Back to Journals » Infection and Drug Resistance » Volume 19
Development and Evaluation of a Duplex Lateral Flow Immunoassay for Rapid Detection of KPC and NDM Carbapenemases
Authors Zhang X, Zhang J, Shen MJ, An WH, Chen ZQ, Xue J ![]()
Received 30 November 2025
Accepted for publication 30 January 2026
Published 6 February 2026 Volume 2026:19 581873
DOI https://doi.org/10.2147/IDR.S581873
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Xian Zhang,1 Jie Zhang,2 Mei-Jing Shen,3 Wen-Hong An,1 Ze-Qiong Chen,1 Jian Xue2
1Department of Hospital Infection, The Third Affiliated Hospital of Zunyi Medical University, The First People’s Hospital of Zunyi, Zunyi, Guizhou, 563002, People’s Republic of China; 2Department of Health Management, Zunyi Medical and Pharmaceutical College, Zunyi, Guizhou, 563006, People’s Republic of China; 3Department of Clinical Laboratory, The Third Affiliated Hospital of Zunyi Medical University, The First People’s Hospital of Zunyi, Zunyi, Guizhou, 563002, People’s Republic of China
Correspondence: Jian Xue, Department of Health Management, Zunyi Medical and Pharmaceutical College, Pingan Road, Zunyi, Guizhou, 563006, People’s Republic of China, Email [email protected]
Background: Carbapenem-resistant Enterobacterales represent a critical global health challenge, with KPC and NDM being the most prevalent carbapenemase families. Rapid and reliable detection tools are essential for guiding infection control and antimicrobial stewardship, particularly in resource-limited settings.
Methods: A lateral flow immunoassay (LFIA) strip was developed for simultaneous detection of KPC and NDM carbapenemases. Monoclonal antibody pairs were screened and assay parameters were optimized to improve analytical performance. Analytical evaluation was performed using recombinant proteins. Clinical evaluation was conducted using 12 non-duplicate clinical Klebsiella pneumoniae (K. pneumoniae) isolates, with blaKPC/blaNDM confirmed by PCR and whole-genome sequencing (WGS).
Results: The LFIA achieved limits of detection of 0.5 ng/mL for KPC and 0.1 ng/mL for NDM using recombinant proteins. No cross-reactivity was observed with other carbapenemases (OXA-48, VIM, IMP). In the clinical K. pneumoniae set, LFIA results showed 100% concordance with the PCR/WGS reference. Test results were visually interpretable within 15 minutes without specialized instrumentation.
Conclusion: This duplex LFIA provides rapid, instrument-free visual screening for KPC and NDM carbapenemases in cultured isolates, supporting routine laboratory screening and workflow decisions. Larger multi-center studies across diverse Enterobacterales species and carbapenemase variants will further define its broader clinical performance.
Keywords: lateral flow immunoassay, KPC, NDM, carbapenem-resistant Enterobacterales
Introduction
The global rise of antimicrobial resistance, largely driven by the misuse and overuse of antibiotics, has emerged as one of the most pressing public health challenges of the 21st century.1 Among resistant pathogens, carbapenem-resistant Enterobacterales (CRE) are of particular concern, as they are frequently associated with healthcare-associated infections and are linked to high morbidity and mortality rates.2 Due to its rapid dissemination and limited treatment options, the World Health Organization has designated CRE as a critical priority pathogen.3
The predominant mechanism of resistance in CRE is the production of carbapenemases, which hydrolyze carbapenems and thereby compromise the last line of defense against multidrug-resistant bacterial infections.4 While the distribution of carbapenemase types varies geographically, KPC and NDM have been reported as the most prevalent globally, and are also the dominant enzyme types in China.5–7 Therefore, accurate and rapid identification of these carbapenemases is essential for timely infection control interventions and guiding therapeutic strategies. In routine clinical microbiology, carbapenemase detection relies on a combination of phenotypic assays (eg, the modified Hodge test, Carba NP, or the EDTA synergy test), immunochromatographic rapid tests, and molecular approaches (eg, targeted PCR), with whole-genome sequencing (WGS) increasingly used as a high-resolution reference for confirmation and genetic characterization. However, phenotypic methods often require additional incubation and may show limited specificity, and their performance can be influenced by enzyme expression levels and co-existing resistance mechanisms.8 In contrast, molecular assays, including PCR and WGS, provide high accuracy and detailed genetic insights but require specialized equipment, higher costs, and considerable technical expertise, which can limit accessibility in routine diagnostics, particularly in resource-limited settings.8,9 Against this background, lateral flow immunoassay (LFIA) offers a practical, instrument-free option that can be performed with minimal training, enabling rapid point-of-care screening for major carbapenemase families.10–12 Collectively, these considerations highlight the need for an affordable duplex LFIA capable of detecting KPC and NDM in a single test, particularly for routine use in resource-limited settings.
In this study, we developed and evaluated a colloidal gold-based LFIA for the simultaneous detection of KPC and NDM carbapenemases. By systematically optimizing antibody selection and assay conditions, we assessed its analytical performance and clinical applicability, aiming to provide a rapid, cost-effective, and user-friendly tool for point-of-care detection of carbapenemase-producing bacteria.
