Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Development and Psychometric Evaluation of a Pulmonary Rehabilitation Information Needs Scale for Patients with Chronic Obstructive Pulmonary Disease
Authors Tang Y, Zhao X, Huang Z, Kaminga AC, Li Z, Xiong Y ![]() , Liu Z, Huang Y, Yang G, Yi Q
, Liu Z, Huang Y, Yang G, Yi Q
Received 26 March 2026
Accepted for publication 4 June 2026
Published 15 June 2026 Volume 2026:21 612119
DOI https://doi.org/10.2147/COPD.S612119
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Zijing Zhou
Yurong Tang,1,* Xun Zhao,2,* Zhuoer Huang,1 Atipatsa Chiwanda Kaminga,3 Zhuoheng Li,1 Yang Xiong,1 Ziyu Liu,1 Yuanxin Huang,1 Guoli Yang,4 Qifeng Yi5
1Xiangya School of Nursing, Central South University, Changsha, People’s Republic of China; 2Department of Emergency Medicine, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 3Mzuzu University, Department of Mathematics and Statistics, Mzuzu, Malawi; 4Department of Pulmonary and Critical Care Medicine, Third Xiangya Hospital, Central South University, Changsha, People’s Republic of China; 5Department of Nursing, the Third Xiangya Hospital, Central South University, Changsha, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qifeng Yi, Department of Nursing, The Third Xiangya Hospital, Central South University, 138 Tongzipo Road, Changsha, Hunan, People’s Republic of China, Tel +86-0731-88618681, Fax: +86-410013, Email [email protected] Guoli Yang, Department of Pulmonary and Critical Care Medicine, Third Xiangya Hospital, Central South University, 138 Tongzipo Road, Changsha, Hunan, People’s Republic of China, Email [email protected]
Purpose: This study aimed to develop and validate a pulmonary rehabilitation information needs scale for patients with chronic obstructive pulmonary disease (COPD) using both classical test theory (CTT) and item response theory (IRT).
Methods: Guided by Alderfer’s ERG theory and Kochen’s information needs theory, the initial item pool was developed through a literature review and semi-structured interviews with 12 COPD patients undergoing pulmonary rehabilitation. Using the Delphi method, 35 experts were consulted to refine the questionnaire into its first draft. A pilot test with 20 COPD patients was then conducted to revise item wording. Data were collected from a convenience sample of 300 COPD patients from February to December 2024 at five hospitals in Changsha, China. Participants had a mean age of 71.01± 9.38 years, and 85.3% were male. Validity and reliability were evaluated using exploratory factor analysis (EFA), confirmatory factor analysis (CFA), internal consistency, and item analysis based on CTT and IRT.
Results: The final questionnaire contains a total of 6 dimensions and 39 items. EFA identified six factors, with all items having factor loadings greater than 0.40 within their respective factors. CFA supported the proposed six-factor structure, with all standardized factor loadings at acceptable levels and the model demonstrating an acceptable fit to the data (χ2/df = 1.804, CFI = 0.984, TLI = 0.983, RMSEA = 0.052, SRMR = 0.065). The content validity index (S-CVI) was 0.935 and the Cronbach’s α coefficient of the scale was 0.936. IRT analysis showed that all items had good discrimination parameters (a > 1.0) and threshold parameters within an appropriate range (b = − 4 to 4).
Conclusion: To our knowledge, the scale is the first tool designed to assess pulmonary rehabilitation-specific information needs in COPD. It demonstrated acceptable validity and reliability for assessing the information needs of patients with COPD who are preparing to participate in or are undergoing pulmonary rehabilitation. The instrument may provide a useful and feasible instrument for supporting clinical assessment and the planning of individualized pulmonary rehabilitation education and support.
Keywords: chronic obstructive pulmonary disease, information needs, pulmonary rehabilitation, classical test theory, item response theory
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous lung condition characterized by chronic respiratory symptoms, persistent airway and/or alveolar abnormalities, and airflow limitation, with diverse etiological factors contributing to its development across the lifespan.1,2 It is a major global public health problem and the third leading cause of death worldwide. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) projects that the number of people living with COPD will approach 600 million by 2050, with associated direct and indirect costs expected to increase more than fivefold.3 Patients with COPD often experience dyspnea as well as limited activity, leading to impaired quality of life.4,5 Therefore, effective long-term management strategies are essential to improve symptoms, functioning, and health outcomes in patients with COPD.
The GOLD guideline strongly recommends pulmonary rehabilitation (PR) as a key component of COPD management.1 Patients with COPD can benefit from long-term PR programs, including enhanced exercise tolerance, reduced dyspnea, improved psychological well-being, and lower hospital readmission rates.6,7 PR is a comprehensive, individualized intervention with exercise training at its core, supported by education and self-management/behavior-change strategies.8 Thus, its implementation and effectiveness depend on patients’ understanding of the rehabilitation plan, as well as their sustained participation and adherence.9
However, evidence indicates that many patients with COPD have limited awareness of PR and insufficient understanding of how to manage their disease through physical activity, breathing exercises, sputum clearance, and emotional regulation.10 Effective participation in PR requires access to adequate, accurate, and understandable information on disease management and rehabilitation-related strategies, which may enhance patients’ disease understanding and support sustained participation.11 Moreover, patients’ information needs vary, and unmet information needs may hinder effective participation in pulmonary rehabilitation, thereby limiting rehabilitation adherence and outcomes.12
Despite the importance of identifying patients’ pulmonary rehabilitation information needs, standardized assessment of these needs is not routinely implemented in clinical practice.13 Existing instruments for patients with COPD, such as the Lung Information Needs Questionnaire (LINQ), mainly assess general educational or disease-related information needs and include some rehabilitation-related domains. Moreover, the LINQ was not specifically designed to assess the information needs of patients undergoing pulmonary rehabilitation, nor was it developed to evaluate patients’ information needs about the pulmonary rehabilitation process. Consequently, its ability to comprehensively assess such needs may be limited.14 Therefore, a validated instrument is needed to assess the pulmonary rehabilitation information needs of patients with COPD systematically and comprehensively.
Given the diverse, multidimensional, and context-specific nature of pulmonary rehabilitation information needs, a theory-guided framework is needed to define their dimensions and support scale development. In this study, Alderfer’s Existence, Relatedness, and Growth (ERG) theory and Kochen’ s information needs theory were used as complementary frameworks to conceptualize patients’ information needs and structure the scale. Accordingly, this study sought to develop and psychometrically evaluate a scale for assessing the pulmonary rehabilitation information needs of patients with COPD. To strengthen item-level evaluation beyond classical test theory, item response theory (IRT) was also applied. The availability of a reliable and valid assessment tool may support more targeted educational and supportive interventions and, ultimately, improve participation in pulmonary rehabilitation and related outcomes.
Materials and Methods
Study Design
This study aimed to develop a Pulmonary Rehabilitation Information Needs Scale for Patients with Chronic Obstructive Pulmonary Disease (PRIN-COPD), and assess its reliability and validity. This study included two phases: (1) scale development, and (2) psychometric evaluation through a cross-sectional survey. The overall study process is shown in Figure 1.
