Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Development and Validation of a Risk Nomogram Model for Predicting Constipation in Patients with Type 2 Diabetes Mellitus
Authors Yuan HL, Zhang X, Peng DZ, Lin GB ![]() , Li HH, Li FX, Lu JJ
, Li HH, Li FX, Lu JJ ![]() , Chu WW
, Chu WW
Received 2 February 2023
Accepted for publication 12 April 2023
Published 20 April 2023 Volume 2023:16 Pages 1109—1120
DOI https://doi.org/10.2147/DMSO.S406884
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Hai-Liang Yuan,1 Xian Zhang,2 Dong-Zhu Peng,1 Guan-Bin Lin,1 Hui-Hui Li,1 Fang-Xian Li,1 Jing-Jing Lu,1 Wei-Wei Chu1
1Department of Gastroenterology, Beilun Branch of the First Affiliated Hospital of Zhejiang University, Ningbo, Zhejiang, People’s Republic of China; 2Department of Endocrinology, the First Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China
Correspondence: Wei-Wei Chu, Department of Gastroenterology, Beilun Branch of the First Affiliated Hospital of Zhejiang University, No. 1288, Lushan East Road, Beilun District, Ningbo, Zhejiang Province, People’s Republic of China, Tel +86-134 56123811, Fax +86- 574 86100266, Email [email protected]
Purpose: Constipation is a common complication of diabetic patients, which has a negative impact on their own health. This study aims to establish and internally validate the risk nomogram of constipation in patients with type 2 diabetes mellitus (T2DM) and to test its predictive ability.
Patients and Methods: This retrospective study included 746 patients with T2DM at two medical centers. Among the 746 patients with T2DM, 382 and 163 patients in the Beilun branch of the First Affiliated Hospital of Zhejiang University were enrolled in the training cohort and the validation cohort, respectively. A total of 201 patients in the First Affiliated Hospital of Nanchang University were enrolled in external validation cohorts. The nomogram was established by optimizing the predictive factors through univariate and multivariable logistic regression analysis. The prediction performance of the nomogram was measured by the area under the receiver operating characteristic curve (AUROC), the calibration curve, and the decision curve analysis (DCA). Furthermore, its applicability was internally and independently validated.
Results: Among the 16 clinicopathological features, five variables were selected to develop the prediction nomogram, including age, glycated hemoglobin (HbA1c), calcium, anxiety, and regular exercise. The nomogram revealed good discrimination with an area under the receiver operating characteristic curve (AUROC) of 0.908 (95% CI = 0.865– 0.950) in the training cohort, and 0.867 (95% CI = 0.790– 0.944) and 0.816 (95% CI = 0.751– 0.881) in the internal and external validation cohorts, respectively. The calibration curve presented a good agreement between the prediction by the nomogram and the actual observation. The DCA revealed that the nomogram had a high clinical application value.
Conclusion: In this study, the nomogram for pretreatment risk management of constipation in patients with T2DM was developed which could help in making timely personalized clinical decisions for different risk populations.
Keywords: constipation, type 2 diabetes mellitus, model, nomogram, prediction
Introduction
Diabetes mellitus (DM) is a common chronic non-communicable disease characterized by hyperglycemia, a group of metabolic diseases characterized by elevated blood glucose levels due to relative or absolute insulin secretion insufficiency and/or pancreatic islet utilization disorders.1 Type 2 diabetes mellitus (T2DM) is the most common type accounting for more than 90% of the cases.2,3 T2DM is prone to multiple organ lesions. In addition, the patients often develop a variety of abnormal metabolic aggregation phenomena, like neuropathy, retinopathy, and nephropathy. These conditions not only endanger human health but also create a heavy economic burden on the family and society.4 The direct medical expenses and economic losses caused by this are estimated to already reach a trillion dollars.5
In addition, up to 50% of patients with diabetic autonomic neuropathy suffer from constipation, which might cause hemorrhoids, infections, anal fissures, and other discomforts due to poor defecation. This could seriously affect the normal treatment and health levels of the patients and increase the medical economic burden.6,7 A few patients with T2DM suffering from constipation experience a sudden rise in blood pressure due to forced defecation. This leads to blood vessel rupture, retinal hemorrhage, acute myocardial ischemia, or cerebral ischemia due to insufficient blood supply to the heart and brain, which greatly increases the mortality and disability rate of patients.8,9 Necessary intervention could be carried out promptly if the risk of constipation in patients with T2DM could be predicted clinically. Currently, the research on constipation in patients with T2DM predominantly focuses on its pathogenesis and treatment.10,11 Moreover, scanty research is available on establishing a prediction model to predict the risk of constipation in T2DM patients.
In modern clinical medicine, the disease risk prediction model is a crucial part of decision-making. In recent years, the nomograph in construction and application represents the progress of prediction tools.12 The nomogram is a statistical prediction model that converts complex mathematical formulas into visual graphics by integrating multiple biological and clinical prediction variables, listing each prediction variable separately, and quantifying it in the form of a score. It then matches the cumulative score of all prediction variables with the resulting scale to generate the probability of occurrence of a certain clinical event for a specific individual.13,14 A nomograph can assess the risk of certain clinical events to specific individuals according to the characteristics of patients and diseases. This is the main advantage of a nomograph.12 It not only meets the strong clinical demand for integrated models, which is easy to apply and promote in clinical practice, but also can provide clinicians with more reasonable and personalized diagnosis and treatment plans for patients.15
Prompt intervention could be carried out if the risk of constipation in patients with T2DM could be predicted clinically. However, only a few reports on the risk prediction model of constipation in T2DM patients were available in previous studies. The purpose of this study was to explore the independent risk factors of constipation risk in T2DM patients and build a nomogram prediction model based on the independent risk factors. The nomogram was evaluated, internally validated, and externally validated to evaluate the risk of constipation more reliably and provide some reference for clinicians in identifying the risk of constipation in T2DM patients.
