatment outcomes in patients with cardiovascular disease, diabetes, and other chronic conditions.78,79 Depression may directly influence both the development and the course and progression of chronic diseases through biological mechanisms, including dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis, increased inflammation, and autonomic dysfunction.80–91
Research also has indicated that the risk of developing chronic diseases increases with age. Individuals with multiple chronic conditions exhibit a higher risk of depression.74,82,83 Several studies have quantified a dose-response relationship between the number of coexisting chronic physical conditions and the risk of a depressive state (DS).84,85
Economic, Health Status, and Depressive Symptoms
Sources of income is another significant factor influencing the depressive state in elderly patients, with a well-established relationship between socioeconomic factors and depression.71,86 In this study, depressive symptoms were more prevalent the unemployed. Disparities in individual socioeconomic status constitute fundamental underlying causes of the emergence and exacerbation of health inequities. Among these, economic is one of the most basic and critical health determinants. It directly impacts key aspects such as livelihood resource adequacy, poor living conditions, access to comprehensive healthcare, and deficiencies in social security systems. Elderly patients with better economic standing can access more specialized care and greater opportunities to obtain health information for self-protection. Conversely, for older adults with limited financial resources, illness led to substantially reduced health-promoting behaviours and reduced assess to medical care, ultimately impacting their self-rated health.87
Health status is a crucial determinant of depressive symptoms, and the relationship between pain and mental health symptoms is complex and bidirectional. Chronic pain, as a source of various health risks, is closely associated with comorbidities such as depression and sleep disturbance, further contributing to increased frailty and depressive states in the elderly.88 This interrelationship among pain, depression, and anxiety symptoms often led to diagnostic uncertainty and excessive polypharmacy, complicating disease management.89 Among hospitalised elderly patients, poor sleep quality, chronic pain, and depressive symptoms frequently co-occur with frailty.90,91 Research has indicated cumulative associations between pain, insomnia (difficulty initiating and maintaining sleep), depressive symptoms, and frailty in older adults. Results demonstrated a synergistic effect of pain, sleep initiation difficulty, and depressive symptoms on frailty, with the odds ratio increasing substantially to 10.20-fold higher than that associated with individual symptoms alone.90,91
Self-rated health (SRH) is the subjective assessment and estimation of health status by older adults, which represents subjective health complaints, defined as any health-related symptom or concern not accompanied by objective pathological signs.92 Previous studies have found a positive correlation between geriatric depression and all subscales of subjective health complaints in older adults.93–95 The results of this study demonstrate that the risk of depressive symptoms among older patients with poor SRH is 3.621 times higher than that among those with good SRH. This association may stem from the fact that SRH largely reflects the objective health status of older adults, which itself significantly predicts depression. As individuals age, physiological functions progressively decline, chronic physical diseases become more prevalent, and the ability to perform activities of daily living diminishes. This can lead to feelings of worthlessness due to a perceived inability to contribute meaningfully, resulting in poorer mental states and an increased susceptibility to depressive symptoms.96
Older inpatients with poor SRH may fear that illnesses will trigger emotional distress, thereby precipitating depressive symptoms. Conversely, those with good SRH are likely to maintain confidence in their health and adopt positive life attitudes, consequently reducing the likelihood of developing depressive symptoms.
Descriptive analysis reveals that older patients with chronic diseases exhibit poorer SRH. This may be attributed to persistent physical discomfort and functional impairments stemming from multimorbidity, which collectively induce a more negative overall health perception.97 As a pivotal metric of perceived health status, declining SRH may impair quality of life and substantially elevate depression risk.98 Older adults with chronic conditions frequently experience physical and mental exhaustion due to chronic pain, functional impairments, and complex medication management.99 The cumulative disease burden exacerbates physical distress and deteriorates health evaluations, significantly diminishing SRH.100
Among older patients with multimorbidity, a positive self-concept helps alleviate stress and loneliness while enhancing perceived control and life satisfaction. Conversely, declining SRH correlates with heightened physical and psychological vulnerability, increased pessimism about the future, and quality-of-life concerns, all factors amplifying depression risk.101,102 Crucially, SRH reflects older adults’ holistic health appraisal,103 and this positive holistic health appraisal enhances well-being while effectively mitigating psychological distress and negative emotions associated with health challenges.104,105
Comparison with Previous Studies
Existing models are mostly based on department specific samples (eg.,Neurology, cancer, surgery).27,106,107 By comparison, our study has included 11,269 inpatients from multiple departments (internal medicine, surgery, geriatrics, neurology, etc)., yielding a more representative sample of geriatric inpatient. This broader overcomes the limitation of poor generalizability of previous models, given that depressive symptoms are prevalent across clinical departments, necessitating a generalizable screening tool.