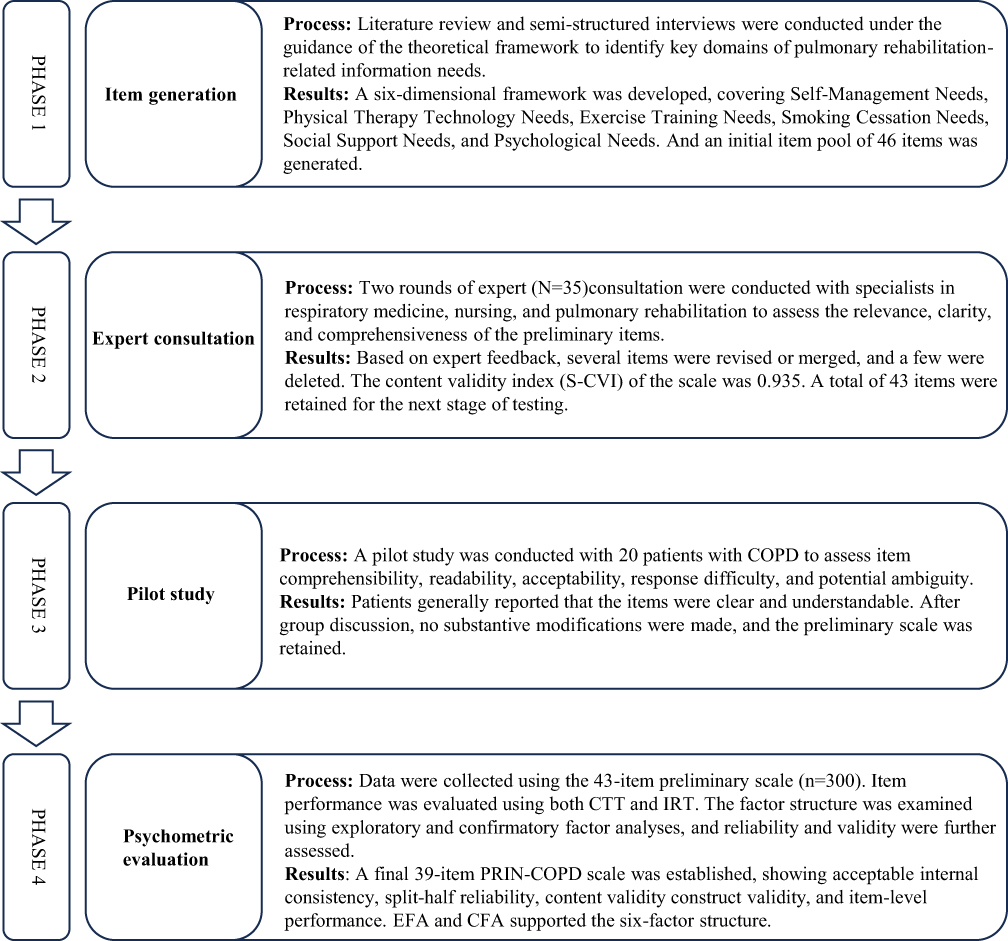 |
Figure 1 Process of development of the Pulmonary Rehabilitation Information Needs Scale for Patients with Chronic Obstructive Pulmonary Disease. |
Scale Development
Item Generation
Based on ERG theory (which refines Maslow’s hierarchy of needs into three core categories of human needs, namely existence (basic survival), relatedness (social connection), and growth (personal development)) and Kochen’s information needs theory (which distinguishes information needs at three levels, namely objective state, cognition, and expression),15,16 a literature review was conducted. Then, to explore patients’ pulmonary rehabilitation-related information needs based on their personal experiences, a semi-structured interview was undertaken. Patients with COPD were recruited using purposive sampling, with recruitment guided by data sufficiency and saturation. The interview participants’ characteristics are summarized in Supplementary Table S1, and the interview outline is provided in Supplementary Table S4. Finally, twelve patients were interviewed. Within 24 hours after the completion of the interviews, the audio recordings were organized and transcribed. The transcribed text was analyzed using NVivo 11.0 software, and thematic analysis was applied. Six themes were identified: Unclear understanding of pulmonary rehabilitation, Difficulties in respiratory management, Difficulties in smoking cessation, Social support needs, Exercise guidance and Emotional distress and coping. Meaning units related to information needs were converted into candidate items. Overlapping content was combined, and unclear or less relevant content was revised or removed after discussion by the research team. Figure 2 shows the mapping of interview themes to the theoretical framework and final scale dimensions. Supplementary Table S5 presents the link between the interview findings and the development of candidate items. An initial pool of 46 items was generated, and a preliminary scale was developed. This scale comprised six dimensions—Disease Self-Management Needs, Physical therapy technology Needs, Exercise Training Needs, Smoking Cessation Needs, Social Support Needs, and Psychological Needs.
 |
Figure 2 Mapping of Qualitative Interview Findings to the Scale Dimensions. |
The preliminary scale was then reviewed via Email by 35 experts from tertiary Grade A hospitals, all of whom had more than 10 years of clinical and research experience. The characteristics of the Delphi experts are presented in Supplementary Table S2. Two rounds of expert consultation were completed, with positive coefficients of 97.20% and 100.00%, respectively. The expert authority coefficients were 0.921 and 0.937. Kendall’s coefficients of concordance were 0.212 and 0.213 (both p < 0.01). Items were retained when both the mean importance score was ≥ 3.50 and the coefficient of variation (CV) was ≤ 0.25. Those not meeting these criteria, or assessed by experts as unclear, repetitive, or beyond the scope of pulmonary rehabilitation information needs, underwent revision or deletion following group discussion. New items were subsequently added following expert input and group deliberation. In Round 1, one dimension was revised; five items were modified, nine items were added, and five items were deleted. In Round 2, four items were revised and six items were deleted. Detailed results of the expert consultation are provided in Supplementary Table S6. The initial PRIN-COPD scale was formed based on Delphi expert consultation including 6 dimensions and 43 items, the language used in the scale development was Chinese.
Pilot Testing
The initial PRIN-COPD scale was pilot tested with 20 patients with COPD using convenience sampling method. The purpose of the pilot test was to assess item comprehensibility, readability, acceptability, response difficulty, and potential ambiguity of the items and response options. After completing the scale independently, patients were invited to provide feedback on unclear wording, repetitive content, difficult expressions, any items that were difficult to answer and the time required for completion. Overall, patients generally reported that the items were understandable and easy to answer. After discussion by the research team, no modifications were deemed necessary. Consequently, a 43-item, five-point Likert scale, for assessing the pulmonary rehabilitation information needs of COPD patients was developed. The characteristics of the patients who participated in the pilot test are provided in Supplementary Table S3.
Psychometric Evaluation
Participant and Setting
Patients with COPD were recruited using convenience sampling from five hospitals in Changsha. The inclusion criteria were as follows: (1) Patients diagnosed with COPD; (2) Age≥40 years; (3) Willing to receive, or currently receiving pulmonary rehabilitation; and (4) Having adequate cognitive and behavioral abilities to independently complete the questionnaires. The exclusion criteria were as follows: (1) Patients with severe visual, hearing and cognitive impairments; and (2) Patients with severe dyspnea or other serious illnesses.
According to sampling guidelines, the sample size should be five to ten times the number of questionnaire items.17 Thus, we aimed to recruit at least 215 patients with COPD. “Before data collection, all participants were informed of the study purpose and procedures, and informed consent was obtained from all participants.” Data were collected using face-to-face questionnaire administration February and December 2024. This study employed a descriptive cross-sectional design and adhered to the STROBE guidelines.18
Data Analysis
IBM SPSS version 25.0 software, and R software were used for data analysis.
