Back to Journals » Risk Management and Healthcare Policy » Volume 19
Determinants of Glycemic Control Among Patients with Diabetes: A Cross-Sectional Study
Received 13 March 2026
Accepted for publication 22 May 2026
Published 28 May 2026 Volume 2026:19 608364
DOI https://doi.org/10.2147/RMHP.S608364
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mecit Can Emre Simsekler
Salha Otaif,1,2 Ghareeb Bahari3
1Jazan Health Cluster, Ministry of Health, Jazan, Saudi Arabia; 2Community, Psychiatric and Mental Health Nursing Department, College of Nursing, King Saud University, Riyadh, 11421, Saudi Arabia; 3Nursing Administration and Education Department, College of Nursing, King Saud University, Riyadh, 11421, Saudi Arabia
Correspondence: Ghareeb Bahari, Nursing Administration and Education Department, College of Nursing, King Saud University, Riyadh, 11421, Saudi Arabia, Email [email protected]
Purpose: Poor glycemic control remains a major challenge and leads to complications among patients with diabetes. In this study, we aimed to identify strategies and factors contributing to improved glycemic control among patients with diabetes in Saudi Arabia.
Patients and Methods: This cross-sectional study used a convenience sample of 144 adults with diabetes who visited primary healthcare centers. Data were collected using a structured questionnaire that incorporated validated tools to assess multiple factors of glycemic control.
Results: Among the 144 participants, only 41.6% achieved optimal HbA1c control, while 58.4% had suboptimal control, including 21.5% with very poor control. Physical activity levels were mostly low to moderate, and two-thirds of the participants reported poor medication adherence. Self-efficacy was moderate, with weaknesses in diet-related confidence. Physical activity was positively correlated with self-efficacy and negatively correlated with medication adherence. Similarly, self-efficacy was negatively associated with medication adherence. Glycemic control was weakly associated with these variables. Regression analysis identified duration since diagnosed with diabetes and medication adherence as significant factors of glycemic control, while self-efficacy and family support were strongly associated with physical activity.
Conclusion: Glycemic control among patients with diabetes remains suboptimal. Targeted interventions that strengthen self-care, foster family support, and address behavioral barriers are essential for improving diabetes management and long-term health outcomes.
Keywords: behavioral barriers, medication adherence, physical activity, self-efficacy
Introduction
Diabetes mellitus is a major global public health concern and substantial health burden.1 The number of people with diabetes is projected to increase to 578 million by 2030 and to 700 million by 2045.2 In the Kingdom of Saudi Arabia, the prevalence of diabetes mellitus is approximately 28% and varies across geographic regions.3 The disease poses a major public health challenge in Saudi Arabia. Accordingly, in alignment with Saudi Vision 2030, addressing the burden of chronic diseases, particularly diabetes, has become a national priority.4 Effective diabetes management requires a multifaceted approach that includes physical activity, medication adherence, and self-efficacy. Physical activity plays an important role in improving glycosylated hemoglobin (HbA1c).5 However, physical activity levels among Saudi adults with diabetes remain suboptimal.6 Individuals who engage in regular physical activity are more likely to achieve better glycemic control through adherence to dietary regimens and weight reduction.7
The primary therapeutic goal in diabetes care is to maintain appropriate glycemic control,1 defined as the extent to which individuals with diabetes mellitus achieve target blood glucose levels.8 Better glycemic control reduces morbidity and improves life expectancy and quality of life.9 Factors associated with glycemic control can be classified into four categories: personal/biological, clinical, medication-related, and behavioral.8 Medication adherence refers to the extent to which patients follow their prescribed diabetes medication regimen.10 Adhering to medication is essential for maintaining glycemic control, slowing disease progression, and reducing morbidity and mortality.11 Many patients with diabetes struggle to adhere to their medication, which is associated with poor glycemic control.12 Improving patients’ understanding of their condition is essential for promoting adherence. Education on the importance of consistent medication use supports effective disease management. Both patients and healthcare providers play key roles in improving adherence.10
Self-efficacy is another important component of diabetes management, influencing patients’ ability to cope with challenges and implement lifestyle changes. Diabetes management self-efficacy reflects an individual’s perceived ability to perform self-management behaviors necessary for glycemic control and the prevention of complications.13 Enhancing self-efficacy may improve patients’ capacity to manage the condition, regulate blood glucose levels, and reduce short- and long-term diabetes-related complications.13 Achieving adequate glycemic control is essential for delaying or preventing diabetes-related complications associated with increased morbidity and mortality. Globally, only about 50% of all patients with diabetes maintain adequate glycemic control, while many experience poor control.14 Effective management of diabetes-related complications requires behavioral modifications supported by strong self-efficacy.15
The self-efficacy theory is a foundational theoretical framework for understanding how individuals’ beliefs in their capabilities affect their actions, particularly in managing health-related behaviors.16 This concept is essential for diabetes management, where patients must continuously engage in self-care behaviors to maintain optimal glycemic control. This theory identifies four primary sources of information that shape self-efficacy and facilitate behavior change.
Mastery experiences, also referred to as performance accomplishments, are central to developing self-efficacy.16 These experiences involve reflecting on past successes to evaluate one’s ability to perform future tasks. Vicarious experiences and social persuasion also contribute to building self-efficacy. Observing others successfully perform tasks can strengthen individuals’ beliefs in their own abilities. Emotional and physiological states, such as depression, anxiety, and stress, can negatively affect self-efficacy and hinder the maintenance of a positive self-attitude.
Interactions among physical activity, medication adherence, and self-efficacy may be associated with glycemic control and overall health outcomes. These relationships are complex and may be shaped by cultural, socioeconomic, and healthcare system factors specific to Saudi Arabia. Although previous studies have examined these factors individually, limited research has explored their combined influence on diabetes outcomes among patients with diabetes in Saudi Arabia. Additionally, evidence regarding how local cultural and lifestyle factors influence these relationships remains insufficient. Understanding such interactions is necessary to develop comprehensive, culturally appropriate interventions to improve diabetes outcomes among Saudi individuals.
The primary aim of this study was to identify factors and strategies associated with glycemic control among patients with diabetes in Saudi Arabia. This study also seeks to address gaps in understanding diabetes management within the Saudi context. By examining physical activity, medication adherence, and self-efficacy across all types of diabetes, the research aimed to provide insights for developing effective strategies to improve glycemic control among patients. The findings may guide healthcare providers, policymakers, and researchers in designing targeted interventions and policies to improve diabetes care in Saudi Arabia.
Materials and Methods
Study Design and Setting
A cross-sectional study design was employed to assess the factors associated with glycemic control among patients living with diabetes in Saudi Arabia. Data were collected at a single point in time through an online survey administered to patients with diabetes. The survey was conducted using validated questionnaires. The study was conducted across various healthcare facilities in Saudi Arabia, including hospitals, primary healthcare centers, and specialized diabetes clinics, as these institutions are well positioned to reach a diverse group of patients with diabetes.