Previous models have incorporated conventional predictors such as age and gender, as well as Activities of Daily Living(ADL) assessed via interviews,106 which necessitates additional time and resources for data collection. All predictors in our model are mandatory fields in the medical record system, ensuring data completeness and alleviating the clinical burden, which is a key advantage for routine clinical application. The model can calculate the risk score at admission, facilitating real-time identification of high-risk patients and prompt intervention. This aligns with the requirements of geriatric mental health management, particularly in high-volume clinical settings.
Limitations
This study has some limitations. All research data were collected from routine hospital medical records, originally collected for clinical care rather than research purposes, which may introduce potential selection and information biases. The study was conducted based on a single-center cohort, which may limit the external generalizability of the established model. Although the large sample size and strict internal Bootstrap validation ensured the stability of the model within the current cohort, the lack of external validation may affect the credibility of the model’s clinical application. The demographic characteristics, disease spectrum and medical environment of different hospitals may affect the model performance. In the future, multi-center external validation is urgently needed to further verify the generalization performance of the model in different clinical institutions and different elderly patient populations.
Conclusions
This study identified the most significant independent risk factors for depressive symptoms among older inpatients and constructed a simple assessment model with good performance. The results suggested that the model has potential due to its discrimination and calibration ability to asses the occurrence of depressive symptoms. The model has undergone only internal validation, and its performance in different populations requires external validation. In addition, the model has good clinical utility, and it is suitable for preliminary depression risk screening in older inpatients at admission but should not be used as a diagnostic tool. High-risk individuals identified through screening require clinical assessment by psychiatrists for confirmation. Future multi-center prospective studies are needed to validate the model’s stability and generalizability across diverse healthcare settings, and to investigate whether model-guided interventions improve patient outcomes.
Data Sharing Statement
The data are availability from the corresponding author on reasonable request.
Ethical Approval
This retrospective study was reviewed and approved by the Ethics Committee of The First Affiliated Hospital of Yangtze University (Approval No. KY202563). The study was conducted in accordance with the World Medical Association Declaration of Helsinki (2024 version). Given the retrospective design and the use of fully anonymized clinical data, the requirement for written informed consent was formally waived by the Ethics Committee, which is consistent with the ethical principles for secondary research involving human data as stipulated in Article 26 of the 2024 Declaration of Helsinki.
Acknowledgments
The authors thank the Department of Information Center of the hospital for providing the data for this research.
Funding
This research did not receive funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Corneliusson L, Gustafson Y, Olofsson B. Prevalence of depressive disorders among the very old in the 21st century. J Affect Disord. 2024;362:706–17. doi:10.1016/j.jad.2024.07.062
2. Lin WJ, Zhang DL, Wang YM. Analysis of depression status and influencing factors in middle-aged and elderly patients with chronic diseases. Front Psychol. 2024;15:1308397. doi:10.3389/fpsyg.2024.1308397
3. Liu TY, Lu SY, Leung DY. Adapting the UCLA 3-item loneliness scale for community-based depressive symptoms screening interview among older Chinese: a cross-sectional study. BMJ Open. 2020;10(12):e041921. doi:10.1136/bmjopen-2020-041921
4. Zhang JH, Zhang D, Xue XZ, et al. Intergenerational psychological capital, disability, and depressive symptoms in the shadow of functional deprivation among middle-aged and older adults in China. Psychol Res Behav Manage. 2025;18:2237–2257. doi:10.2147/PRBM.S552384
5. World Health Organization. Depression and Other Common Mental disturbance:Global Health Estimates. Geneva: World Health Organization; 2017:2.
