")
Back to Journals » International Journal of Women's Health » Volume 14
Determinants of Disagreement with Female Genital Mutilation Among Mothers
Authors Keles E , Eker HH, Bektemur G, Hilowle IA , Kassim MM , Hassan-Kadle MA , Adali A , Karaketir Ş
Received 25 September 2022
Accepted for publication 6 December 2022
Published 28 December 2022 Volume 2022:14 Pages 1863—1870
DOI https://doi.org/10.2147/IJWH.S391043
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Esra Keles,1 Hasan Huseyin Eker,2 Guven Bektemur,3 Ifrah Adan Hilowle,4 Mohamed Mukhtar Kassim,5 Mohamed Abdulkadir Hassan-Kadle,6,7 Ali Adali,5 Şeyma Karaketir8
1Department of Gynecologic Oncology, University of Health Sciences Turkey, Kartal Lütfi Kırdar City Hospital, Istanbul, Turkey; 2Department of Public Health, University of Health Sciences Turkey, Mogadishu Somalia-Turkey Recep Tayyip Erdoğan Training and Research Hospital, Mogadishu, Somalia; 3Department of Public Health, University of Health Sciences Turkey, Faculty of Hamidiye Medicine, Istanbul, Turkey; 4Department of Education, University of Health Sciences Turkey, Mogadishu Somalia-Turkey Recep Tayyip Erdoğan Training and Research Hospital, Mogadishu, Somalia; 5Department of Pediatrics, University of Health Sciences Turkey, Mogadishu Somalia-Turkey Recep Tayyip Erdoğan Training and Research Hospital, Mogadishu, Somalia; 6College of Medicine and Health Science, Abrar University, Mogadishu, Somalia; 7CenterFor Digestive & Liver Diseases, SomGastro Clinic, Mogadishu, Somalia; 8Department of Public Health, Istanbul University, Occupational Health Training Programme, Istanbul School of Medicine, Istanbul, Turkey
Correspondence: Mohamed Abdulkadir Hassan-Kadle, College of Medicine and Health Science, Abrar University, Hodan District, Benadir Region, Mogadishu, Somalia, Tel +252 68 5910409, Email [email protected]
Aim: Female genital mutilation (FGM) is widely practiced in Somalia. Limited data are available on the attitude of the Somalia community regarding FGM. The present study aimed to explore the attitude of mothers toward the practice of FGM.
Methods: A cross-sectional study was conducted from March to July 2021 among mothers attending outpatient clinics at a tertiary referral hospital in Mogadishu, Somalia.
Results: A total of 247 participants were included, 65.2% of whom believed this practice should be continued. The most cited reason reported regarding FGM was a requirement for religion (90.7%). About 73.9% of mothers stated that the most cited reason reported regarding the abandonment of FGM was health complications. About 59.8% of the study participants thought that FGM could be stopped through education. The results revealed that women who graduated from primary school (OR: 2.21; 95% CI: 1.090– 4.51), who had no social media account (OR: 2.305; 95% CI: 1.147– 4.633), and women who were circumcised by a traditional birth attendant (OR: 4.55; 95% CI: 1.57– 13.22) were more likely to think that FGM should be continued compare with their counterparts.
Conclusions: We found that mothers who were less educated, had no social account and those circumcised by a traditional birth attendant had more positive attitudes toward FGM.
