")
Back to Journals » Psychology Research and Behavior Management » Volume 16
Determinants of Depressive Symptoms Among Patients with Rheumatoid Arthritis in China: A Structural Equation Model
Received 4 July 2023
Accepted for publication 11 October 2023
Published 17 October 2023 Volume 2023:16 Pages 4197—4208
DOI https://doi.org/10.2147/PRBM.S428892
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Lijuan Zhang,1,2 Weiyi Zhu,1 Beiwen Wu1
1Department of Nursing, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 2School of Nursing, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China
Correspondence: Beiwen Wu, Department of Nursing, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, 197, Ruijin Er Road, Shanghai, 200025, People’s Republic of China, Tel +86 18917762079, Fax +86 54314096, Email [email protected]
Background: This study aimed to examine how personality traits, social support and clinical features including pain, disease activity, functional status, sleep quality, and fatigue influence on depressive symptoms in Chinese rheumatoid arthritis (RA) patients.
Methods: This study was conducted from November, 2022 to June, 2023 among Chinese RA patients. Pain, disease activity, functional status, sleep quality, fatigue, social support, personality traits, and depressive symptoms were assessed. The following relationships among three hypotheses were analyzed by structural equation model (SEM): H1: clinical features have a direct effect on depressive symptoms; H2: personality traits might work as a mediator between clinical features and depression; H3: social support is related to depressive symptoms, being a direct effect or an indirect effect through clinical features or personality traits.
Results: The final model including 326 RA patients presented a good fit (χ2=103, χ2/df=1.69; GFI=0.96; AGFI=0.93; CFI=0.97; TLI=0.96; RMSEA=0.046). Clinical features had a total effect of 0.59 on depressive symptoms, of which β=0.33 (P=0.013) was an indirect effect through personality traits, indicating a mediating influence between this relationship; moreover, there was a significant direct association between clinical features and depressive symptoms (β=0.26; P=0.022). Personality traits (β=− 0.65; P< 0.001) had a much stronger relation with depressive symptoms than with clinical features. Social support had a total effect of 0.81 on personality traits, being a direct effect of β=0.52 (P< 0.001) and an indirect effect of β=0.29 (P< 0.001) through clinical features. The final proposed model explained 77% of the variance of depressive symptoms.
Conclusion: Personality traits had a considerable influence upon depressive symptoms, while social support seemed to have a major effect on personality traits. It is necessary to apply comprehensive assessment and interventions of patients’ personality traits, clinical features, as well as social support, which could optimize their mental health.
Keywords: rheumatoid arthritis, depressive symptoms, structural equation model, personality traits
Introduction
Rheumatoid arthritis (RA) is a chronic systemic inflammatory disease that affects 1% of the global population.1 Chronic painful state of disease and undefined period of treatment severely imperil psychological well-being.2 Depression is the most common mental disorder in RA, with prevalence rates ranging from 14% to 48%.3 A recent systematic review and meta-analysis from China, which included 21 studies for a total of 4447 Chinese RA patients, reported rates of 48% of depression.4 Various studies illustrate the negative effects of depression in the context of RA, including the low disease remission and treatment response,5 high levels of pain and disease activity,6 increased functional disability,7 reduced health-related quality of life,6 as well as increased mortality,8,9 which add to the disease burden. These highlight that depression among RA patients should be paid more attention than it usually receives from health professionals, not only because it can improve mental health, but also because it can help to aid in management of physical aspects of the disease.
Research10–14 on depressive symptoms and its related factors, such as social demographic factors (eg, age, gender, low socioeconomic status), pain, disease activity, functional status, fatigue and sleep quality has been conducted for a long time. However, there is some uncertainty regarding the relationship between sociodemographic factors and depressive symptoms, possibly, due to some differences among self-report scales for assessing depressive symptoms from different region. From example, a study from Iran14 reported that there was no statistically significant association between sociodemographic factors including gender, income or employment status, and depressive symptoms of RA patients, while Ng KJ et al15 found that female, income, and employment status were significant associated with depressive symptoms among RA patients. To date, much research7,13,14,16 have demonstrated that persistent pain, high disease activity, functional disability, fatigue and sleep disorders have great impacts on depressive symptoms in RA. Therefore, we designated a latent variable named clinical features to denote pain, disease activity, functional status, fatigue and sleep quality in this study. Moreover, we considered that clinical features should have a direct effect on depressive symptoms in Chinese RA patients.
There is a vast amount of literature17–19 describing a relationship between personality and depression. This link can be traced to the major theory of personality predispositions to depression, which indicates that individuals with high levels of self-criticism and/or dependency tend to suffer from depression following negative life events.20 RA is a chronic disease with psychiatric problems, which brings a heavy burden to patients.8 Considering the relevance of the relationship between personality and depression among the general population, it is necessary to investigate whether this association extends to Chinese RA patients or not. Personality seems to be an important psychological variable, which should be taken into consideration because it predisposes to the experience of depression.21,22 Only a study from Portugal23 concluded that personality seemed to play a pivotal mediating role in the relationship between disease impact and depressive symptoms among RA patients. Considering the different study populations and various self-reported tools used, the result is specific to the samples included in the study and can hardly be generalized to Chinese RA patients because there are significant differences in culture, lifestyle and diet between Chinese and Westerners. Therefore, it is essential to examine whether personality plays a mediating variable in the path to depressive symptoms among Chinese RA patients or not.
RA also brings a heavy burden to both family and society.24 There is a growing interest in the relationship between social support and depressive symptoms among RA patients.25–27 Social support is supposed to protect mental health both directly through the benefits of social relationships and indirectly as a buffer against stressful circumstances.28 In some patients with chronic diseases, low level of social support is related to the occurrence of depressive symptoms when exposed to disease.29–31 Similarly, social support is beneficial to the psychological adjustment of RA, and low-level social support has a strong positive association with the experience of depressive symptoms among people suffering from RA.26,27 As it is known, personality plays an important role in the ability to develop and maintain interpersonal relationships and in both the appraisal and effectiveness of supportive interactions that take place in the context of these relationships.20 One study conducted in Netherlands32 found that personality and social support as predictors of first and recurrent episodes of depression. Based on these data, we suggest that social support may play a pivotal role in the relationships among clinical features, personality and depressive symptoms in RA patients.