Preliminary Scale Evaluation
First, item analysis was conducted using SPSS within the framework of classical test theory. Participants were divided into high- and low-scoring groups based on the top 27% and bottom 27% of their total scores. Item discrimination was evaluated using critical ratios, with a critical ratio of 3.0 or greater and P-value < 0.05 considered acceptable Items not meeting these criteria were removed.19 Additionally, item discrimination was evaluated using the adjusted item-total correlation coefficients, and coefficients below 0.30 were considered inadequate.20 Internal consistency was also assessed using Cronbach’ s α if item deleted, and items whose removal increased the overall Cronbach’ s α were identified for potential deletion.
Second, to explore the underlying structure of the scale, the suitability of the data for component analysis was first assessed using the Kaiser–Meyer–Olkin measure of sampling adequacy and Bartlett’ s test of sphericity. The number of components to retain was then determined using Horn’ s parallel analysis, based on the Monte Carlo simulation technique with 10,000 replications, together with examination of the scree plot. Principal component analysis (PCA) with varimax rotation was subsequently conducted. Items with loadings ≥ 0.40 were retained, and items with substantial cross-loadings were considered for removal.21
Finally, item response theory (IRT) analyzes were conducted in R (version 4.4.3) using the mirt package. Essential unidimensionality was evaluated based on bifactor model results. Specifically, explained common variance (ECV) was calculated to quantify the proportion of common variance explained by the general factor, and omega hierarchical (ωH) was used to estimate the proportion of total score variance attributable to the general factor. ECV values above 0.70–0.80 and ωH values above 0.70 were taken as evidence supporting essential unidimensionality.22 When the findings supported essential unidimensionality, a graded response model (GRM) was fitted. Otherwise, a confirmatory multidimensional graded response model (MGRM) was fitted according to the prespecified domain structure.23 For each item, the discrimination (a) and difficulty (b) parameters were extracted to evaluate item quality.
Final Scale Evaluation
The Cronbach’ s α was used to evaluate the internal consistency reliability of the scale. A Cronbach’ s α coefficient ≥ 0.7 indicates good internal consistency of the questionnaire.17 A split-half reliability coefficient above 0.7 is generally considered to indicate good reliability.24
Based on the ratings of 35 experts on each item of the PRIN-COPD scale, the item-level content validity index (I-CVI) and the scale-level content validity index (S-CVI) were calculated. The I-CVI greater than 0.78 and S-CVI greater than 0.90 are considered indicative of high content validity.25
A confirmatory factor analysis (CFA) was conducted to examine the latent structure of the scale. Due to the limited sample size (N = 300), it was not feasible to split the dataset into independent subsamples for EFA and CFA. Therefore, CFA was performed on the same dataset in R (version 4.4.3) using the lavaan package, and this limitation has been acknowledged. CFA was conducted in lavaan using the weighted least squares mean and variance adjusted estimator, as the items were treated as ordered categorical variables. Model fit was evaluated using multiple indices: χ2/df, the Comparative Fit Index (CFI), the Tucker-Lewis Index (TLI), the Root Mean Square Error of Approximation (RMSEA) with 90% confidence interval, and the Standardized Root Mean Square Residual (SRMR).26 To assess the stability of the factor structure identified and tested within the same sample, an ordinary bootstrap procedure with 5000 resamples was applied to obtain 95% confidence intervals for the standardized factor loadings and factor correlations.27 The bootstrap results were used to evaluate the robustness of the standardized factor loadings, with loadings greater than 0.40 and confidence intervals excluding zero considered supportive of a stable factor structure.28
Results
Participants’ Characteristics
A total of 307 questionnaires were collected. Seven questionnaires contained missing responses and were excluded, leaving 300 complete questionnaires for analysis. Table 1 shows the demographic and clinical characteristics of the study participants. This study included 300 COPD patients who required pulmonary rehabilitation. The patients had a mean age of 71.01±9.38 years, and a mean disease duration of 8.56±7.34 years.
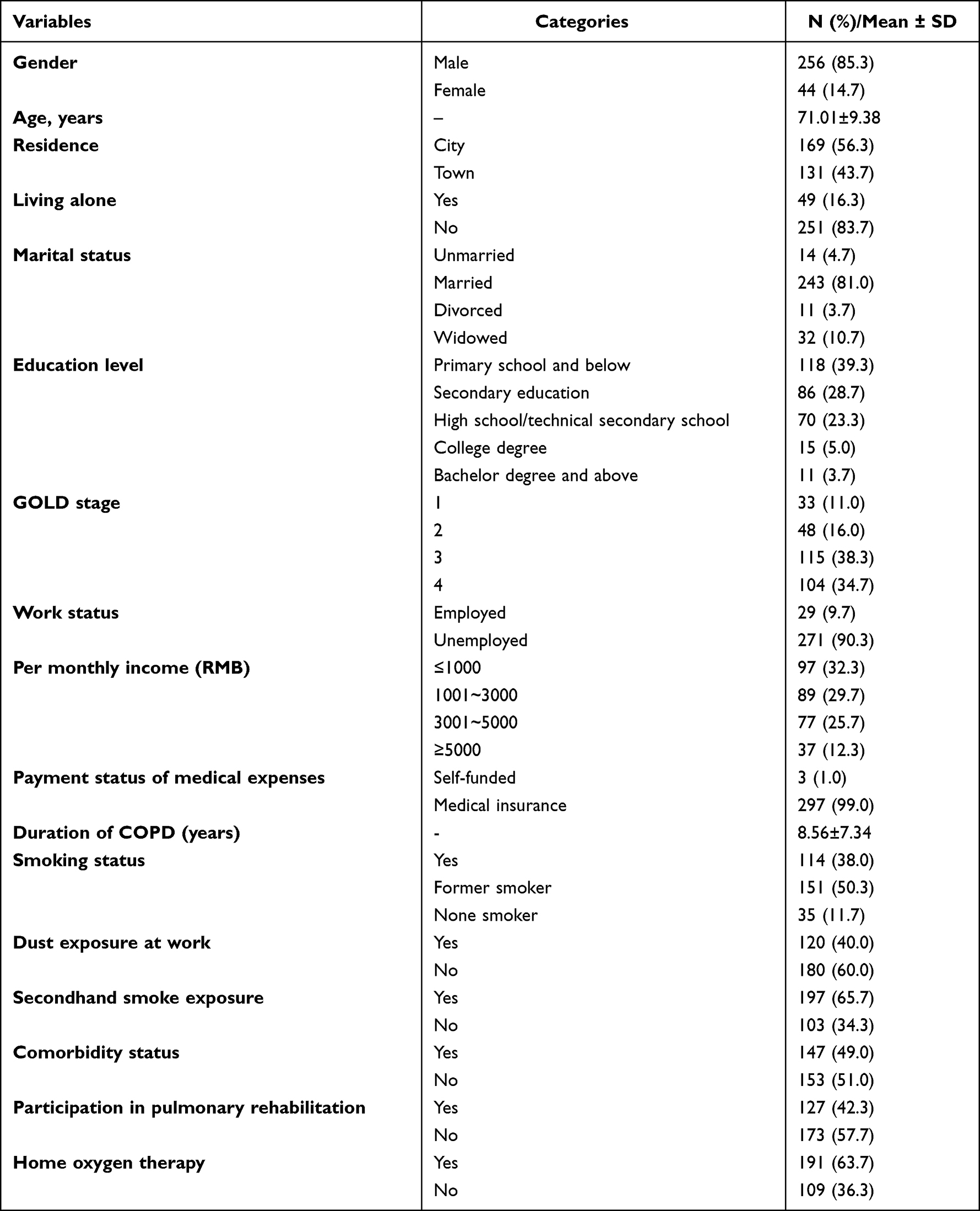 |
Table 1 Demographic and Clinical Characteristics of Participants (N = 300) |
Item Analysis
Analysis of items showed that, except for item 35 (|CR| = 1.410, p = 0.16), all items had significant critical ratio (CR) values (p < 0.05, |CR| > 3), and the corrected item-total correlations ≥ 0.30. Item 35 had a corrected item–total correlation of 0.134, which did not meet this criterion. The initial 43-item scale yielded a Cronbach’s α of 0.938. After removing item 35, Cronbach’s α increased to 0.940, whereas deleting any other single item reduced α to 0.936–0.938. Therefore, item 35 was removed from the scale.
