")
Back to Journals » International Journal of Women's Health » Volume 15
Determinants of Child Marriage and Its Related Adverse Health Outcomes Among Married Women in Sub-Region of Serejeka, Central Region in Eritrea: A Cross-Sectional Study
Authors Mehari H, Haile F, Habtezghi S, Mulugeta Y, Abraham G, Berhe M , Abdu N
Received 15 September 2022
Accepted for publication 18 January 2023
Published 11 February 2023 Volume 2023:15 Pages 215—224
DOI https://doi.org/10.2147/IJWH.S389939
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Hanibal Mehari,1 Feven Haile,1 Sador Habtezghi,1 Yuel Mulugeta,1 Gebru Abraham,1 Michael Berhe,2 Nuru Abdu3
1School of Public Health, Asmara College of Health Sciences, Asmara, Eritrea; 2National Health Observatory, Ministry of Health, Asmara, Eritrea; 3School of Pharmacy, Asmara College of Health Sciences, Asmara, Eritrea
Correspondence: Michael Berhe, Tel +291-7496890, Email [email protected]
Background: Child marriage is a fundamental violation of human rights that can have numerous adverse effects on girls’ social, mental and physical health and wellbeing. Marriage in Eritrea relatively occurs earlier for women. This study aimed to assess the magnitude of child marriage, determinants and its related adverse health outcomes in five selected villages of the sub-region of Serejeka in Central region of Eritrea.
Methods: An analytical cross-sectional study was conducted among 200 married women aged 18 to 30 years who are residents of five selected villages of the sub-region of Serejeka between July 12 and August 20, 2018. The sampling design was stratified random sampling and data were collected using an interview-based questionnaire. Descriptive and analytical statistics including chi-square test and logistic regression were employed using SPSS (v.22).
Results: The prevalence of child marriage was found to be 42% [95% CI (35.1, 48.9)]. The maximum and minimum age at marriage were 14 and 29, respectively. No formal education/primary level (AOR = 22.08, 95% CI: 4.16, 117.24), junior educational level (AOR = 6.95, 95% CI: 3.48, 13.87) and decision on the marriage (AOR = 4.30, 95% CI: 1.03, 17.92) were the significant determinants of child marriage. Prolonged labour (OR = 2.81, 95% CI: 1. 32, 5.98), abortion (OR = 3.95, 95% CI: 1.63, 9.53), hemorrhage during birth (OR = 4.83, 95% CI: 1.68, 13.87), spousal violence (OR = 2.07, 95% CI: 1.15, 3.75), pressure/stress (OR = 4.83, 95% CI: 1.68, 13.87), termination of education (OR = 8.24, 95% CI: 4.35, 15.63) and stigma or isolation from their society (OR = 7.38, 95% CI: 3.03, 17.98) were significant adverse health outcomes associated with child marriage.
Conclusion: This study revealed that child marriage was still a common practice. It is associated with detrimental physical health, psychological well-being and socio-economic status. This mandates policy makers and program managers to focus their programs on delaying entry of children into wedlock and motherhood by providing information, education and enhancing communication with their community.
Keywords: child marriage, determinant, adverse health outcome, married women, Eritrea
Introduction
Child marriage (sometimes referred to as early marriage) is defined as a marriage occurring when one of the spouses is younger than 18 years at the time of marriage or official union.1 It is a human rights violation and so has adverse effects on the children, overwhelmingly on girls who enter into these marriages, and on their future children, creating an intergenerational cycle of disadvantage.
Child marriage occurs in practically every region of the world.1 According to the UNICEF as cited by Groot et al, rates of child marriage (typically measured as the share of women 20 to 24 years old who first married or entered into union before age 18) are highest in low-income countries.2 Besides, it is more prevalent in rural areas of the developing countries when compared to urban areas.3 Globally, more than 700 million women and girls alive today were married before their 18th birthday with seventeen percent of them live in Africa. More than 70% of girls under the age of 18 are married in Niger, Chad and Mali.4
Girls usually become child brides because their parents give them away for economic or social gain. Families are also motivated by the promise of social approval or increased social standing.5 Parents think they are upholding tradition, safeguarding the chastity of their girls, and minimizing the risk that their daughters may bear children out of wedlock.6
However, child marriage has several negative health consequences like poorer maternal and reproductive health, increased risk of HIV, other sexually transmitted infections, maternal mortality and intimate partner violence.7–9 Furthermore, early childbearing increases risks to women’s health, as maternal disorders including complications during pregnancy and child birth which are the leading cause of death among women aged 20–24 years globally and the second leading cause among adolescent girls aged 15 to 19 years.10
In Eritrea, child marriage is associated with deeply rooted traditional norm. Some parents believe that early marriage provides girls a better marriage opportunity and protection from engaging in premarital sex. Child marriage is prohibited under the constitution and by law in Eritrea. According to the Eritrean Civil Code (article 581 and 329), marriage under the age of 18 is strictly prohibited. Moreover, the Eritrean proclamation No.1/1991 specifies that any contract of marriage made below 18 years of age is banned, and that the spouses and witnesses to such marriage shall be punishable under the penal code (Article 614). Despite this legal framework, the practice of child marriage in Eritrea still exists. The Eritrean Population Health Survey (EPHS-2010) indicated that among women aged 20–24, thirteen percent were married by age 15 and forty nine percent were married by age 18.11 Moreover, early marriage is more common in rural than in urban areas. To the best of our knowledge, there was no similar published study conducted in Eritrea to address the determinants and adverse health outcomes of child marriage. Therefore, the aim of the study was to assess the prevalence of child marriage, determinants and its associated adverse health outcomes among married women in five selected villages of sub-region of Serejeka in Central region of Eritrea. The results obtained are expected to contribute in addressing the adverse health outcomes associated with child marriage and thereby minimizing it through a stronger implementation of the existing policies and regulations.