Methodology
Chemicals and Materials
Recombinant KPC antigen (4.6 mg/mL), recombinant NDM antigen (2.0 mg/mL), anti-KPC monoclonal antibody, anti-NDM monoclonal antibody, and goat anti-mouse IgG antibody were purchased from Biocare Diagnostics Ltd. (Zhuhai, China). Chloroauric acid (HAuCl4), bovine serum albumin (BSA), casein, Tween-20, and Triton X-100 were obtained from Sigma-Aldrich (St. Louis, MO, USA). Sodium citrate, sucrose, trehalose, polyethylene glycol 4000 (PEG4000), potassium carbonate (K2CO3), polyvinylpyrrolidone (PVP-400), potassium chloride (KCl), and disodium hydrogen phosphate (Na2HPO4) were supplied by Sinopharm Chemical Reagent Co., Ltd. (Shanghai, China).
Preparation of Colloidal Gold-Antibody Probes
To prepare the gold-antibody conjugate, 5 mL of colloidal gold solution was adjusted to pH 8.0. An appropriate amount of antibody was diluted in ultrapure water and added dropwise to the gold solution under gentle stirring, to achieve a final antibody concentration of 25 μg/mL.13 The mixture was incubated at room temperature for 20 minutes. After incubation, 50 μL of 10% (w/v) BSA solution was added to block nonspecific binding sites. The conjugated solution was transferred to nuclease-free centrifuge tubes and centrifuged at 10,000 rpm for 10 minutes. After centrifugation, the pellet was resuspended in resuspension buffer at 10% of the original volume to obtain the gold-antibody conjugate for subsequent use. The suspension was treated in an ultrasonic water bath to ensure complete dispersion. The resulting colloidal gold-antibody probes were stored for subsequent use in LFIA assembly. Gold nanoparticle size and antibody labeling parameters (conjugation pH and antibody loading) were empirically optimized during assay development (Supplementary Text, Supplementary Table S1 and Supplementary Figures S1–S5).
Screening and Optimization of Antibody Pairs
To identify the optimal monoclonal antibody combinations for KPC and NDM carbapenemase detection, pairwise screening experiments were performed using colloidal gold-based LFIA. For KPC, five anti-KPC monoclonal antibodies (10E1, 10D4, 9A9, 8G12, and 1D7) were tested in 20 different combinations. Recombinant KPC antigen was diluted to 100 ng/mL, 10 ng/mL, and 1 ng/mL in phosphate-buffered saline (PBS) and applied to each pair. The screening criteria included signal intensity across concentrations, background noise, and reproducibility.
For NDM, four monoclonal antibodies (17E6, 9E7, 17D2, and 12D4) were evaluated in 12 pairwise combinations using recombinant NDM antigen at concentrations of 200 ng/mL, 20 ng/mL, and 2 ng/mL. Each combination was tested in parallel with a PBS negative control. The antibody pairs that provided the strongest and most consistent signals with minimal background were selected for LFIA fabrication.
Assembly and Working Principle of The LFIA Strips
As illustrated in Figure 1, the LFIA strip was composed of four components: a sample pad, a conjugate pad, a nitrocellulose (NC) membrane, and an absorbent pad, all mounted sequentially on a polyvinyl chloride (PVC) backing card.14 Colloidal gold nanoparticles (40 nm) were conjugated at pH 8.0 with either anti-KPC or anti-NDM monoclonal antibodies (25 µg/mL), blocked with BSA, centrifuged, and resuspended in buffer before being dispensed onto the glass fiber conjugate pad. Capture antibodies were striped on the NC membrane as follows: anti-KPC at test line 1 (T1), anti-NDM at test line 2 (T2), and goat anti-mouse IgG at the control line, each at a concentration of 1.2 mg/mL. The coating concentrations of capture antibodies on the test lines (T1 and T2) and goat anti-mouse IgG on the control line were optimized to maximize signal intensity and minimize background (Supplementary Tables S2–S4). Following assembly, strips were dried (37 °C, 2 h) and stored with desiccant at 4 °C. Upon sample application, if KPC or NDM carbapenemase was present, the corresponding immune complexes formed with the gold-labeled antibodies migrated along the strip and were captured at the test lines, producing visible red-purple bands. The control line served to verify proper sample migration. Results were interpreted visually within 15 min.
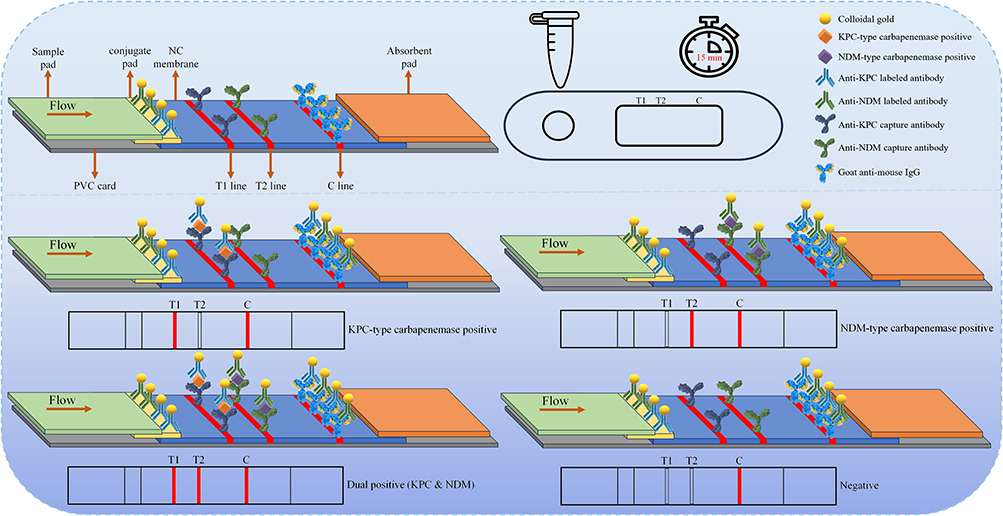 |
Figure 1 The preparation process and principle of LFIA strips. |
Sample Preparation
Twelve non-duplicate clinical Klebsiella pneumoniae (K. pneumoniae) isolates were obtained from leftover bacterial isolates generated during routine diagnostic testing in the Clinical Microbiology Laboratory of The First People’s Hospital of Zunyi in 2021. To minimize duplication, only one isolate per patient episode was included and duplicate isolates from the same patient were excluded. The presence of blaKPC and blaNDM was confirmed by PCR and further verified by whole-genome sequencing (WGS) as the reference method.7,15 To supplement the evaluation of NDM detection beyond K. pneumoniae, eight non-Klebsiella Enterobacterales isolates carrying blaNDM were also tested, including four Escherichia coli carrying blaNDM-5 and four Enterobacter cloacae complex isolates carrying blaNDM-1. For these supplementary isolates, blaNDM was also confirmed by WGS.