6. Yang L, Yang Y, Guo YT. Community social capital and depressive symptoms among older adults relocated for poverty alleviation in Shanxi, China: a cross-sectional study. BMCpublic Health. 2025;25(1):255. doi:10.1186/s12889-025-21483-3
7. Liu HX, Zhou ZL, Fan XJ, et al. Association between multiple chronic conditions and depressive symptoms among older Adults in China: evidence from the China Health and Retirement Longitudinal Study (CHARLS). Int J Public Health. 2023;68:1605572. doi:10.3389/ijph.2023.1605572
8. Meng RW, Yu CQ, Liu N. Association of depression with all-cause and cardiovascular disease mortality among adults in China. JAMA Network Open. 2019;3(2):e1921043.
9. Penninx BW, Leveille S, Ferucci L.Exploring the effect of depression on physical disability: longitudinal evidence from the established populations for epidemiologic studies of the elderly. J Public Health. 1999;89(9):1346–1352. doi:10.2105/ajph.89.9.1346
10. Wayne JK. Clinical and health services relationships between major depression, depressive symptoms, and general medical illness. Biol Psychiatry. 2003;54(3):216–226. doi:10.1016/s0006-3223(03)00273-7
11. Marcelo A, Rosa B, Sofía M. Psychosocial functioning in non-psychiatric acute and chronic inpatients: depression, alexithymia and lack of assertiveness. Revista medica de Chile. 2016;144(11):1424–1431. doi:10.4067/S0034-98872016001100008
12. Galvez V, Ho KA, Alonzo A. Modularization the rapies for geriatric depression. Curr Psych Rep. 2015;7(7):59. doi:10.1007/s11920-015-0592-y
13. Jessica R, Christina W, Carlos A, Zarate J. A predictive coding framework for understanding major depression. Front Human Neurosci. 2022;16:787495. doi:10.3389/fnhum.2022.787495
14. Yan J, Li X, Geng Y. A preliminary prediction model of depression based on whole blood cell count by machine learning method. Zhonghua yu fang Yi Xue Za Zhi Chin J Prevent Med. 2023;57(11):1862–1868. doi:10.3760/CMA.J.CN112150-20221202-01169
15. Fan Y, Sheng J, Liang C. Association of blood lead levels with the risk of depressive symptoms in the elderly Chinese population: baseline data of a cohort study. Biol Trace Elem Res. 2020;194(1):76–83. doi:10.1007/s12011-019-01755-x
16. Jeungok C, Jeeyae C, Woo JC. Predicting depression among community residing older adults: a use of machine learning approch. Stud Health Technol Inform. 2018;250:265. doi:10.3233/978-1-61499-872-3-265
17. Annede H, Mariekevan B, Claudio F. Predicting depression risk in patients with cancer using multimodal data. Stud Health Technol Inform. 2023;2023(302):817–818. doi:10.3233/SHTI230274
18. Lee A, Tang S, Yu G. The smiley as a simple screening tool for depression after stroke: a preliminary study. Int J Nurs Studies. 2008;45(7):1081–1089. doi:10.1016/j.ijnurstu.2007.05.008
19. Jin HM, Wu SD. Use of patient-reported data to match depression screening intervals with depression risk profiles in primary care patients with diabetes: development and validation of prediction models for major depression. JMIR Format Res. 2019;3(4):e13610. doi:10.2196/13610
20. Thalia R, Barak F, Andrey M. Using machine learning-based analysis for behavioral differentiation between anxiety and depression. Sci Rep. 2020;10(1):16381. doi:10.1038/s41598-020-72289-9
21. Deng LF, Luo ST, Wang TY. Depression screening model for middle-aged and elderly diabetic patients in China. Sci Rep. 2024;14(1):29158. doi:10.1038/s41598-024-80816-1
22. Tumpa RS, Momotaz B, Jia U. Feature group partitioning: an approach for depression severity prediction with class balancing using machine learning algorithms. BMC Med Res Method. 2024;24(1):123. doi:10.1186/s12874-024-02249-8
23. Brooke L, Andrea B, Brett DT. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: individual participant data meta-analysis. BMJ. 2019;365:11476. doi:10.1136/bmj.l1476
