Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Development and Expert Consensus of an Evidence-Based Strategy to Prevent Postoperative Delirium in Malnourished Cancer Patients
Received 23 March 2026
Accepted for publication 15 June 2026
Published 24 June 2026 Volume 2026:19 609750
DOI https://doi.org/10.2147/JMDH.S609750
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Tilakavati Karupaiah
Yi-Fang Ma, Qi Wu
Department of Nursing, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, 310003, People’s Republic of China
Correspondence: Qi Wu, Department of Nursing, The First Affiliated Hospital, Zhejiang University School of Medicine, No. 79 Qingchun Road, Hangzhou, Zhejiang, 310003, People’s Republic of China, Tel +8613735838292, Email [email protected]
Background: Cancer patients with malnutrition are at high risk for postoperative delirium. To develop a preliminary prevention strategy for postoperative delirium in malnourished cancer patients based on literature search and Delphi expert consultations.
Methods: Between August 2023 and January 2024, we followed the PIPOST (Population, Intervention, Professional, Outcome, Setting, and Type of evidence) framework to formulate clinical questions and retrieved relevant literatures using the 6S model (Systems, Summaries, Synopses of Syntheses, Syntheses, Synopses of Single Studies, and Single Studies). Based on the evidence, a preliminary strategy for preventing postoperative delirium in malnourished cancer patients was developed. Following two rounds of Delphi expert consultations, the final version of the strategy was created to develop and refine the proposed prevention strategy for postoperative delirium.
Results: The initial literature search yielded 6218 articles, from which 20 core studies were ultimately included. The response rates for the two rounds of Delphi consultations were 96.0% and 100%, with authority coefficient 0.912 and expert concordance coefficient (Kendall’s W) increased from 0.398 to 0.465 (p < 0.01). The finalized prevention strategy comprised four categories, 10 sections, and 27 items.
Conclusion: An evidence-based strategy for preventing postoperative delirium has been developed preliminarily. Further studies are warranted to evaluate its clinical feasibility and efficacy to reduce the incidence of postoperative delirium in malnourished cancer patients.
Keywords: evidence-based approach, Delphi consultation, malnutrition, cancer, postoperative delirium, prevention strategy
Introduction
Postoperative delirium (POD) is a neurocognitive syndrome characterized by the acute onset of fluctuating consciousness and changes in mental status following a surgical procedure.1 Affected patients may exhibit inattention, confusion, disorientation, and sleep–wake cycle disturbances.2 POD could affect up to 61.4% of cancer patients and its incidence varied depending on the cancer type and surgical approaches.3,4 POD is associated not only with increased postoperative complications and mortality but also with prolonged hospital stays, elevated healthcare costs, and long-term cognitive impairment.5–8 Current strategies for preventing POD remain limited by persistent underdiagnosis, implementation challenges, modest pharmacologic efficacy, and inconsistent long-term benefits.9,10 Although multicomponent nonpharmacologic interventions can reduce POD incidence, their effectiveness is often constrained by resource demands and variable adherences, while pharmacologic approaches show limited impact on major outcomes such as mortality, cognition, and quality of life.11,12 In addition, existing strategies inadequately target the underlying biological mechanisms of delirium and have not been shown to prevent long-term cognitive decline, highlighting the need for more standardized clinically effective prevention approaches.13
A critical, yet often overlooked, independent risk factor for POD in this population is malnutrition.14 Malnutrition is strongly associated with an increased risk of POD, likely through multiple interconnected mechanisms, including systemic and neuroinflammation, neurotransmitter imbalance, oxidative stress, micronutrient deficiencies, altered drug pharmacokinetics, reduced neurotrophic support, and decreased cognitive reserve.15–19 Chronic inflammation and hypoalbuminemia promote blood-brain barrier dysfunction and microglial activation, while deficiencies in key nutrients impair neurotransmitter synthesis and antioxidant defenses.20 In addition, malnutrition often coexists with frailty and sarcopenia, further lowering the brain’s resilience to perioperative stress and increasing susceptibility to delirium.21 Cancer patients frequently experience malnutrition due to tumor-related metabolic alterations, eating difficulties, and gastrointestinal side effects from radiotherapy and chemotherapy.22,23 The cancer-related malnutrition can involve unique pathophysiology, such as cachexia, tumor-driven inflammation, and treatment toxicity, that is not addressed adequately by existing POD prevention frameworks.24,25 The National Comprehensive Cancer Network identifies malnutrition as both a predisposing and precipitating factor for POD in older cancer patients.26 Although numerous studies have proposed strategies for managing POD, most have focused on elderly or critically ill patients undergoing routine surgery, often overlooking the specific needs of malnourished cancer patients.27,28 Furthermore, current management approaches are limited by the absence of integrated nutrition–delirium prevention strategies, fragmented perioperative care, and a lack of clearly defined multidisciplinary collaboration.19 All of these have contributed to a significant gap in the clinical practice to prevent POD in malnourished cancer patients, which requires an evidence-based, scientifically rigorous, and targeted framework in this special patient population.
