Back to Journals » Cancer Management and Research » Volume 15
Development and Validation of a Novel Diagnostic Nomogram Model Using Serum Oxidative Stress Markers and AURKA for Prediction of Nasopharyngeal Carcinoma
Authors Wu J ![]() , Luo H, Wang K, Yi B
, Luo H, Wang K, Yi B ![]()
Received 23 December 2022
Accepted for publication 8 September 2023
Published 27 September 2023 Volume 2023:15 Pages 1053—1062
DOI https://doi.org/10.2147/CMAR.S402572
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chien-Feng Li
Jiahui Wu,1,2 Huidan Luo,1,2 Kun Wang,1,2 Bin Yi1,2
1Department of Clinical Laboratory and Medical Research Center, Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China; 2National Clinical Research Center for Geriatric Disorders, Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China
Correspondence: Bin Yi, Department of Clinical Laboratory and Medical Research Center, Xiangya Hospital, Central South University, Changsha, Hunan, 410008, People’s Republic of China, Tel +86-13707495781, Fax +86-73189753200, Email [email protected]
Purpose: The mortality rate of nasopharyngeal carcinoma (NPC) remains high due to the absence of quick and accurate diagnostic approaches at its early stage. Our aim is to evaluate the diagnostic value of the elevated expression of Aurora kinase A (AURKA) and the oxidative stress markers (such as glutathione, superoxide dismutase and malondialdehyde) in serum of NPC patients and to establish a nomogram model for predicting NPC on the ground of these biomarkers.
Patients and Methods: Serum samples from 93 NPC patients and 94 healthy subjects were collected. Enzyme-linked immunosorbent assay (ELISA) was adopted to determine the AURKA level, while oxidative stress markers were measured by commercially available appropriate kits. Logistic regression was used for NPC predictor identification and nomogram construction. The training and validation cohorts (3:1) were randomly split up from the participants. Receiver operating characteristic (ROC) curves, calibration curves, and decision curve analyses (DCAs) were performed to validate the nomogram.
Results: AURKA and malondialdehyde (MDA) levels were significantly high in the NPC population compared to the healthy controls (P < 0.0001). The nomogram resulted in an area under the curve (AUC) of 0.897 (95% confidence interval: 0.848– 0.947) in the training set and AUC of 0.770 (0.628– 0.912) in the validation set. The predicted probability and the actual probability matched well in the nomogram (P > 0.05). DCAs showed good results too.
Conclusion: Serum levels of AURKA, SOD, and MDA have diagnostic values in NPC. The nomogram based on the identified biomarkers is favorable for NPC prediction.
Keywords: nasopharyngeal carcinoma, AURKA, SOD, MDA, nomogram
Introduction
Nasopharyngeal carcinoma (NPC) is a malignancy arising from nasopharyngeal epithelial cells with a remarkable geographic and racial distribution.1 Due to the lack of early typical clinical symptoms, the majority of NPC patients are in advanced stage upon first diagnosis, making clinical intervention very challenging. Although plasma EBV-DNA load and EBV serology tests are frequently used for NPC screening and early prediction in the general population, the resulting low positivity limits their application.2 Therefore, it is necessary to develop novel biomarkers for early diagnosis of NPC.
Maintaining the balance of pro-oxidants and antioxidants can keep the body in a stable redox state and protect homeostasis. Oxidative stress (OS) results from an imbalance between the production of ROS and the antioxidant capacity.3 In tumors, growing evidence indicates that OS has a complicated relationship with tumor development and metastasis.4–6 There are also studies that have considered OS as markers in the diagnosis and grading of tumors.7,8 Both glutathione (GSH) and superoxide dismutase (SOD) are antioxidants that act as free radical scavengers and detoxifying agents in cells to neutralize ROS,9 and they are the most commonly declined metabolites detected during OS.10,11 Malondialdehyde (MDA) is the end product of lipid peroxidation,12 which is often used to detect lipid peroxidation during OS. Prior investigations have demonstrated that MDA is associated with gastric cancer,13 colorectal cancer,14 prostate cancer,15 et al. Serving as a predictive factor for tumor staging and prognosis.15,16 In addition, previous studies have also explored the associations of GSH, MDA, and SOD with head and neck cancers separately,17–19 yet their relationship with NPC staging and prognosis remains unclear.
Aurora kinase A (AURKA) belongs to serine/threonine kinases family and is important for cell-cycle regulation. In squamous-cell carcinomas of the head and neck (SCCHN), AURKA protein expression was significantly upregulated compared to the non-tumorous tissues.20,21 Similarly, most NPC patients also showed elevated mRNA expression levels of AURKA in tumor tissues compared with the matched normal tissues.22 Cancer metastases and tumorigenesis were influenced by AURKA, which participated in cancer-promoting processes through regulation of the cell cycle and activation of the oncogenic signaling pathways, such as p53,23 NF-κB,24 and ROS.25 However, to the best of our knowledge, few investigations have been known to explore whether AURKA is the key molecular in NPC.
In this study, we aimed at comparing the differences of OS status and AURKA expression between the NPC patients and the healthy population. In addition, we managed to construct a nomogram model to evaluate the efficiency of the serum biomarkers in diagnosis and prediction of NPC.