Materials and Methods
Study Design
An analytical cross-sectional study with a quantitative approach was conducted to assess the magnitude of child marriage, determinants and its related adverse health outcomes among married women. Data were collected between July 12 and August 20, 2018 for a period of 30 working days.
Study Setting
Eritrea comprises six regions namely: Maekel (Central), Anseba, Debub, Gash barka, Semenawi Keih Bahri and Debubawi Keih Bahri. Maekel (Central) region has sixteen sub-regions. Of which, thirteen are located in Asmara (the capital city of Eritrea) and are urban. While, the rest three are located outside Asmara and are rural. The study was carried out in the sub-region of serejeka, one of the three rural sub-regions located in Central region. The sub-region of serejeka has 28 villages. Of which, five selected villages (namely: Embaderho, Azen, Kuazen, Beleza and Weki) were included in the study.
Source and Study Population
Residents of the five selected villages of the sub-region of Serejeka were the source population for this study. Married women whose current age at the time of study in the range of 18–30 formed the study population. Women in the range of 18–30 years were chosen to address the current magnitude of child marriage in the study area so as to minimize the recall bias.
Sample Size Determination
Sample size was computed by using the formula:
 The total sample size (n) was calculated using the following assumptions: total number of households in five villages (N = 5921), expected proportion of women married below the age of 18 (p) and those married above the age of 18 (q) were taken as 0.5, Z statistic for 95% level of confidence (Z = 1.96), margin of error (d) of 0.07 and 5% non-response rate. Considering the above assumptions, the final sample size was found to be at least 199.
The total sample size (n) was calculated using the following assumptions: total number of households in five villages (N = 5921), expected proportion of women married below the age of 18 (p) and those married above the age of 18 (q) were taken as 0.5, Z statistic for 95% level of confidence (Z = 1.96), margin of error (d) of 0.07 and 5% non-response rate. Considering the above assumptions, the final sample size was found to be at least 199.
Sampling Design
In order to get representative samples from the five selected villages of the sub-region of Serejeka, stratified random sampling was utilized. The five villages were considered as strata, and samples were taken from each village using systematic random sampling. The computed sample size was proportionally allocated among the five villages.
Variables
The dependent variable used in this analysis, child marriage is based on the self-reported age at which the subjects got married. Women reporting marriage before the age of 18 were defined as experiencing child marriage. Moreover, the determinants of child marriage were taken as independent variable.
During the second phase of the analysis, health outcomes were taken as dependent variables in that they are potentially predicted by child marriage. Health outcomes included in the study were physical, psychological and socio-economic. Physical health outcomes examined included experience of prolonged labour, pre-term birth, abortion, still birth, hemorrhoids, hemorrhage and uterine infection.
The second set of health outcome examined relate to psychological. Psychology-related outcomes examined included experience of spousal violence, pressure or stress and termination of education.
Finally, socio-economic related health outcome examined included whether they had stigma or isolation from society, difficulty in making social interactions, husband refusal to give money and financial dependence.
Subjective health outcomes were assessed through a self-reported question with two response options (whether they experienced the health outcome mentioned or not).
Data Collection Tool and Procedure
A structured and interview-based questionnaire on review of similar published studies2,8,12–14 was used to collect information. The questionnaire was aimed at exploring information on subjects’ socio-demographic characteristics, physical and psychological health effects of child marriage and socio-economic effects as well. The investigators explained purposes of the study to the participants and those who gave consent were enrolled. Then, face-to-face interviews were done. Finally, all the obtained data were documented and no follow-ups were made.
Data Quality Control
To assure the face and content validity, the questionnaire was subjected for peer-review of selected experts in the fields of medicine, public health, nursing and epidemiology. The content validity index (CVI) was computed at item level, and all items rated as relevant were included to make the I-CVI of the final questionnaire one. The questionnaire was then modified and further subjected to a pre-test. The pre-test was conducted on 20 participants on July 2–6, 2018, to ensure comprehensibility and compatibility of the questionnaire at one randomly selected village apart from the five villages included in the study. Accordingly, some modifications were made in the final version of the questionnaire. Prior to the pre-test, a one-day orientation workshop was given to the data collectors.
Statistical Analysis
Data were double entered in Census and Survey Processing System (version 7.0) and analyzed using IBM Statistical Package for Social Sciences ® (version 22). Descriptive summaries of the socio-demographic variables were computed using mean (SD) or median (IQR) as appropriate. Furthermore, factors that were related to child marriage were identified using bivariate logistic regression. Odds ratio (OR) with 95% confidence interval was reported in all logistic regression analyses. All analyses were considered significant when p<0.05.