Materials and Methods
Patients
In this study, patients with T2DM visiting the Beilun branch of the First Affiliated Hospital of Zhejiang University from February 2019 to June 2022, were retrospectively screened and enrolled. The inclusion criteria were as follows: 1) The patients who were in line with the diagnosis of T2DM established by the World Health Organization;16 That is, the symptoms of diabetes and the plasma glucose level at any time ≥ 11.1 mmol/L or the fasting plasma grape (FPG) level ≥ 7.0 mmol/L or in the oral glucose tolerance test, the plasma glucose level at 2 hours ≥ 11.1 mmol/L; and 2) patients who were older than 18 years.
The exclusion criteria were: 1) Incomplete data; 2) Patients having chronic constipation before diabetes was diagnosed; 3) Patients with a medical condition that affected the function of the gastrointestinal tract or had a history of bowel surgery; 4) Patients having T2DM along with conditions including hematological diseases, malignant tumors, and autoimmune system diseases.
An independent validation study was conducted on patients with T2DM in the First Affiliated Hospital of Nanchang University from June 2020 to September 2021, using the same standards as the primary study. The detailed process of data screening is shown in Figure 1.
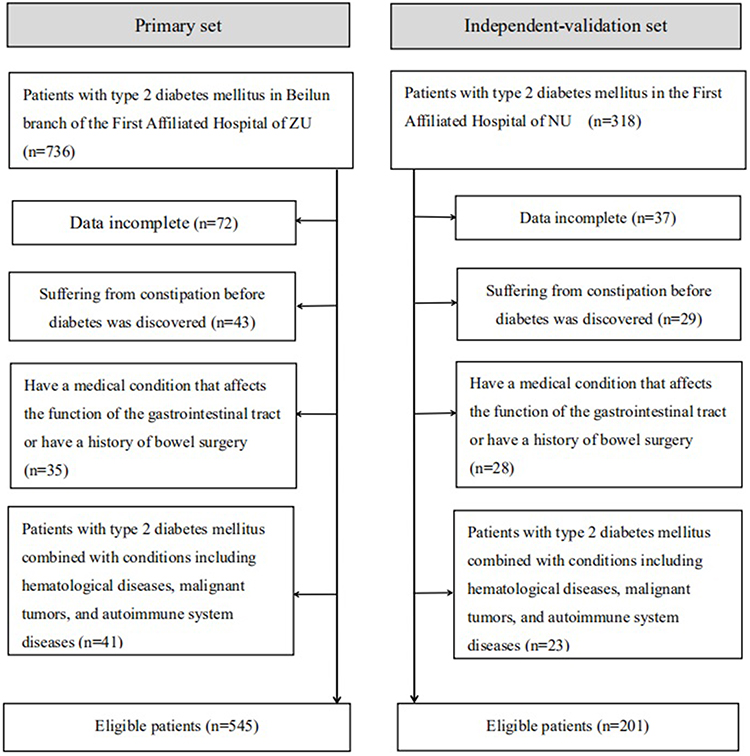 |
Figure 1 Screening process for patients with type 2 diabetes mellitus required for this study. Abbreviations: ZU, Zhejiang University; NU, Nanchang University. |
Baseline and Clinical Variables
The demographic characteristics and clinicopathological variables of each patient were extracted from the case record system of the Beilun Branch of the First Affiliated Hospital of Zhejiang University. Demographic characteristics included body mass index (BMI), smoking history, alcoholism, hypertension, alanine aminotransferase, serum creatinine, total protein (TP), high-density lipoprotein (HDL), low-density lipoprotein (LDL), glycated hemoglobin (HbA1c), regular exercise, calcium supplements, anxiety, and depression. Glycated hemoglobin was used for the assessment of blood glucose control. HbA1c <7.0% was interpreted as good blood glucose control and HbA1c ≥7.0% as poor glucose control.17,18
The Hamilton Depression Scale (HAMD) and the Hamilton Anxiety Scale (HAMA) were utilized as the criteria for judging patients’ anxiety.19 Also, the patients completed HbA1c measurements and scale evaluation during hospitalization. According to the internationally unified Rome III diagnostic criteria for chronic constipation,20 the symptoms of constipation persist for more than 3 months, organic lesions are excluded, and two or more of the following conditions are met: (1) Frequency of spontaneous defecation occurring less than three times a week; (2) difficulty in defecation occurring more than 1/4 of the time; (3) clumps or induration of stool occurring more than 1/4 of the time; (4) feeling of incomplete defecation occurring more than 1/4 of the time; (5) Need for manipulation of defecation occurring more than 1/4 of the time; (6) Anal or anorectal obstruction during defecation occurring more than 1/4 of the time.
