Back to Journals » Journal of Asthma and Allergy » Volume 15
Determinants of Severe Asthma – A Long-Term Cohort Study in Northern Sweden
Authors Backman H ![]() , Stridsman C
, Stridsman C ![]() , Hedman L, Rönnebjerg L
, Hedman L, Rönnebjerg L ![]() , Nwaru BI
, Nwaru BI ![]() , Sandström T, Kankaanranta H
, Sandström T, Kankaanranta H ![]() , Lindberg A
, Lindberg A ![]() , Rönmark E
, Rönmark E
Received 31 May 2022
Accepted for publication 30 August 2022
Published 10 October 2022 Volume 2022:15 Pages 1429—1439
DOI https://doi.org/10.2147/JAA.S376806
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Helena Backman,1 Caroline Stridsman,2 Linnea Hedman,1 Lina Rönnebjerg,3 Bright I Nwaru,3,4 Thomas Sandström,2 Hannu Kankaanranta,3,5,6 Anne Lindberg,2 Eva Rönmark1
1Department of Public Health and Clinical Medicine, Section of Sustainable Health/the OLIN unit, Umeå University, Umeå, Sweden; 2Department of Public Health and Clinical Medicine, Section of Medicine/the OLIN unit, Umeå University, Umeå, Sweden; 3Krefting Research Centre, Institute of Medicine, University of Gothenburg, Gothenburg, Sweden; 4Wallenberg Centre for Molecular and Translational Medicine, Institute of Medicine, University of Gothenburg, Gothenburg, Sweden; 5Department of Respiratory Medicine, Seinäjoki Central Hospital, Seinäjoki, Finland; 6Faculty of Medicine and Health Technology, Tampere University, Tampere, Finland
Correspondence: Helena Backman, Department of Public Health and Clinical Medicine, Section of Sustainable Health/the OLIN Unit, Umeå University, Umeå, Sweden, Email [email protected]
Background: Risk factors for severe asthma are not well described. The aim was to identify clinical characteristics and risk factors at study entry that are associated with severe asthma at follow-up in a long-term prospective population-based cohort study of adults with asthma.
Methods: Between 1986 and 2001, 2055 adults with asthma were identified by clinical examinations of population-based samples in northern Sweden. During 2012– 2014, n = 1006 (71% of invited) were still alive, residing in the study area and participated in a follow-up, of which 40 were identified as having severe asthma according to ERS/ATS, 131 according to GINA, while 875 had other asthma. The mean follow-up time was 18.7 years.
Results: Obesity at study entry and adult-onset asthma were associated with severe asthma at follow-up. While severe asthma was more common in those with adult-onset asthma in both men and women, the association with obesity was observed in women only. Sensitization to mites and moulds, but not to other allergens, as well as NSAID-related respiratory symptoms was more common in severe asthma than in other asthma. Participants with severe asthma at follow-up had lower FEV1, more pronounced FEV1 reversibility, and more wheeze, dyspnea and nighttime awakenings already at study entry than those with other asthma.
Conclusion: Adult-onset asthma is an important risk factor for development of severe asthma in adults, and obesity increased the risk among women. The high burden of respiratory symptoms already at study entry also indicate long-term associations with development of severe asthma.
Keywords: epidemiology, phenotype, precision medicine, prognosis, risk factors
Introduction
The prevalence of severe asthma among adults with asthma has been estimated at 4–8% according to most studies,1–6 and the European Respiratory Society (ERS) summarizes it to be 3–10%.7 The prevalence estimates of severe asthma mainly depend on the criteria used: the ERS/ATS definition gives a lower prevalence8 than the GINA definition.9 The prevalence of difficult-to-treat severe asthma in adults with asthma is even lower.2 According to several studies, severe asthma is more common among women than men.1,2,6,10
Despite similarities in clinical presentation, severe asthma is not a single disease entity, and several different clinically relevant phenotypes have been identified.10–12 Suggested risk factors for severe asthma include environmental pollutants, occupational exposures, active and passive smoking, and obesity.13–16 Both hypothesis-driven and computational approaches such as cluster analysis have previously revealed three major phenotypes of severe asthma;12 childhood-onset allergic,17,18 adult-onset eosinophilic with persistent airflow limitation,19 and adult-onset with obesity which often is non-atopic and occurs predominantly in women.17,20,21 As a consequence of the heterogeneity, the risk factor patterns differ, however a few factors act as risks for several phenotypes, for instance family history of asthma.12,16 However, risk factors for severe asthma are still not well identified and it is unknown why some adults with asthma develop severe disease whereas others do not, a subject for which long-term prospective studies are particularly suitable.
Thus, we aimed to identify clinical characteristics and risk factors at study entry that are associated with severe asthma at follow-up in a long-term prospective population-based cohort study of adults with asthma.
Materials and Methods
Study Population
Study Entry in 1986–2001
The Obstructive Lung Disease in Northern Sweden (OLIN) is an epidemiological research program ongoing since 1985. The OLIN asthma cohort (n = 2055) includes adults with asthma identified at clinical examinations performed between 1986 and 2001, from four cohorts originally sampled from the population register and a fifth cohort of adults with incident asthma, as previously described in detail.22
The examinations at study entry included structured interviews with validated questions about obstructive lung diseases, respiratory symptoms and their triggers as well as potential risk factors for airway disease.23 Spirometry was performed in all participants. Subsamples participated in skin prick testing, reversibility testing and methacholine challenge. In the four original population cohorts, the criteria for reversibility testing was a FEV1<85% in one cohort, and either FEV1/VC<0.70 or FEV1<90% in the other three cohorts.22 In addition, subsamples from three of the population cohorts and all subjects in the fifth cohort were invited to methacholine challenge.22,24
Follow-Up in 2012–2014
All participants in the asthma cohort who were alive and still living in Norrbotten were invited to a clinical follow-up in 2012–2014. The examinations included a structured interview with detailed assessment of asthma treatment during the last 12 months, pre- and post-bronchodilator spirometry in line with current guidelines,25 blood sampling and skin prick testing.4 Of the 1425 invited, 1006 (71%) participated.22
Definitions
Information Collected at Study Entry
Smoking habits: were categorized as current smokers, ex-smokers and never-smokers. Ex-smokers were defined as those who had smoked for at least one year but not during the last 12 months.
Socioeconomic status: was grouped according to classifications by Statistics Sweden based on the most recent occupation (Table 1), where manual workers are considered having the lowest status and professionals and executives the highest.
