Back to Journals » Nature and Science of Sleep » Volume 17

Development and Validation of a 7-Day Postoperative Sleep Disturbance Predictive Nomogram in Non-Cardiovascular Surgical Patients: A Prospective Cohort Study of 3851 Adults
Authors Mao JL ![]() , Shu SH
, Shu SH ![]() , Hu L, Wang XF, Wang S, Fan XQ
, Hu L, Wang XF, Wang S, Fan XQ
Received 28 May 2025
Accepted for publication 1 September 2025
Published 1 October 2025 Volume 2025:17 Pages 2437—2453
DOI https://doi.org/10.2147/NSS.S536630
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Valentina Alfonsi
Jia-Li Mao, Shu-Hua Shu, Ling Hu, Xue-Feng Wang, Sheng Wang, Xiao-Qing Fan
Department of Anesthesiology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei City, Anhui Province, People’s Republic of China
Correspondence: Shu-Hua Shu, Department of Anesthesiology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei City, Anhui Province, People’s Republic of China, Email [email protected]
Purpose: This prospective study developed and validated a nomogram to assess the likelihood of early postoperative sleep disturbance (PSD occurring within 7 days after surgery) following non-cardiovascular surgical procedures.
Participants and Study Protocol: The study enrolled 3851 patients receiving non-cardiac procedures recruited in the First Affiliated Hospital of USTC from April 2024 to December 2024. These 3851 patients were randomly allocated into training cohort (n=2682, 70%) and validation cohorts (n=1169, 30%). Variable selection was performed using least absolute shrinkage and selection operator (LASSO) regression, followed by logistic regression analyses (univariate and multivariate) to identify independent risk factors. Based on these identified factors, a prognostic nomogram was developed and underwent comprehensive validation, including receiver operating characteristic (ROC) curve assessment, calibration plotting, and decision curve analysis (DCA) to evaluate its discriminative performance and clinical applicability.
Results: About 37.7% of patients developed PSD within the first 7 postoperative days, with 12.1% persisting at 1 month after surgery. The analysis revealed ten independent PSD risk factors (all p < 0.05): female, higher ASA class (III), moderate-to-severe anemia, dissatisfaction with ward environment, anxiety, non-use of dexmedetomidine, older age, extended anesthesia time, lower sufentanil doses and higher postoperative NRS score. The nomogram incorporating these ten predictors demonstrated excellent discriminative performance, with AUC values of 0.826 (95% CI: 0.810– 0.843) in the training cohort and 0.822 (95% CI: 0.797– 0.847) in the validation cohort, complemented by optimal calibration.
Conclusion: The prediction model incorporating ten routinely available clinical variables demonstrated excellent predictive accuracy and good calibration, highlighting its clinical utility in identifying short-term high-risk PSD patients (within 7 days postoperatively). This tool facilitates timely interventions to reduce PSD incidence and improve recovery outcomes.
Keywords: risk factors, machine learning, dexmedetomidine, anesthesia, nomograms
Introduction
Postoperative sleep disturbances (PSD) represent a prevalent complication characterized by dysregulated sleep-wake patterns in surgical patients, manifesting through functional cerebral disturbances and autonomic hyperactivity that collectively impair sleep quality. This condition typically presents with prolonged sleep latency, sleep fragmentation, and impaired sleep quality.1
Several previous investigations have reported the incidence of PSD ranging from 30% to 80%,2–4 and more than 10% of patients continue to experience these symptoms for at least 6 months with potential for longer duration.5 Postoperative sleep quality are not routinely assessed, and even when sleep disturbances occur, they are often dismissed as part of normal recovery.
PSD often coexists with pain, depression, or delirium, complicating clinical recognition. Consequently, PSD remains overlooked by patients, families, and medical staff. However, persistent sleep deprivation triggers multiple adverse consequences: increased stress responses, hyperalgesia, cognitive decline, and cardiovascular instability – all significantly impairing recovery.6–10 Moreover, PSD shows strong associations with chronic post-surgical pain development while elevating fall risk and potentially reducing bone density.11
The etiology of PSD is multifactorial, encompassing advanced age, surgical trauma, anesthetic agents, inflammatory responses, psychological factors, postoperative pain, environmental disturbances such as noise, and nursing interventions.12–14 Typically, PSD results from complex interactions among these contributing elements. Current management of PSD incorporates a multimodal approach, including pharmacotherapy (dexmedetomidine, zolpidem, melatonin, and esketamine), ward environment enhancement and adoption of Cognitive Behavioral Therapy for Insomnia (CBT-I).15–18
While some predictive models for PSD have been investigated, current studies remain constrained by small sample sizes and procedure-specific designs like spinal surgeries,19,20 requiring further validation through larger-scale studies. This study aimed to develop and validate a predictive model for PSD in non-cardiovascular surgical patients, with the purpose of enabling early identification of high-risk individuals and guiding timely, targeted interventions to optimize sleep quality and postoperative recovery.
Material and Study Protocol
This prospective cohort study received ethical approval from the First Affiliated Hospital of USTC (Hefei, Anhui province, China) on 10 March, 2024 (No.2024-KY096). Prospective registration of this study was completed in the Chinese Clinical Trial Registry (ChiCTR 2400081957). It enrolled adult patients who underwent surgery with general anesthesia in the First Affiliated Hospital of USTC between April and December 2024. The study complied with the ethical principles of the Declaration of Helsinki, and written informed consent was acquired from all participants.
The study enrolled subjects according to these inclusion criteria: adult patients undergoing non-cardiovascular surgical procedures with general anesthesia, who were mentally competent to provide written informed consent.
Exclusion criteria included: (1) with pre-existing poor sleep quality as determined by Pittsburgh Sleep Quality Index (PSQI, authorized use licensed for this study) score ≥7; (2) duration of anesthesia less than 1 hour or exceeding 8 hours. (3) Regular use of sleep aids during perioperative period; (4) postoperatively transferred to the intensive care unit (ICU); (5) received brain surgery; Participants were consecutively enrolled without randomization.
Clinical Characteristics of All Patients
Thirty potential variables were analyzed in the study, categorized as:
Preoperative Factors
Baseline characteristics: Sex, age, education attainment, body mass index (BMI), preoperative night’s sleep quality and history of cigarette use; Medical history: Hypertension, diabetes mellitus, cardiac disease, obstructive sleep apnea–hypopnea syndrome (OSAHS), anemia, history of tumor, surgical history, depression and anxiety; Clinical metrics: ASA physical status, ward environment satisfaction, type of surgery.
Intraoperative Factors
Anesthesia duration and induction timing (morning/afternoon); Total opioid administration (sufentanil and remifentanil); Use of dexmedetomidine and sevoflurane.
Postoperative Factors
Time to extubation, patient-controlled intravenous analgesia (PCIA) utilization, postoperative nausea and vomiting (PONV), numeric rating scale (NRS) pain scores, length of hospital stay, and blood transfusion requirements.
