")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Determinants of Anemia Among Pregnant Women Attending Antenatal Care Clinic at Public Health Facilities in Kacha Birra District, Southern Ethiopia
Authors Teshome MS, Meskel DH, Wondafrash B
Received 4 May 2020
Accepted for publication 5 August 2020
Published 24 September 2020 Volume 2020:13 Pages 1007—1015
DOI https://doi.org/10.2147/JMDH.S259882
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Melese Sinaga Teshome,* Desalech H Meskel,* Beyene Wondafrash
Department of Nutrition and Dietetics, Faculty of Public Health, Health Institute, Jimma University, Jimma, Ethiopia
*These authors contributed equally to this work
Correspondence: Melese Sinaga Teshome Email [email protected]
Background: Anemia is accountable for 20% of maternal death globally, and it is associated with premature birth, low birth weight, and infant death. According to the WHO report of 2008, 57.1% of pregnant women were anemic in Africa. In Ethiopia, anemia among pregnant women is 62.7%. There were no data in the study area that identified the determinants of anemia.
Objective: To identify the determinants of anemia among pregnant mothers attending ANC clinic in public health facilities in Kacha Birra District, Southern Ethiopia.
Methods: An institutional-based unmatched case–control study was conducted among pregnant women attending antenatal care clinics in public health facilities in Kacha Birra District, Southern Ethiopia, from February 1/2019–May 30/2019. An aggregate of 117 cases and 227 controls were involved in the study. Data were collected using interviewer-administered questionnaires. Controls were pregnant ladies whose blood hemoglobin level was 11 g/dl and above at their first antenatal care clinic, and cases were pregnant ladies whose hemoglobin level less than 11 g/dl. Both bivariate and multivariable logistic regression models were used to isolate independent predictors of anemia.
Results: An overall of 344 respondents (117 cases and 227controls) were included in this study with a response rate of 100%. On multivariable logistic regression models, significant predictors of anemia were: rural residence [AOR= 2.9,95% CI:1.18– 5.84], previous history of heavy menstrual blood flow [AOR=2.75, 95% CI: 2.66– 28.53], age of mother [AOR=4.013, 95% CI: 1.08– 14.90], parasitic infection [AOR=6.39, 95% CI: 1.226– 33.362], food taboo (aversion) [AOR= 3.92, CI: 95% 2.08– 7.35], drinking tea/coffee instantly after meal [AOR=18.49, 95% CI:6.89– 40.64].
Conclusion: Residence, previous heavy menstrual flow, age, parasitic infection, food taboo, and tea/coffee consumption immediately after meals were significant predictors of anemia among pregnant women. So, anemia prevention and control policy should include the promotion of counseling on the consumption of diversified and iron-enriched foods during pregnancy, prevention of parasitic infection as well as mass deworming, awareness creation on cultural norms that makes food aversion during pregnancy.
Keywords: determinants, anemia, pregnant women, case, control
Introduction
Anemia during pregnancy is a condition in which the hemoglobin content of the blood is lower than normal for a person´s, gender, environment, and age, resulting in the decreased oxygen-carrying capacity of the blood.1
Anemia is experiential as a pointer of both poor nutrition and poor health. It harms health and well-being in women and raises the risk of maternal and neonatal adverse effects. During pregnancy, anemia is accountable for numerous problems in women.2 Anemia is a global public health problem affecting many individuals in all age groups, mainly the burden of the problem is greater among pregnant women.3 It underwrites to 20% of all maternal losses. Anemia in pregnancy also leads to low birth weight, fetal impairment, untimely births, and infant losses.3
According to the report of the World Health Organization in 2008; anemia affected 1.62 billion (24.8%) individuals worldwide.1 In developing countries on average 56% anemia is reported with a range being 35% to 100% in different areas of the world. It is more common in developing countries because of the high prevalence of parasitic infections and poor nutritional status. Africa is the greatest affected county, with the prevalence of anemia projected to be 17.2 million among pregnant ladies. This constitutes around 30% of total worldwide cases.5 World Health Organization graded anemia as the 8th prominent root of death in girls and women in developing countries. World Health Organization estimated showed that 35–75% of pregnant women in developing countries, and 18% in advanced countries are anemic.4 Anemia is the major cause of maternal mortality.7
In Ethiopia, iron deficiency anemia is the commonest problem affecting children, women of reproductive age and pregnant women.9 The Federal Ministry of Health established national nutrition package to improve the micronutrient deficiency among pregnant ladies and the system for supplying inclusive and routine nutritional assessment and intervention as including de-worming, folic acid and iron supplementation during pregnancy.8 However, looking into regional differences, the highest prevalence anemia (60%) was observed in Somali region followed by that of Afar Regions (45%), while the lowest prevalence (16.3%) was reported to be in Addis Ababa.10
A prevalence of 40.5% in the general population and 47.2% in the children were stated from the southwest part of Ethiopia.6 A prevalence of as high as 57% was also been described in pregnant women in Jimma.4 However, there is no local document on the determinants of anemia to avert its consequences. Therefore, this study set out to identify determinants of anemia among pregnant women ANC clinics in public health facilities of Kacha Birra District.