Sampling Process
Participants were recruited using convenience sampling, which involves selecting individuals who are readily accessible and willing to participate.17 This method was practical for this study as it enabled the researchers to reach patients with diabetes during their routine visits to healthcare facilities or through online recruitment platforms. By using this approach, participants were selected based on their availability and willingness to complete the survey. This study focused on adults aged ≥18 years living in Saudi Arabia who had a confirmed diagnosis of diabetes (type 1 or type 2) and had been diagnosed at least 1 year prior to study participation. Individuals who were unable to provide consent were excluded, as were pregnant women with gestational diabetes, unless they had a prior diagnosis of diabetes.
Sample Size
The researchers used an electronic calculator tool to estimate the sample size (https://www.danielsoper.com/statcalc/calculator.aspx?id=1). The effect size indicated the strength of the link between the predictors and the outcome, with 0.15 indicating a medium effect. Statistical power, usually set at 0.8, indicates an 80% chance of detecting a real effect if it exists. The number of predictors refers to the independent variables used to predict the outcome. With an effect size of 0.15, power of 0.8, 13 factors (10 items of demographic data and physical activity, self-efficacy, and medication adherence), and a probability level of 0.05, the minimum sample size needed was 131 participants, ensuring sufficient power to detect meaningful associations between variables.
Instrumentation
Data were collected between December 2024 and March 2025 using a self-administered questionnaire. The questionnaire was translated into Arabic using a forward–backward translation process to ensure linguistic accuracy. The translated version was reviewed by two experts for content validity and pilot-tested to ensure clarity and cultural appropriateness. The questionnaire was divided into five parts. The first part of the survey focused on collecting demographic data from participants, and the second part included five items from a physical activity assessment adopted from Cho.18 Cronbach’s alpha was reported as 0.79, indicating good internal consistency. The third part consisted of eight items from the Diabetes Self-Efficacy Scale,19 yielding an excellent Cronbach’s alpha of 0.94. The fourth part involved the Morisky, Green & Levine scale (MGL).20 The scale is a validated tool for measuring medication adherence, and it reported a Cronbach’s alpha value of 0.79. The fifth part involved assessing participants’ glycemic control by collecting their most recent HbA1c readings, which were self-reported.21 The questionnaire’s overall Cronbach’s alpha was 0.889, indicating good internal consistency.
Data Analysis
An online web tool was used to develop and host the survey, ensuring participants could securely and efficiently provide their responses. Collected data were analyzed using IBM Statistical Product and Service Solutions (SPSS) software version 25 (IBM Corp., Armonk, NY, USA). Both descriptive and inferential statistics were used to examine the study variables. Data were examined for outliers, and none were detected. Missing data were addressed using mean imputation for continuous variables and mode imputation for categorical variables. Univariate analyses were performed to describe the characteristics and distributions of the demographic and main study variables. For medication adherence behavior and self-efficacy, mean item scores (ie., the mean of individual item means) were estimated to summarize item-level performance for each scale, an approach commonly used in scale-based research to facilitate interpretability and comparability across item means.