Materials and Methods
Sample Collection
This case–control study recruited 92 NPC patients and 93 healthy subjects from Xiangya Hospital of Central South University between August 2022 and November 2022. The inclusion criteria were as follows: (a) Patients diagnosed with NPC confirmed by histopathology; (b) Patients with complete baseline data and laboratory results. The exclusion criteria included any of the following: (a) Samples showing hemolysis; (b) Patients who recently took anti-inflammatory drugs or received immunosuppressive therapy; (c) Patients with other cancers or those who received anti-tumor treatment; (d) Pregnant or lactating women; (e) Patients with incomplete clinical and pathological data. TNM staging was classified according to the eighth edition of American Joint Committee on Cancer (AJCC) Staging Manual/International Union Against Cancer. All participants were given informed consent, and this study was permitted by the ethics committee of Xiangya Hospital of Central South University (No. 202211237).
Each participant was drawn 5 mL of blood from the elbow vein after 12 hours of fasting. The collected blood was centrifugated at 3000 rpm for 10 minutes and serum samples in the upper layer were isolated and stored at −80°C until they were required for testing.
Measurement of AURKA, GSH, SOD and MDA
AURKA was determined by a monoclonal antibody-based sandwich human AURKA ELISA kit (Animal Union, Shanghai, China). Briefly, 50μL of the double-diluted sera as well as standards were added to the microtiter plate well pre-coated with human AURKA antibody, placed at 37°C for 30 min and washed five times with washing solution. Then, 50μL of HRP-conjugated AURKA antibody were inoculated in the well and incubated at 37 °C for 30 min. Following five washes, 50μL of TMB solution were dropped to each well and preserved at 37°C for 10 min. After that, 50μL of termination solution were pipetted to end the reaction and the absorbance of each well was read at 450 nm on an automatic microplate reader to obtain the concentration of each sample by comparison with the standard curve.
Serum levels of GSH, MDA, and SOD were measured using commercially available kits provided by Nanjing Jiancheng Bioengineering Institute, Nanjing, China. GSH was measured according to the kit instructions. The principles and procedures were as follows: GSH reacted with DTNB to produce a yellow compound which had a maximum absorption peak at 450 nm, thus the GSH content could be calculated by that absorbance on a fully automatic enzyme reader. MDA test was based on the 2-thiobarbituric acid (TBA) method. MDA from degraded products of lipid peroxide could be condensed with thiobarbituric acid to form a red product which could be detected at 532 nm. Followed by reaction between the serum sample and the reagent provided in the kit, the absorbance at 532nm was measured on a microplate reader, and the concentration of the sample was quantified. SOD was determined by the xanthine oxidase method. The WST-1 (2-(4-iodophenyl)-3-(4-nitrophenyl)-5-(2, 4-disulfonic acid phenyl)-2 hydrogen-tetrazolium salt) provided in the kit reacted with superoxide anion to produce a water-soluble dye that could be detected at 450 nm and the results were linearly correlated with SOD activity. Briefly, 20 μL of serum, 20μL of enzyme working solution and 200μL of WST working solution were added into the microplates and incubated at 37°C for 20 min, then the absorbance at 450 nm of each well was read and the concentration of each sample was calculated.
Statistical Analysis
Continuous variables were shown as mean ± SD or median value, while categorical variables were presented as frequency or proportion. The Kolmogorov–Smirnov test was used to determine if the distribution of variables was normality. Pearson’s chi-square test and Wilcoxon test were applied to compare the baseline characteristics of the two groups. We employed multivariate linear regression analysis to explore the correlation between AURKA and other variables. Furthermore, we conducted univariate or multivariate logistic regression to assess independent risk factors for NPC. Variables with a P > 0.05 were adopted to develop the risk prediction model and build the nomogram. All participants were randomly divided into the training group (n = 139) and the validation group (n = 48), and validated and evaluated independently. To evaluate the discrimination ability of the established prediction model, an area under the receiver operating characteristic curve (AUC) was calculated. AUC ≥ 0.75 was considered to have a good discrimination effect, while <0.75 was not. Furthermore, a decision curve analysis (DCA) was conducted to determine whether the prediction model would be clinically favorable by quantifying the net benefits at different threshold probabilities. The statistical analysis was performed by SPSS 20.0 (IBM, Armonk, NY) or R software, version 4.2.1. P value <0.05 was considered statistically significant.
Results
Comparisons of Clinical Characteristics of the Participants
A total of 185 participants were enrolled in the present study, including 92 subjects with NPC and 93 healthy controls, and their clinical characteristics were described and compared in Table 1. There were no significant differences in age and body mass index (BMI) between the two groups (P > 0.050). The mean age of NPC patients was 51.66±10.96 year, and the control subjects, 54.49±11.52 year. However, parameter of gender was significantly different between the two cohorts (P < 0.001). Both serum levels of GSH and SOD in NPC were found to be overwhelmingly decreased (P < 0.001) compared to the controls, inversely, prominent elevations of MDA and AURKA levels in NPC were observed (P < 0.001).