Keywords: female genital mutilation, female genital cutting, education, Somalia
Introduction
Female genital mutilation (FGM) refers to “all procedures involving partial or total removal of the external female genitalia, or any other injury to the female genital organs without medical indication”.1 More than 200 million girls and women have undergone FGM in Africa, the Middle East, and Asia, and an estimated 3 million girls are at risk of cutting every year.2 This practice remains to be a major public health problem in highly prevalent regions like Somalia.3
FGM has no known health benefits and can lead to drastic short- and long-term health consequences. The practice is often performed under unsterile conditions by a traditional birth attendant or a traditional circumciser. FGM has been recognized as a violation of human rights.4,5
FGM is often deeply entrenched in cultural and traditional structures and therefore shapes and influences individuals’ views and attitudes toward FGM.6 The reason for the continuation of FGM varies from one region and ethnic group to another. In Ethiopia, the practice is performed as a rite of passage to adulthood,7 while in Somalia, it is performed as a requirement of religion and a means to ensure a girl’s proper marriage.8 The other reasons given to justify FGM vary within and between regions, countries, and tribes, and include purification, feminity, virtue, family honor, aesthetic reasons, enhancing fertility, virginity, custom, and tradition.9
According to the 2020 Somali Health and Demographic Survey, 99% of girls and women aged 15 to 49 have been subjected to FGM, the majority at the age of 5–9 years.10 Type IIIb FGC is the most extensive type of genital cutting and the most frequently practiced in Somalia.1 This indicates that FGM deeply embedded religious and social beliefs in the context of psychosexual and personal motives, making it extremely difficult to end the practice of FGM.11 Understanding and addressing the drivers of FGM might help policymakers and stakeholders to develop and implement appropriate intervention strategies to reduce and eliminate FGM in Somalia. Therefore, we aimed to investigate the attitudes of mothers toward the practice of FGM.
Methods
This was a descriptive and cross-sectional study conducted between March and July 2021, to evaluate the attitude towards FGM on mothers who attended children’s outpatient clinics of Mogadishu Somali-Turkey Recep Tayyip Erdogan Training and Research Hospital, a tertiary referral hospital with a 200-bed capacity and provides comprehensive level care in the Mogadishu and nearby districts. Mogadishu is the largest city in Somalia with a total population of 2.587.183 people, with 51.0% in living in urban areas. Forty-nine percent of the total population were female, of which 50% were women aged 15–49. Somalia has the highest prevalence rate of FGM (98%) in the world.12
Mothers were invited to take part in the study by a trained midwife (I.AH). Research participants who accepted to participate were briefed about the purpose, methods, and voluntary nature of participation and that they could withdraw from the study at any moment. They were assured that their responses would remain anonymous and confidential. After obtaining written and verbal informed consent, face-to-face interviews were conducted with the research participants using a structured questionnaire (Supplementary Material), which was prepared by reviewing relevant literature on the topic.13,14 The questionnaire comprised of two parts. The first part covered demographic and socioeconomic information. The second part included questions related to mothers’ opinions toward the continuation or discontinuation of FGM, the major reason for the continuation of the practice, any efforts to abandon the practice, age at the time of the procedure, and by whom it was performed.
We performed a sample size calculation based on a previously published study.15 A minimum sample size of 151 was calculated using the OpenEpi software package survey formula using 91% prevalence with a 5% margin of error at a 95% confidence level after considering a 20% nonresponse rate. All participants who applied to polyclinics and met the study criteria were randomly assigned to work without prior knowledge. Missing data were rare and less than 5% for all variables included in the analysis.
Mothers were eligible if they had at least one daughter, were 18 years of age or older, were willing to engage in the study, were able to provide informed consent, and were able to communicate sufficiently with the midwife. Those mothers with mental disorders were excluded from the study.
Database management complies with legislation on privacy and this research is in accordance with the 1964 Declaration of Helsinki and its subsequent amendments or comparable ethical standards. Approval for this research was obtained from the Research Ethics Committee of Mogadishu Somali-Turkey Recep Tayyip Erdogan Training and Research Hospital (Approval number: MSTH/5534 number: 331).
Statistical Analyses
The data analysis was performed using Statistical Package for the Social Sciences (SPSS) for Windows, (Version 23.0.; IBM Corp., Armonk, NY, USA). Descriptive statistics such as mean and standard deviation (mean ± SD) for continuous variables and frequency and percentage for categorical variables were used to describe the quantitative data. The one-sample Kolmogorov–Smirnov test was used for testing the normality of the data distribution. The χ2 test or Fisher’s Exact Test was used to compare categorical variables, and Student’s t-test or Mann–Whitney U-test for continuous variables. Confounding was controlled by a logistic regression analysis. Significant factors identified from univariate analysis were included in the multivariate logistic regression model. The Hosmer-Lemeshow test was used to assess the goodness of fit of the logistic regression model. The odds ratios (OR) and 95% confidence intervals (CI) are reported. A p-value of ≤0.05 was taken for statistical significance.
