")
Back to Journals » Infection and Drug Resistance » Volume 16
Determinants of Unsuccessful TB Treatment Outcomes Among Patients on Directly Observed Treatment Short Course in Jimma Town Health Facilities, Southwest Ethiopia: A Case-Control Study
Authors Teka D, Assegid S, Ahmed J , Debella A , Amentie E , Wami G, Eyeberu A
Received 24 July 2023
Accepted for publication 22 September 2023
Published 28 September 2023 Volume 2023:16 Pages 6427—6435
DOI https://doi.org/10.2147/IDR.S428652
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Derege Teka,1 Sahilu Assegid,1 Jemal Ahmed,2 Adera Debella,3 Eyobel Amentie,4 Girma Wami,4 Addis Eyeberu3
1School of Public Health, Department of Epidemiology, Jimma University, Jimma, Ethiopia; 2School of Public Health, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 3School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 4School of Medicine, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Correspondence: Addis Eyeberu, School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, 138, Dire Dawa, Harar, Ethiopia, Tel +251 910005436, Email [email protected]
Background: Even though Ethiopia’s Federal Ministry of Health has been implementing several programs aimed at reducing the burden of tuberculosis (TB), It does not demonstrate adequate progress. As a result, identifying the determinants of unsuccessful outcomes of directly observed treatment, short-course (DOTS) is critical.
Purpose: This study aimed to assess the determinants of unsuccessful TB treatment outcomes among patients with DOTS in Jimma town, southwest Ethiopia.
Patients and Methods: An unmatched case-control study using secondary data was conducted among 118 cases and 472 controls from April 1 to June 1, 2021. Cases were TB cases with unsuccessful treatment courses whereas controls were those of successful treatment. Data were collected using a standardized tool. Statistical analysis was done using SPSS version 23 software. A binary logistic regression model was used to identify the determinants.
Results: We found that the determinants including age > 35 years (AOR=1.9, 95% CI: 1.14– 3.2), lack of contact person (AOR= 27, 95% CI: 15.8– 46.3), being HIV positive (AOR=7.3, 95% CI: 3.7– 14.2)), and being malnourished (AOR=4.5, 95% CI: 1.5– 12.9) were significantly associated with unsuccessful tuberculosis treatment outcome.
Conclusion: In this study, advanced age, being HIV positive, lack of contact person, and being malnourished were determinant factors for unsuccessful TB treatment outcomes. Hence, careful monitoring, screening, and management of risk factors are recommended.
Keywords: unsuccessful treatment outcome, TB, DOTS, southwest Ethiopia
Introduction
Tuberculosis (TB) is an infectious disease caused by the bacillus Mycobacterium tuberculosis, which is spread by inhaling droplet nuclei from infected patients when coughing, speaking, singing, or sneezing.1,2 According to the World Health Organization (WHO) report in 2022, an estimated 10.6 million people fell ill with TB globally in 2021 and of those, 1.6 million people died (1.4 million deaths among HIV-negative people and 187,000 deaths from HIV-positive people).3,4 Furthermore, the report outlined an increase of 3.6% in the incidence rate of tuberculosis 2021 which was 6.4 million new TB cases.3,5 The burden of drug-resistant tuberculosis increased by 3% in 2021, with 450,000 incident cases of multidrug-resistant (MDR-TB).3,4 Additionally, the estimated proportion of people with TB who had MDR/RR-TB was 18% among those previously treated.4 Africa is among the regions with a high burden of tuberculosis illness in 2019 (25%).6
Ethiopia is among the countries with a high burden of TB, HIV, and MDR-TB.7 Evidence showed that the prevalence of TB / HIV co-infection in Ethiopia was 25.59%.8 A systematic review and meta-analysis study showed that the prevalence of MDR-TB was 7.24% with 2.18% of new cases and 21.07% of previously treated cases with 12.5% death contribution.9 The burden of TB was more aggravated by the epidemics of coronavirus (COVID-19).10,11 TB is a severe public health issue in Ethiopia, with a cure rate of 67%, considerably below the WHO guideline of 85%.12 A study done in Gondar showed that the success rate of TB treatment was 29.5%.13 “Several studies indicated that TB patients on treatment continued to record unsuccessful treatment outcomes’s.13–16