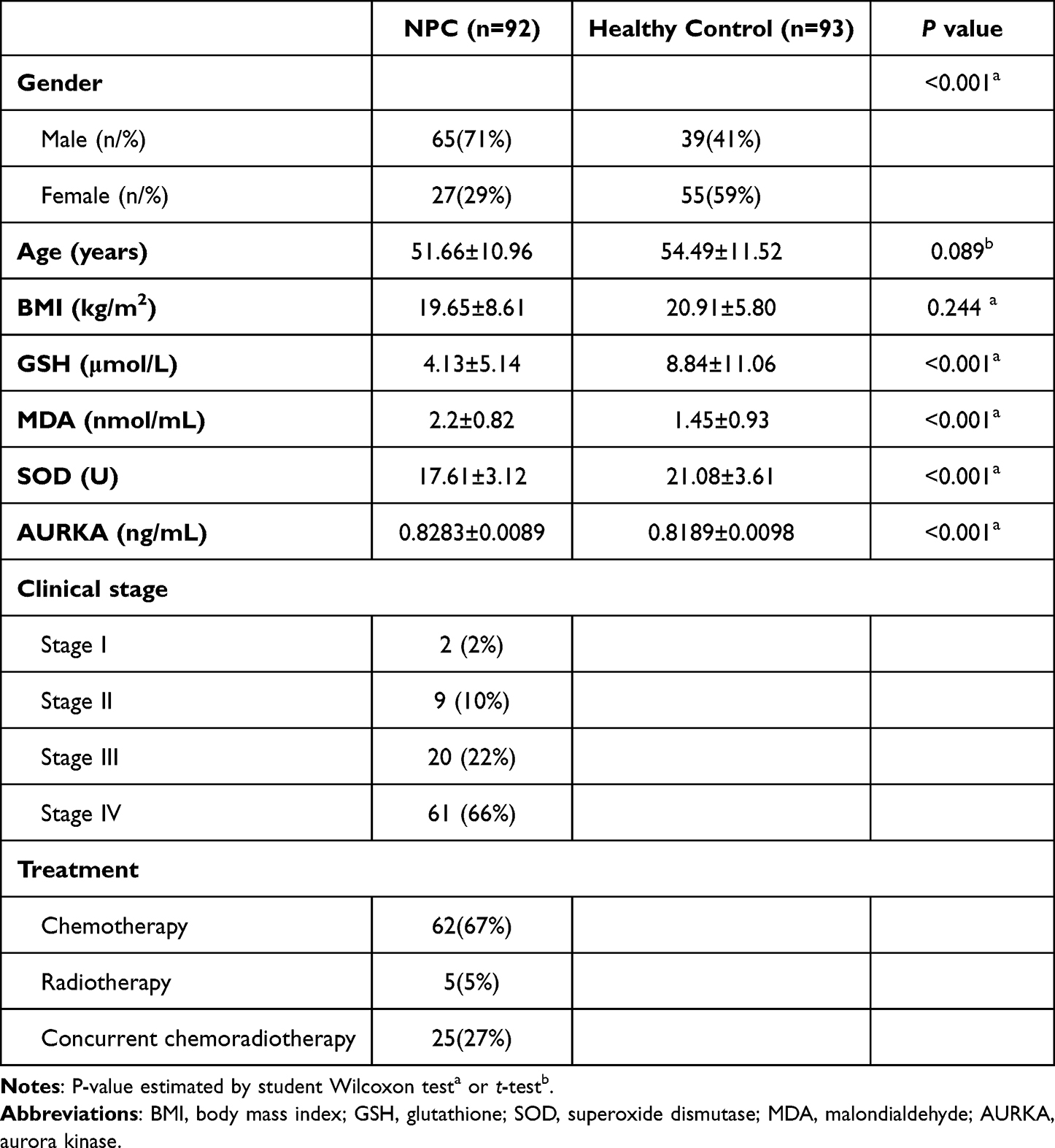 |
Table 1 Clinical Characteristics of the Study Population and Their Comparisons |
Comparisons of Clinical Characteristics of Patients with NPC in Different Stages
When taking cancer stages into account, we found that most patients (88%) were diagnosed at the advanced stages of III/IV. Notably, GSH, SOD, MDA, and AURKA levels were considerably differed (P < 0.050) depending on the stage of NPC (Table 2).