Clinical parameters were prospectively recorded during hospitalization, with targeted assessment of PONV and NRS pain scores specifically performed on postoperative day 3. All follow-up data, including assessments conducted at postoperative day 3, week 1, and month 1, were collected through face-to-face interviews or telephone. All predictive variables and their measurement time points are detailed in Supplementary Table S1.
Assessment of Sleep Disruption
Postoperative sleep quality was measured using the validated PSQI score.21 It assesses seven components (scored 0–3 each): sleep onset latency, total sleep time, sleep maintenance efficiency, nocturnal awakenings, diurnal impairment, sedative medication use, and self-reported sleep quality.
In the study, PSD was assessed twice (at 7 days and 1 month postoperatively) via face-to-face interviews or telephone follow-ups using the PSQI. A PSQI score ≥7 was operationally defined as PSD. The nomogram was developed based solely on the 7-day postoperative PSD data.
Development and Assessment of the Nomogram
Potential predictors of PSD were initially identified using LASSO regression in the training cohort. Variables with non-zero coefficients selected by LASSO were first evaluated via univariate logistic regression, and those demonstrating significant associations (p < 0.05) were subsequently advanced to multivariable logistic regression. To enhance model interpretability and mitigate multicollinearity-though variance inflation factors (VIFs) were not explicitly calculated-LASSO regularization inherently reduced multicollinearity. The final model retained only a limited number of robust predictors, balancing parsimony and predictive performance.
The final predictors were then incorporated into a PSD risk prediction nomogram, developed using the rms package in R software (version 4.3.1). To enhance its clinical utilization, an online dynamic nomogram was created using ShinyApps. The predictive model underwent comprehensive internal validation through the bootstrap resampling method with 1000 iterations.
We evaluated the model’s predictive performance through three complementary approaches: (1) predictive discrimination evaluated using the receiver operating characteristic (ROC) curve’s area under the curve (AUC); (2) calibration accuracy examined through observed-versus-predicted analyses in both training and validation cohorts; and (3) clinical applicability evaluated using decision curve analysis (DCA) across standardized threshold probabilities. All assessments were implemented separately in the training and validation cohorts to ensure robust evaluation.
Sample Size Considerations
The final model incorporated 30 predictors (continuous, binary, and categorical), totaling 38 candidate predictor parameters. Using the conservative 20 events-per-parameter standard, we required ≥760 PSD events. Given the published PSD incidence rates (30–80%), the minimum sample size was 2534.
Statistical Analysis
Continuous variables following normal distribution were presented as mean ± standard deviation (SD) and analyzed via independent samples t-test, while median (interquartile range [IQR]) for non-normally distributed data and assessed using the Mann–Whitney test. Categorical variables were expressed as frequencies (percentages) and compared using the Chi-square test. A two-sided p-value threshold of 0.05 was established for determining statistical significance.
Results
The study initially enrolled a total of 4400 patients. A total of 549 patients were excluded from the study based on the following criteria: surgery cancellation (n=7), change in anesthesia mode (n=17), inappropriate anesthesia duration (less than 1 hour or exceeding 8 hours, n=97), unplanned ICU transfer (n=69), reoperation during hospitalization (n=37), and incomplete postoperative follow-up (n=322). Finally, data from 3851 patients were analyzed (Figure 1).
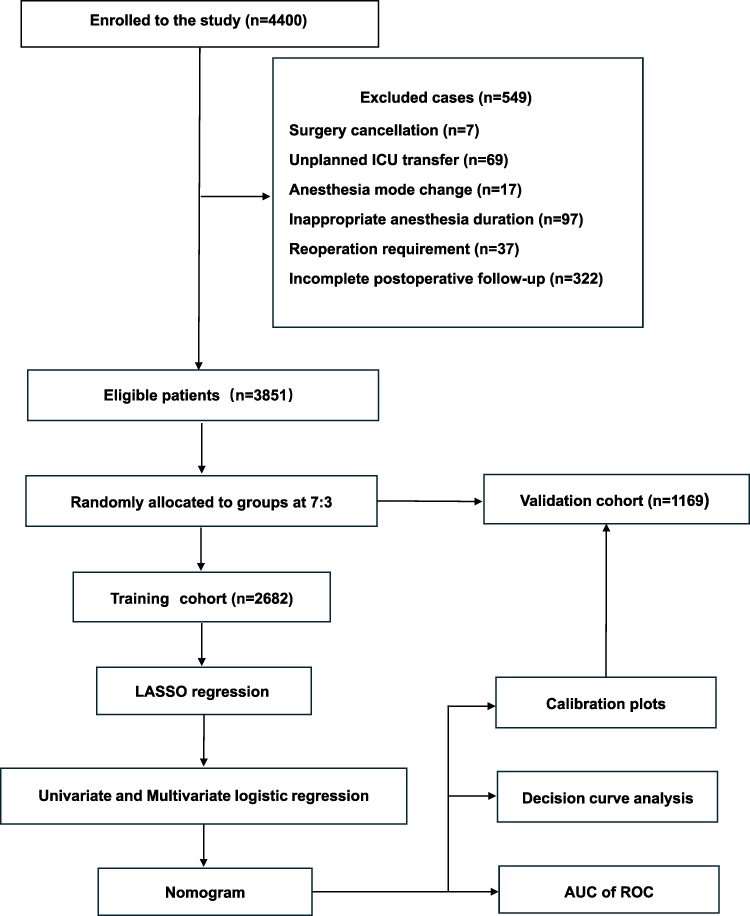 |
Figure 1 Flow chart of the study. Abbreviations: ICU, intensive care unit; AUC, area under the curve; ROC, receiver operating characteristic curve; LASSO, Least Absolute Shrinkage and Selection Operator. |
Baseline Clinical Characteristics
Among the 3851 enrolled patients, the median age was 56 years (IQR 46–66), with gender distribution showing 2447 (63.5%) females and 1404 (36.5%) males. These subjects were allocated to a training cohort (n=2682) and a validation cohort (n=1169). About 37.7% of patients reported PSD within the first week, persisting in 12.1% at 1 month after surgery.
In the training cohort, 992 patients (37.0%) were diagnosed with PSD based on PSQI questionnaire, compared to 459 patients (39.3%) in the validation cohort. Table 1 summarizes the baseline characteristics. Baseline characteristics were well balanced between the training and validation cohorts, with no statistically significant differences observed (all p>0.05), except for procedure type distribution (p=0.040).
 |
Table 1 Participant Characteristics of the Training Cohort and the Validation Cohort |
Screening for Predictive Factors
LASSO regression selected sixteen predictors with non-zero coefficients from the initial thirty candidate variables (Table 2 and Figure 2). Univariate logistic regression analysis of these predictors initially identified twelve perioperative factors showing significant associations with PSD. Ten predictors remained independently associated with PSD in the multivariate analysis, per the following results: Male (p<0.001, odds ratio [OR] 0.53, 95% confidence interval [CI] 0.43–0.66), ASA III (p=0.021, OR 1.37, 95% CI 1.05–1.80), Moderate-to-severe anemia (p<0.001, OR 2.00, 95% CI 1.36–2.92), Satisfaction of ward environment (p<0.001, OR 0.55, 95% CI 0.44–0.69), Anxiety (p<0.001, OR 1.75, 95% CI 1.34–2.28), Dexmedetomidine (p<0.001, OR 0.43, 95% CI 0.35–0.53), Age (p<0.001, OR 1.02, 95% CI 1.01–1.03), Anesthesia time (p<0.001, OR 1.00, 95% CI 1.00–1.01), Sufentanil (p<0.001, OR 0.93, 95% CI 0.90–0.95) and NRS score (p<0.001, OR 1.65, 95% CI 1.54–1.77) (Figure 3).