Bivariate analysis was conducted to examine differences and associations among variables. Independent-samples t-tests and one-way analysis of variance (ANOVA) were used to assess differences between groups, while Pearson’s correlation coefficient was used to examine associations between continuous variables. Finally, multivariable analyses, including multiple linear regression, were performed to explore associations among multiple variables while controlling for covariates. Before conducting regression, linearity, normality, homoscedasticity, and independence of residuals assumptions were assessed, and no violations were detected. Multicollinearity among the independent variables was also evaluated using variance inflation factor and tolerance values, with no problematic multicollinearity detected. Statistical significance was set at P < 0.05.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by the institutional review board of the King Saud University Medical City (Ref. No. 24/1709/IRB) before the start of the study and adhered to strict ethical standards to protect participants’ rights and well-being. The participants were fully informed about the study’s purpose, procedures, potential risks, and benefits. Informed consent was obtained from all participants. The first page of the questionnaire included the statement, “Your completion of the survey indicates your agreement to participate”, followed by a “Start” button to proceed with the survey. The participants were informed that they voluntarily agreed to participate without coercion. All collected data were treated confidentially and accessible only to the research team.
Declaration of Generative Artificial Intelligence (GenAI) Use
AI tool was used to improve language and readability of some sentences, with caution. The content has been reviewed and approved for publication.
Results
Table 1 presents the demographic characteristics of the participants (N = 144). Most of the respondents were female (68.1%), and most were aged 41–50 years (31.9%). Most of the participants were married (84.0%). Two-thirds (66.7%) of the participants had a university degree. Concerning monthly income, 61.1% earned >7,000 SR. More than half of the participants lived in urban areas. Most of the participants had been diagnosed ≥5 years earlier. Table 2 shows that most patients engaged in low-to-moderate physical activity, with very few reporting high levels of physical activity. Medication adherence was low (mean: 1.70 ± 1.52), while self-efficacy was moderate (mean: 6.19 ± 3.11), with only approximately one-third achieving high adherence. Regarding glycemic control, approximately 31.9% had excellent control, while 22.9% and 21.5%, respectively, had fair to very poor control, indicating overall suboptimal diabetes management.
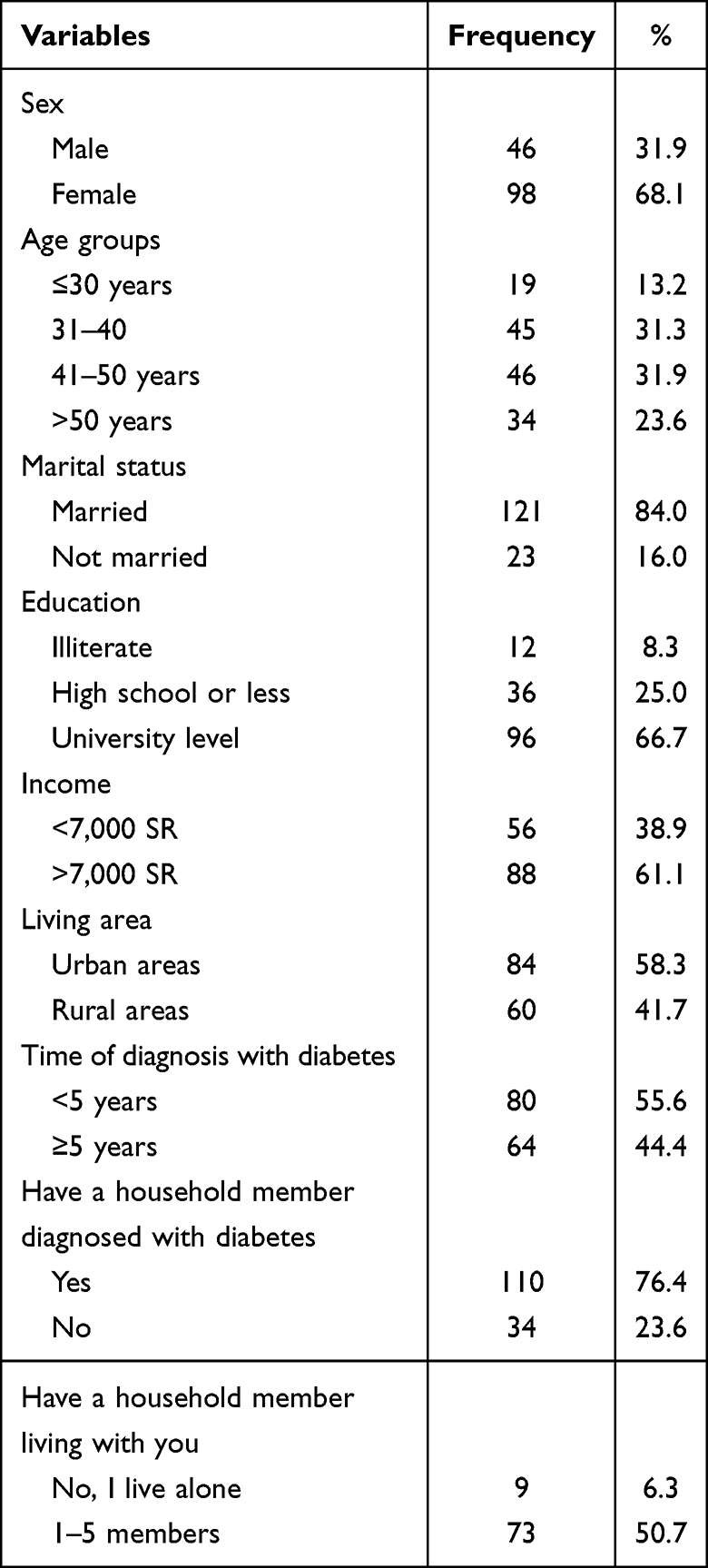 |
Table 1 Sample Characteristics (N = 144) |
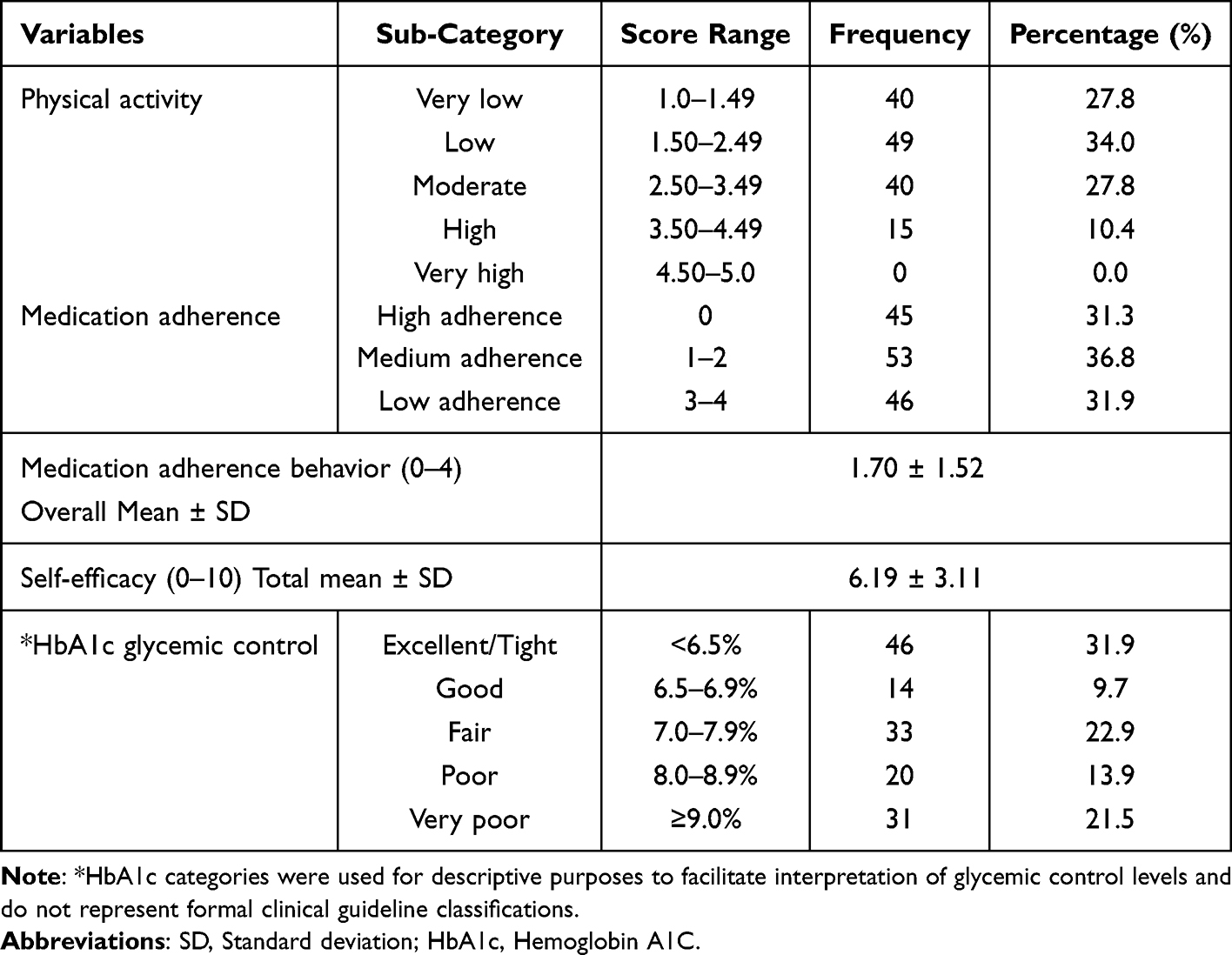 |
Table 2 Characteristics of the Main Variables |
Table 3 presents the self-efficacy assessment of patients’ confidence in managing various aspects of their disease. The scores ranged from 0 (not at all confident) to 10 (completely confident). Among the items assessed, participants reported the highest confidence in judging when symptoms necessitated a visit to the physician (mean: 6.79, SD: 3.10). Lower confidence levels were reported for adhering to a diet when preparing or sharing food with individuals without diabetes (mean: 5.65, SD: 3.17) and for maintaining regular mealtimes, including breakfast (mean: 5.86, SD: 3.26).