Statistical Analysis
SPSS 25.0 software (IBM, USA) and R software (version 4.2.1; https://www.r-project.org/) were used for statistical analysis of the research data. Continuous variables were expressed as mean and standard deviation (mean±SD) and compared between two groups using independent-sample t test.Categorical variables were expressed as frequency and/or percentage and compared by using the Pearson’s Chi squared test. The difference was statistically significant if P<0.05.
Method of Constructing and Verifying the Nomogram Model
Patients with T2DM in the primary set were randomly divided into the training group (70%) and the internal validation group (30%) in a ratio of 7:3. Univariate and multivariable logistic regression analyses were used to calculate and validate the effect of variables in training group.21 A univariate logistic regression model was used to screen the independent risk factors for constipation in type 2 diabetes using the data of the training group which revealed that variables with P<0.05 were included in the multivariable logistic regression analyses model. To identify independent risk factors, the measure of the effect of each variable on chronic constipation was presented as an odds ratio (OR). The nomogram model was constructed and validated using the selected prediction variables. As per the results of the final multivariable logistic regression, the nomogram was constructed to visually score individual risk probabilities of constipation in patients with T2DM.
Calibration curves were measured with 1000 bootstraps resample by plotting the observed probability. The area under the receiver operating characteristic curve (AUROC) was calculated to quantitatively express the ability of the nomogram to predict constipation in patients with T2DM. Finally, the decision curve analysis (DCA) method was applied to determine the clinical value of the prediction model by calculating the net benefits at various threshold probabilities in the validation set.
Results
Demographic and Clinical Features
In our final cohort study, 746 patients were enrolled after a series of screenings with 545 and 201 patients assigned to the primary and the independent-validation cohorts, respectively (Figure 1). A total of 545 patients with T2DM from the Beilun branch of the First Affiliated Hospital of Zhejiang University, were reviewed and randomly divided into the training set (n = 382) and the internal validation set (n = 163). Furthermore, 201 patients with T2DM from the First Affiliated Hospital of Nanchang University comprised the external validation set. The rate of constipation was 20.4% and 23.9% in the primary and independent-validation sets, respectively (P=0.314). The clinical characteristics of the patients in the primary and independent-validation sets have been enlisted in Table 1.
 |
Table 1 Base Characteristics of Patients in the Primary and Validation Cohorts |