Previous research has shown that various variables are linked with failed TB treatment outcomes. Older age, residence, concomitant conditions, a lack of contact person, a sputum smear-negative treatment category at the start of therapy, and HIV-positive status were all linked to poor TB treatment outcomes.14,17,18 While family support, socioeconomic, physician and nurse support, availability to access health services, social stigma, psychological stress, and knowledge were significant factors in the successful treatment of tuberculosis.16,18–22
In Ethiopia, a standardized TB prevention and control program incorporating Directly Observed Treatment, Short Course (DOTS) was started as a pilot in 1992, at the Arsi zone in the Oromia region. Following that, the DOTS method was scaled up and put into practice on a nationwide basis. Currently, 75% of DOTS health facilities are covered geographically, compared to 90% for geographic coverage.6–8
Recent reports showed that Directly Observed Treatment, Short Course (DOTS) was effective in attaining a highly successful treatment rate.19 However, according to several research, DOTS has also negative consequences such as primary drug resistance, acquired drug resistance, and relapse.20–22 “According to the WHO, tuberculosis treatment targets have not been achieved in many regions of the world, even when anti-TB treatments are available, and plans aiming to minimize new cases of TB by 80% by 2030 are in place.23
Even though Ethiopia’s Federal Ministry of Health has been adopting a variety of efforts to lessen the burden of tuberculosis illnesses, it has not been accomplished satisfactorily. So, it is imperative to identify determinant factors of unsuccessful treatment outcomes. Moreover. Because treatment success is recognized as a fundamental parameter of TB control efforts, it is critical to identify and address variables that contribute to poor treatment outcomes to achieve the worldwide goal of treatment success. Thus, the purpose of this study was to investigate factors of failed treatment outcomes among DOTS patients in Jimma town health facilities in southwest Ethiopia.
Methods and Materials
Study Design, Period, and Setting
We conducted an unmatched case-control study using the patients’ records in TB clinics providing DOTS in Jimma town, which is located 357 kilometers southwest of Addis Ababa and has a total area of 4623 hectares, from April 1 to June 1, 2021. The settlement is splitted into three woredas (administrative units that comprise several kebeles) and thirteen kebeles (the smallest administrative unit in Ethiopia). The town’s total anticipated population is 130,254. The town has 5 hospitals (2 public and 3 private), 4 public health centers, and 16 private clinics, with 6 public health institutions and 4 private clinics providing treatments for tuberculosis treatment.
Eligibility Criteria
“The cases were patients aged >15 years with records of adverse or unsuccessful treatment outcomes including TB treatment failures (smear-positives after 5 months of treatment), treatment defaults, and death), whereas controls were those who registered as cured (negative smear microscopy at the end of treatment and on at least one previous follow-up test) or treatment completed. Registries in which treatment outcomes were missing and patients were transferred to other districts, retreatments, MDR treatment, and age < 15 were not included in the study.
Sample Size Determination and Sampling Technique
Double population proportion formulae were used to calculate the required sample size, with the assumption of prior determinants of failed treatment results, a 5% level of significance, and 80% power. In a previous study, we discovered that factor sputum smear-negative treatment category at treatment beginning in Ethiopia18 resulted in the required sample size. As a result, the number of cases and controls was 117 and 468, respectively, and after adjusting for non-response, the final sample size was 129 cases and 516 controls. Records of TB patients from July 1, 2015, to June 30, 2020, were reviewed.
The total sample size was allotted proportionally to each institution (10) based on the total number of patients who began TB treatment in the five years before data collection. The allotted cases were picked from each institution using simple random sampling from a list of cases. To facilitate the comparison of cases and controls, four controls who began therapy in the same week at the same institution were added for one case. If more than four controls began in the same week, the one that was most closely recorded with the case was chosen.