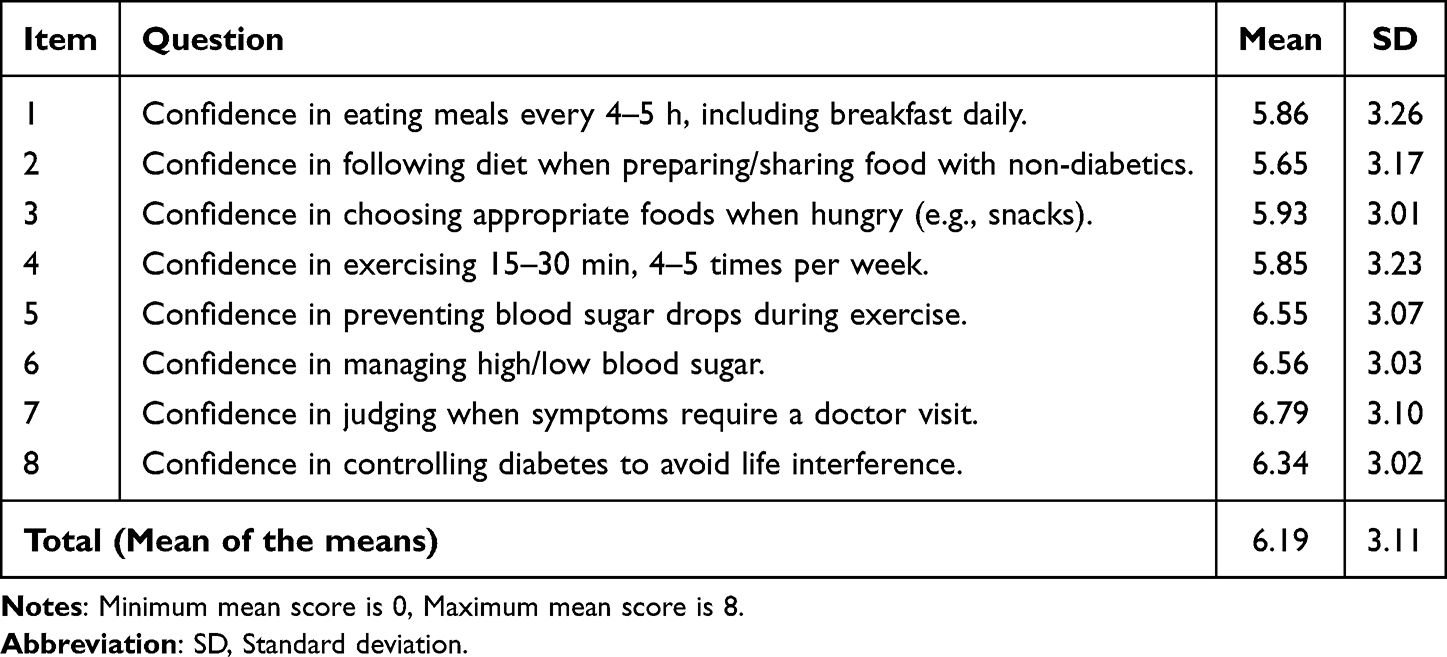 |
Table 3 Self-Efficacy Assessment Among Patients with Diabetes |
Table 4 shows the mean differences in glycemic control, physical activity, medication adherence, and self-efficacy across demographic factors. Physical activity levels significantly differed between the sexes (p = 0.014). Income was significant across self-efficacy (p = 0.001) and physical activity (p = 0.002), and those earning >7,000 SR scored higher. Time since diagnosis also mattered, with patients diagnosed for ≥5 years showing higher self-efficacy and physical activity (p = 0.012 for both). Having a household member with diabetes was significantly related to medication adherence (p = 0.027), self-efficacy (p = 0.001), and physical activity (p = 0.011). Glycemic control was not statistically significant across any demographic factor.
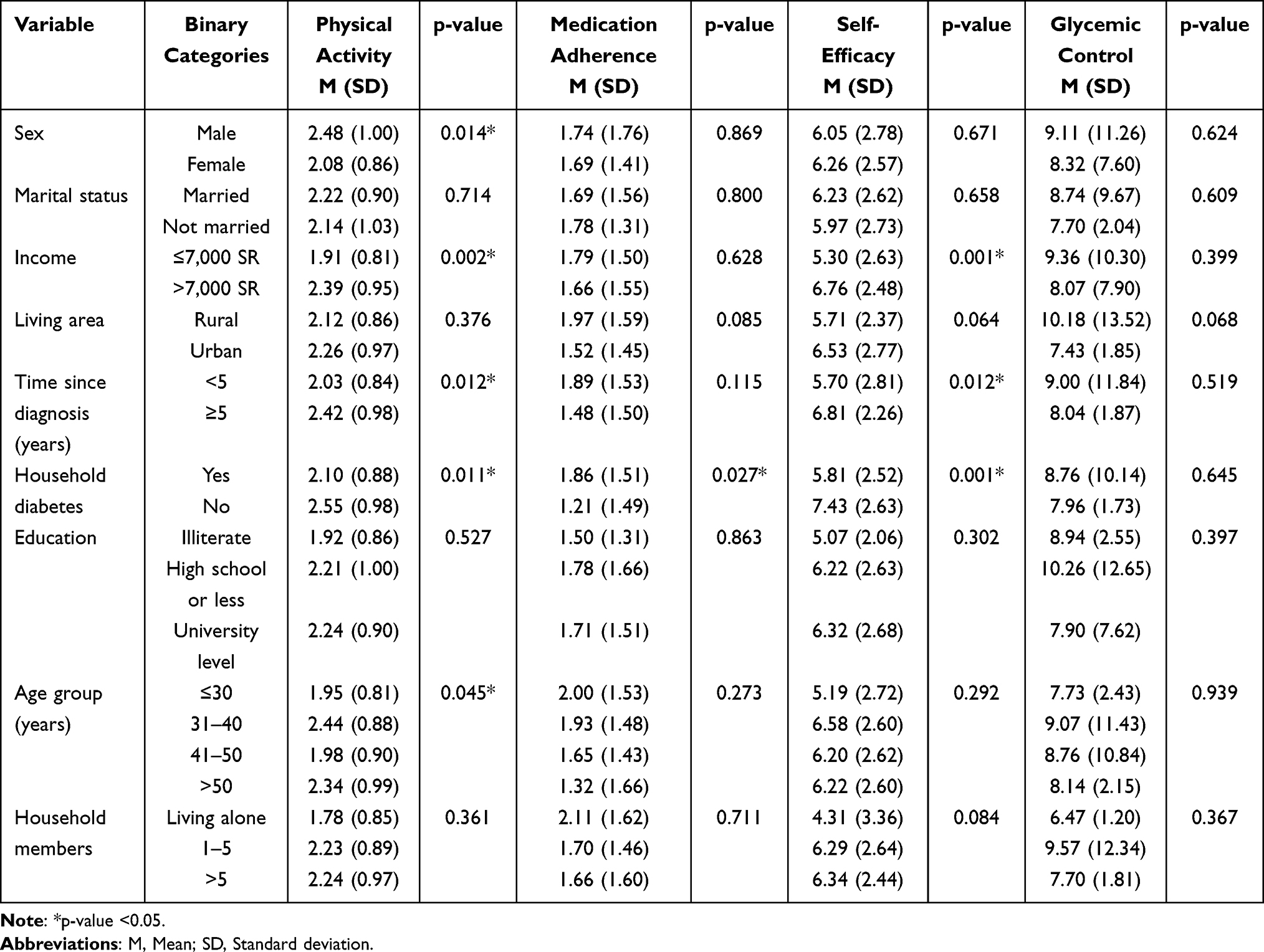 |
Table 4 Differences in the Mean Scores of the Main Variables with Regard to Demographic Factors |
Table 4 also presents differences in the main variables by education, age group, and household size using one-way ANOVA. Outcomes did not differ significantly across education levels, although participants with university-level education reported slightly higher self-efficacy and physical activity compared to illiterate participants. Age had a significant effect on physical activity (p = 0.045), with participants aged 31–40 years reporting the highest levels. However, no significant differences across age groups were found for glycemic control, medication adherence, or self-efficacy. Furthermore, no significant differences were observed across household sizes, although those living alone tended to report lower self-efficacy than those living with others.
Bivariate correlation analysis showed that physical activity was significantly and negatively correlated with medication adherence (r = −0.232, p < 0.05), whereas it was significantly and positively correlated with self-efficacy (r = 0.405, p < 0.05). Medication adherence also demonstrated a significant negative correlation with self-efficacy (r = −0.217, p < 0.05). In contrast, glycemic control was not significantly associated with physical activity (r = 0.060), medication adherence (r = 0.122), or self-efficacy (r = −0.020).