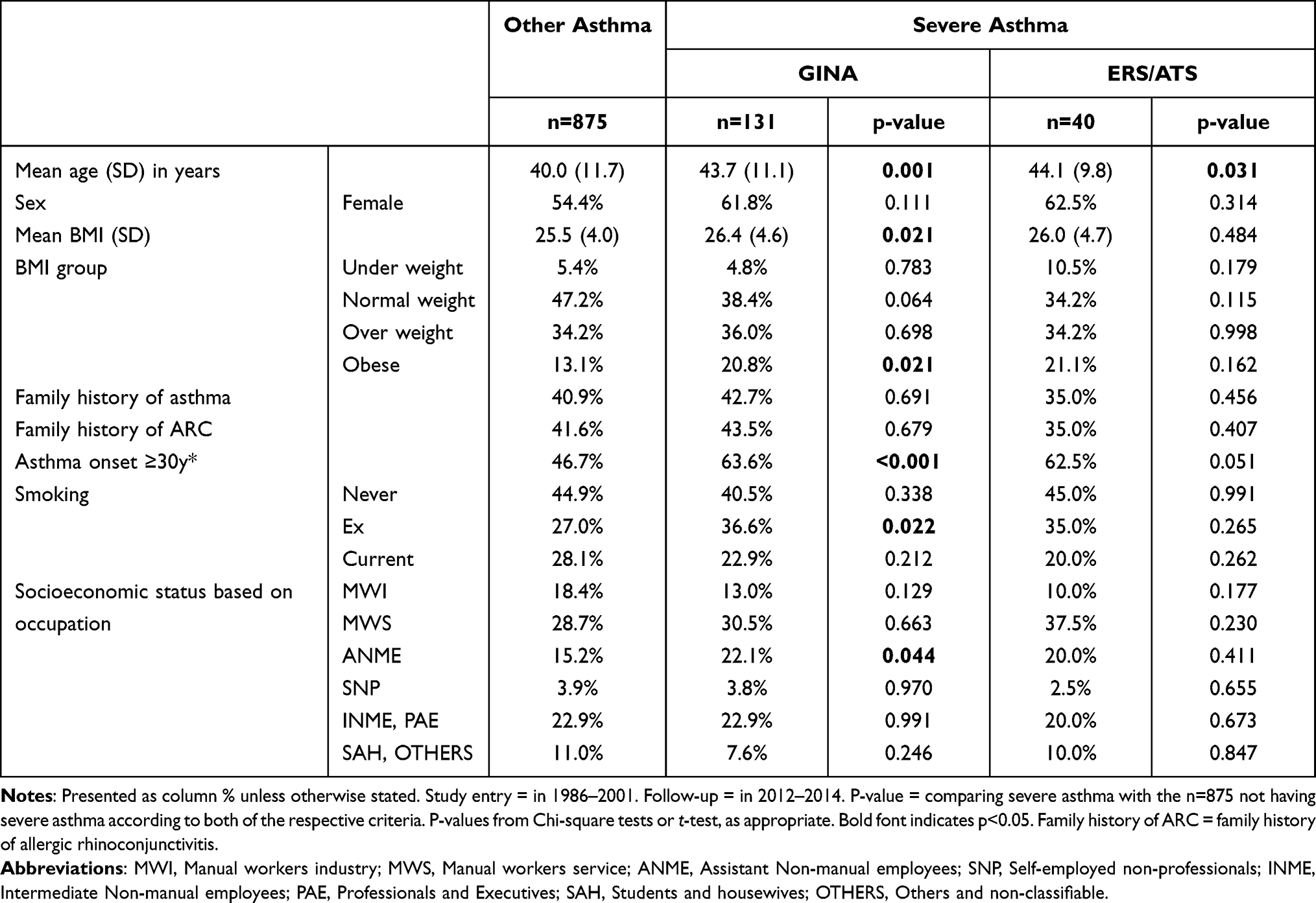 |
Table 1 Demography at Study Entry Among Those with and without Severe Asthma at Follow-Up, According to Two Different definitions of Severe Asthma |
BMI (weight/(height2)): body mass index was categorized as underweight (BMI < 20), normal weight (BMI 20.0–24.9), overweight (BMI 25.0–29.9) and obesity (BMI ≥ 30).
Adult onset asthma was defined as an onset ≥30 years of age.
Triggers for respiratory symptoms: The participants were asked if any of the following ten individual factors triggered their respiratory symptoms: furred animals, pollen, moulds, tobacco smoke, dust, strong scents, traffic exhaust, respiratory infections, cold air or physical activities. The number of triggers (0–10) was also summarized for each participant.
Spirometry results: the OLIN reference values for spirometry26 were used to calculate percent (%) of predicted, Z-scores and lower limits of normal (LLN, defined as the fifth percentile).
Reversibility: was assessed using two different cut-offs for increase in FEV1 after bronchodilation; ≥12% and 200mL, and ≥20%, respectively.
Hyperreactivity: In two cohorts hyperreactivity was defined as a provocation concentration causing ≥20% decrease in FEV1 (PC20)≤2mg/mL methacholine-chloride,27 and PC20≤8mg/mL in the other cohorts,23 which are comparable as different methods were used.
Allergic sensitization: was assessed by skin prick tests for a panel of ten airborne allergens: three pollens (birch, timothy, mugwort), three furred animals (cat, dog, horse), two dust mites (D. Pteronysinus, D. Farinae) and two moulds (Cladosporium, Altenara). A mean wheal diameter of ≥3mm was considered positive.
Information Collected at Follow-Up
Severe asthma according to the ERS/ATS-definition:8 “High dose inhaled corticosteroids (ICS) plus a second controller (and/or systemic corticosteroids)” is required “to prevent asthma from becoming uncontrolled or which remains uncontrolled despite this therapy”. High dose ICS was defined in line with the ERS/ATS-definition.
Severe asthma according to the GINA-definition:9 Asthma on GINA treatment step 4 or 5, ie medium to high dose ICS with at least one second controller and/or OCS.
Uncontrolled severe asthma was defined as severe asthma with at least one of the following: (a) Asthma Control Test (ACT) score < 20, (b) ≥3 bursts of OCS in the previous year, (c) ≥1 hospitalization or urgent care visit in the previous year due to asthma, and (d) FEV1<80% of predicted and FEV1/FVC<LLN.9
NSAID-related respiratory symptoms: was defined as breathing difficulties within three hours after taking nonsteroidal anti-inflammatory drugs (NSAID).
Allergic sensitization at follow-up: was measured in blood (IgE) using the ImmunoCap Phadiatop with 0.35 kU/L as cut-off. Sensitization to specific allergens were tested among those with a positive Phadiatop, including the same allergens as at study entry with the addition of Aspergillus fumigatus.
Statistical Analyses
Statistical analyses were performed with the IBM Statistical Package for the Social Sciences Statistics 26. In bivariate analyses, the Chi-square test was used to test for differences in proportions and Student’s t-test for differences in means between two groups. A p-value < 0.05 was considered statistically significant. Poisson regression with robust errors was utilized to calculate risk ratios (RR) with 95% confidence intervals (CI) for associations with severe asthma according to GINA at follow-up. In attempt to avoid misclassification of severe asthma at follow-up, models with uncontrolled severe asthma as outcome (ie excluding controlled severe asthma) were also constructed. In attempt to exclude severe asthma at study entry and thereby focusing only on cases debuting with severe asthma during follow-up, the regression analyses were also performed by excluding all participants that were using ICS at study entry. To account for different time points of study entry, all regression models were adjusted for initial cohort (1–5), and the follow-up time was included as an offset variable in the models. Due to low number of cases, severe asthma according to ERS/ATS at follow-up was not assessed by multivariable analysis.