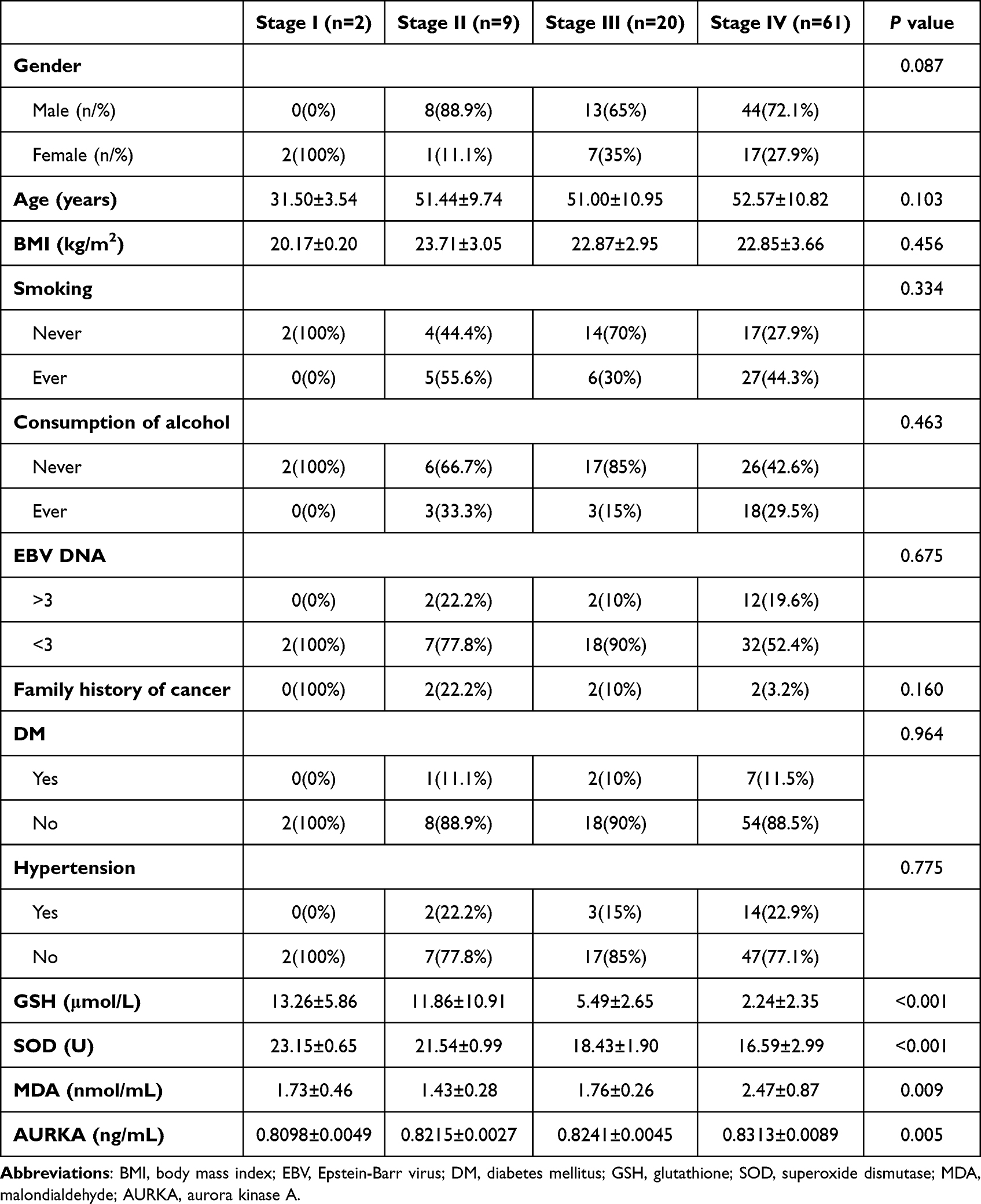 |
Table 2 Comparisons of Clinical Characteristics in Different Clinical Stages of NPC |
Correlations of Serum AURKA Levels with Oxidative Stress Markers and Other Parameters
The results of Spearman correlation analysis revealed a positive association of serum AURKA level with the occurrence of NPC (r = 0.45, P < 0.001). Furthermore, AURKA level had a favorable correlation with MDA (r = 0.353, P < 0.001), but negatively correlated to GSH (r=−0.359, P < 0.001) or SOD (r=−0.403, P < 0.001).
Using serum AURKA levels as the dependent variable while gender, age, and BMI as independent variables, the multivariate linear regression analysis, showed that the occurrence of NPC (standardized β=0.388, P < 0.001) and MDA (standardized β=0.152, P=0.035) were independently and positively associated with serum AURKA level (Table 3).
 |
Table 3 Multivariate Linear Regression Analyses of Factors Associated with Serum AURKA Levels |
Identification of the Predictors of NPC and Construction of the Nomogram Model
The training cohort, including 139 (74.3%) individuals consisting of 73 NPC patients and 66 healthy controls, and the validation cohort, including 48 (25.7%) participants consisting of 19 NPC patients and 29 healthy controls, were randomly assigned at a ratio of around 3:1. No significant differences between the two cohorts were observed in parameters such as age, gender, BMI, GSH, SOD, MDA and AURKA.
The univariate analysis revealed that NPC was significantly associated with gender (P=0.0002), GSH (P=0.0005), SOD (P < 0.001), MDA (P < 0.001) and AURKA (P < 0.001). Further multivariate regression analysis confirmed the inclusion of relevant variables: Gender, SOD, MDA, and AURKA (Table 4). Subsequently, a nomogram was established to visualize the model (Figure 1), meanwhile, an ROC curve and a calibration plot were generated to validate the predictive accuracy of the training cohort and the validation cohort (Figure 2). The results demonstrated that the AUC for training cohort was 0.897 (95% CI: 0.848–0.947), and for validation cohort, 0.770 (0.628–0.912), indicating good performance and reliability of the nomogram on predicting NPC. The calibration curves also exhibited high consistency in predicting the probability of NPC development between the training cohort and the validation cohort in the nomogram model compared to the actual observation (Figure 3A and B). Additionally, the nomogram’s high efficiency in clinical decision-making was demonstrated through the DCA, as shown in Figure 3C and D.
