Back to Journals » Advances in Medical Education and Practice » Volume 16
Developing a Student-Centred Curriculum: Insights from Anaesthetic Placement Experiences for Co-Designing in China’s Greater Bay Area
Authors Huang C ![]() , Xiao Y, Xu D
, Xiao Y, Xu D ![]() , Wong IN
, Wong IN ![]() , Patil NG, Chen J
, Patil NG, Chen J ![]() , Zhang K, Hu W, Zhang J
, Zhang K, Hu W, Zhang J ![]() , Ding S, Kuang M
, Ding S, Kuang M ![]() , Xiao H, Feng X
, Xiao H, Feng X
Received 25 March 2025
Accepted for publication 8 September 2025
Published 18 September 2025 Volume 2025:16 Pages 1695—1704
DOI https://doi.org/10.2147/AMEP.S530349
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Chanyan Huang,1,* Ying Xiao,1,* Dan Xu,2,3,* Io Nam Wong,4 Nivritti Gajanan Patil,4 Jiancong Chen,2 Kunsong Zhang,2 Wenjie Hu,2 Jianrong Zhang,2 Shuqin Ding,2 Ming Kuang,2 Haipeng Xiao,2 Xia Feng1
1Department of Anaesthesiology, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, People’s Republic of China; 2Department of Medical Education, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, People’s Republic of China; 3General Practice Research and International Collaboration, Curtin School of Population Health/Curtin Medical School, Faculty of Health Sciences, Curtin University, Perth, WA, Australia; 4Practice Research, Faculty of Medicine, Macau University of Science and Technology, Macau, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xia Feng, Email [email protected] Ming Kuang, Email [email protected]
Introduction: Medical education standards influence the academic performance and clinical competencies of medical students as career practitioners. With the rising demand for teaching innovation and technological advancement in medical education, clinical teaching in China has faced many challenges, which necessitate a re-evaluation of traditional educational approaches. To overcome these challenges, the tertiary hospital in Guangzhou and the medical school in Macau have initiated the reform of clinical teaching in an undergraduate teaching program with a specific project for Macau medical students to perform clinical placement in anaesthesia at the tertiary hospital in Guangzhou. The project was co-led and co-chaired by both institutions and coordinated by the Anaesthetic Department, International Office, and Medical Education Department at the tertiary hospital in Guangzhou. This project aimed to analyse students’ anaesthetic placement experiences to illustrate the effectiveness of collaborative teaching and the development of a student-co-designed curriculum.
Methods: The participating medical students attended the anaesthetic placement at the tertiary hospital in Guangzhou, which is scheduled to spend one day in operating theatres, recovery rooms, and central theatre pharmacies under supervision. All participating students provided post-placement feedback by answering a pre-designed enquiry questionnaire to develop a co-designed curriculum. Post-placement feedback, including written reflections in response to the enquiry questionnaires, was collected and semantically analysed.
Results: Post-placement feedback in response to the enquiry questionnaires was presented as themes, which formed the core elements of the student-co-designedanaesthetic placement curriculum.
Conclusion: This study demonstrates the effective implementation of collaborative teaching and curriculum co-designed in anaesthesia education at a tertiary hospital in the “Greater Bay Innovative Zones of China”. This curricular design model facilitates the development of a student-centred anaesthetic curriculum for better clinical teaching and learning.
Keywords: student-centred curriculum, curriculum co-design, anaesthetic placement, clinical teaching, clinical learning
Introduction
The standard of medical education is influencing the academic performance of medical students and their subsequent career clinical practice as competent practitioners within the health care system.1–4 As the demand for introducing innovative teaching and learning models with modern technology into medical education in China increases, clinical teaching and learning have encountered many challenges.5 Clinical teaching and learning have taken the centre stage of the medical education reform in China, under the theme of “Education and Training Programme for Excellent Physicians”.1,6 As the reform is underway, the tertiary hospital in Guangzhou and the medical school in Macau have signed a memorandum of understanding for pre-intern year medical students’ teaching and learning exchange with Macau medical students to undertake clinical placement in disciplines of medicine, surgery, anaesthesia, and paediatrics at the tertiary hospital in Guangzhou. The discipline of anaesthesia has been leading the conceptualisation of this study in collaboration with both institutions’ directors and coordinators at the departments of anaesthesia, international affairs, and medical education at the tertiary hospital in Guangzhou.
