Back to Journals » International Journal of General Medicine » Volume 18
Development and Validation of a Machine Learning Model for Predicting Long-Term Depression Risk in ACS Patients After PCI: A Retrospective Cohort Study
Authors Lv H ![]() , Sun F, Zhang Y, Zhou X
, Sun F, Zhang Y, Zhou X
Received 15 February 2025
Accepted for publication 3 June 2025
Published 8 June 2025 Volume 2025:18 Pages 2957—2972
DOI https://doi.org/10.2147/IJGM.S523029
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Huasheng Lv,1,2 Fengyu Sun,1,2 Yuchen Zhang,1,2 Xinrong Zhou1,2
1State Key Laboratory of Pathogenesis, Prevention and Treatment of High Incidence Diseases in Central Asia, Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China; 2The First Affiliated Hospital of Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China
Correspondence: Xinrong Zhou, Email [email protected]
Objective: To develop and validate a machine learning (ML) model for predicting long-term depression risk in ACS patients following percutaneous coronary intervention (PCI).
Methods: This retrospective cohort study included 1951 ACS patients who underwent PCI in 2023. Feature selection was conducted using the Boruta algorithm, and restricted cubic spline (RCS) analysis was applied to assess non-linear associations. Six ML models were trained and tested using a 70:30 train-validation split. Model performance was evaluated using Area under the curve(AUC), sensitivity, specificity, F1-score, calibration curves, and decision curve analysis. SHapley Additive exPlanations (SHAP) were used to interpret feature contributions.
Results: Among the 1951 patients, 382 (19.6%) developed long-term depression. After feature selection via the Boruta algorithm, ten key predictors were identified, including NYHA classification, diabetes, thyroid-stimulating hormone (TSH), and left ventricular ejection fraction (LVEF). The LGBM and XGBoost models achieved the highest discrimination, with AUCs of 0.849 (training) and 0.652 (validation) for LGBM, and 0.814 (training) and 0.699 (validation) for XGBoost. Calibration curves showed good alignment between predicted and observed outcomes. SHAP analysis confirmed NYHA classification, TSH, and diabetes as the most influential features. Decision curve analysis demonstrated the clinical benefit of both models across a range of thresholds.
Conclusion: The models demonstrated potential for early risk stratification of post-PCI depression and may inform targeted clinical interventions.
Plain Language Summary: Depression is a common but often overlooked problem in people recovering from heart procedures. Patients with acute coronary syndrome (ACS) who undergo percutaneous coronary intervention (PCI)—a procedure to open blocked arteries—face a higher risk of long-term depression, which can worsen heart health and reduce quality of life.
In this study, we used machine learning (ML), a type of artificial intelligence, to analyze the medical data of 1951 patients who had PCI. Our goal was to predict who might develop depression in the year after their procedure. We tested six ML models and found that two of them—Light Gradient Boosting Machine (LGBM) and XGBoost—performed the best. These models used routine clinical information like heart function, thyroid levels, and diabetes status to make predictions.
The results showed that about 1 in 5 patients developed depression. The ML models were able to highlight high-risk individuals early, which could help doctors provide mental health support sooner.
This research shows how advanced data analysis can improve patient care after heart procedures. By identifying people at risk earlier, we can move toward more personalized and proactive treatment—not just for the heart, but for mental health too.
Keywords: acute coronary syndrome, percutaneous coronary intervention, depression, machine learning, predictive model
Introduction
Acute coronary syndrome (ACS) remains a leading cause of morbidity and mortality worldwide, with percutaneous coronary intervention (PCI) being the mainstay treatment to restore coronary perfusion and reduce adverse cardiovascular outcomes.1,2 Despite its efficacy, emerging evidence highlights that a substantial proportion of ACS patients experience psychological comorbidities following PCI, particularly depression.3–6 This is not merely a transient emotional reaction, but a clinically significant condition associated with impaired quality of life, poor medication adherence, increased risk of recurrent cardiac events, and higher mortality.
Compared to patients with stable coronary artery disease or those treated with conservative approaches, ACS patients undergoing PCI are at heightened risk of developing depression. This vulnerability stems from the abrupt and life-threatening nature of ACS, the stress of hospitalization and invasive intervention, as well as uncertainty during recovery. Studies report that post-PCI depression affects up to 48% of patients7,8—a notably higher rate than in many other cardiovascular populations. However, depressive symptoms are frequently under-recognized and undertreated due to symptom overlap with cardiovascular disease, stigma, and time-limited follow-up practices.9
Early identification of patients at high risk for post-PCI depression remains a clinical priority but is hindered by the limitations of conventional tools, such as screening questionnaires and linear statistical models. These methods are often inadequate for capturing complex, nonlinear interactions among biological, psychological, and procedural variables.10–13 In contrast, machine learning (ML) offers powerful capabilities to integrate high-dimensional clinical data and uncover subtle patterns predictive of future outcomes.13–15
While ML applications in mental health and cardiovascular research are rapidly expanding, studies specifically targeting long-term depression risk prediction in ACS patients after PCI remain scarce. Most existing models focus on short-term emotional outcomes or general psychiatric populations. Few tools have been developed with a focus on this unique high-risk cardiac subgroup, and even fewer have undergone robust validation or demonstrated clinical utility. Therefore, this study aims to develop and validate ML-based models for predicting long-term depression risk in ACS patients post-PCI. Furthermore, we evaluate their calibration, interpretability, and potential for clinical implementation to support personalized care and timely intervention.