In evidence-based practice, the PIPOST framework serves as a foundational structure for systematically formulating clinical questions.29,30 It comprises six core components: Population, Intervention, Professional, Outcome, Setting, and Type of evidence. This framework enables healthcare professionals to generate focused clinical questions grounded in the best available evidence for a targeted patient population and to develop intervention strategies to achieve desired outcomes. PIPOST can help to clearly define the target research population, intervention, professionals involved, desired outcomes, clinical setting, and acceptable evidence types, which improves the precision, reproducibility, and clinical relevance of the search process while reducing ambiguity and selection bias. Once the clinical questions are formulated using the PIPOST framework, the 6S model (Systems, Summaries, Synopses of Syntheses, Syntheses, Synopses of Single Studies, and Single Studies) can be employed to retrieve relevant evidence-based resources.31 This model functions as a hierarchical pyramid, categorizing evidence by its level of synthesis and clinical applicability—from individual studies at the base to evidence-based guidelines and clinical decision support systems at the apex.32 The 6S model allows researchers to efficiently identify the highest-quality and most synthesized evidence. The integration of the PIPOST framework and the 6S model can enhance methodological rigor, improve consistency in evidence selection, reduce time spent screening heterogeneous literatures, and support the development of recommendations grounded in comprehensive and up-to-date evidence. The combination of PIPOST framework and 6S model has been successfully employed to identify best practices in areas such as lifestyle interventions for metabolic syndrome, treatment adherence in tuberculosis patients, and invasive arterial blood pressure management in critically ill patients.29,33,34
In the present study, we applied the PIPOST framework and the 6S model to develop a preliminary strategy for preventing POD, which was subsequently refined through rigorous Delphi expert consultation to produce a finalized version. Our objective was to bridge the gap between high-level evidence and individualized clinical application, and propose POD prevention strategy for further clinical validation studies in malnourished cancer patients, as well as large multicenter studies in subgroup of cancer patients, since cancer type and surgery approach could impact the POD incidence.
Methods
Study Design and Ethical Approval
Between August 2023 and January 2024, we adopted a multi-step research design that included: (1) formulation of research questions using the PIPOST framework; (2) literature retrieval guided by the 6S model; (3) development of a preliminary POD prevention strategy; and (4) refinement of the strategy through Delphi expert consultation. The study protocol was approved by the ethics committee of The First Affiliated Hospital, Zhejiang University School of Medicine (IRB Approval Numbers: 2024–0091), and informed consent was obtained from all participants.
Study Protocol
Research Question Formulation
The PIPOST model was used to identify key questions regarding POD in malnourished cancer patients. The components of the PIPOST framework were defined as follows: P (Patient Population) — malnourished cancer patients; I (Intervention) — POD prevention-related methods; P (Professional) — clinical medical staff; O (Outcome) — incidence of POD; S (Setting) — operating room, recovery room, and medical ward; and T (Type of Evidence) — clinical decision-making tools, guidelines, expert consensus statements, systematic reviews, and evidence summaries.
Literature Retrieval
A top-down literature search was conducted using the 6S model. English search terms included “malnutrition”, “undernutrition”, “nutritional decline”, “nutritional disorder”, “nutritional disturbance”, “nutritional risk”, “subnutrition”, or “malnourishment”, combined with “postoperative delirium”, “POD”, “delirium”, “postoperative delirium”, “delusion”, “acute brain syndrome”, or “acute organic brain syndrome”. Equivalent Chinese terms were used for Chinese-language databases. The databases searched included UpToDate, BMJ Best Practice, Joanna Briggs Institute evidence-based healthcare database, Guidelines International Network, National Guideline Clearinghouse, Scottish Intercollegiate Guidelines Network, Australia Clinical Practice Guidelines, New Zealand Guidelines Group, Canadian Medical Association clinical practice guideline database, National Institute for Health and Care Excellence, Medlive, Registered Nurses’ Association of Ontario, European Society for Clinical Nutrition and Metabolism, European Society of Anaesthesiology, European Society of Intensive Care Medicine, American Society for Parenteral and Enteral Nutrition, American Association of Nurse Anesthesiology, Society of Critical Care Medicine, American Association of Critical-Care Nurses, American Society of Anesthesiologists, American Medical Association, American Society for Enhanced Recovery, the Chinese Medical Association, the Chinese Nursing Association, PubMed, Web of Science, Cochrane Library, Embase, CINAHL, CNKI, Wanfang Data, VIP Database, and the Chinese Biomedical Literature Database. The search period covered from database inception to December 31, 2024.
The literature included only clinical studies focused on the prevention of POD in malnourished cancer patients. Included literature types were clinical decision-making recommendations, guidelines, expert consensus statements, systematic reviews, and evidence summaries. Literature types excluded from the review included guideline interpretations, case reports, narrative reviews, articles with incomplete information, and duplicate publications.
The Appraisal of Guidelines for Research and Evaluation II (AGREE II) instrument was used to assess guideline quality.35 The Joanna Briggs Institute (JBI) appraisal tools were used to evaluate the quality of expert consensus documents, systematic reviews, and evidence summaries.36 Clinical decision-making resources from UpToDate and BMJ Best Practice were considered high-level evidence by default. Quality assessments were conducted independently by two researchers with training in evidence-based nursing. Discrepancies were resolved through open discussion within the research team.
A preliminary strategy for POD prevention was developed by integrating core evidence extracted from the relevant literature with insights from clinical practice.
Delphi Expert Consultation
Purposeful sampling was used to select a multidisciplinary panel of Delphi experts. The inclusion criteria were as follows: (1) at least 10 years of work experience in relevant specialties such as surgery, anesthesiology, nutrition, nursing, or critical care medicine; (2) an intermediate or higher professional title; (3) a bachelor’s degree or higher; and (4) familiarity with POD management or nutritional support.