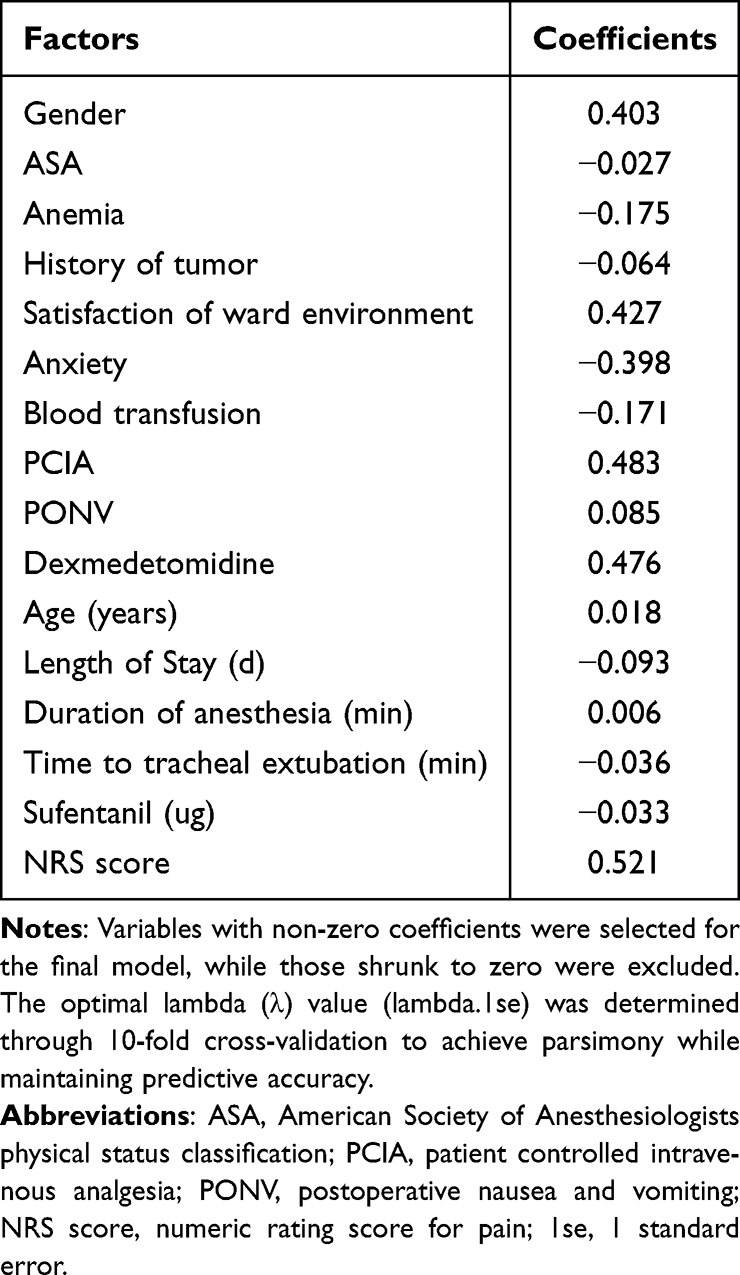 |
Table 2 Coefficients and Lambda. 1se Value of the LASSO Regression |
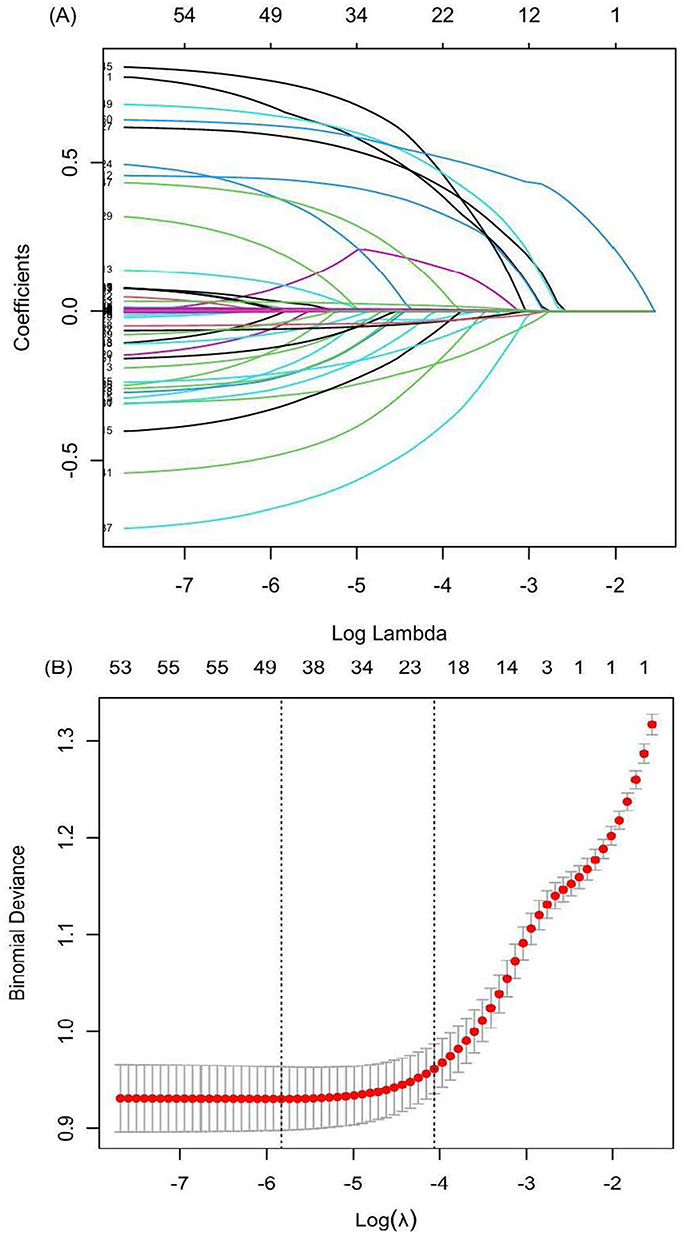 |
Figure 2 Selection of demographic and clinical features using the Least Absolute Shrinkage and Selection Operator (LASSO) regression. (A) Lasso coefficient profile plot. (B) The result of 10-fold Cross-Validation. Dotted vertical lines on the left: the minimum values; Dotted vertical lines on the right: the optimal values. |
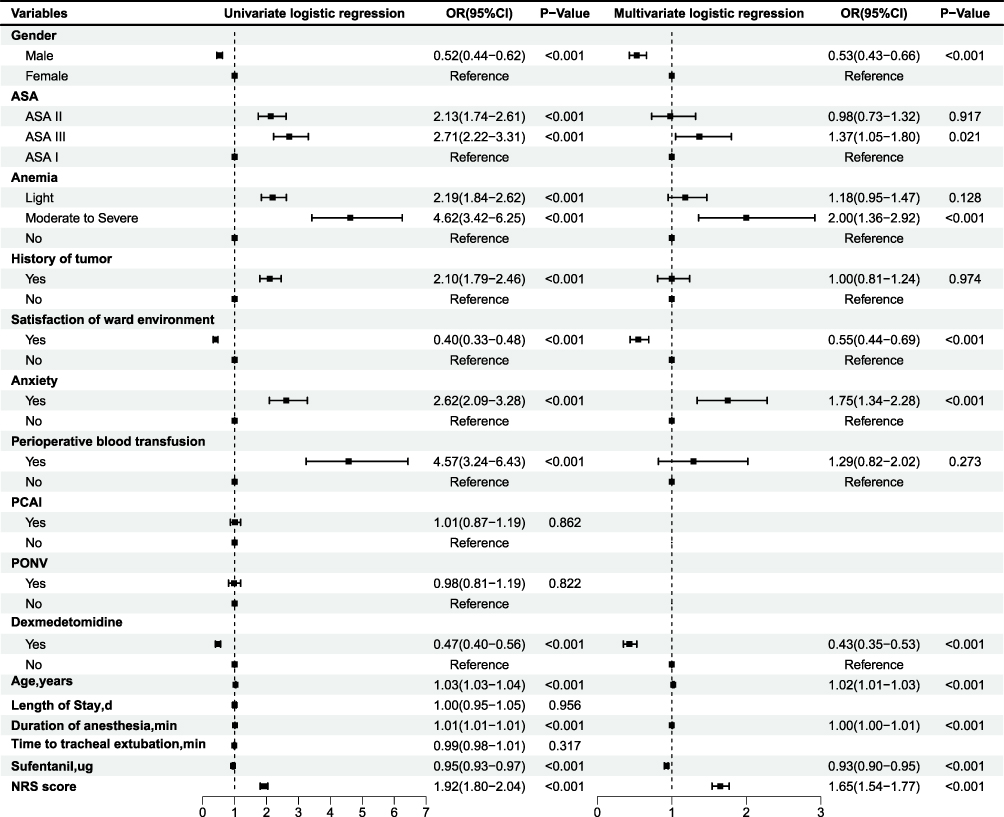 |
Figure 3 Forest plot displaying univariate and multivariate logistic regression results of the 16 variables selected by LASSO regression. Abbreviations: OR, odds ratio; CI, confidence interval; ASA, American Society of Anesthesiologists physical status classification; PCAI, Patient-controlled intravenous analgesia; PONV, Postoperative nausea and vomiting; NRS score, numeric rating score for pain. |
Construction of the Nomogram
These identified predictors were incorporated into a predictive model for PSD (Figure 4). Within the nomogram, each predictor was weighted according to its association with PSD risk factors. These weighted components were integrated into a composite risk score to quantify PSD probability.
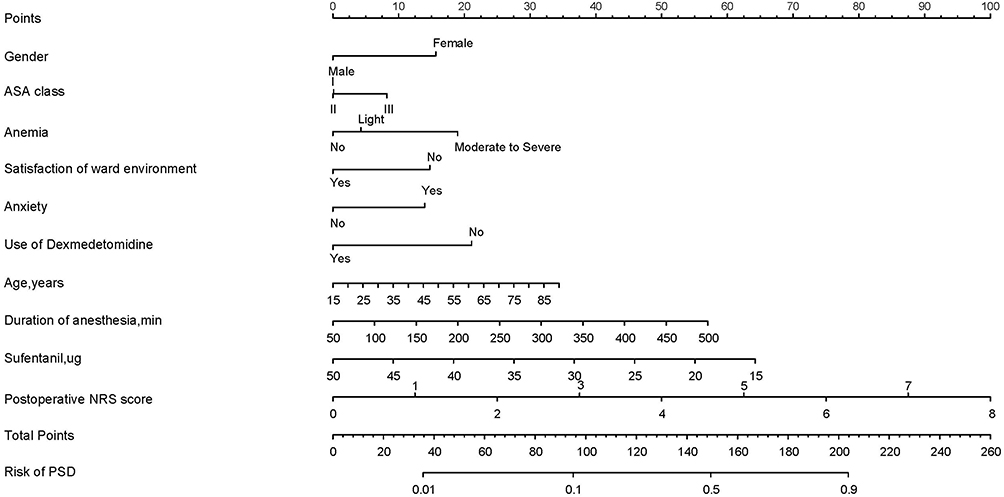 |
Figure 4 Nomogram to predict the probability of PSD in non-cardiac surgery. Place a vertical line at the level of each variable. Add up the points for all variables and place a vertical line downwards at the corresponding total to obtain the predicted probability of PSD. Example Calculation: For a 