Methods
Study Design and Population
This retrospective study included patients who visited the Heart Center of the First Affiliated Hospital of Xinjiang Medical University between January and December 2023. A total of 2261 ACS patients who underwent PCI were initially considered. Eligible participants were adult ACS patients who had undergone PCI. Based on predefined exclusion criteria, 310 patients were excluded: 47 with psychiatric disorders or psychotropic medication use, 53 with cognitive impairment, 35 with substance or alcohol dependence, 21 with major life events in the past six months, 87 who died in-hospital or were lost to follow-up, 41 with severe systemic disease, and 26 with substantial missingness in key clinical variables (eg, laboratory results, NYHA classification). These cases were removed using listwise deletion. In the final analytic dataset (n = 1951), residual missingness was minimal (<5% for any single variable). Median imputation was applied for continuous variables and mode imputation for categorical variables to ensure data completeness. The study was approved by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University (Approval No. 241024-02). Given the retrospective nature of the study, the requirement for informed consent was waived. All patient data were fully anonymized prior to analysis, and patient confidentiality was strictly maintained in accordance with institutional and journal ethical guidelines.
Data Collection
Clinical data were obtained from electronic health records and included demographic information, medical history, laboratory results, and details related to PCI procedures. Data on baseline characteristics, such as age, sex, ethnicity, smoking status, and comorbidities (eg, diabetes, hypertension), were collected. Additionally, relevant medical history, including stroke and previous PCI procedures, was recorded. Laboratory results included white blood cell count (WBC), triglyceride-glucose index (TyG), uric acid levels, thyroid-stimulating hormone (TSH), total cholesterol, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), fasting blood glucose (FBG), and left ventricular ejection fraction (LVEF). These indicators were collected for each patient to assessed potential links with long-term depression risk post-PCI. Prior to analysis, duplicate records were removed, continuous variables (eg, laboratory values) were verified to fall within biologically plausible ranges, and categorical entries (eg, smoking status) were confirmed for validity to ensure data quality. Additionally, the dataset was randomly divided using a fixed random seed, with 70% of the data allocated to the training set (n=1366) and 30% to the validation set (n=585) to facilitate subsequent model construction and evaluation. To mitigate bias and overfitting, the split was stratified by depression status (19.58% prevalence) to ensure proportional representation, and a fixed random seed (123) was used for reproducibility. Data anonymization was ensured prior to analysis.
Depression Assessment and Follow-up
Depression after PCI was recorded based on clinical evaluations conducted during follow-up visits over a minimum period of 12 months. In this study, the PHQ-9 was used to assess depression by asking participants if they had experienced a series of depression symptoms during the follow-up period.16 Depression was diagnosed according to the International Classification of Diseases, Tenth Edition (ICD-10). Patients were stratified into depressed and non-depressed groups based on these evaluations.
Feature Selection
Feature selection was conducted using the Boruta algorithm, a random forest-based wrapper method. The algorithm was run with 300 iterations to ensure robust identification of relevant predictors by comparing the importance of real variables against randomized shadow features and iteratively eliminating non-informative predictors to reduce overfitting and enhance model interpretability. This ensured that only the most relevant predictors were included in the final model.
Restricted Cubic Spline Analysis
Restricted cubic spline (RCS) analysis was applied to evaluate the non-linear associations between the variables selected by the Boruta algorithm and the risk of long-term depression in ACS patients post-PCI. RCS allowed for the modeling of flexible, non-linear relationships between continuous predictors and the outcome by dividing the range of each predictor into segments defined by a set of knots. RCS was used to model non-linear relationships by dividing predictor ranges into segments defined by 3–5 knots, selected based on Akaike’s Information Criterion.
Model Development and Validation
The variables selected through the Boruta algorithm were incorporated into six machine learning models: Light Gradient Boosting Machine (LGBM), Extreme Gradient Boosting (XGBoost), Logistic Regression (LR), Naive Bayes Model (NBM), Support Vector Machine (SVM), and Decision Tree (DT). The models were trained using 70% of the dataset and validated on the remaining 30%. Hyperparameter tuning was performed to optimize predictive accuracy, with specific parameters for XGBoost, LightGBM, LR, and SVM detailed in Supplementary Material 1. Performance was assessed using metrics such as sensitivity, specificity, precision, recall, F1 score, balanced accuracy, and area under the curve (AUC). Model tuning was performed using cross-validation techniques and hyperparameter optimization to maximize the predictive accuracy of each model.
Model Interpretation and Clinical Utility
The best-performing model(s) were selected for further analysis to interpret the contribution of each feature to the prediction of long-term depression risk. SHapley Additive exPlanations (SHAP) analysis was conducted to quantify the influence of each variable on model predictions. This analysis provided insight into the most influential predictors and how they impacted the model’s output. Additionally, the clinical utility of the models was assessed using calibration curves, which evaluated the alignment between predicted probabilities and observed outcomes. Decision curve analysis was performed to assessed the net clinical benefit across various threshold probabilities, helping to determined the practical value of the model in clinical decision-making. Precision-recall curves were also generated to evaluated the trade-offs between precision and recall, providing a detailed assessment of model performance.
Statistical methods
Statistical analysis was performed using R (version 4.4.2). The normality of continuous variables was assessed using the Shapiro–Wilk test, and none were normally distributed. Descriptive statistics were used to summarize baseline characteristics, with continuous variables expressed as medians and interquartile ranges (IQRs), and categorical variables as frequencies and percentages. Group comparisons between depressed and non-depressed patients were conducted using the Mann–Whitney U-test for continuous variables and the Chi-square test for categorical variables.The Boruta algorithm was utilized for feature selection to identify the most significant predictors of long-term depression risk, resulting in 10 important variables. These variables were then used in six ML models: LGBM, XGBoost, LR, NBM, SVM, and DT. LGBM and XGBoost emerged as the best-performing models, and SHAP analysis was conducted to interpret the contributions of each feature in these models. Calibration curves, decision curve analysis, and precision-recall curves were used to evaluate model performance and clinical utility. Statistical significance was defined as a p-value of less than 0.05.