Predictor Selection and Model Development
Univariate logistic regression analysis was performed with the included 16 independent variables, and the results demonstrated that gender, age, HbA1c, calcium, anxiety, and regular exercise were significantly different between the two groups (P<0.05), as presented in Table 2. Next, significant independent variables obtained from the above univariate logistic regression analysis were included in multivariable logistic regression analysis following a backward stepwise regression method. Furthermore, in type 2 diabetic patients, a multivariable logistic regression analysis (Table 2) revealed that five factors, including age (OR = 9.462, 95% CI = 3.712–24.117), HbA1c (OR = 22.015, 95% CI = 10.352–46.819), calcium (OR = 1.976, 95% CI = 0.865–4.513), anxiety (OR = 5.042, 95% CI = 2.027–12.543), and regular exercise (OR = 0.321, 95% CI = 0.123–0.837) were independent predictors of constipation. A prediction model incorporating the above independent variables was developed and presented as a nomogram (Figure 2).
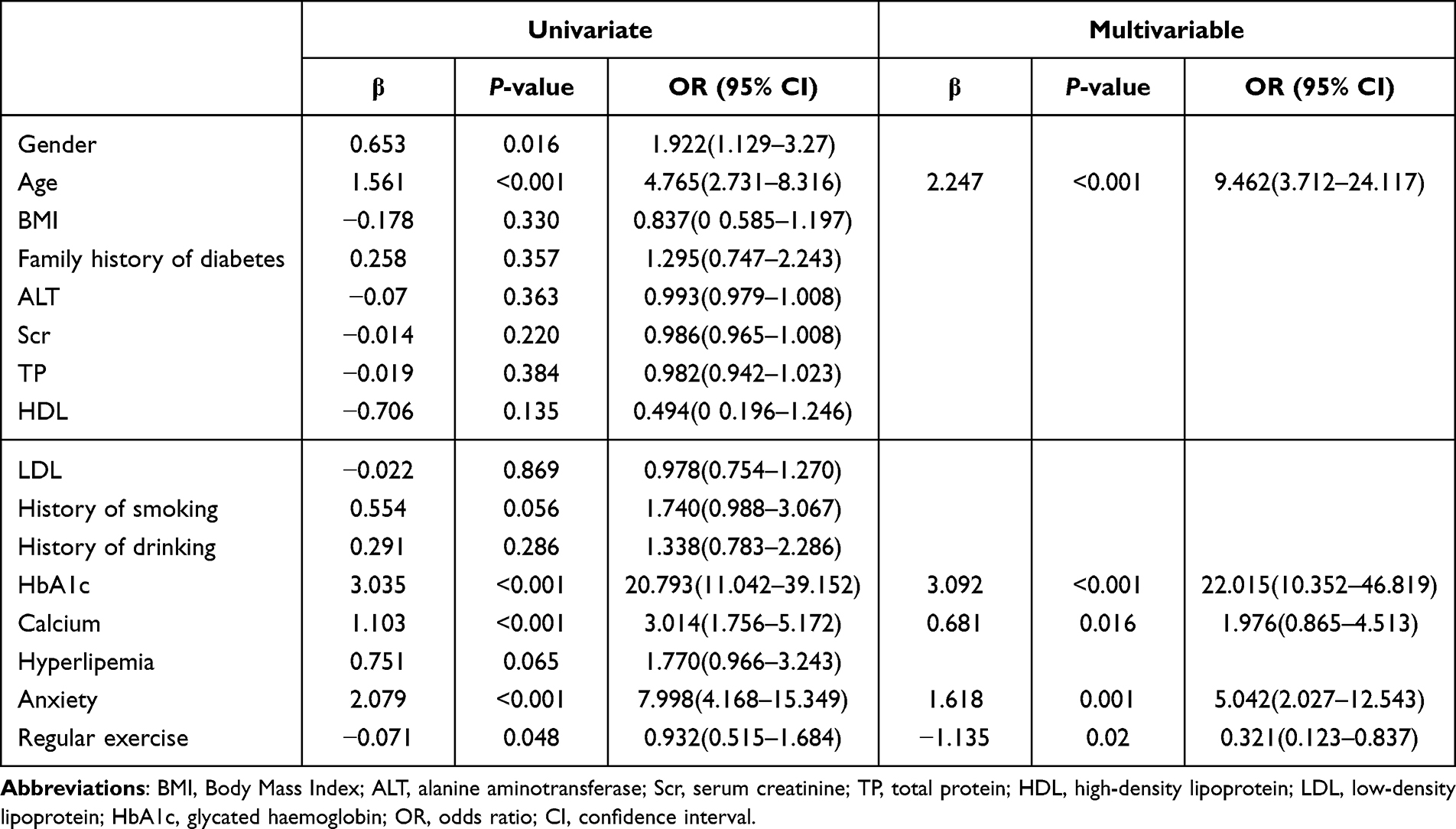 |
Table 2 Results of Univariate and Multivariable Analysis for Prediction of Incidence of Constipation |
 |
Figure 2 The nomogram model for quantifying individual risk of constipation in patients with type 2 diabetes mellitus. |
Performances of Prediction and Calibration
The validation of this prediction model was performed by the ROC curve and the calibration curve. The discrimination ability and prediction performance of the nomogram were represented by the ROC curve (Figure 3). The AUROC of 0.908 (95% CI = 0.865–0.950) for the training set, 0.867 (95% CI = 0.790–0.944) for the internal validation set, and 0.816 (95% CI = 0.751–0.881) for the external validation set indicated that the nomogram had a good valuable prediction for constipation in T2DM patients. Moreover, the calibration curve of the nomogram also depicted good agreement between the observed and predicted probabilities in all three datasets (Figure 4).
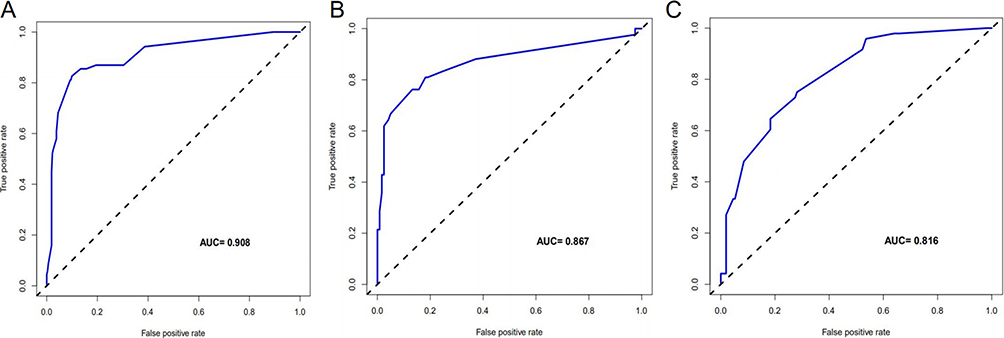 |
Figure 3 Prediction performance of the model. Receiver operating characteristic (ROC) curve plot in the training set (A); ROC curve plot in the internal‑validation set (B); ROC curve plot in the independent‑validation set (C);AUC, the area under the receiver operating characteristic. |
 |
Figure 4 Calibration curve plot in each set. (A) the training set; (B) the internal‑validation set; (C) the independent–validation set. |
The Presentation of the Nomogram and Clinical Risk Management
The clinical validity of this predictive model was assessed using decision curve analysis (DCA) have been presented in Figure 5, which indicated that when the threshold probabilities were in the range of 9%~78.9%, a higher net clinical benefit could be achieved than the hypothetical non-testing or all testing scenarios.