Most studies10–14 examined risk factors of depressive symptoms using the t-test, chi-square test and multifactor logistic/linear regression analysis, which could not analyze the direct and indirect effects of risk factors. The structural equation model (SEM) is a popular method which can fill this gap and quantitatively evaluate the size of the risk factors’ effect or calculate the error of the measurement variables.33 Thus, the current study was conducted to assess not only the interactions among clinical features, personality traits, social support, and depressive symptoms but also the magnitude of the interactions among these factors. A better understanding of these relationships is of great importance to improving mental health outcomes by optimizing the design of interventions. Based on an in-depth literature review, we hypothesized the following: H1: clinical features including pain, disease activity, functional status, sleep quality, and fatigue have a direct effect on depressive symptoms in Chinese RA patients; H2: personality traits might work as a mediator between clinical features and depression; H3: social support is related to depressive symptoms, being a direct effect or an indirect effect through clinical features or personality traits.
Materials and Methods
Participants
RA patients were recruited from the Ruijin Hospital, Shanghai Jiao Tong University School of Medicine between November 2022 and June 2023. When patients came to the hospital for RA-related issues, they were asked if they want to participate in the study. We explained the purpose of the study to the patients, assuring them that all of the information that they provided would remain anonymous and confidential. The inclusion criteria were adults, aged 18 years and older with a diagnosis of RA fulfilling the American College of Rheumatology (ACR) 1987 revised criteria34 for the classification of RA. Patients meeting the following criteria were included: (1) they were aged 18 or above; (2) they were diagnosed with RA according to the 1987 ACR criteria; (3) they were willing to provide written informed consent; (4) they were able to interact in Chinese efficiently. Participants who have organic/structural brain disease, cognitive impairment or current severe diseases, such as cancer, serious infections, or cardiac, respiratory, gastrointestinal, endocrine diseases were excluded by querying the electronic medical records. The preset study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Ethics Committee of the Ruijin Hospital, Shanghai Jiao Tong University School of Medicine.
Measurements
Patients were asked to complete demographic and disease questionnaires including age, gender, BMI, marital status, education, employment, yearly income, health insurance, comorbid condition (eg, high blood pressure, diabetes, fatty liver), disease duration, family and hospitalization history, tobacco and alcohol usage. The medication information including the use of disease modifying anti-rheumatic drugs (DMARDs), nonsteroidal anti-inflammatory drugs (NSAIDs), corticosteroids, and biologics was recorded by querying the electronic medical records or patients’ self-reports. However, we did not record psychiatric medication for depression because most RA patients did not have a definite diagnosis of depression before our investigation.
Disease activity was estimated with the valid and reliable 28-joint Disease Activity Score (DAS28).35 It is a continuous measure of RA disease activity that combines information from 28 swollen joint counts, 28 tender joint counts, the rate of erythrocyte sedimentation rate, as well as the patient’s recognition of disease activity from 0cm (not active at all) to 10cm (very active). The 10-cm horizontal visual analogue score (VAS) was used to assess pain.36
Functional status was evaluated by the Health Assessment Questionnaire-Disability Index (HAQ-DI).37 There are 20 questions in eight categories of functioning which represent a comprehensive set of functional activities- dressing, rising, eating, walking, hygiene, reach, grip, and usual activities. Higher scores (ranging 0–3) indicating low functional status. In the study, the Cronbach’α was 0.876.
Fatigue was assessed by the 14-item Fatigue Scale (FS-14).38 FS-14 comprises 14 items with two dimensions: physical fatigue and mental fatigue. The total fatigue score obtained by adding up all items ranges from 0 to 42, with higher scores indicating more severe fatigue. In the study, the Cronbach’α was 0.854.
Sleep quality was evaluated by the Pittsburgh sleep quality index (PSQI).39 The questionnaire consisted of 19 questions, which was divided into seven aspects. Each aspect has a score of 0 (no difficulty) to 3 (severe difficulty). The total score ranged from 0 to 21, with higher scores indicating poor sleep quality. In the current study, the Cronbach’α was 0.871.
The Chinese version of Social support rating scale (SSRS),40 developed by Xiao, is a 10-item scale including three subscales: subjective support (4 items), objective support (3 items), and the utilization of support (3 items). Higher scores indicate high status of social support. In the present sample, the internal consistency was excellent for the total scale (Cronbach’s alpha = 0.791).
Personality was estimated using the Ten Item Personality Inventory (TIPI),41 which is comprised of 10 items (seven-point Likert scale) with five dimensions: extraversion, agreeableness, conscientiousness, emotional stability and openness to experience. Each dimension is scored as the mean of two items, with higher scores indicating a stronger expression of the respective trait. In this study, the Cronbach’α was 0.834.
Depression was assessed using the 7-item Hospital Depression Scale (HDS).42 It is one of the dimensions of the Hospital Anxiety and Depression Scale and has been verified applicable and satisfactorily reliable in clinical settings. The total score of the scale is 0–21 points, with high scores indicating high levels of depressive symptoms. A cut-off ≥8 correspond to possible depression. In the present study, the Cronbach’α was 0.798.
Data Analysis
IBM SPSS (Version 25) was used to conduct descriptive and correlational analyses. Characteristics of baseline data were presented with mean (standard deviation, SD) for continuous variables and frequency (%) for categorical variables. The correlations of study variables (clinical features, personality, social support and depression) were performed by Pearson correlation analyses.
