Back to Journals » Patient Related Outcome Measures » Volume 10
Development and validation of a patient-centered outcome measure for young adults with pediatric hip conditions: the “Quality of Life, Concerns and Impact Measure”
Authors Gambling T ![]() , Long AF
, Long AF ![]()
Received 30 October 2018
Accepted for publication 17 April 2019
Published 28 June 2019 Volume 2019:10 Pages 187—204
DOI https://doi.org/10.2147/PROM.S192672
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lynne Nemeth
Tina Gambling,1 Andrew F Long2
1School of Healthcare Sciences, College of Biomedical and Life Sciences, Cardiff University, Cardiff, UK; 2School of Healthcare, University of Leeds, Leeds, UK
Purpose: To develop and validate a patient-centered, evaluative outcome measure to assess patient-significant and identified impacts of the three pediatric hip conditions (the “Quality of Life, Concerns and Impact Measure” (QoLC&I)), for use by patients and clinicians in discussions over treatment options and the evaluation of treatment and post-operative rehabilitation.
Patients and methods: The measure was developed through a qualitative study, via two web-based forums (patient narratives, n=84) and one specialist orthopedic adult hip clinic (conducting interviews, n=38). The draft (1) measure was piloted in an asynchronous web-based discussion group forum; following revision, it was piloted with a group of clinicians and patients to assess its patient and clinical utility, face and content validity. The final, refined prototype measure (QoLC&I, draft 3) was subjected to psychometric evaluation.
Results: A total of 230 patients provided useable data for the psychometric analysis: 70% (160) had a confirmed diagnosis of Developmental Dysplasia of the Hip, 15% (35) Perthes, 11% (26) Slipped Upper Femoral Epiphyses; 4% (9) PHC not stated. The scale showed good acceptability (few missing items, good spread, low floor/ceiling effects), relevance (76% stating they would find the measure useful in their discussions with clinicians), and good internal consistency (Cronbach’s α=0.98; average ICC=0.98). Hypotheses on convergent validity (with the General Health Questionnaire, to measure depression, and the International Hip Outcome Tool Short Form, to measure quality of life) and divergent validity (with the General Self-Efficacy Scale, to measure coping) were confirmed.
Conclusion: The 64-item QoL&CI measure is a practical and valid measure addressing areas of clinical and patient significance and has potential value to assist patients and clinicians in discussions about treatment choices and treatment progress. Future research will address further psychometric testing (test–retest validity and responsiveness to change), in additional sites, and embedding the measure into clinical practice.
Keywords: Developmental Dysplasia of the Hip, Perthes disease, Slipped Upper Femoral Epiphyses, psychology, osteoarthritis
Introduction
Pediatric hip conditions
The three main pediatric hip conditions (PHCs) Perthes, Developmental Dysplasia of the Hip (DDH), and Slipped Upper Femoral Epiphyses (SUFE) are all recognized as causes of early degenerative hip osteoarthritis in adults. Many PHC patients will end up with painful arthritis at some stage in their adult life and, if not identified early on, may require a hip replacement at a young age. In DDH, the hip socket is too shallow, and the femoral head is not held tightly in place, so the hip joint is loose. In severe cases, the femur can come out of the socket (dislocate). This results in a mechanical overload of the anterolateral acetabular rim and labrum. The clinical diagnosis of DDH is confirmed by sonographic imaging (in the first months of life), while late presenting pathological DDH (>6 months of age) is usually diagnosed by an X-ray(s) of the pelvis. Dysplasia, subluxation, and dislocation of the hip joint are often associated with the development of premature osteoarthritis (OA) in young adults.2 Perthes disease occurs when the blood supply to the head of the femur (thighbone) is temporarily disrupted. Without an adequate blood supply, the bone cells die, a process called avascular necrosis and the head of the femur then becomes mis-shaped. The condition is most commonly found in children between the ages of 4 and 8, but it has also been identified in children and adolescents between the ages of 2 and 15.1 In the long term, the mis-shapen femoral head can remain so that it produces a permanent deformity, which increases the risk of developing osteoarthritis in adults1 Slipped Upper Femoral Epiphysis is a condition that happens in late childhood/early adolescence; in this condition, the epiphysis of the femoral head displaces or slips out of alignment from the rest of the femur. The longer-term implications of this happening are that there is a change in shape of the hip joint.
It is widely accepted that, for PHCs, an early diagnosis is most beneficial, but many cases go undetected until later childhood, adolescence, or early adulthood. This can result in a lifetime of significant long-term morbidity, including gait abnormalities, chronic pain, and premature degenerative arthritis of the hip and leads to a number of very invasive surgeries.3 In essence, all three conditions can lead to premature arthritis of the hip in later years. The extent of OA depends on how severely the shape of the hip joint is altered by the disease. All the PHCs are complex conditions that are often hard to diagnose, and later early adult manifestation can lead to prolonged disability. Patients will frequently present with symptoms in adolescence or young adulthood, although sometimes they present at older ages, in their 40s or 50s. Unless the PHC is diagnosed promptly, patients will experience pre-arthritic symptoms associated with anterolateral labral tears and synovial cysts which eventually progress to articular cartilage degeneration, unless the hip joint mechanics are corrected by surgical intervention2 The disease progression from pre-surgery presentation, through to corrective surgery to post-surgery and extensive periods of rehabilitation can have serious health implications for the young population affected by these conditions. Corrective surgery for these conditions is very invasive followed by a long period of rehabilitation.
The treatment of arthritic hip disease in young patients is a rapidly evolving area. Surgical acetabular reorientation is the most common surgical approach and can optimize femoral head coverage, decrease articular cartilage loading, delay or prevent the development of secondary osteoarthritis, and enhance patient function and activity2 Treatment is most successful during the early arthritic phase of the disease; thus, early diagnosis is important. However, Nunley2 found that patients with DDH were taking an average of 5.1 years to be diagnosed, by which time symptoms become more profound. If arthritis has progressed, then the options for treatment become more limited. Most commonly, the only option is to replace the hip, which for young patients can mean further revisions throughout their life and can also cause significant psychological distress.3
Surgery is often very invasive, and patients can expect to be walking with crutches for 8–12 weeks followed by a prolonged period of rehabilitation. The rehabilitation process is difficult, and it can take up to one year for a patient to fully feel the benefits of surgery. Treatment of borderline cases is also controversial. Hip arthroscopy has often been the chosen treatment, but it carries a high risk of reoperation. A broad range of surgeries now exists, but no comparison studies have been conducted to look at their effectiveness. There is great uncertainty about the effectiveness of treatment, compounded by lack of agreement about which outcomes should be measured. Very few studies exist that focus on the patient experience of surgery and recovery and rehabilitation.
We know very little about the quality of life (QoL) and psychological impact of PHCs. If left undetected or untreated, they may lead to significant pain and functional problems which will greatly impact on everyday life (for example, ongoing pain, effect on exercise, family and social life) and QoL.4,5 For some, this will lead to profound disability associated with progressive hip degeneration and eventual end-stage disease. Additionally, little research has been conducted on the impact of adult hip conditions focusing on early presentation and symptoms.
The impact of the conditions throughout presentation, diagnosis, treatment, and longer-term effects on patient QoL can be quite significant. For example, patients can face a lifetime of uncertainty as to what the longer-term effects of hip dysplasia are. Long-term studies of surgical treatment for DDH have shown that periacetabular osteotomy (PAO) can last for up to 20 years if the patients had no cartilage damage at the time of surgery. In these studies,6–9 failure was defined as revision to a total hip replacement (THR) and many PAO’s do not last as long as 20 years. What is not clear from the literature is the long-term impact on a patient’s physical and socio-psychological well-being in their everyday life.