Results
Baseline Characteristics
This study enrolled 1951 ACS patients who underwent PCI, with 382 (19.58%) developing depression(Table 1). The overall median age was 63 years (IQR: 54–72), with no significant difference between depressed (64 years, IQR: 55.25–73) and non-depressed groups (63 years, IQR: 54–72, p=0.131). Males comprised 63.92% of the cohort, with a higher proportion in the non-depressed group (65.77% vs 56.28%, p<0.001). Ethnicity showed no significant difference (p=0.099), with Han Chinese being the majority (51.15%). Depressed patients had higher new york heart association(NYHA) class 3 (39.53% vs 24.60%) and class 4 (10.47% vs 6.12%, p<0.001), more frequent PCI history (26.44% vs 18.93%, p<0.001), and higher diabetes prevalence (51.05% vs 34.29%, p<0.001). Sleep disorders were more common in the depressed group (41.10% vs 29.70%, p<0.001). Laboratory findings showed higher WBC counts (7.58 vs 6.94 ×109/L, p<0.001), FBG levels (115.69 vs 108.30 mg/dL, p=0.015), and lower TSH levels (1.71 vs 2.20 mIU/L, p<0.001) and LVEF (61.90%, IQR: 47.09–63.69 vs 61.90%, IQR: 57.97–63.69, p<0.001) in the depressed group.The baseline characteristics of the training and validation sets are provided in Supplementary Table 1, showing no significant differences between the two groups. The research flowchart detailing participant selection and analysis is presented in Figure 1. Supplementary Figure 1 presents the correlation heatmap of continuous variables, highlighting strong positive correlations, such as between total cholesterol and LDL-C, and negative correlations, like the inverse relationship between LVEF and WBC.
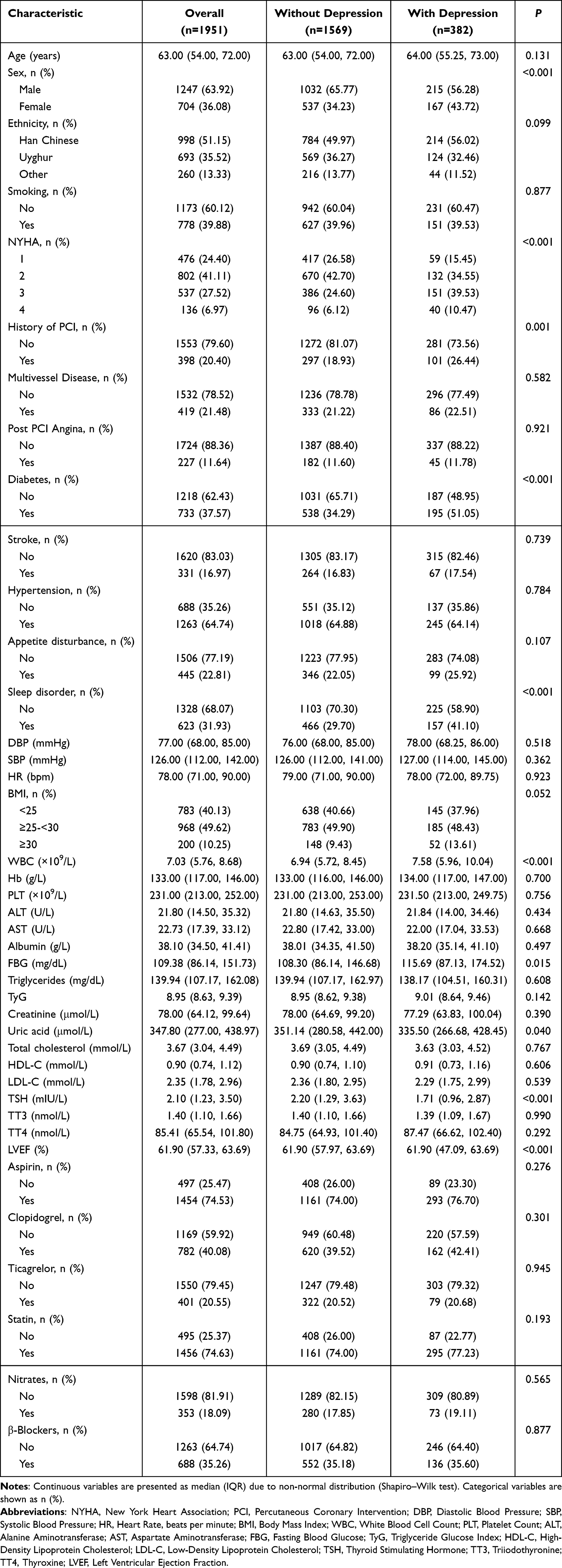 |
Table 1 Baseline Characteristics of ACS Patients Who Underwent PCI Stratified by Depression Status |
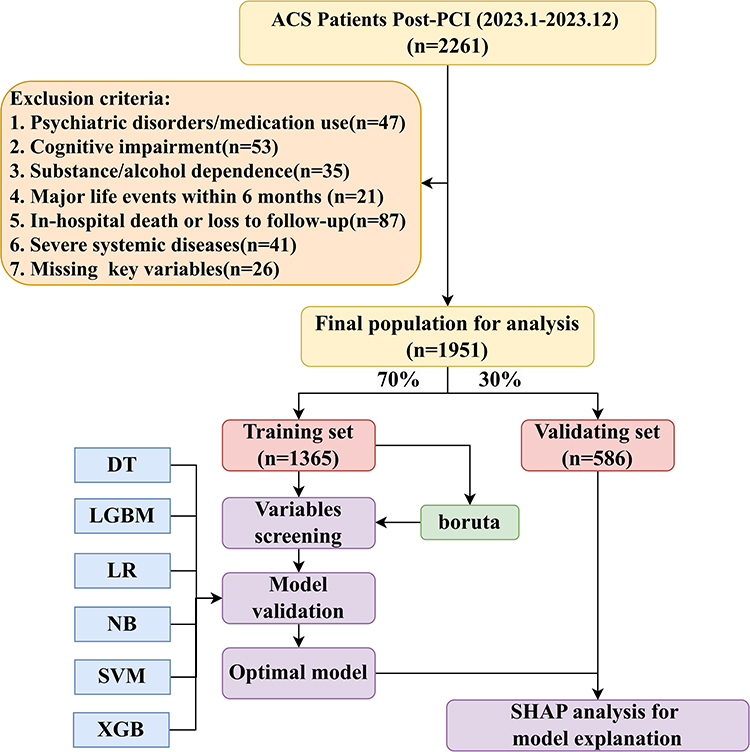 |
Figure 1 Study Flowchart Depicting Participant Selection and Analysis Workflow. |
Feature Selection and Importance Using the Boruta Algorithm
The Boruta algorithm was applied to systematically evaluate the predictive significance of multiple candidate variables for assessing long-term depression risk in ACS patients who underwent PCI. Through this rigorous analysis, 10 variables were identified as critical predictors: NYHA classification, WBC, TyG, uric acid, sleep disorder, LDL-C, TSH, diabetes, total cholesterol, and LVEF. These variables, represented by green bars in Figure 2, were consistently validated as significant contributors to the predictive model. In contrast, yellow bars correspond to variables with tentative importance, while red bars denote those classified as insignificant. This stratified representation underscores the reliability of the feature selection process, ensuring that only robust predictors were included. Supplementary Figure 2 further corroborates these findings by illustrating the variability in feature importance scores across 300 iterations. This iterative stability analysis highlights the consistency and robustness of the selected predictors, further reinforcing the credibility and predictive accuracy of the model.