Before the SEM analysis, we analyzed the normality and multicollinearity of all variables included in the model.43 If the absolute values of Kurtosis and Skewness in the model do not exceed 7 and 2 respectively, then the hypothesis of univariate normality would be proved. The analysis results show that all variables (except for functional status scores) were subject to the Kurtosis of below 7 and the Skewness of below 2, however, there existed violation of multivariate normality. Therefore, we applied the Bollen-Stine Bootstrap for Goodness-of-Fit Measures to SEM with non-normal data.44 Multi-collinearity among covariates was estimated via tolerance and variance inflation factor (VIF) as the cutoff recommended thresholds for tolerance <0.1 and VIF >10. VIF values of all variables included in the model were below 5, excluding multicollinearity as an issue.
AMOS 26.0 was used for SEM analysis, and this SEM model estimation was conducted using maximum-likelihood estimation with the Bollen-Stine Bootstrap. Standardized regression (β) coefficients, with the standard errors and P-values for β, were reported for both direct and indirect effects. Statistically significant effects were assumed for P <0.05. Paths were excluded when they were not significant, leading to the readjustment of the initially proposed model. Moreover, the bias-corrected 95% confidence interval (CI) calculated with 5000 bootstrapping re-samples was performed to test the significance of the mediational path.45 If the 95% CI of indirect effect did not contain 0, it indicated that the mediating effect was significant.
As recommended, multiple indices were used to estimate the model fit, including the relative chi-square (χ2/df) test, root mean square error of approximation (RMSEA), the goodness fit index (GFI), the normed fit index (NFI), Tucker-Lewis index (TLI) and the comparative fit Index (CFI). A good fit of the models was assumed when CFI, NFI, TLI and GFI were larger than 0.90 and the value of χ2/df was less than 3.0; RMSEA values <0.05 were considered ideal.46
Result
Patient Characteristics
A total of 342 questionnaires were distributed. If more than one-third of the questionnaire was missed, we would exclude the questionnaire. Finally, 326 valid questionnaires were collected with an effective recovery rate of 95.3%. Participants’ baseline demographic and clinical characteristics are reported in Table 1. Participants were aged 57.18 ± 13.10 years, with mean disease duration of 7.72 years. Among the participants, most of them were females (81.9%), 84.4% reported having been married. Approximately 16.6% of the participants reported Yearly incomes that were lower than 15,000 renminbi (RMB), and 68.7% were higher than 33,000 RMB. Most of them were unemployed (66.3%) and had no identified comorbidities (54.0%). Approximately 77.9% of the individuals used DAMARDs, and 27.9% used biologics. Almost 26.3% (n = 86) of patients had depressive symptoms.
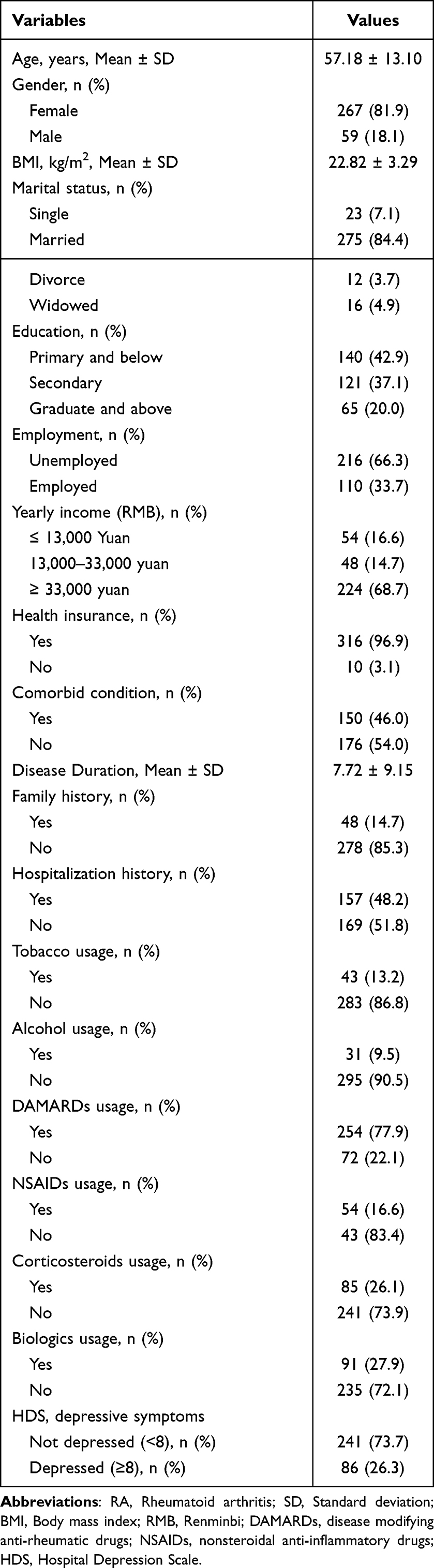 |
Table 1 Characteristics of RA Patients (n=326) |
Bivariate Analysis
The scores and bivariate correlations for all measured variables are presented in Table 2. As expected, depression was found to be positively associated with clinical features including pain, disease activity, functional disability, sleep quality, and fatigue. Subjective support, objective support, and utilization of socio-support were associated, with moderate correlations, with depression and with virtually all aspects of clinical features. Subjective support and utilization of socio-support were not related to DAS28. All personality traits presented low to high negative correlations with depression; low to moderate positive correlations with subjective support, objective support, and utilization of socio-support; and negative correlations, with clinical features, except for DAS28 (not significant at agreeableness).
