")
Back to Journals » International Journal of General Medicine » Volume 16
Development and Evaluation of the International Council of Cardiovascular Prevention and Rehabilitation (ICCPR) Program Certification for Low-Resource Settings
Authors Turk-Adawi KI, Elshaikh U, Contractor A, Hashmi FA, Thomas E, Raidah F, Grace SL
Received 27 May 2023
Accepted for publication 28 September 2023
Published 9 November 2023 Volume 2023:16 Pages 5199—5214
DOI https://doi.org/10.2147/IJGM.S423209
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Satish Chandrasekhar Nair
Karam I Turk-Adawi,1 Usra Elshaikh,1 Aashish Contractor,2 Farzana Amir Hashmi,3 Emma Thomas,4 Fabbiha Raidah,5 Sherry L Grace5,6
1Department of Public Health, College of Health Sciences, QU Health, Qatar University, Doha, Qatar; 2Rehabilitation and Sports Medicine, Sir H.N. Reliance Foundation Hospital, Mumbai, India; 3Preventive Cardiology and Rehabilitation, Tabba Heart Institute, Karachi, Pakistan; 4Centre for Online Health, Centre for Health Services Research, the University of Queensland, Brisbane, Queensland, Australia; 5Faculty of Health, York University, Toronto, Ontario, Canada; 6KITE - Toronto Rehabilitation Institute & Peter Munk Cardiac Centre, University Health Network, University of Toronto, Toronto, Ontario, Canada
Correspondence: Karam I Turk-Adawi, Department of Public Health, College of Health Sciences, Qatar University, P.O. Box: 2713, Doha, Qatar, Tel +974 4403 7508, Fax +974 4403 4801, Email [email protected]
Background: Cardiac rehabilitation (CR) is a proven model of secondary prevention, but new sites, providing quality care, are needed in low-resource settings. This study (1) described the development of International Council of Cardiovascular Prevention and Rehabilitation’s (ICCPR) Program Certification and (2a) tested its implementation, considering (b) appropriateness of quality standards for these settings.
Methods: The Steering Committee finalized 13 standards, requiring 70% be met. They are assessed initially through International CR Registry (ICRR) program survey and patient data; if Certification appears possible, a two-hour virtual site assessment is arranged to corroborate. Standard operating procedures for Assessor training were developed. A multi-method pilot study was then undertaken with a quantitative (description of quality indicators) and qualitative (focus groups on MS Teams) component. ICRR sites with post-program data by April 2022 were invited to participate. Two team members independently analyzed focus group transcripts, using a deductive-thematic approach with NVIVO.
Results: Five CR programs from the Eastern Mediterranean, South-East Asian and American regions participated. Upon application, with some data cleaning, initially four programs were eligible to proceed to virtual site assessment. Ultimately, all five programs were certified, each meeting a minimum of 12/13 standards (peak MET increase and program completion rate were not met by some centres). Four themes resulted from the two focus groups of 13 site data stewards: motivation and benefits (eg, international recognition, additional program resources), logistics (eg, communication, cost, site visit process), the standards and their assessment (eg, balance of rigor and feasibility), and suggestions for improvement (eg, website).
Conclusion: ICCPR’s Program Certification has been demonstrated to be feasible, rigorous, and acceptable. Standards are attainable in low-resource settings. Certified programs reap benefits including additional resources. This first international Certification is suitable for low-resource settings, to complement that from the American and European CR Societies.
Keywords: quality of care, Certification, cardiac rehabilitation, low- and middle-income countries, registries, cardiovascular diseases
Introduction
Cardiovascular diseases (CVD) continue to be a leading burden of mortality and morbidity, which is much higher in low- and middle-income countries (LMICs) than high-income ones.1 Eighty percent of CVD mortalities occur in LMICs, of which nearly 40% are classified as premature.1 Half of the world’s population lives in LMICs, where a disproportionate 57% of global cardiovascular deaths and 59% of disability-adjusted life years (DALY) losses occur.2
Most CVDs are either preventable or treatable if they occur,1 particularly with secondary prevention as delivered comprehensively in cardiac rehabilitation (CR).3 In LMICs, a lack of capacity to detect and treat these diseases contributes to the rapid emergence of advanced complications.1 Despite its affordability and cost-effectiveness,4 the International Council of Cardiovascular Prevention and Rehabilitation’s (ICCPR) global CR Audit revealed a gross dearth of CR capacity in LMICs, with only one CR “spot” available per year for every 66 incident ischemic heart disease patients (compared to 3.4 in high-income countries).5 Clearly, we need rapid increases in CR capacity in LMICs, a mission to which ICCPR is dedicated (https://globalcardiacrehab.com/The-Charter).
CR as delivered where available in LMICs is shown to be highly effective.6 However, there are differences in the nature of CR programs when compared to high-income countries (eg, dose, setting, comprehensiveness, multidisciplinary team), and they are more often privately funded.5 Therefore, a mechanism is needed to not only promote proliferation of CR in LMICs,7,8 but to support quality of these services. Indeed, greater quality of care can result in better patient outcomes.9 Therefore, given none was available, ICCPR developed Program Certification targeted to resource-poor settings. The objectives of this pilot study were to: (1) describe the development of ICCPR’s program certification, and (2a) test implementation of the certification, considering also (b) appropriateness of quality standards to programs in resource-poor settings.