58-year-old female patient with: Gender: Female (→ 15 points); ASA class: II (→ 0 points); Anemia: No (→ 0 points); Satisfaction of ward environment: Yes (→ 0 points); Anxiety: Yes (→ 15 points); Use of Dexmedetomidine: No (→ 20 points);Age: 58 years (→ 20 points); Duration of anesthesia: 100 min (→ 5 points); Sufentanil: 30 ug (→ 36 points); NRS pain score: 3 (→ 38 points) 1. Locate each parameter on corresponding axes 2. Sum all points: 149 points 3. Align 149 points on “Total Points” axis → 50% PSD risk. |
The nomogram demonstrated significant predictive accuracy in the study, with AUC values of 0.826 (95% CI: 0.810–0.843) in the training cohort (Figure 5A) and 0.822 (95% CI: 0.797–0.847) in the validation cohort (Figure 5B).
 |
Figure 5 ROC curves of the nomogram for predicting the probability of PSD. (A) the training cohort; (B) the validation cohort. The area under the curve (AUC) of training cohort and validation cohort were 0.826 and 0.822, respectively. |
Calibration plots assess nomogram prediction accuracy against actual results. In the study, the calibration plots for both training (Figure 6A) and validation (Figure 6B) cohorts showed strong agreement between the nomogram’s predicted probabilities and actual observed outcomes of PSD.
 |
Figure 6 Calibration plots of the nomogram. (A) Training cohort; (B) Validation cohort. |
DCA evaluated the nomogram’s clinical utility across probability thresholds. Compared to the treat-all and treat-none approaches, our model showed significantly better net benefits in both training and validation cohorts (Figure 7).