Results
Demography and Risk Factors
Among the 1006 participants, the mean follow-up time was 18.7 years (min-max 10–28 years), and 131 had GINA-defined severe asthma and 40 ERS/ATS severe asthma during follow-up (and by definition, all with ERS/ATS severe asthma also had severe asthma according to GINA). Data on asthma medication use at follow-up is presented in Supplementary Table S1. In total, 92.5% in ERS/ATS severe asthma and 70.2% in GINA-defined severe asthma had uncontrolled asthma. Ex-smoking was slightly more common in GINA severe asthma, while no significant differences compared to other asthma were seen with regards to sex, heredity for asthma and allergy, current or never-smoking and socioeconomic status based on occupation, with the exception of assistant non-manual employees (Table 1).
Obesity at study entry was more common among those having severe asthma at follow-up according to GINA (20.8%, p = 0.021) and ERS/ATS (21.1%, p = 0.162) compared to other asthma (13.1%), a finding driven by women and not by men (Figure 1). Of the n = 138 with obesity at study entry, only 3 (2.2%) had BMI < 25 at follow-up (and all those 3 had other asthma). Asthma with onset ≥30 years of age was more common in severe asthma according to GINA (Table 1, Figure 1), significantly so among both women (65.8% in severe asthma vs 51.6% in other asthma, p = 0.019) and men (60.0% in severe asthma vs 40.9% in other asthma, p = 0.010). In a regression model including age, sex, smoking and BMI categories, obesity at study entry was the dominating risk factor for severe asthma according to GINA with an adjusted RR of 1.62 (95% CI 1.03–2.55) compared to other asthma. As asthma onset at age ≥30 years associated with severe asthma in unadjusted analyses (Table 1), it was added to the model (instead of age) and yielded RR 1.52 (1.06–2.17) (Table 2). Also when excluding all participants using ICS at study entry, both obesity and asthma onset at age ≥30 years remained significantly associated with severe asthma as well as with severe uncontrolled asthma at follow-up (Table 2).
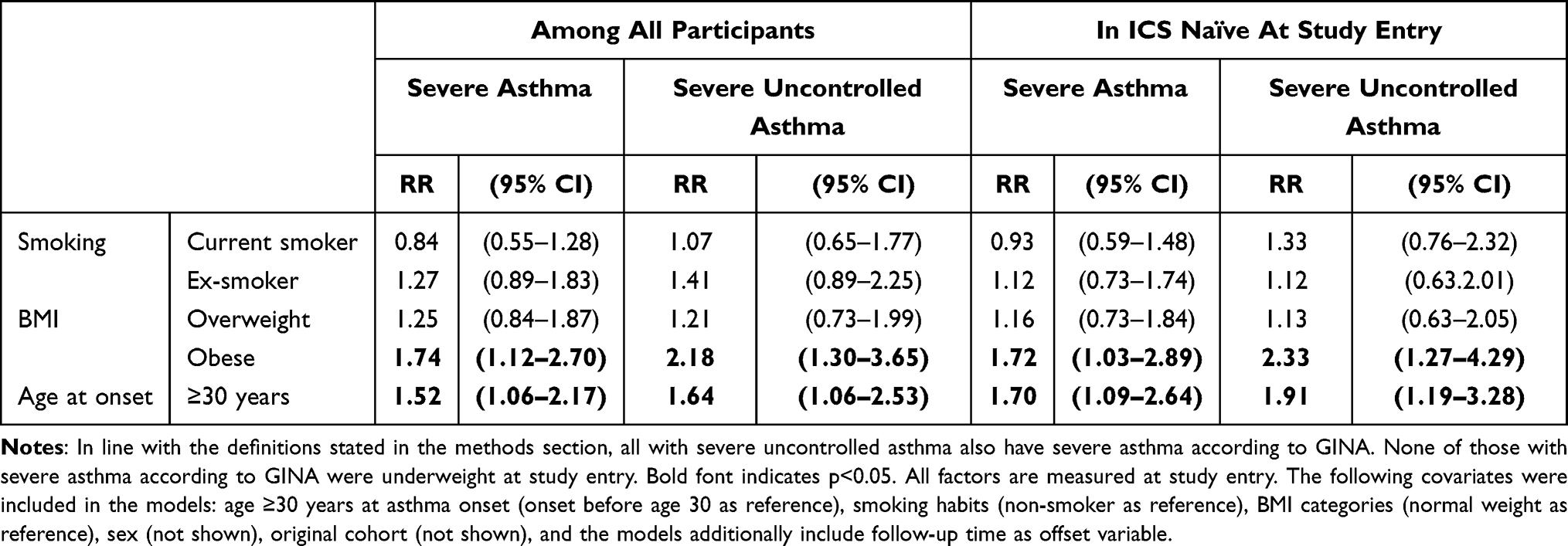 |
Table 2 Factors Assessed at Study Entry in Association with Severe Asthma According to GINA and Severe Uncontrolled Asthma at Follow-Up, Among All Participants and Exclusively in Participants That Were ICS Naïve at Study Entry. Analyzed by Poisson Regression, with Results Presented as Risk Ratios (RR) with 95% Confidence Intervals (95% CI), Including Other Asthma as Reference Category |
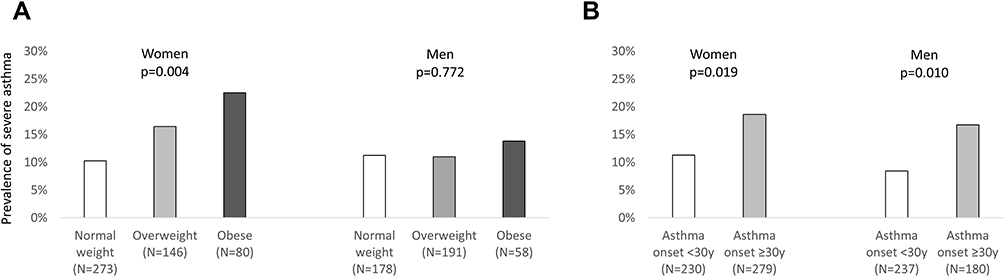 |
Figure 1 Prevalence (%) of severe asthma according to GINA at follow-up, stratified by (A) sex and BMI group at study entry (p from test-for-trend), and (B) sex and age at asthma onset (p from chi-square test). Participants with underweight are excluded due to low numbers. |
Lung Function
Mean FEV1 as well as FVC, both in terms of percent of predicted and Z-scores, were substantially lower at study entry among those with severe asthma at follow-up. The proportion having FEV1<80% of predicted was higher in severe asthma according to GINA (45.7%, p < 0.001) and ERS/ATS (50.0%, p < 0.001) compared to other asthma (20.3%). The proportions with FEV1 reversibility, both defined as increase >12% and 200mL, and >20%, was higher in severe asthma according to both GINA (22.7%, p = 0.002, and 20.4%, p < 0.001, respectively) and ERS/ATS (23.3%, p = 0.035, and 22.2%, p < 0.001, respectively) compared to other asthma (14.7% and 3.3%, respectively). The proportions with hyperreactivity were 87.7% in GINA severe asthma. 94.7% in ERS/ATS severe asthma, and 79.0% in other asthma (Table 3).