24. Little RJ. Missing Data Analysis. Annual Rev Clin Psychol. 2024;20(1):149–173. doi:10.1146/annurev-clinpsy-080822-051727
25. Duffy FF, Chung H, Rivedi M, et al. Systematic use of patient-rated depression severity monitoring: is it helpful and feasible in clinical psychiatry? Psychiatric Serv. 2008;59(10):1148–1154. doi:10.1176/ps.2008.59.10.1148
26. Chen H, Cui H, Geng Y, et al. Development of a nomogram prediction model for depression in patients with systemic lupus erythematosus. Front Psychol. 2022;13:951431. doi:10.3389/fpsyg.2022.951431
27. Chen N, Xia H, Pan Y, et al. Development and validation of a nomogram for predicting depression risk in older adults with cognitive impairment. J Affective Disturbance. 2025;390:119766. doi:10.1016/j.jad.2025.119766
28. Barry MJ, Nicholson WK, Silverstein M, et al. Screening for depression and suicide risk in adults: US preventive services task force recommendation statement. JAMA. 2023;329(23):2057–2067. doi:10.1001/jama.2023.9297
29. Loh HH, Lim LL, Yee A, et al. Association between subclinical hypothyroidism and depression: an updated systematic review and meta-analysis. BMC Psychiatry. 2019;19(1):12. doi:10.1186/s12888-018-2006-2
30. Yoon S, Kim YK. Endocrinological treatment targets for depressive disturbance. Adv Exp Med Biol. 2024;1456:3–25. doi:10.1007/978-981-97-4402-2_1
31. Siu AL, Preventive S. Bibbinsdomingo K.Screening for depression in adults:us preventive services task force recommendation statement. JAMA. 2016;315(4):380–387. doi:10.1001/jama.2015.18392
32. Philippe T. Depression in the elderly and the environment. Soins Gerontologie. 2022;27(158):27–29. doi:10.1016/j.sger.2022.10.008
33. Thomas TS, Patrick CS, Coen DS. Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers and risk of depression among older people with hypertension. J Psychopharmacol. 2020;36(5):594–603. doi:10.1177/02698811221082470
34. Lefevre ML, Preventive ST. Force U.S. Screening for suicide risk in adolescents, adults, and older adults in primary care:U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160(10):719–726. doi:10.7326/M14-0589
35. Luppa M, Sikorski C, Luck T. Age- and gender-specific prevalence of depression in latest-life--systematic review and meta-analysis. J Affective Disturbance. 2012;136(3):212–221. doi:10.1016/j.jad.2010.11.033
36. Albert R. Why is depression more prevalent in women? J Psychiatry Neurosci. 2015;40(4):219–221. doi:10.1503/jpn.150205
37. Ma L, Xu Y, Wang G. What do we know about sex differences in depression:a review of animal models and potential mechanisms. Prog Neuropsychopharmacol Biol Psychiat. 2019;89:48–56. doi:10.1016/j.pnpbp.2018.08.026
38. Qiu WQ, Li J, Li JL, Xu Y. Built form and depression among the Chinese rural elderly: a cross-sectional study. BMJ Open. 2020;10(12):e038572. doi:10.1136/bmjopen-2020-038572
39. Lin HY, Jin MD, Liu D, et al. Gender-specific prevalence and influencing factors of depression in elderly in rural China: a cross-sectional study. J Affective Disturbance. 2021;288:99–106. doi:10.1016/j.jad.2021.03.078
40. Pan L, Li L, Peng HY. Association of depressive symptoms with marital status among the middle-aged and elderly in Rural China-Serial mediating effects of sleep time, pain and life satisfaction. J Affective Disturbance. 2022;303:52–57. doi:10.1016/j.jad.2022.01.111
41. Susan LB, Fen L, Alyssa V. Midlife marital dissolution and the onset of cognitive impairment. Gerontologist. 2021;61(7):1085–1094. doi:10.1093/geront/gnaa193
42. Zhao LY, Zhang K, Gao Y. The relationship between gender, marital status and depression among Chinese middle-aged and older people: mediation by subjective well-being and moderation by degree of digitization. Front Psychol. 2022;13:923597. doi:10.3389/fpsyg.2022.923597