 |
Figure 2 Variable Importance Identified by the Boruta Model for Predicting Long-Term Depression Risk in ACS Patients Who Underwent PCI. |
RCS Analysis of Depression Risk Predictors
RCS analysis revealed significant non-linear associations between key biomarkers and long-term depression risk among ACS patients who underwent PCI (Figure 3). The knot values for these predictors are detailed in Supplementary Table 2. WBC showed an inverted U-shaped relationship, with depression risk peaking at 7.03 and declining at both lower and higher levels. The TyG index demonstrated a sharp rise in risk beyond 8.95, indicating the critical role of metabolic dysfunction. Uric acid exhibited a threshold effect at 347.8, with risk increasing sharply above this level. LDL-C and total cholesterol showed linear positive trends, with knots at 2.35 and 3.67, respectively, suggesting their contribution to depression risk. TSH followed a U-shaped curve, with both hypo- and hyperthyroidism increasing risk, and a critical threshold at 2.1. LVEF displayed a consistent protective effect, with a negative association and a knot at 61.9. These findings highlight the heterogeneity of these biomarkers’ roles and the importance of accounting for non-linear effects when assessing depression risk.
 |
Figure 3 Restricted Cubic Spline Analysis of Key Features and Long-Term Depression Risk in ACS Patients Who Underwent PCI. The plots show the relationship between various biomarkers and the odds of developing long-term depression in ACS patients after PCI, as modeled using restricted cubic splines (RCS). (A) White Blood Cell Count (WBC), (B) Triglyceride-Glucose Index(TyG), (C) Left Ventricular Ejection Fraction (LVEF), (D) Total Cholesterol, (E) Low-Density Lipoprotein Cholesterol (LDL-C), (F) Thyroid Stimulating Hormone (TSH), and (G) Uric Acid. The P-value for the overall test and the P-value for the non-linear association are provided in each plot. The dashed line represents the reference point for each biomarker. |
Performance Comparison of ML Models
The predictive performance of six ML models—LGBM, XGBoost, LR, NBM, SVM, and DT—was assessed for predicting long-term depression risk in ACS patients who underwent PCI. As shown in the receiver operating characteristic curves (Figure 4) and summarized in Table 2, LGBM and XGBoost outperformed the other models, achieving the highest AUC values in both training and validation datasets. XGBoost achieved an AUC of 0.814 (95% CI: 0.788–0.840) in the training set and 0.699 (95% CI: 0.643–0.756) in the validation set, while LGBM obtained the highest training AUC of 0.849 (95% CI: 0.826–0.873) and a validation AUC of 0.652 (95% CI: 0.593–0.711). In terms of balanced accuracy, LGBM achieved 0.771 in the training set and 0.594 in the validation set, followed by XGBoost with 0.743 and 0.636, respectively. In contrast, LR demonstrated moderate performance, while DT exhibited slightly lower predictive capability. NBM and SVM performed the weakest, showing limited discriminative ability. Supplementary Figure 3, presenting a heatmap of model performance metrics, further highlights the consistent superiority of LGBM and XGBoost in predictive accuracy.
 |
Table 2 Performance Comparison of Six Machine Learning Models in Training and Validation Sets |
 |
Figure 4 Receiver operating characteristic Curve Comparison of Models for Predicting Long-Term Depression Risk in ACS Patients Who Underwent PCI. The plots show the ROC curves of (A) Extreme Gradient Boosting, (B) Light Gradient Boosting Machine, (C) Logistic Regression, (D) Naive Bayes, (E) Support Vector Machine, and (F) Decision Tree in predicting long-term depression risk in ACS patients after PCI. Each plot displays the AUC values for the test and training datasets, with test AUC and train AUC represented by red and blue curves, respectively. |
Model Calibration and Clinical Decision Support
Calibration and decision curve analyses (Figure 5) provided additional insights into the models’ performance and clinical utility. Brier scores ranged from 0.118 to 0.166 in the training set, and from 0.134 to 0.166 in the validation set (Supplementary Table 3). Among all models, LGBM and XGBoost demonstrated relatively better calibration, with predicted probabilities aligning more closely with observed outcomes. Decision curve analyses indicated meaningful net clinical benefit across a wide range of threshold probabilities, particularly for LGBM and XGBoost. Precision-recall curves further supported their robustness, with LGBM showing slightly improved balance between precision and recall, reinforcing its potential value in clinical risk stratification.