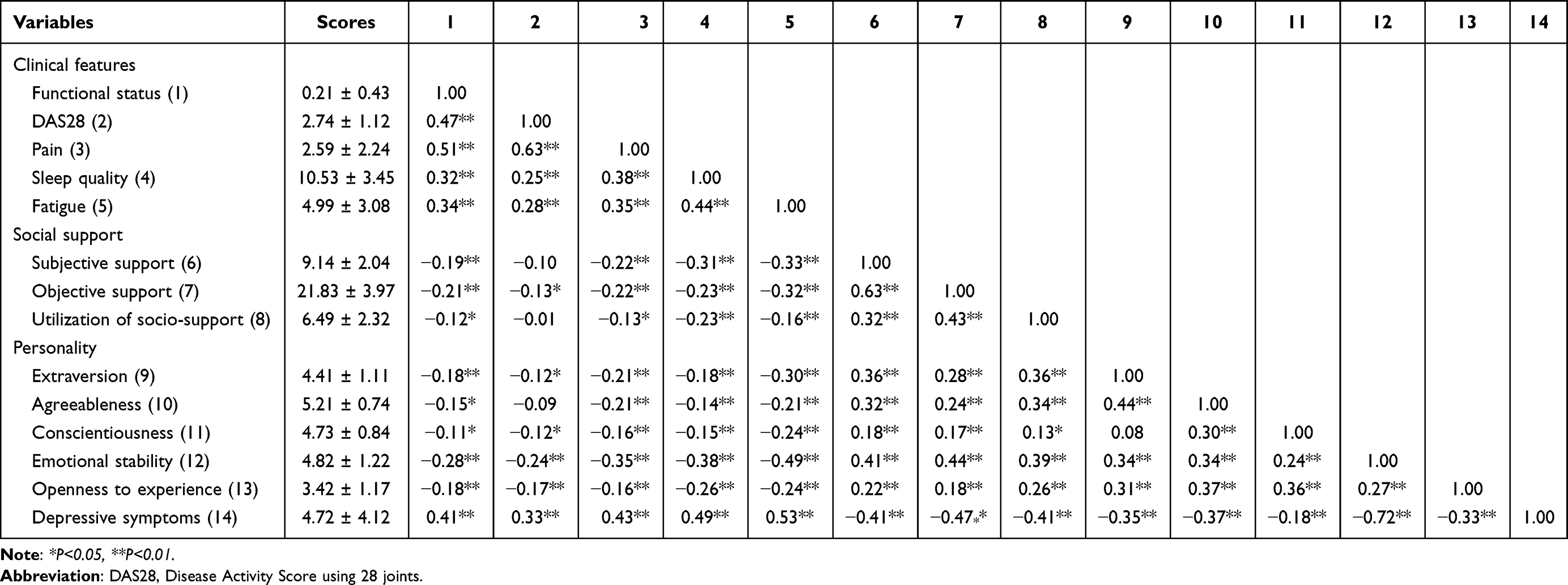 |
Table 2 Correlations and Scores Among All Study Variables (N =326) |
Structural Equation Model
Figure 1 showed the final model. The indices of the goodness-of-fit demonstrated that the final model was an excellent fit to the data, thus permitting the examination of the structural model (χ2=103, χ2/df=1.69; GFI=0.96; AGFI=0.93; CFI=0.97; TLI=0.96; RMSEA=0.046). Although the χ2 statistic was significant (P<0.05), its ratio to the df was acceptable (χ2/df < 3). Standardized regression coefficients for the final model are summarized in Table 3 and Figure 1. The bootstrap indirect effects are reported in Table 4.
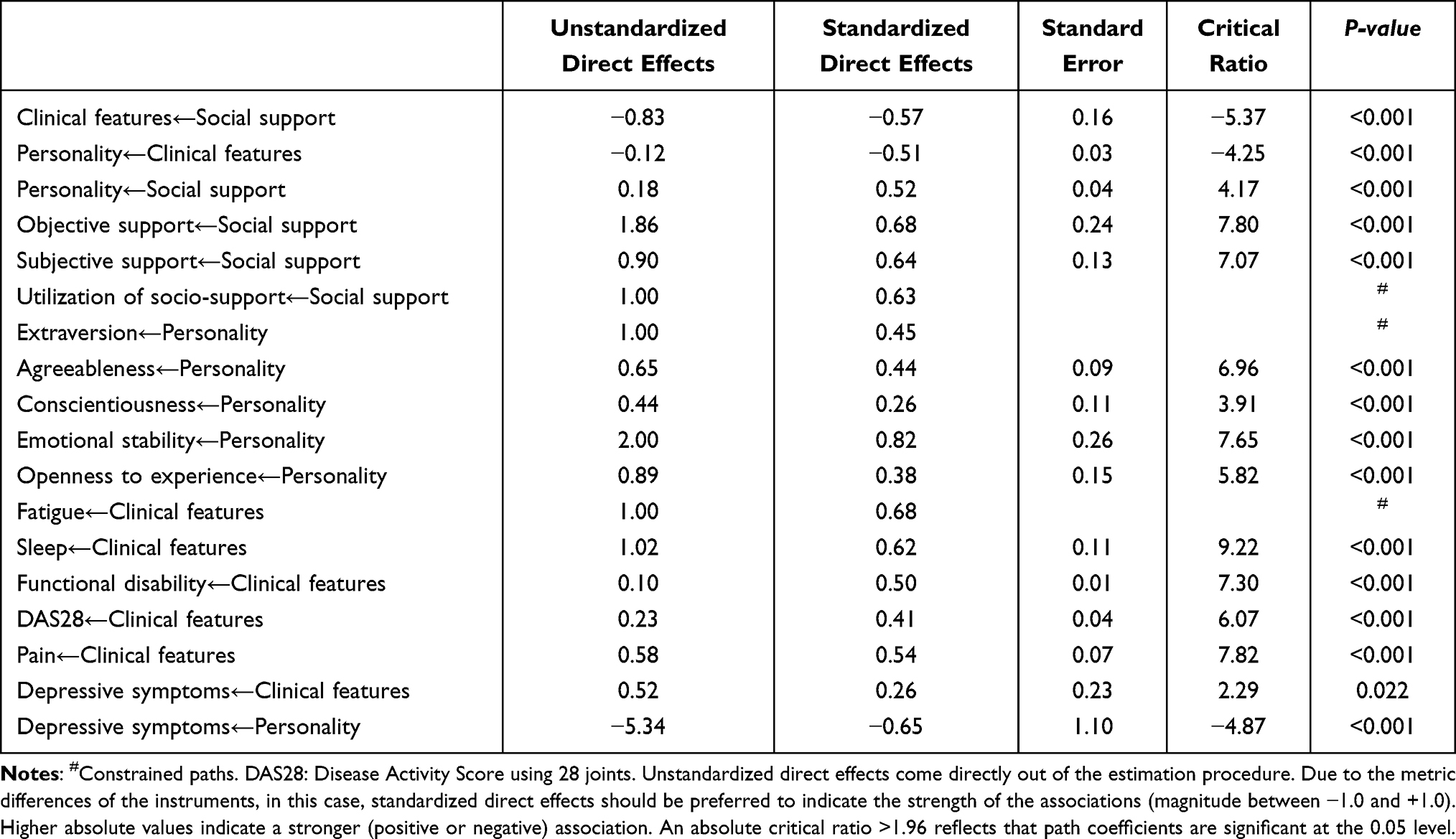 |
Table 3 Regression Weights Between Structural Parameters |
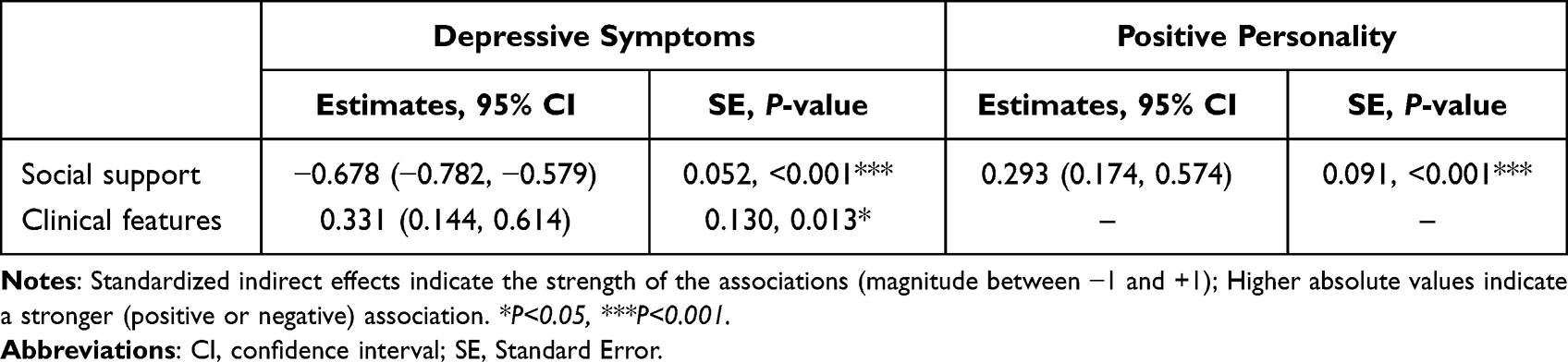 |
Table 4 Bootstrap Results for Indirect Effects Between Structural Parameters |
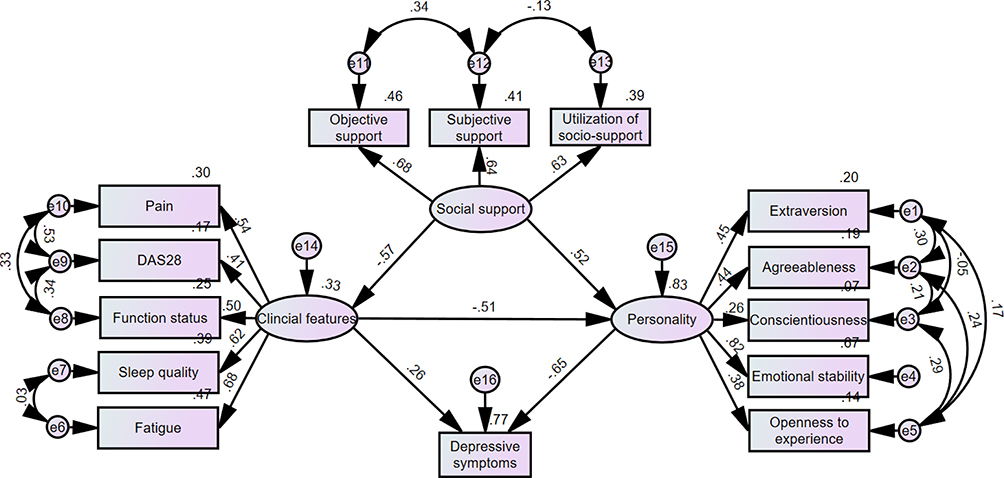 |
Figure 1 Estimated standardized direct effects for the proposed model. |
According to results of SEM: (1) There was a significant direct association between clinical features and depressive symptoms (β=0.26; P=0.022). (2) Clinical features had a total effect of 0.59 on depressive symptoms, of which β=0.33 (P=0.013) was an indirect effect through personality traits, indicating a mediating influence between this relationship; Personality traits (β=−0.65; P<0.001) had a much stronger relation with depressive symptoms than with clinical features. (3) Although there was no direct relationship between social support and depressive symptoms, social support had a total effect of 0.81 on personality traits, being a direct effect of β=0.52 (P<0.001) and an indirect effect of β=0.29 (P<0.001) through clinical features.
The final proposed model explained 77% of the variance of depressive symptoms. The standardized factor load of variables showed that the standardized load of emotional stability was as high as 0.82, indicating that it is the most important factor affecting depression. The standardized load of fatigue, sleep quality, objective support, subjective support and the utilization of support were more than 0.60, while the standardized load of other variables included in the SEM model were all less than 0.60.