43. Liu H, Zhang Y, Burgard SA. Marital status and cognitive impairment in the United States: evidence from the National Health and Aging Trends Study. Ann Epidemiol. 2019;38:28–34,e2. doi:10.1016/j.annepidem.2019.08.007
44. Atsushi N, Koichiro S, Masamichi H. Does community-level social capital mitigate the impact of widowhood & living alone on depressive symptoms? A prospective, multi-level study. Soc Sci Med. 2020;259:113140. doi:10.1016/j.socscimed.2020.113140
45. Ansari S, Muhammad T, Dhar M. How does multi-morbidity relate to feeling of loneliness among older adults? Evidence from a population-based survey in India. J Popul Ageing. 2021;3(16):45–66. doi:10.1007/s12062-021-09343-5
46. ShobhitS S, Himanshu C. Feeling about living arrangements and associated health outcomes among older adults in India: a cross-sectional study. BMC Public Health. 2021;21(1):1322. doi:10.1186/s12889-021-11342-2
47. Cheng C, Bai J. Association between polypharmacy, anxiety, and depression among Chinese older adults: evidence from the Chinese longitudinal healthy longevity survey. Clin Interventions Aging. 2022;17:235–244. doi:10.2147/CIA.S351731
48. Maria AM. Marital status and trajectories of depressive symptoms among older adults of Mexican descent. Int J Aging Human Develop. 2019;88(1):22–45. doi:10.1177/0091415017752940
49. Beate EM, Markus WB. Understanding the interplay of sleep and aging: methodological challenges. Psychophysiology. 2020;57(3):e13523. doi:10.1111/psyp.13523
50. Wu CR, Chen PY, Hsieh SH, et al. Sleep mediates the relationship between depression and cognitive impairment in older men. Am J Men’s Health. 2019;13(1):1557988319825765. doi:10.1177/1557988319825765
51. Martino FP, Sogol J, Manuel ST. What cardiologists should know about sleep. Eur Heart J. 2022;43(31):2911–2913. doi:10.1093/eurheartj/ehac349
52. Miner B. Kryger MH.Sleep in the aging population. Sleep Med Clin. 2020;15(2):311–318. doi:10.1016/j.jsmc.2020.02.016
53. Dao TH, Seib C. Prevalence and correlates of sleep disturbance among older women in Vietnam. J Clin Nurs. 2018;27(17–18):3307–3313. doi:10.1111/jocn.14080
54. Jaqua EE, Hanna M, Labib W, Moore C, Matossian V. Common sleep disturbance affecting older adults. Permanente J. 2023;27(1):122–132. doi:10.7812/TPP/22.114
55. Ganidagli S, Ozturk E, Ozturk ZA. Risk factors of poor sleep quality in older adults:an analysis based on comprehensive geriatric assessment. Curr Med Res Opin. 2023;39(5):701–706. doi:10.1080/03007995.2023.2192124
56. Behrens A, Anderberg P, Berglund JS. Sleep disturbance predicts worse cognitive performance in subsequent years: a longitudinal population-based cohort study. Arch Gerontol Geriatr. 2023;106:104899. doi:10.1016/j.archger.2022.104899
57. Pigeon WR, Hegel M, Unüitzer J. Is insomnia a perpetuating factor forlate-life depression in the IMPACT cohort? Sleep. 2008;31:481–488. doi:10.1093/sleep/31.4.481
58. Leblanc MF, Desjardins S, Desgagné A. Sleep cognition associated with anxiety and depression in the elderly. Clin Interventions Aging. 2015;10:575–582. doi:10.2147/CIA.S77384
59. Huang MN, Liu K, Liang CG. The relationship between living alone or not and depressive symptoms in older adults: a parallel mediation effect of sleep quality and anxiety. BMC Geriatr. 2023;23(1):506. doi:10.1186/s12877-023-04161-0
60. Trezise A, Mclaren S, Gomez R. Resiliency among older adults: dispositional hope as a protective factor in the insomnia-depressive symptoms relation. Aging Mental Health. 2018;22(8):1088–1096. doi:10.1080/13607863.2017.1334191
61. Mirchandaney R, Barete R, Asarnow LD. Moderators of cognitive behavioral treatment for insomnia on depression and anxiety outcomes. Curr Psychiat Rep. 2022;24(2):121–128. doi:10.1007/s11920-022-01326-3
62. Zhang Y, Yu G, Bai W. Association of depression and sleep quality with frailty: a cross-sectional study in China. Front Public Health. 2024;12(4):1361745. doi:10.3389/fpubh.2024.1361745