Multiple linear regression analysis was performed to identify the factors associated with glycemic control among patients with diabetes. The model explained approximately 21.1% of the variance in glycemic control and was significant (p = 0.002), indicating a good overall fit. Results revealed that two variables were significant factors of glycemic control. Only duration since diagnosis and medication adherence showed significant associations with glycemic control. Duration since diagnosis was positively associated with glycemic control (β = 0.867, p = 0.015), indicating that longer duration since diagnosis was related to glycemic control. Medication adherence was also significantly and negatively associated with glycemic control (β = −0.196, p = 0.016). Other variables, including age, sex, marital status, education, income, living area, physical activity, self-efficacy, and family history, were not significant factors (see Table 5).
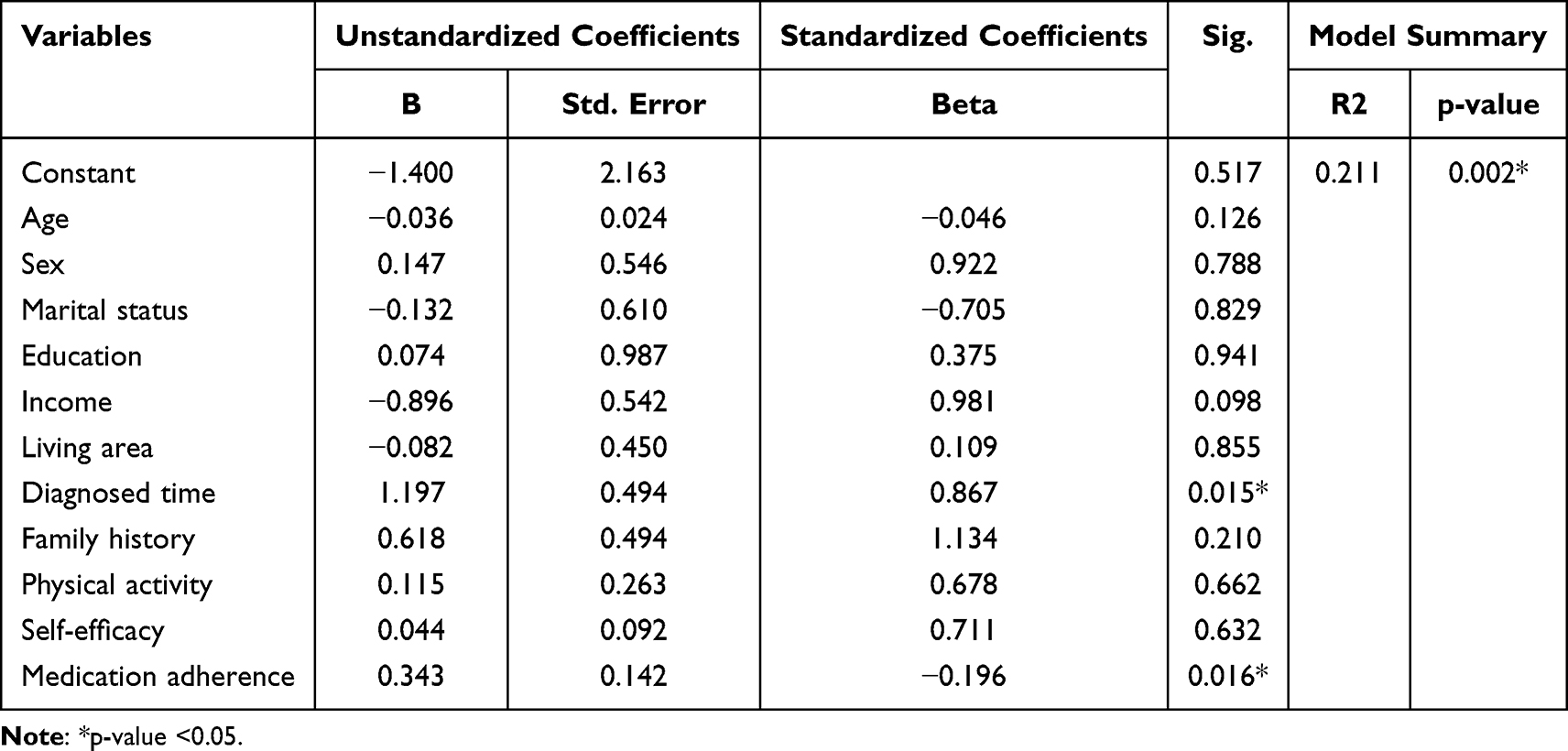 |
Table 5 Multiple Linear Regression Analysis for the Factors Affecting Glycemic Control |
Discussion
In this study, we investigated physical activity, medication adherence, and self-efficacy and their association with glycemic control among patients with diabetes in Saudi Arabia, while accounting for relevant sociodemographic factors.
Physical Activity
In the present study, participants demonstrated limited engagement in physical activity, with activities generally characterized by low frequency, light intensity, shorter duration, and limited diversity. These patterns may reflect the Saudi context, where factors such as climate and cultural norms contribute to lower levels of regular physical activity. These findings appear inconsistent with current recommendations encouraging regular aerobic, resistance, flexibility, and balance exercises, as well as reducing sedentary behavior among individuals with diabetes.22 Consistent with the present findings, contemporary reviews note that most patients with diabetes do not meet recommended activity targets,23 and many remain at early stages of behavioral change.
A cross-sectional study reported that many patients were in the pre-contemplation or contemplation stages of physical activity engagement and demonstrated low levels of physical activity.24 Meta-analytic evidence demonstrates the benefits of structured exercise. Across 32 randomized controlled trials, structured exercise was associated with reductions in HbA1c, fasting glucose, body mass index, and waist circumference.7 Additional studies have reported improved time-in-range and reduced glycemic variability25 and a modest but significant improvement in HbA1c across diverse physical activity interventions.26
Medication Adherence
In the present study, a limited proportion of participants demonstrated high medication adherence. This distribution indicates a substantial treatment gap, as frequent dose omissions or timing errors may compromise sustained glycemic control for many patients. Although the between-group ANOVA on HbA1c did not reach statistical significance, the adherence profile remained clinically meaningful because HbA1c reflects glycemic patterns and self-management behaviors over time. Further, cross-sectional grouping may have limited statistical power in the presence of high variability, and adherence was assessed using brief self-report measures. The negative associations reported between medication adherence, physical activity, and self-efficacy may suggest that some participants relied more on non-pharmacological self-care behaviors than on medication use. Thus, such findings should be interpreted cautiously due to the cross-sectional design, and further studies are warranted to clarify these relationships.
The pattern aligns with multicenter and regional evidence indicating that medication non-adherence remains widespread, particularly in low- and middle-income settings. A study from northwest Ethiopia reported low adherence among patients with comorbidities and poor glycemic control, with factors such as cost coverage, income, self-monitoring of blood glucose, number of medications, and comorbidity predicting adherence.12 In contrast, research conducted in a tertiary center in India documented very high adherence and better glycemic control among adherent patients; however, comorbidity and substance use still eroded adherence.27
Self-Efficacy
In the present study, item-level self-efficacy scores clustered around moderate confidence for symptom appraisal and glycemia management, whereas lower confidence was reported for maintaining dietary behaviors in social contexts and sustaining a regular diet. Notably, the reported composite score indicated substantial variability and appeared lower than the average item-level responses. Interpreting these findings together suggests that patients may feel capable of managing acute glycemic events but have lower confidence in maintaining routine behavior, particularly dietary practices, which may limit consistent day-to-day control.