Methods
This is a multi-method study, incorporating qualitative (focus groups with data stewards) and quantitative (description of standards at pilot sites) methods. It was approved by the Institutional Review Boards of both Hamad Corporation and Qatar University (Protocol No: MRC 02-20-359, QU-IRB 1518-EA/21), as well as York University (e2020-147).10
ICCPR Program Certification Development
ICCPR’s Program Certification was developed in a rigorous fashion, by a steering committee comprised 8 geographically and disciplinarily diverse CR experts, mostly from a low-resource setting, with input from the ICCPR community. It is a complement to their International Cardiac Rehabilitation Registry (ICRR), development and testing of which have been described elsewhere.11,12
The purpose of the Certification is to recognize CR programs in resource-poor settings,13 who meet a minimum quality standard with regard to program structure, processes, and patient outcomes.10 Program certification is a peer-reviewed process designed to assess CR programs for adherence to quality standards of the ICCPR, also recognized other professional societies. It was ultimately approved by ICCPR Executive and then Council in December 2021, including the quality standards, policies, procedures, and steering committee Terms of Reference (https://globalcardiacrehab.com/Program-Certification).
Development of the Program Certification was based on learnings from other CR certifications, chiefly the longest-running one by the British Association of Cardiovascular Prevention and Rehabilitation (BACPR; http://www.cardiacrehabilitation.org.uk/),14,15 as well as that of the American Association of Cardiovascular and Pulmonary Rehabilitation (AACVPR; https://www.aacvpr.org/Program-Certification),16,17 and the European Association of Preventive Cardiology (EAPC;https://www.escardio.org/Education/CareerDevelopment/Accreditation/EAPC-centre-accreditation).18 A review of quality indicators of the major CR societies informed decisions on the quality standards,3,8,18–22 with consideration of feasibility based on what is assessed in ICRR’s program survey and variable list.11 Proposed standards were then discussed by the Program Certification steering committee, for approval to pilot test.
ICCPR’s program certification is based on meeting 3 mandatory (ie, comprehensive program that offers at least initial assessment and structured exercise, cardiac emergencies policy in place and minimum peak MET increase from pre to post-program) and ≥70% overall of 13 quality indicators (eg, team comprised at least 2 different disciplines, assessment of tobacco use and blood pressure, at least 50% program completion rate, increase in quality of life post-program, as well as patient knowledge regarding medications, lipid control, diet and return to life roles), ascertained through analysis of the site’s data entered into the registry and as demonstrated in a 2-hour virtual site visit should results of the former warrant (Table 1). Application requirements are found elsewhere (https://globalcardiacrehab.com/Program-Certification), but include that at least one staff member holds ICCPR’s provider certification (CR Foundations Certification; https://globalcardiacrehab.com/Certification), that a minimum of 4 months of post-program data have been entered in the ICRR on ≥60 consecutive patients, and that the site is in good standing with ICRR data entry (ie, no completeness or other data quality issues).
 |
Table 1 ICCPR Program Certification Quality Standards, and Pilot Program Assessment Results, N=5 |
A standard operating procedure was created for the Secretary and Applicant Assessment Oversight co-chair to process received applications. If requirements are met, the Secretary downloads the site’s ICRR program survey,11 and patient data, and analyses the quality standards using developed SPSS syntax, entering results into the developed Applicant Assessment Form (Supplementary item 1). Then, based on whether there are further needed materials, and whether or not minimum standards are met, a standardized, templated email is sent to the site. Where a virtual site visit is warranted, arrangements for securing site assessors (preferably with language ability matching the first language spoken of patients at the applying site where possible) and date are made.
A standard operating procedure for training virtual site assessors was also developed and approved by the Steering Committee (Supplementary item 2). ICRR sub-committee and ICCPR Program Certification committee members are eligible to serve, and must sign a conflict of interest and confidentiality form (Supplementary Item 3; note potential conflicts must be declared for specific sites as well prior to any virtual site assessment). Potential site assessors are then sent details about the certification, arrangements are made to observe a virtual assessment, and then a one-on-one 45-minute video call is held with the Secretary and Assessment Oversight co-chair to ensure potential site assessor’s knowledge of: the purpose, standards, and requirements for Certification, as well as on preparation for and execution of site visits, handling various scenarios, and post-site visit processes.10
ICCPR Program Certification Process
As shown in Figure 1, registry-participating programs were invited to apply via email, attaching required documents. As per the standard operating procedures, the site was assessed as to meeting initial requirements, the 3 mandatory quality standards, and meeting a minimum of 9 of the 13 standards which are assessed in the program survey and patient data. Once processed by the Secretary and eligibility was confirmed by the Assessment Oversight co-chair, standard email correspondence was sent to each program to arrange the virtual site assessment (Supplementary item 4), with a reminder sent one week before. The Program Certification Secretary and at least 2 trained site assessors were in attendance at each virtual assessment and were provided the site-specific results from ICRR analysis in relation to the standards, as well as five random patient registry identification numbers for the site in advance of the online assessment.
 |
Figure 1 ICCPR Program Certification process. Abbreviation: ICCPR, International Council of Cardiovascular Prevention and Rehabilitation. Note: Reproduced from International Council of Cardiovascular Prevention and Rehabilitation (ICCPR). Copyright 2010. Available from https://globalcardiacrehab.com/Program-Certification. Accessed October 31, 2023.23 |
Assessments are held via an online web platform with videos on. Sites are asked to maintain the confidentiality of patient identity. As per the procedures on which site assessors are trained and which are shared with sites (Supplementary item 5), first sites are asked to show the centre overall and where the various components are delivered, as well as functional capacity testing. Team members are questioned one-by-one, who explain their clinical role in the program, to confirm the multidisciplinary expertise, and also show emergency procedure policies and answer questions about it. Next, the assessors confer with a patient where possible, to understand their care journey and education received. Finally, a review of random patient charts is undertaken, to confirm assessment of risk factors and program comprehensiveness.