 |
Figure 5 Model Performance Comparison Across Six Models in Training and Validation Sets. Each curve represents a different model: DT (Decision Tree), LGBM (Light Gradient Boosting Machine), LR (Logistic Regression), NBM (Naive Bayes Model), SVM (Support Vector Machine), and XGBoost (Extreme Gradient Boosting). (A) Calibration curve for the training set. (B) Decision curve analysis for the training set. (C) Precision-recall curve for the training set. (D) Calibration curve for the validation set. (E) Decision curve analysis for the validation set. (F) Precision-recall curve for the validation set. |
SHAP Analysis of Feature Contributions in LGBM and XGBoost Models
We selected the best-performing models, LGBM and XGBoost, from six ML algorithms for predicting long-term depression risk in ACS patients who underwent PCI, and conducted SHAP analysis to interpret their feature contributions (Figure 6). Both models consistently identified NYHA classification, diabetes, and TSH as the most important predictors, with the LGBM model (Figure 6A) ranking TSH as the top feature, followed by NYHA classification and diabetes. In contrast, the XGBoost model (Figure 6B) highlighted NYHA classification as the most influential feature, followed by diabetes and TSH. SHAP summary plots demonstrated that higher NYHA classifications and the presence of diabetes were strongly associated with increased depression risk, while TSH exhibited a U-shaped relationship, indicating heightened risk at both low and high levels. SHAP value distribution plots (Figure 6C and D) provided additional insights into feature-specific variability, illustrating non-linear relationships such as a positive linear association for LDL-C and threshold effects for TyG and uric acid, where risk sharply increased beyond critical values. Supplementary Figure 4 shows the SHAP dependence plots for LGBM and XGBoost models, further illustrating the feature-specific relationships.
 |
Figure 6 SHAP Analysis of Feature Contributions in Predicting Long-Term Depression Risk Using XGBoost. (A) SHAP summary plot for LGBM, ranking features by importance. (B) SHAP summary plot for XGBoost, ranking features by importance. (C) SHAP dependence plot for LGBM, showing SHAP-feature value relationships. (D) SHAP dependence plot for XGBoost, showing similar trends. |
Discussion
This study successfully developed and validated ML models to predict long-term depression risk in ACS patients following PCI, addressing a significant gap in comorbidity management. The LightGBM and XGBoost models exhibited superior predictive performance, with AUC values ranging from 0.86 to 0.89. These models effectively integrated 10 multidimensional predictors, including NYHA classification, TSH levels, diabetes status, and lipid profiles. Additionally, the observed discrepancy between training and validation AUCs for LGBM (0.849 vs 0.652) and XGBoost (0.814 vs 0.699), along with reduced balanced accuracy in the validation set, suggests potential overfitting. This performance gap may reflect intrinsic data complexity or differences in predictor interactions across subsets. Although internal validation techniques such as early stopping and regularization were employed, future research should incorporate K-fold cross-validation and external validation cohorts to enhance generalizability and reduce overfitting risk. SHAP analysis revealed non-linear relationships between these factors and depression risk, highlighting the unique advantage of ML in capturing complex interactions that traditional methods may miss.
Depression is prevalent among ACS patients post-PCI, with a rate of 19.58% in this study, aligning with previous research emphasizing the high incidence of depression in this population.17–19 Depression among ACS patients contributes to poor outcomes, including reduced quality of life and increased cardiovascular mortality,20,21 underscoring the necessity for routine screening and treatment. Our study further identifies depression as a key predictor of poor prognosis, especially in patients with comorbidities like diabetes and thyroid dysfunction, supported by De Luca et al.22
The importance of early identification and intervention is further supported by Hayajneh et al23 who highlighted that depression in older adults with ACS seeking emergency care significantly affects clinical outcomes, including length of hospital stays. Miao et al24 developed a nomogram predicting depression in post-PCI patients and identified key factors like baseline PHQ-9 scores that could guide prediction. Our results are in line with these findings, as we identified several key predictors of depression, including sleep disorders, diabetes, and TSH levels. Additionally, our use of ML models (eg, LightGBM and XGBoost) to predict depression risk complements findings by Podolec et al25 who demonstrated that depression is a major risk factor for adverse cardiovascular events, particularly after interventions like PCI. This reinforces the critical need for early identification and intervention in post-PCI patients, as failure to address depression can worsen cardiovascular outcomes.
Psychosocial interventions have been shown to significantly reduce depression levels post-ACS, as demonstrated by Lim et al.26 This supports our call for integrated mental health strategies in cardiac care. Moreover, the lack of significant difference in treatment efficacy among various depression therapies post-ACS, as shown by Sanchez et al27 highlights the complexity of treating depression after a cardiac event. Despite this, the predictive tools we have developed could potentially facilitate more personalized interventions, improving patient outcomes by focusing on high-risk individuals. The work of Liu et al28 suggests that non-pharmacological interventions, such as Tai Chi, can help manage anxiety and depression post-PCI, reinforcing the importance of a holistic approach to care. Similarly, Wang et al29 emphasized that psychological distress, including depression, is closely linked to poorer physical function and cardiovascular events, further highlighting the need for integrated care in ACS patients.