Two rounds of expert consultations were conducted anonymously to evaluate the preliminary POD prevention strategy. A questionnaire was developed based on the initial strategy and included three sections: (1) expert background information; (2) self-assessment of authority (including familiarity with the topic and basis for judgment); and (3) POD prevention and management strategies (first-round Delphi expert questionnaire in Supplementary Materials Table S1). The third section used a 5-point Likert scale (1 = very unimportant, 5 = very important) and included a comment section for additional suggestions.
After the first round of consultation, the questionnaire was revised based on items with an importance score ≥ 4.0 and a coefficient of variation (CV) ≤ 0.25, in combination with expert feedback. In the second round (second-round Delphi expert questionnaire in Supplementary Materials Table S2), the expert coefficient of concordance was used to assess agreement among panel members. Necessary modifications were made to strengthen the final expert recommendations.
Statistical Analysis
All statistical analyses were performed using SPSS software (version 26.0; IBM, USA). The following metrics were reported: expert response rate; authority coefficient (Cr) calculated as Cr = (familiarity coefficient [Cs] + judgment basis coefficient Ca)/2, coefficient of concordance (Kendall’s W), and CV.
Results
Literature Retrieval and Quality Assessment
A total of 6218 articles were initially retrieved. After removing duplicates, conducting a preliminary screening based on titles and abstracts, and performing a full-text review, 20 core articles were ultimately included, consisting of five clinical decision-making documents, three guidelines, six expert consensus statements, three systematic reviews, and three evidence summaries (Figure 1).
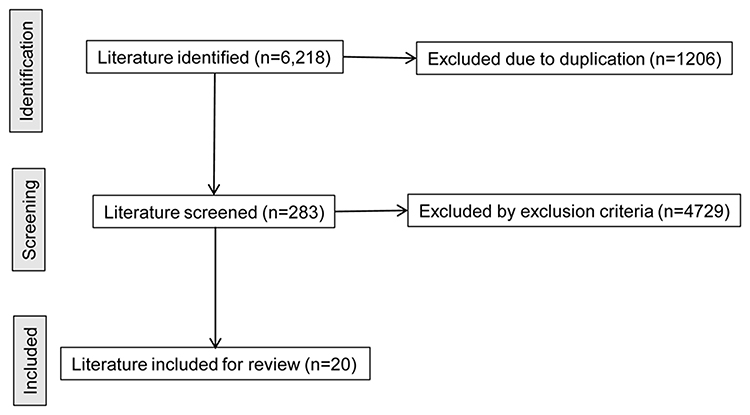 |
Figure 1 Literature selection flowchart. |
The overall methodological quality of the included literature was high. Among the guidelines, two were rated as Level A and one as Level B. All systematic reviews were graded as Level 3a, and all expert consensus documents were rated as Level 5b.
Delphi Expert Consultation
A total of 25 experts participated in the study, including 7 surgeons, 5 anesthesiologists, 4 nutritionists, 6 nurses, and 3 specialists in critical care medicine. There were 13 males (52.0%) and 12 females (48.0%), with ages ranging from 39 to 63 years and a mean age of 47.2 (±5.6) years. Work experience ranged from 10 to 38 years, a mean of 23.6 (±7.1) years. Nineteen participants (76.0%) held senior-level positions and 6 (24.0%) held intermediate-level titles. Twelve experts (48.0%) held doctoral degrees, 8 (32.0%) had master’s degrees, and 5 (20.0%) held bachelor’s degrees.
In the first round of expert consultation, 25 questionnaires were distributed, and 24 valid responses were received, yielding an effective response rate of 96.0%. In the second round, 24 revised questionnaires were distributed, and all were returned, yielding a 100% response rate and indicating a high level of engagement among the experts.
Expert reliability analysis demonstrated a familiarity coefficient (Cs) of 0.923, a judgment basis coefficient (Ca) of 0.901, and an authority coefficient (Cr) calculated as (0.923 + 0.901)/2 = 0.912. Since Cr > 0.8, the results indicated strong authority and reliability among the participating experts.
An analysis of expert opinion consistency showed the following:
- First Round of Consultation:
The summarized results of first round of consultation is shown in Supplementary Materials Table S3. The mean importance scores for each item ranged from 3.92 to 4.95, with CVs between 0.13 and 0.27. Two items with importance scores below 4.0 were removed. In response to concerns regarding unclear assessment timing, cognitive stimulation measures, and the definition of care provider roles, experts refined the POD prevention strategy. Key modifications included:
- The timeline for nutritional screening and assessment was clarified as within 24 and 48 h, respectively.
- The method was defined as the “three questions” approach, with the frequency of implementation specified.
- Responsibilities within the multidisciplinary team were explicitly defined:
- Physicians develop the overall therapeutic plan.
- Nutritionists lead nutritional assessment and intervention.
- Nurses conduct clinical symptom screening and longitudinal monitoring.
- Anesthesiologists optimize pre- and intra-operative plans.
- Rehabilitation therapists manage early mobilization and postoperative exercise.
Following these revisions, a second preliminary version of the POD prevention strategy—comprising four categories, 10 sections, and 27 items—was used in the second round of expert consultation.
- Second round of consultation:
The summarized results of second round of consultation is shown in Supplementary Materials Table S4. The mean importance scores ranged from 4.25 to 4.98, with CVs between 0.07 and 0.18, all of which met the inclusion criteria. The expert coefficient of concordance (Kendall’s W) was 0.465 (P < 0.01), significantly higher than in the first round (0.398), indicating satisfactory consistency in expert opinions.
Then, a finalized POD prevention strategy was developed, consisting of four categories, 10 sections, and 27 items (Table 1).