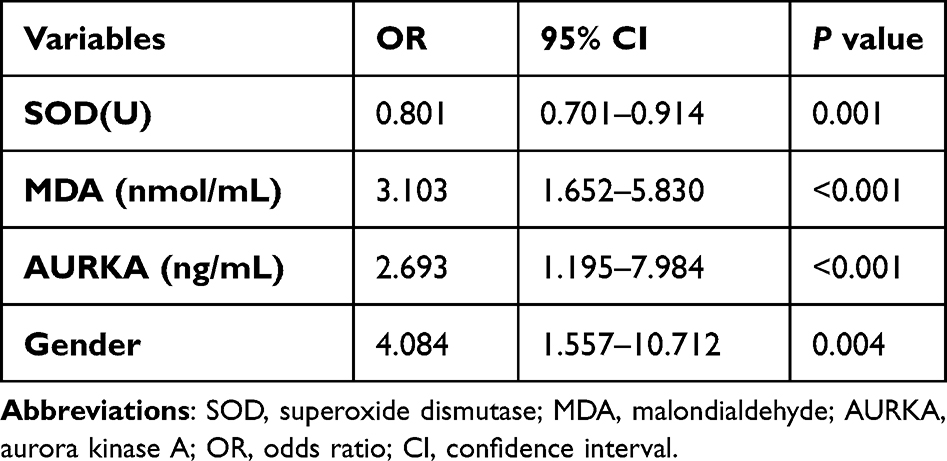 |
Table 4 Multivariate Logistic Analyses of Factors for NPC Diagnosis |
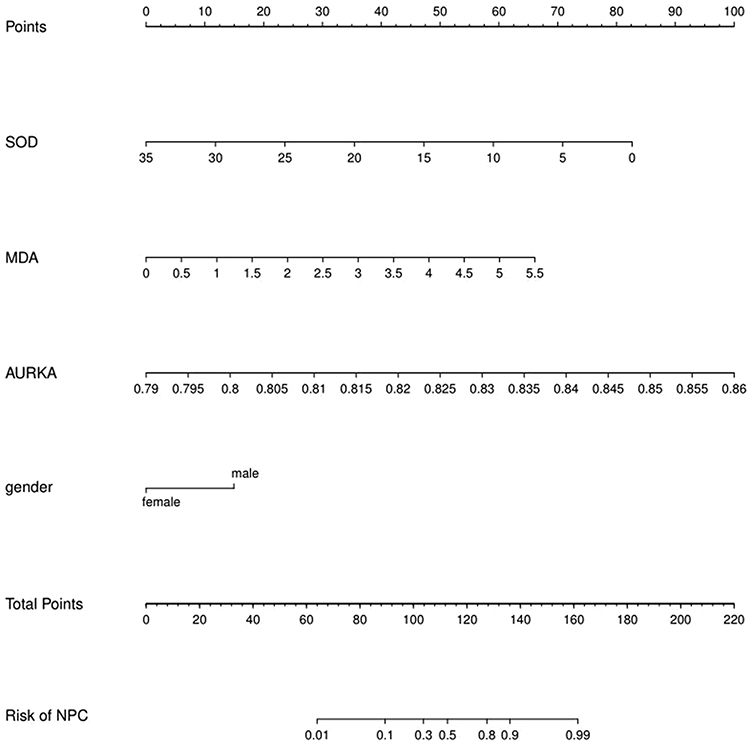 |
Figure 1 Nomogram for diagnosis of NPC. Abbreviations: SOD, superoxide dismutase; MDA, malondialdehyde; AURKA, aurora kinase A; NPC, Nasopharyngeal carcinoma. |
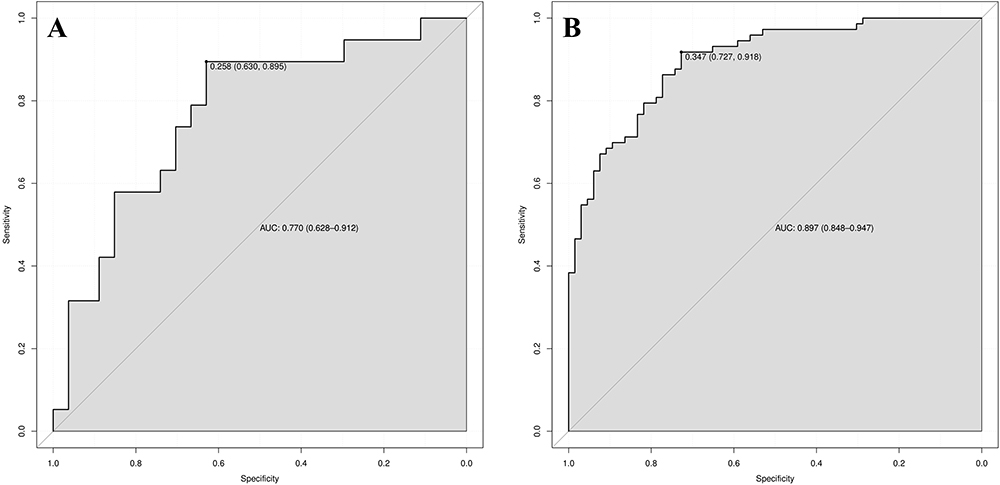 |
Figure 2 Decision curve analysis of the nomogram. (A) the validation cohort; (B) the traning cohort. |
 |
Figure 3 Calibration and DCA curve of the nomogram. (A) Calibration curve of the training cohort; (B) Calibration curve of the validation cohort, the dashed line represents the original performance, and the solid dashed line represents the performance during validation by bootstrapping (B = 1000 repetitions). (C) DCA curve of the training cohort; (D) DCA curve of the validation cohort. None: All patients receive no specific intervention, representing the scenario where the Nomogram model is not applied for prediction, indicating that all patients are not diagnosed with NPC. ALL: The predictive results of the Nomogram model are used to intervene in all patients, representing the scenario where all patients are diagnosed with NPC. The red line illustrates the net benefit of the Nomogram model relative to the default strategy at different threshold probabilities. |
Discussion
In this study, we first investigated serum levels of GSH, SOD, MDA and AURKA, and their comparisons between the NPC patients and the healthy subjects. We found that MDA and AURKA levels were significantly elevated in NPC (P < 0.001), whereas GSH and SOD were largely reduced (P < 0.001). Our findings on changes of MDA and GSH were consistent with previous studies.17,18 SOD was considered to be a prominent target of oxidative damage, according to recent publications.25,26 In the presence of high levels of OS, decline in GSH, SOD, and rise in MDA were typically observed.27–29 Cancer cells are in an unbalanced redox state, which allows the generation of drug-resistant cells and leads to treatment failure.30 Tumor cells are more susceptible to ROS-mediated oxidative damage due to increased OS compared to normal cells,31 which explains the high levels of OS and the variations of the indicators observed in advanced NPC in this study. It may help create OS-induced relevant research ideas for the treatment of advanced NPC.