For LFIA testing, each isolate was subcultured on 5% sheep blood agar plates at 37 °C for 48 hours. Briefly, 3–5 colonies were picked and suspended in 500 μL PBS, pH 7.4, followed by thorough vortexing. A 100 μL aliquot of the suspension was applied directly to the sample pad of the LFIA strip. After incubation at room temperature for 15 minutes, results were visually interpreted based on the appearance of colored lines in the control and test regions.
Determination of Analytical Sensitivity
The sensitivity of the LFIA strips was evaluated using serial dilutions of recombinant KPC and NDM antigens in PBS. The antigen concentrations tested were 10, 5, 1, 0.5, and 0.1 ng/mL for KPC, and 5, 1, 0.5, 0.1, and 0.05 ng/mL for NDM. Each concentration was tested in triplicate.
Evaluation of Specificity, Reproducibility, and Stability
The specificity of the LFIA strips was evaluated using reference strains producing KPC, NDM, OXA-48, VIM, and IMP carbapenemases, along with a non-carbapenemase-producing K. pneumoniae strain as a negative control. Each strain was tested according to the standard LFIA procedure, and results were visually interpreted after 15 minutes.
Reproducibility was assessed by comparing results obtained from three independently prepared batches (inter-batch) and repeated tests within the same batch (intra-batch).
For stability evaluation, the LFIA strips were sealed with desiccant and stored at room temperature for up to six months. Their performance was checked at regular intervals using recombinant KPC and NDM antigens to determine whether signal intensity and background remained consistent.