Results
The sociodemographic characteristics of mothers who agree or disagree with the continuation of the practice are shown in Table 1. A total of 247 participants were included in the present study. The mean age of mothers who had an opinion on continuation was 31±8.0 years, the mean age at first cut was 8±2.1 years, the mean age at marriage was 19±4.8 years, and those who disagreed on continuation were 32±7,0 years, 7±1.6 years, and 19±4.0 years, respectively. Mothers’ education status, having social media account, and by whom the practice was performed were factors found to be statistically significantly associated with whether mothers want that the practice should continue or stop. With regard to educational status, at least five out of ten mothers (54.4%) without formal education wanted FGM to continue whereas 9.5% of those with higher education wanted to do the same (p=0.004). Noteworthy differences in having a social media account can be seen in the study sample, it was found that 57% of mothers who support the continuation of the practice had a social media account, while this was in 81.2% of mothers who disagreed with the continuation of the practice (p≤0.001). It was found that a great proportion (69.2%) of women who favor the continuation of FGM practice were circumcised by a traditional circumciser. Fifteen percent of mothers who favor the discontinuation of FGM practice were circumcised by a doctor (p=0.002).
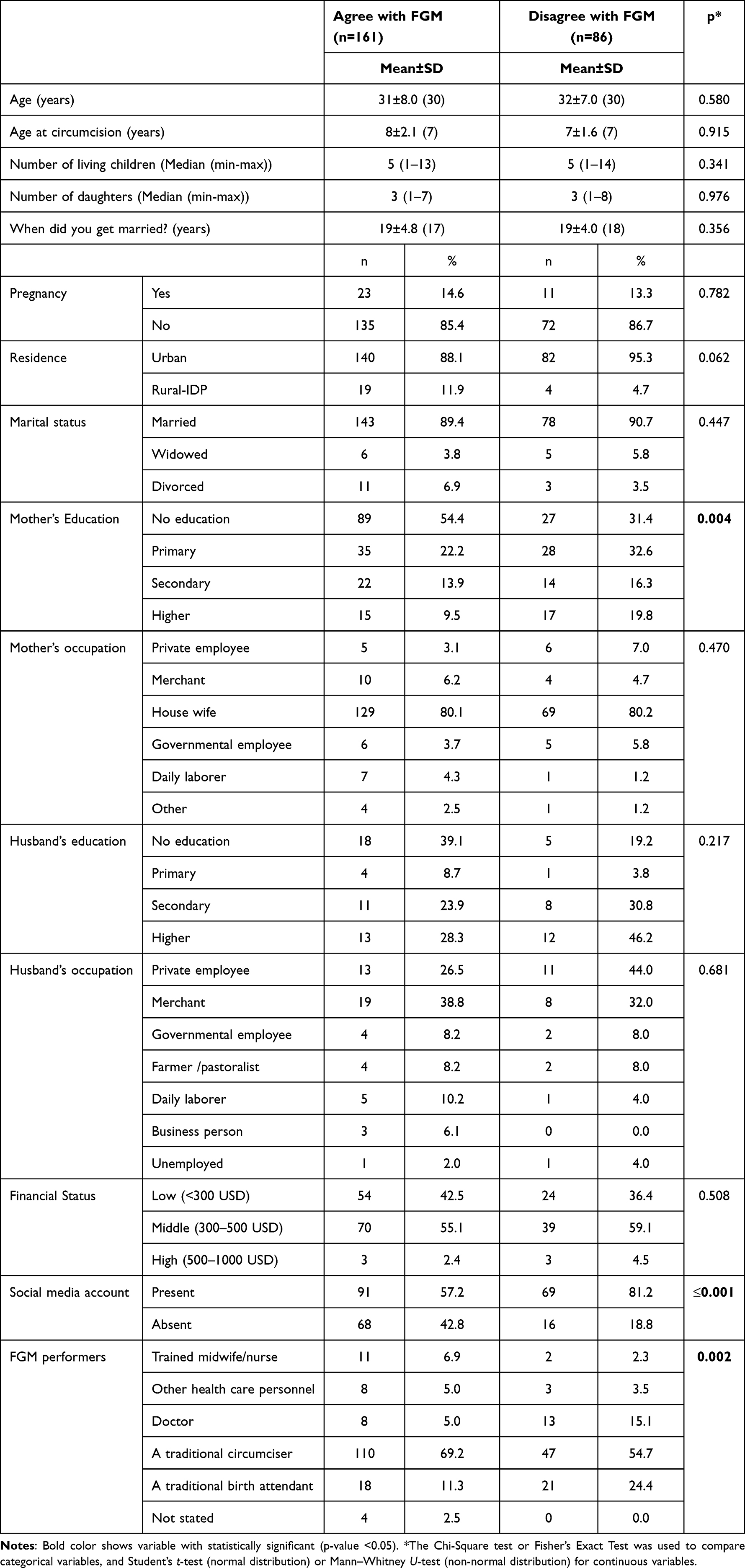 |