Measuring PHC outcomes
Careful selection of meaningful outcome measures is crucial in conducting clinical trials to include outcomes that matter to patients. A recent systematic review of the efficacy of PAO’s highlighted that there was a lot of variance in the way that studies reported clinical outcomes.10 This study highlighted that progress in this field is dependent on measuring accurate, clear, and consistent outcomes which in turn is dependent on the development of new validated, patient-based outcome measures. This would allow more precise and wide-ranging analysis of clinical improvement. In young adult hips, operative success has been measured by using objective measures such as radiologic imaging which measures the anatomical variation in the hip and how it varies from normal and deformity correction after surgery, improvements in range of motion are also measured.11 Additionally, standardized hip outcome scores are frequently used in the literature including the modified Harris Hip Score (mHHS), Hip Outcome score Activities of Daily Living (HOS-ADL), HOS-Sport-Specific Subscales (HOS-SSS), 12-item Short Form Health Survey (SF-12), and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC).12–15 The scores have all been validated for assessing advanced OA in a much older population, but they may not be fit for purpose in a young adult hip population. Young adults often have higher physical activity expectations and outcomes will vary. For example, being able to simply complete daily activities of life may not be deemed a positive outcome in young adults.15–17 These measures do not always embrace high impact activities that young adults will demand of their hips post-operatively.15–17
For patients undergoing hip preservation surgery, patient-reported outcome (PRO) measures are becoming an integral part of measuring the efficacy of treatment. Ramisetty et al18 conducted a systematic review, their specific aim was to critically appraise the quality of PRO’s in order to recommend the most appropriate PRO tool(s) for future use. They included studies which compared patients with a variety of hip conditions, and surgical methods used to treat the conditions, including arthroscopy and surgery for dysplastic and non-dysplastic hips. Six PRO tools from ten articles were identified. The most recently developed PRO tools - the hip outcome score (HOS), the Copenhagen hip and groin outcome score (HAGOS) and the International Hip Outcome Tool (iHOT-33) - scored better than the others. The iHOT-33 scored best of all the PRO tools, and they recommended it for future use in hip preservation surgery. The iHOT-33 was developed with the cooperation of the multi-center arthroscopy of the hip outcomes research network (MAHORN) and it was designed to measure the outcomes of treatment in young active patients with hip disorders (18 or older and up to 60 years old). However, this measure has primarily been used in patients undergoing arthroscopy. Many would argue that these patients are not as debilitated as patients with more severe hip dysplasia, Perthes, and SUFE who are undergoing osteotomies. It is also noticeable that psychological impact is not measured in any of the measures reviewed in this study despite this being a significant factor for adult patients with a PHC.4
Broader outcome measures used in hip studies
Sim et al (2015)19 conducted a systematic review to evaluate the reporting of non-hip score outcomes following surgical management of femora-acetabular impingement (FAI). Patients diagnosed with hip dysplasia and Perthes can also have impingement. The most common non-hip score outcomes reported included: patient satisfaction (72.7%), symptom improvement (24.7%), pain improvement (12.4%), hip range of motion (12.3%), and return to sport (6.8%)19 What is interesting about this study is that a discrepancy exists between what outcomes the literature suggests should be reported and what outcomes are often reported. For example, “return to sport” is often held as a major patient-important outcome yet it is rarely reported in studies assessing the efficacy of FAI surgery. This systematic review highlighted differences between what patients consider to be an important outcome and non-hip score outcomes reported in the literature.19 Impellizzeri et al20 also found that “reduction in hip pain” was the most cited reason for pursuing surgery, followed by ability to “return to sport”. This lends further credence to the need for outcome measures focused on young people which measure aspects important to their needs and can be incorporated clinical trials. Although most research in hip dysplasia has focused on pain and function, there has been a recent and growing interest in measuring the real-world impact on patients through broader assessments of QoL. Several studies have focused on the emerging area of movement and movement analysis21 Movement analysis provides an objective examination of hip mechanics in the patient and therefore measures different aspects of the effects of hip dysplasia. Problems with walking have been documented in patients with untreated hip dysplasia.21–24 This can have a significant impact on patients as they will walk with a defined limp and abnormal-appearing posture. However, its physical and psychological impact and impact on body image are to date unexplored.
Hip pain itself may prevent participation in social, recreational, and sports activities and directly impact QoL. Numerous studies on outcomes after PAO focus on instruments of QoL and hip function such as the WOMAC and the Harris Hip Score.17 Although these instruments provide information about patients’ functional limitations and pain, they do not directly assess activity level and sports participation. Patients who participated in sports before surgery may wish to resume their activities after surgery. The “wish to return to recreation” often is cited by patients with hip pain as an important component of their disability.25 There is limited evidence, to date, regarding the physical activity levels patients can expect to achieve after surgery and which factors may affect resumption of or improvement on preoperative activity levels. Simple scores from a questionnaire may not give the full picture as patients may change activities by reducing impact sports. For example, Klit et al26 studied activity in patients with hip dysplasia seven years after PAO. The relatively low visual analog scores together with the relatively low score in the dimensions “sport and recreation” and “participation” may indicate that the patients reduce their sport activities and participation after PAO to minimize their symptoms, but at a psychological price, involving trying to manage expectations.
There is also limited research considering broader aspects of QoL post-surgery. For example, “return to work” was studied in only one study27 This paper also considered that “limb length discrepancy” was an important factor for patient morale, motivation, and post-operative satisfaction. Some research28 has been conducted considering “insomnia and sleep” and their overall impact on QoL. Gambling and Long (2013),3 in their qualitative studies, also found that many patients struggled with their body image and self-esteem if there were long delays in diagnosis. Currently, measures do not exist which consider this global impact of PHCs in young adults. Furthermore, Perthes, with its occurrence in very young children, is a challenging area for instrument development; however, work is being conducted to develop an outcome measure for children with Perthes.29
In summary, little is known about the psychological, economic, and personal impact of pediatric hip conditions.30 This lack of evidence makes it very difficult to assess patient need and evaluate treatments that best support patients. Whilst it is known that surgery can provide pain relief and improve hip function, the availability and use of an appropriate outcome measure focused on patient concerns and the potential impact of hip dysplasia on a broad range of factors, including pain, psychological health, social and familial impact, and QoL, would potentially improve treatment experience and patient–clinician interactions and provide an additional tool to use within the evaluation of clinical practice.
This paper reports on the development of an outcome measure to assess the patient-significant and patient-identified impact of PHCs. The aim was to develop a patient-centered,31 evaluative32 outcome measure for pediatric hip conditions (the “Quality of Life, Concerns and Impact Measure” - QoLC&I) to be used by both patients and clinicians in discussions over treatment options and the evaluation of treatment and post-operative rehabilitation. Our guiding criteria were multiple, for the measure: to be based on the patient’s perspective and thus be user-centered; to have clinical utility and feasibility to use in clinical practice; and to have good psychometric properties (reliability, validity, and responsiveness to change). Appendix 1 summarizes the detail of our requirements.33,34,35 For a measure to be used in practice, it must also be of perceived high relevance to patients’ concerns and useful for them and clinicians.31 Our measure has been designed to do this and is based on previous qualitative research. The implementation of the outcome measure would enable a clearer picture of the QoL impact and wider social and psychological impact on pediatric hip conditions.