Results
Screening and Optimization of Antibody Pairs
Screening results demonstrated that, among all combinations tested, the antibody pair 10E1 (capture) and 9A9 (label) for KPC detection yielded the highest signal intensity with no visible background in the negative control (Table 1). Similarly, for NDM detection, the 17D2 (capture) and 9E7 (label) combination exhibited the strongest and most stable signal performance, maintaining visible detection down to 2 ng/mL without cross-reactivity (Table 2). Based on these results, the 10E1/9A9 and 17D2/9E7 antibody pairs were selected as the optimal combinations for constructing the LFIA strips targeting KPC and NDM carbapenemases, respectively.
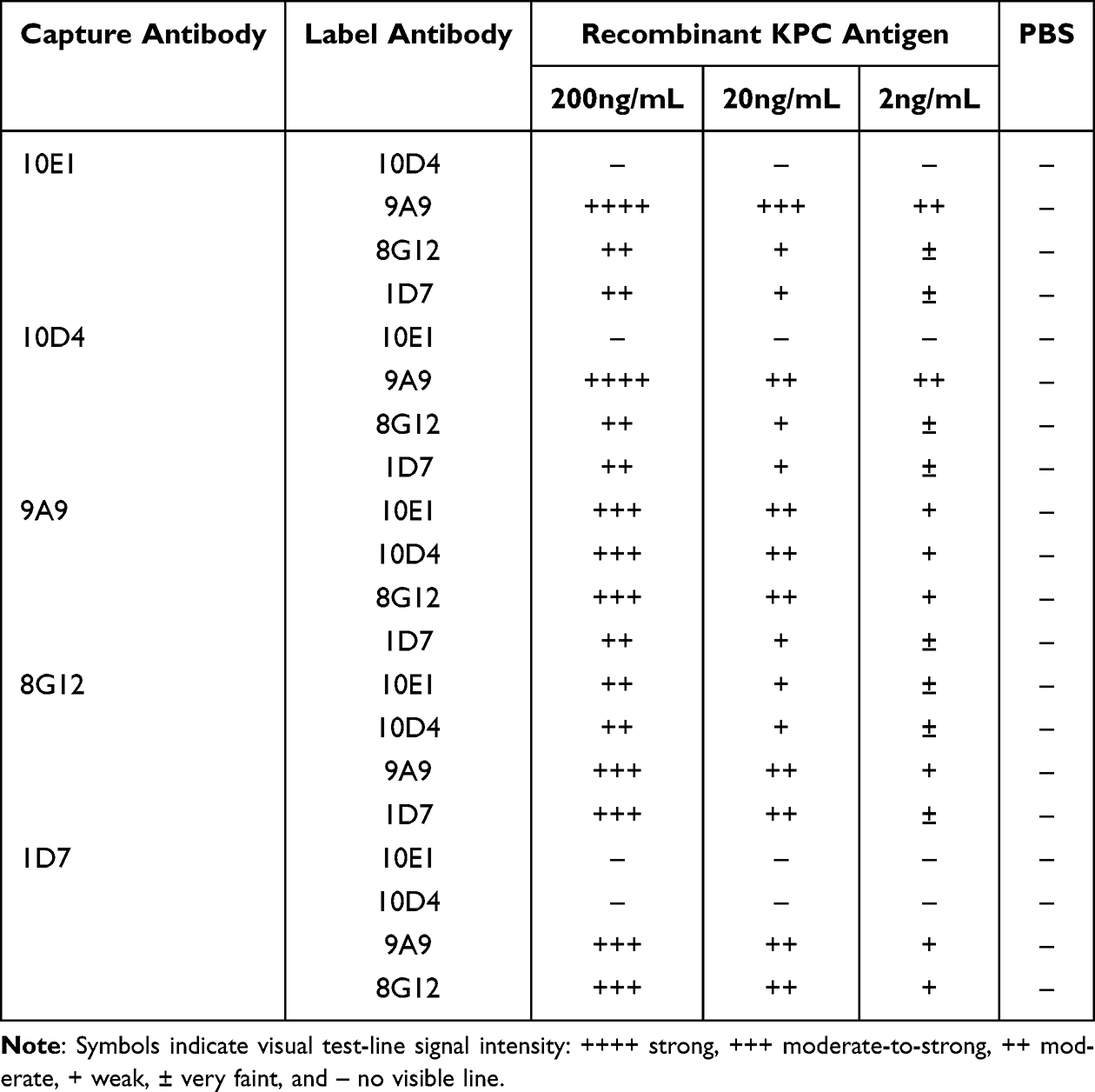 |
Table 1 Screening Results of Antibody Pairs for KPC Detection |
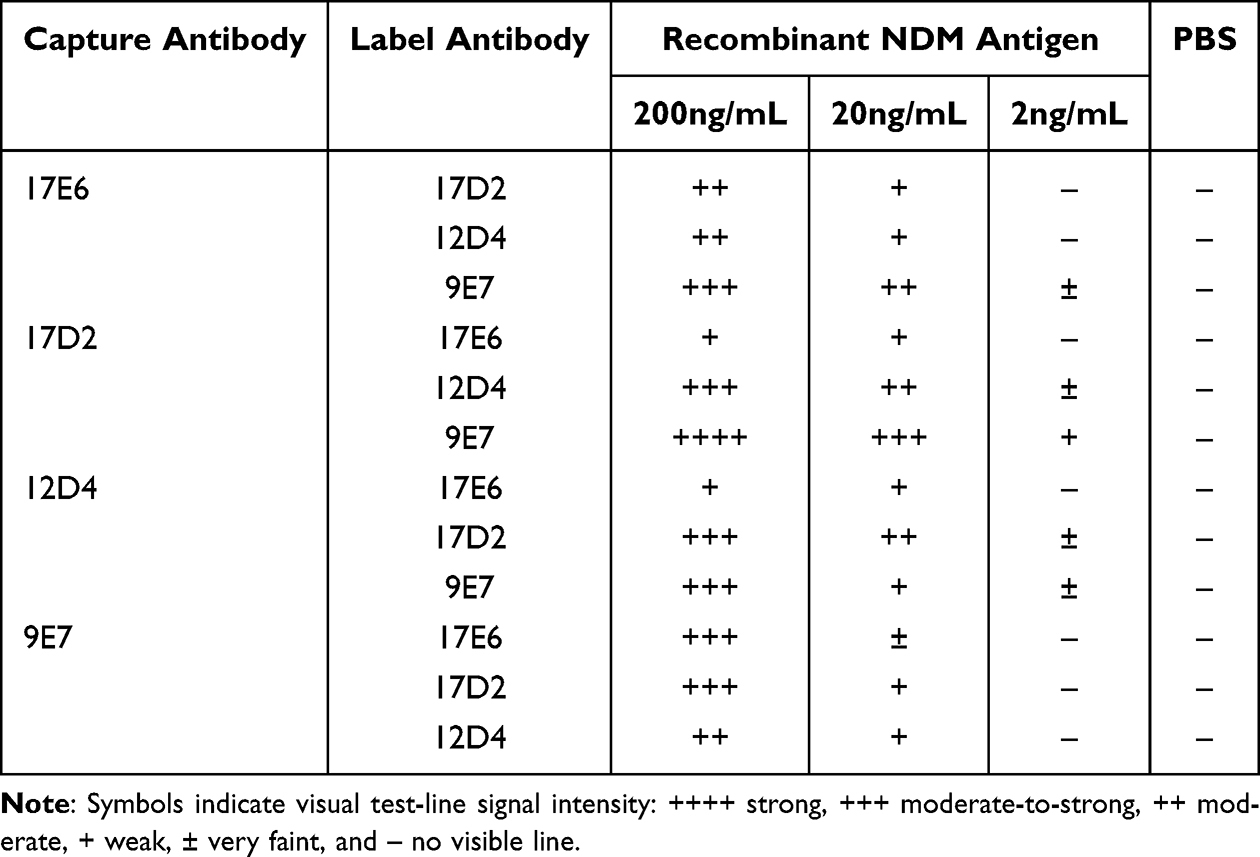 |
Table 2 Screening Results of Antibody Pairs for NDM Detection |
Sensitivity of The LFIA Strips
The analytical sensitivity of the optimized LFIA was evaluated using serial dilutions of recombinant KPC and NDM antigens. As shown in Table 3, for KPC detection, a faint but visible test line was observed at 0.5 ng/mL, while at 0.1 ng/mL, the signal was inconsistent. Thus, the limit of detection (LOD) for the KPC LFIA strip was defined as 0.5 ng/mL. The corresponding visual results from one of the three parallel replicates are presented in Figure 2.