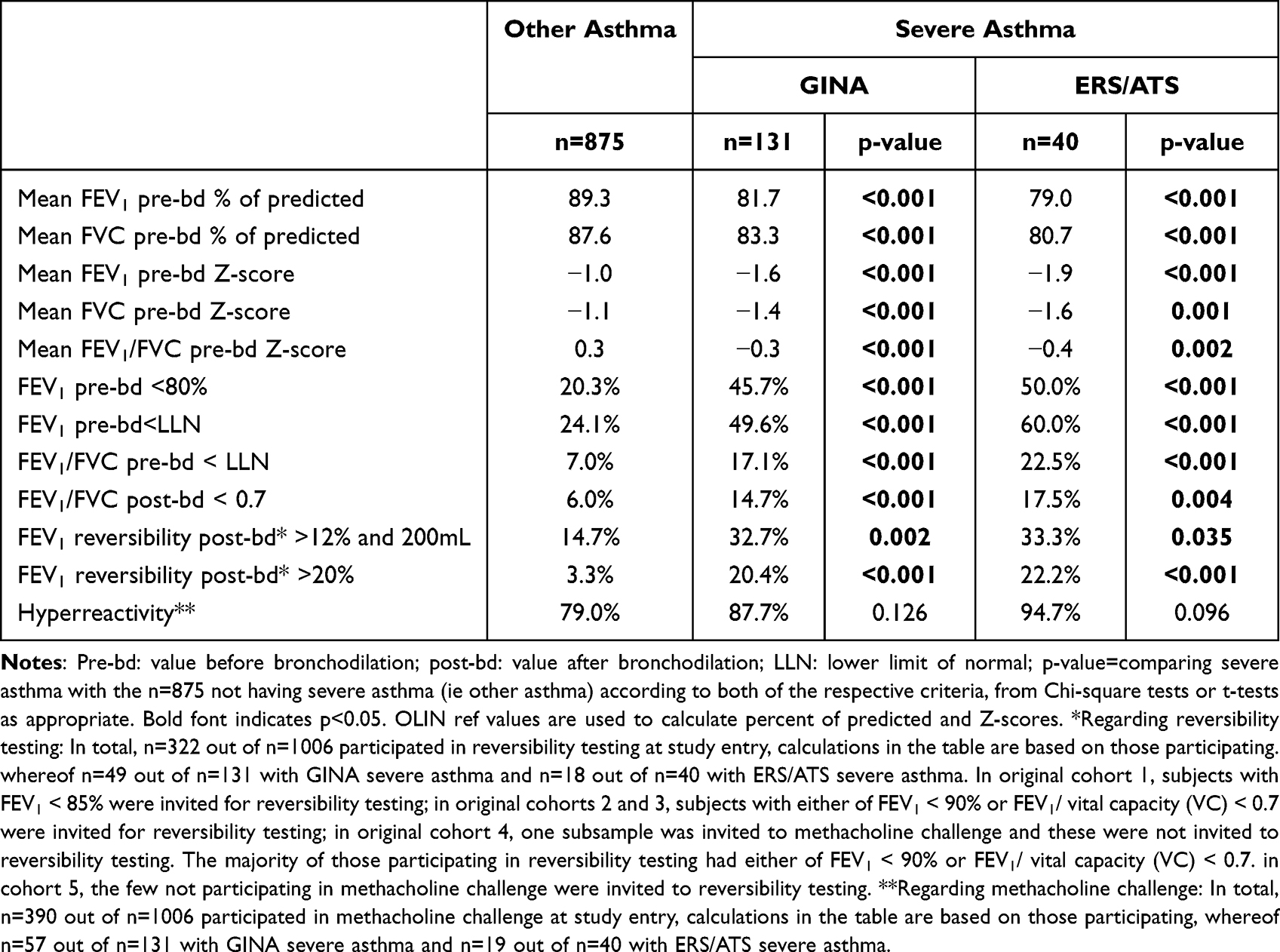 |
Table 3 Lung Function at Study Entry Among Those with and without Severe Asthma at Follow-Up |
When lung function measures were added one at the time to a regression model including age, sex, smoking and BMI categories, the following RR (95% CI) for severe asthma were estimated: 3.85 (1.95–7.62) for >20% FEV1 reversibility, 2.62 (1.86–3.69) for FEV1<80% of predicted, 2.28 (1.63–3.20) for FEV1<LLN, and 1.82 (1.05–3.17) for >12% and 200mL FEV1 reversibility (Figure 2).
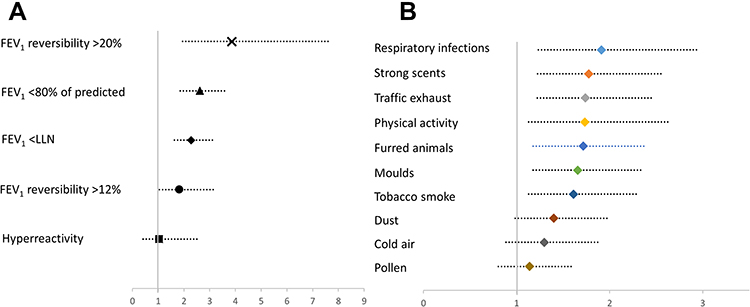 |
Figure 2 Association between (A) lung function measures, and (B) triggers for respiratory symptoms at study entry and severe asthma according to GINA at follow-up. Results expressed as risk ratios with 95% CI adjusted for age, sex, smoking and BMI categories. |
Respiratory Symptoms, Treatment and Comorbid Conditions
Asthmatic wheeze, persistent wheeze, dyspnea, attacks of shortness of breath and nighttime awakenings at study entry were more common among those with severe asthma at follow-up, while longstanding cough and productive cough were not (Table 2). Regarding comorbidities at study entry, no statistically significant differences were seen with regards to eczema, nasal polyps or ischemic heart disease, while rhinitis was more common in GINA severe asthma than in other asthma. The opposite was found for hay fever, which was less common in ERS/ATS severe asthma and tended to be less common in GINA severe asthma than in other asthma (Table 4).