The measure is intended to add insight into physical, social, psychological, self-esteem and QoL factors of importance to patients and widen understanding about both patient treatment responses and factors that patients’ value. As outlined above, limited knowledge of the socio-psychological and QoL effects of these conditions results in a clinical emphasis on physical/functional problems, without consideration of the wider social and psychological impact. The implementation of the outcome measure would enable a clearer picture of the QoL impact and wider social and psychological impact on PHCs. An overview of the study design for the development and validation of the measure is presented in Figure 1.
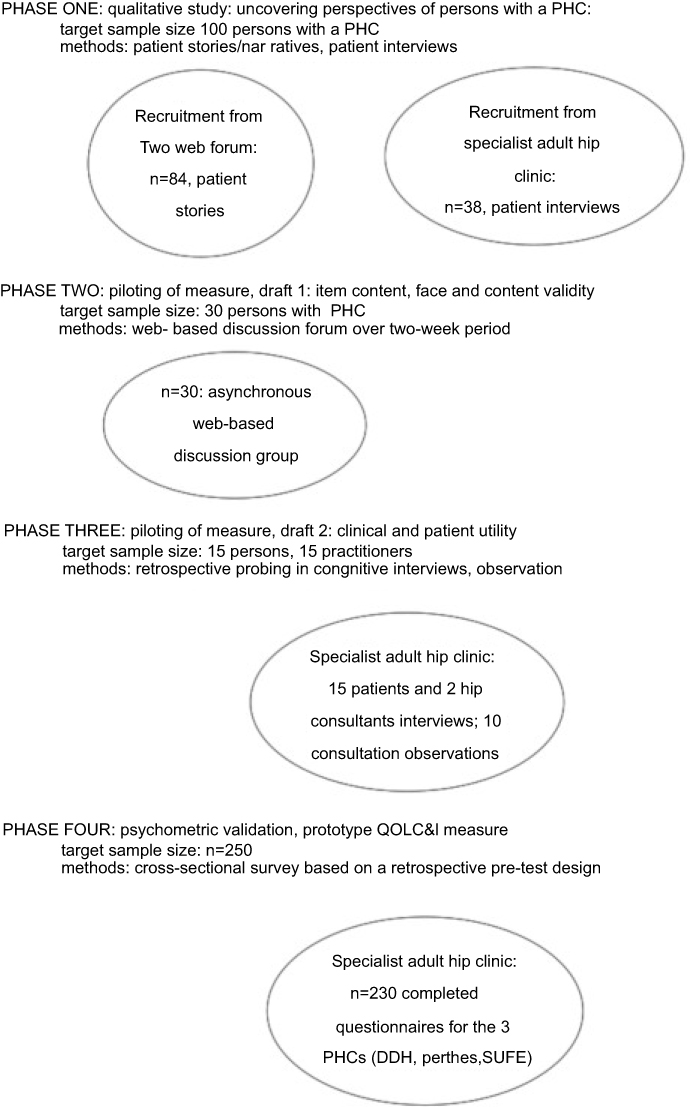 |
Figure 1 Overview of development and validation study design. Abbreviations: QOL, quality of life; QOLC&I, quality of life concerns and impact; DDH, developmental dysplasia of the hip; SUFE, slipped upper femoral Epiphyses. |
Methods
Development phase
A qualitative study was conducted (2013-early 2015), drawing on two sources: two web-based forums (using patient narratives) and a specialist orthopedic adult hip clinic (conducting interviews).
Participants were carefully selected, using the principle of diversity from the web sources. The use of two websites enabled diversity, allowing access to participants from a wider geographical area, some being close to specialist centers and others much further away; this would influence the nature and possibly quality of the care they had or were receiving. In addition, we were potentially able to recruit patients internationally, from the USA, Australia, and Europe. Recruiting from one specialist adult hip clinic (in the Royal Orthopaedic Hospital NHS Foundation Trust, Birmingham) enabled insight into the perspective of patients who were receiving the best care.
The aim was to recruit around 100 participants from the two sources and to ensure variability in time of first diagnosis (childhood or adulthood), clinical presentational time (pre or up to 12 months post-operative), and treatment stage (preventive, “to save my joints” or treatment following points of failure). By carefully selecting participants to ensure the potential for the expression of different experiences, such a sample size was expected to capture the required depth and richness of data. Ethical approval was given by Cardiff University Ethics Committee for the websites and NHS Ethical Committee (the Royal Orthopaedic Hospital NHS Foundation Trust) for the specialist clinic; the latter committee deemed the study as evaluation and thus as part of clinical practice development.
Inclusion criteria were
- Women and men with a confirmed diagnosis of DDH, Perthes, or SUFE
- Having an extensive DDH-, Perthes-, or SUFE-related treatment history following diagnosis in childhood/adolescence or newly diagnosed as young adults or following a recurrence/new symptom
- Aged 18 or over
- English speakers
- Active member of one of the two web forums/or attending the specialist orthopedic hip clinic.
Patient recruitment
To recruit participants from the web sources, the site moderators were asked if they would allow access to their sites. Once agreement was ascertained, a message was posted on the websites seeking volunteers who fitted the research eligibility criteria. The message directed interested persons to a secure University of Cardiff-hosted website where further information about the research project was posted. Participants completed an electronic consent form, which included their e-mail contact details. Participants were then asked to complete a simple screening questionnaire. If they fitted the study criteria, they were invited to write a narrative about their experiences, covering, for example, their diagnosis, treatment history, treatment experiences and impact of the PHC on their lives and sense of self and feelings about the future. To assist their story writing, an indicative structure36,37 was provided of key areas to frame their story around, while encouraging them to write up their personal history in any way that they wished.
In the specialist hip clinics, patients were recruited via the consultant hip surgeon who applied the inclusion criteria, dividing planned clinic consultations by type of visit (discuss treatment options, follow-up 6 weeks to 24 months post-treatment). The appointment clerk in each site sent consecutive patients meeting the inclusion criteria a participant information sheet, consent pro forma and, for the later part of the study, the draft outcome measure. Patients willing to take part in the study were asked to bring the completed consent pro forma and, where relevant, the completed outcome measure to their next clinic appointment. Data were collected on 84 patients through the websites and 38 patients from the clinics.
Data analysis
Data were analyzed in a thematic manner, exploring participants’ meanings surrounding particular experiences, events, and states. A set of emerging themes (Figure 2) provided the basis for an initial model specification. These areas highlighted the impact of the condition and their concerns. They covered pain, physical activity, work, family and social impact, psychological impact, and overall QoL.