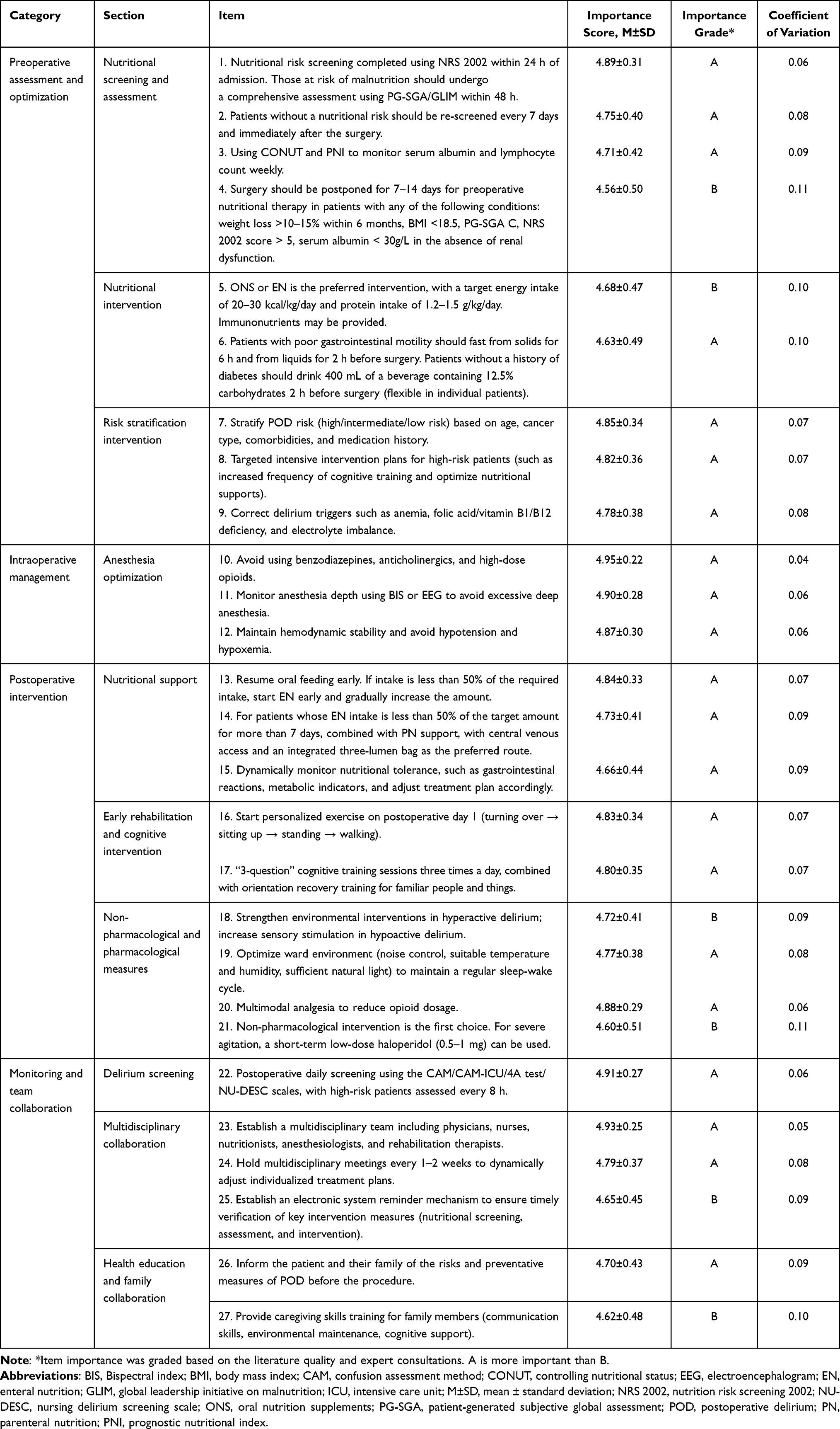 |
Table 1 Postoperative Delirium Prevention Strategy Developed After Literature Retrieval and Delphi Expert Consultation |
Discussion
In this study, we developed a POD prevention strategy for malnourished cancer patients by formulating clinical questions using the PIPOST framework, retrieving evidence based on the 6S model, and conducting Delphi expert consultations.
After formulating the research questions using the PIPOST framework, we conducted a top-down literature search guided by the 6S model. A total of 20 high-quality sources were included, encompassing various types of evidence such as clinical decision-making tools, guidelines, expert consensus documents, and systematic reviews, thereby ensuring the scientific rigor and comprehensiveness of the prevention strategy. Most of the core literature was rated as high-level evidence. Based on this evidence, we developed a preliminary questionnaire outlining the POD prevention strategy. Following two rounds of Delphi expert consultation, we finalized the strategy, which includes four categories, 10 sections, and 27 items.
Regarding preoperative nutritional assessment and optimization, and in accordance with the 2021 Clinical Nutrition Guidelines for Cancer Patients issued by the European Society for Clinical Nutrition and Metabolism,37 our POD prevention strategy mandates nutritional risk screening using the NRS 2002 within 24 h of admission for all preoperative cancer patients. For patients identified as being at high risk of malnutrition, a comprehensive nutritional assessment using the PG-SGA/GLIM criteria is required within 48 h.38
To enhance the effectiveness of subsequent interventions, these assessments should consider patient baseline characteristics, comorbidities, and planned chemoradiation regimens. Additionally, dynamic monitoring of nutrition-related biomarkers—such as serum albumin levels and lymphocyte counts—has been shown to reflect the efficacy of nutritional therapy and support real-time adjustments to intervention plans.39,40 Meanwhile, staff limitation and resource constrains to complete these necessary nutritional assessment and monitoring timely, along with other urgent clinical management, should be coordinated.
