Back to Journals » International Journal of General Medicine » Volume 18
Development and Validation of a Risk Prediction Model for New-Onset Atrial Fibrillation in Sepsis
Authors Chai YG, Gou Y ![]() , Cong Y, Li DD, Yang JZ, Peng P
, Cong Y, Li DD, Yang JZ, Peng P
Received 3 October 2025
Accepted for publication 9 December 2025
Published 11 December 2025 Volume 2025:18 Pages 7471—7482
DOI https://doi.org/10.2147/IJGM.S567490
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Ya-Ge Chai,1 Yi Gou,1 Yun Cong,2 Dan-Dan Li,1 Jian-Zhong Yang,1 Peng Peng1
1Emergency Trauma Center, The First Affiliated Hospital of Xinjiang Medical University, Urumqi, People’s Republic of China; 2Surgery for Hepatic and Biliary Echinococcosi, The First Affiliated Hospital of Xinjiang Medical University, Urumqi, People’s Republic of China
Correspondence: Peng Peng; Jian-Zhong Yang, Email [email protected]; [email protected]
Background: Sepsis patients face a high risk of new-onset atrial fibrillation (NOAF), which increases mortality. Thus, it is significant to construct a risk prediction model for early risk stratification.
Objective: To construct and validate a risk prediction model for NOAF in sepsis.
Methods: A total of 423 sepsis patients were randomly divided into training (n=299) and validation (n=124) cohorts. Predictors were selected using least absolute shrinkage and selection operator (LASSO) regression, and independent risk factors were identified by multivariate logistic regression to construct a nomogram. Model performance was assessed by the area under the receiver operating characteristic curve (AUC), Hosmer–Lemeshow test, and calibration curves. Clinical utility was evaluated using decision curve analysis (DCA) and clinical impact curves (CIC).
Results: Log interleukin-6 (Log IL-6), blood urea nitrogen (BUN), and heart rate (HR) were identified as independent risk factors for NOAF. The nomogram demonstrated strong discriminative ability, with AUCs of 0.925 in the training cohort and 0.866 in the validation cohort. Calibration was good in both cohorts, and DCA and CIC indicated favorable clinical utility across a range of threshold probabilities.
Conclusion: A risk prediction model incorporating Log IL-6, BUN, and HR effectively could predict NOAF in sepsis patients, with good discrimination, calibration, and potential clinical applicability for early risk identification. However, prior to further clinical application, additional multicenter, prospective studies are required for external validation.
Keywords: new-onset atrial fibrillation, sepsis, prediction model
Introduction
Atrial fibrillation is the most common clinical arrhythmia, affecting more than 30 million people worldwide.1 NOAF refers to AF occurring in patients with no previous history of AF.2 NOAF is a common complication in patients with acute and critical illnesses.2,3 Sepsis, a common acute critical illness, is defined as a life-threatening organ dysfunction caused by a dysregulated host immune response to infection.4 Sepsis patients are prone to AF.5,6 It is reported that the incidence rate ranges from 7.2% to 42%.1,7–10 Compared with sepsis patients without NOAF, the risk of ischemic stroke, heart failure and death is significantly higher than those with NOAF.3,11–13 Screening high-risk patients as early as possible, with the aim of achieving early identification, early prevention, and early intervention, is crucial for reducing the incidence and mortality of NOAF. Previous studies have found that advanced age, hypotension, heart failure, coronary heart disease, and mechanical ventilation (MV) are independent risk factors for NOAF in sepsis.1,7,10 However, risk factor analysis cannot visually calculate the specific probability of disease occurrence. Additionally, these studies have primarily included sepsis patients admitted to the intensive care unit (ICU). Most sepsis patients first present to the emergency department; achieving early identification and diagnosis of NOAF in the emergency department enables earlier intervention, thereby improving patients’ prognosis to the greatest extent. In the busy clinical practice, emergency physicians need a simple and efficient tool to identify patients at high risk of NOAF among a large number of patients. However, risk factor analysis cannot simply and intuitively calculate the probability of NOAF occurrence. By selecting independent risk factors and developing a nomogram, the risk prediction model can screen high-risk patients in a simple, intuitive, and visualized manner, and provide clinicians with individualized risk assessments. Therefore, this study retrospectively analyzed the clinical data of sepsis patients in the emergency rescue area. By establishing a nomogram, it visualized the probability of NOAF, aiming to provide clinical evidence for the early identification and early diagnosis of NOAF in septic patients in the emergency department.
Method
Patients
The study was conducted in accordance with the 1964 Declaration of Helsinki and its subsequent amendments, and was approved by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University (K202412-69). Because this study was retrospective, informed consent was waived by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University. To protect patient privacy, all personally identifiable information was deidentified, ensuring that data were used exclusively by the research team in anonymized form.