63. Cho HJ, Lavretsky H, Olmstead R. Sleep disturbance and depression recurrence in community-dwelling older adults:a prospective study. Am J Psychiatry. 2008;165:1543–1550. doi:10.1176/appi.ajp.2008.07121882
64. Yaremchuk K. Sleep disturbance in the elderly. Clin Geriatric Med. 2018;34(2):205–216. doi:10.1016/j.cger.2018.01.008
65. Khurshid KA. Comorbid insomnia and psychiatric disturbance: an update. Innovat Clin Neurosci. 2018;15(3–4):28–32. PMID:29707424.
66. Xie H, Jiang Y, Liu L, Peng H, Li J, Chen Z. Global prevalence and risk factors of depression in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis from 2000 to 2022. J Psychosom Res. 2023;175:111537. doi:10.1016/j.jpsychores.2023.111537
67. Charles C, Bardet A, Larive A, et al. Characterization of depressive symptoms trajectories after breast cancer diagnosis in women in France. JAMA Network Open. 2022;5:e225118. doi:10.1001/jamanetworkopen.2022.5118
68. Liu L, Li X, Marshall LJ, Bhalla A, Wang Y, O’Connell MD. Trajectories of depressive symptoms 10 years after stroke and associated risk factors: a prospective cohort study. Lancet. 2023;402(1):S64.
69. Lu X, Liu C, Lu H, et al. Eight-year total, cognitive affective, and somatic depressive symptoms trajectories and risks of cardiac events. Transl Psychiatry. 2024;14:356. doi:10.1038/s41398-024-03063-y
70. Triolo F, Vetrano DL, Sjöberg L, et al. Somatic disease burden and depression risk in late life: a community-based study. Epidemiol Psychiatr Sci. 2024;33e6. doi:10.1017/S2045796024000064
71. Zhou P, Wang S, Yan Y, et al. Association between chronic diseases and depression in the middle-aged and older adult Chinese population-a seven-year follow-up study based onCHARLS. Front Public Health. 2023;11:1176669. doi:10.3389/fpubh.2023.1176669
72. Guo C, Zheng X. Health challenges and opportunities for an aging China. Am J Public Health. 2018;108:890–892. doi:10.2105/AJPH.2018.304444
73. Khera R, Valero EJ, Nasir K. Financial toxicity in atherosclerotic cardiovascular disease in the United States:Current stateand future directions. J Am Heart Assoc. 2020;9:e017793. doi:10.1161/JAHA.120.017793
74. Yan R, Hu YZ, Yang JX. Depressive symptoms and chronic disease trajectories and predictors in middle-aged and older adults in China: an eight-year multi-trajectory analysis. Global Health Med. 2025;7(3):241–251. doi:10.35772/ghm.2025.01061
75. Sibel E, Yeşim GK, Fusun T. Polypharmacy,physical and nutritional status, and depression in the elderly: do polypharmacy deserve some credits in these problems? Experi Aging Res. 2020;47(1):79–91. doi:10.1080/0361073X.2020.1846949
76. Maina JG, Balkhiyarova Z, Nouwen A, Pupko I, Ulrich A, Boissel M. Bidirectional mendelian randomization and multiphenotype was show causality and shared pathophysiology between depression and type 2 diabetes. Diabetes Care. 2023;46:1707–1714. doi:10.2337/dc22-2373
77. Bowen L, Siyu G, Chuan H. Depression severity and chronic disease risk: interactive effects on cognitive function and life satisfaction in Chinese middle-aged and older adults. Front Public Health. 2025;13:1530513. doi:10.3389/fpubh.2025.1530513
78. Tang T, Jiang J, Tang X. Prevalence of depressive symptoms among older adults in mainland China: a systematic review and meta-analysis. J Affective Disturbance. 2021;293:379–390. doi:10.1016/j.jad.2021.06.050
79. Li BW, Guan SY, Huang C, Li C, Du YR, Wan CX. Depression severity and chronic disease risk: interactive effects on cognitive function and life satisfaction in Chinese middle-aged and older adults. Front Public Health. 2025;13:1530513. doi:10.3389/fpubh.2025.1530513
80. Dudek KA, Dion AL, Lebel M, Le CK, Labrecque S, Tuck E. Molecular adaptations of the blood-brainbarrier promote stress resilience vs.depression. Proc Natl Acad Sci US. 2020;117:3326–3336.