The study aims to reflect on students’ anaesthetic placement experiences to showcase the collaboration and co-design model approach in developing student-centred curriculum for the anaesthetic placement in China’s “Greater Bay Innovative zones” by the joint expertise teams from both institutions. In contrast to the traditional curriculum design, modern curriculum design requires not only specific learning objectives but also specific time allocation and other relevant influencing factors. One of the most relevant factors in today’s rapidly changing landscape of curriculum design is the concept of “Co-Design”, which engages students by curriculum designers in providing feedback and completing pre-designed questionnaires by students as shared responsibilities with curriculum designers to refine and enhance the curriculum.7 This study reports the results of feedback to pre-design enquiry questionnaires distributed to exchanged students having completed a one-day anaesthesia placement as part of a students’ co-designed process, aiming to develop a more comprehensive and co-designed curriculum for future students from both institutions during anaesthetic placement.
Materials and Methods
Study Design and Setting
Fourteen pre-intern year medical students from a medical school in Macau attended a one-day anaesthetic placement at the tertiary hospital in Guangzhou. The international collaboration offices at both institutions delegated a senior anaesthetist to coordinate the plan for curricular integration through this exchange program to upgrade the plan to a student-centred co-design curriculum in China’s “Greater Bay Innovative Zones”. On completion of the one-day anaesthetic placement, our study administered a pre-designed questionnaire, which is a validated and modified survey instrument used by some co-authors in several previous published studies8–11 to collect participants’ feedback and reflections. The pre-designed questionnaire was modified to be relevant to the discipline of anaesthesia by three anaesthesiologists from survey questionnaires in previous published studies.8–11 The modified survey questionnaire was then further validated through pilot testing of the survey by a panel of expert clinicians, including anaesthetists, surgeons, physicians and experienced medical educators.
Placement Schedule and Activities
During this supervised placement, the participating students were scheduled to spend the entire morning and early afternoon in the operating theatres, post-anaesthesia care unit, and central theatre pharmacy to learn clinical anaesthesia under the guidance of experienced anaesthesiologists (Table 1).
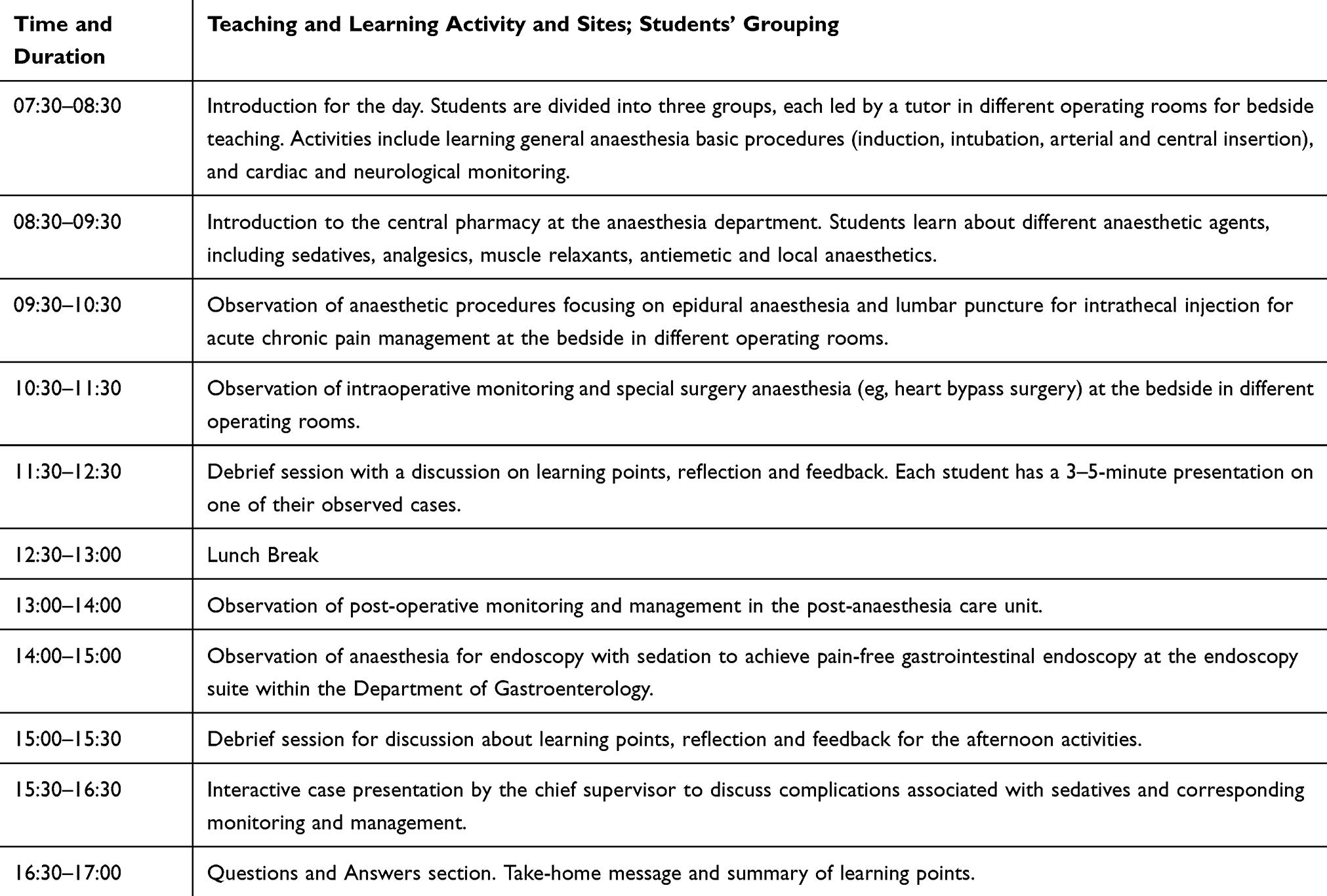 |
Table 1 Anaesthesia Placement Daily Schedule |