Methods
Study Area and Period
This study was conducted in Kacha Birra District located 327 km from Addis Ababa and 144km southwest of the regional capital Hawasa at latitude and longitude of 7°12′N and 37°46′E with an elevation of 1875 meters above sea level. It has 23-kebeles (2 urban and 21 Rural) with a total population of 127,000 population, with 64,770 women and 62, 230, men. The District has four health centers namely Buge Health Center, Hobichaka Health Center, Mesafe Heath Center, Kacha Health Center, and one Primary Hospital. The Hospital and all the health centers in the District give ANC services.10
An unmatched case-control study was employed from February 1, 2019 –May 30, 2019. All pregnant women who were attending ANC in public health facilities in Kacha Birra District during the study were considered as a source population. The study population was all randomly selected pregnant women who were receiving their ANC in the health facilities during the study period and included in the sample. Inclusion criteria: All pregnant women who attended ANC in health facilities and who are residents for a minimum of 6 months in the District were involved in the study. Exclusion criteria: pregnant women who were seriously ill and those who came for the 2nd and 3rd visits were excluded.
Sample Size and Sampling Procedure
The sample size was calculated using the double population proportion formula using Epi Info version 7.02 statistical software with the assumption of 95% confidence level (Zα/2=1.96), 90% power (Zβ= 1.28), control to case ratio of 2:1 (r=2), and an odds ratio of 2 and proportion of cases having a chronic disease of 17% and controls having chronic diseases of 5.76%.15 Considering 5% non-response rate, the maximum sample size was 344 (117 cases and 227 controls).
All health facilities found in the district were included in the study. The number of study participants was allocated to each health facility proportional to their customer size attended per year. Finally, the study participants were selected from each health facility using a systematic random sampling technique with a sampling interval of four (k=4).
Proportional allocation of the sample to the size of the population of women who were receiving their ANC in those health facilities.
Measurements
The data were collected by face to face interview using pretested and interviewer-administered English version questionnaire that was translated into Amharic. The questionnaire was back-translated into English by another person. The standardized tool for measurement of wealth index was adopted from Ethiopia Demographic and Health Survey 2016 (EDHS-2016) and analyzed using principal components analysis (PCA).
Blood Sample
The hemoglobin level of the mothers was measured from capillary blood by taking 1 drop of blood. The finger of the mother pierced after rubbing the fingertip with sterilized cotton (dipping in 70% alcohol) with a sterilized throwaway lancet. Automated Hemocue Hb 301, Hemocue Ab, Angelholm Sweden serial number 1,322,813,143 was used to determine the hemoglobin level, adjusted for altitude and the finding were stated in g/dL based on World Health Organization (WHO) cut off point.25,26 The altitudes of the study area were measured by using a handheld Global Positioning System (GPS); Mark: GPS 72H GARMIN. The hemoglobin levels were adjusted for altitude variations.25
Stool Examination
The fresh stool sample was collected from every study subject using a hygienic and wide-mouthed and leak-proof stool goblet. Then, the stool wet mount was equipped using saline (0.85%) and/or iodine and observed microscopically for the identification of intestinal helminths and protozoa parasites within half an hour of collection. A portion of the stool was handled with a direct microscopic method to identify intestinal parasites instantly. For the detection of helminths, larvae, eggs, and cysts of protozoan parasites and analysis was done using direct microscopy (saline smear) for determining intestinal parasite infection.