Ethical Approval and Consent to Participate
Ethical approval was obtained from the Ministry of Health (MOH) research ethics and protocol review committee and Asmara College of Health Sciences (ACHS) ethical clearance committee. Besides, permission was obtained beforehand from the administrators of the villages. The subjects of the study were informed on the aim and objectives of the study and written informed consents were obtained from all the participants prior to data collection. All the information gathered will be held confidential and for the purpose of this study only. This study conforms to the principles outlined in the Declaration of Helsinki.
Results
Socio-demographic and Background Characterstics
A total of 200 married women with a median age of 26 (IQR: 5) were enrolled in the study. One hundred thirteen (56.5%) respondents had achieved secondary and higher educational level. All the respondents were Christians and of Tigrigna ethnicity. The prevalence of child marriage was found to be 42% [95% CI (35.1, 48.9)]. The maximum and minimum age at marriage were 14 and 29, respectively. About 33% of the respondents had two pregnancies. Moreover, 38.5% of them had three or more children (Table 1).
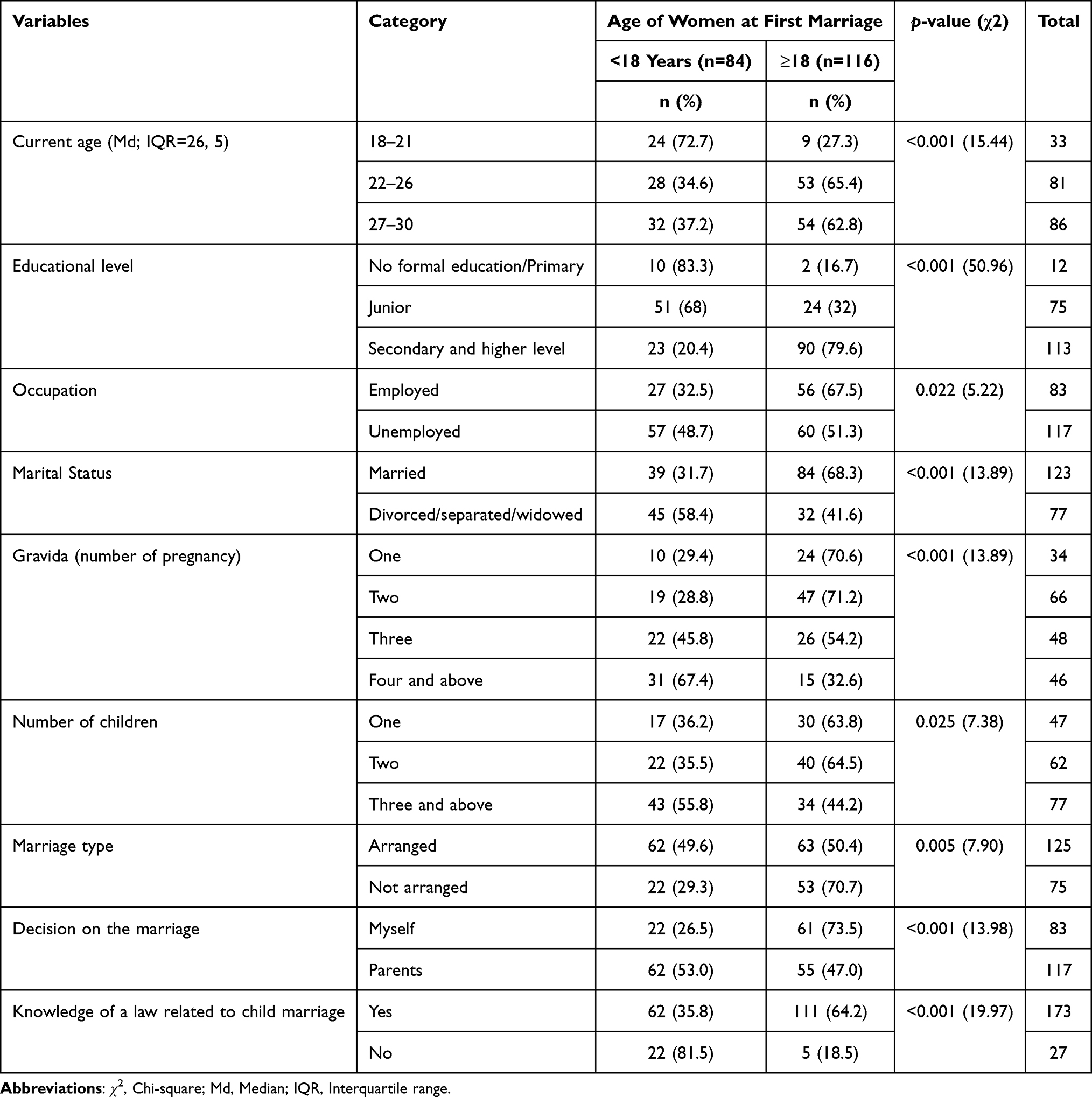 |
Table 1 Socio-Demographics and Other Background Characteristics of the Respondents (N = 200) |
Determinants of Child Marriage
No formal education/primary level (AOR = 22.08, 95% CI: 4.16, 117.24), junior educational level (AOR = 6.95, 95% CI: 3.48, 13.87) and decision on the marriage (AOR = 4.30, 95% CI: 1.03, 17.92) were the significant determinants of child marriage (Table 2).