Following the site assessment, assessors confer in camera about whether each standard was met, with comments notated. They then reach consensus on a decision to: (a) certify, (b) potentially certify with specific remediation, (c) deny certification, or (d) request more information prior to rendering a decision. This is all documented in the Applicant Assessment form, and decisions are shared with the Assessment Oversight co-chair for approval. Then, a standardized email communicating the decision is shared with the program (Supplementary item 6).
Where the decision is to certify, the program is provided a certificate (Supplementary item 7) and marketing toolkit. ICCPR shares the news via their social media channels and website. CR programs will be ICCPR-certified for 3 full calendar years from the date of certification issue.
Procedure
After all pilot sites completed the Certification consideration process as outlined above, in December 2022, focus groups were held with eligible participants. All participants provided written informed consent included for publication of anonymized responses. The focus groups were led by the last author (ICCPR Program Certification co-chair), and the first author (ICRR co-chair) and UE took notes and recorded non-verbal communication. Participants knew the co-chairs, and so to minimize bias all participants were asked not to respond in a socially desirable manner in case this familiarity would impact their responses, being reminded that the goal was to receive as much constructive feedback as possible to ensure the utmost utility of the Certification program.
The focus groups were held via MS Teams. To facilitate communication despite several different languages, live auto-transcription was enabled, all parties had their cameras on, and the focus group guide was shared with participants in advance and on the screen during the focus groups. Proceedings were video-recorded, again with consent.
Programs and Participants
Interested CR programs with ethics approval to participate in the registry and who met criteria to apply for program certification at the time of the pilot (April–November, 2022) were considered eligible. The posted program certification application fee was waived for pilot programs (see: https://globalcardiacrehab.com/Program-Certification). Quality standards from these programs were considered. All program staff from the centres involved in the certification process, including application, any communications, and/or the virtual site visit, were invited to the focus groups. Those who expressed difficulty with spoken English were invited to submit written input.
Measures
Each Program Certification quality standard is listed in Table 1, along with the source to assess them. Full explanations of each are available elsewhere (https://globalcardiacrehab.com/Program-Certification).
The focus group guide for the data stewards was developed by the ICRR co-chairs, and input was sought from the Steering Committee (Supplementary item 8). It assessed their perceptions of the application process, including communications, the virtual site visit and suggestions for improvement.
Analyses
A descriptive analysis of participating program characteristics was undertaken, using frequencies and percentages and means and standard deviations as applicable. Results for each quality standard were computed by site using descriptive statistics accordingly. Each quality standard was categorized as met or not met, and the percentage of met quality standards was computed by site. SPSS v28 was used for descriptive analyses.