These findings are consistent with evidence that higher diabetes self-efficacy is associated with better glycemic control and well-being. A study in India reported an inverse correlation between self-efficacy and HbA1c, and found strong associations between self-efficacy and diet adherence, family support, socioeconomic advantage, and participation in educational programs.28 Similarly, research in Saudi Arabia found that each one-point increase on the Self-Efficacy for Managing Chronic Disease 6-Item Scale was associated with better glycemic control and improved well-being.29
The relatively lower confidence in diet-related behaviors observed in the present study mirrors findings from a primary-care study in Vietnam. Network analysis in that study identified diet-related self-efficacy as the most central component among patients with well-controlled glycemia, suggesting that diet-related confidence may support broader self-care routines.30
Self-efficacy alone may not guarantee adequate glycemic control. A Zambian study reported high self-efficacy and good self-care among many participants despite poor control, although good self-care remained associated with increased and better control.31 These findings suggest that environmental, clinical, and structural factors, such as medication complexity, healthcare access, and comorbidity burden, may limit the translation of self-efficacy into improved glycemic outcomes if not addressed concurrently. An Omani multi-site study similarly documented low mean self-efficacy alongside moderate control, with variations according to age and marital status.32 These findings indicate that demographic and contextual factors may also be associated with self-efficacy patterns in the Saudi population.
Glycemic Control
In this study, more than half of the patients did not meet the recommended targets for glycemic control, increasing their risk for diabetes-related complications. Factors, such as limited diabetes education, lifestyle patterns, high obesity prevalence, and physical inactivity, may contribute to the suboptimal glycemic control observed in this population. Notably, the analysis did not identify significant associations between glycemic control and demographic variables, suggesting that behavioral and healthcare-related factors may play a more prominent role in determining glycemic outcomes.
These findings are consistent with previous studies from Saudi Arabia and other regions reporting similarly low rates of glycemic control. For example, previous studies from Saudi Arabia33 and China34 similarly reported limited achievement of adequate glycemic control among patients with diabetes. Although the proportion of patients with well-controlled glycemia in the present study was somewhat higher, most participants still exceeded recommended HbA1c thresholds, indicating that inadequate glycemic control remains a widespread challenge.
Other studies have identified several factors associated with improved glycemic outcomes. Azzam, et al1 reported that education, employment, and physical activity were significantly associated with better glycemic outcomes in Egyptian patients, while Tarekegn, et al35 and Phuwilert, et al36 emphasized the roles of longer diabetes duration and lower education level in worsening control in Ethiopia and Thailand, respectively. In contrast to these findings, the present study did not identify significant demographic associations. This discrepancy may reflect contextual differences in the Saudi healthcare system, sample characteristics, or cultural patterns that shape diabetes care.
Demographic Factors
The analysis of demographic factors revealed several patterns related to physical activity, medication adherence, and self-efficacy, although glycemic control did not vary significantly across subgroups. Sex differences were observed in physical activity levels, with men reporting significantly higher activity than women. This pattern may reflect sociocultural and environmental barriers to women’s participation in physical activity in Saudi Arabia, including limited access to exercise facilities and social constraints on outdoor activity. Similar patterns have been reported in China, where female patients were less likely than male patients to achieve optimal glycemic control.34
Income was strongly associated with both self-efficacy and physical activity. Participants with higher income reported greater confidence in managing their diabetes and engaged more frequently in physical activity. These findings are consistent with studies from Ethiopia and Iran, which reported that lower socioeconomic status was associated with poorer glycemic control and reduced self-care engagement.35,37 Income may influence access to healthier diets, exercise opportunities, and healthcare resources, highlighting structural factors that affect diabetes management in the Saudi context.
Duration of diabetes was also associated with behavioral outcomes. Patients living with diabetes for five years or more reported higher levels of self-efficacy and physical activity than those with shorter disease duration. Similar findings have been reported in studies conducted in Thailand and Saudi Arabia, suggesting that longer disease duration may support the development of coping strategies and self-management routines.33,36 Previous research also indicates that very long disease duration may be associated with treatment fatigue and worsening glycemic control, suggesting that the benefits of accumulated experience may be offset by the physiological progression of diabetes over time.36
The presence of another household member with diabetes was associated with higher adherence, self-efficacy, and physical activity. This finding highlights the role of family and social support in diabetes management. Previous studies conducted in India and Vietnam similarly found that family involvement improves self-efficacy, dietary adherence, and overall glycemic outcomes.28,30 In the Saudi context, where family structures are strong, such support may provide motivation, shared knowledge, and accountability in disease management.
Age was also associated with physical activity, with older patients reporting lower activity levels. This finding aligns with global evidence that physical activity declines with age because of comorbidities, reduced mobility, and lower motivation.26,38 Similarly, research from Iran reported that physical activity was influenced by age, education, and disease duration.24
Correlation analysis demonstrated that HbA1c was not significantly associated with physical activity, self-efficacy, or adherence, suggesting that glycemic outcomes may be influenced by complex and multifactorial pathways. In contrast, self-efficacy and physical activity were strongly and positively correlated, consistent with evidence that higher confidence in disease management promotes greater engagement in physical activity. Interestingly, both physical activity and self-efficacy were negatively correlated with medication adherence. This relationship should be interpreted with caution, as it may reflect differences in disease severity, treatment complexity, or limitations in behavioral measurement rather than a substitution between medication use and lifestyle management.8 It is also possible that participants with greater confidence in self-management or higher engagement in lifestyle modification relied more on non-pharmacological approaches to diabetes management. Conversely, individuals with more severe or uncontrolled diabetes may have required stricter medication regimens despite lower engagement in physical activity and self-management practices.
Regression Analysis
The regression analysis provided further insight into factors associated with glycemic control. Longer duration of diabetes and medication adherence were significant factors associated with glycemic outcomes, suggesting that disease progression, increased treatment complexity, and challenges in maintaining consistent follow-up may impact metabolic control. Similar results have been reported in studies from Saudi Arabia33 and Thailand,36 where longer disease duration was strongly associated with HbA1c levels, reflecting the cumulative effects of pancreatic β-cell decline, treatment fatigue, and increased complications over time. The association reported between medication adherence and glycemic control may also reflect that patients with uncontrolled HbA1c levels are more frequently prescribed intensive treatment regimens and require closer medication management. Thus, further longitudinal research is recommended to better clarify the relationship between medication adherence and glycemic control over time. The role of medication adherence is supported by findings from Jordan39 and Spain,40 reinforcing the notion that adherence is an important component of glycemic control across healthcare settings.