Likewise, we uncovered a strong relationship between AURKA expression and the levels of OS (standardized β=0.152, P=0.035). It was believed that AURKA expression played a crucial role in the early progression of prostate cancer.23–25 Some studies reported that AURKA levels were raised in gastric,32,33 pancreatic,34 breast,35 and ovarian cancer tissues and cells,36 and were linked to a poor prognosis. Bioinformatics research on NPC proved that the high- and low-AURKA expression groups were highly discriminative,22 which was in parallel to our results on elevated serum AURKA levels in NPC.
In early mitosis, OS could cause hyperphosphorylation of Aurora A,37 and AURKA knockdown markedly induced apoptosis and ROS production in oral squamous cell carcinoma (OSCC) cell lines,20 indicating an association between AURKA and OS, which is strengthened by the findings in our investigation that MDA is closely related to AURKA, even though more evidences on their relationship are required.
Combining previous findings and the risk factors of gender, SOD, MDA and AURKA in our analysis, we established a nomogram model for predicting the risk of NPC. Participants with a high score have a high risk of NPC. Furthermore, the AUC in the training cohort for variables to distinguish NPC from healthy individuals reached 0.897, suggesting a high prediction quality. The ideal and bias-corrected lines produced by the nomogram in the current study were in good agreement with the calibration curves in both of the training and validation cohorts. The decision curve also graphically depicted the model’s therapeutic advantages. Indeed, our study confirmed the elevation of these OS markers in advanced NPC.
To our knowledge, this is the first work to build a prediction nomogram for predicting NPC that incorporates OS markers and AURKA. However, there are still some limitations in this study. Firstly, this was a case–control study and was unable to determine causality between NPC and its risk factors. Secondly, while we employed a standardized and widely utilized nomogram model to predict the risk of NPC, some limitations may arise when applied within the context of a case–control design.38 Furthermore, this nomogram model was established in limited samples and did not provide positive and negative predictive values for the diagnostic assessment of NPC (a rare disease), therefore, cautious consideration is warranted in the application of the model. Finally, we did not compare our model with other existing theoretical models due to the shortage of literature and difficulties such as in collecting EBV-DNA data from healthy subjects.
Clinically, we have established a predictive model for NPC using OS markers and AURKA. Our model can further enrich early diagnosis of NPC and provide insights for future research. Additionally, the utilization of readily available serum tests for screening high-risk populations could serve as a potential alternative diagnostic strategy to the relatively harder-to-obtain or costlier CT/MRI or invasive nasopharyngoscopy examinations. Specially, after evaluating clinical symptoms, if a patient shows some clinical indications of NPC, clinicians can further utilize this nomogram model to assess the risk of disease to support next decision-making. This approach has the potential benefits to reduce unnecessary expenditures on imaging and invasive examinations for patients.
Conclusion
As a result, our work sheds light on the association between AURKA and OS markers with NPC, and significance of these clinical characteristics in predicting NPC. AURKA may be one of the potential therapeutic targets for management of NPC. Furthermore, we have constructed a nomogram model with robust performance, applicable for estimating early diagnosis of NPC, thereby offering supplementary information for clinical diagnosis and decision-making. Nonetheless, given that our design is an observational study, advanced evidence from large-scale samples remains required to further validate these findings.
Abbreviations
NPC, Nasopharyngeal carcinoma; OS, oxidative stress; GSH, glutathione; SOD, superoxide dismutase; MDA, malondialdehyde; AURKA, aurora kinase A; SCCHN, squamous-cell carcinomas of the head and neck; TBA, 2-thiobarbituric acid; CI, confidence interval.
Ethical Approval and Informed Consent
The studies involving human participants were reviewed and approved by Ethics Committee of Xiangya Hospital of Central South University, which conformed to the ethical guidelines of the 1975 Declaration of Helsinki. The patients have signed their informed consent to participate in this study.