The focus group recording transcripts were cleaned to be verbatim and anonymized by UE. A deductive-thematic approach was used for analysis of the transcripts by the senior author and UE using NVIVO 1.5.1,24 as outlined by Crabtree and Miller.25–27 Disagreements were reconciled with the first author. To ensure credibility, themes with sub-themes were then shared with all focus group participants to inquire whether they resonated, and requesting any input (ie, member checking).28 Each sub-theme was supported by illustrative quotations (note: where the respondent’s first language was other than English, some minor edits were made to increase clarity where needed).
Results
The first five ICRR-contributing programs across three World Health Organization regions agreed to be part of the pilot (Figure 2; 100% response rate). One was in a high-income country, but considered resource-poor given they are the sole program in the country. Program characteristics are shown in Table 2.
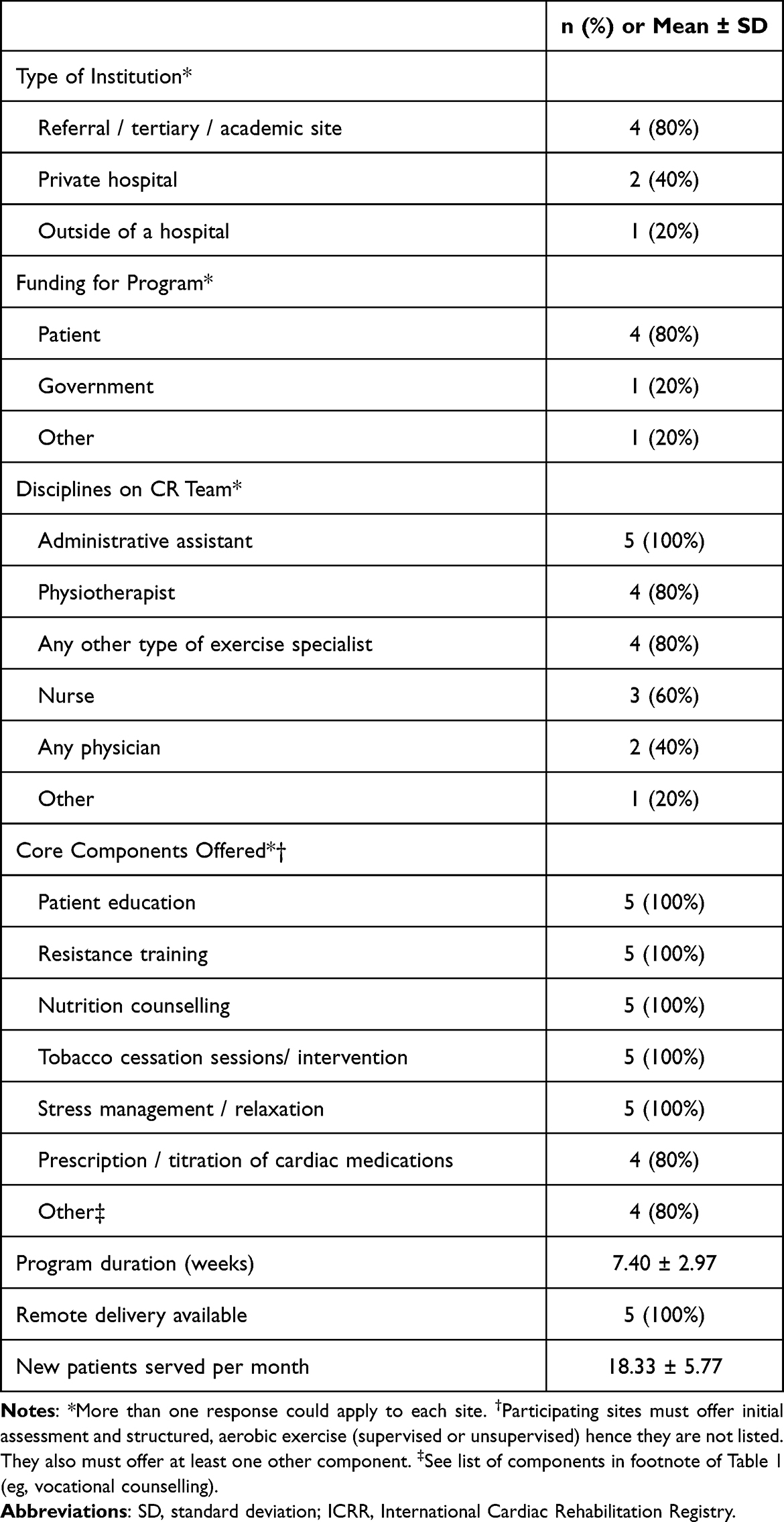 |
Table 2 Characteristics of ICRR-Participating Pilot Cardiac Rehabilitation (CR) Programs, N=5 |
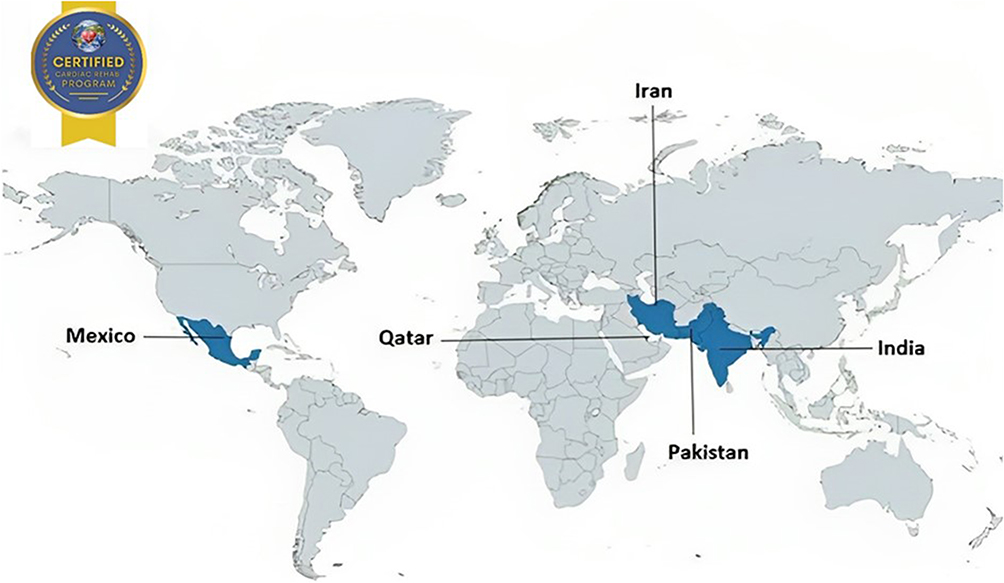 |
Figure 2 Map depicting cardiac rehabilitation programs which participated in pilot testing of ICCPR’s Program Certification. Abbreviation: ICCPR, International Council of Cardiovascular Prevention and Rehabilitation. Note: All sites were ultimately certified. |
Upon application, some centres had outstanding data quality issues that needed to be rectified prior to analysis of ICCPR quality standards. While site assessments are in English, there were some challenges securing site assessors with proficiency in the primary first language of patients served at participating programs. For one site visit, the site was not prepared at the beginning of the assessment, the centre was not viewable, and no patient had been arranged. There was also the experience of patient education materials not being in English and not fully viewable via the webcamera. At another point, it was difficult to view ICRR patient charts.
Results for quality standard assessment of each site are shown in Table 1. As shown, 4 of the 5 centres were eligible for virtual site visit based on the initial data analysis. One site did not meet the mandatory standard of a 0.5 Metabolic Equivalent of Task increase from pre- to post-program, yet met all 12 other standards. A meeting of the Steering Committee was held, and it was decided to invite the program to provide context for the finding but to allow them to proceed to virtual site assessment, given evidence of many other areas of program quality.
Following site assessments, the decision for all applying centres was to certify; results for each standard are shown in Table 1. Based on the findings of the pilot and discussion with the Steering Committee, only one change was made to the standards. For the peak METs standard (#7), rather than a 0.5 MET increase overall, it now specified that at least 75% of program completers meet this threshold, given the short duration of some programs due to out-of-pocket patient cost, and the complexity of patients in these settings (eg, heart failure, comorbidity).