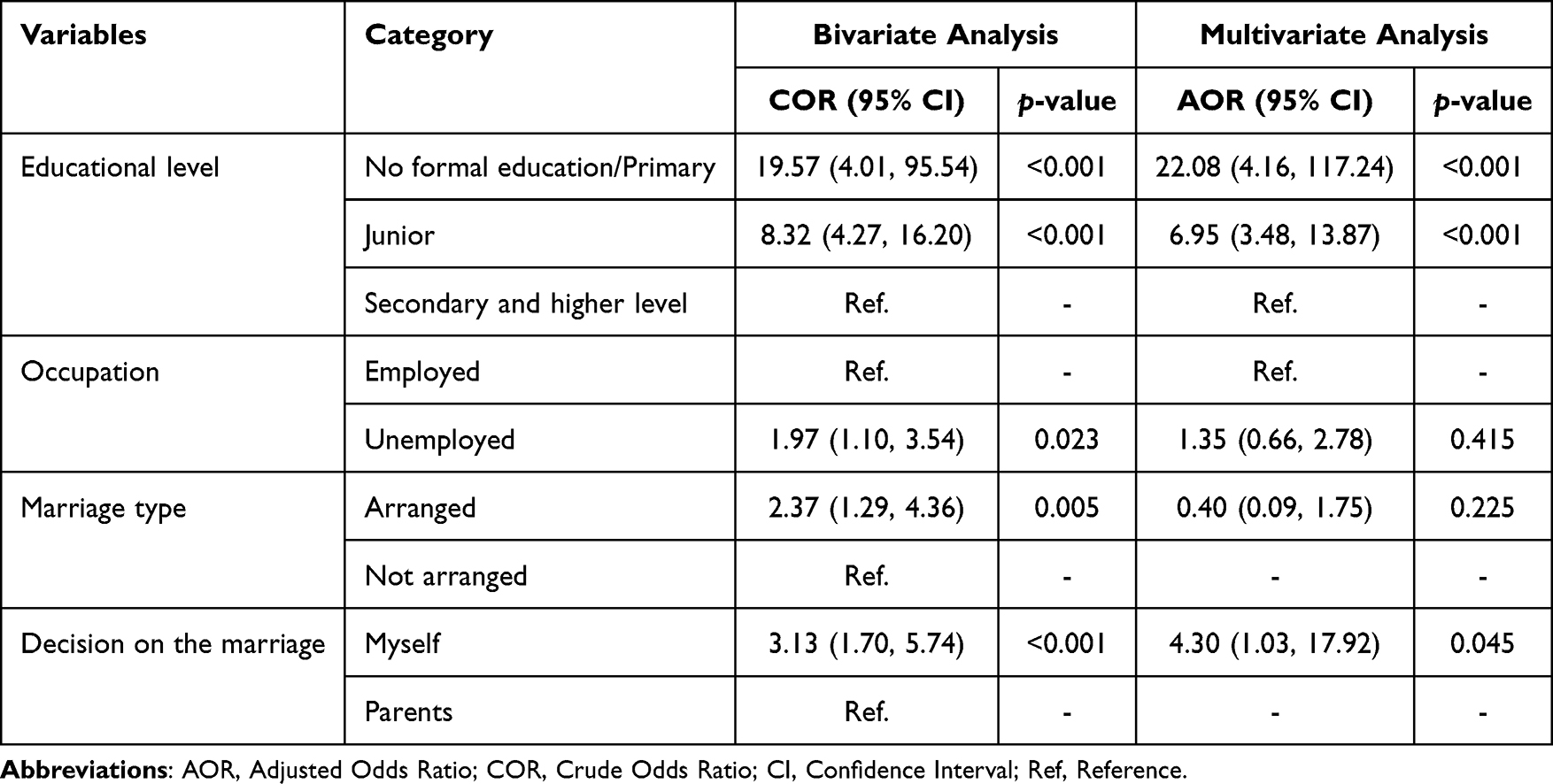 |
Table 2 Determinants of Child Marriage with Socio-Demographic and Other Background Characteristics |
Women with no formal education or primary level were twenty two times more likely to be married below the age of 18 than those women with higher level of education (AOR = 22.08, 95% CI: 4.16, 117.24). Similarly, women with junior educational level were approximately seven times more likely to be married below the age of 18 than those women with higher level of education (AOR = 6.95, 95% CI: 3.48, 13.87). Regarding decision on the marriage, women who decided by themselves were four times more likely to be married early than those women who did not decided by themselves (AOR = 4.30, 95% CI: 1.03, 17.92).
Adverse Health Outcomes Associated with Child Marriage
Physical and Psychological Adverse Health Outcomes Associated with Child Marriage
Prolonged labour (OR = 2.81, 95% CI: 1. 32, 5.98), abortion (OR = 3.95, 95% CI: 1.63, 9.53), hemorrhage during birth (OR = 4.83, 95% CI: 1.68, 13.87), spousal violence (OR = 2.07, 95% CI: 1.15, 3.75), pressure/stress (OR = 4.83, 95% CI: 1.68, 13.87) and termination of education (OR = 8.24, 95% CI: 4.35, 15.63) were significant physical and psychological health outcomes associated with child marriage (Table 3).