 |
Table 3 KPC LFIA Strip Sensitivity Test Results |
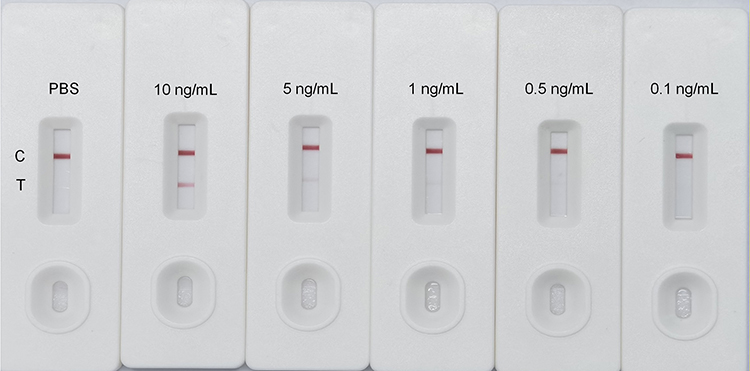 |
Figure 2 Analytical sensitivity of the KPC-LFIA using recombinant KPC antigen (10, 5, 1, 0.5, and 0.1 ng/mL), with PBS as a negative control; a visible control line (C) indicates a valid test, and a visible test line (T) indicates KPC positivity. |
As shown in Table 4, for NDM detection, the test line was clearly visible at 0.1 ng/mL in all three replicates, indicating consistent positive results. However, at 0.05 ng/mL, the signal was not consistently detected. Therefore, the LOD for the NDM LFIA strip was determined to be 0.1 ng/mL. Figure 3 displays the strip results from one representative replicate among the three parallel tests.
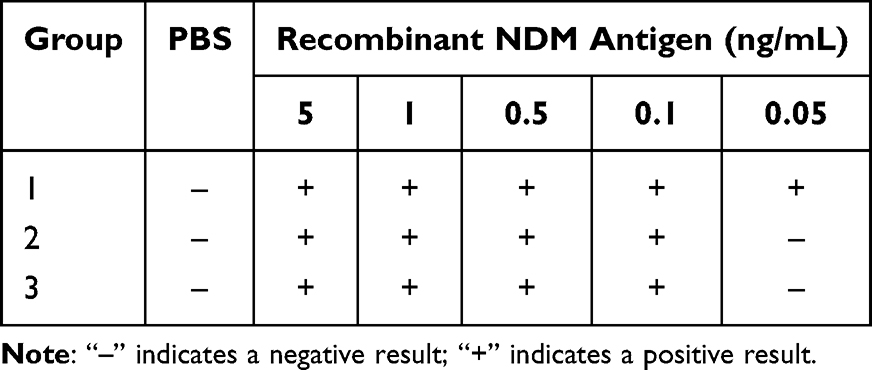 |
Table 4 NDM LFIA Strip Sensitivity Test Results |
 |
Figure 3 Analytical sensitivity of the NDM-LFIA using recombinant NDM antigen (5, 1, 0.5, 0.1 and 0.05 ng/mL), with PBS as a negative control; a visible control line (C) indicates a valid test, and a visible test line (T) indicates NDM positivity. |
Specificity of the LFIA Strips
To evaluate the specificity of the LFIA strips, six well-characterized bacterial strains were selected, including five carbapenemase-producing strains and one negative control strain. These included: an NDM-producing strain (K. pneumoniae ATCC BAA-2146), a KPC-producing strain (K. pneumoniae ATCC BAA-1705), an OXA-48-producing strain (K. pneumoniae NCTC 13442), a VIM-producing strain (K. pneumoniae NCTC 13439), and an IMP-producing strain (Escherichia coli NCTC 13476). A non-carbapenemase-producing strain (K. pneumoniae ATCC BAA-1706) was included as a negative control. Each strain was tested using the standard LFIA procedure described above, and results were visually interpreted after 15 minutes.
As shown in Table 5, Figures 4 and 5, the KPC strip produced positive signals exclusively with KPC-producing strains, whereas the NDM strip was positive only with NDM-producing strains. No cross-reactivity was observed with OXA-48-, VIM-, IMP-producing strains or the negative control strain. These findings confirm that the LFIA strips possess high analytical specificity for their respective target carbapenemases.
 |
Table 5 Specificity Evaluation Results of the KPC and NDM LFIA Strips |
 |
Figure 4 Analytical specificity of the KPC-LFIA evaluated using carbapenemase-producing reference strains (NDM, KPC, OXA-48, VIM, and IMP) and a non-carbapenemase control (None); a visible control line (C) indicates a valid test, and a visible test line (T) indicates KPC positivity. |
 |
Figure 5 Analytical specificity of the NDM-LFIA evaluated using carbapenemase-producing reference strains (NDM, KPC, OXA-48, VIM, and IMP) and a non-carbapenemase control (None); a visible control line (C) indicates a valid test, and a visible test line (T) indicates NDM positivity. |
Reproducibility and Stability of the LFIA Strips
LFIA strips from three independent batches showed consistent detection results for both KPC and NDM antigens, confirming good reproducibility. Repeated tests within the same batch also yielded uniform results with no signal variation.