Data Collection Tools and Techniques
Data were extracted from the medical records of TB patients using well-structured questionnaires adapted from the TB registration logbook. The checklist includes patient sociodemographic, clinical, and investigational features, treatment history, anthropometric measures, and treatment results. The data were collected by ten well-trained nurses who were overseen by an experienced nurse. To assure data quality, data collection instruments were pre-tested at one hospital and one health center that was not included in the study. During data collection, each checklist was validated for completeness.
Operational Definitions
A pulmonary tuberculosis patient who was smear-negative or culture-negative in the latest month of therapy and on at least one preceding occasion is considered cured. Treatment completed refers to a tuberculosis patient who finished treatment without evidence of failure but has no record demonstrating that sputum smear or culture results in the last month of treatment and on at least one previous occasion were negative, either because tests were not performed or because results are unavailable. A TB patient who has a positive sputum smear or culture at month 5 or later during therapy is considered to be in treatment failure.
TB defaulters are defined as tuberculosis patient who has discontinued anti-tb medication for eight weeks or longer and does not complete the treatment. Died refers to TB patients who died while getting TB treatment; the reason for death may or may not be connected to TB. Treatment success is the sum of cured and finished treatments. Adverse treatment outcomes are total treatment failure, default, and death.
Data Processing and Analysis
Data were entered into the SPSS version 23 statistical program for analysis after being checked for completeness and consistency. Descriptive statistics were used to investigate the background features. To investigate the association between the outcome variables and selected determinants, a backward stepwise logistic regression model was utilized. The variables recorded on the TB registration logbook were included in the logistic regression to evaluate determinants of adverse TB treatment outcomes. To adjust for all possible confounders, all variables with P 0.25 in the bivariable analysis were included in the final model of multivariate analysis. The Hosmer-Leme show statistic was used to assess the model’s goodness of fit. The multi-collinearity test was used to examine the association between independent variables using the variance infiltration component. The odds ratio with 95% CI was used to determine the direction and intensity of the statistical connection. As a measure of association, the odds ratio (OR) with a 95% confidence interval (CI) was computed. P-values of 0.05 or below were deemed statistically significant.
Results
Sociodemographic Characteristics
A total of 590 patient records were reviewed, with the mean age of the cases being 39.8 years with a standard deviation of 16.57, and the mean age of the controls being 33.45 years with a standard deviation of 14.06. The majority of the cases and controls were males, with 75 (63.8%) and 287 (60.8%) respectively. The majority of cases 64 (54.2%) and controls 346 (73.3%) were city dwellers (Table 1).
 |
Table 1 Socio-Demographic Characteristics of Study Participants in Jimma Town Health Facilities, Southwest Ethiopia, 2021 |
Clinical Related Characteristics
In the tuberculosis category, 113 (95.8%) and 447 (94.7%) were new TB cases and controls, respectively. In terms of TB type, 48 (40.7%) of cases and 198 (41.9%) of controls were pulmonary TB positive, while 32 (27.1%) of cases and 133 (28.2%) controls were extrapulmonary TB. More than two-thirds of cases 32 (66.7%) were positive for AFB in the second-month sputum, whereas the majority of controls 177 (89.4%) were negative. Regarding HIV test status, the majority of cases 62 (52.5%) were HIV positive, whereas the majority of controls 427 (90.5%) were HIV negative. In terms of nutritional status (BMI), the majority of patients 93 (78.8%) were malnourished, while the majority of controls 383 (81.1%) had normal nutritional status (Table 2). Regarding antiretroviral treatment (ART) treatment, the majority of patients 32 (51.6%), and controls 45 (100%) had begun ART. Only 11 (17.7%) of HIV-positive individuals among cases had started cotrimoxazole prophylaxis, whereas 44 (97.8%) of controls had started cotrimoxazole prophylaxis (Table 2).
 |
Table 2 Clinical-Related Characteristics of the Study Subjects in Jimma Town Health Facilities, Southwest Ethiopia, 2021 |
Determinants of Unsuccessful Treatment Outcomes
After adjusting for possible confounders, variables including age, HIV-positive status, malnutrition, and absence of contact person were significantly associated with unsuccessful treatment outcomes in the multivariable logistic regression model.