For patients at high risk of POD, correction of delirium-inducing factors and implementation of targeted interventions, such as intensive cognitive training, are recommended. The American Society for Parenteral and Enteral Nutrition recommends oral nutritional supplements or enteral nutrition (EN) as first-line therapies.41 Immunonutrition enriched with arginine and omega-3 fatty acids should also be incorporated into the nutritional plan to reduce POD incidence in cancer patients.42 The underlying mechanism is thought to involve immune modulation and suppression of the systemic inflammatory response. Additionally, preoperative intake of carbohydrate-containing beverages has been shown to significantly reduce preoperative hunger and anxiety, improve postoperative insulin sensitivity, and lower the risk of postoperative complications.43–45 Collectively, this body of evidence was integrated into the current POD prevention strategy. Whether this strategy integrating different nutritional supplements could reduce the incidence of POD requires further clinical validation.
Intraoperative anesthetic management was optimized in strict accordance with the European Society of Anaesthesiology (ESA) guidelines for POD prevention.46 The use of benzodiazepines and high-dose opioids is discouraged, as these agents may increase the risk of delirium by causing excessive central nervous system depression and disrupting neurotransmitter homeostasis.47 The guidelines recommend maintaining an appropriate depth of anesthesia, targeting a bispectral index (BIS) score of 40–60, and ensuring intraoperative hemodynamic stability—both of which have been shown to reduce the incidence of cerebral hypoperfusion, a key pathophysiological trigger for delirium.48,49 Moreover, low-dose dexmedetomidine (0.2–0.5 μg/kg/h) may be considered as an adjunct to reduce the risk of delirium, with careful monitoring for adverse effects such as bradycardia and hypotension.50 Further studies are required to identify the most appropriate agents to balance between adequate intraoperative anesthesia and minimized postoperative complications.
During postoperative management, nutritional support should be initiated early, with the enteral route preferred, to provide adequate metabolic support.38 Nutritional balance must be monitored continuously to enable data-driven adjustments to the feeding regimen and ensure that patients’ metabolic requirements are met. Postoperative physical rehabilitation—including early mobilization and exercise within 24 h, followed by gradual progression to the maximum tolerable intensity—has been shown to significantly improve cognitive function and physical recovery.51
Cognitive interventions, such as daily “three questions” training and orientation recovery exercises, have been shown to reduce POD incidence and are incorporated into our strategic plan.52 Non-pharmacological measures—including environmental optimization, frequent reorientation, sleep hygiene practices, and the use of sensory aids—serve as multi-component strategies to lower the risk of POD.53 Additionally, a multimodal analgesia approach helps reduce opioid-related cognitive impairment and aligns with the principles of enhanced recovery after surgery (ERAS).54 All of these evidence-based measures have been synthesized into our comprehensive POD prevention strategy. Further studies are required to determine how cognitive interventions, non-pharmacological measures, and multimodal analgesia can be effectively integrated to minimize the POD incidence.
In terms of monitoring and interdisciplinary collaboration, postoperative patients require daily delirium screening, with increased screening frequency for those at high risk. A multimodal screening approach—utilizing validated tools such as the Confusion Assessment Method (CAM) and the Nursing Delirium Screening Scale (Nu-DESC)—can enhance the sensitivity and specificity of delirium detection in postoperative cancer patients.55 Multiple studies have also demonstrated that a multidisciplinary collaboration model—comprising physicians, nurses, nutritionists, anesthesiologists, and rehabilitation therapists—facilitates the seamless delivery of nutritional support, anesthetic management, and rehabilitation interventions. This synergistic approach has been shown to significantly reduce the incidence of POD.56 Of course, the collaboration among different medical specialties and resource allocations should be optimized at the hospital level.
After developing a preliminary POD prevention strategy, we conducted two rounds of Delphi expert consultations. The expert authority coefficient reached 0.912, indicating a high level of reliability and consensus among a multidisciplinary panel.
Here, we developed a POD prevention strategy in malnutrition cancer patients. However, the clinical practice settings could have significant heterogeneity. Different environments, such as staff shortage and training, resource constraints, training requirements, and workflow, as well as patient characteristics, including cancer type and severity of malnutrition, could impact their nutrition needs and POD prevention approaches, challenging the clinical implementation of the proposed strategy. Further studies in patients in these different subgroups are required.
Limitations
This study had several limitations. It was conducted at a single medical institution with a relatively small sample size of experts, which may limit the generalizability of the findings. Additionally, our focus was limited to malnourished cancer patients, without considering the heterogeneity across different cancer types and varying degrees of malnutrition. Finally, we developed this POD preventive strategy but did not evaluate it in clinical patients. The efficacy of this strategy in patient short-term postoperative complications and long-term cognitive and functional status needs to be studied. Future multicenter, randomized clinical trials should be performed to test this newly developed strategy in hospitals with different surgical and oncology settings. Participating centers would implement this POD prevention strategy using standardized training and protocols. Outcomes, such as POD incidence, length of hospital stay, complications, and patient adherence to the intervention could be compared before and after implementation of this strategy. Multicenter collaboration would help to evaluate the feasibility, generalizability, and clinical efficacy of this POD prevention strategy across diverse healthcare settings, in order to develop more personalized preventive strategies tailored to specific malignancy types and levels of malnutrition.