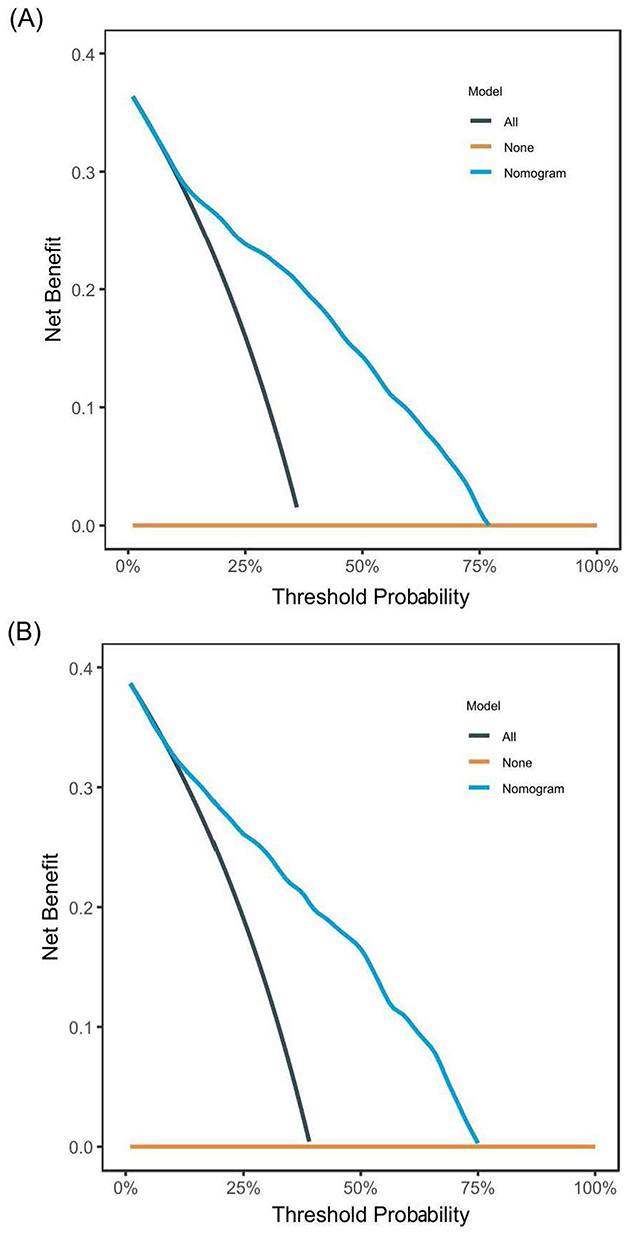 |
Figure 7 Decision curve analysis of the nomogram. (A) Training cohort. (B) Validation cohort. The dark green line (All-line) represents the assumption that intervention is performed on all patients. The Orange line (None-line) represents the assumption that intervention is performed on no patients. The blue line represents the nomogram. |
We subsequently created an interactive online nomogram (available at: https://flower123.shinyapps.io/DynNomapp2/) incorporating the ten identified predictors using the ShinyApps platform. The incidence of PSD [0.655 95% CI: (0.587–0.718)] in a virtual patient can be calculated by entering relevant clinical information on this online nomogram (Supplementary Figure S1).
Discussion
Sleep serves as an essential biological imperative in humans. Adequate sleep duration and quality provide significant physiological benefits, including enhanced immune competence, improved neurocognitive development and memory consolidation, as well as better metabolic regulation.22
The PSQI was selected in this study for its comprehensive seven distinct dimensions (including sleep latency, efficiency, and daytime dysfunction), which better captures the nature of postoperative sleep disturbances. Although designed with a 1-month recall period, the PSQI has demonstrated validity for shorter-term assessment (3, 7, and 28 days).23 Thus, the PSQI was used to evaluate postoperative sleep quality at 1-week and 1-month follow-ups.
The observed prevalence of PSD in our study was moderate (37.7%), potentially attributable to the duration of postoperative follow-up. In our study, we specifically documented patients with persistent sleep disturbances at 1 week postoperatively. Notably, a substantial proportion of patients who developed early postoperative sleep dysfunction (days1-3) demonstrated progressive improvement over time. Consequently, while 37.7% of patients still exhibited sleep-related problems at 1 week postoperatively, the prevalence declined markedly to 12.1% by the 1-month follow-up. Continued sleep deprivation can cause negative emotions, hemodynamic instability, chronic pain, impaired respiratory function, postoperative delirium and early postoperative fatigue, all of which may detrimentally affect postoperative outcome.24–26
Previous studies have established that female sex, anxiety, pain, and environmental dissatisfaction are significant contributors to sleep disruption,27–30 this study further confirms their additional role in predicting PSD among non-cardiac surgery patients. Female patients exhibit increased vulnerability to PSD due to interrelated psychosocial and biological factors. Psychosocial contributors include heightened concern for familial and social relationships, which may predispose to anxiety and depressive symptoms. Concurrently, biological factors such as hormonal fluctuations directly influence sleep-wake regulation mechanisms.31,32 Multiple studies have consistently identified anxiety as a significant predictor of sleep disorder prevalence across diverse populations.33 Clinical evidence indicates patient anxiety primarily originates from biopsychosocial factors, particularly disease-related hypervigilance and treatment-associated financial strain within family. Advanced neuroimaging modalities have delineated overlapping neural substrates underlying the comorbidity of sleep and anxiety disorders, characterized by maladaptive crosstalk among dopaminergic (D2), serotonergic (5-HT1A), and adenosinergic (A2A) receptor systems that collectively perpetuate a pathophysiological cycle of sleep fragmentation and hyperarousal.34,35 Pain is recognized as the fifth vital sign. Postoperative pain typically peaks within 24–72 hours after surgery and persists for 4–6 days, potentially disrupting sleep through multiple pathways: surgical trauma-induced nociceptive stimuli directly impair sleep continuity; inflammatory mediators trigger peripheral sensitization and central transmission via neural, humoral and cellular routes across the blood–brain barrier, dysregulating key neurotransmitter systems (particularly norepinephrine and dopamine) and altering sleep architecture.36,37 Furthermore, pain-related sympathetic hyperactivity and metabolic changes may additionally contribute to postoperative sleep impairment.16
This study revealed increasing age was also one of the risk factors for PSD. Sleep duration exhibits a progressive decline with advancing age in humans. Age-related sleep alterations include progressively shortened duration, reduced arousal thresholds, increased nocturnal awakenings with prolonged wake-after-sleep onset, and daytime sleepiness. Notably, elderly patients showed significantly decreased urinary 6-sulfatoxy melatonin levels versus younger, suggesting impaired melatonin-mediated circadian regulation contributes to PSD. Therefore, elderly women constitute a high-risk population for PSD.