During six months of storage under ambient conditions, the strips maintained stable performance, showing no decline in signal intensity or increase in background. These results demonstrate that the developed LFIA strips exhibit excellent reproducibility and storage stability, supporting their suitability for routine use.
Practical Application of the LFIA Strips
To evaluate the practical performance of the developed LFIA strips, a panel of 12 clinical K. pneumoniae isolates was tested. These strains had been previously characterized by WGS.7 Among them, 4 were confirmed to produce KPC carbapenemase only, 4 produced NDM carbapenemase only, and 4 co-produced both KPC and NDM carbapenemase. Bacterial suspensions were prepared according to the standard protocol and applied to the LFIA strips. Results were visually interpreted within 15 minutes. The strips correctly identified all target enzymes: KPC-producing strains yielded a positive band on the KPC test line, NDM-producing strains on the NDM test line, and dual producers showed positive signals on both test lines. As shown in Figure 6, the LFIA results were fully concordant with WGS based identification, demonstrating 100% agreement. In addition, the assay showed positive NDM test-line signals in all eight non-Klebsiella NDM-producing Enterobacterales isolates included for supplementary evaluation (Supplementary Figure S6).
 |
Figure 6 Representative LFIA strip results in isolate testing. Strips were numbered for clarity: 1, negative control; 2–5, dual-positive (C, T1 and T2); 6–9, KPC-positive (C and T1); 10–13, NDM-positive (C and T2). C, control line; T1, KPC test line; T2, NDM test line. |
These findings confirm that the developed LFIA strips provide a rapid, reliable, and cost-effective approach for routine screening and point-of-care diagnostics in clinical microbiology laboratories, particularly in resource-limited settings.
Discussion
Compared with existing diagnostic approaches, the LFIA developed in this study offers distinct advantages in terms of simplicity, speed, and accessibility. These features make LFIA especially suitable not only for clinical microbiology laboratories, but also for decentralized scenarios such as smaller hospitals, outbreak investigations, and surveillance in resource-limited environments. In this context, the present LFIA is intended as an affordable, preliminary screening tool for cultured isolates in areas with similar resistance epidemiology, while negative results should be further confirmed by phenotypic or molecular testing according to local laboratory policies.
For routine implementation, assay design should also balance analytical performance with manufacturability and cost. Accordingly, a simplified duplex strip design targeting KPC and NDM was adopted. In large-scale production, manufacturing yield is a key determinant of overall cost. Commercial carbapenemase detection kits that simultaneously screen for five major carbapenemase types in CRE (KPC, NDM, OXA-48, VIM, IMP) are relatively expensive, as their complex multi-line structures increase material consumption, preparation steps, and the risk of lower manufacturing yield. In addition, increasing the number of test lines will shorten the distance between adjacent lines, leading to fluidic interference, signal bleed-over, and a higher likelihood of cross-reactivity, which ultimately increases the risk of result misinterpretation.16 In contrast, selectively targeting the most prevalent carbapenemase types in a given region, such as KPC and NDM in China, allows for reducing the number of detection lines without compromising diagnostic efficacy. The two-line configuration used in this study was therefore a fit-for-purpose and cost-saving design choice that simplifies strip structure, decreases antibody and material consumption, and lowers production and training costs while maintaining strong analytical performance. This streamlined approach minimizes structural complexity and offers a cost-effective solution for rapid, on-site screening of CRE colonization, particularly valuable in regions where KPC and NDM predominate.
The LFIA developed in this study demonstrated both high specificity and practical sensitivity for detecting KPC- and NDM-producing strains. In our evaluation, the KPC and NDM test lines reacted exclusively with their corresponding producers, with no cross-reactivity observed against OXA-48-, VIM-, IMP-producing strains or negative controls, underscoring the robustness of the selected monoclonal antibodies and assay design. This high specificity is clinically significant, as misclassification of carbapenemase types can result in inappropriate infection control interventions or misguided therapeutic decisions. For example, meropenem-vaborbactam, ceftazidime-avibactam, and imipenem-cilastatin-relebactam are active against KPC-producing strains but not against NDM producers, whereas ceftazidime-avibactam in combination with aztreonam may be effective in NDM cases.17,18 In terms of sensitivity, the LFIA achieved a detection limit sufficient for routine application, even though molecular methods such as real-time PCR provide higher sensitivity for low-copy-number genes. Importantly, in clinical workflows carbapenemase-producing strains are generally cultured and enriched before testing, ensuring bacterial loads are adequate for LFIA detection. Thus, while LFIA may not fully replace molecular assays, it offers a rapid and cost-effective frontline tool for guiding timely clinical decisions and infection control, with confirmatory testing performed as needed according to local workflows and molecular or sequencing-based methods used when detailed genetic characterization is required.19,20
Importantly, the LFIA platform itself is technically modular and can be easily adapted to accommodate other carbapenemase targets. In regions where OXA-48-, VIM-, IMP-producing strains are more prevalent, the same assay configuration can be applied by substituting capture and detector antibodies with those specific to local enzyme types. This modular design provides a clear framework for expanding the diagnostic spectrum in future iterations and supports the development of region-specific LFIA panels that reflect local resistance epidemiology.