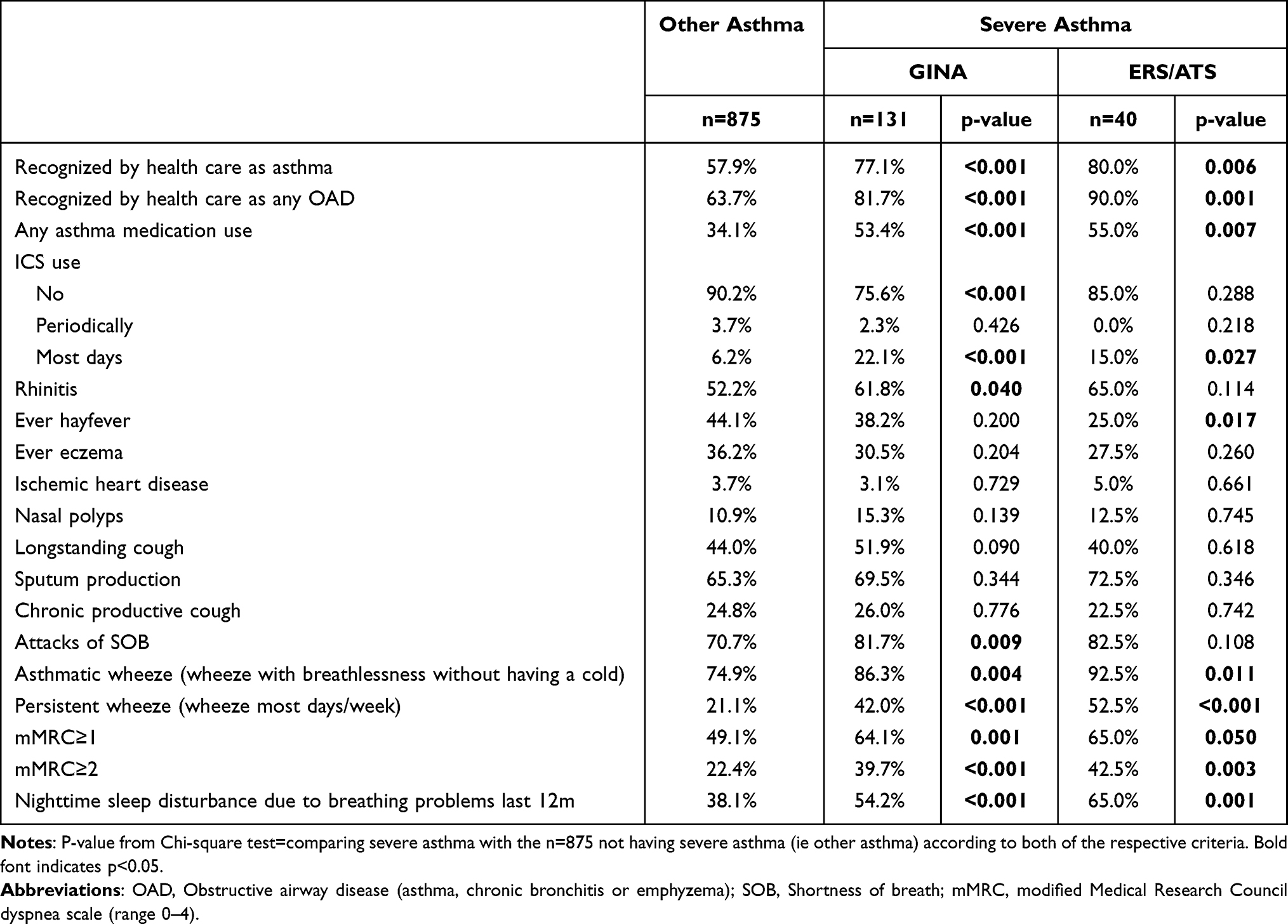 |
Table 4 Clinical Characteristics (%) at Study Entry Among Those with and without Severe Asthma at Follow-Up, According to Two Different Definitions of Severe Asthma |
At follow-up, allergic sensitization tended to be less common in severe asthma, with the exceptions of mites and moulds, especially aspergillus and alternaria, which were more common in severe asthma. Multisensitization was also more common in severe than other asthma (Supplementary Tables S2 and S3). Further, 12.5% (p = 0.005) in ERS/ATS severe asthma and 9.2% (p = 0.003) in GINA severe asthma had NSAID-related respiratory symptoms at follow-up, compared to 3.6% in other asthma. Both blood eosinophils and neutrophils were higher in GINA severe asthma than in other asthma (Supplementary Table S3).
Trigger Factors
Those with severe asthma reported that their respiratory symptoms were triggered by a greater number of different factors at study entry compared to other asthma (Supplementary Figure S1). As individual factors, furred animals, moulds, tobacco smoke, dust, strong scents, traffic exhaust, respiratory infections and physical activities were reported more frequently in GINA severe asthma than in other asthma (Table 5). The individual triggers for respiratory symptoms were added one-by-one to a regression model including age, sex, smoking and BMI categories, in which respiratory infections, strong scents, traffic exhaust, physical activity, furred animals, moulds, and tobacco smoke yielded RRs in the 1.6–1.9 range with p < 0.05 (Figure 2).
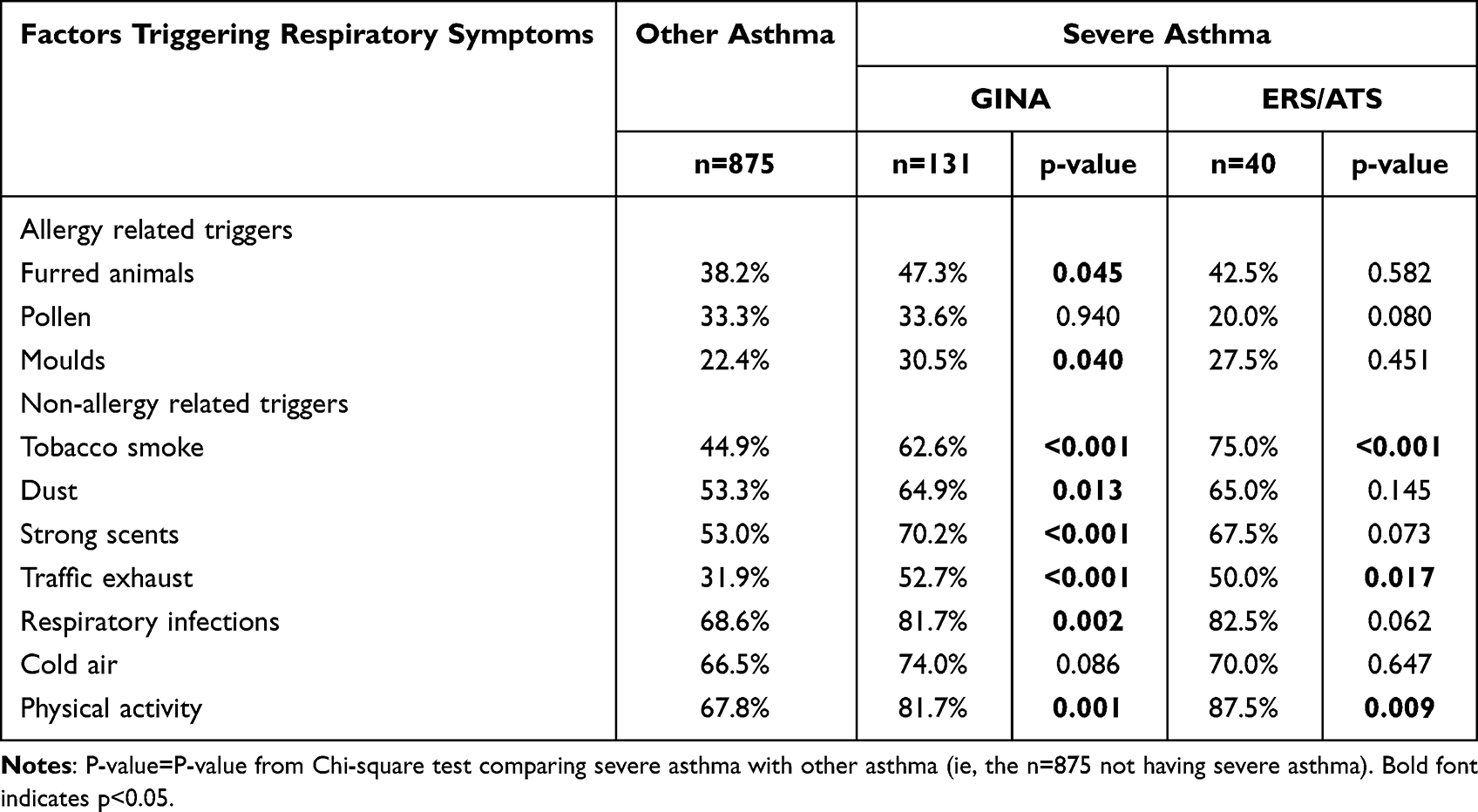 |
Table 5 Factors That Triggered Respiratory Symptoms at Study Entry Among Those with and without Severe Asthma at Follow-Up |
Discussion
The main findings were that obesity at study entry and adult onset asthma were associated with an increased risk of severe asthma after 18 years of follow-up. Severe asthma was more common in individuals with adult-onset asthma in both men and women, while obesity was associated with severe asthma only in women. Participants with severe asthma at follow-up also had lower FEV1 and more pronounced FEV1 reversibility, as well as more wheeze, nighttime awakenings and dyspnea than adults with other asthma at study entry, ie already 10–28 years earlier. Further, those with severe asthma were more frequently multi-sensitized to airborne allergens, presented with mite or mould sensitization, and reported a greater number of different factors which triggered their symptoms compared to those with other asthma.
Obesity is known to associate with a more severe asthma in adults,28–30 and the adult female obese phenotype of severe asthma has also previously been characterized,17,20,21 but our observed associations between obesity and the development of severe asthma after 18 years of follow-up are novel. It is certainly noteworthy that this association with obesity only was observed among women and not among men. The pathways between obesity and asthma may be linked to the metabolic syndrome,31 with molecular consequences of insulin affecting both the structure and function of the lungs.32 We could speculate that women, whose airways are smaller and whose lung function more affected by tobacco smoke,33 probably are vulnerable also to other exposures, and that also hormonal aspects may contribute.34
In our study, adult-onset asthma was a risk factor for severe asthma among both women and men. Compared to asthma with onset in childhood, adult onset asthma is often associated with comorbid conditions and less responsive to ICS treatment,8,9 and there are also indications of particularly poor prognosis with limited remission.29,35 As it is known that obesity is associated with adult onset asthma,24 we also explored age at onset in relation to BMI, and found that adult onset was less related to high BMI at study entry in severe asthma than in other asthma (Supplementary Table S4). The results from the adjusted regression analyses also suggested independent associations between each of obesity and adult onset for development of severe asthma. Thus, taken all together, our results indicate that obesity and age at onset act as independent risk factors with regards to long-term associations with severe asthma among adults.