Dietary and Anthropometric Measurements
Dietary Diversity Score was calculated from a single 24 hours recall and all the liquids and the foods consumed a day before the study were categorized into 9 food groups. Consuming a food item from any of the groups was assigned a score of “1” and a score of “0” if the food was not taken. Thus, a Dietary Diversity Score of nine points was calculated by adding the values of all the food groups. After that, it was classified as low (less than or equal to three) medium (four-six) and high (seven-nine). Furthermore, nutritional status was measured by taking anthropometric body measurements of the mothers from mid-upper arm circumference taken by MUAC tape reader.
Data Processing and Analysis Procedures
The data were entered into Epi-data version 3.1 and then exported to SPSS software program version 25 for analysis. Percentages, frequencies, and summary statistics were computed to describe the study participants in relation to relevant variables.
Bivariate binary logistic regression analysis was done to select the candidate variable to final model multivariable analysis and crude odds ratios with 95% CI were obtained. Then, variables observed in the bivariate analysis with p < 0.25 were subsequently included in the final models of multivariable logistic regression to control for possible confounding effects and to assess the separate effects of each independent variable on the outcome variable.
The strength of statistical association was measured by adjusted odds ratios and 95% confidence intervals (CI). Forward stepwise LR (likely hood ratio) method was used for entering variables and The goodness of the model was tested by Hosmer Lemeshow show test` and the model was fit with P =0.289. Principal component Analyses were done for household wealth score and ranked into tertiles.
Data Quality Management
The questionnaire was translated to Amharic and back to English for consistency, a 2 days intensive training was given for data collectors, and on the spot inspection and modification was made for incomplete questionnaire by supervisor. The overall data collection process was controlled by the principal investigator. A pre-test was conducted at five percent of the total sample size in Hadaro Health Center which was not selected in a sampling procedure that was before a week of the actual data collection.