Qualitative Perspectives on ICCPR’s Program Certification
Characteristics of the 13 focus group participants are shown in Table 3. Most attended the first focus group, but a second was held with 3 participants who had conflicts or needed extra time due to language barriers. There were 4 main themes resulting from analysis of all the qualitative data: (1) motivation and benefits, (2) logistics, (3) standards and their assessment, and (4) areas for improvement. Sub-themes and corresponding illustrative quotes are shown in Table 4.
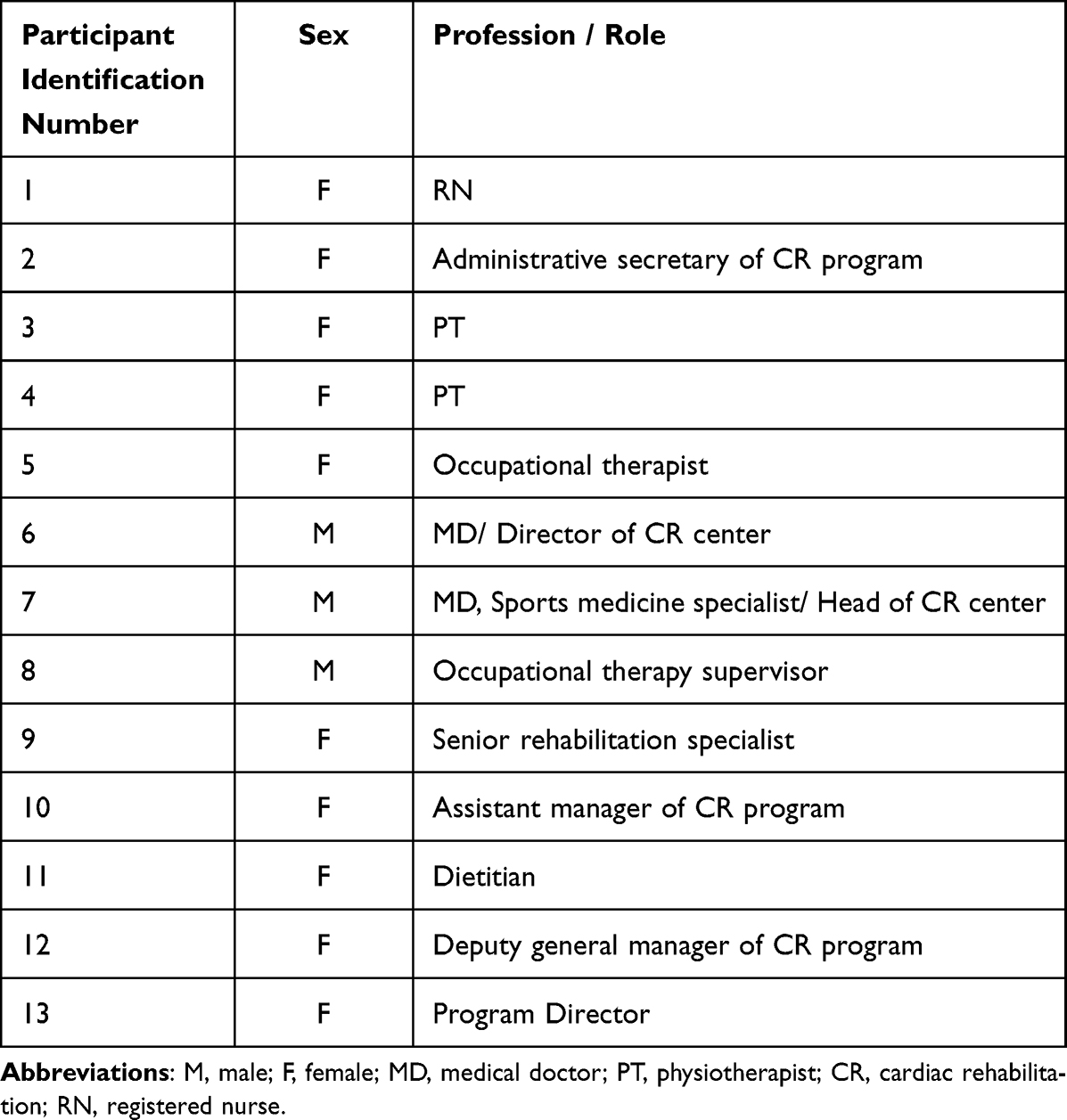 |
Table 3 Focus Group Participant Characteristics |
 |
Table 4 Four Major Themes Regarding ICCPR’s Program Certification, with Illustrative Quotes by Sub-Theme |
The first theme pertained to the motivations for programs to pursue ICCPR certification, and the benefits of doing so. The first sub-theme was to showcase their quality at an international calibre, and the pride associated with certification. The 13 standards are publicly available, thus making it clear what level of quality a program meets. One of the standards relates to a staff member having also completed ICCPR provider certification (ie, CR Foundations Certification; https://globalcardiacrehab.com/Certification), thus signalling the calibre of team members. The next sub-theme related to how the certification promoted the program with multiple stakeholders from patients, through institutional leadership and policy-makers. Recipients proudly displayed their certification on the walls of their gym, in welcome letters to new patients, in internal corporate communications, social media accounts and websites, and with national CR Societies. The final sub-theme related to how certification facilitated access to resources (eg, funding, space) and even service expansion.
The second major theme related to the logistics of applying, ensuring their registry data quality was sufficient for assessment, communication with ICCPR, and the site visit itself. For the first subtheme, communication with ICCPR was perceived as timely, unbiased, private, and helpful, despite language and time differences. Second, while pilot sites did not pay for certification in return for their involvement, they perceived the fees –including those for 3-year re-certification—to be reasonable. Note that one site noted challenges paying for the fee for one staff to complete ICCPR’s provider certification. Finally, the site visit was perceived as rigorous, comprehensive, transparent, objective and fair. While preparation for the site was daunting, the technical rehearsal instituted alleviated this. While judgment was necessarily involved, the tone was supportive, unbiased and confidential.