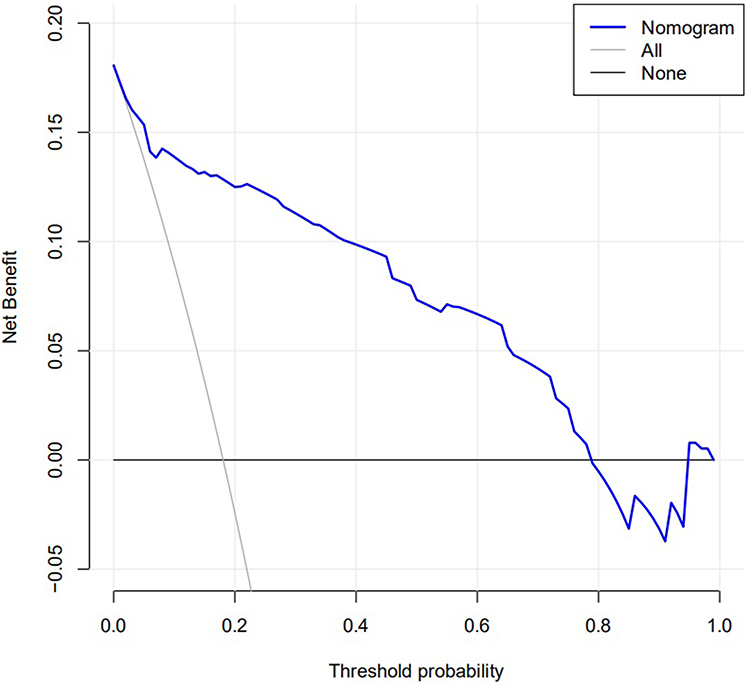 |
Figure 5 Decision curve analysis for classification of different risk population. |
Discussion
Constipation, caused by autonomic neuropathy in patients with diabetes, is one of the common complications of gastrointestinal dysfunction. Its incidence accounts for about 25% of patients with diabetes.22 If constipation is not diagnosed and treated effectively and on time, it would seriously affect the quality of life of patients with diabetes, aggravate their bad mood, increase insulin resistance, affect the stability of blood sugar of patients with diabetes, and also result in cardiovascular and cerebrovascular accidents, intestinal rupture and perforation, sudden death, and other serious complications.23 Therefore, an urgent problem to be solved in the diagnosis and treatment of patients with diabetes is to keep the defecation unobstructed.
Presently, as a disease risk prediction tool in clinical research, a nomogram can predict the probability of disease occurrence by analyzing and integrating the risk factors that affect the occurrence and development of disease. It has the characteristics of high reliability, strong practicality, and simplicity. Additionally, it has been widely used in the prediction and prognostic research of several diseases.14 In this study, the method of combining single-factor analysis and a multifactor regression model is used to screen predictive variables. This weakens the influence of multicollinearity. Also, by obtaining a more concise and efficient set of predictive variables, it plays a role in the selection of these variables.15
The results of this study revealed that age, HbA1c, calcium, anxiety, and regular exercise were independent predictors for constipation in T2DM patients (P<0.05). The study plans to establish a nomograph prediction model to predict the risk of constipation in T2DM patients based on a single factor and logistic regression multi-factor analysis. This study also aims to provide a reference and basis for clinical screening and early intervention of constipation in T2DM patients.
In T2DM patients, HbA1c ≥ 7.0% is the most important risk factor for the development of constipation. HbA1c reflects the overall blood glucose level of the patient for 2–3 months. A study has discovered that the severity of symptoms in T2DM patients is associated with the level of glycosylated hemoglobin.24 The gastrointestinal nervous system is vulnerable to the influence of blood glucose. Additionally, continuous hyperglycemic stimulation activates the polyol pathway on the cell membrane. The polyol pathway is an abnormal glucose metabolism pathway that results in the catalyzation of glucose by aldose reductase. In the process of catalysis, a large amount of glutathione with a reducing effect is consumed, resulting in insufficient intestinal antioxidant capacity and an inability to resist the damage caused by peroxide.25 Therefore, hyperglycemia leads to intestinal dysfunction, slow peristalsis, dysexcretion, and increased prevalence of constipation through polyol pathway metabolism. Nevertheless, hyperglycemia could also result in the retrograde transportation of glucose to intestinal epithelial cells through glucose transporter 2, participation in intracellular glucose metabolism, reprogramming of transcription proteins, and destruction of the compactness and integrity of adhesion of intestinal cells, thereby changing the cell permeability. Hyperglycemia destroys the intestinal barrier causing bacterial diffusion and resulting in the spread of inflammation to the whole intestine and the body. This causes the development of a serious bacterial infection.26 The intestinal defecation function is impaired because of damage to the intestinal barrier function or bacterial infection. Thus, this increases the prevalence of constipation in T2DM. Excessive blood glucose fluctuation produces a large number of reactive oxygen species that deplete the antioxidants in the gastrointestinal tract.27 Moreover, when the body generates reactive oxygen species, it also forms glycosylation end products, activates the expression of inflammatory factors, and further intensifies the apoptosis of intestinal nerve cells.25 Therefore, in T2DM patients, long-term poor control of blood glucose results in neurodegenerative changes in the gastrointestinal tract which is an important reason for the development of constipation.
The age factor is mainly manifested in old-aged patients with diabetes mellitus. The physical quality level of older patients gradually changes, and their clinical symptoms gradually become obvious.28 Older patients gradually lose their gastrointestinal function with the increase in their age, thus increasing the probability of constipation.29 With the increase of age, the intestinal peristalsis function of older patients decreases, the secretion of digestive enzymes in the gastrointestinal and pancreas decreases, and the muscle tension involved in defecation decreases. These factors result in the prolongation of defecation time and interval and cause excessive absorption of stool water in the intestinal tract and difficulty in excretion.30 In addition, due to the long course of the disease, older patients with diabetes have a greater probability of developing autonomic neuropathy involving the digestive system, which is more likely to induce constipation.31
One of the important factors that cause constipation is the lack of regular physical exercise. This happens because the intestinal peristalsis function of patients with less physical exercise is weakened. This easily leads to the development of insufficient abdominal pressure for defecation, thus causing constipation.32 This is common among older diabetic patients. The food intake and consumption of older diabetic patients are uneven due to the decrease in their activity.33 In addition, some patients experience numbness, swelling, and slow reaction after the onset of the disease, which affects their levels of exercise activity.34 The reduction in exercise activity causes a slowing down of intestinal peristalsis, a decline in appetite, and abdominal muscle relaxation, thus inducing constipation.35 In this study, it was confirmed that lack of exercise is a risk factor for the development of constipation in patients with T2DM. Therefore, advocating for T2DM patients to maintain proper physical exercise could prevent constipation.