This one-day placement aims to provide students with a comprehensive introduction to anaesthesiology, equipping them with foundational anaesthesia knowledge and clinical expertise understanding which are required by clinicians irrespective of their career choice of specialty. The intended learning outcomes fit into part of the overall training with surgical specialties, and included the following items: 1) pre-operative assessmenty; 2) management of airway and fluid balance; 3) anaesthesia types with indications and contraindications; 4) pharmacology of anaesthetics; 5) induction and airway maintenance; 6) intraoperative monitoring; 7) common anaesthetic procedures and techniques; 8) complications associated with anaesthesia; 9) post-anaesthesia monitoring; and 10) indications and contraindications of mechanical ventilation and resuscitation.
All participating students were invited via an online portal to provide post-anaesthesia clerkship feedback by answering a pre-designed questionnaire (Figure 1). The pre-designed questionnaire included five quantitative questions using a Likert scale and sixteen qualitative/open-ended questions relevant to curriculum design, designed to gather student input for developing a student-centred co-designed curriculum. Fourteen responses were received with feedback and reflection data, indicating a response rate of 100%. To ensure the reliability of students’ feedback and reflections, the pre-designed questionnairewas completed anonymously via an online portal.
 |
Figure 1 Post-anaesthesia placement feedback questionnaire for students. Notes: The structured questionnaire was administered to medical students from the Macau University of Science and Technology after completing their anaesthesia placement. It consisted of 21 questions covering students’ prior expectations, perceptions of teaching models, adequacy of case preparation, opportunities for interaction with supervisors, knowledge and skill acquisition, and overall satisfaction with the placement. The questionnaire also collected suggestions for improving teachingduring the anaesthesia placement and input for the co-designed curriculum. |
Data Collection and Analysis
After completing the placement, students’ responses to the pre-designed questionnaires were collected via an online anonymous portal established by the main authors at the Guangzhou tertiary hospital anaesthetic department to monitor and verify inter-rater reliability as well as to ensure the validation of the coding method. High inter-rater reliability has been observed in our study, indicating higher rating consistency and lower discrepancy with pilot testing of the survey questionnaire among expert clinicians. Qualitative data from written reflections and feedback responses were analysed manually using descriptive and semantic analysis to ensure the accuracy.12
Consent for Participation
Written informed consent was obtained from all participants via an online invitation including the participant information and consent form, with the consent for the publication of participants’ anonymised responses.