Anesthetic agents have a significant impact on patients’ postoperative sleep architecture. Dexmedetomidine, a highly selective α2-adrenergic receptor agonist, demonstrates potent sedative, analgesic, and anxiolytic effects. Furthermore, this agent enhances sleep quality by reducing fragmentation, shifting N1 to N2 stage, and restoring circadian rhythm, thereby promoting physiological sleep.38,39 Thus, dexmedetomidin reduces the incidence of PSD and improves postoperative sleep quality.40 It can be effectively administered via intravenous infusion, nasal drip or nasal spray, with varying concentrations available.41,42 In our study, intraoperative infusion of dexmedetomidine (0.2 µg·kg−¹·h−¹) was identified as a protective factor against PSD. The finding confirms that low-dose (compared to higher-dose) intravenous dexmedetomidine effectively improves postoperative sleep quality in patients, consistent with previous reports.43,44 In the study, the utilization rate of total intravenous anesthesia (TIVA) was 33.0%. Although volatile anesthetics (especially sevoflurane and isoflurane) have been shown to disrupt sleep and increase fragmentation,45,46 this study found TIVA was not significantly better than balanced inhalation anesthesia for maintaining postoperative sleep quality. This may be attributed to the transient disruption of sleep architecture and circadian rhythms by inhalation anesthetics, which typically resolves within 24–72 hours postoperatively.47 The long-term effects of inhaled anesthetics on sleep require further investigation.
Therefore, we recommend a comprehensive intervention strategy for high-risk populations, particularly patients with anxiety and elderly women. This approach encompasses: routine preoperative psychological screening followed by psychosocial or pharmacological intervention when clinically warranted; intraoperative administration of dexmedetomidine; strict implementation of perioperative multimodal analgesia protocols; and judicious melatonin supplementation for elderly patients with objectively confirmed circadian rhythm disturbances. Collectively, these measures aim to significantly mitigate the risk of PSD.
Currently, a limited number of studies have focused on developing PSD predictive models for general anesthesia patients. Du et al established an 8-predictor model exclusively for spinal surgery patients,20 whereas Yang et al constructed a 9-variable nomogram model based on 881 non-cardiac surgery patients, demonstrating AUC values of 0.82 and 0.80 in the training and validation cohorts, respectively.19 All the studies employed LASSO regression for variable selection followed by logistic regression. Our predictive model incorporated ten clinically accessible perioperative variables, including female sex, anxiety status, ward environment dissatisfaction, lower intraoperative sufentanil dosage, non-use of dexmedetomidine, and higher NRS pain scores, aligning with those two previous studies. Distinctively, this study incorporated perioperative anemia and ASA physical status classification into the final nomogram. The ASA classification system assesses a patient’s preoperative physical status. Multiple studies have demonstrated that patients with higher ASA classification grades exhibit significantly increased perioperative mortality rates.48,49 Patients with ASA class III typically present with severe chronic comorbidities, particularly cardiovascular and respiratory diseases. These conditions contribute to both sleep architecture disruption with fragmentation and sustained systemic inflammatory activation. Through blood–brain barrier penetration, proinflammatory mediators may further impair circadian rhythm regulation by modulating hypothalamic suprachiasmatic nucleus (SCN) activity.
Furthermore, these patients typically demonstrate prolonged postoperative recovery periods and frequently require multidisciplinary care coordination. Consequently, patients with ASA class III status exhibit significantly higher incidence rates of PSD compared to ASA class I–II counterparts.
Perioperative anemia is a common clinical concern, with an Incidence of 35.9% in our study cohort. Multiple large-scale retrospective cohort studies have established anemia as a significant predictor of 30-day postoperative mortality.50,51 Furthermore, anaemia is strongly associated with the development of sleep disorders in adults.52,53 Neuroimaging evidence demonstrates that reduced cerebral blood flow in the frontotemporal region correlates with lower hemoglobin levels, while cortical thinning in this area is linked to shorter sleep duration.54,55 Furthermore, chronic anemia may contribute to psychological distress, including anxiety, which can exacerbate sleep disturbances.
While prior studies have established a significant association between poor sleep quality and OSAHS,56 our study did not confirm this association. Only 3% of our cohort had comorbid OSAHS. This low prevalence may result from preoperative diagnostic limitations, which consequently excluded it from consideration as a PSD risk factor. Future investigations employing standardized OSAHS diagnostic criteria are needed to definitively establish its association with PSD.
Nomograms serve as user-friendly visual prediction tools. Our study developed a nomogram based on 3851 patients (notably larger than previous studies), achieving the C-index values of 0.826 in the training cohort and 0.822 in the validation cohort, indicating robust discriminative performance. All incorporated variables are both clinically routine and readily obtainable in practice. Nevertheless, the current study has certain limitations. First, as a single-center study developing this prediction model exclusively in patients without pre-existing sleep disorders, our findings may have limited generalizability. The model’s performance may differ in patients with pre-existing sleep disturbances, those undergoing alternative anesthesia techniques (eg, regional anesthesia), or in different clinical settings. Second, the study focused on early PSD prediction (1-week postoperatively). While this provides timely clinical guidance, the short follow-up precludes assessment of persistent sleep disturbances. Future studies should extend the follow-up to 6–12 months to identify chronic predictors and develop corresponding long-term prediction models. Third, although the PSQI is a validated assessment tool, its reliance on subjective self-reporting may compromise measurement accuracy, particularly among older adults and individuals with limited education. Future investigations should incorporate objective measures such as polysomnography to complement self-reported data.
Conclusion
This study developed and validated a clinically applicable nomogram for predicting early PSD within 7 days after non-cardiovascular surgery. By integrating 10 perioperative predictors using rigorous prospective data from 3851 patients, the model demonstrates high predictive accuracy and optimal calibration, offering clinicians a comprehensive risk assessment tool. For those identified as high-risk, targeted interventions – including preoperative psychological support, environmental modifications, anemia correction, and judicious intraoperative anesthetic management may effectively reduce PSD incidence and improve recovery outcomes. The nomogram requires multicenter validation with objective polysomnographic measures to confirm its generalizability beyond the current single-center study design.
Data Sharing Statement
All data supporting the findings of this study are available upon reasonable request from the corresponding author. The authors are willing to provide relevant data when appropriate while adhering to ethical and privacy protection requirements.
Author Contributions
Jia-Li Mao (First Author): Conceptualization, Data curation, Formal analysis, Investigation, Software, Methodology, Writing-original draft, Writing – review & editing
Shu-Hua Shu (Corresponding Author): Conceptualization, Methodology, Project administration, Resources, Supervision, Writing – review & editing
Ling Hu: Methodology, Data curation, Investigation, Writing – review & editing
Xue-Feng Wang: Conceptualization, Investigation, Data curation, Writing – review & editing
Sheng Wang: Conceptualization, Project administration, Writing – review & editing
Xiao-Qing Fan: Investigation, Data curation, Writing – review & editing
All authors approved the version submitted for publication; agreed to the journal this paper was submitted and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
All authors have no competing interests to disclose.