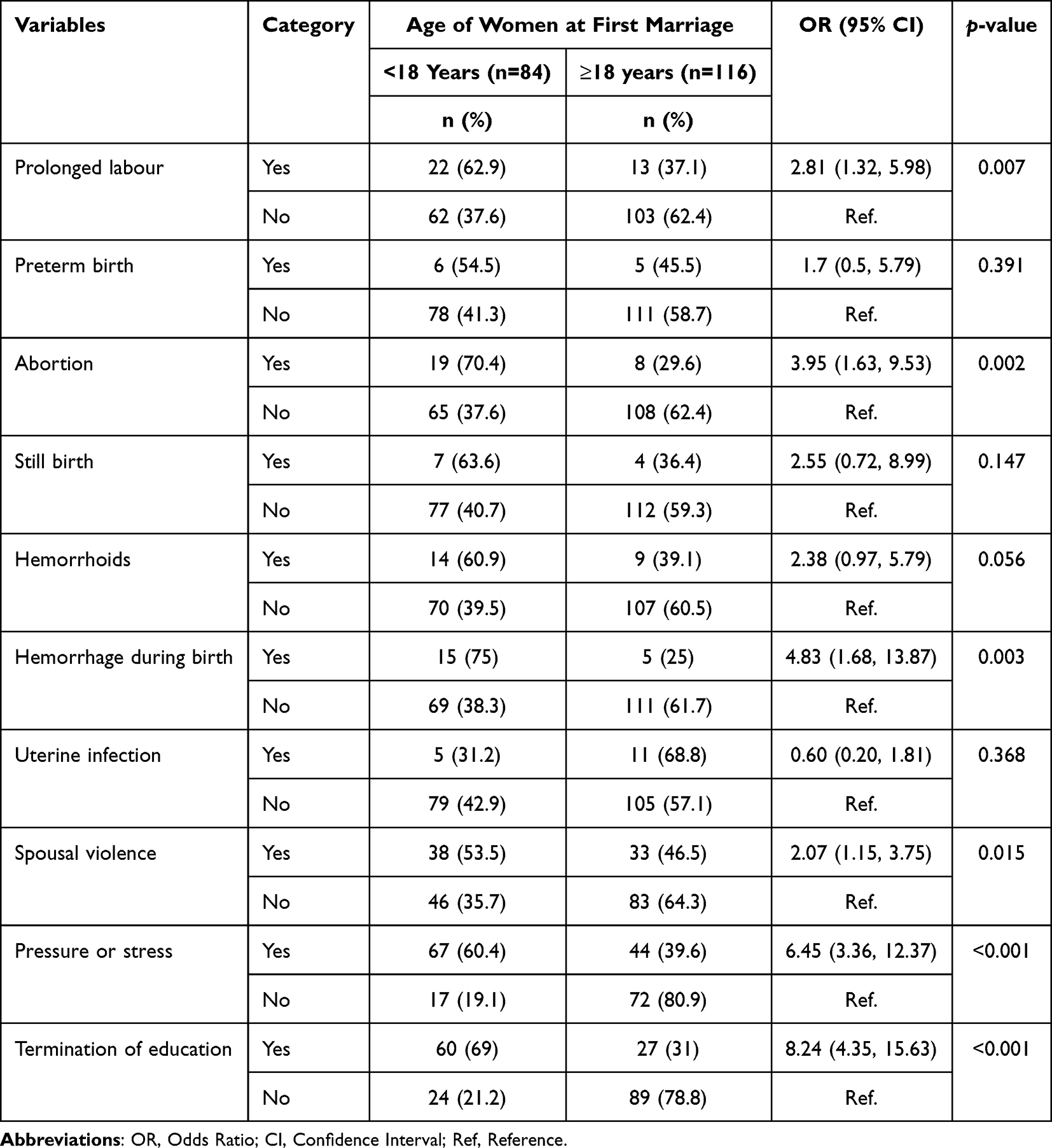 |
Table 3 Physical and Psychological Adverse Health Outcomes Associated with Child Marriage |
Respondents who were married under the age of 18 were approximately three times more likely to have prolonged labour than those who were married above the age of 18 (OR = 2.81, 95% CI: 1.32, 5.98). Likewise, respondents who married early were approximately four times more likely to have abortion (OR = 3.95, 95% CI: 1.63, 9.53). Similarly, they were approximately five times more likely to experience hemorrhage during birth (OR = 4.83, 95% CI: 1.68, 13.87) than those who married above the age of 18.
Women who married early were two times more likely to experience spousal violence than those who married after the age of 18 (OR = 2.07, 95% CI: 1.15, 3.75). Moreover, they were approximately seven times to experience pressure or stress (OR = 4.83, 95% CI: 1.68, 13.87) and eight times to terminate their education (OR = 8.24, 95% CI: 4.35, 15.63) than those who married above the age of 18.
Socio-Economic Adverse Health Outcomes Associated with Child Marriage
Stigma or isolation from their society (OR = 7.38, 95% CI: 3.03, 17.98) was the only socio-economic health outcome significantly associated with child marriage (Table 4). Women who were married early were seven times more likely to experience stigma or isolation than those who were married late (OR = 7.38, 95% CI: 3.03, 17.98).