Results
Fourteen students, including six males and eight females, responded to the post-placement pre-designed questionnaire with the following illustrated themes generated by thematic analysis. These themes formed the basis of the supervisors’ and students’ co-designed anaesthetic placement curriculum, which are summarised at the end of each theme topic.
Theme 1: Students’ Learning Expectations and Definitions of Anaesthesia Before the Anaesthesia Placement
The thematic analysis created three groups of expectations and definitions as follows.
Group 1: The students were accepting whatever would be provided to them by the tutor and had no clear thoughts about what anaesthesia should be like prior to the placement.
Group 2: Students expected to learn about general procedures preparing patients for surgery, including pre-operative assessments, common types of anaesthesia, intra-operative monitoring, and post-operative recovery. Their understanding of anaesthesia was centred on pain insensitivity and reduced consciousness by administering drugs before surgery.
Group 3: Students sought a deeper understanding of anaesthesia, including knowledge of various anaesthetic agents, routes of administration, choosing clinically appropriate drugs in a real-life setting, and monitoring adverse effects and complication management. The layman’s definition of anaesthesia by the students was the use of different medications to induce a temporary loss of sensation and awareness, ensure the maintenance of vital signs, and relieve post-surgical pain.
Supervisors’ and students’ input summary for the co-designed anaesthetic placement curriculum: The co-designed curriculum would enable three cohorts of students with different levels of expectations with bedside anaesthetic learning to meet the expectations of group 2 students as the basic entry level of anaesthesia training for doctors in non-anaesthesia specialties. Combining group 2 and 3 expectations will be the advanced level of anaesthesia training for doctors in both non-anaesthesia specialties and anaesthesia specialties training, including general practitioner (GP) subspecialty training as a GP anaesthetist.
Theme 2: Students’ Preferences and Beliefs of Teaching Models Used in Achieving Better Learning Outcomes
Case-based learning and lectures are equally rated as the most preferred teaching models by the students, followed by clinical bedside teaching and problem-based learning to be rated equally in second place (Figure 2A).
 |
Figure 2 Teaching Models: (A) Preferences for teaching models; (B) Students’ responses on whether visiting the central pharmacy of the anaesthetic department is appropriate for students’ learning. |
Supervisors’ and students’ input summary for the co-designed anaesthetic placement curriculum: The co-designed curriculum will enable the weighted distribution based on the time allocation of “Case-based learning and lectures” being 55% and “clinical bedside teaching and problem-based learning” being 45%.
Theme 3: Students’ Perception of Case Preparation for Theatre-Bedside Clinical Learning
Most students (92.86%) reported that the cases prepared for the one-day anaesthesia placement were adequate. Furthermore, all students (100%) agreed that case preparation allowed sufficient time for case interaction and discussion with supervisors. Additionally, all students (100%) felt that the proportion of cases allocated for bedside teaching inside operating theatres and small-group teaching in the tutorial room were appropriate. Specifically, the placement included 5–7 cases of bedside teaching in operating theatres and 1–2 cases of small-group teaching in the tutorial room. This distribution was designed to ensure a balanced educational experience across different teaching environments.
In terms of the most memorable case of the day, eight out of 14 students considered the case of small-group teaching to be the most memorable, while five students preferred the cases presented during bedside teaching. Additionally, one student felt that all cases, from both bedside and small-group teaching, were equally memorable.
Supervisors’ and students’ input summary for a co-designed anaesthetic placement curriculum: The co-designed curriculum will enable the delivery of one case as the most memorable case and six cases for bedside teaching in operating theatres.