Conclusions
We developed a comprehensive preliminary strategy for preventing POD in malnourished cancer patients by integrating an evidence-based approach with Delphi expert consultation. The final strategy comprises four categories, 10 sections, and 27 items. Future multicenter, randomized clinical trials are necessary to validate this POD prevention strategy and determine its feasibility and efficacy in various real-world settings.
Implications
A multidisciplinary collaboration and nutrition-delirium integrated intervention strategy can reduce POD and guide clinical staff to implement standardized, personalized care across pre-, intra- and postoperative phases. The strategy also provides a replicable evidence-based framework for healthcare institutions to optimize oncological surgical care, while highlighting the need for multicenter trials to enhance generalizability and refine stratified, cancer-specific POD prevention protocols.
Abbreviations
AGREE II, Appraisal of Guidelines for Research and Evaluation II; BIS, Bispectral index; CNKI, China National Knowledge Infrastructure; CAM, Confusion Assessment Method; ERAS, Enhanced recovery after surgery; ESA, European Society of Anaesthesiology; EN, Enteral nutrition; JBI, Joanna Briggs Institute; NRS, Nutrition Risk Screening; Nu-DESC, Nursing Delirium Screening Scale; POD, Postoperative delirium; PG-SGA, Patient-Generated Subjective Global Assessment.
Data Sharing Statement
Data are available on reasonable requests to the corresponding author.
Ethics Approval and Informed Consent
The study protocol was approved by the hospital’s ethics committee, and informed consent was obtained from all participants.
Acknowledgment
We thank Medjaden Inc. for scientific editing of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Traditional Chinese Medicine Science and Technology Program of Zhejiang Province (Grant no.: 2024ZL560); the Nursing Discipline Construction Research Project of the First Affiliated Hospital, Zhejiang University School of Medicine (Grant no.: 2023ZYHL45); Nursing Discipline Construction Research Project of The First Affiliated Hospital, Zhejiang University School of Medicine (Grant no.: 2024ZYHL46); Zhejiang Provincial Department of Education project (Grant no.: Y202454983).
Disclosure
We declare that we have no conflict of interest.
References
1. Thedim M, Vacas S. Postoperative delirium and the older adult: untangling the confusion. J Neurosurg Anesthesiol. 2024;36(3):184–11. doi:10.1097/ANA.0000000000000971
2. Bowman EML, Sweeney AM, McAuley DF, et al. Assessment and report of individual symptoms in studies of delirium in postoperative populations: a systematic review. Age Ageing. 2024;53(4). doi:10.1093/ageing/afae077
3. Martinez-Arnau FM, Buigues C, Perez-Ros P. Incidence of delirium in older people with cancer: systematic review and meta-analysis. Eur J Oncol Nurs. 2023;67:102457. doi:10.1016/j.ejon.2023.102457
4. Varpaei HA, Robbins LB, Farhadi K, Bender CM. Preoperative cognitive function as a risk factor of postoperative delirium in cancer surgeries: a systematic review and meta-analysis. J Surg Oncol. 2024;130(2):222–240. doi:10.1002/jso.27730
5. Papaconstantinou D, Frountzas M, Ruurda JP, et al. Risk factors and consequences of post-esophagectomy delirium: a systematic review and meta-analysis. Dis Esophagus. 2023;36(8). doi:10.1093/dote/doac103
6. Koyama R, Koyama R, Kuchiba A, et al. Medical cost of postoperative delirium after highly invasive cancer resection: a prospective cohort study. Jpn J Clin Oncol. 2025;55(9):985–990. doi:10.1093/jjco/hyaf085
7. Goldberg TE, Chen C, Wang Y, et al. Association of Delirium With Long-term Cognitive Decline: a Meta-analysis. JAMA Neurol. 2020;77(11):1373–1381. doi:10.1001/jamaneurol.2020.2273
8. Kunicki ZJ, Ngo LH, Marcantonio ER, et al. Six-year cognitive trajectory in older adults following major surgery and delirium. JAMA Intern Med. 2023;183(5):442–450. doi:10.1001/jamainternmed.2023.0144
9. Paternò DS, Via L, Putaggio A, et al. Perioperative neurocognitive disorders: a narrative review of pathophysiology, prevention, and management strategies. J Clin Med. 2026;15(3):1253. doi:10.3390/jcm15031253
10. Kim S, Choi E, Jung Y, Jang I. Postoperative delirium screening tools for post-anaesthetic adult patients in non-intensive care units: a systematic review and meta-analysis. J Clin Nurs. 2023;32(9–10):1691–1704. doi:10.1111/jocn.16157
11. Burton JK, Craig LE, Yong SQ, et al. Non-pharmacological interventions for preventing delirium in hospitalised non-ICU patients. Cochrane Database Syst Rev. 2021;7(7):Cd013307. doi:10.1002/14651858.CD013307.pub2
12. Toyota E, Sharma V. Pharmacotherapeutic approaches for the effective treatment of postoperative delirium: the state of play. Expert Rev Neurother. 2025;25(9):1061–1074. doi:10.1080/14737175.2025.2532075
13. Wang T, Huang X, Sun S, et al. Recent advances in the mechanisms of postoperative neurocognitive dysfunction: a narrative review. Biomedicines. 2025;13(1):115.