The third major theme pertained to the level of difficulty of the standards, considering the certification is geared towards resource-poor settings. For the first sub-theme, discussion centered on finding the right balance between ensuring the standards and process are feasible, but also needing to ensure rigor, to ensure quality and that certification is internationally- recognized as such. Participants spoke of the competing priorities; a lot of work was involved in entering data into the registry for several months to enable evaluation of candidacy for the virtual site assessment. Overall however, programs considered the effort worthwhile. The second sub-theme subsumed comments regarding the number of standards, whether the appropriate areas were covered, and the feasibility of the benchmarks in resource-poor settings. While there were some challenges regarding the lipid knowledge indicator as many patients do not get tested due to cost, and some discussion about potentially adding other standards, there was overall consensus that the standards were highly appropriate.
The final theme pertained to potential areas for improvement, with the first sub-theme relating to the website organization. The second and final sub-theme grouped “other” suggestions, including being mailed a hard copy of the certificate, and ensuring multiple forms of payment (eg, Paypal is not available in Pakistan).
Discussion
Herein, development of the first international CR program certification was described, followed by pilot testing in five low-resource sites, establishing its feasibility, rigor and acceptability. Results also establish the appropriateness and attainability of the 13 certification standards, with all sites ultimately achieving at least 12 of 13-well above the required 70%. Analysis of the focus groups showcased the potential benefits for certified programs, as well as corroborated the appropriateness of the standards for resource-poor settings while also recognizing some logistical challenges (eg, human resources). Finally, some areas for improvement were identified.
There have been several other studies on CR program quality assessment,19,29,30 and a few from the United Kingdom on CR program certification specifically,14,15 but all in high-resource settings to our knowledge. While program reports in the United States and Canada suggest sites are assessing quality, and those that elect to report similarly high quality, data from the BACPR’s audit across the whole population of CR programs show much more variation in quality, with many programs not meeting minimum standards.
Some barriers to CR program certification were identified during this research in the low-resource settings. The time to get approvals to participate in the registry was very lengthy, particularly in India. Securing time to enter registry data and the associated human resources required were considered challenging. Thus, it took considerable time to reach 60 patients to be eligible for Certification consideration. Also, preparation for the virtual site visit was considered daunting, to get the needed technical equipment ready.
There are three other CR program certifications available globally, also from well-reputed CR Societies, with BACPR’s not available outside of the United Kingdom. The AACVPR has certified 1338 programs as of November 2022, and the most-recently initiated EAPC certification has certified 11 as of January 2023. As a single-country association, the AACVPR certification is heavily based on American regulations, and costs more than ICCPR’s at $960USD. There is an annual application window (others are rolling); application is facilitated by registry participation, but a documentation-only option is available. The EAPC requires a program be operational at least two years and that one staff be a paid member of EAPC. Similar to AACVPR, many documents are to be provided, following the patient journey, considering clinical and emergency scenarios, as well as regarding staff qualifications, infrastructure and equipment. There is a nominal application fee, with certification then requiring €5700, which would be out of reach for programs in LMICs.
In addition to the above differences between these certifications, there are some important differences with ICCPRs. These certifications are in English; English is the primary language for ICCPR’s certification as well, but they do attempt to accommodate other languages through the use of translation of patient materials, securing bilingual virtual site assessors or interpreters where possible. There is a sliding scale of fees (for cost recovery only) to support ICCPR’s certification, which is based on country income classification and funding source (private or public); while pilot sites did not perceive the nominal fee would be a barrier to application, one site did have a challenge paying the lower $100USD fee for provider certification of one staff member even to be eligible to apply. Inherently, lack of resources in LMICs will be a challenge to achieving broad reach of ICCPR’s certification.
Based on the findings of this study, some changes and improvements were made to the Program Certification. Some clarifications were made to the website, and content broken down into sub-pages. Some photos from certified sites were added, as well as a figure depicting the overall process (Figure 1). A first report of the ICRR was created, highlighting successes of the Program Certification, and including testimonials from participating programs.
In addition, registry-participating programs can now be informed about the availability of Program Certification option from inception, because it has been formally launched subsequent to this study. There was one small change made to one of the program standards (#7). The application process was made more explicit through the use of an online survey (https://yorkufoh.ca1.qualtrics.com/jfe/form/SV_0JPMyfAeXiArpZk), where required documentation can be uploaded.
Moreover, some clarifications and details were added to the email templates for communication with applicant programs at each stage of the certification consideration process (see Supplementary items 4 and 6). For example, specifying two cameras on wheels may be needed and regarding languages of proficiency for the virtual site visit. The training and documentation to support site assessors during the virtual site visit were also improved, and a site visit recorded (with consent) for training purposes. A technical rehearsal step was added with the Secretary prior to the virtual site visit, to ensure for example stable internet connection, camera visibility, sound, and screen sharing.
In future, we will develop the policies and procedures for the three-year certification, which will not be reliant upon registry data entry. The Steering Committee is also contemplating a certification stream where registry participation is not required. We will also consider the logistics of mailing a token of certification to approved programs. Finally, quality improvement initiatives will be supported with interested registry-participating programs; resulting webinars will be posted to ICRR’s website.