Inclusion criteria: 1) Age ≥ 18 years; 2) Diagnosis of sepsis, based on the sepsis-3 diagnostic criteria;4 3) Hospitalization duration > 24 hours. Exclusion criteria were as follows: 1) Past medical history of malignant tumor; 2) Past medical history of AF; 3) Incomplete data. The diagnostic criteria for atrial fibrillation are determined by an electrocardiogram report and the hourly rhythm record in the nursing record.14 NOAF was defined as:15 1) no history of AF; 2) AF lasting more than 1 h; or 3) paroxysmal AF or atrial flutter intervened with pharmacological treatment or electrical cardioversion. We included 520 sepsis patients admitted to the Emergency Resuscitation Area of the First Affiliated Hospital of Xinjiang Medical University from September 2022 to December 2024. A total of 97 patients were excluded according to the exclusion criteria. Finally, a retrospective analysis was performed on the clinical data of 423 sepsis patients. These patients were randomly assigned to the training cohort or validation cohort at a ratio of 7:3, resulting in 299 patients in the training cohort and 124 in the validation cohort. A flowchart of patient enrollment is shown in Figure 1.
 |
Figure 1 Flow diagram of study design. |
Data Collection
Comprehensive clinical data were obtained on the first day of admission to emergency resuscitation area, which included: Age, gender, sequential organ failure assessment (SOFA), acute physiology and chronic health evaluation II (APACHE-II), glasgow coma scale (GCS), comorbidities, infection site, MV, temperature, mean arterial pressure (MAP), HR, respiratory rate, blood gas analysis indicators, blood electrolytes, complete blood count, coagulation indicators, myocardial enzymes, inflammatory markers, and cardiac function indicators, etc. Since the levels of IL-6 vary by thousands of folds among patients, we performed logarithmic transformation to reduce the impact of extreme values and improve the applicability of subsequent statistical analyses and the reliability of the results. First, LASSO regression was used to screen for predictive variables. Then, multivariate logistic regression analyses were performed to identify the independent risk factors for AF. Subsequently, a nomogram was constructed using these independent risk factors. The ROC curve was used to evaluate the discriminative ability of the model, the Hosmer-Lemeshow tests and calibration curve were used to assess degree of calibration, and DCA and CIC were used to evaluate clinical applicability.
Statistical Analyses