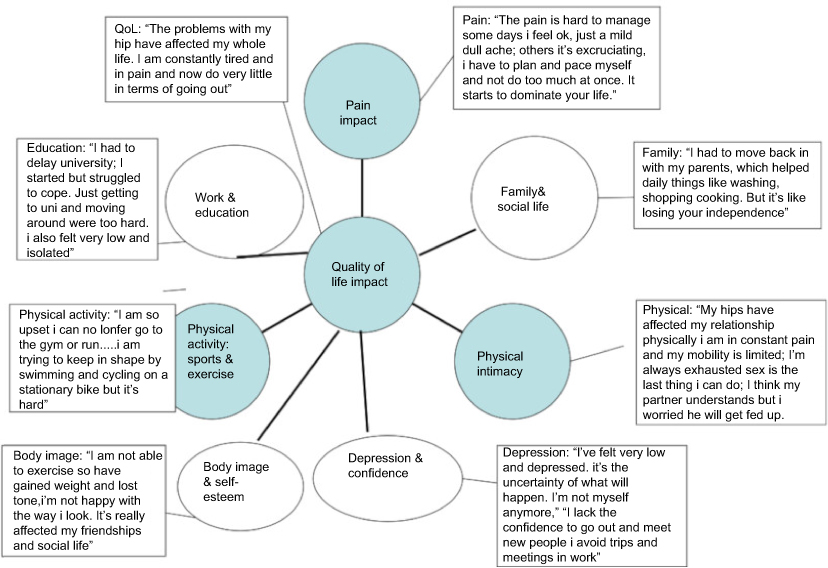 |
Figure 2 Emerging themes and illustrative extracts. |
The topic areas, or domains, were translated into questions, built around a five-level Likert scale, and a draft measure developed and then piloted. Firstly, the draft (1) measure was piloted with a subset of the online recruited participants (n=30), using an asynchronous38 web-based discussion group design, asking them to comment on the ease of understanding of its content, accessibility of language, ease of completion and coverage, including missing or suggested additional areas and question phrasing. The asynchronous nature meant that participants did not have to be present at the same time. Participants contributed their comments by responding to the initial discussion question or by responding to each other. All these responses were shown in the form of an outline or thread so that responses appeared following the entry to which they were replying. This discussion took place over a defined two-week period and was moderated by one of the research team (TG). Working together with the participants, enabling co-construction of the measure, ensured the patient-centered focus of the measure. The results of the pilot were analyzed with a view to refine the form, mode, and coverage of the questions within the measure in order to develop a revised outcome measure (draft 2) for psychometric validation.
Second, this refined measure (draft 2) was piloted with both a group of clinicians and patients to assess its patient and clinical utility. The rationale for this further piloting related to the notion that, the more a measure focuses on aspects that matter to patients and to clinicians, the greater its validity, usefulness and likelihood of take-up by patients and into clinical practice. A target sample size of 5 practitioners and 15 patient interviews was set. Given the in-depth interview process, this sample size was sufficient to enable insight into the potential utility of the measure and ways to enhance this.39
In-depth interviews supplemented with observation were used. Patients attending for a consultation at the Birmingham specialist hip clinic were asked to: complete the prototype the “Quality of Life, Concerns and Impact Measure” (draft 2) measure prior to their clinical consultation; share the completed measure with the practitioner; and take part in a semi-structured post-consultation interview. To assess face and content validity, a sample of 20 patients took part. Each patient participant was interviewed using a semi-structured instrument, at the end of their consultation (if convenient to the patient) or take part in a telephone interview at an agreed date and time. The interview used retrospective verbal probing, an established approach within cognitive interviews,40,41 and recommended way to clarify the participant’s understanding of the items and use of a new instrument (DeWalt et al 2007).42 The interview explored: how their responses to the measure were used in the consultation; how useful/helpful they found this; how useful and relevant they found the items in the measure; perceived potential value of the measure in assessing/recognizing changes in their condition; and ways that the measure’s utility might be increased.
The practitioners were asked to: talk through the patient’s responses to the items in the measure, as relevant to the consultation’s focus; at consultation/clinic end, write down perceptions of the usefulness of the instrument in assisting in the discussion with the patient over treatment options for subsequent sharing with the research team; and take part in an open-ended interview at the end of patient data collection. One interview with each hip consultant was conducted sharing their earlier notes on the usefulness of the measure. The interview used “retrospective” verbal probing, exploring how they made use of the measure in the consultation in general and the potential value of the measure in assessing changes in symptoms and impact; and ways that the measure’s utility might be increased. Four practitioners, the only ones with whom the patients had a consultation, were interviewed.
To gain additional insight into how the consultants used the measure, a member of the research team observed a small number (10) of their consultations, with the patient’s permission. All interviews were audiotaped and transcribed, and field notes made for the clinic consultation observation. Directed content analysis43 was used, drawing on the core interview question headings, with an openness to additional areas, to summarize perceived utility, ways to enhance this and factors facilitating and inhibiting utility.
Following data analysis, a prototype (draft 3) measure was created ready for psychometric evaluation, based around the final conceptual model (Figure 3). The measure was targeted at persons with a PHC aged 16 years to 49 years.
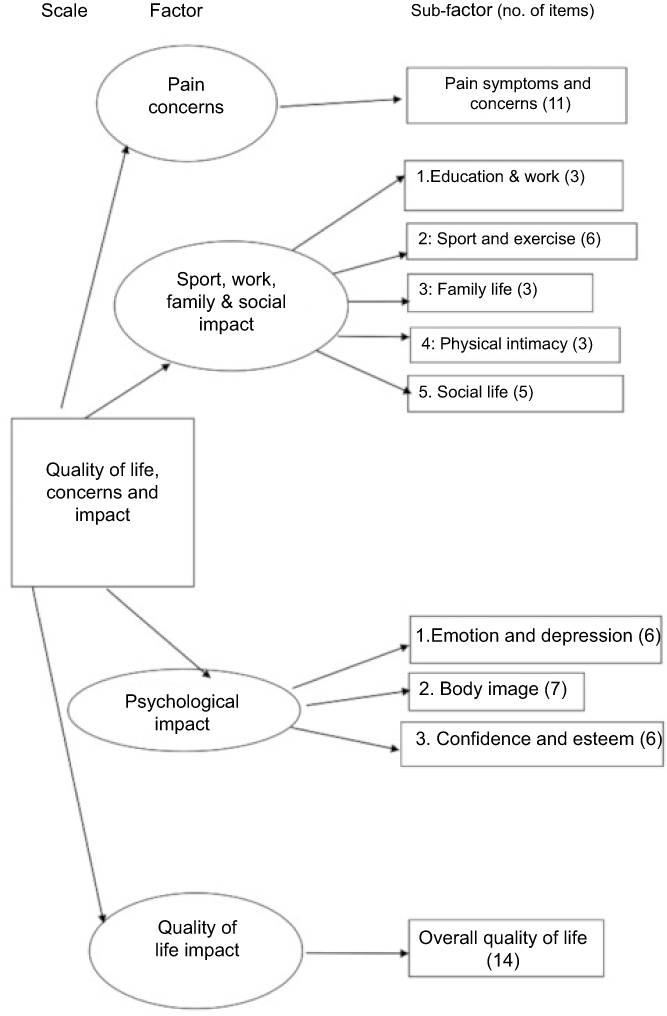 |
Figure 3 Model specification for the quality of life, concerns, and impact measure. |
Testing and validation phase
Study design
A cross-sectional survey based on a retrospective pre-test design was used to explore measure validity. Test–retest validity and responsiveness to change were left for latter evaluation, due to administrative difficulties in the hip clinic in following up and re-contacting respondents. The retrospective pre-test design allowed respondents to report on their contemporary and retrospective (3 months before), in one section relating to QoL from the same individual reference point (with the benefit of knowledge of how their condition had changed). This design is recognized as being realistic, feasible, efficient, and reducing the likelihood of missing data44 and of demonstrable value where interest lies in changes in health-related quality of life.45
To assess validity, a target sample size of 250 was set (125 for DDH; 125 for Perthes and SUFE together), calculated on the basis of recommended guidance on minimum number of cases (5) per item in the prototype measure and a 95% confidence interval for Cronbach’s alpha (reliability) coefficient of ≥0.746 and the measure having a maximum of 25–30 items. To ensure this target level was achieved, a 25% allowance for “not responding to invitation to participate” (participation rate) and a 25% allowance for subsequent “non-response to questionnaire completion” was made, leading to a sample size of around 375–400. NHS Ethical approval was provided by the Royal Orthopaedic Hospital NHS Foundation Trust Birmingham, and the research was conducted in the specialist hip in that site, over the time period, 2015–2016.