Exploratory Factor Analysis
In this study, Kaiser-Meyer-Olkin measure of sampling adequacy (0.908) and Bartlett’s test of sphericity (χ2 = 6471.449, df = 861, p < 0.001) indicated that the data were suitable for factor analysis. Based on Cattell’s scree test, the eigenvalue-greater-than-one criterion, and Horn’s parallel analysis,29 the results supported a six-factor structure (Figure 3). After removing three items owing to cross-loading in the initial EFA (item 24,25,26), all factor loadings exceeded 0.4 without any cross-loading issues, ranging from 0.432 to 0.836 (Table 2). The six factors were labeled according to the characteristics of their items: Disease Self-Management Needs (14 items), Breathing and Sputum Clearance Training Needs (4 items), Exercise Training Needs (5 items), Smoking Cessation Needs (7 items), Social Support Needs (4 items), and Psychological Needs (5 items). This is consistent with the theoretical framework underlying the initial scale development. Six factors’ cumulative variance explained rate after rotation was 56.90%.
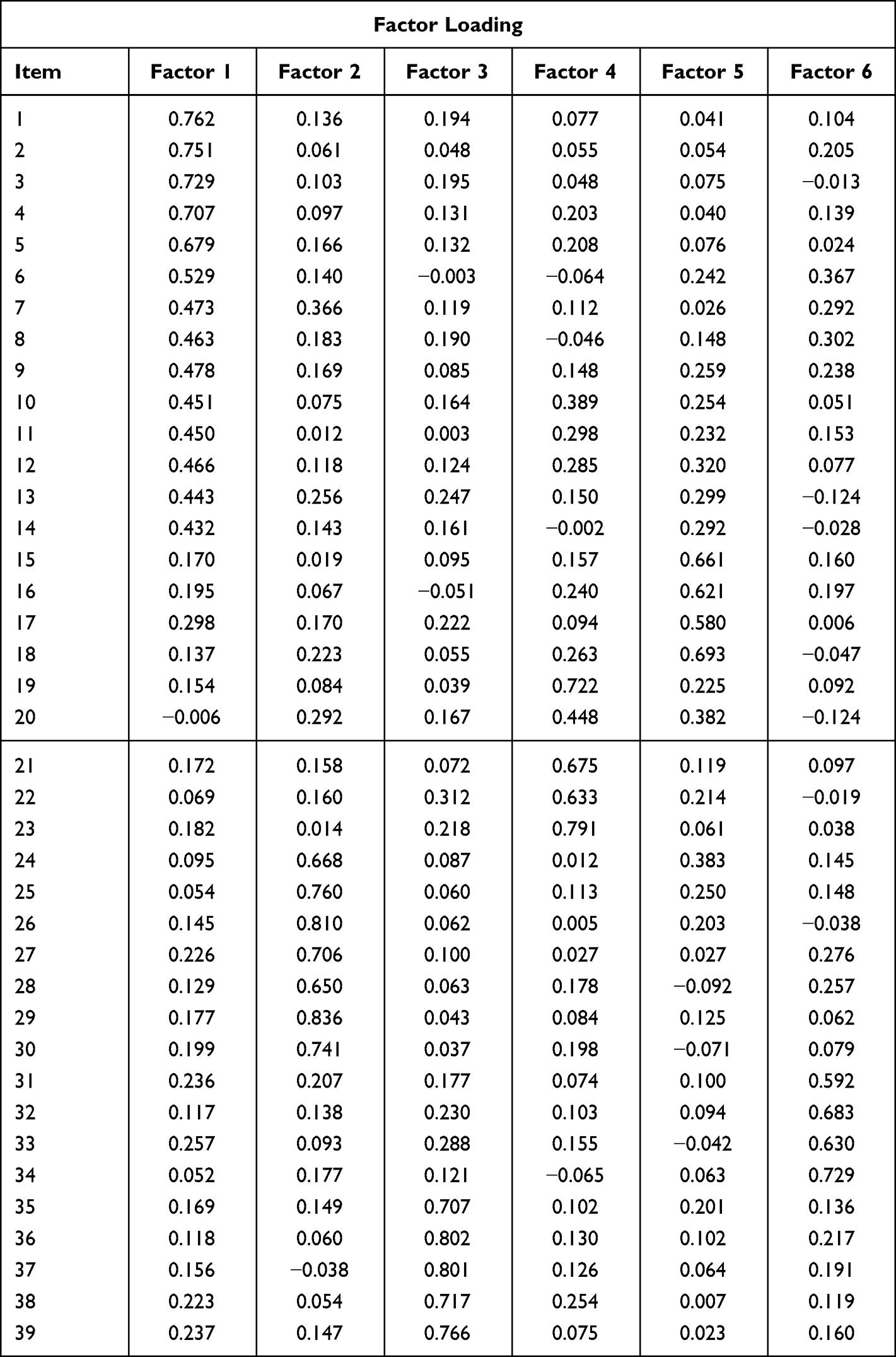 |
Table 2 Factor Loading on Items of the Scale (n =300) |
 |
Figure 3 Scree Plot for EFA with Parallel Analysis. |
Item Response Theory Results
The bifactor CFA model showed acceptable fit to the data (CFI = 0.986, TLI = 0.984, RMSEA = 0.050, SRMR = 0.065). However, essential unidimensionality was not fully supported by the bifactor indices (ECV = 0.522; Omega-H = 0.839). Therefore, a Multidimensional Graded Response Model (MGRM) was fitted according to the prespecified domain structure. The model converged successfully and showed acceptable model fit (M2 = 1469.08, RMSEA = 0.062, SRMSR = 0.066, CFI = 0.958, TLI = 0.954). Based on the fitted MGRM, item parameters were estimated, including discrimination (a) and difficulty (b), were estimated for the modeled subdimension (Table 3). All items exhibited discrimination parameters greater than 1.0, and difficulty parameters fell within the range from-4 to 4.