Despite these advantages, several limitations should be acknowledged. First, the LFIA was designed to detect only KPC and NDM carbapenemases. Although these remain the predominant enzymes in China and in many other regions globally, the distribution of carbapenemase types varies geographically.21,22 To improve the regional applicability, future test strips should be tailored to cover the locally dominant carbapenemase. Second, although the number of tested isolates was limited and mainly represented the predominant alleles blaKPC-2, blaNDM-1 and blaNDM-5, all monoclonal antibodies used were commercially validated for high affinity and broad reactivity toward multiple KPC and NDM variants, supporting the assay’s theoretical capability to detect a wider range of clinically relevant variants. Future work should include larger, multi-center validation in more diverse Enterobacterales species and across a broader range of carbapenemase genes/variants to better define clinical performance under routine laboratory workflows. Third, the LFIA provides qualitative results that rely on visual interpretation. Integrating the strips with portable readers could enhance objectivity, enable semi-quantitative analysis, and support digital connectivity with laboratory information systems.23 Finally, although PCR and WGS were used as reference methods in this study, the LFIA is best viewed as part of a complementary diagnostic framework. Routine confirmation can be performed as needed using locally available phenotypic assays and targeted molecular tests. WGS is mainly reserved for high-resolution characterization and surveillance, such as outbreak investigation and monitoring emerging carbapenemase variants and resistance mechanisms. Together, these tools may support both immediate infection-control decisions and longer-term stewardship strategies.24,25
Conclusion
In conclusion, this study demonstrates the feasibility of a rapid, instrument-free LFIA for detecting KPC and NDM carbapenemases, with high analytical specificity, operational simplicity, and a short turnaround time. In a pilot clinical evaluation of 12 non-duplicate K. pneumoniae isolates, the assay showed complete concordance with PCR/WGS. The LFIA provides a qualitative visual readout based on the presence or absence of test lines. Therefore, the LFIA is best positioned as a practical frontline screening and clinical decision-support tool for cultured isolates to support timely infection control and antimicrobial stewardship, while confirmatory phenotypic and molecular testing should be performed according to local laboratory workflows. Moreover, this work establishes a flexible methodological framework that can be adapted to regional resistance epidemiology and expanded to additional carbapenemase targets. Further multi-center validation in larger and more diverse Enterobacterales collections, including a broader range of carbapenemase variants, is warranted to define broader clinical applicability.
Abbreviations
CRE, carbapenem-resistant Enterobacterales; LFIA, lateral flow immunoassay; WGS, whole-genome sequencing; PCR, polymerase chain reaction; LOD, limit of detection; PBS, phosphate-buffered saline; BSA, bovine serum albumin; KPC, Klebsiella pneumoniae carbapenemase; NDM, New Delhi metallo-β-lactamase; OXA-48, oxacillinase-48; VIM, Verona integron-encoded metallo-β-lactamase; IMP, imipenemase; C, control line.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author (Jian Xue) upon reasonable request.
Ethical Approval and Informed Consent
This study was approved by the Ethics Committee of The First People’s Hospital of Zunyi (Ethics no. (2025)-1-340). The requirement for informed consent was waived because only anonymized bacterial isolates obtained from routine clinical procedures were used.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Guizhou Provincial Department of Science and Technology (Grant No. [QKHJC-MS-2025] 036); United funds of Zunyi Municipal Bureau of Industry and Science and Technology & Zunyi Medical and Pharmaceutical College (HZ-2024-399); United funds of Zunyi Municipal Bureau of Industry and Science and Technology & The First People’s Hospital of Zunyi (HZ-2025-61); Guizhou Provincial Health Commission [2024GZWJKJXM1416].
Disclosure
The authors declare that they have no competing financial or non-financial interests that could have appeared to influence the work reported in this paper.
References
1. Collaborators GBDAR. Global burden of bacterial antimicrobial resistance 1990-2021: a systematic analysis with forecasts to 2050. Lancet. 2024;404(10459):1199–11. doi:10.1016/S0140-6736(24)01867-1
2. Ma J, Song X, Li M, et al. Global spread of carbapenem-resistant Enterobacteriaceae: epidemiological features, resistance mechanisms, detection and therapy. Microbiol Res. 2023;266:127249. doi:10.1016/j.micres.2022.127249
3. Sati H, Carrara E, Savoldi A, et al. The WHO bacterial priority pathogens list 2024: a prioritisation study to guide research, development, and public health strategies against antimicrobial resistance. Lancet Infect Dis. 2025;25(9):1033–1043. doi:10.1016/S1473-3099(25)00118-5
4. Bonomo RA, Burd EM, Conly J, et al. Carbapenemase-producing organisms: a global scourge. Clin Infect Dis. 2018;66(8):1290–1297. doi:10.1093/cid/cix893