Osteoporosis is a common complication of patient with diabetes. Such patients often need calcium supplementation. Diabetes mellitus is a chronic disease with multiple clinical manifestations. If timely and effective intervention is not provided to patients, blood sugar would be at a higher level for a longer duration. This would very easily result in the development of several complications.36 This study revealed that long-term calcium supplementation could increase the risk of constipation. Among them, T2DM patients with osteoporosis is the most common. Additionally, diabetes tends to occur in middle and old-aged individuals. Such patients have different degrees of bone mineral density reduction, which further increases the risk of osteoporosis.37 Most patients have accompanied joint pain to a certain extent. In severe cases, the dysfunction could occur, and the risk of fracture might increase. This has become one of the important causes of diabetes disability.38 At present, clinically, oral calcium and vitamin D supplementation is commonly prescribed to patients. These supplements relieve the symptoms and pain of patients to varying degrees.39 However, calcium carbonate contained in calcium agents eventually forms calcium phosphate under the action of gastric acid. This directly inhibits intestinal peristalsis and causes constipation.40
Psychological and emotional abnormalities, like anxiety or depression, could also induce constipation in patients.41 It has been reported that abnormal scores on the anxiety and depression scale could increase the risk of constipation; This might be due to psychological factors, like anxiety and depression that affect the sensory, motor, and secretory functions of the gastrointestinal tract. Additionally, they also inhibit the parasympathetic nerves and blunt the defecation reflex, thus inducing or aggravating constipation.42 A few studies have highlighted that due to the high negative emotions of patients, the probability of mental tension in the management of diabetic patients is increased.43,44 Most diabetic patients have symptoms of anxiety and depression after onset. If they are not effectively controlled, such symptoms would gradually worsen and cause neurological disorders and endocrinal disorders in patients. Thus, the probability of constipation in patients would also increase.45
In summary, this study reveals that a simple risk assessment model based on five clinical indicators can reliably predict the risk of constipation in patients with T2DM. Constipation often occurs in patients with T2DM which can be prevented by timely and effective intervention. This prediction model can be used by clinicians to assess the risk of constipation in T2DM patients in clinical practice. Furthermore, it can be used to design future clinical trials that would prevent type 2 diabetic patients from developing constipation.
This study has limitations. Firstly, a retrospective analysis was adopted in this research. A few patients did not complete the corresponding examination due to the complexity of T2DM and constipation, the severity of the disease, and economic factors. This resulted in incomplete admission data. In addition, it was difficult to judge the effect of treatment on patients correctly because the condition record of patients was not detailed at the time of admission. Finally, further prospective multicentric clinical studies should be conducted to prove the clinical efficacy of the findings of this study.
Conclusion
This study systematically developed and validated a new nomograph model to predict the risk of constipation in T2DM patients. With this easy-to-use scoring system, clinicians can preprocess the management of patients with T2DM, which is convenient for timely personalized clinical decision-making.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and was approved by the Beilun branch of the First Affiliated Hospital of Zhejiang University for Clinical Investigation (No. 2022LP016). All the patients provided written informed consent for their medical information to be stored and used in the hospital database at the first visit to our center. We have paid great attention to the protection of the privacy of patient personal information during the retrospective collection of patient information. This study has not caused any harm to patients from beginning to end, and is in line with the Helsinki Declaration and the International Code of Ethics for Biomedical Research Involving Human Beings.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Science Project of Traditional Chinese Medicine of Zhejiang Province, China (No. 2020ZA108).
Disclosure
The authors declare that they have no competing interests.