Theme 4: Learning Anaesthetic Medications and Their Routes of Administration
Placement allocated time for students to visit the central pharmacy of the Department of Anaesthesia. The majority of the students (64.29%) strongly agreed that visiting the central pharmacy was an effective approach to learn about the process of anaesthesia, with 35.71% agreeing with this approach (Figure 2B). This visit was considered a valuable educational experience.
Supervisors’ and students’ input summary for the co-designed anaesthetic placement curriculum: The co-designed curriculum will allocate at least 30 minutes/up to 60 minutes (after the bedside teaching cases) to visit the central pharmacy of the Department of Anaesthesia with educational discussions associated with bedside teaching cases in operating theatres.
Theme 5: Students’ Feedback on the Overall Curriculum Design of the One-Day Anaesthesia Placement
The data showed that 71.43% of the students felt the one-day placement enabled them to freely describe all the different anaesthetic concepts (such as induction) and commonly used anaesthetic medications during anaesthesia (Figure 3A). In addition, 85.71% of the students felt confident describing common anaesthetic complications, including pre-operative, intra-operative, and post-operative complications, following placement (Figure 3B). However, 28.57% of the students felt that the one-day placement had not given them enough contact hours to consolidate what they had learned in one day, and they suggested repeating the same one-day curriculum for two days, or even one week.
 |
Figure 3 (A) Students’ feedback on the placement’s enabling effects on their ability to freely describe anaesthetic concepts and medications; (B) Students’ response on the placement’s enabling effects on their ability to freely describe anaesthetic complications. |
All students agreed that anaesthesia should be an independent placement, which provided many opportunities to learn clinical skills (Figure 4A) and enabled knowledge translation into clinical practice (Figure 4B). Overall, all students were satisfied with the placement (Figure 4C) and expressed willingness to help co-design an anaesthesia curriculum by giving feedback to supervisors who developed the one-day plan/schedule of anaesthesia placement.
 |
Figure 4 (A) Students’ perception on whether the placement helps more clinical skill acquisition; (B) Students’ perception on whether the placement helps more knowledge acquisition; (C) Students’ satisfactory rating with the placement overall. |
Supervisors’ and students’ input summary for co-designed anaesthetic placement curriculum: The co-designed curriculum will be weighted distribution of the following items: 1) introductory lectures including basic knowledge of anaesthesia, such as induction and recovery for 60 minutes; 2) six cases of bedside teaching for 240 minutes (every 60 minutes with 15 minutes break time then total 300 minutes for the section), 3) visiting the central pharmacy for 60 minutes, 4) case-based learning and summary lectures with the most memorable case for 60 minutes; and 5) introduction of two days into the co-designed curriculum by repeating items 2, 3, and 4.
Discussion
The feedback and reflection from the students underscore the necessity for a student-centred co-designed curriculum in anaesthetic placement, aligning with contemporary educational models that emphasise active learner involvement. Anaesthesia placement is an essential educational experience which is often overlooked by many medical schools, and many consider anaesthesia placement only for those who have a career interest in anaesthesia.13 With respect to the generated themes in our study focusing on what we should teach in anaesthetic placement, there have been numerous educational studies by curricular designers to define what should be in anaesthesia placement,14,15 however there was a lack of consensus opinions, albeit with some similarities outlined in the literature initially identified by Cooper and Hutto16 as follows: (1) resuscitation, (2) practical procedures, (3) consent and ethics, (4) rapid history taking and preoperative assessment, (5) pre-admission assessment, (6) acute and chronic pain control, (7) recovery ward experience, (8) fluid balance and clinical pharmacology, and (9) intensive care and the consequences of technological medicine. The above nine points has clearly reflected in our study by showing the incorporation of our students’ expectations of what should be learned into our supervisors’ desire in developing a consensus and student co-designed curriculum framework. As evidence demonstrating how to prepare a consensus curriculum framework to guide undergraduate education in anaesthesia,17 the consensus guide proposes eight domains of anaesthetic and critical care practice, setting out what everyone believes to be the key capabilities of a competent anaesthetist, including (1) manipulation of consciousness (sedation, anaesthesia, and psychological techniques, eg anxiety management), (2) airway management, (3) circulation management, (4) pain management, (5) Preoperative assessment: understanding and communication of risk and safety, and discussion and decision-making relating to the appropriateness of interventions; (6) operating theatre/perioperative management and leadership; (7) specific and generic procedural skills; (8) discussions around end-of-life care; and (9) recognition and care of the deteriorating patient. This consensus guide has defined the academic contents of the curricular framework, which has echoed the results of our study. With these framework curricula in place, a formal curriculum rather than a placement schedule or plan will be important for any anaesthetic placement to ensure the delivery of knowledge and skills for clinical competency in a supervised and structured way.