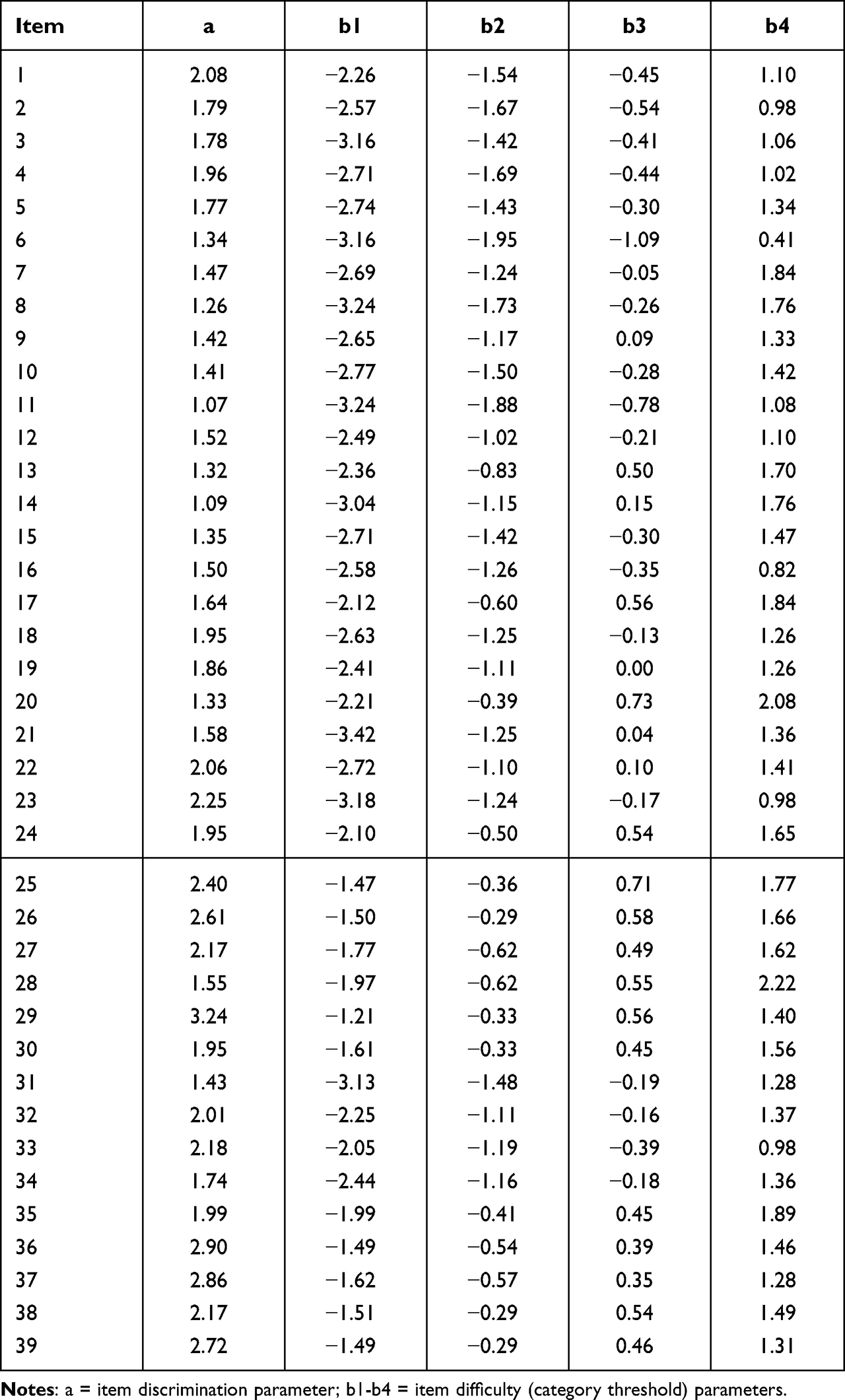 |
Table 3 IRT-Based Item Analysis Results |
Reliability
The findings showed that the PRIN-COPD scale had excellent reliability. The overall Cronbach’s α for the entire questionnaire was 0.936 and the Cronbach’s α coefficients for the subscale coefficients ranged from 0.742 to 0.897. For the total scale, the Spearman–Brown split-half reliability coefficient was 0.818, indicating good internal consistency. Table 4 provides a concise overview of the key reliability indices of the PRIN-COPD scale.
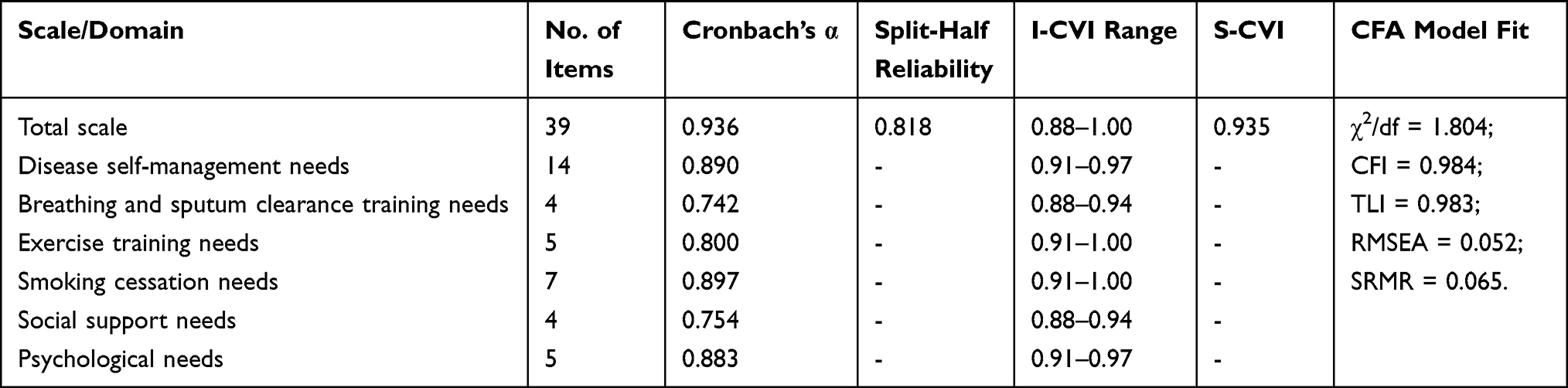 |
Table 4 Psychometric Indices of the PRIN-COPD Scale |
Content Validity
The findings indicated that the item-level I-CVI values ranged from 0.88 to 1.00, demonstrating a high degree of content validity for individual item. Furthermore, the S-CVI for the entire questionnaire was 0.935, suggesting that the questionnaire exhibited strong overall content validity.
Confirmatory Factor Analysis
The six-factor measurement model was assessed using the CFA. Model fit indices indicated a moderate fit to the data: χ2 = 1239.248, p < 0.001, df=687, χ2/df = 1.804; CFI = 0.984; TLI = 0.983; RMSEA = 0.052; SRMR = 0.065. Standardized factor loadings ranged from 0.50 to 0.87, all exceeding the recommended threshold of 0.40 (Figure 4). In addition, bootstrap analysis with 5,000 resamples showed that the 95% confidence intervals of all loadings did not include zero, supporting the stability of the estimates. Figure 4 showed the path diagram of the six-factor model, including standardized loadings and factor correlations. The final PRIN-COPD scale included 6 dimensions and 39 items, and the language used in scale development was Chinese (Supplementary Table S7).