The study found that individuals older than 34.7 years were twice as likely as those younger than 34.7 years to have unsuccessful TB treatment outcomes (AOR=1.9; 95% CI:1.14–3.2).
Those who had no contact person at the time of TB treatment commencement were more likely to have unsuccessful therapy than those who had contact person (AOR= 27; 95% CI: 15.8–46.3).
Those who were HIV positive have 7 times higher unsuccessful TB treatment outcomes than those who were HIV negative (AOR= 7.3; 95% CI: 3.7–14.2). Those who were malnourished at the time of initiation of TB treatment had approximately 4.5 times more unsuccessful treatment outcomes than those who were normal nutritional status (AOR= 4.5; 95% CI: 1.5–12.9), and those whose nutritional status was unknown had 81% less unsuccessful TB treatment outcomes than those who were normal nutritional status (AOR=0.18; 95% CI: 0.07–0.5) (Table 3).
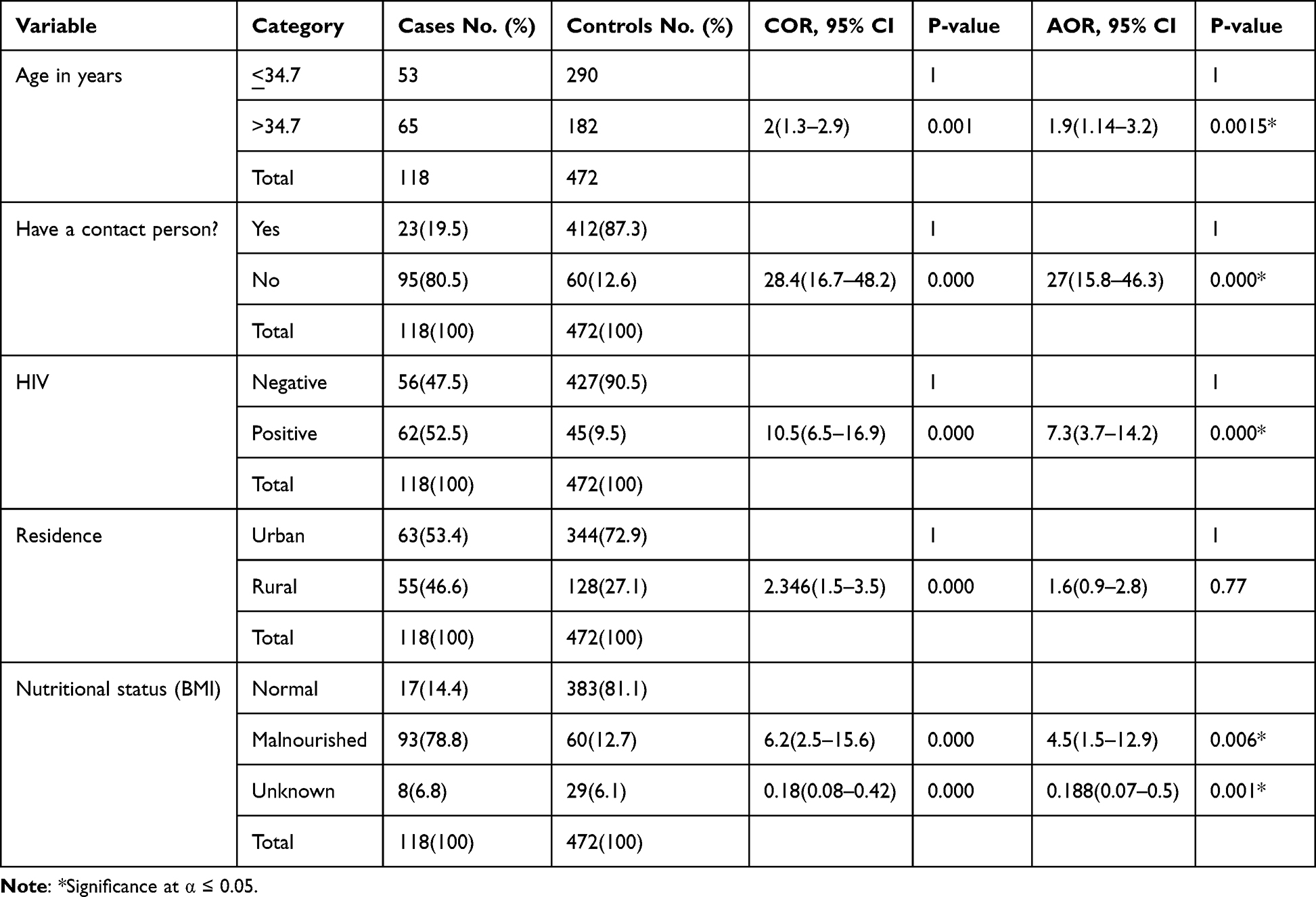 |
Table 3 Predictors of Unsuccessful Treatment Outcomes Among Patients on DOTS in Jimma Town Health Facilities, Southwest Ethiopia, 2021 |
Discussion
The purpose of this study was to identify the determinants of unsuccessful TB treatment outcomes among patients with DOTS in Jimma town health facilities, in southwest Ethiopia. According to this study factors such as age, HIV-positive status, malnutrition, and lack of contact were independent predictors of unsuccessful treatment outcomes. It is crystal clear that the finding from this study has paramount benefits to the policymakers as it plays a vital and pivotal role in enhancing the ways the patients in this cohort of treatment are handled. Thus, the finding serves as an alarming call for those stakeholders and researchers to further explore this essential area. We found that study participants aged greater than 34.7 years were 2 times more likely to have unsuccessful treatment outcomes than those aged ≤34.7. This finding agrees with the results of studies conducted in Tigray, Ethiopia,24 Arba Minch, Ethiopia,25 Eastern Ethiopia,14 South Africa,26 Malaysia,17 and China.27 The plausible rationale might be that older people frequently have