Recruitment process
Following informed consent and a signed consent form, the site’s research nurse gave each participant a copy of the questionnaire measure and, if necessary, a stamped addressed envelope to return the questionnaire to the research team. Patients were requested to complete the measure in relation to the hip they were currently receiving treatment for or, if both hips were symptomatic, the most problematic hip. Non-responders at this stage were sent, by the research nurse, one reminder letter only after two weeks, together with another copy of the questionnaire. Any non-responders after this were considered as refusals. The participants were asked to: complete the “Quality of Life, Concerns and Impact Measure” measure, together with short pro-forma seeking additional demographic (age, gender) and condition related data (height, weight, hip condition, length of time from the onset of symptoms to the definitive diagnosis).
Procedures and measures
The prototype measure had nine domains (Symptoms (11 items); Education and Work (3); Sports and Exercise (7); Family Life (3); Physical Intimacy (3); Social Life and Relationships with Others (5); Confidence and Esteem (6); Body Image (10); and Overall QoL (14)) and three open questions relating to hopes and fears and potential usefulness of the measure in discussions with their clinicians (see Appendix 2 for a copy of the measure). To assess practicality, respondents were also asked to rate the ease of completion and time taken to complete the measure.
To explore construct validity (convergent and divergent), all participants were also asked to complete some additional, validated tools which measured domains of the prototype measure. Patients’ self-esteem, body image, and feelings of self-efficacy and quality of life were explored, using the following measures:
- Depression: General Health Questionnaire (GHQ) (10 items)47
- Quality of Life: International Hip Outcome Tool (iHOT-12) (12 items)16
- Coping: General Self-Efficacy Scale (GSE).48
Psychometric analysis
Items were subjected to statistical examination, using IBM SPSS for Windows versions 19–23 (SPSS Inc. Armonk, NY, USA), to explore issue of acceptability and practicality (response rate, missing item proportions, relevance to treatment decision-making), item analysis (item redundancy), reliability (internal consistency), and convergent/discriminant validity (Appendix 1). Following redundancy analysis, the psychometric properties of the reduced item version were assessed.
Findings
Respondents
As Table 1 shows, the sample 230 persons comprised 160 (70%) persons with a confirmed diagnosis of DDH, 35 (15%) with Perthes and 26 (11%) with SUFE; nine (4%) of the respondents did not indicate which PHC they had). The age and gender variation by condition, were as expected,1,49 similar to other studies. For example, 44% of those with DDH were female and aged 20–<35 and 11% were female aged 16–<20. In contrast, 53% of those with Perthes were male and aged 20–<35, whereas for SUFE, half were male and half female. About half of those with DDH and SUFE were affected in one hip, either the left or right, and about twice as many of those with Perthes were unilaterally affected. About three-fifths (61%) of the sample were working full or part-time, 17% were in education (school, FE college, or university) and 12% were unable to work due to ill-health. Just over three-fifths (60–64%) were either deciding what treatment to have or waiting for treatment for their left or right hip and 42–44% waiting for or had joint conservation surgery. Between 9% and 18% of the sample had had a THR in either the right or left hip, a substantial proportion (35%, left hip; 31%, right hip) having a THR aged under 30.
 |
Table 1 Respondent characteristicsa |
Psychometric evaluation
Acceptability, practicality, and patient usefulness
The scale showed good acceptability. There were a number of questionnaires where the respondent, asked to complete the instrument while awaiting their outpatient hip appointment, had not had sufficient time to complete all the questions (approximately 20). Otherwise, there were very few missing items. There were low floor/ceiling effects (2 for the pain sub-sub-scale and 1 for sport and exercise), and the majority of sub-scales (6/10) had no extreme skewness. Exceptions were the pain, sports and exercise, social life, and overall QoL sub-sub-scales. There was also good spread over the range of the sub-scales and full scale (Table 2). Three-quarters of respondents (76%) indicated that they would find the measure useful in their discussions with clinicians (Table 2). For example, it gave the clinician insight into “the emotional and the physical,” “a better understanding of my lifestyle” and “its impact on my everyday life”. Around three-fifths (61%) of those who indicated that they would not find it helpful stated that “ít was too late” as their treatment was completed or “these (areas) have already been discussed”.
 |
Table 2 Accessibility, practicality, and data quality (n=230) |
Reliability
The measure had good internal consistency (Cronbach’s α =0.98; average ICC =0.98), as did the sub-scales (Cronbach’s α =0.95- 0.96; average ICC = 0.95-0.96) and each of the sub-sub-scales (Cronbach’s α =0.85–0.97; ICC =0.59–0.89) (Table 3). Test–retest reliability remains to be evaluated in the next stage of the study.
 |
Table 3 Factor analysis - internal consistency and reliability (n=230) |
Item analysis
Analysis of all the sub-sub scales indicated substantial loadings (67–93%) on all items in the one rotated factor solution, confirming their predicted uni-dimensionality. The one exception was the QoL sub-sub-scale, which had two factors; all items except for three (“I don’t feel good about myself”; “lost my life and identity”; “given up things I used to do and now have no normal life”) having high loadings on factor one (0.54–0.86) and the second comprising predominantly emotion-related items. The two sub-scales with multiple sub-sub-scale components, “sport, work, family and social impact” and “psychological impact” had, respectively, a three or two factor solution. For the former, the three factors were: impact on sports and exercise, impact on social relationships and education/work, and impact on family life and physical intimacy. For the latter, the two factors were impact on body image, and impact on feelings of self-worth and embarrassment. The full measure had a 10-factor solution, confirming the relevance and appropriateness of the sub-scale and sub-sub scale components, as indicated in the final model specification (Figure 2).
Convergent and divergent validity
Three validated outcome measures – GHQ, i-HOT-12 and GSE) – were used. Parts of our measure addressed psychological and emotion/depression and QoL impact; these would be expected to show evidence of convergent validity with both the GHQ and i-HOT-12. In contrast, divergent validity was assessed against the GSE, as it was not self-evident or plausible why a relationship, albeit but small, would be expected with the QoLC&I. As Table 4 shows, the predictions were fulfilled. The “psychological impact” sub-scale and the “QoL impact” sub-scales had, respectively, moderate convergent validity with GHQ and high convergent validity with the i-HOT-12. The GSE, assessing coping, was contrasted with the “psychological impact” and “sport, work, family and social impact” sub-scales; a low correlation was found for both. Together, these results provide supporting evidence for the convergent and divergent validity of the measure.