The proper functioning of laboratory reagents, instruments, and technical performance was tested using quality control samples. Standard operating procedures and manufacturers’ instructions were strictly followed starting from sample collection up to result reporting. All laboratory procedures were controlled by laboratory B.sc graduators and comparisons of hemocue machines with Cell blood counter machines were done to check proper functionality and its correlation. Hemocue with the CBC machine was checked. Comparisons of Hemocue machines with CBC (Complete blood count) machine, Sysmex analyzer (Sysmex XS-500i, made in China) were done. This was just to be self-assured on the working devices by themselves but not on technical issues behind the machines. But, to check if there were problems during the storage and transportation of Hemocue machines. The results of Pearson correlation coefficients for survey Hemocue machines with Sysmex analyzer were: 0.979, 0.987, 0.996, and 0.995. Before data analysis cleaning was done and outliers were identified and managed. Multicollinearity for independent predictors of anemia was checked.
Results
A total of 344 pregnant women with 117 cases and 227controls were enrolled in this study with a 100% response rate. The age of study subjects ranged from 15 to 38 years of age. From these above, one-fourth 180 (52.2%) were found in the age range of 25–29 (50.4%) of the fifty-nine of cases and 121 (53.3%) of the controls were found between 25 and 29 years. Concerning to maternal educational status, 32 (34.5%) cases and 92 (40.5%) controls were at the primary educational level (Table 1).
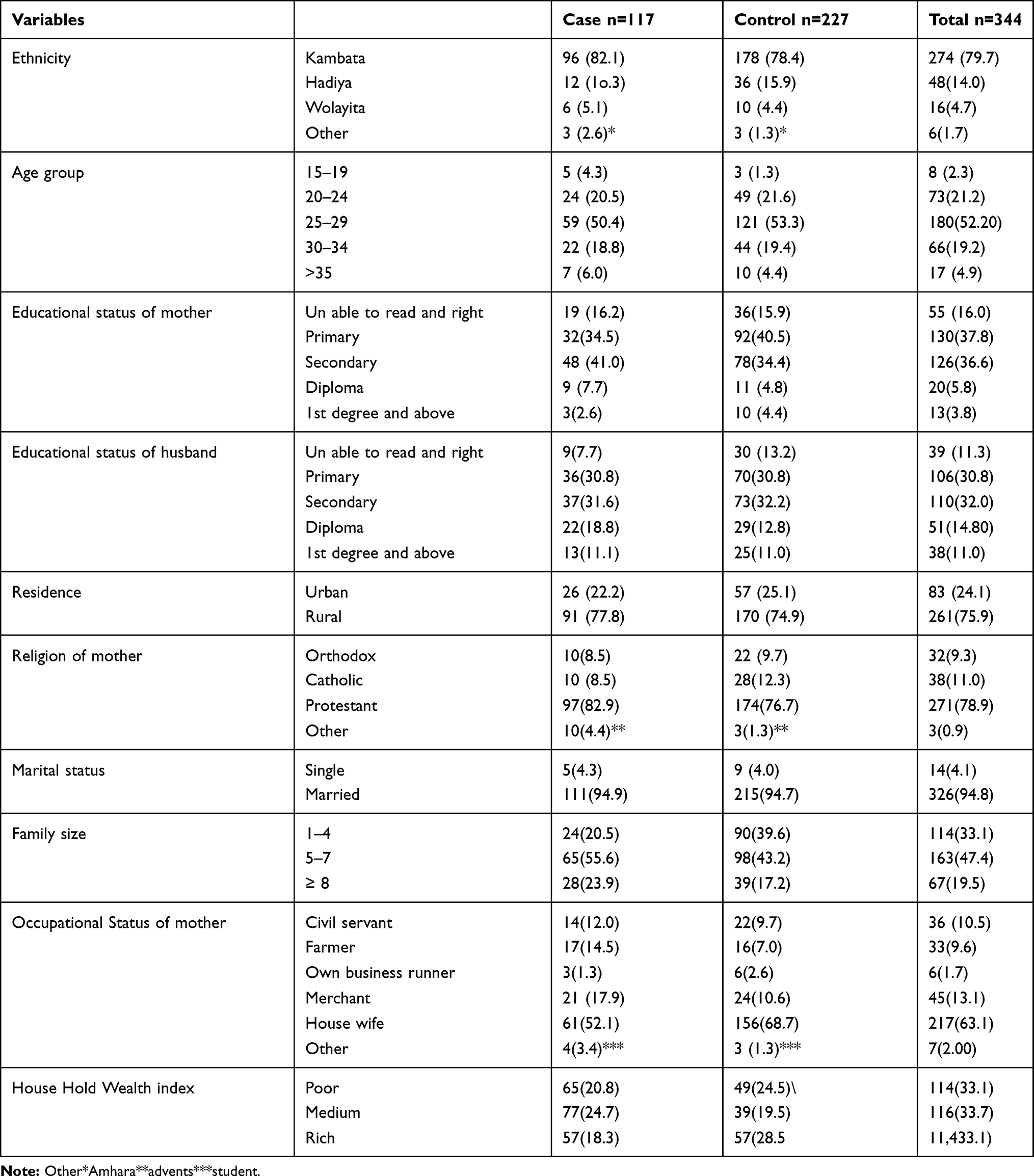 |
Table 1 Socio-Demographic and Economic Characteristics of Pregnant Mothers in Kacha Birra Woreda Health Centers February to May 2019 |
Obstetrics Characteristics of the Study Participants
Among pregnant women who were receiving ANC at health facilities, 91 (77.8%) cases and 162 (71.4%) controls had the previous history of pregnancy. Out of those who had a history of birth, nearly one-fourth of the cases, 40.2%, and 38.8 controls had a birth interval of more than 2 years. Among antenatal care attendees, 72.6% cases and 75.3% controls had history contraceptive use. More than half of the antenatal care attendees, 64.1% cases, and 21.6% of women had heavy menstrual flow before they become pregnant. Concerning gestational age, the majority of the participants, 61.5% cases and 48.5% controls were at the third trimester of their ANC booking (Table 2).