81. Wang XJ, Wu YJ, Zheng DZ. Specific types of depressive symptoms trajectories and risk of chronic lung diseases events in middle-aged and older adults: result from two prospective cohort studies. J Affect Disturbance. 2025;388:119588. doi:10.1016/j.jad.2025.119588
82. Wu XH, Huang RY, Fei Y, et al. Body pain and depressive symptoms: patterns and associations in middle-aged and older chinese adults. Depression Anxiety. 2025:4027080. doi:10.1155/da/4027080
83. Li D, Su M, Guo X, Liu B, Zhang T. The association between chronic disease and depression in middle-aged and elderly people: the moderating effect of health insurance and health service quality. Front Public Health. 2023;11:935969. doi:10.3389/fpubh.2023.935969
84. Zhou Y, Huang YJ, Zhang AH. Determinants of self-rated health among elderly patients with hypertension: a cross-sectional analysis based on the Chinese longitudinal healthy longevity survey. Ann Clin Exp Hypertens. 2023;45(1):2224942. doi:10.1080/10641963.2023.2224942
85. Zhang HG, Wang JF, Anfeirea J. Relationship between multimorbidity burden and depressive symptoms in older Chinese adults: a prospective 10-year cohort study. J Affective Disturbance. 2025;119714. doi:10.1016/j.jad.2025.119714
86. Ostojic P, Zivojinovic S, Reza T. Symptoms of depression and anxiety in Serbian patients with systemic sclerosis: impact of disease severity and socioeconomic factors. Modern Rheumatol. 2010;20(4):353–357. doi:10.1007/s10165-010-0285-7
87. He G, Xie J, Zhou J. Depression in left-behind elderly in rural China: prevalence and associated factors. Geriatrics Gerontol Int. 2016;16(5):638–643. doi:10.1111/ggi.12518
88. Kawada T. Associations between symptoms of pain, insomnia and depression, and frailty in older adults: comment on Liu et al. (2021). Int J Nurs Studies. 2021;123:104068. doi:10.1016/j.ijnurstu.2021.104068
89. Senthil RM, Senthil RM, Arushi K, Shahrzad M, Joel ES. Impact of pain interference on treatment outcomes among older adults with depressive and anxiety symptoms receiving collaborative mental health care.The. Am J Geriatric Psychiatry. 2020;28:4S,S94–S95. doi:10.1016/j.jagp.2020.01.120
90. Shen SS, Zeng XK, Yang YH. Associations of poor sleep quality, chronic pain and depressive symptoms with frailty in older patients: is there a sex difference? BMC Geriatr. 2022;22(1):862. doi:10.1186/s12877-022-03572-9
91. Shen PS, Zhao Z, Guo RR, et al. The impacts of low back pain and sleep duration on the long-term change in depressive symptoms among middle-aged and older Chinese adults. J Affective Disturbance. 2025;386:119476. doi:10.1016/j.jad.2025.119476
92. Liu MH, Hou TX, Nkimbeng M, et al. Associations between symptoms of pain, insomnia and depression, and frailty in older adults: a cross-sectional analysis of a cohort study. Int J Nurs Studies. 2021;117:103873. doi:10.1016/j.ijnurstu.2021.10387
93. Başcıllar M, Karakaya C. Subjective health complaints and life satisfaction in older adults: the predictive role of geriatric depression. Psychogeriatrics. 2025;25(1):e13230. doi:10.1111/psyg.13230