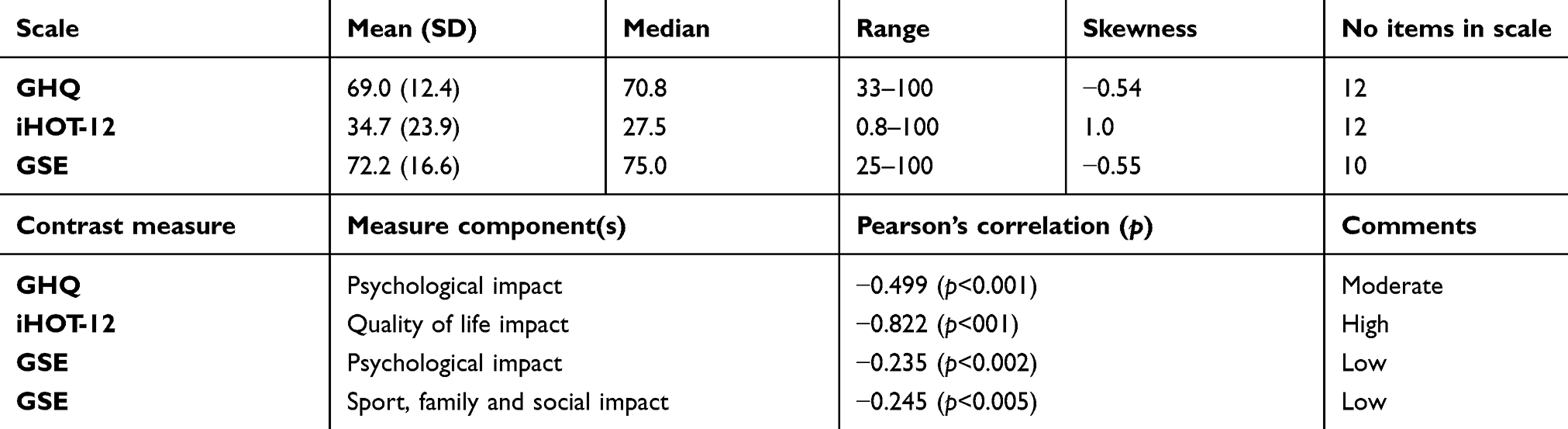 |
Table 4 Convergent and divergent validity (n=230) |
Discussion
The study has demonstrated that the 64-item QoLC&I measure, targeted at persons with a PHC aged 16–49 years, is acceptable to patients, has patient relevance, face and content validity, addresses areas of clinical importance, and is of potential value to both patients and clinicians in their interactions, discussions about treatment choices and treatment progress. The factor analysis shows good reliability (internal consistency) and provides supportive evidence of construct validity. Most importantly, the measure is grounded in the patient’s perspective, based on prior qualitative research by the authors. It priorities areas of importance and significance to patients with a PHC and is expressed in a set of understandable, and patient-derived and validated, Likert-type questions. Two validation areas remain to be explored - test–retest validity and responsiveness to change; both will form part of our next research study. It is also our intention and at the request of the hip clinicians in our research site at Birmingham to embark on a program to embed the current measure into clinical practice, studying these two outstanding validation aspects alongside.
A major purpose behind the design of our measure was to create a measure directed specially to patients with a PHC, in contrast to other measures, for example, those reviewed by Ramisetty et al,18 and one with good coverage of areas (domains) identified as important and significant to patients. The mode of administration, via a self-completed questionnaire in a paper or Word format, supports easy and non-time-consuming completion and facilitates the feasibility and ease of clinical administration. Furthermore, the language that the measure is written in has been both derived from, and validated by, patients and confirmed as clinically relevant by a set of clinicians in the study site.
The four sub-domains (sub-scales) cover a wide set of substantive areas, all of importance to patients. This set - pain concerns; sport, work, family and social impact; psychological impact; quality of life impact - has a broader coverage of key patient concerns than all other existing measures, including HAGOS and the iHot-12. This breadth is important, as it encompasses the perspective of the patient with a PHC; moreover, it provides clinicians with insight into patient concerns and the impact of the PHC on their everyday family life, social relationships, and QoL.
The development of the measure, and its subsequent emergent validation, provides further evidence on the severity and impact of PHCs on patients and their families in their everyday lives. It also makes it clearer that impact is not just on QoL, unlike the iHOT-12/33. As noted earlier, the iHOT-33 was developed to address the concerns of young adult patients with hip disorders but has primarily been used in patients undergoing arthroscopy.4946 In contrast, patients with PHCs are often much more severely affected by their condition and the surgery is infinitely more invasive and a much longer recovery period. While mobility and pain have been measured previously in these patients (for example, in research studies using WOMAC, mHHS, and HOS-ADL), our measure also considers the effect and concerns about impaired mobility and pain, impact on self-esteem and body image, along with other areas. Again, specific measures exist that focus specifically and in detail on both constructs (for example, the Rosenberg self-esteem scale,50 The Body Image Disturbance Questionnaire BIDQ).51,52 However, these issues, for those with a PHC, also have a psychological impact on patients and also affect their social networks and ability to study or work. Our measure, unlike the i-HOT-12, explores psychological impact, as one core domain, along with impact on work/education and overall QoL.
The qualitative work ensured that the measure was patient-centered and covered areas that patients felt were important. There were some important differences to other measures described in the literature review within arthritis, for example, less emphasis on pain and function and greater emphasis on self-esteem and body image. It is evident from our work that issues surrounding self-esteem and body image can arise specifically in patients with PHCs, related to the difficulties they have with mobility and posture. In addition, such patients are much younger than those who traditionally suffer from arthritis. They are mainly aged 18–40. Any chronic illness is likely greatly to affect education, work, family, and social life and more so than for older adults. Due to societal pressures to conform to social and physical stereotypes, PHC patients are also more likely to suffer self-esteem, confidence, and body image issues. Their psychological impact is likely to be profound and to affect several psychological constructs, including emotion and depression, body image, confidence, and self-esteem. PHC patients are more likely to display these psychological effects as they face life-changing events such as going to university, starting work and having children.
The measure was developed to be used alongside other clinically focused measures in clinical trials or longitudinal outcome studies. Use of the QoLC&I in these studies would facilitate a better understanding of this patient group and gain additional insight into the physical and psychological impact of PHCs. Further knowledge of the psychological impact of PHCs would encourage development of psychological interventions to support patient recovery. Following further validation, the QoLC&I measure could also be used to identify patients who had become physically or psychologically impaired. As the management of painful borderline dysplastic hip is an issue of great controversy and is common in young adults with hip pain (a reported prevalence of 37.6% in selected patient hip dysplasia cohorts)53 our measure might support decision making, with such cases.
Knowing the overall impact that a PHC has on the individual, physically and socially and psychologically, would help to inform decisions about treatment options and type of surgery. Clinicians in our study who have used the measure reported that it helped support conversations with patients about QoL, psychological impact, and socio-economic impact. It was also easy to use and could be completed before a consultation and then discussed within the consultation. Moreover, patients liked using the measure as it prompted clinicians to ask about wider issues. Future work needs to consider in detail how the measure informs decision making.
Study strengths and limitations
The study has a number of strengths. First, the development of the measure was based on our previous DDH qualitative studies,3,4 which explored participants’ experiences from their stories about their everyday life with DDH and piloting of the emerging measure with a subset of these participants. Second, the refined measure was further piloted with a set of clinicians in the research site in relation to clinical utility and feasibility of use in routine clinical practice. Third, an adequate sample size was achieved for the development and psychometric validation of the measure.
The study also has a number of limitations. First, participants in the qualitative study were self-selecting, responding to requests for participants on the web forums. It could be the case that the more vocal and potentially wishing to put forward strong views were more likely to take part. Second, there was potential self-selection in terms of who might seek, join, and make use of the web forums, as a source of support and advice. The bias effect of both of these cannot be assessed. Recruitment from dedicated PHC web forums is one of the few ways to access a diversity of participants; moreover, web forums are becoming a common and well-utilized mode for persons with a particular ill-health condition to gain insight into others’ experiences and as a source of support and advice.54,55,56 Thirdly, the validation study was conducted in a single, specialist hip site, and valuably one where patients with one of the PHCs were referred to for specialist treatment. Interpretation of the study findings should take heed of these limitations. Further validation, in particular of test–retest validity and responsiveness to change, in additional specialist hip clinics would be valuable.