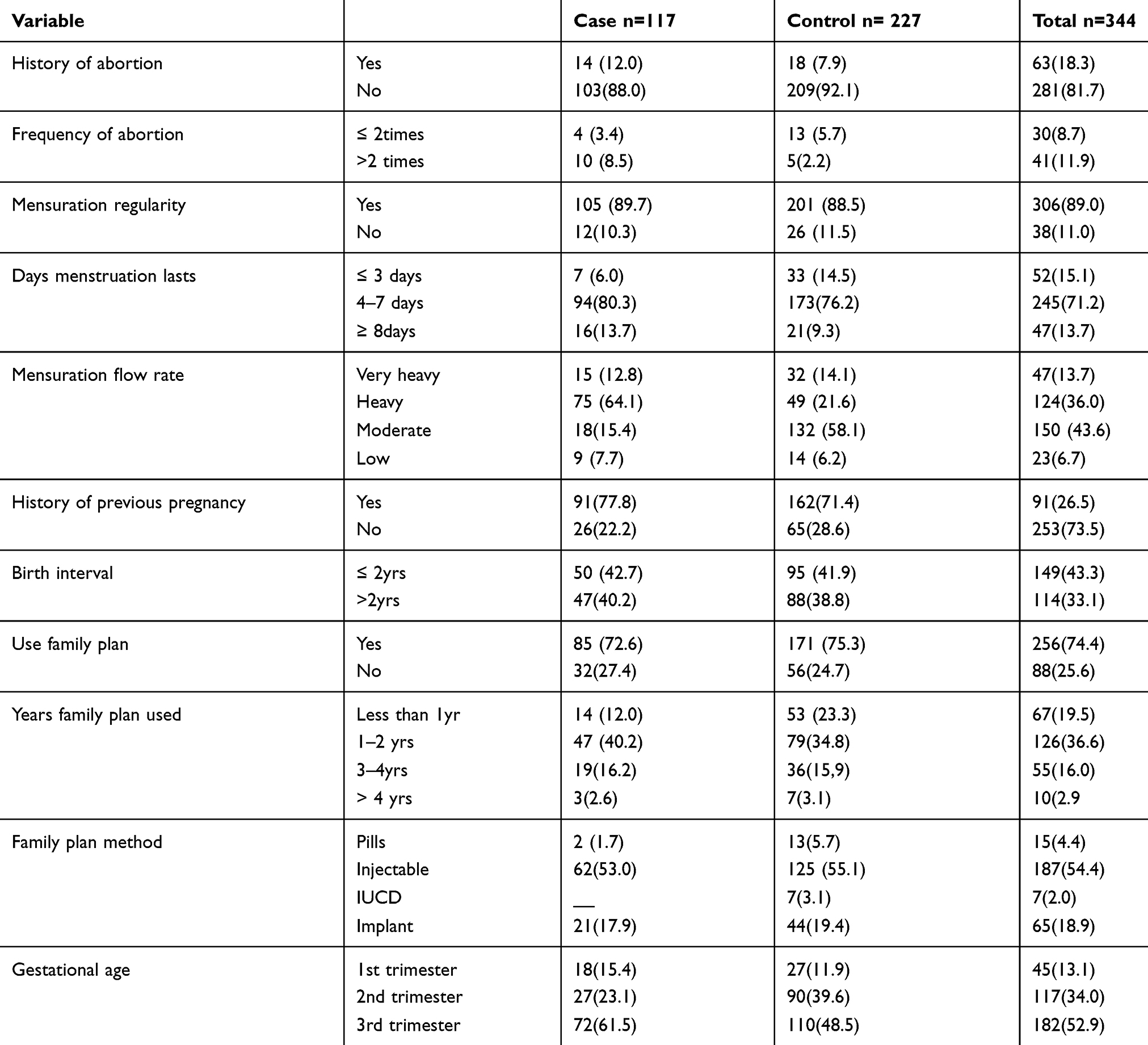 |
Table 2 Obstetrics-Related Characteristics of Pregnant Mothers in Kacha Birra Woreda Health Centers February to May 2019 |
In bivariate analysis a total of 17 variables (age of mother, residence, educational status of the mother, occupational status of the mother, family size, birth interval, water source, meal frequency, the staple food of mother, food pica, food taboo, tea/coffee, menstruation flow rate, history of abortion, history of chronic illness stool examination, gestational age, DDS, household wealth index with p-value <0.25) were chosen for multivariate analysis.
Crude odds ratio (COR) was done for each independent variable. Variables having a p-value of less than 0.25 were chosen for multivariate analysis.
Forward stepwise logistic regression was used to get adjusted odds ratio with 95% CI and finally 7 variables (age of mother, residence, menstrual blood flow rate, food taboo tea/coffee consumption, DDS, stool examination) with p-value <0.05 were significantly associated with anemia independently.
Multivariable logistic regression analysis indicated that the odds of getting anemia in pregnant women who lived in rural were nearly 3 times more likely to have anemia compared to those mothers who live in urban areas [AOR= 2.9, 95% CI: 1.18–5.84]. Pregnant mothers who had previous heavy menstrual blood flow rate were 2.7 times more likely to have anemia than those who do not have a history heavy menstrual blood flow rate [AOR=2.7, 95% CI: 2.66–28.53].
Similarly, pregnant mothers who were in the age range of 20−24 were 4 times more likely to develop anemia as compared to pregnant women’s in the age range of >35 [AOR=4.013, 95% CI: 1.08–9.0].