Discussion
To our knowledge, this is the first study providing a comprehensive model that illustrates the correlations among clinical features (pain, disease activity, functional status, sleep quality, and fatigue), personality traits, social support and depression in Chinese patients with RA. Indeed, most studies10–14 have investigated the relationships among clinical features, personality traits, social support and depression among RA patients, but they have rarely explored how these factors influenced each other and the magnitude of the interactions among these factors. Our findings also indicate that personality traits mediate (and mitigate) the association between clinical features and depressive symptoms. Personality traits have much stronger relations with depression than with clinical features, which have implications for interventions to decrease depression in RA. Overall, the results of this study suggest that the model has a good fit.
In line with hypothesis, clinical features had a total effect of 0.59 on depression, which was not only directly associated with depression but also had an indirect effect on depression in Chinese RA patients. This finding was consistent with previous studies,13,14,16 which suggested that pain, disease activity, functional disability, sleep disorders, fatigue and depression were mutually associated. RA-related clinical features can cause feelings of hopelessness self-worthlessness, guilt, as well as somatic symptoms such as loss of appetite and energy, which subsequently exacerbates depressive symptoms. However, they did not permit causal inferences because systemic inflammation might lead to depressive symptoms among RA patients, and depression also inversely increased inflammation.2 Furthermore, our study supported the mediating role of personality traits on the association between clinical features and depression in Chinese RA patients, which was similar with the result of study conducted in Portugal, indicating that there was strong association between personality and depression in RA.23 The relationship between personality and depression is well established in the literature, suggesting that depression is associated with traits such as emotional stability, extraversion or conscientiousness.19,47 In particular, we found that personality traits had much stronger relations with depressive symptoms than with clinical features, further supporting the importance of personality in the development of depression. What’s more, our study suggested that the standardized load of emotional stability was as high as 0.82, indicating that it is the most important traits affecting depression. As noted by Jeronimus and colleagues48 in their meta-analysis of 59 prospective longitudinal studies on 443,313 participants, the relationship between neuroticism (emotional stability) and mental disorders is particularly in line with the vulnerability model. It is thought that depression emerges when neuroticism exceeds the threshold that varies from person to person.49 RA is a chronic disease with poor mental health and brings a heavy burden to patients, family and society,24 which may lead to higher neuroticism in the development of depression, compared to the general population. Taken together, these data highlight that personality traits (especially emotional stability) should be taken into consideration when healthcare professionals design strategies to optimize outcomes in the management of RA. In fact, clinical features and personality explained around 77% of the depressive symptoms.
Although social support did not directly influence depression, the present study indicates the mechanism by which social support may affect personality traits and in turn influence depression among Chinese RA patients. Our results demonstrated that social support had a total effect on personality traits, being a direct effect and an indirect effect through clinical features in this path analysis. Despite the fact that genes have a great impact on personality traits, personality traits can be changed by life stressors and major shifts in social roles and relationships.22,50 For patients, RA is an important negative life event, which may change their personality traits. Social support as a buffer against stressful circumstances is assumed to improve individuals’ positive interactions that can help them adopt positive attitudes in life’s challenging events.28,31 Our results underline the salience of addressing both social support and personality traits among Chinese RA patients to reduce depressive symptoms. Prior research25–27 also suggested that low levels of social support might aggravate the impact of RA-related symptoms and emphasized the significance of considering various sources of social support and their relationships to depression. Healthcare professionals should consider the development of targeted social support programs with a view to helping reduce mental health problems amongst RA patients.
Some limitations should be considered in the interpretation of the results. First, the cross-sectional study design makes it difficult to correlate causes with effects from the findings. Our study can only provide potential hypothesis for future longitudinal and intervention study. Second, as the recruitment was carried out in a single center, our sample was not representative of the full population of RA in China, which likely limits the generalizability of our findings. Third, the self-assessment tool rather than a clinical diagnostic interview was used in our study, which might impact the accuracy of our results. However, the HDS has shown high reliability as well as sensitivity and specificity to predict the diagnosis of depression.42 Fourth, we did not include some potential influential factors such as the dose of steroid, comorbidities or socioeconomic status in the SEM analyses, despite its potential confounder effect.23
Conclusion
In summary, our study indicated that personality traits had a considerable influence upon depression, while social support seemed to have a major effect on personality traits among Chinese RA patients. Personality traits may be another realm of potential intervention towards minimizing the impacts of clinical features on patients’ depression. Positive psychology interventions such as mindfulness interventions, optimistic interventions, strength-building measures, and cognitive behavior interventions may be of paramount importance for improving the individual patient’s mental health.
Acknowledgments
The authors appreciate all participants for their cooperation in this study.
Funding
This study was supported by Grants from the Chinese National Natural Science Foundation (Grant No.71904118), Innovative research team of high level local universities in Shanghai (Grant No. SHSMU-ZDCX20210602), and the Nursing Program of Shanghai Jiao Tong University School of Medicine (Grant No. SJTUHLXK2023).
Disclosure
The authors report no conflicts of interest in this study.