Caution is warranted in interpreting these results. Given the limited sample size of a pilot study, results are not representative of all resource-poor CR programs, and thus generalizability of findings is unknown. Indeed, as outlined above, in comparison to data in the United Kingdom across the population of CR programs, there may have been a ceiling effect with some of the standards given the high-caliber of early ICRR-adopting programs. Second, with regard to measurement, as identified in the ICRR pilot study,31 there may be socially desirable responding on the part of patients to the registry knowledge items. Even though some sites were commenting about low levels of cholesterol testing due to out-of-pocket cost, still most participants reported they knew their “cholesterol level and how to control it” (ICRR data dictionary, variable 25). Third, efforts were made prior to interviews and throughout the pilot period of study to minimize impacts of social desirability of program staff, but this may have skewed results to be more positive. Efforts were also made to ensure interviewer neutrality, and coding for all qualitative data included a non-ICRR chair. Finally, the nature of the design precludes causal conclusions.
Conclusion
In conclusion, ICCPR’s first international CR Program Certification initiative has been developed, and pilot-tested in five centres in three regions. Results revealed that it may be feasible, rigorous and acceptable to programs in low-resource settings, and improvements were made based on results. Thus, in line with our aim of promoting and recognizing quality CR services where they are needed most, the Steering Committee is now poised to accept applications. While there are some logistical challenges to certification consideration in resource-poor settings, the many benefits of certification –including provision of more resources for delivery and expansion – have been established.
Abbreviations
CVD, Cardiovascular disease; LMICs, Low and middle-income countries; DALY, Disability adjusted life years; CR, Cardiac rehabilitation; ICCPR, International Council of Cardiovascular Prevention and Rehabilitation; ICRR, International Cardiac Rehabilitation Registry; BACPR, British Association for Cardiovascular Prevention and Rehabilitation; AACVPR, American Association of Cardiovascular and Pulmonary Rehabilitation; EAPC, European Association of Preventive Cardiology; METs; Metabolic equivalents of task; JCI, Joint Commission International.
Data Sharing Statement
The datasets generated and/or analysed during the current study are not publicly available. For the qualitative part, due to the small number of interviewees, participant identity could be identified. For the quantitative component, agreement to share data by participating sites in the ICRR was not obtained. Data are available from the corresponding author on reasonable request.
Acknowledgments
We are grateful to ICCPR’s former Secretary Ms. Carol Tran for implementation of the standard operating procedures with pilot programs. We are also grateful to the other members of ICCPR’s Program Certification steering committee, namely Drs. Jonathan Gallagher, Diann Gaalema, Won-Seok Kim, and Abraham Babu, as well as Mr. Jonathan David. We also thank the International Cardiac Rehabilitation Registry (ICRR) site data stewards for their efforts which under-propped this work, including notably Drs. Masoumeh Sadeghi, Jorge Antonio Lara Vargas, Theodoros Papasavvas, and Anjali Zende.
Funding
The International Cardiac Rehab Registry was co-funded by Qatar University, grant number (IRCC-2020-005), and York University (no grant number). E.E.T. is funded by a fellowship from the National Heart Foundation of Australia (105215). The findings achieved herein are solely the responsibility of the authors.
Disclosure
AC serves on the Program Certification Steering Committee and also put his program forward for certification consideration. To mitigate any conflict, assessment of his site’s data and the virtual site assessment were handled by other members of the committee without communication with AC until the decision had been reached. Two other authors were involved in this paper and their site was assessed, however they did not play a role in assessing their own site or have access to their certification data. Otherwise, the authors declare that they have no conflicts of interest.
References
1. Prabhakaran D, Anand S, Watkins D, et al. Cardiovascular, respiratory, and related disorders: key messages from disease control priorities, 3rd edition. Lancet. 2018;391(10126):1224–1236. doi:10.1016/S0140-6736(17)32471-6
2. Qureshi NQ, Mufarrih SH, Bloomfield GS, et al. Disparities in cardiovascular research output and disease outcomes among high-, middle- and low-income countries - an analysis of global cardiovascular publications over the last decade (2008–2017). Glob Heart. 2021;16(1):4. doi:10.5334/gh.815
3. Grace SL, Turk-Adawi KI, Contractor A, et al. Cardiac rehabilitation delivery model for low-resource settings. Heart. 2016;102(18):1449–1455. doi:10.1136/heartjnl-2015-309209
4. Shields GE, Wells A, Doherty P, Heagerty A, Buck D, Davies LM. Cost-effectiveness of cardiac rehabilitation: a systematic review. Heart. 2018;104(17):1403–1410. doi:10.1136/heartjnl-2017-312809
5. Pesah E, Turk-Adawi K, Supervia M, et al. Cardiac rehabilitation delivery in low/middle-income countries. Heart. 2019;105(23):1806–1812. doi:10.1136/heartjnl-2018-314486
6. Mamataz T, Uddin J, Ibn Alam S, Taylor RS, Pakosh M, Grace SL. Effects of cardiac rehabilitation in low-and middle-income countries: a systematic review and meta-analysis of randomised controlled trials. Prog Cardiovasc Dis. 2022;70:119–174. doi:10.1016/j.pcad.2021.07.004
7. Babu AS, Lopez-Jimenez F, Thomas RJ, et al. Advocacy for outpatient cardiac rehabilitation globally. BMC Health Serv Res. 2016;16(1):471. doi:10.1186/s12913-016-1658-1
8. Grace SL, Turk-Adawi KI, Contractor A, et al. Cardiac rehabilitation delivery model for low-resource settings: an international council of cardiovascular prevention and rehabilitation consensus statement. Prog Cardiovasc Dis. 2016;59(3):303–322. doi:10.1016/j.pcad.2016.08.004
9. Doyle C, Lennox L, Bell D. A systematic review of evidence on the links between patient experience and clinical safety and effectiveness. BMJ Open. 2013;3(1):e001570. doi:10.1136/bmjopen-2012-001570
10. Donabedian A. The quality of care. How can it be assessed? JAMA. 1988;260(12):1743–1748. doi:10.1001/jama.1988.03410120089033
11. Chowdhury MI, Turk-Adawi K, Babu AS, et al. Development of the international cardiac rehabilitation registry including variable selection and definition process. Glob Heart. 2022;17(1):1. doi:10.5334/gh.1091
12. Abukhadijah HJ, Turk-Adawi KI, Dewart N, Grace SL. Qualitative study measuring the usability of the international cardiac rehabilitation registry. BMJ Open. 2022;12(8):e064255. doi:10.1136/bmjopen-2022-064255
13. Van Zyl C, Badenhorst M, Hanekom S, Heine M. Unravelling ‘low-resource settings’: a systematic scoping review with qualitative content analysis. BMJ Glob Health. 2021;6(6):e005190. doi:10.1136/bmjgh-2021-005190
14. Furze G, Doherty PJ, Grant-Pearce C. Development of a UK national certification programme for cardiac rehabilitation. Br J Cardiol. 2016;23:102–105.