Table 1 Comparison of Characteristics of Mothers Who Have Concordant or Discordant Opinions About the Continuation of FGM |
Table 2 presents the questions which were designed to measure the attitude of mothers toward the practice of FGM. Mothers were asked whether the FGM practice should be continued or not. Sixty-five percent mother believed that this practice should continue, while 35% believed that the practice should be stopped. Ninety percent of mothers reported that FGM was a requirement for religion (90.7%). About 73.9% of mothers stated that the most important reason for the abandonment of FGM was health complications. When the mothers were asked about the recommendation of circumcision by their religion: 62.4% of mothers thought it was recommended while 36.0% of mothers thought that it was not recommended and approximately 1.6% of mothers answered: “no comment” to this question. About 59.8% of the study participants who had a positive attitude toward the discontinuation of the practice believed that FGM could be stopped through education.
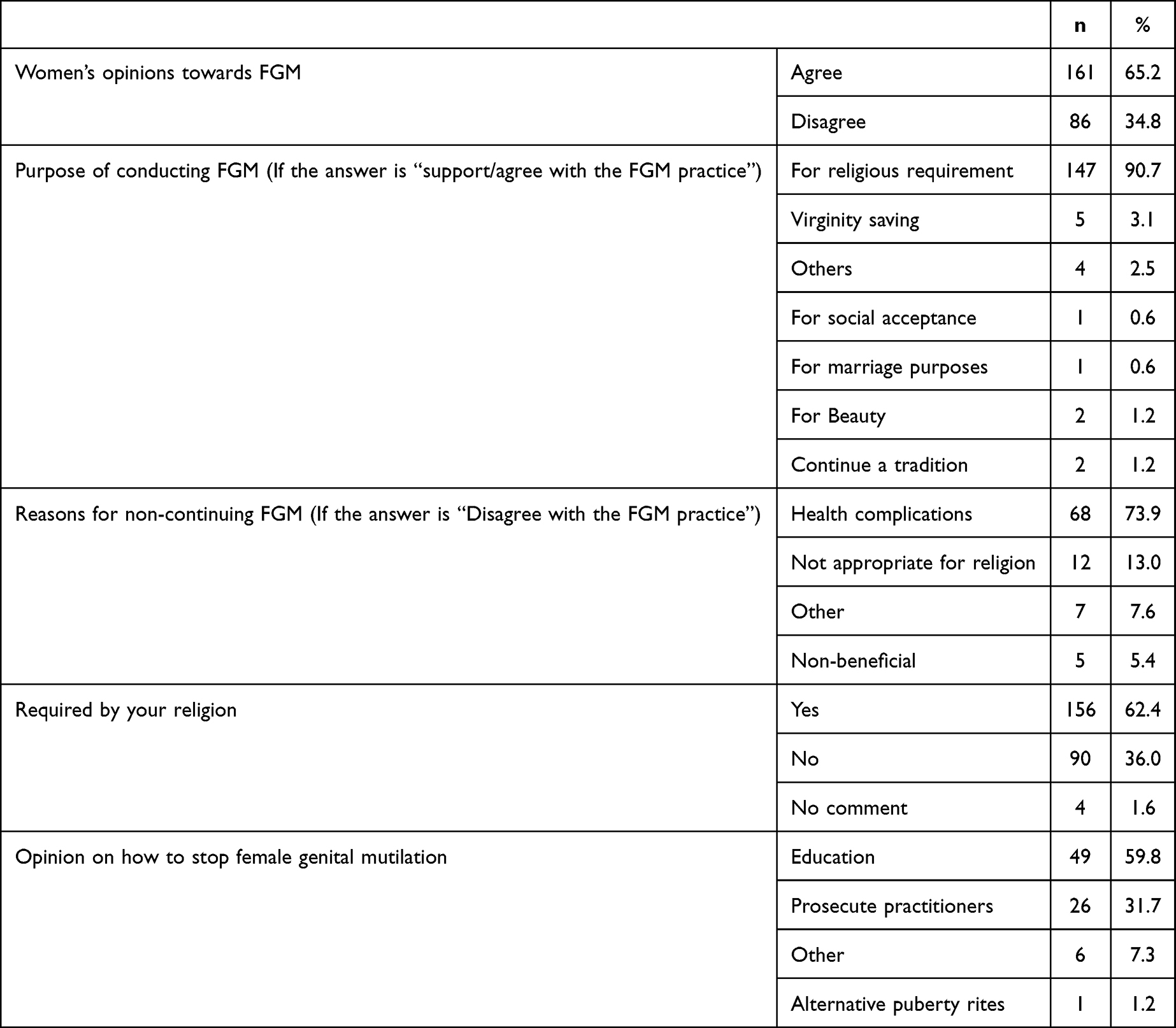 |
Table 2 Reasons for Final Decision of Mothers to Either Cut Their Daughter or Leave Her Uncut |
Table 3 presents the results of a regression analysis of the independent variables and the outcome variable. Education status, having social media account, and by whom the practice was performed were significantly different between the two groups. The results revealed that, mothers who graduated from primary