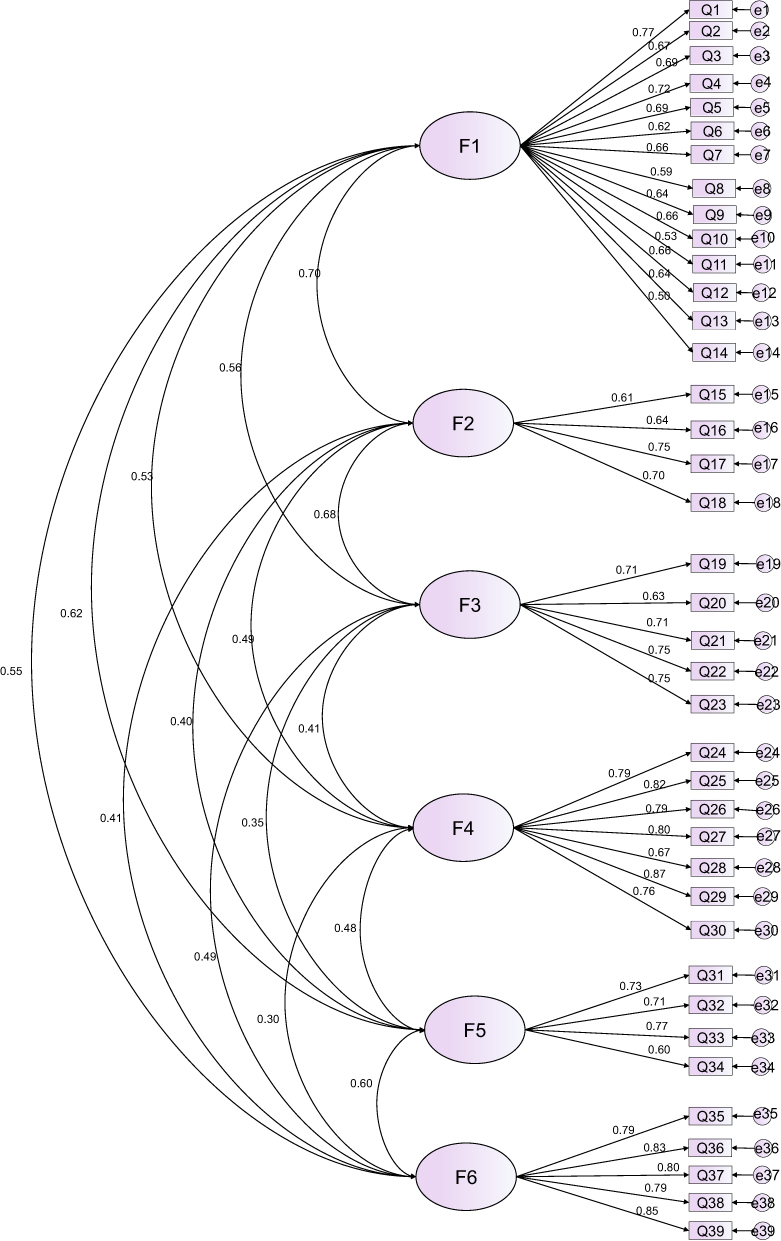 |
Figure 4 A schematic diagram of standardized model fitting of the scale (n = 300). |
Discussion
The PRIN-COPD scale developed in this study was to provide a comprehensive and accurate assessment of the information needs related to pulmonary rehabilitation among patients with chronic obstructive pulmonary disease (COPD). The instrument comprises 39 items grouped into six factors, which together explained 56.90% of the total variance in a sample of 300 patients. The development of the six dimensions of this scale was guided by Alderfer’s Existence, Relatedness and Growth (ERG) Theory; and Kochen’s information needs Theory. Thus, based on ERG Theory, needs related to disease self-management, breathing and sputum clearance training, exercise training, and smoking cessation were interpreted as reflecting existence needs; social support needs were interpreted as reflecting relatedness needs; and psychological needs were interpreted as reflecting growth needs. Similarly, these dimensions correspond to Kochen’s three levels of information needs: objective state (information about disease status and rehabilitation behaviors, eg., self-management, breathing, exercise, and smoking cessation); recognition (information and feedback from others, eg., social support); and expression (information related to the articulation and understanding of one’s inner psychological needs).The six factors of the scale embody these theoretical perspectives in a practical way. Specifically, Factor 1 assesses Disease Self-Management Needs that include patients’ ability to manage their condition and adhere to treatment, which is necessary for maintaining stability and optimizing disease management.30 Factor 2 assesses Breathing and Sputum Clearance Training Needs that include patients’ capacity to perform appropriate respiratory exercises and sputum clearance, which is essential for improved lung functionality and reduced complications.31 Factor 3 assesses Exercise Training Needs that addresses engagement in suitable physical activity, which is essential for enhancing endurance, physical function, and overall quality of life.32 Factor 4 assesses Smoking Cessation Needs that reveal patients’ ability to adopt strategies to reduce or quit smoking, and this can contribute to slowing disease progression and improving rehabilitation outcomes.33 Factor 5 assesses Social Support Needs, capturing competence in seeking and utilizing support from family, peers, and healthcare providers, which can reduce stress and promote adherence to rehabilitation.34 Factor 6 assesses Psychological Needs that represent patients’ capacity to manage emotional challenges such as anxiety or depression, which is necessary for supporting mental well-being and sustained participation in rehabilitation.35
Effectively supporting patients with COPD in pulmonary rehabilitation requires a comprehensive understanding of their diverse information needs.36 The PRIN-COPD scale reflects this multidimensional nature through six domains that together capture the core aspects of patients’ information concerns throughout rehabilitation. These domains are consistent with previous findings that emphasized the importance of empowering patients through tailored education and skill-building to enhance rehabilitation adherence and quality of life.37 Previous studies also showed that unmet information needs in COPD patients were closely associated with poor adherence to pulmonary rehabilitation, inadequate symptom management, and increased levels of anxiety and depression.38 Therefore, the PRIN-COPD scale could serve as a practical tool for healthcare professionals to assess the level and distribution of information needs among patients with COPD. The scale may also be incorporated into clinical workflows, such as pre-rehabilitation assessment, rehabilitation education planning, follow-up, and home-based rehabilitation management. If possible, the scale developed in this study could be integrated with electronic health records (EHRs) in future clinical practice. This assessment can help determine the overall level of pulmonary rehabilitation-related information needs among patients with COPD and identify domains in which needs are relatively higher or lower. These findings may guide clinicians in prioritizing educational content and providing more precise and individualized support, such as optimizing breathing techniques, adjusting exercise intensity, formulating smoking cessation strategies, and facilitating access to community or psychological support resources. While, the scale’s sensitivity to longitudinal change following educational or rehabilitative interventions has not yet been evaluated, and we will identify this as a priority for future research.
The IRT analyzes indicated that the PRIN-COPD scale was an appropriate instrument. The discrimination parameters (a) of the scale indicated moderate to high discrimination across the items. In addition, the threshold parameters (b) increased monotonically across response categories, suggesting that the response options functioned as intended. The distributional pattern of the threshold parameters suggested that the scale covered a relatively broad range of latent information needs, while being somewhat more sensitive to distinguishing respondents with low to moderate levels of information needs than those at the extreme high end. From a practical perspective, the scale appears particularly useful for identifying patients with emerging information needs and for differentiating relatively low to moderate levels of need in routine care. However, the current items mainly reflect basic and commonly expressed information needs, and may be less sensitive to more complex or highly individualized concerns. Adding items that target higher levels of information need may improve measurement precision among patients at the upper end of the construct.
Regarding model fit, confirmatory factor analysis (CFA) indicated acceptable-to-good fit to the data. The relative fit indices were high (CFI = 0.984; TLI = 0.983), and the absolute fit indices were within commonly accepted ranges (RMSEA = 0.052; SRMR = 0.065). Nevertheless, because EFA and CFA were conducted on the same dataset, the reported fit may be somewhat optimistic due to capitalization on chance.39 Future studies should replicate and cross-validate the factor structure in an independent sample to confirm its stability and generalizability.
To further evaluate the stability of the measurement structure, a bootstrap procedure with 5,000 resampling operations was conducted.27 Results indicated that all observed variables had standardized factor loadings exceeding the practical threshold of 0.40, and their bootstrap confidence intervals did not include zero. These findings suggested that, although the overall model fit could be further optimized in independent samples, the relationships between each observed item and its respective latent factor were stable, significant, and substantively meaningful.40 Collectively, the CFA and bootstrap results provided strong evidence for the reliability and internal structure of the scale, supporting its use as a foundation for subsequent research.