5. Hu Y, Yang Y, Feng Y, et al. Prevalence and clonal diversity of carbapenem-resistant Klebsiella pneumoniae causing neonatal infections: a systematic review of 128 articles across 30 countries. PLoS Med. 2023;20(6):e1004233. doi:10.1371/journal.pmed.1004233
6. Zarras C, Karampatakis T, Pappa S, et al. Genetic characterization of carbapenem-resistant Klebsiella pneumoniae clinical isolates in a Tertiary Hospital in Greece, 2018-2022. Antibiotics. 2023;12(6):976. doi:10.3390/antibiotics12060976
7. Xian Z, Jian X, Mei-Jing S, Wen-Hong A, Ze-Qiong C, Kai-Feng W. Molecular typing and drug resistance analysis of carbapenem-resistant Klebsiella pneumoniae from paediatric patients in China. J Infect Dev Countries. 2022;16(11). doi:10.3855/jidc.17003
8. Caliskan-Aydogan O, Alocilja EC. A review of carbapenem resistance in enterobacterales and its detection techniques. Microorganisms. 2023;11(6):1491. doi:10.3390/microorganisms11061491
9. Weinmaier T, Conzemius R, Bergman Y, et al. Validation and application of long-read whole-genome sequencing for antimicrobial resistance gene detection and antimicrobial susceptibility testing. Antimicrob Agents Chemother. 2023;67(1):e0107222. doi:10.1128/aac.01072-22
10. Ben-Haim O, Azrad M, Saleh N, Tkhawkho L, Peretz A. Evaluation of the NG-test CARBA 5 kit for rapid detection of carbapenemase resistant Enterobacteriaceae. Lab Med. 2021;52(4):375–380. doi:10.1093/labmed/lmaa084
11. Mendez-Sotelo BJ, Lopez-Jacome LE, Colin-Castro CA, et al. Comparison of lateral flow immunochromatography and phenotypic assays to PCR for the detection of carbapenemase-producing gram-negative bacteria, a multicenter experience in Mexico. Antibiotics. 2023;12(1):96. doi:10.3390/antibiotics12010096
12. Bernabeu S, Bonnin RA, Dortet L. Comparison of three lateral flow immunochromatographic assays for the rapid detection of KPC, NDM, IMP, VIM and OXA-48 carbapenemases in Enterobacterales. J Antimicrob Chemother. 2022;77(11):3198–3205. doi:10.1093/jac/dkac303
13. Liu HC, Liu RC, Hu MR, et al. Development of high-concentration labeled colloidal gold immunochromatographic test strips for detecting African swine fever virus p30 protein antibodies. Heliyon. 2024;10(3):e25214. doi:10.1016/j.heliyon.2024.e25214
14. Khatmi G, Klinavicius T, Simanavicius M, et al. Lateral flow assay sensitivity and signal enhancement via laser micro-machined constrains in nitrocellulose membrane. Sci Rep. 2024;14(1):22936. doi:10.1038/s41598-024-74407-3
15. Rahmani S, Basu S, Simner PJ, Kambli P, Shetty A, Rodrigues C. Evaluation of the rapid lateral flow assay (LFA) for detection of five major carbapenemase enzyme families in genotypically characterised bacterial isolates. Indian J Med Res. 2025;161(6):695–701. doi:10.25259/IJMR_1976_2024
16. Wu Y, Zhou Y, Leng Y, Lai W, Huang X, Xiong Y. Emerging design strategies for constructing multiplex lateral flow test strip sensors. Biosens Bioelectron. 2020;157:112168. doi:10.1016/j.bios.2020.112168
17. Tamma PD, Heil EL, Justo JA, Mathers AJ, Satlin MJ, Bonomo RA. Infectious Diseases Society of America 2024 guidance on the treatment of antimicrobial-resistant gram-negative infections. Clin Infect Dis. 2024. doi:10.1093/cid/ciae403
18. Al Musawa M, Bleick CR, Herbin SR, Caniff KE, Van Helden SR, Rybak MJ. Aztreonam-avibactam: the dynamic duo against multidrug-resistant gram-negative pathogens. Pharmacotherapy. 2024;44(12):927–938. doi:10.1002/phar.4629
19. Cuffari S, Aiezza N, Antonelli A, Giani T, Rossolini GM. Evaluation of three commercial lateral flow immunoassays for the detection of KPC, VIM, NDM, IMP and OXA-48-like carbapenemases. J Antimicrob Chemother. 2024;79(10):2724–2727. doi:10.1093/jac/dkae262
20. Tychala A, Meletis G, Mantzana P, et al. Replacement of the double meropenem disc test with a lateral flow assay for the detection of carbapenemase-producing enterobacterales and pseudomonas aeruginosa in clinical laboratory practice. Antibiotics. 2023;12(4):771. doi:10.3390/antibiotics12040771
21. Kedisaletse M, Phumuzile D, Angela D, Andrew W, Mae NF. Epidemiology, risk factors, and clinical outcomes of carbapenem-resistant Enterobacterales in Africa: a systematic review. J Glob Antimicrob Resist. 2023;35:297–306. doi:10.1016/j.jgar.2023.10.008
22. Alvisi G, Curtoni A, Fonnesu R, et al. Epidemiology and genetic traits of carbapenemase-producing enterobacterales: a global threat to human health. Antibiotics. 2025;14(2):141. doi:10.3390/antibiotics14020141
23. Han X, Fang R, Liang Y, et al. Breakthrough of the lateral flow assay technology for on-site detection of foodborne pathogenic bacteria: resonance among the recognition reagents, nanomaterial labels, and multi-technological integration. Food Chem. 2025;493(Pt 3):145832. doi:10.1016/j.foodchem.2025.145832
24. Nishida S, Ihashi Y, Yoshino Y, Ono Y. Evaluation of an immunological assay for the identification of multiple carbapenemase-producing gram-negative bacteria. Pathology. 2022;54(7):917–921. doi:10.1016/j.pathol.2022.05.007
25. Lee AS, Dolan L, Jenkins F, Crawford B, van Hal SJ. Active surveillance of carbapenemase-producing Enterobacterales using genomic sequencing for hospital-based infection control interventions. Infect Control Hosp Epidemiol. 2024;45(2):137–143. doi:10.1017/ice.2023.205
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.