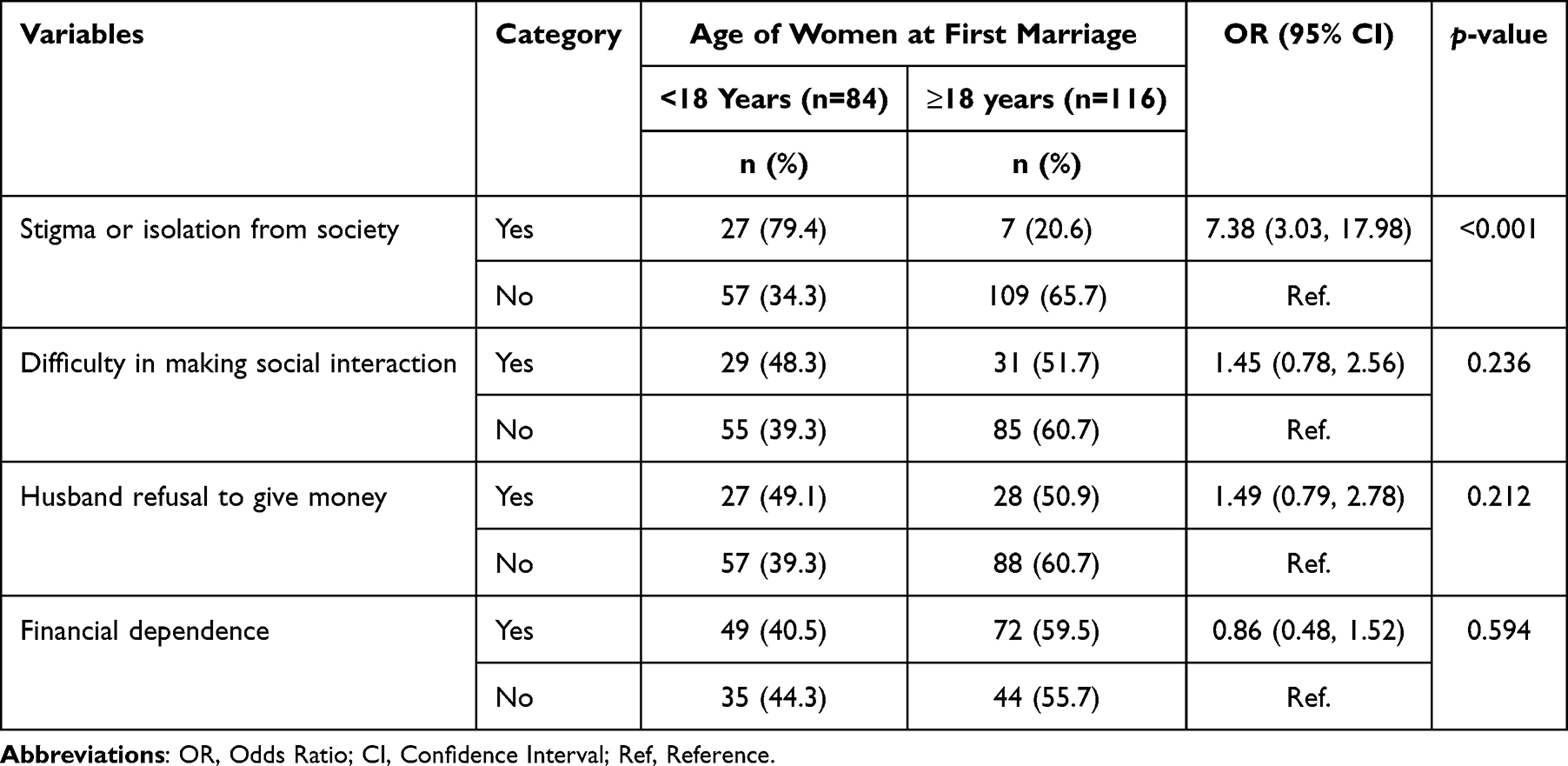 |
Table 4 Socio-Economic Health Outcomes Associated with Child Marriage |
Discussion
In the current study, the prevalence of child marriage was 42% [95% CI (35.1, 48.9)]. This finding was comparable with findings of similar studies conducted in Cameroon (38.4%)3 and Uganda (40%).15 It was however lower than those reported in Ethiopia (47%)16 and India (63%).9 This finding was higher than studies conducted in Kenya (26%)17 and Gambia (36%).18 The difference in prevalence of child marriage might be due to differences in study design, study setting, data sources used and the slight age difference among the subjects. Furthermore, it might be explained by socio-economic and cultural differences across different countries.
No formal education/primary level, junior educational level and decision on the marriage were the significant determinants of child marriage. This result was similar with studies conducted in West Bengal,19 Indonesia20 and Ethiopia21 when it comes to educational level. Educational accomplishment increases knowledge and awareness about reproductive health including suggested age of marriage and the adverse health outcomes of child marriage, whereas there may be poor information and knowledge about child marriage and its related problems among girls with lower educational level.22 In Eritrea, guided by “Education for all policy” and “social justice”, education is provided at a highly nominal cost through public schools. This mandates policy makers and program managers to provide awareness-raising programs targeting parents, religious and traditional leaders so as to understand the importance of education on decreasing early marriage.
Concerning decision on the marriage, women who decided to marry early by themselves were four times more likely to be married early than those women who did not decided by themselves. This might be due to the fact that the girls’ noticed marriage as a way to realize freedom and social character as a crucial measure of transition to adulthood.23 Furthermore, the girls’ might believe that marriage would bring them reverence, harmony, love, and autonomy in decision-making in their future life.