Further research
Further research areas include psychometric evaluation in additional specialist hip clinics, extension of the evaluation to explore test–retest reliability and responsiveness to change, and embedding the final measure into routine clinical practice, especially in secondary specialist care and rehabilitation. Additionally, the study’s findings could valuably be disseminated into primary care, to extend the insight of GPs and physiotherapists to PHCs and significant issues of key importance to persons with a hip condition, with subsequent study of its impact. At present, it is evident from our qualitative study that such persons are often wrongly perceived as, for example, having a groin strain or their symptoms being part of the maturity process, and thus often dismissed and inappropriately treated; this has significant impact on the delays to definitive diagnosis and referral to specialist hip treatment and care.2,3,4
High-quality clinical research in PHC orthopedic surgery is beginning to emerge, previously predominantly being observational case series.53 One of the barriers to developing randomized controlled trials in this area is a paucity of robust outcome measures that access the range of desirable outcomes, thus the potential significance of our QoLC&I measure, and its capturing outcomes that are meaningful to the patient population and consider the wider impact of the conditions. Perry et al57 identified several priority areas that hip surgeons considered of high importance to study. All three PHCs featured among these priorities. For example, one aspect was phrased as “what are the current approaches used in the management of late presenting hip dysplasia in infants, and how may differences in treatment choices influence outcomes?” For research to be beneficial to the patient group more meaningful outcome measures will need to be developed, for example, in Perthes where we, with colleagues in Liverpool, have been developing and testing a young-child friendly and self-completed measure.28
Conclusion
Patient-related outcomes measures should correspond to specific clinical situations and bring the opportunity to improve quality of care.58 An outcome measure must not only demonstrate the expected methodological properties and performance but also offer a positive contribution to patient care. The study has demonstrated that the 64-item QoLC&I measure is acceptable to patients, has patient relevance, addresses areas of clinical importance, and is of potential value to both patients and clinicians in their discussions about treatment choices and treatment progress. Most importantly, the measure is grounded in the patient’s perspective, based on prior qualitative research. It priorities areas of importance and significance to patients with a PHC and is expressed in a set of understandable, and patient-derived and validated, Likert-type questions. Measuring these important outcomes will enable us to learn more about the overall impact of PHC and facilitate the development of interventions which are focused on addressing the broader impact of the condition. Further work should focus on further psychometric testing and embedding the measure into clinical practice.
Acknowledgments
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Cardiff University, and NHS ethical approval, UK.
Informed consent
Written informed consent was obtained from all subjects before the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nelitz M, Lippacher S, Krauspe R, Reichel H. Perthes disease: current principles of diagnosis and treatment. Dtsch Arztebl Int. 2009;106(31–32):517–523.
2. Nunley RM, Prather H, Hunt D, Schoenecker PL, Clohisy JC. Clinical presentation of symptomatic acetabular dysplasia in skeletally mature patients. J Bone Joint Surg Am. 2011;93(2):17–21. doi:10.2106/JBJS.J.01735
3. Gambling T, Long AF. Experiences of young women living with developmental dysplasia of the hip: insight into their experiences of surgery and recovery. Chron Ill. 2013;9(1):16–28. doi:10.1177/1742395312450177
4. Gambling T, Long AF. An exploratory study of young women adjusting to developmental dysplasia of the hip and deciding on treatment choices. Chron Ill. 2011;8(1):17–30. doi:10.1177/1742395311417638
5. West S, Witt J. A patients Journey - Bilateral developmental dysplasia of the hips. BMJ. 2011;342:
6. Clohisy JC, Barrett SE, Gordon JE, Delgado ED, Schoenecker PL. Periacetabular osteotomy for the treatment of severe acetabular dysplasia. J Bone Joint Surg Am. 2005;87(2):254–259. doi:10.2106/JBJS.D.02093
7. Clohisy JC, Barrett SE, Gordon JE, Delgado ED, Schoenecker PL. Periacetabular osteotomy in the treatment of severe acetabular dysplasia: surgical technique. J Bone Joint Surg Am. 2006;88(1 suppl pt 1):65–83. doi:10.2106/JBJS.E.01302
8. Clohisy JC, Nunley RM, Curry MC, Schoenecker PL. Periacetabular osteotomy for the treatment of acetabular dysplasia associated with major aspherical femoral head deformities. J Bone Joint Surg Am. 2007;89:1417–1423.
9. Millis MB, Kain M, Sierra R, et al. Periacetabular osteotomy for acetabular dysplasia in patients older than 40 years. Clin Orthop Relat Res. 2009;467(8):2041–2052. doi:10.1007/s11999-009-0824-8
10. Clohisy JC, Schutz AL, John S, Schoenecker PN, Wright RW. Periacetabular osteotomy: a systematic literature. Rev Clin Orthop Relat Res. 2009;467(8):2041–2052. doi:10.1007/s11999-009-0842-6
11. Mokkink LB, Terwee CB, Patrick DL, et al. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: an international Delphi study. Qual Life Res. 2010;19:539–549. doi:10.1007/s11136-010-9655-z
12. Deshpande PR, Rajan S, Sudeepthi BL, et al. Patient-reported outcomes: a new era in clinical research. Perspect Clin Res. 2011;2(9):137–144. doi:10.4103/2229-3485.86879
13. Thorborg K, Roos EM, Bartels EM, et al. Validity, reliability and responsiveness of patient-reported outcome questionnaires when assessing hip and groin disability: a systematic review. Br J Sports Med. 2010;44(10):1186–1196. doi:10.1136/bjsm.2008.049783
14. Tijssen M, van Cingel R, vanMelick N, de Visser E. Patient-reported outcome questionnaires for hip arthroscopy: a systematic review of the psychometric evidence. BMC Musculoskelet Disord. 2011;12. doi:10.1186/1471-2474-12-117
15. Byrd JW, Jones KS. Hip arthroscopy for labral pathology: prospective analysis with10-year follow-up. Arthroscopy. 2009;25(4):365–368. doi:10.1016/j.arthro.2009.02.001
16. Mohtadi NGH, Griffin DR, et al. The development and validation of a self-administered quality-of-life outcome measure for young, active patients with symptomatic hip disease: the international hip outcome tool (iHOT-33) arthroscopy. J Arthroscopic Relat Surg. 2012;28(5):595–610. doi:10.1016/j.arthro.2012.03.013
17. Mohtadi NGH. Outcome assessment of non - arthroplasty hip disease in. NHO Sj Leunig M. Larson CM, Bedi A Kelly BT, (Eds). Hip Arthroscopy and hip joint preservation surgery. New York (NY): Springer 2014; 255–278.
18. Ramisetty N, Kwon Y, Mohtadi N. Patient-reported outcome measures for hip preservation surgery-a systematic review of the literature. J Hip Preserv Surg. 2015;6(2):
19. Sim Y, Horner NS, Darren de SA, Simunovic N, Karlsson J, Ayeni OR. Reporting of non-hip score outcomes following femoroacetabular impingement surgery: a systematic review. J Hip Preserv Surg. 2015;2:224–241. doi:10.1093/jhps/hnv048
20. Impellizzeri FM, Mannion AF, Naal FD, Hersche O, Leunig M. The early outcome of surgical treatment for femoroacetabular impingement: success depends on how you measure it. Osteoarthr Cart. 2012;20:638–645. doi:10.1016/j.joca.2012.03.019
21. Jacobsen J, Nielsen DB, Sørensen H, Søballe K, Mechlenburg I. Joint kinematics and kinetics during walking and running in 32 patients with hip dysplasia 1 year after periacetabular osteotomy. Acta Orthop. 2014;85:592–599. doi:10.3109/17453674.2014.886030
22. Romano CL, Frigo C, Randelli G, Pedotti A. Analysis of the gait of adults who had residual of congenital dysplasia of the hip. J Bone Joint Surg Am. 1996;78:1468–1479.