comorbid ailments, have overall physiological decline with age, and are less able to access health care services.28 The older age group may have a high death rate due to co-morbidity, and recurrent exposure to therapy may result in poor treatment outcomes. This study showed that older persons should be prioritized in terms of policy since they are more likely to have unsatisfactory treatment outcomes. This is partially because the older the patients, their likelihood of coping the TB infections absolutely less.29,30
In this study, individuals who had no contact person at the time of starting TB treatment had a greater failure rate than those who had contact person. This finding is supported by findings from eastern Ethiopia14 and Somalia.31 The probable explanation is that having a contact person’s phone number allows participants to ask questions and acquire solutions, which can raise the success of treatment results. These studies also show that the lack of contact persons for patients at the time of commencing TB therapy was a significant cause of missed follow-up. As a result, it is critical to raise knowledge about the availability of a contact person at the time of commencing TB treatment for all TB patients at DOTS to improve treatment outcomes. Furthermore, healthcare professionals working in TB units must collect the cell phone numbers of contact persons regularly to allow effective tracing of patients during lost to follow-up time and the use of health extension workers for TB control programs.
We found that HIV-positive status is identified as a determinant of unsuccessful TB treatment outcomes. This finding is in line with studies done in Arba Minch and southern Ethiopia,25,32 and Ukraine.29 The failure of therapy in individuals with tuberculosis and HIV might be attributed to pill load, an increase in unpleasant effects, drug-to-drug interactions, immunological reconstitution inflammatory syndrome, and a risk factor for drug-resistant tuberculosis due to immune system suppression. HIV/AIDS counseling and testing should be performed regularly as part of patient monitoring while receiving DOT medication.