Data analyses were performed using R software (version 4.5.1). Quantitative data were expressed as mean ± standard deviation or median (interquartile range, 25th–75th percentiles). For normally distributed quantitative data, comparisons between two groups were performed using the t-test; for non-normally distributed data, intergroup comparisons were performed using the Mann–Whitney U-test. Categorical data were presented as n (%), and intergroup comparisons were made using the χ2-test. To prevent overfitting, LASSO regression was employed to select optimal features. LASSO feature selection was performed using the “corrplot” and “glmnet” package. Multivariate logistic regression analyses were performed using the “glm” package. Nomograms were plotted using the “regplot” package. ROC curve plotting and AUC calculation were performed using the “pROC” package. Hosmer-Lemeshow tests and calibration plots were generated using the “rms” package. DCAs were performed using the “rmda” package. CICs were plotted using the “ggplot2” package.
Results
Of the 426 sepsis, 137 had AF and 286 did not. The clinical characteristics of patients in the two groups are presented in Table 1 and Table 2. These patients were randomly assigned to the training cohort or validation cohort at a ratio of 7:3, resulting in 299 patients in the training cohort and 124 in the validation cohort. No significant differences were observed in age, male, SOFA, APACHE-II, GCS, infection site, and MV between the training and validation cohorts, indicating that the two cohorts were comparable (Supplementary Table 1).
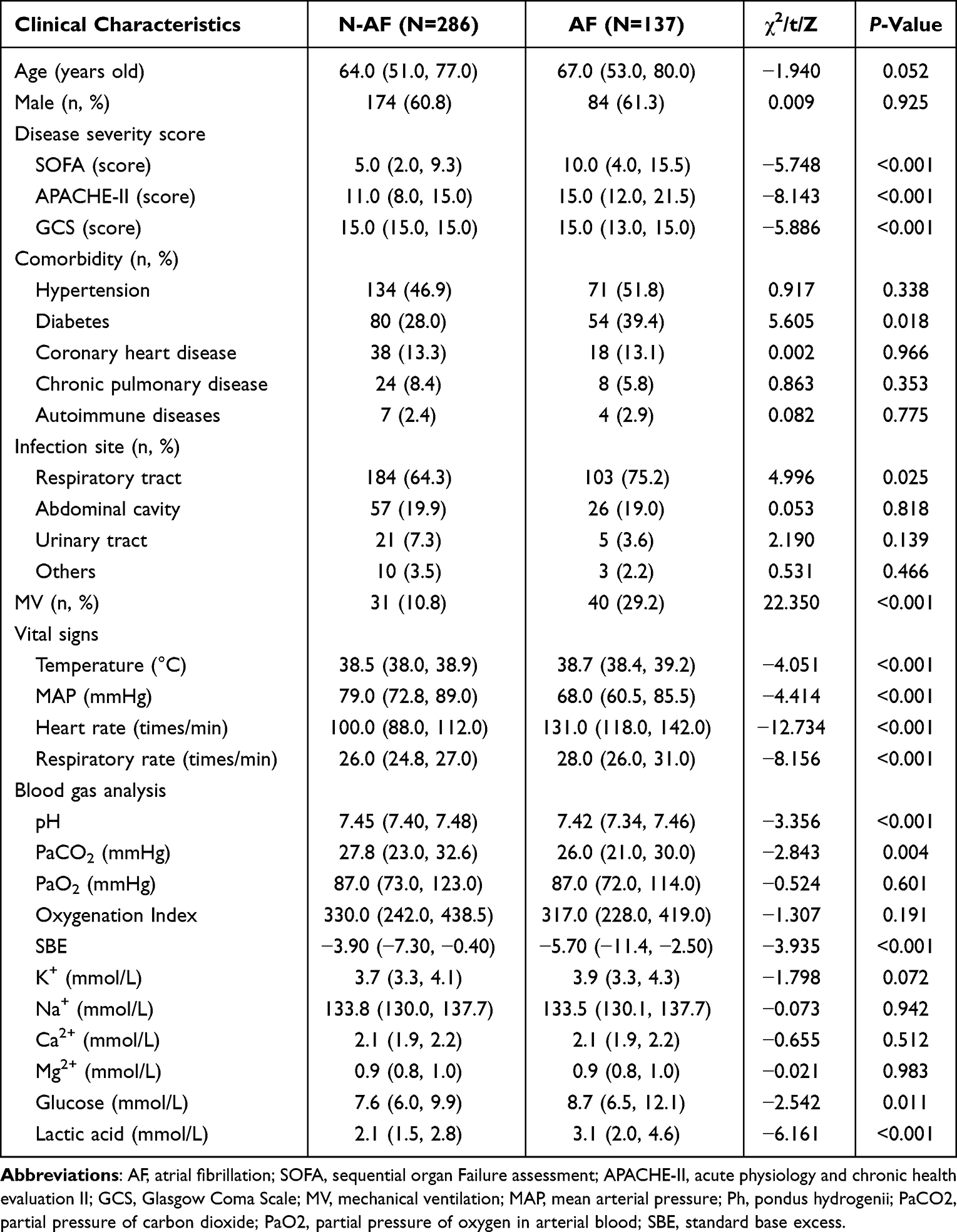 |
Table 1 A Comparison of the Clinical Characteristics of N-AF and AF Groups |
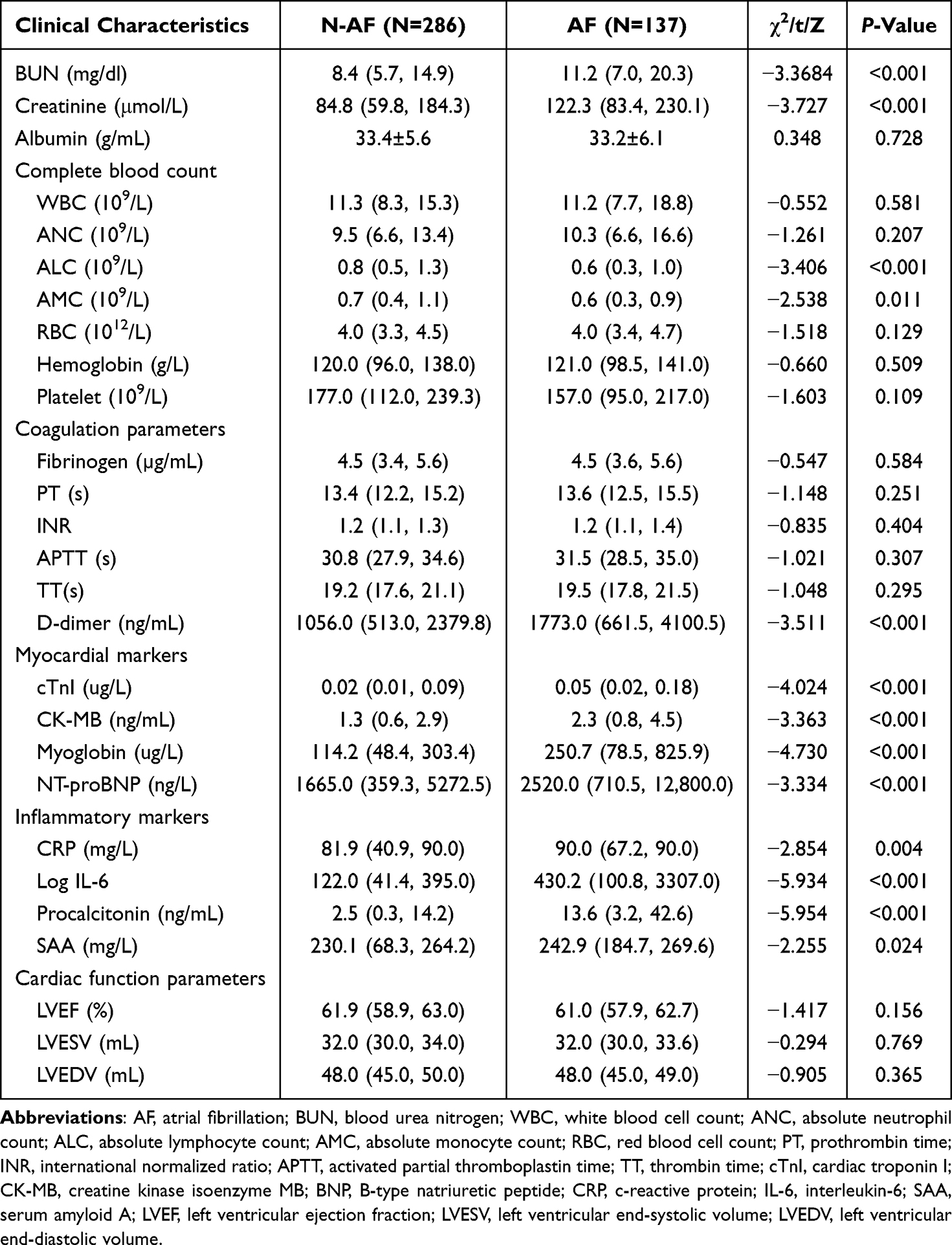 |
Table 2 A Comparison of the Auxiliary Examinations of N-AF and AF Groups |
Independent Risk Factors in the Training Cohort
We used LASSO regression to eliminate redundant variables and reduce the risks of collinearity and overfitting. In the training cohort, LASSO regression analysis was performed with cross-validation, and 5 variables with non-zero coefficients (HR, SOFA, BUN, AMC, and Log IL-6) were selected based on optimal λ and 1 standard error (Figure 2A and B). In our training cohort (n=299), the number of patients with the outcome event (NOAF) was 91, and 5 predictive parameters were retained in the final LASSO model. This results in an events per variable of 18.2 (91/5), which meets the widely accepted minimum threshold of 10–20 events per variable. Through multivariate logistic regression analyses, we determined that HR, BUN, and Log IL-6 were independent risk factors for NF (Table 3).
 |
Table 3 Results of the Multivariate Logistic Regression Analysis Using the Training Cohort |
 |
Figure 2 Variable selection for the LASSO regression model. (A) Coefficient profile plot was constructed based on the log(λ) sequence. (B) By deriving the optimal lambda, 5 variables with non-zero coefficients were selected. After validating the optimal λ in the LASSO model, we plotted the partial likelihood deviance (binomial deviance) curve against log(lambda), with dashed vertical lines drawn according to the 1-standard error criterion. |
Development of NF‑Predicting Nomogram