school (OR: 2.21; 95% CI: 1.090–4.51), who had a social media account (OR: 2.305; 95% CI: 1.147–4.633), and mothers who were circumcised by a doctor (OR: 4.55; 95% CI: 1.57–13.22) were more likely to think that FGM should be discontinued compared with their counterparts, had no education, had no social media, and who circumcised by a traditional birth attendant.
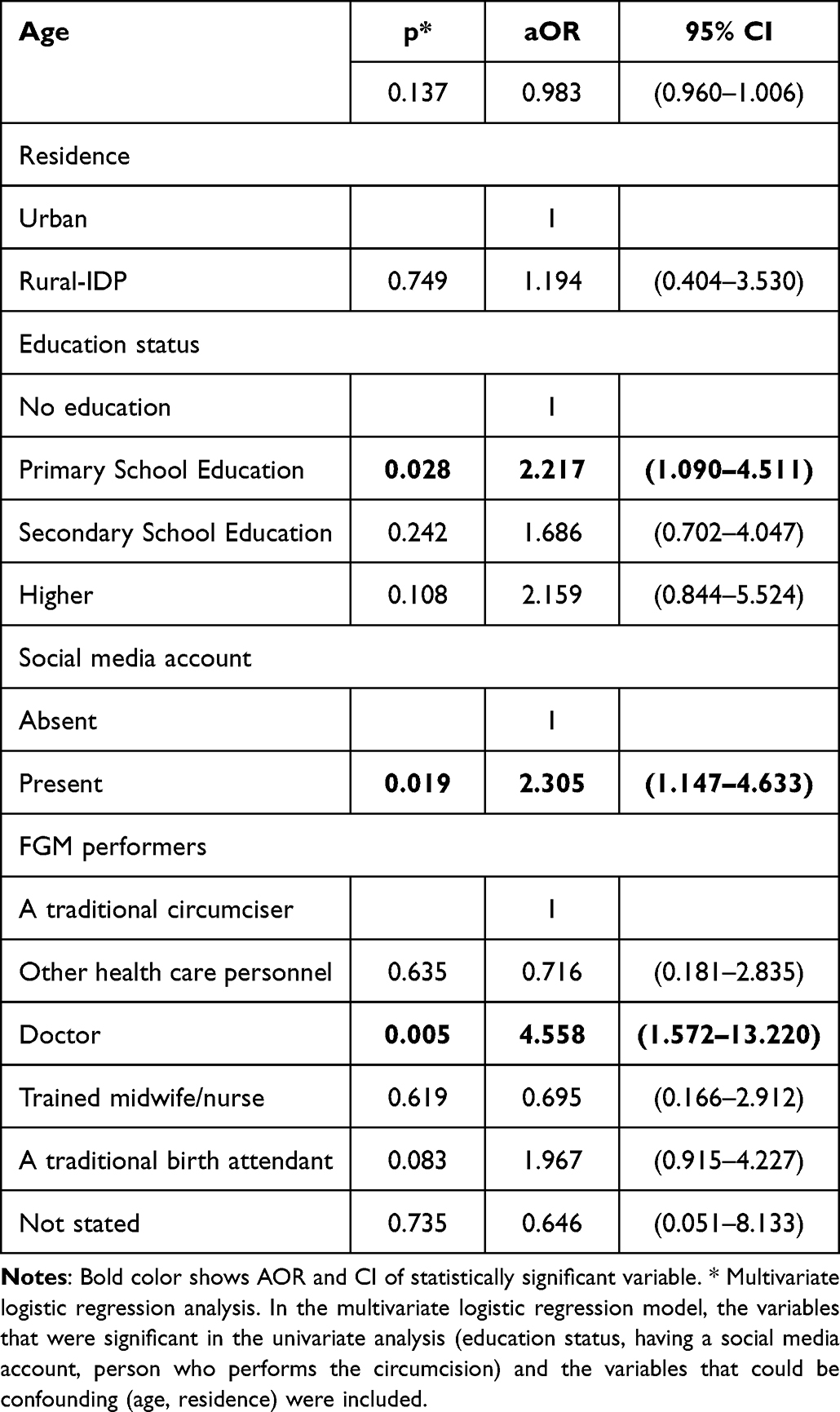 |
Table 3 Predictors of the Mothers’ Decision Not to Cut Their Daughter |
Discussion
The FGM practice is still a neglected public health problem necessitating urgent response in Somalia. The findings of this study indicated a significant proportion of mothers adopted a positive attitude towards the continuation of FGM, with religious requirements as the most underpinning reason. Whereas mothers who had negative attitude toward the practice are those better educated and who had social media. Health concerns were the most commonly cited reasons by mothers for choosing not to cut their daughters.
The present study found that mothers who had no formal education had more positive attitudes toward FGM. These results were in line with the earlier studies that have investigated the association between education and FGM.6,16–19 Education formed the central focus of a study by Ameyaw et al from Sierra Leone in which the authors found that as the levels of education of the women increased, their intention to cut their daughters decreased.20 Similarly, a recent community-based study from Sudan showed that education plays a key role in mothers taking a decision on cutting their daughters or their attitude towards the practice.16 Another study carried out in Nigeria also found that people with no formal education were more likely to support the continuation of FGM.21 Additionally, Rawat et al investigating FGM across six African countries concluded that education is vital in ending FGM.22 A possible explanation might be that educated women are aware of the adverse health effects of FGM and understand the short- and long-term consequences of the practice. As noted by researchers, education is an essential and crucial part of multi-sectoral interventions aimed at eliminating FGM, as it alone is not sufficient to end FGM.21
The current study found that mothers who reported having a social media account more likely to choose not to cut their daughters. A recent study in Sudan showed that households exposed to anti-FGM campaigns were more likely to support the discontinuation of FGM.22 Similarly, another study in Egypt reported that women who were exposed to mass media were more likely to support the abandonment of the practice.18 This might be attributed to the fact that individuals with access to mass media are more aware of the harmful health consequences of FGM. More efforts are needed to understand the characteristics of individuals with limited access to mass media and to determine the most effective approaches to transmit FGM abandonment messages to these groups.