This study also showed those who were malnourished at the time of initiation of TB treatment were more likely to have unsuccessful treatment outcomes than those of normal nutritional status. This finding is supported by studies conducted in Addis Ababa,30 Malawi,33 and the Philippines.34 The likely explanation might be related to the malabsorption of major anti-TB medications, late diagnosis and treatment, and starvation, which means that their immunity was subsidized and makes it difficult for them to deal with the side effects of the drugs and comorbidities.35 “This study implies that programs and policies should place a greater emphasis on dealing with malnutrition to reduce the disease burden”. Furthermore, nutritional assessment, counseling, and management should be performed regularly as part of patient monitoring while undergoing DOT therapy.
Strengths and Limitations of the Study
The study’s limitations include the use of routine program data; consequently, the Ethiopian health institution TB logbook may not have a comprehensive enough checklist to determine the entire TB patients’ features, so, additional factors remain uninvestigated. Moreover, being the cases are very rare, as a solution, we employed cases to control the ratio into 1:4 which in turn may affect the statistical power of the study. The nature of the study participants, as well as the larger sample size, contribute to the research’s strength.
Conclusion
This study provides helpful insights into the determinants of failed tuberculosis treatment outcomes and has implications for enhancing treatment success in tuberculosis control programs. Age, lack of contact person, HIV-positive status, and malnutrition were all significant indicators of unsatisfactory tuberculosis treatment outcomes.
Data Sharing Statement
The data sets used in this investigation are accessible from the relevant authors upon reasonable request. After the defense, the thesis was uploaded to websites. Thus, the unpublished thesis paper is available on the Jimma University repository website (https://repository.ju.edu.et//handle/123456789/7956).
Ethical Approval
The Institutional Ethical Review Board Committee of Jimma University’s College of Health Sciences granted ethical approval. The ethical approval number was JHRPGN/2620. To gain access to patients’ data, a letter of consent was issued to Jimma town health institutions. Informed, voluntary, written, and signed consent was obtained from Jimma Health Institution administrators before the data collection. Since the study was based on secondary data, anonymity was maintained by using the medical registration number. Besides, all data extracted were kept confidential. Parental/legal guardian consent for participation in this study was obtained for all participants under the age of 18 years. The research was conducted per the Helsinki Declaration.
Acknowledgment
The authors would like to express their gratitude to Jimma University, the Jimma City health office, field supervisors, and data collectors for their assistance and contributions to this study.
Author Contributions
All authors contributed significantly to the work reported, whether in the conception, study design, execution, data acquisition, analysis, and interpretation, or all of these areas; participated in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article was submitted; and agree to be accountable for all aspects of the work.
Funding
Jimma University contributed to the funding of this study. However, the sponsor was not involved in data analysis, or interpretation, in the writing of the report and publication.
Disclosure
The authors report no competing interests in this work.
References
1. Migliori GB, Nardell E, Yedilbayev A, et al. Reducing tuberculosis transmission: a consensus document from the World Health Organization Regional Office for Europe. Eur Respir J. 2019;53(6):1900391. doi:10.1183/13993003.00391-2019
2. Migliori GB, Ong CW, Petrone L, D’Ambrosio L, Centis R, Goletti D. The definition of tuberculosis infection based on the spectrum of tuberculosis disease. Breathe. 2021;17(3):210079. doi:10.1183/20734735.0079-2021
3. Bagchi S. WHO’s global tuberculosis report 2022. Lancet Microbe. 2023;4(1):e20. doi:10.1016/S2666-5247(22)00359-7
4. World Health Organization. Global tuberculosis report 2022. License: CC BY-NC-SA 3.0 IGO. Geneva: World Health Organization; 2022.
5. Chakaya J, Khan M, Ntoumi F, et al. Global tuberculosis report 2020–Reflections on the global TB burden, treatment and prevention efforts. Int J Infect Dis. 2021;113:S7–S12. doi:10.1016/j.ijid.2021.02.107
6. Fukunaga R, Glaziou P, Harris JB, Date A, Floyd K, Kasaeva T. Epidemiology of tuberculosis and progress toward meeting global targets—worldwide, 2019. MMWR Morb Mortal Wkly Rep. 2021;70(12):427. doi:10.15585/mmwr.mm7012a4
7. World Health Organization. WHO global lists of high burden countries for tuberculosis (TB), TB/HIV and multidrug/rifampicin-resistant TB (MDR/RR-TB), 2021–2025: background document; 2021.