The key predictors identified in our study are closely linked to the biological mechanisms underlying depression. The NYHA classification reflects cardiac function, while a reduced LVEF is indicative of heart failure. Heart failure may increase depression risk through mechanisms such as chronic hypoxia, inflammation, and fatigue.30–32 The U-shaped relationship observed between TSH and depression risk suggests that both suppressed and elevated thyroid function may adversely affect mood regulation. At the low end, hyperthyroidism or subclinical hyperthyroidism may lead to heightened sympathetic nervous system activity and hypothalamic–pituitary–adrenal (HPA) axis dysregulation, contributing to anxiety and mood instability. Conversely, hypothyroidism has been associated with impaired serotonergic neurotransmission, reduced neurogenesis, and cerebral hypometabolism—all of which are implicated in depressive symptoms. This bidirectional association supports the role of TSH as a sensitive neuropsychiatric biomarker.33–35 Our findings align with previous large-scale studies that have reported similar U-shaped associations between FT4 or TSH and depressive symptoms or events in euthyroid individuals.36,37 Given the relatively subtle but consistent associations, the model we propose could have practical value in risk stratification and targeted screening of subclinical thyroid dysfunction in patients at risk of depression.
Diabetes further elevates the risk of depression through insulin resistance and chronic inflammation.38 A cross-sectional study involving over 160,000 individuals in South Korea found that higher depression risk is associated with insulin resistance, with a 4% and 17% increase in depression risk among young individuals and non-diabetic individuals, respectively, as insulin resistance increases.39 The TyG index, a recently developed marker of insulin resistance, not only reflects insulin resistance but also correlates with adverse health conditions such as diabetes, metabolic syndrome, and lipid metabolism disorders.40–44
Lower uric acid levels in individuals with depression, compared to the general population, suggest that uric acid may play a role in antioxidant stress.45,46 However, other studies have found a significant association between higher uric acid levels and depression symptoms, particularly in postmenopausal women.47,48 Our study revealed a non-linear relationship between uric acid levels and depression risk, with higher risk at both low and high levels. Elevated WBC count, reflecting systemic inflammation, supports the neuroinflammatory hypothesis of depression.49,50 Inflammatory markers can affect the brain either by crossing the blood-brain barrier or by influencing cerebral capillary function, thereby impacting neuronal activity and the synthesis and release of neurotransmitters (such as serotonin and dopamine), which are closely linked to depressive symptoms.49 Sleep disorders have a bidirectional relationship with depression, acting both as a symptom and a risk factor.51,52 Specifically, sleep disorders can disrupt neurotransmitter balance, further increasing the risk of depression.53 Elevated LDL-C and total cholesterol levels may contribute to depression through their impact on cerebral blood flow and neuronal function.54,55 These biological mechanisms support the rationale for selecting the predictors used in our study.
Clinically, the developed ML models offer practical value by enabling early risk stratification for long-term depression following PCI. Integrated into hospital electronic health systems, these tools can help flag high-risk patients for targeted psychological screening and proactive management. This may improve mental health outcomes and overall prognosis by guiding early multidisciplinary interventions.
Limitations
Despite the strengths, this study has several limitations. Firstly, the retrospective nature of the study may introduce selection bias and information bias. Although we attempted to control for confounding factors, unmeasured variables may still have influenced the results. Future studies should consider a prospective cohort design to minimize these biases. Secondly, the model performance was relatively lower in the validation set compared to the training set, indicating potential overfitting. Although we used cross-validation and hyperparameter optimization techniques, further efforts are needed to improve the generalizability of the models. Thirdly, the study only included patients from a single center, which may limit the external validity of the findings. Future studies should validate the models in different populations and settings to ensure their applicability. Finally, the interpretation of SHAP values requires caution, as it is based on the statistical associations rather than causal relationships. Future studies should explore causal inference methods to better understand the underlying mechanisms.
Conclusion
This study developed and validated ML models to predict long-term depression risk in ACS patients following PCI. The models demonstrated promising predictive performance and identified key clinical and laboratory factors associated with depression risk, offering potential utility for future clinical applications. These findings underscore the potential of ML to facilitate early risk stratification and targeted intervention among high-risk patients. However, further research is warranted to overcome current limitations, enhance model generalizability and interpretability, and investigate causal mechanisms underlying these associations. Future studies should also aim to develop and test more effective prevention and treatment strategies to improve long-term outcomes in this population.
Data Sharing Statement
The data has not been previously presented orally or by poster at scientific meetings. The data used or generated in this study are available from the corresponding author upon reasonable request.
Ethical Approval
This study was conducted in accordance with the principles of the Helsinki Declaration and was approved by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University (241024-02). As this study is retrospective, the medical record data used were obtained from previous clinical diagnoses and treatments, and the requirement for informed consent was waived by the Ethics Committee.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the State Key Laboratory of Pathogenesis, Prevention and Treatment of High Incidence Diseases in Central Asia Fund (SKL-HIDCA-2024-RWS3).