References
1. Butris N, Tang E, Pivetta B, et al. The prevalence and risk factors of sleep disturbances in surgical patients: A systematic review and meta-analysis. Sleep Med Rev. 2023;69:101786. doi:10.1016/j.smrv.2023.101786
2. Halle I, Westgaard T, Wahba A, Oksholm T, Rustøen T, Gjeilo K. Trajectory of sleep disturbances in patients undergoing lung cancer surgery: a prospective study. Interact Cardiovasc Thorac Surg. 2017;25:285–291. doi:10.1093/icvts/ivx076
3. Ida M, Onodera H, Yamauchi M, Kawaguchi M. Preoperative sleep disruption and postoperative functional disability in lung surgerypatients: a prospective observational study. J Anesth. 2019;33:501–508. doi:10.1007/s00540-019-02656-y
4. Canfieldm J, Creminsm S, Vellanky S, et al. Evaluating the success of perioperative self-guided meditation in reducing sleep disturbance after total knee arthroplasty. J Arthroplasty. 2021;36:215–220. doi:10.1016/j.arth.2021.01.070
5. Altman MT, Knauert MP, Pisani MA. Sleep disturbance after hospitalization and critical illness: a systematic review. Ann Am Thorac Soc. 2017;14:1457–1468. doi:10.1513/AnnalsATS.201702-148SR
6. O’Gara B, Gao L, Marcantonio E, Subramaniam B. Sleep, pain, and cognition: modifiable targets for optimal perioperative brain health. Anesthesiology. 2021;135:1132–1152. doi:10.1097/ALN.0000000000004046
7. Nishtala M, Robbins S, Savage S, et al. Patients follow different financial hardship trajectories in the year after injury. Ann Surg. 2022;276:959–966. doi:10.1097/SLA.0000000000005432
8. Zheng JW, Wang LL, Wang W, et al. Association and prediction of subjective sleep quality and postoperative delirium during major non-cardiac surgery: a prospective observational study. BMC Anesthesiol. 2023;23:306–312. doi:10.1186/s12871-023-02267-x
9. Rampes S, Ma K, Divecha YA, Alam A, Ma D. Postoperative sleep disorders and their potential impacts on surgical outcomes. J Biomed Res. 2020;34:271–280. doi:10.7555/JBR.33.20190054
10. Hillman DR. Sleep loss in the hospitalized patient and its influence on recovery from illness and operation. Anesth Analg. 2021;132:1314–1320. doi:10.1213/ANE.0000000000005323
11. Varallo G, Giusti EM, Manna C, et al. Sleep disturbances and sleep disorders as risk factors for chronic postsurgical pain: a systematic review and meta-analysis. Sleep Med Rev. 2022;63:101630. doi:10.1016/j.smrv.2022.101630
12. Wesselius HM, Van DEES, Jelmer A, et al. Quality and quantity of sleep and factors associated with sleep disturbance in hospitalized patients. JAMA Intern Med. 2018;178:1201–1208. doi:10.1001/jamainternmed.2018.2669
13. Haack M, Simpson N, Sethna N, Kaur S, Mullington J. Sleep deficiency and chronic pain: potential underlying mechanisms and clinical implications. Neuropsychopharmacology. 2020;45:205–216. doi:10.1038/s41386-019-0439-z
14. Luo Z, Li L, Wang D, Wang H, Pei F, Zhou Z. Preoperative sleep quality affects postoperative pain and function after total joint arthroplasty: a prospective cohort study. J Orthop Surg Res. 2019;14:378. doi:10.1186/s13018-019-1446-9
15. Huang X, Lin D, Sun Y, Wu A, Wei C. Effect of dexmedetomidine on postoperative sleep quality: a systematic review. Drug Des Devel Ther. 2021;15:2161–2170. doi:10.2147/DDDT.S304162
16. Luo M, Song B, Zhu J. Sleep disturbances after general anesthesia: current perspectives. Front Neurol. 2020;7:629. doi:10.3389/fneur.2020.00629
17. Qiu D, Wang XM, Yang JJ, et al. Effect of intraoperative esketamine infusion on postoperative sleep disturbance after gynecological laparoscopy: a randomized clinical trial. JAMA Netw Open. 2022;5:e2244514. doi:10.1001/jamanetworkopen.2022.44514
18. Renner C, Jeitziner MM, Albert M, et al. Guideline on multimodal rehabilitation for patients with post-intensive care syndrome. Crit Care. 2023;27:301. doi:10.1186/s13054-023-04569-5
19. Yang ST, Zhang Q, Xu YF, et al. Development and validation of nomogram prediction model for postoperative sleep disturbance in patients undergoing non-cardiac surgery: a prospective cohort study. Nat Sci Sleep. 2021;13:1473–1483. doi:10.2147/NSS.S319339
20. Du J, Zhang HG, Ding Z, et al. Development and validation of a nomogram for postoperative sleep disturbance in adults: a prospective survey of 640 patients undergoing spinal surgery. BMC Anesthesiol. 2023;23:154–166. doi:10.1186/s12871-023-02097-x
21. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213. doi:10.1016/0165-1781(89)90047-4
22. Mukherjee S, Patel SR, Kales SN et al. An official American thoracic society statement: the importance of healthy sleep. Recommendations and future priorities. Am J Respir Crit Care Med. 2015;191:1450–1458. doi:10.1164/rccm.201504-0767ST
23. Broderick JE, Junghaenel DU, Schneider S, et al. Pittsburgh and Epworth sleep scale items: accuracy of ratings across different reporting periods. Behav Sleep Med. 2013;11(3):173–188. doi:10.1080/15402002.2012.654549
24. Sun Y, Laksono I, Selvanathan J, et al. Prevalence of sleep disturbances in patients with chronic non-cancer pain: a systematic review and meta-analysis. Sleep Med Rev. 2021;6:101467. doi:10.1016/j.smrv.2021.101467
25. Lu Y, Li YW, Wang L, et al. Promoting sleep and circadian Health may prevent postoperative delirium: a systematic review and meta-analysis of randomized clinical trials. Sleep Med Rev. 2019;48:101207. doi:10.1016/j.smrv.2019.08.001
26. Rault C, Sangare A, Diaz V, et al. Impact of sleep deprivation on respiratory motor output and endurance. A physiological study. Am J Respir Crit Care Med. 2020;201:976–983. doi:10.1164/rccm.201904-0819OC
27. Wang Y, Liu Y, Li X, et al. Prospective assessment and risk factors of sleep disturbances in total hip and knee arthroplasty based on an enhanced recovery after surgery concept. Sleep Breath. 2021;25:1231–1237. doi:10.1007/s11325-020-02213-y
28. Zhang Y, Guo X, Guo J, et al. Sleep quality in acromegaly and changes after transsphenoidal surgery: a prospective longitudinal study. Sleep Med. 2020;67:164–170. doi:10.1016/j.sleep.2019.11.1256