Our results on long-term associations are also well in line with other previously identified phenotypes of severe asthma such as the adult-onset eosinophilic with persistent airflow limitation.19 In cross-sectional studies, severe asthma is often associated with impaired lung function and/or more symptoms despite high dose ICS treatment,8,9 and our cohort study showed that already at study entry these treatable traits were more common in those having severe asthma at follow-up. Results from eg, the severe asthma research program (SARP) has particularly highlighted the importance of assessing FEV1 before and after bronchodilation as these clinical characteristics, along with age at onset, with 80% accuracy could determine phenotype and severity of asthma in the SARP sample, and thereby likely also treatment response.17 Occupation-related,15,36 and smoking-associated and neutrophilic37 severe asthma are other previously suggested phenotypes with high symptom burden and impaired lung function, but as our cohort includes adults presenting with asthma already at study entry, it is selected in such a way that causality with regards to occupational aspects cannot be assessed. However, when taken together, some of these findings highlight a possibility of primary or secondary prevention eg, along the lines of improved diet, physical activity, smoking cessation and preventive measures regarding smoking initiation, where also socioeconomy may play a role.9,38,39
Mite and mould sensitization, as well as multi-sensitization, was most common in severe asthma in our study, in line with previously identified phenotypes of severe asthma.10–12,18,29,40 Particularly sensitization to Aspergillus and Alternaria4,39 was more common in severe asthma than in other asthma in our study, as well as higher prevalence of NSAID-intolerance.41 We further explored sensitization patterns in relation to age at asthma onset and found that, in line with previous findings,42 sensitization was more common among those with asthma onset earlier in life, both in severe and other asthma. Further, our findings also align with recent results showing that early onset of sensitization is associated with both higher IgE levels and multi-sensitization.43 The relatively great proportion with high levels of blood eosinophils indeed open the doors for new effective treatment, while we still lack effective treatment for those with neutrophil related asthma.9
Studies investigating triggering factors among individuals with severe asthma are important to enable preventive measures, precision medicine and personalized care. Individuals with severe asthma reported a greater number of different factors triggering their symptoms at study entry. Avoidance of these factors most likely have a beneficial effect on the disease course for the affected individuals. And further, we would like to highlight the importance of accurately identifying44 and managing45 severe asthma, in order to enable equal and appropriate care.
The strengths of our study include the population-based design, enabling estimations of long-term real-world associations, and use of the same validated methods both at recruitment and follow-up. Furthermore, patients reporting high dose ICS or OCS as maintenance treatment at follow-up underwent additional detailed clinical examinations including evaluation of treatment and treatment adherence, inhalation technique, and assessment of comorbidities. Regarding weaknesses, the recognition of asthma has improved and treatment regimens have changed during the study period, factors that may have affected the results as early initiation of treatment has major effects on lung function and the development of disease. The follow-up time differed substantially between participants, which we addressed by adjusting for both original cohort and follow-up duration in the regression models. The study was performed before the introduction of biological treatments for severe asthma, and thus these have not been evaluated and have not impacted the results. Further, as the data regarding asthma medication use was not detailed enough at study entry, we could not distinguish severe asthma already at study entry according to modern guidelines. In attempt to account for this, we performed the risk factor analysis both among all participants and exclusively among those being ICS naïve at study entry, and the results thereof confirmed our main findings. Further, the main findings on associations with obesity and adult onset were also confirmed when only focusing on severe asthma that was uncontrolled.