94. Fan X, Guo X, Ren Z. The prevalence of depressive symptoms and associated factors in middle-aged and elderly Chinese people. J Affective Disturbance. 2021;293:222–228. doi:10.1016/j.jad.2021.06.044
95. Feng WJ, Geng PX, Ge HJ. The influence of intergenerational relationships on depressive symptoms in elderly patients with multiple chronic conditions: the mediating roles of self-rated health and well-being. BMC Public Health. 2025;25(1):1478. doi:10.1186/s12889-025-22759-4
96. Su D, Wu XN, Zhang YX. Depression and social support between China’ rural and urban empty-nest elderly. Arch Gerontol Geriatrics. 2012;55(3):564–569. doi:10.1016/j.archger.2012.06.006
97. Fortin M, LapointeL HC. Multimorbidity and quality of life in primary care: a systematic review. Health Qual Life Outcomes. 2004;2:51. doi:10.1186/1477-7525-2-51
98. Mavaddat N, Kinmonth AL, Sanderson S, Surtees P, Bingham S, Khaw KT. What determines Self-Rated health (SRH)? A cross-sectional study of SF-36 health domains in the EPIC-Norfolk cohort. J Epidemiol Commun Health. 2011;65(9):800–806. doi:10.1136/jech.2009.090845
99. Bayliss EA, Steiner JF, Fernald DH, Crane LA, Main DS. Descriptions of barriers to self-care by persons with comorbid chronic diseases. Ann Fam Med. 2003;1(1):15–21. doi:10.1370/afm.4
100. Mavaddat N, Valderas JM, VanderLinde R, Khaw KT, Kinmonth AL. Association of self-rated health with multimorbidity, chronic disease and psychosocial factors in a large middle-aged and older cohort from general practice: a cross-sectional study. BMC Fam Pract. 2014;15:185.
101. Xu Q, Li H, Zhang Y. The impact of inter generational support on the mental health of the elderly: evidence from China. Int J Environ Res Public Health. 2017;14(8):882.
102. Chang QH, Xue MZ, Bi RD, Zhen CL, Ji RY, Qing XL. Health status and risk for depression among the elderly: a meta-analysis of published literature. Age Ageing. 2010;39(1):23–30.
103. Benyamini Y. Why does self-rated health predict mortality? An update on current knowledge and a research agenda for psychologists. Psychol Health. 2011;26(11):1407–1413. doi:10.1080/08870446.2011.621703
104. Steptoe A, Deaton A, Stone AA. Subjective well being, health, and ageing. Lancet. 2015;385(9968):640–648. doi:10.1016/S0140-6736(13)61489-0
105. Song KY, Chang YW, Zhao ZJ, Govindasamyl K. Leisure activities, self-reported health, anxiety, and depression in Chinese older adults: a structural equation model analysis. Front Public Health. 2025;13:1459236. doi:10.3389/fpubh.2025.1459236
106. Murri MB, Sciavicco G, Specchia M, et al. Risk prediction models for depression in older adults with cancer. BMC Psychiatry. 2025;25(1):1106. doi:10.1186/s12888-025-07578-6
107. Mony N, Shimul MH, Pantho SA, et al. Proportion and predictors of postoperative depression among elderly urology patients in Bangladesh. Discover Mental Health. 2025;5(1):175. doi:10.1007/s44192-025-00316-0
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Analysis of Risk Factors and Development of a Predictive Model for Prognosis in Early-Stage Rectal Cancer Patients
Zhang CT
International Journal of General Medicine 2025, 18:3961-3968
Published Date: 16 July 2025