Based on the results of multivariable logistic regression analysis, a nomogram was constructed to predict the risk of NF (Figure 3).
 |
Figure 3 Independent risk factors-HR, BUN, and Log IL-6 for nomogram prediction model. Annotation: The red circle in the figure indicates the scoring process for an example patient: Draw a vertical line downward from the first red dot on the “Points” axis to intersect with the red dot on the “BUN” axis, indicating that when BUN = 5, the Points is −0.43; Draw a vertical line downward from the second red dot on the “Points” axis to intersect with the red dot on the “Log IL-6” axis, indicating that when Log IL-6 = 0.47, the corresponding Points is 1.56; Draw a vertical line downward from the third red dot on the “Points” axis to intersect with the red dot on the “HR” axis, indicating that when HR = 131.25, the corresponding points is 2.06; Sum up the points of the three variables: the Total points = 3.19. Draw a vertical line downward from the total points to intersect with the “Risk of atrial fibrillation” axis, showing that a total points of 3.19 corresponds to a predicted risk of atrial fibrillation of 81.11%. |
Evaluation and Validation of Nomogram
Discrimination Ability
The ROC curve was used to evaluate the discriminative ability of the predictive model. The AUC of the nomogram was 0.925 in the training cohort (Figure 4A) and 0.866 in the validation cohort (Figure 4B), indicating excellent performance.
 |
Figure 4 ROC of the NF risk nomogram prediction. (A) The blue line represents the performance of the nomogram in the training cohort. (B) The red line represents the performance of the nomogram in the validation cohort. |
Calibration Ability
A calibration curve and Hosmer–Lemeshow test were used to assess the calibration of the predictive model. From the calibration curves, the model showed a good fit in both the training and validation cohorts. As shown by the Hosmer–Lemeshow test, the predicted and actual probabilities were highly consistent (Figure 5A and B).
 |
Figure 5 Calibration curve of risk of AF. The y-axis represents actual diagnosed cases of AF, the x-axis represents the predicted risk of AF. (A) training cohort; (B) validation cohort. |
Clinical Usefulness
DCA showed that in the training cohort, if the threshold probability was within the range of 3%–97%, using this nomogram to predict the risk of NF could yield a net benefit (Figure 6A); in the validation cohort, the threshold probability range for net benefit was 2%–75% (Figure 6B). As indicated by the CIC, in the training cohort, when the threshold probability was 40%–79% (Figure 6C), the number of high-risk individuals predicted by this nomogram was close to the number of actual cases; in the validation cohort, this threshold probability was 55%–87% (Figure 6D). Taken together, the DCA and CIC results indicate that this model has good clinical applicability.