Study Limitations
The study provides insights into factors associated with glycemic control by examining physical activity, medication adherence, self-efficacy, and demographics in a clinical population. The use of validated instruments strengthened the reliability of the measurements, and the focus on patients receiving routine care increased the practical relevance of the findings. However, several limitations should be acknowledged. First, the study relied on self-reported data, which may be subject to recall and social desirability bias. Second, the cross-sectional design limits the ability to establish causal relationships between glycemic control and behavioral factors. Third, the HbA1c values were self-reported rather than clinically verified, which may have introduced variability. Additionally, the single-center design and relatively small sample size may limit generalizability and statistical power. The absence of objective measures, such as activity trackers or pharmacy records, may limit the precision of the behavioral assessments. Finally, differences between Type 1 and Type 2 diabetes were not examined. Future research should distinguish between diabetes types and incorporate objective measurements and longitudinal designs to provide a more comprehensive understanding of glycemic control.
Implications of the Study
Nurses play a key role in supporting patients with diabetes by guiding lifestyle changes, building confidence, and ensuring equitable access to care, especially for those in rural or low-resource settings. Nurse managers should strengthen systems that support regular follow-up and counseling. Nursing education should integrate the medical and behavioral aspects of diabetes to prepare future nurses to better understand and manage patient needs. Finally, nursing research should employ longitudinal designs and objective measures to better understand how self-care behaviors affect glycemic control.
Conclusions
Less than half of the patients in this study achieved adequate glycemic control, and many reported low levels of physical activity, moderate self-efficacy, and challenges in diet management. Medication adherence and duration since diagnosed with diabetes were key factors of glycemic outcomes; whereas, family support was associated with improved self-efficacy. These findings suggest that diabetes management strategies should emphasize patient education, behavioral support, and strategies that promote adherence and physical activity, while also providing psychosocial support for those with a family history of diabetes. Moreover, interventional research is necessary to develop and identify effective strategies for improving diabetes management.
Institutional Review Board Statement
This study was approved by the institutional review board of King Saud University (Ref. No. 24/1709/IRB), dated 20 November 2024.
Abbreviations
ANOVA, Analysis of variance; HbA1c, Glycosylated hemoglobin; MGL, Morisky, Green & Levine scale.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available due to privacy and ethical restrictions but are available from the corresponding author upon reasonable request.
Informed Consent Statement
Informed consent was obtained from all participants.
Acknowledgments
The authors extend their appreciation to the Ongoing Research Funding program (ORF-2026-438) at King Saud University, Riyadh, Saudi Arabia.
Funding
This research was funded by the Ongoing Research Funding program, (ORF-2026-438) at King Saud University, Riyadh, Saudi Arabia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Azzam MM, Ibrahim AA, Abd El-Ghany MI. Factors affecting glycemic control among Egyptian people with diabetes attending primary health care facilities in Mansoura District. Egypt J Intern Med. 2021;33(1). doi:10.1186/s43162-021-00065-w
2. Metwally AS, Aljohani ZA, Maashi MI, et al. Knowledge, attitude, and practice regarding the risk of diabetic feet among diabetic patients in the Madinah Region, Saudi Arabia. Cureus. 2023;15(12):e49933. doi:10.7759/cureus.49933
3. Alwadeai KS, Alhammad SA. Prevalence of type 2 diabetes mellitus and related factors among the general adult population in Saudi Arabia between 2016–2022: a systematic review and meta-analysis of the cross-sectional studies. Medicine. 2023;102(24):e34021. doi:10.1097/MD.0000000000034021
4. Itumalla R, Kumar R, Tharwat Elabbasy M, Perera B, Torabi MR. Structural factors and quality of diabetes health services in Hail, Saudi Arabia: a cross-sectional study. Healthcare. 2021;9(12):1691. doi:10.3390/healthcare9121691
5. Gallardo-Gómez D, Salazar-Martínez E, Alfonso-Rosa RM, et al. Optimal dose and type of physical activity to improve glycemic control in people diagnosed with type 2 diabetes: a systematic review and meta-analysis. Diabetes Care. 2024;47(2):295–13. doi:10.2337/dc23-0800
6. Sinclair J, Ageely H, Mahfouz MS, et al. Effects of a home-based physical activity programme on blood biomarkers and health-related quality of life indices in Saudi Arabian type-2 diabetes mellitus patients: protocol for a randomised controlled trial. Int J Environ Res Public Health. 2022;19(8):4468. doi:10.3390/ijerph19084468
7. Shah SZA, Karam JA, Zeb A, et al. Movement is improvement: the therapeutic effects of exercise and general physical activity on glycemic control in patients with type 2 diabetes mellitus: a systematic review and meta-analysis of randomized controlled trials. Diabetes Ther. 2021;12(3):707–732. doi:10.1007/s13300-021-01005-1
8. Bin Rakhis SA, AlDuwayhis NM, Aleid N, AlBarrak AN, Aloraini AA. Glycemic control for type 2 diabetes mellitus patients: a systematic review. Cureus. 2022;14(6):e26180. doi:10.7759/cureus.26180
9. Abdissa D, Hirpa D. Poor glycemic control and its associated factors among diabetes patients attending public hospitals in West Shewa Zone, Oromia, Ethiopia: an institutional based cross-sectional study. Metabol Open. 2022;13:100154. doi:10.1016/j.metop.2021.100154
10. AlShayban DM, Naqvi AA, Alhumaid O, et al. Association of disease knowledge and medication adherence among out-patients with type 2 diabetes mellitus in Khobar, Saudi Arabia. Front Pharmacol. 2020;11:60. doi:10.3389/fphar.2020.00060
11. Suprapti B, Izzah Z, Anjani AG, Andarsari MR, Nilamsari WP, Nugroho CW. Prevalence of medication adherence and glycemic control among patients with type 2 diabetes and influencing factors: a cross-sectional study. Global Epidemiol. 2023;5:100113. doi:10.1016/j.gloepi.2023.100113
12. Sendekie AK, Netere AK, Kasahun AE, Belachew EA, Suksatan W. Medication adherence and its impact on glycemic control in type 2 diabetes mellitus patients with comorbidity: a multicenter cross-sectional study in Northwest Ethiopia. PLoS One. 2022;17(9):e0274971. doi:10.1371/journal.pone.0274971
13. Khalooei A, Hasheminejad Z. Association of diabetes management self-efficacy with adherence to medication, glycemic control, and disease outcomes among type 2 diabetes patients. Shiraz E-Med J. 2023;24(10). doi:10.5812/semj-138227
14. Yahaya JJ, Doya IF, Morgan ED, Ngaiza AI, Bintabara D. Poor glycemic control and associated factors among patients with type 2 diabetes mellitus: a cross-sectional study. Sci Rep. 2023;13(1):9673. doi:10.1038/s41598-023-36675-3
15. Oluma A, Abadiga M, Mosisa G, Fekadu G, Turi E. Perceived self-efficacy and associated factors among adult patients with type 2 diabetes mellitus at public hospitals of Western Ethiopia, 2020. Patient Prefer Adherence. 2020;14:1689–1698. doi:10.2147/PPA.S275887
16. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. doi:10.1037/0033-295X.84.2.191
17. Tappen RM. Advanced Nursing Research: From Theory to Practice.
18. Cho M-H. Preliminary reliability of the five item physical activity questionnaire. J Phys Ther Sci. 2016;28(12):3393–3397. doi:10.1589/jpts.28.3393
19. Lorig KR, Sobel DS, Ritter PL, Laurent D, Hobbs M. Effect of a self-management program on patients with chronic disease. Eff Clin Pract. 2001;4(6):256–262.
20. Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67–74. doi:10.1097/00005650-198601000-00007
21. Mori T, Nagata T, Nagata M, Fujimoto K, Fujino Y, Mori K. Diabetes severity measured by treatment control status and number of anti-diabetic drugs affects presenteeism among workers with type 2 diabetes. BMC Public Health. 2021;21(1):1865. doi:10.1186/s12889-021-11913-3
22. Kanaley JA, Colberg SR, Corcoran MH, et al. Exercise/physical activity in individuals with type 2 diabetes: a consensus statement from the American College of sports medicine. Med Sci Sports Exerc. 2022;54(2):353–368. doi:10.1249/MSS.0000000000002800
23. Bassin SR, Srinath R. The impact of physical activity in patients with type 2 diabetes. Am J Lifestyle Med. 2025;19(1):147–161. doi:10.1177/15598276231180541
24. Amerzadeh M, Bahrami M, Samie F, et al. Level of physical activity in patients with type 2 diabetes. J Diabetes Metab Disord. 2023;23(1):673–680. doi:10.1007/s40200-023-01333-y
25. Zhu X, Zhao L, Chen J, et al. The effect of physical activity on glycemic variability in patients with diabetes: a systematic review and meta-analysis of randomized controlled trials. Front Endocrinol. 2021;12:767152. doi:10.3389/fendo.2021.767152
26. De Cock D, Schreurs L, Steenackers N, et al. The effect of physical activity on glycaemic control in people with type 1 diabetes mellitus: a systematic literature review and meta-analysis. Diabet Med. 2024;41(10):e15415. doi:10.1111/dme.15415
27. Shah S, Barot P, Patel H, Shukla A. Assessment of medication adherence in diabetes mellitus patients at a tertiary care teaching hospital in India. Cureus. 2025;17(2):e78391. doi:10.7759/cureus.78391
28. S A, S S, Ts A, Mahadevan S. Diabetes self-efficacy on glycemic control and well-being of patients with type 2 diabetes mellitus: an analytical cross-sectional study. Cureus. 2024;16(7):e64005. doi:10.7759/cureus.64005
29. Alshaikh AA, Al-Qahtani FS, Alqahtani SAM, et al. Exploring the self-efficacy of patients with diabetes: its role as a predictor of diabetes management and well-being. Front Endocrinol. 2024;15:1347396. doi:10.3389/fendo.2024.1347396
30. Quynh Anh LHT, Quoc Huy NV, Minh Tam N, et al. Exploring the relationships between self-efficacy, self-care, and glycaemic control in primary care diabetes management. SAGE Open Medicine. 2024;12:20503121241310016. doi:10.1177/20503121241310016
31. Kalonga N, Mukwato PK, Wahila R. Self- efficacy and self- care practices, in glycemic control among adults with diabetes mellitus receiving care at kitwe teaching hospital, Ktiwe, Zambia. Nurs Primary Care. 2023;7(1):1–8. doi:10.33425/2639-9474.1234
32. AlShezawi IA, Rawwad THA, Aldirawi AA, Alwawi AA, Fazari HSA, Shah AH. Exploring the impact of self-efficacy on glycemic control in Omani type 2 diabetes patients. Front Endocrinol. 2025;16:1597274. doi:10.3389/fendo.2025.1597274
33. Ewid M, Algoblan AS, Elzaki EM, et al. Factors associated with glycemic control and diabetes complications in a group of Saudi patients with type 2 diabetes. Med. 2023;102(38):e35212. doi:10.1097/MD.0000000000035212
34. Xing X-Y, Wang X-Y, Fang X, et al. Glycemic control and its influencing factors in type 2 diabetes patients in Anhui, China. Front Public Health. 2022;10:980966. doi:10.3389/fpubh.2022.980966
35. Tarekegn ET, Gobezie MY, Haile MB, Zerga AA. Glycemic control and associated factors among type 2 diabetes patients attending at Dessie comprehensive specialized hospital outpatient department. Sci Rep. 2025;15(1):9286. doi:10.1038/s41598-025-93739-2
36. Phuwilert P, Khiewkhern S, Phajan T, et al. Factors affecting glycemic control in patients with type 2 diabetes in Kalasin Province, Thailand: an analytical cross-sectional study. Healthcare. 2024;12(19):1916. doi:10.3390/healthcare12191916
37. Dinavari MF, Sanaie S, Rasouli K, Faramarzi E, Molani-Gol R. Glycemic control and associated factors among type 2 diabetes mellitus patients: a cross-sectional study of Azar cohort population. BMC Endocr Disord. 2023;23(1):273. doi:10.1186/s12902-023-01515-y
38. Chang CR, Russell BM, Dempsey PC, Christie HE, Campbell MD, Francois ME. Accumulating physical activity in short or brief bouts for glycemic control in adults with prediabetes and diabetes. Can J Diabetes. 2020;44(8):759–767. doi:10.1016/j.jcjd.2020.10.013
39. Al-Qerem W, Jarab AS, Badinjki M, Hammad A, Ling J, Alasmari F. Factors associated with glycemic control among patients with type 2 diabetes: a cross-sectional study. Eur Rev Med Pharmacol Sci. 2022;26(7):2415–2421. doi:10.26355/eurrev_202204_28475
40. Zamanillo-Campos R, Zaforteza Dezcallar M, Boronat Moreiro MA, et al. Non-adherence to non-insulin glucose-lowering drugs: prevalence, predictors and impact on glycemic control and insulin initiation. A longitudinal cohort study in a large primary care database in Spain. Eur J Gen Pract. 2023;29(1):2268838. doi:10.1080/13814788.2023.2268838
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Self-Efficacy, Exercise Anticipation and Physical Activity in Elderly: Using Bayesian Networks to Elucidate Complex Relationships
Chen X, Yang S, Zhao H, Li R, Luo W, Zhang X
Patient Preference and Adherence 2022, 16:1819-1829
Published Date: 28 July 2022
The Impact of Smartphone Addiction on Chinese University Students’ Physical Activity: Exploring the Role of Motivation and Self-Efficacy
Lin B, Teo EW, Yan T
Psychology Research and Behavior Management 2022, 15:2273-2290
Published Date: 23 August 2022
Self-Efficacy as Moderator and Mediator Between Medication Beliefs and Adherence in Elderly Patients with Type 2 Diabetes
Wu J, Shen J, Tao Z, Song Z, Chen ZL
Patient Preference and Adherence 2023, 17:217-226
Published Date: 21 January 2023
Drug Attitude and Medication Adherence of Patients with Early Psychosis in South Korea: Mediating Effect of Medication Adherence Self-Efficacy
Choi YA, Kweon YR
Patient Preference and Adherence 2023, 17:1247-1255
Published Date: 12 May 2023
Community Efficacy for Non-Communicable Disease Management and Medication Adherence: The Sequential Mediating Role of Self-Efficacy and Depressive Symptoms
Zhu G, Malhotra R, Xiong S, Chen X, Zhang M, Wu Y, Gong E, Wang Z, Tian X, Peng W, Østbye T, Yan LL
Patient Preference and Adherence 2023, 17:3421-3433
Published Date: 14 December 2023