14. Hung KC, Chiu CC, Hsu CW, et al. Association of preoperative prognostic nutritional index with risk of postoperative delirium: a systematic review and meta-analysis. Front Med. 2022;9:1017000. doi:10.3389/fmed.2022.1017000
15. Mosharaf MP, Alam K, Gow J, Mahumud RA. Cytokines and inflammatory biomarkers and their association with post-operative delirium: a meta-analysis and systematic review. Sci Rep. 2025;15(1):7830. doi:10.1038/s41598-024-82992-6
16. Ceolin C, Papa MV, De Rui M, Devita M, Sergi G, Coin A. Micronutrient deficiency and its potential role in delirium onset in older adults: a systematic review. J Nutr Health Aging. 2023;27(9):785–790. doi:10.1007/s12603-023-1976-z
17. Liu J, Li J, Wang J, Zhang M, Han S, Du Y. Associated factors for postoperative delirium following major abdominal surgery: a systematic review and meta-analysis. Int J Geriatr Psychiatry. 2023;38(6):e5942. doi:10.1002/gps.5942
18. Moellmann HL, Alhammadi E, Boulghoudan S, et al. Risk of sarcopenia, frailty and malnutrition as predictors of postoperative delirium in surgery. BMC Geriatr. 2024;24(1):971. doi:10.1186/s12877-024-05566-1
19. Meza Monge K, Shapiro ALB, Coughlan C, et al. From bench to bedside: new frontiers in understanding and treating postoperative delirium. J Clin Med. 2025;14(23):8418. doi:10.3390/jcm14238418
20. Li W, Shi Q, Bai R, et al. Advances in research on the pathogenesis and signaling pathways associated with postoperative delirium (Review). Mol Med Rep. 2025;32(2):1–21. doi:10.3892/mmr.2025.13585
21. Hu F, Liu H, Liu X, et al. Nutritional status mediates the relationship between sarcopenia and cognitive impairment: findings from the WCHAT study. Aging Clin Exp Res. 2021;33(12):3215–3222. doi:10.1007/s40520-021-01883-2
22. Arends J. Malnutrition in cancer patients: causes, consequences and treatment options. Eur J Surg Oncol. 2024;50(5):107074. doi:10.1016/j.ejso.2023.107074
23. Dirjayanto VJ, Yiu DSM, Chen R, Fan KH. Nutrition in hepatocellular carcinoma: pathophysiological insights, impact, and implications for clinical practice. J Gastroenterol Hepatol. 2025;41(1):78–95. doi:10.1111/jgh.70186
24. Scannell C, Sullivan ES, Ryan A. Appetite for change - the need to revisit malnutrition screening and assessment in oncology. Proc Nutr Soc. 2026;1–10. doi:10.1017/S0029665126102195
25. Sabajo CR, Ten Cate DWG, van Grinsven S, et al. Nationwide implementation of multimodal prehabilitation and complications after colorectal cancer surgery. JAMA Surg. 2026. doi:10.1001/jamasurg.2026.1519
26. You X, Xu Y, Zhao J, et al. The association of geriatric nutritional risk and perioperative anesthesia-related adverse reactions in elderly patients with colorectal cancer-a prospective study. Transl Cancer Res. 2025;14(10):7419–7427. doi:10.21037/tcr-2025-1140
27. Lam AB, Sorensen L, Moore VA, et al. Perioperative supportive care interventions to enhance surgical outcomes for older adults with cancer: a systematic review. JCO Oncol Pract. 2025;21(8):1106–1117. doi:10.1200/OP-24-00762
28. Peden CJ, Miller TR, Deiner SG, Eckenhoff RG, Fleisher LA. Members of the perioperative brain health expert p. Improving perioperative brain health: an expert consensus review of key actions for the perioperative care team. Br J Anaesth. 2021;126(2):423–432. doi:10.1016/j.bja.2020.10.037
29. Chen MJ, Chen Y, Lin JQ, et al. Evidence summary of lifestyle interventions in adults with metabolic dysfunction-associated steatotic liver disease. Front Nutr. 2024;11:1421386. doi:10.3389/fnut.2024.1421386
30. Miao X, Fu Z, Luo X, et al. Evidence-based management strategies for endocrine complications after pituitary adenoma surgery. Ibrain. 2025;11(2):245–258. doi:10.1002/ibra.12156
31. Waltho D, Kaur MN, Haynes RB, Farrokhyar F, Thoma A. Users’ guide to the surgical literature: how to perform a high-quality literature search. Can J Surg. 2015;58(5):349–358. doi:10.1503/cjs.017314
32. Kendall S, Ryu M, Walsh C. Evidence-based medicine resources tool kit revisited. Can Fam Physician. 2017;63(6):490–492.