 |
Figure 6 DCA curves and CIC of the nomogram prediction model for the risk of AF in sepsis patients. (A) DCA curves for training cohort; (B) DCA curves for validation cohort; (C) CIC for training cohort; (D) CIC for validation cohort. Notes: For (A) and (B) (DCA): This yellow line marks a critical threshold where the nomogram yields net benefit (within 3%–97% range in training cohort and within 2%–75% range in validation cohort); For (C) and (D) (CIC): This yellow line marks a critical threshold where the number of predicted high-risk individuals is close to the number of actual cases (within 40%–79% range in training cohort and within 55%–87% range in validation cohort). |
Discussion
Studies have shown that sepsis is a risk factor for AF, and that the occurrence of AF in sepsis patients significantly increases the length of hospital stay, mortality rate, and incidence of stroke.2,11,13,16 Thus, early identification of high-risk populations for NOAF in sepsis is a key focus for emergency and critical care physicians. Although risk factors for NOAF in sepsis-such as advanced age, organ dysfunction, obesity, and heart rate-have been identified,16,17 relying solely on risk factor analysis cannot conveniently or quickly calculate the specific probability of AF occurrence. In contrast, predictive models integrate multiple variables to estimate the probability of an outcome more comprehensively and efficiently. In this study, LASSO regression identified HR, SOFA score, BUN, AMC, and Log IL-6 as potential predictors for NOAF in sepsis. These were subsequently incorporated into a multivariate logistic regression, which ultimately established a final model based on HR, BUN, and Log IL-6. The evaluation demonstrated that this model possesses good discriminative ability, calibration, and clinical utility, indicating its value for the accurate risk stratification of NOAF in septic patients.
Notably, the variables integrated into our nomogram encompass distinct categories: an inflammatory marker (IL-6), a biochemical parameter (BUN), and a vital sign (HR). This diversity enhances the model’s clinical utility, as these routinely available tests facilitate implementation even in resource-limited settings. Furthermore, this specific combination of indicators may reflect the pathophysiological process of NOAF: IL-6 potentially acts as an initial driver, promoting changes in physiological markers like BUN; these subsequent alterations in organ function may then manifest as heart rate instability, ultimately culminating in the onset of NOAF. Similarly, Yu et al18 reported a model combining IL-6, BUN, and MAP for sepsis prediction (AUC: 0.848). Together, these findings suggest that clinicians should extend the application of such biomarkers beyond assessing severity and prognosis to include the proactive prediction of complications. While Akash Batta et al19 have extensively explored the bidirectional relationship between coronary artery disease (CAD) and AF—where CAD promotes AF through ischemia-induced electrical remodeling, and AF, in turn, accelerates atherosclerosis and thrombus formation20,21—our study did not identify CAD as an independent risk factor for NOAF in sepsis. Nevertheless, their work underscores the critical role of ischemia and endothelial dysfunction in AF pathogenesis. This mechanism is highly relevant to sepsis, wherein systemic hypoperfusion, inflammatory cytokine storms, and widespread endothelial injury collectively create a substrate that markedly increases the risk of NOAF. Inflammation is central to the pathogenesis of NOAF, where pro-inflammatory cytokines like IL-6 instigate a cytokine storm. This cascade promotes atrial fibrosis and electrophysiological alterations, ultimately destabilizing the heart’s electrical activity.22
IL-6 is a pleiotropic cytokine central to regulating inflammatory, immune, and hematopoietic processes. Upon its release from local inflammatory sites into the circulation, it stimulates the hepatic production of acute-phase proteins (eg, CRP, SAA, fibrinogen).23 It is precisely this pivotal role in orchestrating systemic inflammation that positions IL-6 as a primary driver of the immune dysregulation underlying sepsis.24 Elevated IL-6 levels are an established risk factor for poor prognosis in sepsis,25,26 and its specific link to AF is increasingly recognized. A multicenter analysis by Li et al14 demonstrated that the IL-6-induced acute-phase proteins CRP and fibrinogen are risk factors for NOAF in sepsis; a model incorporating these markers showed high predictive accuracy (AUC: 0.861 training, 0.845 validation). Consistently, Bai et al27 reported significantly higher serum IL-6 concentrations in AF patients. Complementing these clinical findings, experimental evidence from Keefe et al28 revealed that macrophage-specific deletion of the IL-6 receptor prevented postoperative AF in mice, directly implicating IL-6 signaling in AF pathogenesis. Our previous studies in septic mice with AF revealed an upregulation of sphingosine-1-phosphate receptor 2 (S1PR2), an upstream regulator of IL-6. Critically, inhibiting S1PR2 with JTE-013 significantly reduced AF incidence.29 In conclusion, IL-6 is strongly and closely associated with NOAF in sepsis. Clinically, a sharp rise in IL-6 should alert physicians to an increased risk of NOAF. Furthermore, as over 90% of BUN is renally excreted, its elevation in our model likely reflects sepsis-associated renal dysfunction, which may contribute to AF susceptibility through electrolyte and metabolic disturbances.