References
1. Zimmet P, Alberti KG, Shaw J. Global and societal implications of the diabetes epidemic. Nature. 2001;414(6865):782–787. doi:10.1038/414782a
2. Mayer-Davis EJ, Lawrence JM, Dabelea D, et al. Incidence trends of type 1 and type 2 diabetes among youths, 2002-2012. N Engl J Med. 2017;376(15):1419–1429. doi:10.1056/NEJMoa1610187
3. Divers J, Mayer-Davis EJ, Lawrence JM, et al. Trends in incidence of type 1 and type 2 diabetes among youths - selected counties and Indian reservations, United States, 2002-2015. Mmwr Morb Mortal Wkly Rep. 2020;69(6):161–165. doi:10.15585/mmwr.mm6906a3
4. Chatterjee S, Khunti K, Davies MJ. Type 2 diabetes. Lancet. 2017;389(10085):2239–2251. doi:10.1016/S0140-6736(17)30058-2
5. Tomic D, Shaw JE, Magliano DJ. The burden and risks of emerging complications of diabetes mellitus. Nat Rev Endocrinol. 2022;18(9):525–539. doi:10.1038/s41574-022-00690-7
6. Du YT, Rayner CK, Jones KL, et al. Gastrointestinal symptoms in diabetes: prevalence, assessment, pathogenesis, and management. Diabetes Care. 2018;41(3):627–637. doi:10.2337/dc17-1536
7. Sommers T, Mitsuhashi S, Singh P, et al. Prevalence of chronic constipation and chronic diarrhea in diabetic individuals in the United States. Am J Gastroenterol. 2019;114(1):135–142. doi:10.1038/s41395-018-0418-8
8. Sangnes DA, Lundervold K, Bekkelund M, et al. Gastrointestinal transit and contractility in diabetic constipation: a wireless motility capsule study on diabetes patients and healthy controls. United European Gastroenterol J. 2021;9(10):1168–1177. doi:10.1002/ueg2.12169
9. Sumida K, Molnar MZ, Potukuchi PK, et al. Constipation and risk of death and cardiovascular events. Atherosclerosis. 2019;281:114–120. doi:10.1016/j.atherosclerosis.2018.12.021
10. Prasad VG, Abraham P. Management of chronic constipation in patients with diabetes mellitus. Indian J Gastroenterol. 2017;36(1):11–22. doi:10.1007/s12664-016-0724-2
11. Yoshinobu S, Hasuzawa N, Nagayama A, et al. Effects of elobixibat, an inhibitor of ileal bile acid transporter, on glucose and lipid metabolism: a single-arm pilot study in patients with t2dm. Clin Ther. 2022. doi:10.1016/j.clinthera.2022.08.009
12. Bandini M, Fossati N, Briganti A. Nomograms in urologic oncology, advantages and disadvantages. Curr Opin Urol. 2019;29(1):42–51. doi:10.1097/MOU.0000000000000541
13. Balachandran VP, Gonen M, Smith JJ, et al. Nomograms in oncology: more than meets the eye. Lancet Oncol. 2015;16(4):e173–e180. doi:10.1016/S1470-2045(14)71116-7
14. Morlacco A, Modonutti D, Motterle G, et al. Nomograms in urologic oncology: lights and shadows. J Clin Med. 2021;10:5. doi:10.3390/jcm10050980
15. Summers RM. Nomograms for automated body composition analysis: a crucial step for routine clinical implementation. Radiology. 2021;298(2):330–331. doi:10.1148/radiol.2020203956
16. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a who consultation. Diabet Med. 1998;15(7):539–553. doi:10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S
17. Qaseem A, Vijan S, Snow V, et al. Glycemic control and type 2 diabetes mellitus: the optimal hemoglobin a1c targets. A guidance statement from the American college of physicians. Ann Intern Med. 2007;147(6):417–422. doi:10.7326/0003-4819-147-6-200709180-00012
18. Ding L, Xu Y, Liu S, et al. Hemoglobin a1c and diagnosis of diabetes. J Diabetes. 2018;10(5):365–372. doi:10.1111/1753-0407.12640
19. Baykan H, Baykan O, Durmaz O, et al. Plasma neuropeptide-s levels in populations diagnosed with generalized anxiety disorder: a controlled study. Noro Psikiyatr Ars. 2019;56(1):52–56. doi:10.29399/npa.22907
20. Tack J, Talley NJ. Functional dyspepsia--symptoms, definitions and validity of the Rome iii criteria. Nat Rev Gastroenterol Hepatol. 2013;10(3):134–141. doi:10.1038/nrgastro.2013.14
21. Sauerbrei W, Boulesteix AL, Binder H. Stability investigations of multivariable regression models derived from low- and high-dimensional data. J Biopharm Stat. 2011;21(6):1206–1231. doi:10.1080/10543406.2011.629890
22. Rodrigues ML, Motta ME. Mechanisms and factors associated with gastrointestinal symptoms in patients with diabetes mellitus. J Pediatr (Rio J). 2012;88(1):17–24. doi:10.2223/JPED.2153
23. Ghadiri-Anari A, Gholami S, Zolfaghari F, et al. Prediabetes and gastrointestinal (gi) symptoms; A cross-sectional study. Diabetes Metab Syndr. 2019;13(1):844–846. doi:10.1016/j.dsx.2018.12.005
24. Bytzer P, Talley NJ, Leemon M, et al. Prevalence of gastrointestinal symptoms associated with diabetes mellitus: a population-based survey of 15,000 adults. Arch Intern Med. 2001;161(16):1989–1996. doi:10.1001/archinte.161.16.1989
25. Chandrasekharan B, Anitha M, Blatt R, et al. Colonic motor dysfunction in human diabetes is associated with enteric neuronal loss and increased oxidative stress. Neurogastroenterol Motil. 2011;23(2):131–138, e26. doi:10.1111/j.1365-2982.2010.01611.x
26. Thaiss CA, Levy M, Grosheva I, et al. Hyperglycemia drives intestinal barrier dysfunction and risk for enteric infection. Science. 2018;359(6382):1376–1383. doi:10.1126/science.aar3318