29. Oh CM, Kim HY, Na HK, Cho KH, Chu MK. The effect of anxiety and depression on sleep quality of individuals with high risk for insomnia: a population-based study. Front Neurol. 2019;10:849. doi:10.3389/fneur.2019.00849
30. Reid E. Factors affecting how patients sleep in the hospital enviroment. Br J Nurs. 2001;10:912–915. doi:10.12968/bjon.2001.10.14.5278
31. Sivertsen B, Krokstad S, Øverland S, Mykletun A. The epidemiology of insomnia: associations with physical and mental health. The HUNT-2 study. J Psychosom Res. 2009;67:109–116. doi:10.1016/j.jpsychores.2009.05.001
32. Jaussent I, Dauvilliers Y, Ancelin ML, et al. Insomnia symptoms in older adults: associated factors and gender differences. Am J Geriatr Psychiatry. 2011;19:88–97. doi:10.1097/JGP.0b013e3181e049b6
33. Lee SH, Lee H, Kim YS, Kim KU, Park HK, Lee MK. Factors associated with sleep disturbance in patients with chronic obstructive pulmonary disease. Clin Respir J. 2020;14:1018–1024. doi:10.1111/crj.13235
34. Chellappa SL, Aeschbach D. Sleep and anxiety: from mechanisms to interventions. Sleep Med Rev. 2022;61:101583. doi:10.1016/j.smrv.2021.101583
35. Lofthouse N, Gilchrist R, Splaingard M. Mood-related sleep problems in children and adolescents. Child Adolesc Psychiatr Clin N Am. 2009;18:893–916. doi:10.1016/j.chc.2009.04.007
36. Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. 2006;367:1618–1625. doi:10.1016/S0140-6736(06)68700-X
37. Irwin MR. Sleep and inflammation: partners in sickness and in health. Nat Rev Immunol. 2019;19:702–715. doi:10.1038/s41577-019-0190-z
38. Oxlund J, Toft P, Sorberg M, Knudsen T, Jennum PJ. Dexmedetomidine and sleep quality in mechanically ventilated critically ill patients: study protocol for a randomised placebo-controlled trial. BMJ Open. 2022;12:e50282. doi:10.1136/bmjopen-2021-050282
39. Chamadia S, Hobbs L, Marota S, et al. Oral dexmedetomidine promotes non-rapid eye movement stage 2 sleep in humans. Anesthesiology. 2020;133:1234–1243. doi:10.1097/ALN.0000000000003567
40. Motaghi E, Pirbalooti MG, Bozorgi H, Eslami M, Rashidi M. Safety and efficacy of dexmedetomidine in breast surgeries: a systematic review and meta-analysis. J Perianesth Nurs. 2021;36:179–186. doi:10.1016/j.jopan.2020.09.011
41. Weber F, Dan Y. Circuit-based interrogation of sleep control. Nature. 2016;538:51–59. doi:10.1038/nature19773
42. Wu J, Liu X, Ye C, et al. Intranasal dexmedetomidine improves postoperative sleep quality in older patients with chronic insomnia: a randomized double-blind controlled trial. Front Pharmacol. 2023;14:1223746. doi:10.3389/fphar.2023.1223746
43. Cai J, Chen Y, Hao X, et al. Effect of intraoperative dexmedetomidine dose on postoperative first night sleep quality in elderly surgery patients: a retrospective study with propensity score-matched analysis. Front Med. 2020;7:528. doi:10.3389/fmed.2020.00528
44. Duan G, Wang K, Peng T, Wu Z, Li H. The effects of intraoperative dexmedetomidine use and its different dose on postoperative sleep disturbance in patients who have undergone non-cardiac major surgery: a real-world cohort study. Nat Sci Sleep. 2020;12:209–219. doi:10.2147/NSS.S239706
45. Mori K, Komatsu T, Fujiwara Y, Fujita Y. Comparison of the effects of desflurane and sevoflurane on variations in salivary melatonin and sleep disturbance after total knee arthroplasty: a single center, prospective, randomized, controlled, open-label study. J Perianesth Nurs. 2024;39:101–108. doi:10.1016/j.jopan.2023.07.007
46. Li S, Song B, Li Y, Zhu J. Effects of intravenous anesthetics vs inhaled anesthetics on early postoperative sleep quality and complications of patients after laparoscopic surgery under general anesthesia. Nat Sci Sleep. 2021;13:375–382. doi:10.2147/NSS.S300803
47. Wren-Dail MA, Dauchy RT, Blask DE, et al. Effect of isoflurane anesthesia on circadian metabolism and physiology in rats. Comp Med. 2017;67:138–146.
48. Bruin LD, Pasma W, Van der Werff DB, et al. Perioperative hospital mortality at a tertiary paediatric institution. Br J Anaesth. 2015;115:608–615. doi:10.1093/bja/aev286
49. Hilden M, Wretenberg P, Ekstrom W. Good overall morbidity prediction with the POSSUM scoring system in patients having a total Hip or knee replacement—a prospective study in 227 patients. Clin Interv Aging. 2018;13:1747–1754. doi:10.2147/CIA.S165698
50. Musallam KM, Tamim HM, Richards T, et al. Preoperative anaemia and postoperative outcomes in non-cardiac surgery: a retrospective cohort study. Lancet. 2011;378:1396–1407. doi:10.1016/S0140-6736(11)61381-0
51. Saager L, Turan A, Reynolds LF, Dalton JE, Kurz A, Kurz A. The association between preoperative anemia and 30-day mortality and morbidity in noncardiac surgical patients. Anesth Analg. 2013;117:909–915. doi:10.1213/ANE.0b013e31828b347d
52. Chen-Edinboro LP, Murray-Kolb LE, Simonsick EM, et al. Association between non-iron-deficient anemia and insomnia symptoms in community-dwelling older adults: the Baltimore Longitudinal Study of Aging. J Gerontol a Biol Sci Med Sci. 2018;73:380–385. doi:10.1093/gerona/glw332
53. Jackowska M, Kumari M, Steptoe A. Sleep and biomarkers in The english longitudinal study of ageing: associations with C-reactive protein, fibrinogen, dehydroepiandrosterone sulfate and hemoglobin. Psychoneuroendocrinology. 2013;38:1484–1493. doi:10.1016/j.psyneuen.2012.12.015
54. Gottesman RF, Sojkova J, Beason-Held LL, et al. Patterns of regional cerebral blood flow associated with low hemoglobin in the Baltimore longitudinal study of aging. J Gerontol A Biol Sci Med Sci. 2012;67:963–969. doi:10.1093/gerona/gls121
55. Spira AP, Gonzalez CE, Venkatraman VK, et al. Sleep duration and subsequent cortical thinning in cognitively normal older adults. Sleep. 2016;39:1121–1128. doi:10.5665/sleep.5768
56. Chung F, Liao P, Yang Y, et al. Postoperative sleep-disordered breathing in patients without preoperative sleep apnea. Anesth Analg. 2015;120:1214–1224. doi:10.1213/ANE.0000000000000774
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.