The odds of developing anemia among pregnant women with a parasitic infection on current pregnancy were nearly 6.4 times more likely to have a parasitic infection than those women who do not have a parasitic infection on current pregnancy [AOR=6.39, 95% CI: 1.2–33.3].
In this study, food taboo was found to be a significant predictor of anemia. Those pregnant women who were experiencing food restriction during pregnancy due to cultural beliefs were 3.9 times more likely to develop anemia as compared to those who do not food restriction during pregnancy [AOR= 3.9, 95% CI: 2.0–7.3].
The probabilities of developing anemia among pregnant women’s who were drinking tea/coffee instantly after food were 3.6 times more likely to develop anemia as compared to than those mothers who did not drink tea/coffee [AOR=3.6, 95% CI: 1.72–7.42] (Table 3).
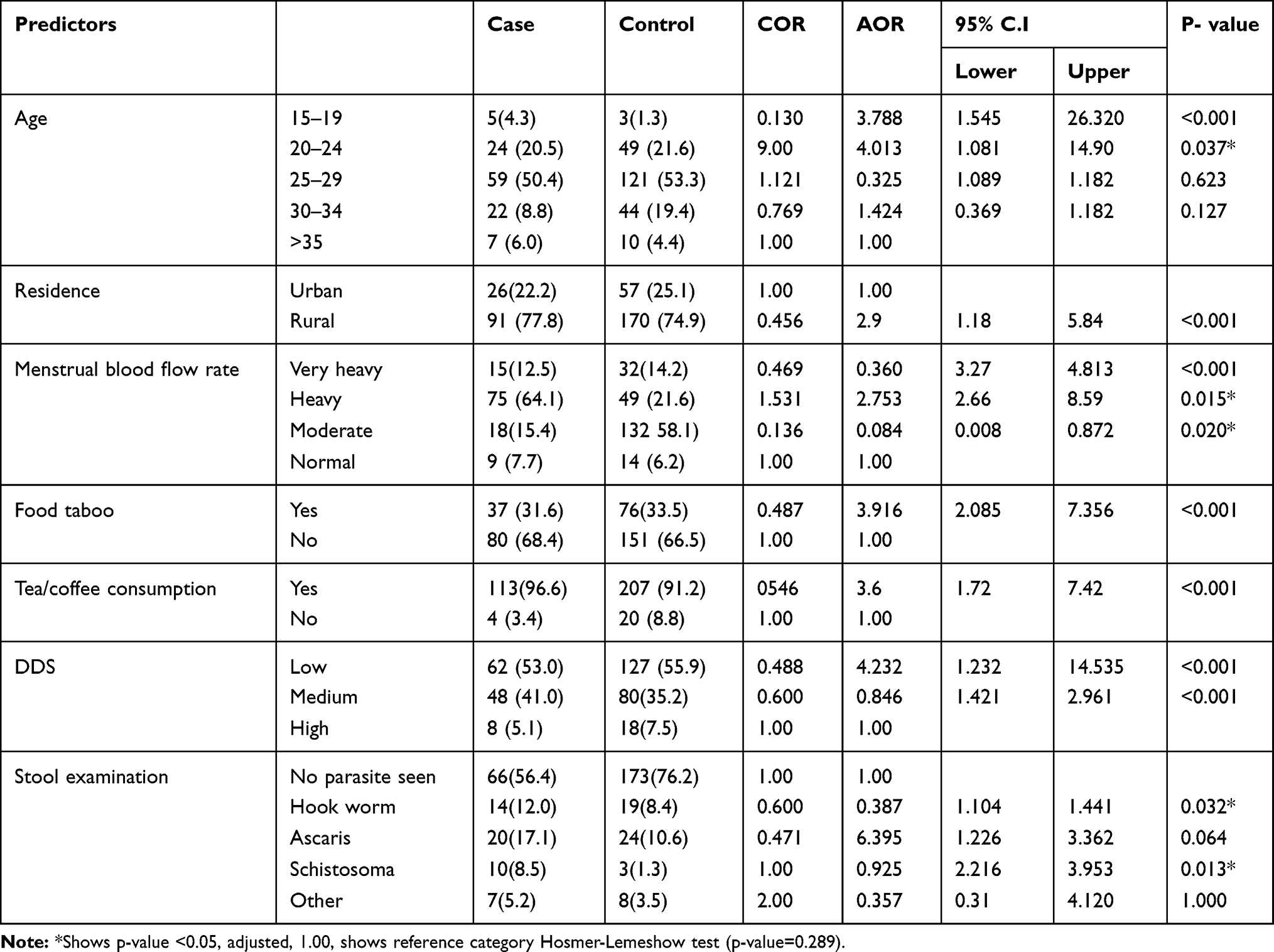 |
Table 3 Multivariable Logistic Regression Model Predicting Anemia Among Pregnant Mothers Attending ANC in Public Health Facilities of Kacha Birra Woreda February to May 2019 |
Discussion
To successfully avert anemia during pregnancy, it’s important to pinpoint the factors which underwrite to the cause of anemia. This study aimed to pinpoint the main forecasting risk factors of anemia using data gained from ANC clinics of health facilities found in Kacha Birra district, Southern Ethiopia.