27. Brownlee M. The pathobiology of diabetic complications: a unifying mechanism. Diabetes. 2005;54(6):1615–1625. doi:10.2337/diabetes.54.6.1615
28. Yamada E, Namiki Y, Takano Y, et al. Clinical factors associated with the symptoms of constipation in patients with diabetes mellitus: a multicenter study. J Gastroenterol Hepatol. 2018;33(4):863–868. doi:10.1111/jgh.14022
29. Black CJ, Ford AC. Chronic idiopathic constipation in adults: epidemiology, pathophysiology, diagnosis and clinical management. Med J Aust. 2018;209(2):86–91. doi:10.5694/mja18.00241
30. Lucak S, Lunsford TN, Harris LA. Evaluation and treatment of constipation in the geriatric population. Clin Geriatr Med. 2021;37(1):85–102. doi:10.1016/j.cger.2020.08.007
31. Cui S, Yang Q, Xie S, et al. Acupuncture for chronic constipation in patients with diabetes mellitus: a protocol for systematic review. Medicine. 2021;100(9):e24886. doi:10.1097/MD.0000000000024886
32. Kirwan JP, Sacks J, Nieuwoudt S. The essential role of exercise in the management of type 2 diabetes. Cleve Clin J Med. 2017;84(7Suppl 1):S15–S21. doi:10.3949/ccjm.84.s1.03
33. Warner SO, Yao MV, Cason RL, et al. Exercise-induced improvements to whole body glucose metabolism in type 2 diabetes: the essential role of the liver. Front Endocrinol (Lausanne). 2020;11:567. doi:10.3389/fendo.2020.00567
34. Gao R, Tao Y, Zhou C, et al. Exercise therapy in patients with constipation: a systematic review and meta-analysis of randomized controlled trials. Scand J Gastroenterol. 2019;54(2):169–177. doi:10.1080/00365521.2019.1568544
35. Tariq O, Rosten C, Huber J. Experiences of living with type 2 diabetes in Pakistan: the role of culture and family in physical activity. Int J Equity Health. 2022;21(1):103. doi:10.1186/s12939-022-01706-4
36. Schacter GI, Leslie WD. Diabetes and osteoporosis: part i, epidemiology and pathophysiology. Endocrinol Metab Clin North Am. 2021;50(2):275–285. doi:10.1016/j.ecl.2021.03.005
37. Napoli N, Chandran M, Pierroz DD, et al. Mechanisms of diabetes mellitus-induced bone fragility. Nat Rev Endocrinol. 2017;13(4):208–219. doi:10.1038/nrendo.2016.153
38. Kurra S, Fink DA, Siris ES. Osteoporosis-associated fracture and diabetes. Endocrinol Metab Clin North Am. 2014;43(1):233–243. doi:10.1016/j.ecl.2013.09.004
39. Mohsin S, Baniyas MM, Aldarmaki RS, et al. An update on therapies for the treatment of diabetes-induced osteoporosis. Expert Opin Biol Ther. 2019;19(9):937–948. doi:10.1080/14712598.2019.1618266
40. Reid IR, Bristow SM, Bolland MJ. Calcium supplements: benefits and risks. J Intern Med. 2015;278(4):354–368. doi:10.1111/joim.12394
41. Corsetti M, Brown S, Chiarioni G, et al. Chronic constipation in adults: contemporary perspectives and clinical challenges. 2: conservative, behavioural, medical and surgical treatment. Neurogastroenterol Motil. 2021;33(7):e14070. doi:10.1111/nmo.14070
42. Van Oudenhove L, Vandenberghe J, Demyttenaere K, et al. Psychosocial factors, psychiatric illness and functional gastrointestinal disorders: a historical perspective. Digestion. 2010;82(4):201–210. doi:10.1159/000269822
43. Gonzalez JS, Tanenbaum ML, Commissariat PV. Psychosocial factors in medication adherence and diabetes self-management: implications for research and practice. Am Psychol. 2016;71(7):539–551. doi:10.1037/a0040388
44. Bouchoucha M, Fysekidis M, Deutsch D, et al. Biopsychosocial model and perceived constipation severity according to the constipation phenotype. Dig Dis Sci. 2021;66(10):3588–3596. doi:10.1007/s10620-020-06654-z
45. Owens-Gary MD, Zhang X, Jawanda S, et al. The importance of addressing depression and diabetes distress in adults with type 2 diabetes. J Gen Intern Med. 2019;34(2):320–324. doi:10.1007/s11606-018-4705-2
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk Factors Analysis and the Establishment of Nomogram Prediction Model of Hidden Blood Loss After Total Hip Arthroplasty for Femoral Neck Fracture in Elderly Women
Hong WS, Zhang YX, Lin Q, Sun Y
Clinical Interventions in Aging 2022, 17:707-715
Published Date: 4 May 2022
Development and Validation of a Model That Predicts the Risk of Diabetic Nephropathy in Type 2 Diabetes Mellitus Patients: A Cross-Sectional Study
Yang J, Jiang S
International Journal of General Medicine 2022, 15:5089-5101
Published Date: 20 May 2022
Development of Risk Prediction Model for Muscular Calf Vein Thrombosis with Acute Exacerbation of Chronic Obstructive Pulmonary Disease
Hu X, Li X, Xu H, Zheng W, Wang J, Wang W, Li S, Zhang N, Wang Y, Han K
International Journal of General Medicine 2022, 15:6549-6560
Published Date: 10 August 2022
A Nomogram for Predicting Vision-Threatening Diabetic Retinopathy Among Mild Diabetic Retinopathy Patients: A Case–Control and Prospective Study of Type 2 Diabetes
Ke J, Li K, Cao B
Diabetes, Metabolic Syndrome and Obesity 2023, 16:275-283
Published Date: 27 January 2023
Applying a Combined Model to Evaluate the Risk of Poor Treatment Outcomes in Rifampicin Resistant Tuberculosis Patients: A Multicenter Retrospective Study
Yang Y, Chen J, Liu L, Li L, Yang R, Lu K, Qiu Y, Yang X, Xu L
Infection and Drug Resistance 2024, 17:5287-5298
Published Date: 29 November 2024