References
1. Roberts MH, Erdei E. Comparative United States autoimmune disease rates for 2010–2016 by sex, geographic region, and race. Autoimmun Rev. 2020;19(1):102423. doi:10.1016/j.autrev.2019.102423
2. Nerurkar L, Siebert S, McInnes IB, Cavanagh J. Rheumatoid arthritis and depression: an inflammatory perspective. Lancet Psychiatry. 2019;6(2):164–173. doi:10.1016/s2215-0366(18)30255-4
3. Matcham F, Rayner L, Steer S, Hotopf M. The prevalence of depression in rheumatoid arthritis: a systematic review and meta-analysis. Rheumatology. 2013;52(12):2136–2148. doi:10.1093/rheumatology/ket169
4. Fu X, Li ZJ, Yang CJ, et al. The prevalence of depression in rheumatoid arthritis in China: a systematic review. Oncotarget. 2017;8(32):53623–53630. doi:10.18632/oncotarget.17323
5. Michelsen B, Kristianslund EK, Sexton J, et al. Do depression and anxiety reduce the likelihood of remission in rheumatoid arthritis and psoriatic arthritis? Data from the prospective multicentre NOR-DMARD study. Ann Rheum Dis. 2017;76(11):1906–1910. doi:10.1136/annrheumdis-2017-211284
6. Zhang L, Cai P, Zhu W. Depression has an impact on disease activity and health-related quality of life in rheumatoid arthritis: a systematic review and meta-analysis. Int J Rheum Dis. 2020;23(3):285–293. doi:10.1111/1756-185x.13774
7. Silva CFR, Duarte C, Ferreira RJO, Santos E, Da silva JAP. Depression, disability and sleep disturbance are the main explanatory factors of fatigue in rheumatoid arthritis: a path analysis model. Clin Exp Rheumatol. 2020;38(2):314–321. doi:10.55563/clinexprheumatol/hkhbad
8. Fakra E, Marotte H. Rheumatoid arthritis and depression. Joint Bone Spine. 2021;88(5):105200. doi:10.1016/j.jbspin.2021.105200
9. Ang DC, Choi H, Kroenke K, Wolfe F. Comorbid depression is an independent risk factor for mortality in patients with rheumatoid arthritis. J Rheumatol. 2005;32(6):1013–1019.
10. Uda M, Hashimoto M, Uozumi R, et al. Factors associated with anxiety and depression in rheumatoid arthritis patients: a cross-sectional study. Adv Rheumatol. 2021;61(1):65. doi:10.1186/s42358-021-00223-2
11. Soósová MS, Macejová Ž, Zamboriová M, Dimunová L. Anxiety and depression in Slovak patients with rheumatoid arthritis. J Ment Health. 2017;26(1):21–27. doi:10.1080/09638237.2016.1244719
12. Li YC, Chou YC, Chen HC, Lu CC, Chang DM. Interleukin-6 and interleukin-17 are related to depression in patients with rheumatoid arthritis. Int J Rheum Dis. 2019;22(6):980–985. doi:10.1111/1756-185x.13529
13. Fragoulis GE, Cavanagh J, Tindell A, et al. Depression and anxiety in an early rheumatoid arthritis inception cohort. associations with demographic, socioeconomic and disease features. RMD Open. 2020;6(3):e001376. doi:10.1136/rmdopen-2020-001376
14. Jamshidi AR, Banihashemi AT, Paragomi P, Hasanzadeh M, Barghamdi M, Ghoroghi S. Anxiety and depression in rheumatoid arthritis: an epidemiologic survey and investigation of clinical correlates in Iranian population. Rheumatol Int. 2016;36(8):1119–1125. doi:10.1007/s00296-016-3493-4
15. Ng KJ, Huang KY, Tung CH, et al. Risk factors, including different biologics, associated with depression and anxiety in patients with rheumatoid arthritis: a cross-sectional observational study. Clin Rheumatol. 2020;39(3):737–746. doi:10.1007/s10067-019-04820-x
16. Hughes M, Chalk A, Sharma P, Dahiya S, Galloway J. A cross-sectional study of sleep and depression in a rheumatoid arthritis population. Clin Rheumatol. 2021;40(4):1299–1305. doi:10.1007/s10067-020-05414-8
17. Choi Y, Choi SH, Yun JY, et al. The relationship between levels of self-esteem and the development of depression in young adults with mild depressive symptoms. Medicine. 2019;98(42):e17518. doi:10.1097/md.0000000000017518
18. Coyne JC, Whiffen VE. Issues in personality as diathesis for depression: the case of sociotropy-dependency and autonomy-self-criticism. Psychol Bull. 1995;118(3):358–378. doi:10.1037/0033-2909.118.3.358
19. Valerio MP, Blasco B, Tagni F, Szmulewicz AG, Martino DJ. Personality disturbances in melancholic and nonmelancholic unipolar major depression: a systematic review and meta-analysis. J Nerv Ment Dis. 2020;208(10):810–817. doi:10.1097/nmd.0000000000001212
20. Adams P, Abela JR, Auerbach R, Skitch S. Self-criticism, dependency, and stress reactivity: an experience sampling approach to testing Blatt and Zuroff’s (1992) theory of personality predispositions to depression in high-risk youth. Pers Soc Psychol Bull. 2009;35(11):1440–1451. doi:10.1177/0146167209343811
21. Santos EJF, Duarte C, Ferreira RJO, Pinto AM, Geenen R, da Silva JAP. Determinants of happiness and quality of life in patients with rheumatoid arthritis: a structural equation modelling approach. Ann Rheum Dis. 2018;77(8):1118–1124. doi:10.1136/annrheumdis-2017-212934
22. Kendler KS, Myers J. The genetic and environmental relationship between major depression and the five-factor model of personality. Psychol Med. 2010;40(5):801–806. doi:10.1017/s0033291709991140
23. Santos EF, Duarte CM, Ferreira RO, Pinto AM, Geenen R, da Silva JP. Multifactorial explanatory model of depression in patients with rheumatoid arthritis: a structural equation approach. Clin Exp Rheumatol. 2019;37(4):641–648.