Prolonged labour, abortion, post-partum hemorrhage, spousal violence, pressure or stress, termination of education and stigma or isolation from society were significant adverse health outcomes of child marriage. This result was consistent with some studies elsewhere.7,9,13,14,24,25 This reflects that child brides experience numerous adverse health effects. They are more likely to have pregnancy and delivery-related complication. In addition, they also suffer from social isolation7,24,25 and are usually forced to terminate their education early and are unable to access schooling development programs.26 The school dropout halts the girls’ ability to interact with peers of the same age and socialize outside of the family unit.27
Prolonged labour occurs when the baby does not exist the pelvis during delivery due to physical blockage.28,29 This resulted in complications for the baby and the mother. The baby does not get the necessary oxygen which may lead to death. Moreover, the chances of the mother being infected, having uterine rupture and post-partum hemorrhage increases.28,30 The possible explanation for the prolonged labour could be due to small pelvis of the girls during delivery.
In the current study, women who married early were two times more likely to experience spousal violence than those who married after the age of 18. This finding was similar to studies conducted in Nepal,31 India,32 Pakistan33 and Bangladesh.34 The possible explanation for the physical violence may be due to variation in age and psychological maturity between spouses.
Taking the adverse health outcomes of child marriage into consideration, policy makers and program managers should strictly implement the existing laws and policies that prohibit child marriage. Moreover, the negative health outcomes of child marriage and the importance of education in the reduction of early marriage and psychological maturity should be enlightened to the public via an appropriate promotional method.
Strengths and Limitations of the Study
This is the first study in Eritrea to assess the magnitude of child marriage, its determinants and related adverse health outcomes among women inhabitants of sub-region of Serejeka. The study had a high response rate (100%) and applied a rigorous data quality and management approaches.
Due to the cross-sectional nature of the study design, this study did not confirm the cause-effect relationship. Besides, the findings reported here are specific to the five villages of the sub-region of Serejeka. Thus, our findings are not necessarily generalizable to the sub-region, the region and the country as a whole. So it is recommended to conduct further research to determine the magnitude and problems of child marriage in the country.
Conclusion
The current study revealed that child marriage was a common practice and associated with adverse physical, psychological and socio-economic health outcomes. This clearly showed that child marriage is an important public health concern that needs a greater attention in protecting and supporting the young girls from being victims of child marriage’s negative health outcomes.
To minimize the occurrence of child marriage a change of customs and beliefs towards child marriage through programmed education of parents, religious leaders and the public as a whole should be enhanced. Besides, strong implementation of the present laws and policies regarding child marriage should be promoted.
Abbreviations
ACHS, Asmara College of Health Sciences; AOR, Adjusted Odds Ratio; CI, Confidence Interval; CVI, Content Validity Index; EPHS, Eritrean Population and Health Survey; HIV, Human Immunodeficiency Virus; IQR, Interquartile Range; MOH, Ministry of Health; OR, Odds Ratio; SD, Standard Deviation; SPSS, Statistical Package for Social Sciences; UNICEF, United Nations Children’s Fund.
Data Sharing Statement
The data used in this study are available from the corresponding author and can be accessed upon reasonable request.
Ethical Approval and Consent to Participate
Ethical approval was obtained from the Ministry of Health (MOH) research ethics and protocol review committee and Asmara College of Health Sciences (ACHS) ethical clearance committee. Besides, permission was obtained beforehand from the administrators of the villages. The subjects of the study were informed on the aim and objectives of the study and written informed consents were obtained from all the participants prior to data collection. All the information gathered will be held confidential and for the purpose of this study only. This study conforms to the principles outlined in the Declaration of Helsinki.
Acknowledgment
We would like to forward our sincere gratitude to Dr. Zerabruk Tesfamariam and Eyasu Habte for their invaluable comments on the manuscript. We owe our thanks to administrators of the selected villages of sub-region of Serejeka who have warmly accepted and approved the study to be conducted in their villages. We would also like to thank all participants of this study for being cooperative in the process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There was no source of funding for the study or manuscript preparation.
Disclosure
The authors declare that they have no conflicts of interest in relation to this work.
References
1. Brides GN. Girls not brides; 2017. Available from: http://girlsnotbrides.org/child-marriage.
2. Richard de Groot MYK, Palermo T. Child marriage and associated outcomes in northern Ghana: a cross-sectional study. BMC Public Health. 2018;18(285):1–12.
3. UNICEF. 2015 based on the demographic health survey for republique du cameroun published in 2011. Available from: https://data.unicef.org/topic/child-protection/child-marriage/.
4. International center for research on women analysis of demographic and health survey. Available from: http://www.icrw.org/child-marriage-facts-and-figures.
5. United Nations. “Secretary general’s report on the girl child” (A/66/257, 2011). Available from: http://www.un.org/ga/search/view_doc.asp?symbol=A%2F66%2F257&Submit=Search&Lang=E.
6. A note on child marriage. World day of prayer and action for children secretariat New York July 2012. Available from: http://www.unicef.org/policyanalysis/files/Note_on_Child_Marriage.pdf.
7. Nour NM. Child marriage: a silent health and human rights issue. Rev Obstet Gynecol. 2009;2(1):51.
8. Kidman R. Child marriage and intimate partner violence: a comparative study of 34 countries. Int J Epidemiol. 2016;46(2):662–675.