Therefore, among the foremost forecasting risk factors recognized in this study, pregnant mothers who had heavy menstrual bleeding (6–8 days) before the index pregnancy. Women who had prolonged menstrual period before the index pregnancy were 2.7 times more likely to be anemic during pregnancy than who had less duration of menstruation (3–5 days), this result is in covenant with a study done in Mekelle City,19 Dessie Hospital,15 Yirgalem and Hawassa cities,20 and in Durame town public health centers southern Ethiopia.17 Persistent menstrual bleeding (> five days) was significantly related with the existence of severe anemia among pregnant mothers who came for ANC visits in Mekelle city public hospitals.21 Mizantepi Teaching Hospital.3 This might be because heavy blood loss during extended menstrual bleeding, might lead to iron deficiency anemia.
Living in a rural place was statistically associated with iron deficiency anemia among pregnant mothers who came for ANC visits. Pregnant women living in a rural area were 2.9 times more likely to be anemic than those who live in urban areas, which is consistent with a study showed in Mekelle city public hospitals.18 This might be due to geographical variation of the study area. Socioeconomic factors, cultural differences, a lack of information about adequate nutrition during pregnancy, and the remoteness of health-care facilities in the rural areas.21 To reduce the risk of anemia, women need to be empowered economically, participating in decision making, and receive nutrition education and counseling services for dietary diversification.
Pregnant women with low dietary diversity were 4.21 times more likely to be anemic related to those with a high Dietary Diversity Score, which agrees with the study conducted in Tigray.18 Poor dietary diversity might lead to a deficiency of micronutrients such as vitamins, minerals, and others trace elements that may increase the bioavailability of iron, thus cause iron malabsorption or it affecting iron status. This could be because pregnancy is an exceptional period with increased nutrient and energy requirements, which can be achieved with increased meal frequency and diversification.
Another exciting finding of this study is that a highly significant association was experiential between intestinal parasitic infection and anemia. The current study showed that anemia was highly associated with parasitic infestations. Pregnant mothers who had intestinal parasitic infection were nearly 6.4 times more likely to be anemic. This result is in agreement with a study done in South Sudanese Refugees Pugnido Western Ethiopia.27
The study was done in Gonder Azezo hospital,13 Yirgalem Hawassa cities,22 Durame Town public health centers.17 This might be due to water sources, shoe-wearing habit, eating of raw meat eating habit, blood loss caused by intestinal parasitic infestations which could be exposed mothers at high risk of iron deficiency anemia. Infections with common intestinal parasites such as Ascaris lumbricoides, Schistosoma, and hookworm among pregnant mothers were found to be independent predictors of iron deficiency anemia. Likewise, drinking tea/coffee instantly after the food was also a strong positive association with anemia during pregnancy. The probabilities of developing anemia among pregnant women who were drinking tea/coffee instantly after food were 3.6 times greater. These findings are in agreement with a study conducted East Anatolian Province Hospital Turkey,23 tertiary level hospital, Kathmandu with14,16 Pakistan with times among tea or coffee consumers24 and Tikur Anbesa Specialized Hospital which indicated a significant association between anemia and drinking of tea/coffee.3 This might be consumption tea/coffee after food intake immediately may interfere with iron absorption which leads to insufficient dietary iron intake in the pregnant mother, tea reduces iron absorption.