24. Roodenrijs NMT, van der Goes MC, Welsing PMJ, et al. Difficult-to-treat rheumatoid arthritis: contributing factors and burden of disease. Rheumatology. 2021;60(8):3778–3788. doi:10.1093/rheumatology/keaa860
25. Fitzpatrick R, Newman S, Archer R, Shipley M. Social support, disability and depression: a longitudinal study of rheumatoid arthritis. Soc Sci Med. 1991;33(5):605–611. doi:10.1016/0277-9536(91)90218-2
26. Doeglas DM, Suurmeijer TP, van den Heuvel WJ, et al. Functional ability, social support, and depression in rheumatoid arthritis. Qual Life Res. 2004;13(6):1053–1065. doi:10.1023/b:Qure.0000031339.04589.63
27. Nebhinani N, Mattoo SK, Wanchu A. Quality of life, social support, coping strategies, and psychiatric morbidity in patients with rheumatoid arthritis. J Neurosci Rural Pract. 2022;13(1):119–122. doi:10.1055/s-0041-1742137
28. Callaghan P, Morrissey J. Social support and health: a review. J Adv Nurs. 1993;18(2):203–210. doi:10.1046/j.1365-2648.1993.18020203.x
29. Liu Y, Meng H, Tu N, Liu D. The relationship between health literacy, social support, depression, and frailty among community-dwelling older patients with hypertension and diabetes in China. Front Public Health. 2020;8:280. doi:10.3389/fpubh.2020.00280
30. Jordan J, Thompson NJ, Dunlop-Thomas C, Lim SS, Drenkard C. Relationships among organ damage, social support, and depression in African American women with systemic lupus erythematosus. Lupus. 2019;28(2):253–260. doi:10.1177/0961203318815573
31. Gariépy G, Honkaniemi H, Quesnel-Vallée A. Social support and protection from depression: systematic review of current findings in Western countries. Br J Psychiatry. 2016;209(4):284–293. doi:10.1192/bjp.bp.115.169094
32. Noteboom A, Beekman ATF, Vogelzangs N, Penninx B. Personality and social support as predictors of first and recurrent episodes of depression. J Affect Disord. 2016;190:156–161. doi:10.1016/j.jad.2015.09.020
33. Stein CM, Morris NJ, Hall NB, Nock NL. Structural equation modeling. Methods Mol Biol. 2017;1666:557–580. doi:10.1007/978-1-4939-7274-6_28
34. de Launay D, van de Sande MG, de Hair MJ, et al. Selective involvement of ERK and JNK mitogen-activated protein kinases in early rheumatoid arthritis (1987 ACR criteria compared to 2010 ACR/EULAR criteria): a prospective study aimed at identification of diagnostic and prognostic biomarkers as well as therapeutic targets. Ann Rheum Dis. 2012;71(3):415–423. doi:10.1136/ard.2010.143529
35. van Riel PL, Renskers L. The Disease Activity Score (DAS) and the disease activity score using 28 joint counts (DAS28) in the management of rheumatoid arthritis. Clin Exp Rheumatol. 2016;34(5 Suppl 101):S40–S44.
36. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: visual analog scale for pain (VAS Pain), numeric rating scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), chronic pain grade scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and measure of intermittent and constant osteoarthritis pain (ICOAP). Arthritis Care Res. 2011;63(Suppl 11):S240–252. doi:10.1002/acr.20543
37. Fries JF. The hierarchy of quality-of-life assessment, the Health Assessment Questionnaire (HAQ), and issues mandating development of a toxicity index. Control Clin Trials. 1991;12(4 Suppl):106s–117s. doi:10.1016/s0197-2456(05)80016-9
38. Morriss RK, Wearden AJ, Mullis R. Exploring the validity of the Chalder Fatigue scale in chronic fatigue syndrome. J Psychosom Res. 1998;45(5):411–417. doi:10.1016/s0022-3999(98)00022-1
39. Backhaus J, Junghanns K, Broocks A, Riemann D, Hohagen F. Test-retest reliability and validity of the Pittsburgh sleep quality index in primary insomnia. J Psychosom Res. 2002;53(3):737–740. doi:10.1016/s0022-3999(02)00330-6
40. Lei X, Kantor J. Social support and family functioning in Chinese families of children with autism spectrum disorder. Int J Environ Res Public Health. 2021;18(7):3504. doi:10.3390/ijerph18073504
41. Chapman BP, Elliot AJ. Brief report: how short is too short? An ultra-brief measure of the big-five personality domains implicates “agreeableness” as a risk for all-cause mortality. J Health Psychol. 2019;24(11):1568–1573. doi:10.1177/1359105317720819
42. Yang Y, Ding R, Hu D, Zhang F, Sheng L. Reliability and validity of a Chinese version of the Hads for screening depression and anxiety in psycho-cardiological outpatients. Compr Psychiatry. 2014;55(1):215–220. doi:10.1016/j.comppsych.2013.08.012
43. McDonald RP, Ho MH. Principles and practice in reporting structural equation analyses. Psychol Methods. 2002;7(1):64–82. doi:10.1037/1082-989x.7.1.64
44. Enders CK. Applying the bollen-stine bootstrap for goodness-of-fit measures to structural equation models with missing data. Multivariate Behav Res. 2002;37(3):359–377. doi:10.1207/s15327906mbr3703_3
45. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. 2008;40(3):879–891. doi:10.3758/brm.40.3.879
46. Lt H, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling. 1999;6(1):1–55. doi:10.1080/10705519909540118
47. Forestell CA, Nezlek JB. Vegetarianism, depression, and the five factor model of personality. Ecol Food Nutr. 2018;57(3):246–259. doi:10.1080/03670244.2018.1455675
48. Jeronimus BF, Kotov R, Riese H, Ormel J. Neuroticism’s prospective association with mental disorders halves after adjustment for baseline symptoms and psychiatric history, but the adjusted association hardly decays with time: a meta-analysis on 59 longitudinal/prospective studies with 443 313 participants. Psychol Med. 2016;46(14):2883–2906. doi:10.1017/s0033291716001653
49. Klein DN, Kotov R, Bufferd SJ. Personality and depression: explanatory models and review of the evidence. Annu Rev Clin Psychol. 2011;7:269–295. doi:10.1146/annurev-clinpsy-032210-104540
50. Kandler C, Bleidorn W, Riemann R, Spinath FM, Thiel W, Angleitner A. Sources of cumulative continuity in personality: a longitudinal multiple-rater twin study. J Pers Soc Psychol. 2010;98(6):995–1008. doi:10.1037/a0019558
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.