There are many social drivers and root causes of FGM including social acceptance, proof of virginity, religion, and tradition.23 The present study found that health concerns were the most commonly cited reasons for the discontinuation of FGM, while religious requirements were for its continuation. In a study in Ethiopia, the percentage of circumcised women was lowest among Orthodox women and highest among Muslim women.24 By contrast, in Nigeria, the prevalence rates were lowest among Muslim populations and highest among Christian populations.25 This implies that FGM is practiced in most of the countries on the African continent across religions and cultures for thousands of years.25,26 Governments and anti-FGM program implementers must attract the support of local religious and community leaders. It may be effective if the campaigns focus on the religious interpretation of FGM and its adverse health effects, which may shift the attitudes toward FGM.24,27
The study was limited as it reflected the perspectives of a small number of people who participated in the research. Since the determinants of FGM might differ from region to region, the findings could not be generalized to the whole Somalia community. In addition, the interviews were conducted with only recruited mothers who visited a health center so women’s perceptions may not reflect the views of men and may lead to unconscious bias. Restricting the study sample to women who presented to the obstetrics and gynecology outpatient clinics at a hospital may limit the utility of the study findings, and thus may not be generalized to the wider population. Finally, the study is cross-sectional in nature, causal inferences should be made with caution. One of the significant strengths of this study is that it captured several background characteristics such as the age of the daughters, the total number of children, and the total number of daughters which might influence the mothers’ decision to leave their daughters uncut.
This paper has identified the possible drivers of FGM including religious requirements, lack of education, and limited access to social media. While raising awareness of FGM and its health consequences is critical, programs for abandonment of the practice must engage education and mass media.
Data Sharing Statement
The dataset used and/or analyzed in the study are available from the corresponding author on reasonable request.
Ethical Statement
Ethical approval for this study was provided by the Somalia. Mogadishu–Turkey Recep Tayyip Erdogan Training and Research Hospital Ethics Committee (Approval number: 24.02.2021- MSTH/5534). The database management in accordance with privacy legislation and the presented study in accordance with the ethical principle of the Declaration of Helsinki.
Acknowledgments
The authors would like to thank the study participants for their contribution.
Funding
No funds were received in support of this work. No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript.
Disclosure
The authors report no conflicts of interest.
References
1. World Health Organization. Eliminating female genital mutilation: an interagency statement UNAIDS, UNDP, UNECA, UNESCO, UNFPA, UNHCHR, UNHCR, UNICEF, UNIFEM. WHO; 2008. Available from: http://apps.who.int/iris/bitstream/10665/43839/1/9789241596442_eng.pdf.
2. World Health Organization. Female genital mutilation: fact sheet. World Health Organization; 2016; Available from: www.who.int/mediacentre/factsheets/fs241/en/.
3. Chalmers B, Hashi KO. 432 Somali women’s birth experiences in Canada after earlier female genital mutilation. Birth. 2000;27(4):227–234. PMID: 11251507. doi:10.1046/j.1523-536x.2000.00227.x
4. World Health Organization. Female genital mutilation. Fact sheet N° 241. World Health Organization; 2014. Available from: https://apps.who.int/iris/bitstream/handle/10665/112328/WHO_RHR_14.12_eng.pdf.
5. United Nations Children’s Fund. Female Genital Mutilation/Cutting: a statistical overview and exploration of the dynamics of change. UNICEF; 2013. Available from: https://data.unicef.org/resources/fgm-statistical-overview-and-dynamics-of-change/.
6. Pashaei T, Rahimi A, Ardalan A, et al. Related factors of female genital mutilation (FGM) in Ravansar (Iran). J Women’s Health Care. 2012;1(2):1000108. doi:10.4172/2167-0420.1000108
7. EGLDAM. Old Beyond Imaginings: Ethiopia Harmful Traditional Practices. National Committee for Traditional Practices in Ethiopia (NCTPE); 2008. Available from: https://www.cartercenter.org/resources/pdfs/health/ephti/library/modules/degree/mod_htp_final.pdf.
8. Hussein MA, Adem A, Mohammed MA. Knowledge, attitude and practice of female genital mutilation among women in Jigjiga Town, Eastern Ethiopia. Gaziantep Med J. 2013;19(3):164–168. doi:10.5455/GMJ-30-2013-157
9. Alo OA, Gbadebo B. Intergenerational attitude changes regarding female genital cutting in Nigeria. J Womens Health. 2011;20(11):1655–1661. doi:10.1089/jwh.2010.2610
10. Somalia National Bureau of Statistics. Federal Government of Somalia. The Somali Health and Demographic Survey; 2020. Available from: https://somalia.unfpa.org/sites/default/files/pub-pdf/shds_report_2020_1.pdf.