Conclusions
Obesity and asthma onset in adulthood increased the risk for developing severe asthma after 18 years of follow-up. While severe asthma was more common in those with adult-onset asthma in both men and women, obesity was a risk factor for development of severe asthma only among women. Higher levels of blood eosinophils and neutrophils were observed, and both sensitization to mites and moulds and multi-sensitization was more common in severe asthma than in other asthma, and so was NSAID exacerbated asthma. Further, the high burden of respiratory symptoms and lower lung function already at study entry also indicate long-term associations with development of severe asthma.
Abbreviations
ACT, Asthma Control Test; ATS, American Thoracic Society; ARC, Allergic rhinoconjunctivitis; BMI, Body Mass Index; CI, Confidence Interval; ERS, European Respiratory Society; FEV1, Forced expiratory volume in 1 second; GINA, Global Initiative for Asthma; ICS, Inhaled Corticosteroids; IGE, Immunoglobulin E; LLN, Lower Limit of Normal; mMRC, modified Medical Research Council dyspnea scale; NSAID, Nonsteroidal anti-inflammatory drug; OAD, Obstructive airway disease (asthma, chronic bronchitis or emphyzema); OCS, Oral Corticosteroids; OLIN, Obstructive Lung Disease in Northern Sweden; PC20, Provocation concentration causing ≥20% decrease in FEV1; PRE-BD, before bronchodilation; RR, Risk Ratio; SD, Standard Deviation; SOB, Shortness of breath; VC, Vital Capacity.
Data Sharing Statement
The dataset used and analysed during the current study is available from the corresponding author on reasonable request and with ethical permission.
Ethics Approval and Consent to Participate
The study was approved by the Regional Ethical Review Board at Umeå University. Informed consent was obtained at the time of examinations. The study complies with the declaration of Helsinki.
Acknowledgments
We would like to acknowledge the participants in the study. Also the research staff within the OLIN-studies is acknowledged for their excellent work. We thank the funding bodies for financial support, as described elsewhere. Finally, we would especially like to acknowledge the invaluable support by Professor Bo Lundbäck, founder of the OLIN-studies.
Funding
Unrestricted financial support was received mainly from The Swedish Heart & Lung Foundation, The Swedish Research Council, a regional agreement between Umeå University and Västerbotten County Council (ALF), Norrbotten County Council, the Swedish Asthma-Allergy Foundation, and VISARE NORR Fund: Northern county councils Regional federation. Additional unrestricted support was provided by ThermoFisher, Uppsala, Sweden.
Disclosure
HB reports personal fees from AstraZeneca and Boehringer Ingelheim outside the submitted work. CS reports personal fees from AstraZeneca, Boehringer Ingelheim and Novartis outside the submitted work. LR reports personal fees from AstraZeneca outside the submitted work. HK reports personal fees from AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Sanofi, Orion Pharma, MSD, Chiesi Pharma, Mundipharma and Novartis outside the submitted work. AL reports personal fees from AstraZeneca, Boehringer Ingelheim, Bonnier Healthcare Sweden AB, GlaxoSmithKline, and Novartis outside the submitted work. The aforementioned authors report no other potential conflicts of interest in relation to this work. LH, BIN, TS and ER report no conflicts of interest in relation to this work.
References
1. von Bulow A, Kriegbaum M, Backer V, Porsbjerg C. The prevalence of severe asthma and low asthma control among Danish adults. J Allergy Clin Immunol Pract. 2014;2(6):759–767. doi:10.1016/j.jaip.2014.05.005
2. Hekking PP, Wener RR, Amelink M, Zwinderman AH, Bouvy ML, Bel EH. The prevalence of severe refractory asthma. J Allergy Clin Immunol. 2015;135(4):896–902. doi:10.1016/j.jaci.2014.08.042
3. Rönnebjerg L, Axelsson M, Kankaanranta H, et al. Severe asthma in a general population study: prevalence and clinical characteristics. J Asthma Allergy. 2021;14:1105–1115. doi:10.2147/JAA.S327659
4. Backman H, Jansson SA, Stridsman C, et al. Severe asthma - A population study perspective. Clin Exp Allergy. 2019;49:819–828. doi:10.1111/cea.13378
5. Ilmarinen P, Tuomisto LE, Niemela O, Kankaanranta H. Prevalence of patients eligible for Anti-IL-5 treatment in a cohort of adult-onset asthma. J Allergy Clin Immunol Pract. 2018;7:165–174.
6. Nagase H, Adachi M, Matsunaga K, et al. Prevalence, disease burden, and treatment reality of patients with severe, uncontrolled asthma in Japan. Allergol Int. 2020;69(1):53–60. doi:10.1016/j.alit.2019.06.003
7. Busse WW. Definition and impact. In: Chung KF, Israel E, Gibson PG, editors. ERS Monograph Number 84 Severe Asthma. European Respiratory Society; 2019:1–15.
8. Chung KF, Wenzel SE, Brozek JL, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43(2):343–373. doi:10.1183/09031936.00202013
9. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention (2020 update). Available from: https://ginasthma.org/wp-content/uploads/2020/06/GINA-2020-report_20_06_04-1-wms.pdf. Accessed October 3, 2022.
10. Wenzel S. Severe asthma in adults. Am J Respir Crit Care Med. 2005;172(2):149–160. doi:10.1164/rccm.200409-1181PP
11. Israel E, Reddel HK, Drazen JM. Severe and difficult-to-treat asthma in adults. N Engl J Med. 2017;377(10):965–976. doi:10.1056/NEJMra1608969
12. Kim TB, Bel EH, Moore W. Clinical phenotypes: adults. In: Chung KF, Israel E, Gibson PG, editors. ERS Monograph Number 84 Severe Asthma. European Respiratory Society; 2019:48–63.
13. Del Giacco SR, Bakirtas A, Bel E, et al. Allergy in severe asthma. Allergy. 2017;72(2):207–220. doi:10.1111/all.13072
14. Westerhof GA, Vollema EM, Weersink EJ, Reinartz SM, de Nijs SB, Bel EH. Predictors for the development of progressive severity in new-onset adult asthma. J Allergy Clin Immunol. 2014;134(5):1051–6.e2. doi:10.1016/j.jaci.2014.05.005
15. Ilmarinen P, Pardo A, Tuomisto LE, et al. Long-term prognosis of new adult-onset asthma in obese patients. Eur Respir J. 2021;57(4):2001209.