8. Tesfaye B, Alebel A, Gebrie A, Zegeye A, Tesema C, Kassie B. The twin epidemics: prevalence of TB/HIV co-infection and its associated factors in Ethiopia; A systematic review and meta-analysis. PLoS One. 2018;13(10):e0203986. doi:10.1371/journal.pone.0203986
9. Girum T, Muktar E, Lentiro K, Wondiye H, Shewangizaw M. Epidemiology of multidrug-resistant tuberculosis (MDR-TB) in Ethiopia: a systematic review and meta-analysis of the prevalence, determinants, and treatment outcome. Trop Dis Travel Med Vaccines. 2018;4:1–12. doi:10.1186/s40794-018-0065-5
10. McQuaid CF, McCreesh N, Read JM, et al. The potential impact of COVID-19-related disruption on tuberculosis burden. Eur Respir J. 2020;56(2):2001718. doi:10.1183/13993003.01718-2020
11. McQuaid CF, Vassall A, Cohen T, Fiekert K, White R, White RG. The impact of COVID-19 on TB: a review of the data. Int J Tuberc Lung Dis. 2021;25(6):436–446. doi:10.5588/ijtld.21.0148
12. Salaam-Blyther T. USAID Global Health Programs: FY2001-FY2012 Request. Washington DC: Congressional Research Service; 2011.
13. Tessema B, Muche A, Bekele A, Reissig D, Emmrich F, Sack U. Treatment outcome of tuberculosis patients at Gondar University Teaching Hospital, Northwest Ethiopia. A five-year retrospective study. BMC Public Health. 2009;9(1):1–8. doi:10.1186/1471-2458-9-371
14. Amante TD, Ahemed TA. Risk factors for unsuccessful tuberculosis treatment outcome (failure, default, and death) in public health institutions, Eastern Ethiopia. Pan Afr Med J. 2015;20:247. doi:10.11604/pamj.2015.20.247.3345
15. Getahun B, Ameni G, Medhin G, Biadgilign S. Treatment outcome of tuberculosis patients under directly observed treatment in Addis Ababa, Ethiopia. Braz J Infect Dis. 2013;17(5):521–528. doi:10.1016/j.bjid.2012.12.010
16. Endris M, Moges F, Belyhun Y, Woldehana E, Esmael A, Unakal C. Treatment outcome of tuberculosis patients at Enfraz Health Center, Northwest Ethiopia: a five-year retrospective study. Tuberc Res Treat. 2014;2014:1–7. doi:10.1155/2014/726193
17. Nik Nor Ronaidi NM, Mohd NS, Nik Rosmawati NH. Factors associated with unsuccessful treatment outcome of pulmonary tuberculosis in Kota Bharu, Kelantan. Malays J Public Health Med. 2011;2011:6–15.