33. Xie F, Yao R, Liang L, et al. Evidence-based summary on medication adherence management for adult tuberculosis patients with multi-dimensional strategies and practice framework. J Eval Clin Pract. 2025;31(7):e70280. doi:10.1111/jep.70280
34. Zhang W, Zhang X, Han J, et al. Best evidence summary for monitoring and management of invasive arterial blood pressure in critically ill patients: an evidence-based review. Nurs Crit Care. 2025;30(6):e70215. doi:10.1111/nicc.70215
35. Hoffmann-Esser W, Siering U, Neugebauer EA, Brockhaus AC, Lampert U, Eikermann M. Guideline appraisal with AGREE II: systematic review of the current evidence on how users handle the 2 overall assessments. PLoS One. 2017;12(3):e0174831. doi:10.1371/journal.pone.0174831
36. Porritt K, Gomersall J, Lockwood C. JBI’s Systematic Reviews: study selection and critical appraisal. Am J Nurs. 2014;114(6):47–52. doi:10.1097/01.NAJ.0000450430.97383.64
37. Muscaritoli M, Arends J, Bachmann P, et al. ESPEN practical guideline: clinical nutrition in cancer. Clin Nutr. 2021;40(5):2898–2913. doi:10.1016/j.clnu.2021.02.005
38. Weimann A, Bezmarevic M, Braga M, et al. ESPEN guideline on clinical nutrition in surgery - Update 2025. Clin Nutr. 2025;53:222–261. doi:10.1016/j.clnu.2025.08.029
39. Li Y, Chen L, Yang X, et al. Dynamic association of serum albumin changes with inflammation, nutritional status and clinical outcomes: a secondary analysis of a large prospective observational cohort study. Eur J Med Res. 2025;30(1):679. doi:10.1186/s40001-025-02925-5
40. Alwarawrah Y, Kiernan K, MacIver NJ. Changes in nutritional status impact immune cell metabolism and function. Front Immunol. 2018;9:1055. doi:10.3389/fimmu.2018.01055
41. Compher C, Bingham AL, McCall M, et al. Guidelines for the provision of nutrition support therapy in the adult critically ill patient: the American Society for parenteral and enteral nutrition. JPEN J Parenter Enteral Nutr. 2022;46(1):12–41. doi:10.1002/jpen.2267
42. Matsui R, Sagawa M, Inaki N, Fukunaga T, Nunobe S. Impact of perioperative immunonutrition on postoperative outcomes in patients with upper gastrointestinal cancer: a systematic review and meta-analysis of randomized controlled trials. Nutrients. 2024;16(5):577. doi:10.3390/nu16050577
43. Kumar SM, Anandhi A, Sureshkumar S, et al. Effect of preoperative oral carbohydrate loading on postoperative insulin resistance, patient-perceived well-being, and surgical outcomes in elective colorectal surgery: a randomized controlled trial. J Gastrointest Surg. 2024;28(10):1654–1660. doi:10.1016/j.gassur.2024.07.027
44. Joshi GP, Abdelmalak BB, Weigel WA, et al. 2023 American society of anesthesiologists practice guidelines for preoperative fasting: carbohydrate-containing clear liquids with or without protein, chewing gum, and pediatric fasting duration-a modular update of the 2017 American society of anesthesiologists practice guidelines for preoperative fasting. Anesthesiology. 2023;138(2):132–151. doi:10.1097/ALN.0000000000004381
45. Ricci C, Ingaldi C, Alberici L, et al. Preoperative carbohydrate loading before elective abdominal surgery: a systematic review and network meta-analysis of Phase II/III randomized controlled trials. Clin Nutr. 2022;41(2):313–320. doi:10.1016/j.clnu.2021.12.016
46. Aldecoa C, Bettelli G, Bilotta F, et al. European society of anaesthesiology evidence-based and consensus-based guideline on postoperative delirium. Eur J Anaesthesiol. 2017;34(4):192–214. doi:10.1097/EJA.0000000000000594
47. Wang D, Huang C, Yang C. The heterogeneity of PND: perspectives from anesthetic sensitivity and resilience in the aging brain. Anesthesiol Perioper Sci. 2025;4:54–56. doi:10.1007/s44254-025-00144-z
48. Perez-Otal B, Aragon-Benedi C, Pascual-Bellosta A, et al. Neuromonitoring depth of anesthesia and its association with postoperative delirium. Sci Rep. 2022;12(1):12703. doi:10.1038/s41598-022-16466-y
49. Evered LA, Chan MTV, Han R, et al. Anaesthetic depth and delirium after major surgery: a randomised clinical trial. Br J Anaesth. 2021;127(5):704–712. doi:10.1016/j.bja.2021.07.021
50. Maagaard M, Barbateskovic M, Andersen-Ranberg NC, et al. Dexmedetomidine for the prevention of delirium in adults admitted to the intensive care unit or post-operative care unit: a systematic review of randomised clinical trials with meta-analysis and trial sequential analysis. Acta Anaesthesiol Scand. 2023;67(4):382–411. doi:10.1111/aas.14208
51. Patel BK, Wolfe KS, Patel SB, et al. Effect of early mobilisation on long-term cognitive impairment in critical illness in the USA: a randomised controlled trial. Lancet Respir Med. 2023;11(6):563–572. doi:10.1016/S2213-2600(22)00489-1
52. Collis N, Stanley PR, Sharpe DT, Batman PA. Rhinoscleroma: an interesting differential diagnosis. Br J Plast Surg. 1998;51(1):78–79. doi:10.1054/bjps.1997.1001
53. Hsiao CC, Lin CJ, Hasan F, et al. Comparative efficacy of nonpharmacological interventions for preventing postoperative delirium in hospitalized older adults: a systematic review and network meta-analysis. Age Ageing. 2025;54(9). doi:10.1093/ageing/afaf264
54. Huang L, Zhang T, Wang K, Chang B, Fu D, Chen X. Postoperative multimodal analgesia strategy for enhanced recovery after surgery in elderly colorectal cancer patients. Pain Ther. 2024;13(4):745–766. doi:10.1007/s40122-024-00619-0
55. Taberna M, Gil Moncayo F, Jane-Salas E, et al. The Multidisciplinary Team (MDT) approach and quality of care. Front Oncol. 2020;10:85. doi:10.3389/fonc.2020.00085
56. Igwe EO, Nealon J, Mohammed M, et al. Multi-disciplinary and pharmacological interventions to reduce post-operative delirium in elderly patients: a systematic review and meta-analysis. J Clin Anesth. 2020;67:110004. doi:10.1016/j.jclinane.2020.110004
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.