BUN is a routine clinical biomarker primarily used to assess renal function, with additional utility in evaluating systemic conditions. Its prognostic value in sepsis is well-established. For instance, BUN has been identified as an independent risk factor for both the presence and severity of neonatal sepsis,30 a predictor of sepsis in patients with acute pancreatitis,31 and a key indicator in models predicting sepsis in pyogenic liver abscess.32 Furthermore, BUN contributes to outcome prediction, as demonstrated by its role in forecasting 28-day mortality in sepsis-induced liver injury based on machine learning.33 Beyond overall prognosis, BUN is valuable for anticipating specific sepsis complications. It is an independent risk factor for acute respiratory distress syndrome34 and a significant component in models predicting persistent sepsis-associated acute kidney injury.35 Importantly, elevated BUN levels are also associated with an increased risk of atrial fibrillation,36 reinforcing its relevance in the context of NOAF. In sepsis, the heart and kidneys engage in a detrimental crosstalk, where dysfunction of one organ exacerbates injury to the other through intertwined hemodynamic and neurohumoral pathways.37 Elevated BUN often signifies renal impairment, which can promote arrhythmogenesis through two principal mechanisms: the accumulation of uremic toxins that suppress myocardial contractility, and the induction of electrolyte disturbances. This pathophysiological link is further illuminated by the work of Chen et al38 who demonstrated that hydrogen sulfide alleviates sepsis-induced cardiorenal injury by activating the PINK1/Parkin pathway to enhance mitophagy. This process polarizes macrophages from a pro-inflammatory (M1) to an anti-inflammatory (M2) phenotype, improving mitochondrial function and reducing inflammatory infiltration in both organs. Therefore, the excessive inflammatory response and cytokine storm represent a common mechanism underpinning both renal and cardiac damage in sepsis. Clinically, BUN should not be viewed solely as a marker of renal function; its levels should also alert clinicians to potential cardiac implications, including sepsis-induced myocardial injury and associated NOAF. HR refers to the number of times the heart beats per minute, and it is affected by a variety of factors, such as exercise, body temperature, infection, and inflammation. AF is characterized by absolute irregularity of heart rhythm and a relatively rapid HR. While increased HR lacks specificity, in sepsis patients, if there is concomitant elevation of IL-6 and BUN, clinical vigilance should be exercised regarding the risk of NOAF.
Although the predictive model established in this study exhibits excellent discriminative ability, calibration, and clinical applicability, it still has the following limitations. First, this study is a single-center retrospective study. The disease severity, infection sites, etiologies, patient populations, and diagnostic and therapeutic levels of sepsis patients in different regions and hospitals vary, and thus the results of this single-center study may not be extrapolated to other clinical settings. Additionally, retrospective studies cannot effectively control biases in a prospective manner. In the future, it is necessary to conduct multicenter, prospective studies to reduce selection bias and enhance clinical utility. Second, although the indicators included in the predictive model of this study cover inflammatory markers, biochemical markers, and vital signs, these indicators are affected by multiple factors and lack specificity. Therefore, it will be necessary to develop indicators with both sensitivity and specificity in future research. Previous studies have demonstrated the value of omics in identifying diagnostic and predictive biomarkers,39,40 and omics-based research may provide clues for screening diagnostic and predictive biomarkers of NOAF with both sensitivity and specificity. Third, although our study included factors potentially associated with NOAF development-such as comorbidities, mechanical ventilation, serum potassium, serum calcium, serum magnesium, and inflammatory markers-it did not incorporate the use of norepinephrine. Norepinephrine is commonly used in sepsis patients and exerts an impact on heart rate and rhythm. Exploring its effect on NOAF may be of great value. Fourth, the model validation in this study was conducted via internal validation, which fails to assess the model’s generalizability and robustness. Prior to clinical application, multicenter validation is further required.
Conclusion
Despite these limitations, our study demonstrates that log IL-6, BUN, and HR are independent risk factors for NOAF in sepsis patients. The predictive model developed using these factors exhibits good discriminative ability, calibration, and clinical applicability, which may provide a reference for the early identification of NOAF induced by sepsis.
Abbreviations
NOAF, new-onset atrial fibrillation; LASSO, Least Absolute Shrinkage and Selection Operator; AUC, area under the receiver operating characteristic curve; DCA, Decision Curve Analysis. CIC, Clinical Impact Curve; IL-6, interleukin-6; BUN, blood urea nitrogen; HR, heart rate; MV, mechanical ventilation; SOFA, Sequential Organ Failure Assessment; APACHE-II, Acute Physiology and Chronic Health Evaluation II; GCS, Glasgow Coma Scale; MAP, mean arterial pressure; CAD, coronary artery disease; CRP, c-reactive protein; SAA, serum amyloid A; S1PR2, sphingosine-1-phosphate receptor.
Data Sharing Statement
Data are available upon request from corresponding author.
Ethics Statement
The study was approved by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University (K202412-69). Because this study was retrospective, so informed consent was waived by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University. To protect patient privacy, all personally identifiable information was deidentified, ensuring that data were used exclusively by the research team in anonymized form.