18. Ejeta E, Beyene G, Balay G, Bonsa Z, Abebe G. Factors associated with unsuccessful treatment outcome in tuberculosis patients among refugees and their surrounding communities in Gambella Regional State, Ethiopia. PLoS One. 2018;13(10):e0205468. doi:10.1371/journal.pone.0205468
19. Chaulk C, Kazandjian V; Public Health Tuberculosis Guidelines Panel; Directly observed therapy for treatment completion of pulmonary tuberculosis: consensus statement of the Public Health Tuberculosis Guidelines Panel. JAMA. 1998;279(12):943–948. doi:10.1001/jama.279.12.943
20. Weis SE, Slocum PC, Blais FX, et al. The effect of directly observed therapy on the rates of drug resistance and relapse in tuberculosis. N Engl J Med. 1994;330(17):1179–1184. doi:10.1056/NEJM199404283301702
21. Fiseha D, Demissie M. Assessment of Directly Observed Therapy (DOT) following tuberculosis regimen change in Addis Ababa, Ethiopia: a qualitative study. BMC Infect Dis. 2015;15(1):405. doi:10.1186/s12879-015-1142-2
22. Queiroz EM, De-la-torre-ugarte-guanilo MC, Ferreira KR, Bertolozzi MR. Tuberculosis: limitations and strengths of directly observed treatment short-course. Rev Lat Am Enfermagem. 2012;20(2):369–377. doi:10.1590/S0104-11692012000200021
23. Chakaya J, Petersen E, Nantanda R, et al. The WHO global tuberculosis 2021 report–not-so-good news and turning the tide back to End TB. Int J Infect Dis. 2022;124:S26–S29. doi:10.1016/j.ijid.2022.03.011
24. Berhe G, Enquselassie F, Aseffa A. Treatment outcome of smear-positive pulmonary tuberculosis patients in Tigray Region, Northern Ethiopia. BMC Public Health. 2012;12(1):1–9. doi:10.1186/1471-2458-12-537
25. Dale D, Nega D, Yimam B, Ali E. Predictors of poor tuberculosis treatment outcome at Arba Minch General Hospital, Southern Ethiopia: a case-control study. J Tuberc Ther. 2017;2(110):2.
26. Azeez A, Ndege J, Mutambayi R. Associated factors with unsuccessful tuberculosis treatment outcomes among tuberculosis/HIV coinfected patients with drug-resistant tuberculosis. Int J Mycobacteriol. 2018;7(4):347–354. doi:10.4103/ijmy.ijmy_140_18
27. Chen C, Zhu L, Yang D, et al. Risk factors associated with TB, a case-control study in a Chinese population. J Public Health Emerg. 2017;1(6):58. doi:10.21037/jphe.2017.05.09
28. Daniels O, Oladapo O, Alausa O. Default from a tuberculosis treatment program in Sagamu, Nigeria. Niger J Med. 2006;15(1):63–67. doi:10.4314/njm.v15i1.37119
29. Aibana O, Slavuckij A, Bachmaha M, et al. Patient predictors of poor drug-sensitive tuberculosis treatment outcomes in Kyiv Oblast, Ukraine. F1000Research. 2017;6:1873. doi:10.12688/f1000research.12687.1
30. Sahile Z, Tezera R, Haile Mariam D, Collins J, Ali JH. Nutritional status and TB treatment outcomes in Addis Ababa, Ethiopia: an ambi-directional cohort study. PLoS One. 2021;16(3):e0247945. doi:10.1371/journal.pone.0247945
31. Ali MK, Karanja S, Karama M. Factors associated with tuberculosis treatment outcomes among tuberculosis patients attending tuberculosis treatment centers in 2016–2017 in Mogadishu, Somalia. Pan Afr Med J. 2017;28(1). doi:10.11604/pamj.2017.28.197.13439
32. Shaweno D, Worku A. Tuberculosis treatment survival of HIV positive TB patients on directly observed treatment short-course in Southern Ethiopia: a retrospective cohort study. BMC Res Notes. 2012;5(1):1–8. doi:10.1186/1756-0500-5-682
33. Zachariah R, Spielmann M, Harries A, Salaniponi F. Moderate to severe malnutrition in patients with tuberculosis is a risk factor associated with early death. Trans R Soc Trop Med Hyg. 2002;96(3):291–294. doi:10.1016/S0035-9203(02)90103-3
34. White LV, Edwards T, Lee N, et al. Patterns and predictors of co-morbidities in Tuberculosis: a cross-sectional study in the Philippines. Sci Rep. 2020;10(1):4100. doi:10.1038/s41598-020-60942-2
35. Seid G, Ayele M. Undernutrition and mortality among adult tuberculosis patients in Addis Ababa, Ethiopia. Adv Prev Med. 2020;2020:1–9. doi:10.1155/2020/5238010
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.