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019. J Am Coll Cardiol. 2020;76(25):2982–3021. doi:10.1016/j.jacc.2020.11.010
2. Byrne RA, Rossello X, Coughlan JJ, et al. 2023 ESC guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44(38):3720–3826. doi:10.1093/eurheartj/ehad191
3. Song X, Song J, Shao M, et al. Depression predicts the risk of adverse events after percutaneous coronary intervention: a meta-analysis. J Affect Disord. 2020;266:158–164. doi:10.1016/j.jad.2020.01.136
4. Damen NL, Versteeg H, Boersma E, et al. Depression is independently associated with 7-year mortality in patients treated with percutaneous coronary intervention: results from the RESEARCH registry. Int J Cardiol. 2013;167(6):2496–2501. doi:10.1016/j.ijcard.2012.04.028
5. van Dijk MR, Utens EMWJ, Dulfer K, et al. Depression and anxiety symptoms as predictors of mortality in PCI patients at 10 years of follow-up. Eur J Prev Cardiol. 2016;23(5):552–558. doi:10.1177/2047487315571889
6. Hou Y, Zhang D, Zhu J, et al. Short report: depression and anxiety symptoms as predictors of adverse cardiovascular events in Chinese patients after percutaneous coronary intervention. Psychol Health Med. 2021;26(9):1126–1133. doi:10.1080/13548506.2020.1837388
7. Dong Z, Yang Q, Chen H. Estimating the prevalence of depression in people with acute coronary syndromes: a systematic review and meta-analysis. Medicine. 2024;103(17):e37906. doi:10.1097/MD.0000000000037906
8. Saini RK, Chaudhury S, Singh N, et al. Depression, anxiety, and quality of life after percuataneous coronary interventions. Ind Psychiatry J. 2022;31(1):6–18. doi:10.4103/ipj.ipj_126_21
9. Simon GE, Moise N, Mohr DC. Management of depression in adults: a review. JAMA. 2024;332(2):141–152. doi:10.1001/jama.2024.5756
10. Tan J, Ma C, Zhu C, et al. Prediction models for depression risk among older adults: systematic review and critical appraisal. Ageing Res Rev. 2023;83:101803. doi:10.1016/j.arr.2022.101803
11. Lin W, Zhang D, Wang Y, et al. Analysis of depression status and influencing factors in middle-aged and elderly patients with chronic diseases. Front Psychol. 2024;15. doi:10.3389/fpsyg.2024.1308397
12. Kang H-J, Stewart R, Bae K-Y, et al. Predictors of depressive disorder following acute coronary syndrome: results from K-DEPACS and EsDEPACS. J Affect Disord. 2015;181:1–8. doi:10.1016/j.jad.2015.04.004
13. Abd-Alrazaq A, AlSaad R, Shuweihdi F, et al. Systematic review and meta-analysis of performance of wearable artificial intelligence in detecting and predicting depression. Npj Digital Med. 2023;6(1):1–16. doi:10.1038/s41746-023-00828-5
14. Rauschert S, Raubenheimer K, Melton PE, et al. Machine learning and clinical epigenetics: a review of challenges for diagnosis and classification. Clin Clin Epigenet. 2020;12(1):51. doi:10.1186/s13148-020-00842-4
15. Greener JG, Kandathil SM, Moffat L, et al. A guide to machine learning for biologists. Nat Rev Mol Cell Biol. 2022;23(1):40–55. doi:10.1038/s41580-021-00407-0
16. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
17. Li C, Wan S, Li W, et al. Higher neutrophil to lymphocyte ratio at admission is association with Post-PCI depressive symptoms in patients with ACS. Neuropsychiatr Dis Treat. 2022;18:2981–2990. doi:10.2147/NDT.S387582
18. Guan J, Wang Y, Dong C, et al. The impact of the triglyceride-glucose index on the development of depression in patients with coronary atherosclerotic heart disease. Neuropsychiatr Dis Treat. 2024;20:2105–2113. doi:10.2147/NDT.S484745
19. Moise N, Davidson KW, Clarke GN, et al. Differences in the prevalence of screen-detected depression after acute coronary syndrome between health systems in the USA: findings from CODIACS-QoL randomized controlled trial. J Gen Intern Med. 2022;37(7):1808–1810. doi:10.1007/s11606-021-07049-0
20. Leong LK, Zuhdi ASM, Hafidz MIA. Clinical depression among patients after acute coronary syndrome: a prospective single-tertiary centre analysis. Singapore Med J. 2021;62(12):653–658. doi:10.11622/smedj.2020079
21. Pan R, Fan Q, Tao R. Depression following acute coronary syndrome: a review. Rev Cardiovasc Med. 2023;24(9):247. doi:10.31083/j.rcm2409247
22. De Luca L, Temporelli PL, Amico AF, et al. Impact of history of depression on 1-year outcomes in patients with chronic coronary syndromes: an analysis of a contemporary, prospective, nationwide registry. Int J Cardiol. 2021;331:273–280. doi:10.1016/j.ijcard.2020.12.086
23. Hayajneh AA, Rababa M, Al-Nusour EA, et al. Predictors of depression amongst older adults with acute coronary syndrome seeking emergency care. Int J Clin Pract. 2021;75(7):e14203. doi:10.1111/ijcp.14203
24. Miao X, Chen Y, Qiu X, et al. Construction and validation of a nomogram predicting depression risk in patients with acute coronary syndrome undergoing coronary stenting: a prospective cohort study. J Cardiovasc Dev Dis. 2023;10(9):385. doi:10.3390/jcdd10090385
25. Podolec J, Kleczyński P, Piechocki M, et al. Depression in cardiac patients is a major cardiovascular event risk factor: a 12-month observational study. J Clin Med. 2024;13(22):6911. doi:10.3390/jcm13226911
26. Lim GE, Tang A, Chin YH, et al. A network meta-analysis of 12,116 individuals from randomized controlled trials in the treatment of depression after acute coronary syndrome. PLoS One. 2022;17(11). doi:10.1371/journal.pone.0278326
27. Sanchez GJ, Sumner JA, Schwartz JE, et al. Anhedonic depression is not associated with risk of recurrent major adverse cardiac events and all-cause mortality in acute coronary syndrome patients. Ann Behav Med. 2023;57(2):155–164. doi:10.1093/abm/kaab092
28. Liu J, Yu P, Lv W, et al. The 24-Form Tai Chi improves anxiety and depression and upregulates miR-17-92 in coronary heart disease patients after percutaneous coronary intervention. Front Physiol. 2020;11:149. doi:10.3389/fphys.2020.00149