Funding
This study was supported by the In-hospital Program for the Cultivation of Excellent Talents and Innovative Teams of the First Affiliated Hospital of Xinjiang Medical University (cxtd202408) and the National Natural Science Foundation of China grant (82260379).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Liu Y-W, Wang Y-F, Chen Y, et al. A nationwide study on new onset atrial fibrillation risk factors and its association with hospital mortality in sepsis patients. Sci Rep. 2024;14(1):12206. doi:10.1038/s41598-024-62630-x
2. Guan C, Gong A, Zhao Y, et al. Interpretable machine learning model for new-onset atrial fibrillation prediction in critically ill patients: a multi-center study. Crit Care. 2024;28(1):349. doi:10.1186/s13054-024-05138-0
3. Walkey AJ, Wiener RS, Ghobrial JM, et al. Incident Stroke and Mortality Associated With New-Onset Atrial Fibrillation in Patients Hospitalized With Severe Sepsis. JAMA. 2011;306(20). doi:10.1001/jama.2011.1615
4. Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
5. Wetterslev M, Hylander MM, Granholm A, et al. Atrial Fibrillation (AFIB) in the ICU: incidence, Risk Factors, and Outcomes: the International AFIB-ICU Cohort Study. Crit Care Med. 2023;51(9):1124–1137. doi:10.1097/CCM.0000000000005883
6. Leng Y, Li Y, Wang J, et al. Sepsis as an independent risk factor in atrial fibrillation and cardioembolic stroke. Front Endocrinol. 2023;14:1056274. doi:10.3389/fendo.2023.1056274
7. Walkey AJ, Greiner MA, Heckbert SR, et al. Atrial fibrillation among Medicare beneficiaries hospitalized with sepsis: incidence and risk factors. Am Heart J. 2013;165(6):949–955.e3. doi:10.1016/j.ahj.2013.03.020
8. Honorato MO, Sousa Filho JT, Honorato Junior LFB, et al. Atrial Fibrillation and Sepsis in Elderly Patients and Their Associaton with In-Hospital Mortality. Arq Bras Cardiol. 2023;120(3):e20220295. doi:10.36660/abc.20220295
9. Rucci JM, Bosch NA, Quinn EK, et al. External Validation of a Risk Score for Daily Prediction of Atrial Fibrillation among Critically Ill Patients with Sepsis. Ann ATS. 2022;19(4):697–701. doi:10.1513/AnnalsATS.202107-787RL
10. Kuipers S, Klouwenberg PMK, Cremer OL. Incidence, risk factors and outcomes of new-onset atrial fibrillation in patients with sepsis: a systematic review. Crit Care. 2014;18(6):688. doi:10.1186/s13054-014-0688-5
11. Walkey AJ, Hammill BG, Curtis LH, et al. Long-term Outcomes Following Development of New-Onset Atrial Fibrillation During Sepsis. Chest. 2014;146(5):1187–1195. doi:10.1378/chest.14-0003
12. Meng H, Guo L, Pan Y, et al. Machine learning based clinical prediction model for 1-year mortality in Sepsis patients with atrial fibrillation. Heliyon. 2024;10(21):e38730. doi:10.1016/j.heliyon.2024.e38730
13. Gandhi S, Litt D, Narula N. New-onset atrial fibrillation in sepsis is associated with increased morbidity and mortality. Neth Heart J. 2015;23(2):82–88. doi:10.1007/s12471-014-0641-x
14. Li Z, Pang M, Li Y, et al. Development and validation of a predictive model for new-onset atrial fibrillation in sepsis based on clinical risk factors. Front Cardiovasc Med. 2022;9:968615. doi:10.3389/fcvm.2022.968615
15. Klein Klouwenberg PMC, Frencken JF, Kuipers S, et al. Incidence, Predictors, and Outcomes of New-Onset Atrial Fibrillation in Critically Ill Patients with Sepsis. A Cohort Study. Am J Respir Crit Care Med. 2017;195(2):205–211. doi:10.1164/rccm.201603-0618OC
16. Li J, Wang S, Ma C, et al. Sepsis-Induced Coagulopathy Score is Associated with an Increased Risk of New-Onset Atrial Fibrillation in Septic Patients: a Two-Centered Retrospective Study. JIR. 2024;17:5889–5899. doi:10.2147/JIR.S467424
17. Bosch NA, Cohen DM, Walkey AJ. Risk Factors for New-Onset Atrial Fibrillation in Patients With Sepsis: a Systematic Review and Meta-Analysis. Crit Care Med. 2019;47(2):280–287. doi:10.1097/CCM.0000000000003560
18. Yu B, Chen M, Zhang Y, et al. Diagnostic and Prognostic Value of Interleukin-6 in Emergency Department Sepsis Patients. IDR. 2022;15:5557–5566. doi:10.2147/IDR.S384351
19. Batta A, Hatwal J, Sharma Y. Assessment of Coronary Artery Disease in Non-Valvular Atrial Fibrillation: is This Light at the End of the Tunnel? VHRM. 2024;20:493–499. doi:10.2147/VHRM.S484638
20. Batta A, Hatwal J, Batta A, et al. Atrial fibrillation and coronary artery disease: an integrative review focusing on therapeutic implications of this relationship. World J Cardiol. 2023;15(5):229–243. doi:10.4330/wjc.v15.i5.229