11. Masho SW, Matthews L. Factors determining whether Ethiopian women support continuation of female genital mutilation. Int J Gynaecol Obstet. 2009;107(3):232–235. doi:10.1016/j.ijgo.2009.07.022
12. United Nations Children’s Fund. Somalia: multiple indicator cluster survey. UNICEF; 2006. Available from: https://www.unicef.org/northmacedonia/reports/multiple-indicator-cluster-survey-2005-2006.
13. Abathun AD, Sundby J, Gele AA. Attitude toward female genital mutilation among Somali and Harari people, Eastern Ethiopia. Int J Womens Health. 2016;8:557. doi:10.2147/IJWH.S112226
14. Pashaei T, Ponnet K, Moeeni M, et al. Daughters at risk of female genital mutilation: examining the determinants of mothers’ intentions to allow their daughters to undergo female genital mutilation. PLoS One. 2016;11(3):e0151630. doi:10.1371/journal.pone.0151630
15. Adigüzel C, Baş Y, Erhan MD, et al. The female genital mutilation/cutting experience in somali women: their wishes, knowledge and attitude. Gynecol Obstet Invest. 2019;84(2):118–127. doi:10.1159/000493130
16. Sabahelzain MM, Eldin AG, Babiker S, et al. Decision-making in the practice of female genital mutilation or cutting in Sudan: a cross-sectional study. Glob Health Res Policy. 2019;4:5. doi:10.1186/s41256-019-0096-0
17. Afifi M. Women’s empowerment and the intention to continue the practice of female genital cutting in Egypt. Arch Iran Med. 2009;12(2):154–160.
18. Dalal K, Lawoko S, Jansson B. Women’s attitudes towards discontinuation of female genital mutilation in Egypt. J Inj Violence Res. 2010;2(1):41. doi:10.5249/jivr.v2i1.33
19. Tamire M, Molla M. Prevalence and belief in the continuation of female genital cutting among high school girls: a cross-sectional study in Hadiya Zone, Southern Ethiopia. BMC Public Health. 2013;13(1):1–9. doi:10.1186/1471-2458-13-1120
20. Ameyaw EK, Tetteh JK, Armah-Ansah EK, et al. Female genital mutilation/cutting in Sierra Leone: are educated women intending to circumcise their daughters? BMC Int Health Hum Rights. 2020;20(1):1. doi:10.1186/s12914-020-00240-0
21. Rawat R. The association between economic development, education and FGM in six selected African countries. J Midwifery Womens Health. 2017;11(3):137–146. doi:10.12968/ajmw.2017.11.3.137
22. Al Nagar S, Gindeel RH, Salah A. Understanding the key elements for designing and implementing social marketing campaigns to inform the development of creative approaches for FGM/C abandonment in Sudan. Evidence to End FGM/C: research to Help Women Thrive. New York: Population Council; 2018. doi: 10.31899/rh6.1040.
23. United Nations Children’s Fund. Changing a harmful social convention: female genital mutilation/cutting, Innocenti Digest, no 12. UNICEF; 2005. Available from: https://www.unicef-irc.org/publications/396-changing-a-harmful-social-convention-female-genital-mutilation-cutting.html.
24. Abathun AD, Gele AA, Sundby J, et al. Attitude towards the practice of female genital cutting among school boys and girls in Somali and Harari regions, eastern Ethiopia. Obstet Gynecol Int. 2017;2017. doi:10.1155/2017/1567368
25. Anuforo PO, Oyedele L, Pacquiao DF. Comparative study of meanings, beliefs, and practices of female circumcision among three Nigerian tribes in the United States and Nigeria. J Transcult Nurs. 2004;15(2):103–113. doi:10.1177/1043659603262486
26. Kaplan-Marcusan A, Torán-Monserrat P, Moreno-Navarro J, et al. Perception of primary health professionals about female genital mutilation: from healthcare to intercultural competence. BMC Health Serv Res. 2009;9(1):1–8. doi:10.1186/1472-6963-9-11
27. Ahmed HM, Kareem MS, Shabila NP, et al. Knowledge and perspectives of female genital cutting among the local religious leaders in Erbil governorate, Iraqi Kurdistan region. Reprod Health. 2018;15(1):1–4. doi:10.1186/s12978-018-0459-x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.