9. Santhya KG, Ram U, Acharya R, Jejeebhoy SJ, Ram F, Singh A. Associations between early marriage and young women’s marital and reproductive health outcomes: evidence from India. Int Perspect Sex Reprod Health. 2010;36(03):132–139. doi:10.1363/3613210
10. Mokdad AH, Forouzanfar MH, Daoud F, et al. Global burden of diseases, injuries, and risk factors for young people’s health during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2016;387(10036):2383–2401. doi:10.1016/S0140-6736(16)00648-6
11. Eritrean population health survey; 2010. Available from: https://www.afro.who.int/sites/default/files/2017-05/ephs2010_final_report_v4.pdf.
12. Mikyas Abera AN, Tefera Y, Gelagay AA. Early marriage and women’s empowerment: the case of child-brides in Amhara National Regional State, Ethiopia. BMC Int Health Hum Rights. 2020;20(30):1–16. doi:10.1186/s12914-019-0221-7
13. Sekine K, Hodgkin ME, Gammage S. Effect of child marriage on girls’ school dropout in Nepal: analysis of data from the Multiple Indicator Cluster Survey 2014. PLoS One. 2017;12(7):e0180176. doi:10.1371/journal.pone.0180176
14. Godha D, Hotchkiss DR, Gage AJ. Association between child marriage and reproductive health outcomes and service utilization: a multi-country study from South Asia. J Adolesc Health. 2013;52(5):552–558. doi:10.1016/j.jadohealth.2013.01.021
15. UNICEF. 2015 based on a 2011 DHS survey conducted in Uganda. Available from: https://dhsprogram.com/pubs/pdf/FR264/FR264.pdf.
16. Erulkar A. Early marriage, marital relations and intimate partner violence in Ethiopia. Int Perspect Sex Reprod Health. 2013;39(1):6–13. doi:10.1363/3900613
17. Kenya National Bureau of Statistics. Kenya Demographic and Health Survey 2008/2009. Available from: http://dhsprogram.com/pubs/pdf/fr229/fr229.pdf.
18. Report of the Office of the United Nations High Commissioner for Human Rights. “Preventing and eliminating early, child and forced marriages”, based on MICS data for the Gambia published in 2010; 2014.
19. Avijit Roy PC, Walker DA, McKenna C. A mixed‑method analysis of associated socio‑cultural and environmental factors of child marriage in Malda district of West Bengal. SN Soc Sci. 2022;2(22):1–19. doi:10.1007/s43545-021-00300-9
20. Lauren Rumble AP, Irdiana N, Triyana M, Minnick E. An empirical exploration of female child marriage determinants in Indonesia. BMC Public Health. 2018;18(407):1–13.
21. Abay Kassa Tekile AAW, Basha GW. Determinants of early marriage among female children in Amhara Region, Ethiopia. Afr Health Sci. 2020;20(3):1190–1195. doi:10.4314/ahs.v20i3.22
22. Addisu M, Addisu D. Determinants of early marriage among married women in Injibara town, north West Ethiopia: community-based crosssectional study. BMC Women’s Health. 2019;19(1):134. doi:10.1186/s12905-019-0832-0
23. Simin Montazeri MG, Mohammadi N, Rad JA, Ardabili HE, Eftekhar Ardabili H. Determinants of early marriage from married girls’ perspectives in Iranian setting: a qualitative study. J Environ Public Health. 2016;2016:1–8. doi:10.1155/2016/8615929
24. Le Strat Y, Dubertret C, Le Foll B. Child marriage in the United States and its association with mental health in women. Pediatrics. 2011;128(3):524–530. doi:10.1542/peds.2011-0961
25. Parsons J, Edmeades J, Kes A, Petroni S, Sexton M, Wodon Q. Economic impacts of child marriage: a review of the literature. Rev Faith Int Aff. 2015;13(3):12–22. doi:10.1080/15570274.2015.1075757
26. Vogelstein RB. Ending Child Marriage: How Elevating the Status of Girls Advances US Foreign Policy Objectives. Council on Foreign Relations; 2013.
27. UNICEF O. Hidden in Plain Sight: A Statistical Analysis of Violence Against Children. New York: UNICEF; 2014.
28. Okonkwo UT, Nkoli.N E. The relationship between early marriage/childbearing and prolonged labour in Enugu State: a perception study. Int J Innov Res Adv Stud. 2017;4(4):156–160.
29. World Health Organization. Making Pregnancy Safer: Adolescent Pregnancy. Geneva: World Health Organization; 2011.
30. Neilson J, Lavender T, Quenby S, Wray S. Obstructed labour. Br Med Bull. 2003;67:191–204. doi:10.1093/bmb/ldg018
31. Adhikari R. Child marriage and physical violence: results from a nationally representative study in Nepal. J Health Promot. 2018;6:49–59. doi:10.3126/jhp.v6i0.21804
32. Speizer IS, Pearson E. Association between early marriage and intimate partner violence in India: a focus on youth from Bihar and Rajasthan. J Interpers Violence. 2011;26:1963–1981. doi:10.1177/0886260510372947
33. Nasrullah M, Zakar R, Zakar MZ. Child marriage and its associations with controlling behaviors and spousal violence against adolescent and young women in Pakistan. J Adolesc Health. 2014;55:804–809. doi:10.1016/j.jadohealth.2014.06.013
34. Rahman M, Hoque A, Mostofa G, Makinoda S. Association between adolescent marriage and intimate partner violence: a study of young adult women in Bangladesh. Asia Pac J Public Health. 2014;26:160–168. doi:10.1177/1010539511423301
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.