Moreover, the overall Cronbach’s α coefficient of the scale was 0.936, and the Cronbach’s α values for the six dimensions ranged from 0.742 to 0.897, all exceeding the commonly accepted threshold of 0.70,41 suggesting that the items within each dimension consistently measured the intended constructs. However, among the six domains, the Breathing and Sputum Clearance Training Needs (α = 0.742) and Social Support Needs (α = 0.754) domains showed relatively lower but still acceptable internal consistency. This may be attributed to the inherent variability in patients’ understanding and engagement with breathing techniques, or their access to and reliance on social support resources. That is, such domains are prone to being strongly influenced by individual disease status, rehabilitation experience, and social context,42 which can naturally introduce greater response diversity among patients. Previous COPD-related studies reported similar findings, indicating that constructs involving behavioral and social factors often yielded slightly lower internal consistency due to contextual and individual differences.37 Thus, overall, the reliability results indicated that the PRIN-COPD scale demonstrated acceptable internal consistency and stability across its dimensions.
Because the scale was developed and tested among Mandarin-speaking patients with COPD in China, further adaptation is needed before it is used in other cultural or language settings. Differences in healthcare systems, pulmonary rehabilitation services, and health literacy may influence how patients understand and respond to the items. Cross-cultural adaptation, including forward and backward translation, expert review, and pilot testing, should therefore be conducted, followed by re-evaluation of the scale’s reliability and validity in the target population.43
Limitations
Although the PRIN-COPD scale demonstrated acceptable reliability and structural validity, several limitations should be noted. First, participants were recruited from one city, which may limit the generalizability of the findings to patients in other regions with different demographic or healthcare systems. In addition, the psychometric evaluation sample consisted of patients who were undergoing or willing to undergo pulmonary rehabilitation, which was consistent with the focus of this study on information needs in the context of pulmonary rehabilitation. However, patients who were unfamiliar with, skeptical about, or unwilling to participate in pulmonary rehabilitation, as well as those with lower health literacy or greater functional impairment, may have been underrepresented. As a result, the information needs profile identified in this study may not fully reflect the needs of patients with lower acceptance of, or greater barriers to, pulmonary rehabilitation, and caution is needed when extending these findings to the broader COPD population. Moreover, because of sample size constraints, the EFA and CFA were conducted using the same dataset rather than independent samples, which may limit the verification of the stability of the factor structure. In addition, convergent validity was not analyzed in this study. Future studies should recruit larger multicenter samples and include more diverse patients with COPD to conduct CFA, comprehensively assess convergent validity, and further evaluate the robustness, applicability, and generalizability of the scale.
Conclusion
This study developed and validated a 39-item, five-point Likert scale to assess pulmonary rehabilitation-related information needs in patients with COPD. The PRIN-COPD scale includes six dimensions: disease self-management needs, breathing and sputum clearance training needs, exercise training needs, smoking cessation needs, social support needs, and psychological needs, with higher scores indicating greater information needs. It showed acceptable reliability and construct validity. Unlike general information needs measures, this scale focuses specifically on pulmonary rehabilitation and, to our knowledge, is the first validated tool designed to assess pulmonary rehabilitation-related information needs among patients with COPD. It can be used to assess both the overall level of information needs and the domains in which patients report relatively higher or lower needs. Its use may help clinicians identify the gap between current support and patient needs and inform more individualized, patient-centered pulmonary rehabilitation education and follow-up support.
Abbreviations
CFA, Confirmatory factor analysis; CFI, Comparative fit index; COPD, Chronic obstructive pulmonary disease; ECV, explained common variance; EFA, Exploratory factor analysis; ERG, Existence, Relatedness, and Growth; GOLD, Global Initiative for Chronic Obstructive Lung Disease; I-CVI, Item-level content validity index; IRT, Item response theory; LINQ, Lung Information Needs Questionnaire; MGRM, Multidimensional graded response model; RMSEA, Root Mean Square Error of Approximation; S-CVI, Scale-level content validity index; SRMR, Standardized Root Mean Square Residual; TLI, Tucker–Lewis index.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study is available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Xiangya School of Nursing, Central South University (approval number: E201934, approval date: June 20, 2021), and the study was conducted in accordance with the ethical principles of the World Medical Association Declaration of Helsinki. The ethical approval covered all phases of the study, including the item generation interviews, expert consultation, pilot testing, and the cross-sectional survey used for psychometric evaluation. Informed consent was obtained from all participants, and participants had the right to withdraw from the study at any time. No individual was forced to participate against their will. All collected information was kept strictly confidential and properly managed. The collected data were used solely for the purposes of this study.
Acknowledgments
We thank all participants for taking the time to complete the questionnaire and contribute to this study. We also thank the healthcare professionals who supported participant recruitment.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
1) Hunan Province’s Natural Science Foundation Project (Grant No. 2025JJ50579); 2) Project of the Center for Capacity Building and Continuing Education, National Health Commission of the People’s Republic of China (Grant No. GWJJMB202510023017); and 3) 2025 Special Project of the Hunan Nursing Association (Grant No. HNKYY202504).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Celli B, Fabbri L, Criner G, et al. Definition and nomenclature of chronic obstructive pulmonary disease: time for its revision. Am J Respir Crit Care Med. 2022;206(11):1317–16. doi:10.1164/rccm.202204-0671PP
2. Confalonieri M, Braga L, Salton F, Ruaro B, Confalonieri P. Chronic obstructive pulmonary disease definition: is it time to incorporate the concept of failure of lung regeneration? Am J Respir Crit Care Med. 2023;207(3):366–367. doi:10.1164/rccm.202208-1508LE
3. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for prevention, diagnosis and management of COPD: 2026 report. Version 1.3. 2026. Available from: https://goldcopd.org/wp-content/uploads/2026/01/GOLD-REPORT-2026-v1.3-8Dec2025_WMV2.pdf.
4. Agustí A, Celli BR, Criner GJ, et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Eur Respir J. 2023;61(4):1. doi:10.1183/13993003.00239-2023
5. Putcha N, Maselli DJ, Bon J, Lester MG, Drummond MB. Dyspnea in chronic obstructive pulmonary disease: expert assessment of management in clinical practice. Pulm Ther. 2025;11(4):553–567. doi:10.1007/s41030-025-00318-x
6. Gloeckl R, Spielmanns M, Stankeviciene A, et al. Smartphone application-based pulmonary rehabilitation in COPD: a multicentre randomised controlled trial. Thorax. 2025;80(4):209–217. doi:10.1136/thorax-2024-221803
7. Troosters T, Janssens W, Demeyer H, Rabinovich RA. Pulmonary rehabilitation and physical interventions. Eur Respir Rev. 2023;32(168):220222. doi:10.1183/16000617.0222-2022
8. Rochester CL, Alison JA, Carlin B, et al. Pulmonary rehabilitation for adults with chronic respiratory disease: an official American Thoracic Society clinical practice guideline. Am J Respir Crit Care Med. 2023;208(4):e7–e26. doi:10.1164/rccm.202306-1066ST
9. Benzo RP. Self-management programs and the pursuit of behavior change. Respir Care. 2024;69(6):678–685. doi:10.4187/respcare.11987
10. Hug S, Cavalheri V, Gucciardi DF, Hill K. Quantifying uptake and completion of pulmonary rehabilitation programs in people with chronic obstructive pulmonary disease known to tertiary care. Chron Respir Dis. 2024;21:14799731231224781. doi:10.1177/14799731231224781
11. Qin H, Jia P, Yan Q, et al. Barriers and facilitators to pulmonary rehabilitation in COPD: a mixed-methods systematic review. BMC Pulm Med. 2025;25(1):314. doi:10.1186/s12890-025-03769-9
12. Muijsenberg AJ, Houben-Wilke S, Tatousek J, Lacroix J, Spruit MA, Janssen DJ. Educational needs of people with COPD or asthma entering pulmonary rehabilitation and their significant others: a cross-sectional study. Chron Respir Dis. 2025;22:14799731251316891. doi:10.1177/14799731251316891
13. Mendes MA, Rodrigues G, Janssen DJA, Spruit MA, Marques A. Understanding the determinants and outcomes of education in pulmonary rehabilitation: moving toward person-centered care. Chest. 2025;167(6):1615–1627. doi:10.1016/j.chest.2025.01.005
14. Hyland ME, Jones RCM, Hanney KE. The Lung Information Needs Questionnaire: development, preliminary validation and findings. Respir Med. 2006;100(10):1807–1816. doi:10.1016/j.rmed.2006.01.018
15. Alderfer CP. An empirical test of a new theory of human needs. Organ Behav Hum Perform. 1969;4(2):142–175. doi:10.1016/0030-5073(69)90004-X