15. Doherty P, Salman A, Furze G, et al. Does cardiac rehabilitation meet minimum standards: an observational study using UK national audit? Open Heart. 2017;4(1):e000519. doi:10.1136/openhrt-2016-000519
16. Thomas RJ, Balady G, Banka G, et al. 2018 ACC/AHA clinical performance and quality measures for cardiac rehabilitation: a report of the American College of Cardiology/American Heart Association task force on performance measures. J Am Coll Cardiol. 2018;71(16):1814–1837. doi:10.1016/j.jacc.2018.01.004
17. Pack QR, Bauldoff G, Lichtman SW, et al. Prioritization development, and validation of American Association of cardiovascular and pulmonary rehabilitation performance measures. J Cardiopulm Rehabil Prev. 2018;38(4):208–214. doi:10.1097/HCR.0000000000000358
18. Abreu A, Frederix I, Dendale P, et al. Standardization and quality improvement of secondary prevention through cardiovascular rehabilitation programmes in Europe: the avenue towards EAPC accreditation programme: a position statement of the secondary prevention and rehabilitation section of the European Association of Preventive Cardiology (EAPC). Eur J Prev Cardiol. 2020;28:496–509.
19. Moghei M, Oh P, Chessex C, Grace SL. Cardiac rehabilitation quality improvement: a NARRATIVE REVIEW. J Cardiopulm Rehabil Prev. 2019;39(4):226–234. doi:10.1097/HCR.0000000000000396
20. Mehra VM, Gaalema DE, Pakosh M, Grace SL. Systematic review of cardiac rehabilitation guidelines: quality and scope. Eur J Prev Cardiol. 2020;27(9):912–928. doi:10.1177/2047487319878958
21. Aktaa S, Gencer B, Arbelo E, et al. European Society of cardiology quality indicators for cardiovascular disease prevention: developed by the working group for cardiovascular disease prevention quality indicators in collaboration with the European Association for preventive cardiology of the European Society of Cardiology. Eur J Prev Cardiol. 2022;29(7):1060–1071. doi:10.1093/eurjpc/zwab160
22. Zecchin R, Candelaria D, Ferry C, et al. Development of quality indicators for cardiac rehabilitation in Australia: a modified delphi method and pilot test. Heart Lung Circ. 2019;28(11):1622–1630. doi:10.1016/j.hlc.2018.08.004
23. International Council of Cardiovascular Prevention and Rehabilitation. ICCPR Program Certification. 2010. Available from https://globalcardiacrehab.com/Program-Certification.
24. Krippendorff K. Content Analysis: An Introduction to Its Methodology. Sage Publications; 2018.
25. Crabtree BF, Miller WL. Doing Qualitative Research. Sage Publications; 2022.
26. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis: striving to meet the trustworthiness criteria. Int J Qual Methods. 2017;16(1):1609406917733847. doi:10.1177/1609406917733847
27. Fereday J, Muir-Cochrane E. Demonstrating rigor using thematic analysis: a hybrid approach of inductive and deductive coding and theme development. Int J Qual Methods. 2006;5(1):80–92. doi:10.1177/160940690600500107
28. Hashimov E. Qualitative data analysis: a methods sourcebook and the coding manual for qualitative researchers. Tech Comm Quart. 2015;24(1):109–112. doi:10.1080/10572252.2015.975966
29. Astley CM, Beleigoli A, Tavella R, et al. Assessing the quality of cardiac rehabilitation programs by measuring adherence to the Australian quality indicators. BMC Health Serv Res. 2022;22(1):267. doi:10.1186/s12913-022-07667-2
30. Gallagher R, Ferry C, Candelaria D, Ladak L, Zecchin R. Evaluation of cardiac rehabilitation performance and initial benchmarks for Australia: an observational cross-state and territory snapshot study. Heart Lung Circ. 2020;29(9):1397–1404. doi:10.1016/j.hlc.2020.01.010
31. Turk-Adawi K, Ghisi GL, Tran C, et al. First report of the International Council of Cardiovascular Prevention and Rehabilitation’s registry (ICRR). Expert Rev Cardiovasc Ther. 2023;21(5):357–364. doi: 10.1080/14779072.2023.2199154
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.