In our study, the students’ reflections on the delivery of the student co-designed anaesthetic curriculum with an innovative, structural and student-centred teaching model, highlighting the novelty of our study results being both student-centred and student co-designed. A study conducted in Palestine examined a two-week anaesthetic placement of senior medical students and concluded that educators used active and effective teaching or training approaches less frequently during the anaesthesia placements, leading to medical student dissatisfaction with their competencies after their anaesthesia placement,18 claiming a lack of structured curriculum. To build a structural curriculum with a student co-designed model is what our current research outcome demonstrates, and where our research results’ novelty lies. In addition, modern-time curricula focus less on the acquisition of knowledge and instead on achieving competencies to equip students to work in complex clinical settings.19 Our research results have highlighted the modern-time curricula focus on participating students’ competency achievement by delivering a student-centred curriculum in real-life clinical setting. Another critical point has been shown with clinical setting being the centrepiece of learning objectives and outcomes. Guided by learning objectives and outcomes, students’ learning needs include facts, values, attitudes, and behaviour with emerging new theories of learning emphasis on the views with learning as the consequence of an individual’s interpretation and interaction with their environment.19 Learners become proactively involved in curriculum design, while teachers are conduits of factual content and even more important as “enablers” for accessing to a community of learning.20 Our results have certainly showcased participating students’ active engagement in curriculum design for improving their factual knowledge. Factual knowledge is only complete when there is a combined array of knowledge communication, moral and ethical dimension to complement cognitive understanding. To achieve all these facets of clinical reasoning learning, it is critically important that adequate time for anaesthetic placement is stated clearly to be allocated in the clinical environment.21 The time factor is also an important feedback point from the participating students in our study, which is consistent with international literature.
Modern curriculum design requires not only specific learning objectives but also specific time allocation and other relevant influencing factors. One of the most relevant factors in today’s rapidly changing landscape of curriculum design is the concept of “Co-Design” especially our current study’s student-centred co-design approach of inviting students to enquire and query the curriculum as well as to give feedback and answer the predesigned questionnaire. Students’ queries, enquiries, feedback, and answers to the questionnaires were then incorporated into developing and updating the placement curriculum.
Co-design, known as collaborative design, is an act of co-creation in reference to any action of “collective inquiry and creativity”22 with the concept of “shared responsibility” and the application of co-creation to the full design process.23,24 Through the students’ feedback with answers to the collective enquiry, our current study clearly reflected the concept of co-design curriculum, which is a mindset change for both students and teachers, an innovative method of curriculum design, and a collection of enquiry tools and survey of students’ expectations that span across the design process. This design process has been demonstrated in previous research.25 Furthermore, co-design can be described as a combination of collaborative inquiry and expectations,26 which has been clearly shown in our study that both teachers and students come together to identify and inquire into the need for a mutually agreeable curriculum, design it, apply it and evaluate it. The co-design curriculum embraces both students’ and teachers’ expectations, experience and expertise to discuss ideas about developing and evaluating the curriculum, in which this approach has been seen in our study as well as in another study.26 The extent to which different participants are able to engage in these activities of discussion, expression, sharing, and negotiating strongly affects the end-result of the collaboration and the effectiveness of the team.26 The newly developed co-design curriculum (Supplementary Material) has showcased the engagement of students as a co-design partner in our study, which has been well described in a university handbook.27
Limitations
This study had two limitations. First, the number of students involved in the co-design process was relatively small, which may not have fully captured the diverse perspectives and contributions of a larger group of students. This limitation could affect the comprehensiveness of student feedback incorporated into curriculum design. Second, there were an insufficient number of supervisors available for bedside teaching, which may have impacted the quality and breadth of the hands-on learning experience during placement. Finally, the one-day curriculum may limit the learning opportunities of bedside teaching, as reflected by some students’ statements of inadequate contact hours to consolidate the one-day learning and fully achieve specific learning objectives. Future studies are being planned to address these limitations.