29. Wang J, Li T, Gu Y, et al. The value of anxiety and depression in predicting physical function and major adverse cardiovascular events in patients with acute coronary syndrome. J Thorac Dis. 2024;16(10):6849–6862. doi:10.21037/jtd-24-576
30. Husain MI, Chaudhry IB, Husain MO, et al. Depression and congestive heart failure: a large prospective cohort study from Pakistan. J Psychosom Res. 2019;120:46–52. doi:10.1016/j.jpsychores.2019.03.008
31. Zhang L, Wang Q, Cui H-S, et al. Assessing myocardial indices and inflammatory factors to determine anxiety and depression severity in patients with chronic heart failure. World J Psychiatry. 2024;14(1):53–62. doi:10.5498/wjp.v14.i1.53
32. Lossnitzer N, Feisst M, Wild B, et al. Cross-lagged analyses of the bidirectional relationship between depression and markers of chronic heart failure. Depress Anxiety. 2020;37(9):898–907. doi:10.1002/da.23041
33. Van der lingen A-LCJ, Rijnierse MT, Hooghiemstra AM, et al. The link between cardiac status and depression and anxiety in implantable cardioverter defibrillator patients: design and first results of the PSYCHE-ICD study. J Psychosom Res. 2023;167:111182. doi:10.1016/j.jpsychores.2023.111182
34. Hong JW, Noh JH, Kim D-J. Association between subclinical thyroid dysfunction and depressive symptoms in the Korean adult population: the 2014 Korea national health and nutrition examination survey. PLoS One. 2018;13(8):e0202258. doi:10.1371/journal.pone.0202258
35. Wu J, Wang Z, Xu H, et al. Thyroid dysfunction in young, first-episode and drug-naïve patients with major depressive disorder: prevalence and associated clinical factors. Front Psychiatry. 2023;14:1156481. doi:10.3389/fpsyt.2023.1156481
36. Roa Dueñas OH, Hofman A, Luik AI, et al. The cross-sectional and longitudinal association between thyroid function and depression: a population-based study. J Clin Endocrinol Metab. 2023;109(5). doi:10.1210/clinem/dgad620
37. Ma Y, Wang M, Zhang Z. The association between depression and thyroid function. Front Endocrinol. 2024;15. doi:10.3389/fendo.2024.1454744
38. Fetahu A, Rrustemi K, Henein MY, et al. Obesity and uncontrolled diabetes predict depression in HF patients. J Clin Med. 2021;10(23):5663. doi:10.3390/jcm10235663
39. Lee J-H, Park SK, Ryoo J-H, et al. The association between insulin resistance and depression in the Korean general population. J Affect Disord. 2017;208:553–559. doi:10.1016/j.jad.2016.10.027
40. Shi -Y-Y, Zheng R, Cai -J-J, et al. The association between triglyceride glucose index and depression: data from NHANES 2005–2018. BMC Psychiatry. 2021;21(1):267. doi:10.1186/s12888-021-03275-2
41. Liu X, Li J, He D, et al. Association between different triglyceride glucose index-related indicators and depression in premenopausal and postmenopausal women: NHANES, 2013–2016. J Affect Disord. 2024;360:297–304. doi:10.1016/j.jad.2024.05.084
42. Zhang X, Zhao D, Guo S, et al. Association between triglyceride glucose index and depression in hypertensive population. J Clin Hypertens. 2024;26(2):177–186. doi:10.1111/jch.14767
43. Behnoush AH, Mousavi A, Ghondaghsaz E, et al. The importance of assessing the triglyceride-glucose index (TyG) in patients with depression: a systematic review. Neurosci Biobehav Rev. 2024;159:105582. doi:10.1016/j.neubiorev.2024.105582
44. Xu C, Wang D, Sun M, et al. Joint effects of depressive symptoms and triglyceride-glucose index on cardiovascular events in acute coronary syndrome patients: the mediating role of TyGi. J Psychosom Res. 2025;189:112034. doi:10.1016/j.jpsychores.2024.112034
45. Meng X, Huang X, Deng W, et al. Serum uric acid a depression biomarker. PLoS One. 2020;15(3):e0229626. doi:10.1371/journal.pone.0229626
46. Wang J, Yang M, Lin H, et al. Association between uric acid and the risk of depressive symptoms in US adults: results from NHANES 2005–2018. Sci Rep. 2024;14(1):24097. doi:10.1038/s41598-024-74869-5
47. Chen J, Zhou W, Huang Y. Association between serum uric acid levels and depressive symptoms according to menopausal status. J Affect Disord. 2024;350:240–246. doi:10.1016/j.jad.2024.01.108
48. Kim JO, Park GN, Oh JW, et al. Association between uric acid and depressive symptoms in older adults: the Korea national health and nutrition examination survey. Int J Geriatr Psychiatry. 2023;38(7):e5963. doi:10.1002/gps.5963
49. Wang L, Liu L, Liu X, et al. The association between neutrophil percentage-to-albumin ratio (NPAR) and depression among US adults: a cross-sectional study. Sci Rep. 2024;14(1):21880. doi:10.1038/s41598-024-71488-y
50. Su M, Ouyang X, Song Y. Neutrophil to lymphocyte ratio, platelet to lymphocyte ratio, and monocyte to lymphocyte ratio in depression: a meta-analysis. J Affect Disord. 2022;308:375–383. doi:10.1016/j.jad.2022.04.038
51. Yasugaki S, Okamura H, Kaneko A, et al. Bidirectional relationship between sleep and depression. Neurosci Res. 2025;211:57–64. doi:10.1016/j.neures.2023.04.006
52. Fang H, Tu S, Sheng J, et al. Depression in sleep disturbance: a review on a bidirectional relationship, mechanisms and treatment. J Cell Mol Med. 2019;23(4):2324–2332. doi:10.1111/jcmm.14170
53. Cheng M, Lei X, Zhu C, et al. The association between poor sleep quality and anxiety and depression symptoms in Chinese patients with coronary heart disease. Psychol Health Med. 2022;27(6):1347–1356. doi:10.1080/13548506.2021.1874440
54. Han K-T, Kim SJ. Are serum cholesterol levels associated with cognitive impairment and depression in elderly individuals without dementia?: a retrospective cohort study in South Korea. Int J Geriatr Psychiatry. 2021;36(1):163–173. doi:10.1002/gps.5410
55. Zhong X, Ming J, Li C. Association between dyslipidemia and depression: a cross-sectional analysis of NHANES data from 2007 to 2018. BMC Psychiatry. 2024;24(1):893. doi:10.1186/s12888-024-06359-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.