Funding
This work was supported by the National Nature Science Foundation of Hunan Province under [grant number 2021JJ41023]; National Key Research and Development Program [grant number 2021YFC2009302].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen YP, Chan ATC, Le QT, Blanchard P, Sun Y, Ma J. Nasopharyngeal carcinoma. Lancet. 2019;394(10192):64–80. doi:10.1016/S0140-6736(19)30956-0
2. Zhou X, Cao SM, Cai YL, et al. A comprehensive risk score for effective risk stratification and screening of nasopharyngeal carcinoma. Nat Commun. 2021;12(1):5189. doi:10.1038/s41467-021-25402-z
3. Bansal A, Simon MC. Glutathione metabolism in cancer progression and treatment resistance. J Cell Biol. 2018;217(7):2291–2298. doi:10.1083/jcb.201804161
4. Mazzuferi G, Bacchetti T, Islam MO, Ferretti G. High density lipoproteins and oxidative stress in breast cancer. Lipids Health Dis. 2021;20(1):143. doi:10.1186/s12944-021-01562-1
5. Braga-Neto MB, Costa DVS, Queiroz DMM, et al. Increased oxidative stress in gastric cancer patients and their first-degree relatives: a prospective study from Northeastern Brazil. Oxid Med Cell Longev. 2021;2021:6657434. doi:10.1155/2021/6657434
6. Wu Z, Huang H, Han Q, et al. SENP7 senses oxidative stress to sustain metabolic fitness and antitumor functions of CD8+ T cells. J Clin Invest. 2022;132(7). doi:10.1172/JCI155224
7. Wigner P, Szymanska B, Bijak M, et al. Oxidative stress parameters as biomarkers of bladder cancer development and progression. Sci Rep. 2021;11(1):15134. doi:10.1038/s41598-021-94729-w
8. Bilgin E, Atli G, Duman BB, Okten AI. Evaluation of oxidative stress biomarkers in brain metastatic and non-metastatic lung cancer patients with different cell types. Anticancer Agents Med Chem. 2021;21(15):2032–2040. doi:10.2174/1871520621666210211163055
9. Niu B, Liao K, Zhou Y, et al. Application of glutathione depletion in cancer therapy: enhanced ROS-based therapy, ferroptosis, and chemotherapy. Biomaterials. 2021;277:121110. doi:10.1016/j.biomaterials.2021.121110
10. Pakfetrat A, Dalirsani Z, Hashemy SI, et al. Evaluation of serum levels of oxidized and reduced glutathione and total antioxidant capacity in patients with head and neck squamous cell carcinoma. J Cancer Res Ther. 2018;14(2):428–431. doi:10.4103/0973-1482.189229
11. Xue N, Zhou R, Deng M, et al. High serum superoxide dismutase activity improves radiation-related quality of life in patients with esophageal squamous cell carcinoma. Clinics. 2021;76:e2226. doi:10.6061/clinics/2021/e2226
12. Perluigi M, Coccia R, Butterfield DA. 4-Hydroxy-2-nonenal, a reactive product of lipid peroxidation, and neurodegenerative diseases: a toxic combination illuminated by redox proteomics studies. Antioxid Redox Signal. 2012;17(11):1590–1609. doi:10.1089/ars.2011.4406
13. Wang YK, Chiang WC, Kuo FC, et al. Levels of malondialdehyde in the gastric juice: its association with Helicobacter pylori infection and stomach diseases. Helicobacter. 2018;23(2):e12460. doi:10.1111/hel.12460
14. Zińczuk J, Maciejczyk M, Zaręba K, et al. Antioxidant barrier, redox status, and oxidative damage to biomolecules in patients with colorectal cancer. can malondialdehyde and catalase be markers of colorectal cancer advancement? Biomolecules. 2019;9(10):637. doi:10.3390/biom9100637
15. Dillioglugil MO, Mekık H, Muezzinoglu B, Ozkan TA, Demir CG, Dillioglugil O. Blood and tissue nitric oxide and malondialdehyde are prognostic indicators of localized prostate cancer. Int Urol Nephrol. 2012;44(6):1691–1696. doi:10.1007/s11255-012-0221-1
16. Kaynar H, Meral M, Turhan H, Keles M, Celik G, Akcay F. Glutathione peroxidase, glutathione-S-transferase, catalase, xanthine oxidase, Cu-Zn superoxide dismutase activities, total glutathione, nitric oxide, and malondialdehyde levels in erythrocytes of patients with small cell and non-small cell lung cancer. Cancer Lett. 2005;227(2):133–139. doi:10.1016/j.canlet.2004.12.005
17. Gargouri B, Lassoued S, Ben Mansour R, et al. High levels of autoantibodies against catalase and superoxide dismutase in nasopharyngeal carcinoma. South Med J. 2009;102(12):1222–1226. doi:10.1097/SMJ.0b013e3181bb85b5
18. Gargouri B, Lassoued S, Ayadi W, et al. Lipid peroxidation and antioxidant system in the tumor and in the blood of patients with nasopharyngeal carcinoma. Biol Trace Elem Res. 2009;132(1–3):27–34. doi:10.1007/s12011-009-8384-z