Conclusions and Future Perspectives
This study highlighted collaborative teaching and learning in anaesthesia through anaesthetic curricular co-design at a tertiary hospital in China’s “Global Innovation Hub” zones. By integrating supervisors’ discipline-specific input with students’ expectation-focused input summary as part of the co-designed process, the curricular co-design approach can facilitate the development of a student’s codesign anaesthetic curriculum to be introduced into anaesthetic placements. An academically weighted co-designed anaesthetic curriculum has been developed and implemented in this study, albeit a few limitations have been observed. Further studies are needed to involve more students and supervising doctors in the co-design process and enable a co-design approach to significantly improve students’ clinical reasoning learning with anaesthetic placement. Another study was undertaken to address the limitation of inadequate contact hours for final-year medical students, especially those seeking a career in anaesthesia in future medical practice through evaluation research pre- and post-implementation of student-codesign curriculum with a focus group approach. The ultimate goal of these future studies is to establish a student-centred and student-codesigned anaesthetic placement curriculum for international benchmarking.
Human Ethics, Copyright and Consent to Participate
Ethical approval was obtained from the Human Research Ethics Committee and Institutional Review Board of the First Affiliated Hospital of Sun Yat-sen University and the Faculty of Medicine at the Macau University of Science and Technology. Written informed consent was obtained from all student participants via an online invitation including the participant information and consent form. All methods were performed in accordance with the relevant guidelines and regulations. The study was conducted in compliance with the Declaration of Helsinki.
Data Sharing Statement
The datasets analysed in this study are available from the corresponding author upon reasonable request.
Acknowledgments
We acknowledge Dr. Shaoting Feng and the staff at the First Affiliated Hospital, Sun Yat-sen University and the Faculty of Medicine of Macau University of Science and Technology for their administrative support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by a grant from Guangzhou Clinical High-tech Major Characteristic Technology Project (2023P-GX10).
Disclosure
There are no competing interests to be declared.
References
1. Shi Z, Li C, Wu H. Effects of the education and training programme for excellent physicians in China on medical students’ academic performance: a cross-sectional study. BMJ Open. 2023;13(9):e072940. doi:10.1136/bmjopen-2023-072940
2. Hays RB, Ramani S, Hassell A. Healthcare systems and the sciences of health professional education. Adv Health Sci Educ Theory Pract. 2020;25(5):1149–1162. doi:10.1007/s10459-020-10010-1
3. Johnson SB, Fair MA, Howley LD, et al. Teaching public and population health in medical education: an evaluation framework. Acad Med. 2020;95(12):1853. doi:10.1097/ACM.0000000000003737
4. Boroumand S, Stein MJ, Jay M, Shen JW, Hirsh M, Dharamsi S. Addressing the health advocate role in medical education. BMC Med Educ. 2020;20(1):28. doi:10.1186/s12909-020-1938-7
5. Yang G, Wang Y, Zeng Y, et al. Rapid health transition in China, 1990–2010: findings from the Global Burden of Disease Study 2010. Lancet. 2013;381(9882):1987–2015. doi:10.1016/S0140-6736(13)61097-1
6. Wang W. Medical education in China: progress in the past 70 years and a vision for the future. BMC Med Educ. 2021;21(1):453. doi:10.1186/s12909-021-02875-6
7. Wang L, Shen W, Xie H, Neelamkavil J, Pardasani A. Collaborative conceptual design—state of the art and future trends. Computer-Aided Des. 2002;34(13):981–996. doi:10.1016/S0010-4485(01)00157-9
8. Zhang J, Tang Y, Feng S, et al. Collaborative teaching and curricular integration in pre-intern clinical placements: insights from the Greater Bay Area. Adv Med Educ Pract. 2024;15:1027–1037. doi:10.2147/AMEP.S471782
9. Feng S, Yang D, Zhang K, et al. Reflecting on experiences of senior medical students’ external clinical teaching visits in general practice placements: a pilot study. Adv Med Educ Pract. 2024;15:207–216. PMID: 38525099, PMCID: PMC10961076. doi:10.2147/AMEP.S454467
10. Feng S, Yang D, Zhang K, et al. Reflecting on experiences of GP trainees teaching senior medical students during GP placement: a pilot study. Australian J General Pract. 2024;2024.