21. Pintea Bentea G, Berdaoui B, Morissens M, et al. Pathophysiology, Diagnosis, and Management of Coronary Artery Disease in the Setting of Atrial Fibrillation. J Am Heart Assoc. 2024;13(23):e037552. doi:10.1161/JAHA.124.037552
22. Tamazyan V, Khachatryan A, Batikyan A, et al. Sepsis-induced Atrial Fibrillation: can We Predict and Prevent This High-Risk Complication? Cureus. 2025;17(6):e85387. doi:10.7759/cureus.85387
23. Tanaka T, Narazaki M, Kishimoto T. IL-6 in Inflammation, Immunity, and Disease. Cold Spring Harbor Perspect Biol. 2014;6(10):a016295–a016295. doi:10.1101/cshperspect.a016295
24. Hamilton FW, Thomas M, Arnold D, et al. Therapeutic potential of IL6R blockade for the treatment of sepsis and sepsis-related death: a Mendelian randomisation study. PLoS Med. 2023;20(1):e1004174. doi:10.1371/journal.pmed.1004174
25. Šundalić S, Košuta I, Baršić LI, et al. Interleukin-6 and Leukocyte Cell Population Data in Newly Diagnosed Sepsis-A Prospective Study. Medicina. 2025;61(3):468. doi:10.3390/medicina61030468
26. Tsai YH, Hung KY, Fang WF. Leptin and Iinterlukin-6 relationship and influence of mortality in sepsis. BMC Infect Dis. 2025;25(1):460. doi:10.1186/s12879-025-10829-2
27. Bai W, Liu ZQ, He PY, et al. The role of IL-6, IL-10, TNF-α and PD-1 expression on CD4 T cells in atrial fibrillation. Heliyon. 2023;9(8):e18818. doi:10.1016/j.heliyon.2023.e18818
28. Keefe JA, Aguilar-Sanchez Y, Navarro-Garcia JA, et al. Macrophage-mediated IL-6 signaling drives ryanodine receptor–2 calcium leak in postoperative atrial fibrillation. J Clin Investig. 2025;135(9):e187711. doi:10.1172/JCI187711
29. Ling X, Shen J, Liang J, et al. Comparison of the Cecum Ligation and Puncture Method and the Intraperitoneal Lipopolysaccharide Injection Method for the Construction of a New-Onset Atrial Fibrillation Model of Sepsis. J Inflamm Res. 2024;17:9103–9117. doi:10.2147/JIR.S485142
30. Li X, Li T, Wang J, et al. Higher blood urea nitrogen level is independently linked with the presence and severity of neonatal sepsis. Annals of Medicine. 2021;53(1):2194–2200. doi:10.1080/07853890.2021.2004317
31. Liu F, Yao J, Liu C, et al. Construction and validation of machine learning models for sepsis prediction in patients with acute pancreatitis. BMC Surg. 2023;23(1):267. doi:10.1186/s12893-023-02151-y
32. Li J, Wang Y, Luo J, et al. Development and validation of a nomogram for predicting sepsis in patients with pyogenic liver abscess. Sci Rep. 2023;13(1):10849. doi:10.1038/s41598-023-37907-2
33. Wen C, Zhang X, Li Y, et al. An interpretable machine learning model for predicting 28-day mortality in patients with sepsis-associated liver injury. PLoS One. 2024;19(5):e0303469. doi:10.1371/journal.pone.0303469
34. Xu C, Zheng L, Jiang Y, et al. A prediction model for predicting the risk of acute respiratory distress syndrome in sepsis patients: a retrospective cohort study. BMC Pulm Med. 2023;23(1):78. doi:10.1186/s12890-023-02365-z
35. Jiang W, Zhang Y, Weng J, et al. Explainable Machine Learning Model for Predicting Persistent Sepsis-Associated Acute Kidney Injury: development and Validation Study. J Med Internet Res. 2025;27:e62932. doi:10.2196/62932
36. Lan Q, Zheng L, Zhou X, et al. The Value of Blood Urea Nitrogen in the Prediction of Risks of Cardiovascular Disease in an Older Population. Front Cardiovasc Med. 2021;8:614117. doi:10.3389/fcvm.2021.614117
37. Pei Y, Guo L, Zhou G, et al. Biomarkers for Predicting of Sepsis-Induced Cardiorenal Syndrome in Emergency Settings. Cardiorenal Med. 2025;15(1):198–208. doi:10.1159/000543462
38. Chen Y, Cao W, Li B, et al. The potential role of hydrogen sulfide in regulating macrophage phenotypic changes via PINK1/parkin-mediated mitophagy in sepsis-related cardiorenal syndrome. Immuno and Immunotoxicology. 2024;46(2):139–151. doi:10.1080/08923973.2023.2281901
39. Gou Y, Lv BH, Zhang JF, et al. Identifying early predictive and diagnostic biomarkers and exploring metabolic pathways for sepsis after trauma based on an untargeted metabolomics approach. Sci Rep. 2025;15(1):12068. doi:10.1038/s41598-025-92631-3
40. Gou Y, Liu JJ, Zhang JF, et al. Identifying biomarkers distinguishing sepsis after trauma from trauma-induced SIRS based on metabolomics data: a retrospective study. Sci Rep. 2025;15(1):13748. doi:10.1038/s41598-025-94701-y
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.