23. Pedersen EN, Simonsen EB, Alkjaer T, Soballe K. Walking pattern in adults with congenital hip dysplasia: 14 women examined by inverse dynamics. Acta Orthop Scand. 2004;75(1):2–9. doi:10.1080/00016470410001708010
24. Sucato DJ, Tulchin K, Shrader MW, DeLaRocha A, Gist T, Sheu G. Gait, hip strength and functional outcomes after a Ganz periacetabular osteotomy for adolescent hip dysplasia. J Pediatr Orthop. 2010;30(4):344–350. doi:10.1097/BPO.0b013e3181d9bfa2
25. Naal FD, Miozzari HH, Kelly BT, et al. The hip sports activity scale (HSAS) for patients with femoroacetabular impingement. Hip Int. 2013;23:204–211. doi:10.5301/hipint.5000006
26. Klit J, Hartig-Andreasen C, Jacobsen S, Troelsen A. Periacetabular osteotomy: sporting, social and sexual activity 9–12 years post surgery. Hip Int. 2014;24(1). doi:10.5301/hipint.5000077
27. Oken FO, Yildirim OA, Asilturk M. Factors affecting the return to work of total hip arthroplasty due to of developmental hip dysplasia in in young patients. J Orthop J Orthpaedics. 2018;15:450–454. doi:10.1016/j.jor.2018.03.030
28. Prather H, Creighton A, Sorenson C, Simpson S, Hunt MR, Rho M. Anxiety and insomnia in young and middle-aged adult hip pain patients with and without femoroacetabular impingement and developmental hip dysplasia. PM&R. 2018;10(5):455–461. doi:10.1016/j.pmrj.2017.10.007
29. Giuseppe D, Gambling T, Long AF, Murphy R, Jones H, Perry DC. The outcomes of Perthes’ disease of the hip: a study protocol for the development of a core outcome set. Trials. 2018;19:374. doi:10.1186/s13063-018-2695-3
30. Gambling T Hip conditions in the young - effective management strategies. Impact. ESRC; 2018.
31. Long AF, Dixon P. Monitoring outcomes in routine practice: defining appropriate measurement criteria. J Eval Clin Prac. 1996;2:71–78. doi:10.1111/j.1365-2753.1996.tb00029.x
32. Kirshner B, Guyatt G. A methodological framework for assessing health indices. J Chron Dis. 1985;38:27–36. doi:10.1016/0021-9681(85)90005-0
33. Scientific Advisory Committee of the Medical Outcomes Trust. Assessing health status and quality-of-life instruments: attributes and review criteria. Qual Life Res. 2002;11:193–205.
34. Smith SC, Lamping DL, Banerjee S, et al.Measurement of health-related quality of life for people with dementia: development of a new instrument (DEMQOL) and an evaluation of current methodology. Health Technol Assess (Rockv). 2005;9(10):1–112.
35. Greenhalgh J, Long AF, Brettle AJ, Grant MJ. Reviewing and selecting outcome measures for use in routine practice. J Eval Clin Pract. 1998;4:339–350
36. Frank AW. Just listening: narratives and deep illness. Fam Syst Health. 1998;16:197–212. doi:10.1037/h0089849
37. Frank AW. The Wounded Storyteller: Body, Illness and Ethics. Chicago: University of Chicago Press; 1995.
38. Mann C, Stewart F. Internet Communication and Qualitative Research: A Handbook for Researching Online. London: Sage Publications; 2000.
39. Ritchie J, Lewis J, editors. Qualitative Research Practice: A Guide for Social Science Students and Researchers. London: Sage Publications; 2003.
40. Fonteyn M, Bauer-Wu S. Using qualitative evaluation in a feasibility study to improve and refine a complementary therapy intervention prior to subsequent research. Complement Ther Clin Pract. 2005;11(4):247–252. doi:10.1016/j.ctcp.2005.05.007
41. Willis GB. Cognitive Interviewing: A Tool for Improving Questionnaire Design. Sage Research Methods. Thousand Oaks Ca: Sage Publications; 2005.
42. DeWalt D, Dilling MH, Rosenthal MJ, Pignone MP. Low parental literacy is associated with worse asthma care measures in children. Ambulatory Pediatr. 2007;7(1):25–31. doi:10.1016/j.ambp.2006.10.001
43. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
44. Pratt CC, McGuigan WM, Katzev AR. Measuring program outcomes: using retrospective pretest methodology. Am J Eval. 2000;21(3):341–349. doi:10.1177/109821400002100305
45. McPhail S, Beller E, Haines T. Physical function and health‐related quality of life of older adults undergoing hospital rehabilitation: how strong is the association. J Am Geriatric Soc. 2010;58(12):2435–2437. doi:10.1111/j.1532-5415.2010.03163.x
46. Streiner DL, Norman GR. Health Measurement Scales: A Practical Guide to Their Development and Use.
47. Hankins M. The factor structure of the twelve item General Health Questionnaire (GHQ-12): the result of negative phrasing. Clin Pract Epidemiol Ment Health. 2008;4:10. doi:10.1186/1745-0179-4-10
48. Schwarzer R, Jerusalem M. Generalized self-efficacy scale. In: Weinman J, Wright S, Johnston M, editors. Measures in Health Psychology: A User’s Portfolio. Causal and Control Beliefs. Windsor (UK): NFER-NELSON; 1995:35–37.
49. Clohisy JC, Knaus ER, Hunt DM, Lesher JM, Harris-Hayes M, Prather H. Clinical presentation of patients with symptomatic anterior hip impingement. Clin Orthop Relat Res. 2009;467(3):638–644. doi:10.1007/s11999-008-0680-y
50. Gray-Little B, Williams VSL, Hancock TD. An item response theory analysis of the Rosenberg Self-Esteem Scale. Pers Soc Psychol Bull. 1997;23:443–451. doi:10.1177/0146167297235001
51. Cash TF, Phillips KA, Santos MT, Hrabosky JI. Measuring “negative body image”: validation of the body image disturbance questionnaire in a non-clinical population. Body Image. 2004;1:363–372. doi:10.1016/j.bodyim.2004.10.001
52. Cash TF, Grasso K. The norms and stability of new measures of the multidimensional body image construct. Body Image. 2005;2:199–203. doi:10.1016/j.bodyim.2005.03.007
53. Wyatt MC, Beck M. The management of the painful borderline dysplastic hip. J Hip Preserv Surg. 2015;5(2):105–112. doi:10.1093/jhps/hny012
54. Soderberg S, Lundman B, Norberg A. Struggling for dignity: The meaning of women’s experiences of living with fibromyalgia. Qual Health Res. 1999; 9: 575.
55. Van Uden-Kraan CF, Drossaert ET, Shaw BR, Seydel ER, van de Laar AF. Empowering processes and outcomes of participation in online support groups for patients with breast cancer, arthritis, or fibromyalgia. Qual Health Res. 2008;18:405. doi:10.1177/1049732307313429
56. Beck C. Benefits of participating in internet interviews: women helping women. Qual Health Res. 2005;15:411. doi:10.1177/1049732304270837
57. Perry DC, Wright JG, Cooke S, et al. A consensus exercise identifying priorities for research into clinical effectiveness among children’s orthopaedic surgeons in the United Kingdom. J Bone Joint Surg. 2018;100-B:680–684. doi:10.1302/0301-620X.100B5.BJJ-2018-0051
58. Farnik M, Pierzchała W, Brożek G, Zejda JM, Skrzypek M. Quality of life protocol in the early asthma diagnosis in children. Pediatr Pulmonol. 2010;45(11):1049–1148. doi:10.1002/ppul.21293
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.