11. Xu D, Feng S, Yang D, et al. Reflecting on students’ experiences of an innovative teaching model during aged care visit in clinical placements: a qualitative pilot study. Adv Med Educ Pract. 2023;14:1339–1346. PMID: 38046262, PMCID: PMC10693279. doi:10.2147/AMEP.S436905
12. Cooper N, Bartlett M, Gay S, et al. Consensus statement on the content of clinical reasoning curricula in undergraduate medical education. Med Teach. 2021;43(2):152–159. doi:10.1080/0142159X.2020.1842343
13. Galway UA. Designing an optimally educational anesthesia clerkship for medical students–survey results of a new curriculum. J Educ Perioper Med. 2014;12(1):E054. PMID: 27175386, PMCID: PMC4719530.
14. Rohan D, Ahern S, Walsh K. Defining an anaesthetic curriculum for medical undergraduates. A Delphi study. Med Teach. 2009;31:e1e5. doi:10.1080/01421590802334291
15. Overton MJ, Smith NA. Anaesthesia priorities for Australian and New Zealand medical school curricula: a Delphi consensus of academic anaesthetists. Anaesth Intensive Care. 2015;43:51e8. doi:10.1177/0310057X1504300108
16. Cooper G, Hutton P. Anaesthesia and the undergraduate medical curriculum. Br J Anaesth. 1995;74:3e5. doi:10.1093/bja/74.1.3
17. Smith A, Carey C, Sadler J, Smith H, Stephens R, Frith C. Undergraduate education in anaesthesia, intensive care, pain, and perioperative medicine: the development of a national curriculum framework. Med Teach. 2019;41(3):340–346. PMID: 29968485. doi:10.1080/0142159X.2018.1472373
18. Shawahna R, Jaber M, Maqboul I, et al. Teaching approaches and satisfaction of medical students during anesthesia rotations: a multicenter cross-sectional study. BMC Med Educ. 2023;23:641. doi:10.1186/s12909-023-04603-8
19. O’Connor E, Moore M, Cullen W, Cantillon P. A qualitative study of undergraduate clerkships in the intensive care unit: it’s a brand new world. Perspect Med Educ. 2017;6:173e81. doi:10.1007/S40037-017-0349-X
20. Goodwin D, Pope C, Mort M, Smith AF. Access, boundaries and their effects: legitimate participation in anaesthesia. Sociol Health Illn. 2005;27:855e71. doi:10.1111/j.1467-9566.2005.00477.x
21. England AJ, Jenkins BJ. Time spent in the clinical environment is the most important aspect of medical education—we need to protect it. Anaesthesia. 2017;72:1306–1311. doi:10.1111/anae.14049
22. Trischlera J, Dietrichb T, Rundle-Thiele S. Co-design: from expert- to user-driven ideas in public service design. Public Manage Rev. 2019;21:1595–1619. doi:10.1080/14719037.2019.1619810
23. Sanders E, Stappers P. Co-creation and the new landscapes of design. CoDesign. 2008;4:5–18. doi:10.1080/15710880701875068
24. Stratos co-design: a powerful force for creativity and collaboration; 2016. Available from: https://medium.com/@thestratosgroup/co-design-a-powerful-force-for-creativity-and-collaboration-bed1e0f13d46.
25. Sanders E, Stappers P. Convivial Toolbox: Generative Research for the Front End of Design. BIS Publishers; 2012.
26. Steen M. Co-design as a process of joint inquiry and imagination. Des Issues. 2013;29:16–28. doi:10.1162/DESI_a_00207
27. Dollinger M, D’Angelo B. Co-Design for Student Success. Handbook for La Trobe University; 2020.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.