19. Bozan N, Demir H, Gursoy T, et al. Alterations in oxidative stress markers in laryngeal carcinoma patients. J Chin Med Assoc. 2018;81(9):811–815. doi:10.1016/j.jcma.2018.02.004
20. Dawei H, Honggang D, Qian W. AURKA contributes to the progression of oral squamous cell carcinoma (OSCC) through modulating epithelial-to-mesenchymal transition (EMT) and apoptosis via the regulation of ROS. Biochem Biophys Res Commun. 2018;507(1–4):83–90. doi:10.1016/j.bbrc.2018.10.170
21. Mehra R, Serebriiskii IG, Burtness B, Astsaturov I, Golemis EA. Aurora kinases in head and neck cancer. Lancet Oncol. 2013;14(10):e425–e435. doi:10.1016/S1470-2045(13)70128-1
22. Huang C, Chen L, Zhang Y, et al. Predicting AURKA as a novel therapeutic target for NPC: a comprehensive analysis based on bioinformatics and validation. Front Genet. 2022;13:926546. doi:10.3389/fgene.2022.926546
23. Du R, Huang C, Liu K, Li X, Dong Z. Targeting AURKA in Cancer: molecular mechanisms and opportunities for Cancer therapy. Mol Cancer. 2021;20(1):15. doi:10.1186/s12943-020-01305-3
24. Katsha A, Soutto M, Sehdev V, et al. Aurora kinase A promotes inflammation and tumorigenesis in mice and human gastric neoplasia. Gastroenterology. 2013;145(6):1312–1322 e1311–1318. doi:10.1053/j.gastro.2013.08.050
25. Skorska KB, Placzkowska S, Prescha A, et al. Serum total SOD activity and SOD1/2 concentrations in predicting all-cause mortality in lung cancer patients. Pharmaceuticals. 2021;14(11):1067. doi:10.3390/ph14111067
26. Strycharz-Dudziak M, Foltyn S, Dworzanski J, et al. Glutathione Peroxidase (GPx) and Superoxide Dismutase (SOD) in oropharyngeal cancer associated with EBV and HPV coinfection. Viruses. 2020;12(9):1008. doi:10.3390/v12091008
27. Liu Q, Ding X, Xu X, et al. Tumor-targeted hyaluronic acid-based oxidative stress nanoamplifier with ROS generation and GSH depletion for antitumor therapy. Int J Biol Macromol. 2022;207:771–783. doi:10.1016/j.ijbiomac.2022.03.139
28. Verlaet AAJ, Breynaert A, Ceulemans B, et al. Oxidative stress and immune aberrancies in attention-deficit/hyperactivity disorder (ADHD): a case-control comparison. Eur Child Adolesc Psychiatry. 2019;28(5):719–729. doi:10.1007/s00787-018-1239-4
29. Wu Q, Shang Y, Shen T, Liu F, Zhang W. Biochanin A protects SH-SY5Y cells against isoflurane-induced neurotoxicity by suppressing oxidative stress and apoptosis. Neurotoxicology. 2021;86:10–18. doi:10.1016/j.neuro.2021.06.007
30. Forman HJ, Zhang H. Targeting oxidative stress in disease: promise and limitations of antioxidant therapy. Nat Rev Drug Discov. 2021;20(9):689–709. doi:10.1038/s41573-021-00233-1
31. Wu J, Ning P, Gao R, et al. Programmable ROS-mediated cancer therapy via magneto-inductions. Adv Sci. 2020;7(12):1902933. doi:10.1002/advs.201902933
32. Gomaa A, Peng D, Chen Z, et al. Epigenetic regulation of AURKA by miR-4715-3p in upper gastrointestinal cancers. Sci Rep. 2019;9(1):16970. doi:10.1038/s41598-019-53174-6
33. Xie Y, Zhu S, Zhong M, et al. Inhibition of Aurora Kinase A induces necroptosis in pancreatic carcinoma. Gastroenterology. 2017;153(5):1429–1443 e1425. doi:10.1053/j.gastro.2017.07.036
34. Wang-Bishop L, Chen Z, Gomaa A, et al. Inhibition of AURKA reduces proliferation and survival of gastrointestinal cancer cells with activated KRAS by preventing activation of RPS6KB1. Gastroenterology. 2019;156(3):662–675 e667. doi:10.1053/j.gastro.2018.10.030
35. Peng F, Xu J, Cui B, et al. Oncogenic AURKA-enhanced N(6)-methyladenosine modification increases DROSHA mRNA stability to transactivate STC1 in breast cancer stem-like cells. Cell Res. 2021;31(3):345–361. doi:10.1038/s41422-020-00397-2
36. Sun H, Wang H, Wang X, et al. Aurora-A/SOX8/FOXK1 signaling axis promotes chemoresistance via suppression of cell senescence and induction of glucose metabolism in ovarian cancer organoids and cells. Theranostics. 2020;10(15):6928–6945. doi:10.7150/thno.43811
37. Wang GF, Dong Q, Bai Y, et al. Oxidative stress induces mitotic arrest by inhibiting Aurora A-involved mitotic spindle formation. Free Radic Biol Med. 2017;103:177–187. doi:10.1016/j.freeradbiomed.2016.12.031
38. Huang Y, Pepe MS. Assessing risk prediction models in case-control studies using semiparametric and nonparametric methods. Stat Med. 2010;29(13):1391–1410. doi:10.1002/sim.3876
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.