16. Burke W, Fesinmeyer M, Reed K, Hampson L, Carlsten C. Family history as a predictor of asthma risk. Am J Prev Med. 2003;24(2):160–169. doi:10.1016/S0749-3797(02)00589-5
17. Moore WC, Meyers DA, Wenzel SE, et al. Identification of asthma phenotypes using cluster analysis in the Severe Asthma Research Program. Am J Respir Crit Care Med. 2010;181(4):315–323. doi:10.1164/rccm.200906-0896OC
18. Siroux V, Basagana X, Boudier A, et al. Identifying adult asthma phenotypes using a clustering approach. Eur Respir J. 2011;38(2):310–317. doi:10.1183/09031936.00120810
19. Lefaudeux D, De Meulder B, Loza MJ, et al. U-BIOPRED clinical adult asthma clusters linked to a subset of sputum omics. J Allergy Clin Immunol. 2017;139(6):1797–1807. doi:10.1016/j.jaci.2016.08.048
20. Haldar P, Pavord ID, Shaw DE, et al. Cluster analysis and clinical asthma phenotypes. Am J Respir Crit Care Med. 2008;178(3):218–224. doi:10.1164/rccm.200711-1754OC
21. Schatz M, Hsu JW, Zeiger RS, et al. Phenotypes determined by cluster analysis in severe or difficult-to-treat asthma. J Allergy Clin Immunol. 2014;133(6):1549–1556. doi:10.1016/j.jaci.2013.10.006
22. Backman H, Hedman L, Stridsman C, et al. A population-based cohort of adults with asthma: mortality and participation in a long-term follow-up. Eur Clin Respir J. 2017;4(1):1334508. doi:10.1080/20018525.2017.1334508
23. Lundbäck B, Stjernberg N, Rosenhall L, Lindström M, Jönsson E, Andersson S. Methacholine reactivity and asthma. Report from the Northern Sweden obstructive lung disease project. Allergy. 1993;48(2):117–124. doi:10.1111/j.1398-9995.1993.tb00696.x
24. Ronmark E, Andersson C, Nystrom L, Forsberg B, Jarvholm B, Lundback B. Obesity increases the risk of incident asthma among adults. Eur Respir J. 2005;25(2):282–288. doi:10.1183/09031936.05.00054304
25. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
26. Backman H, Lindberg A, Oden A, et al. Reference values for spirometry - report from the Obstructive Lung Disease in Northern Sweden studies. Eur Clin Respir J. 2015;2:26375. doi:10.3402/ecrj.v2.26375
27. Malmberg P, Larsson K, Thunberg S. Increased lung deposition and biological effect of methacholine by use of a drying device for bronchial provocation tests. Eur Respir J. 1991;4(7):890–898.
28. Brumpton B, Langhammer A, Romundstad P, Chen Y, Mai XM. General and abdominal obesity and incident asthma in adults: the HUNT study. Eur Respir J. 2013;41(2):323–329. doi:10.1183/09031936.00012112
29. Ronmark E, Lindberg A, Watson L, Lundback B. Outcome and severity of adult onset asthma--report from the obstructive lung disease in northern Sweden studies (OLIN). Respir Med. 2007;101(11):2370–2377. doi:10.1016/j.rmed.2007.06.011
30. Ekerljung L, Bossios A, Lotvall J, et al. Multi-symptom asthma as an indication of disease severity in epidemiology. Eur Respir J. 2011;38(4):825–832. doi:10.1183/09031936.00143710
31. Brumpton BM, Camargo CA, Romundstad PR, Langhammer A, Chen Y, Mai XM. Metabolic syndrome and incidence of asthma in adults: the HUNT study. Eur Respir J. 2013;42(6):1495–1502. doi:10.1183/09031936.00046013
32. Singh S, Prakash YS, Linneberg A, Agrawal A. Insulin and the lung: connecting asthma and metabolic syndrome. J Allergy. 2013;2013:627384. doi:10.1155/2013/627384
33. Langhammer A, Johnsen R, Gulsvik A, Holmen TL, Bjermer L. Sex differences in lung vulnerability to tobacco smoking. Eur Respir J. 2003;21(6):1017–1023. doi:10.1183/09031936.03.00053202
34. Real FG, Svanes C, Omenaas ER, et al. Lung function, respiratory symptoms, and the menopausal transition. J Allergy Clin Immunol. 2008;121(1):72–80.e3. doi:10.1016/j.jaci.2007.08.057
35. Tuomisto LE, Ilmarinen P, Niemela O, Haanpaa J, Kankaanranta T, Kankaanranta H. A 12-year prognosis of adult-onset asthma: Seinajoki Adult Asthma Study. Respir Med. 2016;117:223–229. doi:10.1016/j.rmed.2016.06.017
36. Le Moual N, Siroux V, Pin I, Kauffmann F, Kennedy SM. Epidemiological Study on the Genetics and Environment of Asthma. Asthma severity and exposure to occupational asthmogens. Am J Respir Crit Care Med. 2005;172(4):440–445. doi:10.1164/rccm.200501-111OC
37. Wenzel SE, Balzar S, Cundall M, Chu HW. Subepithelial basement membrane immunoreactivity for matrix metalloproteinase 9: association with asthma severity, neutrophilic inflammation, and wound repair. J Allergy Clin Immunol. 2003;111(6):1345–1352. doi:10.1067/mai.2003.1464
38. Håkansson KEJ, Backer V, Ulrik CS. Socioeconomic biases in asthma control and specialist referral of possible severe asthma. Eur Respir J. 2021;58(6):2100741. doi:10.1183/13993003.00741-2021
39. Porsbjerg C, Ulrik C, Skjold T, et al. Nordic consensus statement on the systematic assessment and management of possible severe asthma in adults. Eur Clin Respir J. 2018;5(1):1440868. doi:10.1080/20018525.2018.1440868
40. Denning DW, O’Driscoll BR, Hogaboam CM, Bowyer P, Niven RM. The link between fungi and severe asthma: a summary of the evidence. Eur Respir J. 2006;27(3):615–626. doi:10.1183/09031936.06.00074705
41. Mascia K, Haselkorn T, Deniz YM, et al. Aspirin sensitivity and severity of asthma: evidence for irreversible airway obstruction in patients with severe or difficult-to-treat asthma. J Allergy Clin Immunol. 2005;116(5):970–975. doi:10.1016/j.jaci.2005.08.035
42. Warm K, Hedman L, Lindberg A, Lotvall J, Lundback B, Ronmark E. Allergic sensitization is age-dependently associated with rhinitis, but less so with asthma. J Allergy Clin Immunol. 2015;136(6):1559–1562. doi:10.1016/j.jaci.2015.06.015
43. Bunne J, Hedman L, Perzanowski M, et al. The majority of children sensitized before school-age develop allergic disease before adulthood: a longitudinal population-based study. J Allergy Clin Immunol Pract. 2022;10(2):577–585.e3. doi:10.1016/j.jaip.2021.10.023
44. Ryan D, Heatley H, Heaney LG, et al.Potential severe asthma hidden in UK primary care. J Allergy Clin Immunol Pract. 2021;(4):1612–1623.e9. doi:10.1016/j.jaip.2020.11.053
45. Holguin F, Cardet JC, Chung KF, et al. Management of severe asthma: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2020;55(1):1900588. doi:10.1183/13993003.00588-2019
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Level of Education Modifies Asthma Mortality in Norway and Sweden. The Nordic EpiLung Study
Backman H, Bhatta L, Hedman L, Brumpton B, Vähätalo I, Lassmann-Klee PG, Nwaru BI, Ekerljung L, Krokstad S, Aalberg Vikjord SA, Lindberg A, Kankaanranta H, Rönmark E, Langhammer A
Journal of Asthma and Allergy 2024, 17:209-218
Published Date: 18 March 2024