16. Belkin NJ. Anomalous states of knowledge as a basis for information retrieval. Can J Inform Sci. 1980;5:133–143.
17. Wang Z, Li X, Zhang F, et al. Development and validation of a Chinese version of an Information Needs Questionnaire for patients with breast cancer undergoing radiotherapy. J Clin Nurs. 2025;34(7):2690–2701. doi:10.1111/jocn.17682
18. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting of observational studies. Internist. 2008;49(6):688–693. doi:10.1007/s00108-008-2138-4. German.
19. Shen F, Hu LH, Huang HS, Li L. Development and validation of the scale for symptom clusters in patients with myasthenia gravis. BMC Neurol. 2023;23(1):196. doi:10.1186/s12883-023-03240-4
20. Latif A, Boonyoung N, Chawalit A. Development and psychometric evaluation of Registered Nurses’ Clinical Leadership Scale (RN-CLS) in Bangladesh. Med Res Arch. 2025;13(3). doi:10.18103/mra.v13i3.6386
21. Ahmad N, Sinaii N, Panahi S, et al. The FACIT-Sp spiritual wellbeing scale: a factor analysis in patients with severe and/or life-limiting medical illnesses. Ann Palliat Med. 2022;11(12):3663–3673. doi:10.21037/apm-22-692
22. Redelinghuys K, Morgan B. Psychometric properties of the Burnout Assessment Tool across four countries. BMC Public Health. 2023;23(1):824. doi:10.1186/s12889-023-15604-z
23. Depaoli S, Tiemensma J, Felt JM. Assessment of health surveys: fitting a multidimensional graded response model. Psychol Health Med. 2018;23(suppl 1):13–31. doi:10.1080/13548506.2018.1447136
24. Qian Z, Yang Y, Tan J, et al. Psychometric evaluation of the Chinese version of the Mental Health System Responsiveness Questionnaire for psychiatric outpatients: classical test theory and item response theory approaches. Patient Prefer Adherence. 2025;19:729–740. doi:10.2147/PPA.S503016
25. Shi J, Mo X, Sun Z. Content validity index in scale development. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2012;37(2):152–155. doi:10.3969/j.issn.1672-7347.2012.02.007. Chinese.
26. Józefowicz J, Kowalczyk-Grębska N, Brzezicka A. Validation of Polish version of Dispositional Flow Scale-2 and Flow State Scale-2 questionnaires. Front Psychol. 2022;13:818036. doi:10.3389/fpsyg.2022.818036
27. Efron B, Tibshirani RJ. An Introduction to the Bootstrap. New York, NY: Chapman & Hall; 1993.
28. Ang CS, Tan JP, Fam SY. Psychometric properties of the Training Parenting Style Scale in a Malaysian sample of adolescents: factor analysis, internal consistency, and measurement invariance. J Child Fam Stud. 2016;25(5):1505–1514. doi:10.1007/s10826-015-0333-1
29. Chua WL, Smith D, Wee LPC, et al. Development and psychometric evaluation of the Attitudes Towards Recognising Early and Noticeable Deterioration (ATREND) scale. J Clin Nurs. 2023;32(11–12):2684–2699. doi:10.1111/jocn.16350
30. Lenferink A, Brusse-Keizer MGJ, van der Palen J, Effing TW. Personalizing self-management interventions in COPD-looking beyond one-size-fits-all. Int J Chron Obstruct Pulmon Dis. 2025;20:65–68. doi:10.2147/COPD.S511278
31. Chen Q, Wu Y. Effects of respiratory function exercise combined with detailed nursing on patients with chronic obstructive pulmonary disease. Int J Clin Exp Med. 2022;15(3):112–117.
32. Chen Y, Zhang P, Dong Z, et al. Effect of Baduanjin exercise on health and functional status in patients with chronic obstructive pulmonary disease: a community-based, cluster-randomized controlled trial. NPJ Prim Care Respir Med. 2024;34(1):43. doi:10.1038/s41533-024-00400-y
33. Jakobsen RK, Farver-Vestergaard I, Løkke A. The uphill journey of smoking cessation in chronic obstructive pulmonary disease: why a well-built vehicle matters. Front Health Serv. 2025;5:1659295. doi:10.3389/frhs.2025.1659295
34. Leukel PJ, Piette JD, Lee AA. Impact of loneliness and social support on acute health service use and symptom exacerbation among adults with asthma and COPD. J Clin Psychol Med Settings. 2025;32(2):375–384. doi:10.1007/s10880-024-10046-0
35. Volpato E, Farver-Vestergaard I, Brighton LJ, et al. Nonpharmacological management of psychological distress in people with COPD. Eur Respir Rev. 2023;32(167):220170. doi:10.1183/16000617.0170-2022
36. Almonacid C, Gómez R, Morán I, et al. Support needs of patients with chronic obstructive pulmonary disease (COPD) and asthma throughout their patient journey: a qualitative study. Int J Chron Obstruct Pulmon Dis. 2025;20:2639–2658. doi:10.2147/COPD.S526548
37. Barradell AC, Bourne C, Alkhathlan B, Larkin M, Singh SJ. A qualitative assessment of the pulmonary rehabilitation decision-making needs of patients living with COPD. NPJ Prim Care Respir Med. 2022;32(1):23. doi:10.1038/s41533-022-00285-9
38. Siltanen H, Aine T, Huhtala H, Kaunonen M, Paavilainen E. The information needs of people with COPD-the holistic approach with special reference to gender and time since diagnosis. Nurs Open. 2021;8(5):2498–2508. doi:10.1002/nop2.773
39. Zhou X. Evaluation of the split-data strategy in factor analysis. master’s thesis. Urbana, IL: University of Illinois at Urbana-Champaign; 2022.
40. Nevitt J, Hancock GR. Performance of bootstrapping approaches to model test statistics and parameter standard error estimation in structural equation modeling. Struct Equation Model. 2001;8(3):353–377. doi:10.1207/S15328007SEM0803_2
41. Toksoz F, Acikgoz A, Mutlu FS, Sayik D. Febrile convulsion knowledge scale for parents/caregivers: a validity and reliability study. J Pediatr Nurs. 2023;73:e509–e515. doi:10.1016/j.pedn.2023.10.023
42. Bottle A, Adamson A, Zhang X, Hayhoe B, Quint JK. What happens between first symptoms and first acute exacerbation of COPD-observational study of routine data and patient survey. Health Soc Care Deliv Res. 2024;12(43):1–80. doi:10.3310/CGTR6370
43. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25(24):3186–3191. doi:10.1097/00007632-200012150-00014
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.