The chances of being anemic were 4 times higher among pregnant mothers aged between 25 and 24 years compared to women age >35 years. Similar studies in Ghana21 and Tikur Anbesa specialized hospital12 have also shown a significant association between age groups and anemia.14 This study showed that late pregnancy is a significantly associated with an amplified risk of developing anemia. It is commonly believed that anemia in pregnancy increases with rising parity and maternal age besides the general body weakness with advanced maternal age; older women are expected to be multigravidae. Multigravida might persuade anemia by decreasing maternal iron reserves at each pregnancy and by causing blood loss at every delivery.11
This study used an unmatched case-control study to isolate the determinants of anemia in the study area. However, we acknowledge the following limitations. We used 24-hour recall to capture dietary practices. Although dietary practices tend to be similar on an average, this may not show the seasonal variations.
Conclusion
This study acknowledged important factors that determine anemia among pregnant mothers in the study area. Among these determinant factors, food taboo during pregnancy, dietary diversity, the rural residence of mothers consumption tea/coffee instantly after food intake, older age of pregnant women, history of heavy menstrual blood flow before the index pregnancy and presence of parasitic infestations in current pregnancy were the determinants of anemia during pregnancy.
It is recommended that intervention based on policies and strategies on pinpoint the determinant factors especially; control or eradication and prevention of intestinal parasitosis infection and nutrition correlated problems resolving strategies will be very vital or crucial to struggle anemia among the group.
Further community-based study with robust study design and large sample size should be conducted to detect other risk factors of anemia associated with pregnant mother to address those mother that are incapable to appear the ANC clinic follow up in health facilities.
Abbreviations
ANC, antenatal care; AOR, adjusted odds ratio; CDC, Center for Disease Control and Prevention; CI, confidence interval; COR, crude odds ratio; DDS, Dietary Diversity Score; G/dl, gram per deciliter; HCG, human chorionic gonadotropin; Hgb, hemoglobin; HMB, heavy menstrual bleeding; LMP, last menopausal period; SOP, standard operational procedure; WHO, World Health Organization.
Ethics Approval and Informed Consent
Ethical clearance was obtained from the Ethical Review Board of Jimma University’s official letter of cooperation from Jimma University was given to Kacha Birra district health office. Participants under the age of 18 years were approved by the Ethical Review Board of Jimma University to provide informed consent on their behalf. Study subjects were informed about the significance of the study and awareness of their contribution is critical to generate helpful information to themselves and the nation. Informed written consent was obtained from each study participants given with full information including the objectives of the study, selection criteria, confidentiality, and benefits of the study. The response of each participant was reserved confidential and it will be used only for research purposes. Every laboratory investigation was done according to the requirement of the patient.
Acknowledgments
First of all, we would like to thank the almighty God for helping us in the whole work of our study. Secondly, I gratefully thank Jimma University, institute of health, faculty of public, Nutrition, and Dietetics Department for sponsoring this study. The authors would also like to thank the study participants and data collectors.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The study was entirely sponsored by Jimma University, Institute of Health, and Faculty of Public Health.
Disclosure
The authors report no conflicts of interest in this work.
References
1. McLean E, Cogswell M, Egli I, Wojdyla D, De Benoist B. Worldwide prevalence of anaemia, WHO vitamin and mineral nutrition information system, 1993–2005. Public Health Nutr. 2009;12(4):444–454. doi:10.1017/S1368980008002401
2. Telatar B, Erginöz E, Akın Y, et al. Iron use in pregnant women and prevalence of prenatal anemia. Turk J Fam Med Prim Care. 2014;8(1):13. doi:10.5455/tjfmpc.31798
3. Zekarias B, Meleko A, Hayder A, Nigatu A, Yetagessu T. Prevalence of anemia and its associated factors among pregnant women Attending Antenatal Care (ANC) in Mizan Tepi University Teaching Hospital, South West Ethiopia. Health Sci J. 2017;11(5):1–8. doi:10.21767/1791-809X.1000529
4. World health organization division of family Health Geneva. 1993.
5. Goddard AF. Guidelines for the management of iron deficiency anaemia. Gut. 2000;46(suppl 90004):iv1–iv5. doi:10.1136/gut.46.suppl_4.iv1
6. Gangopadhyay R, Karoshi M, Keith L. Anemia and pregnancy: a link to maternal chronic diseases. Int J Gynecol Obstet. 2011;115:S11–S15. doi:10.1016/S0020-7292(11)60005-2
7. Ayano B, Amentie B. Assessment of prevalence and risk factors for anemia among pregnant mothers attending Anc clinic at Adama Hospital Medical Collage, Adama, Ethiopia, 2017. J Obstet Gynecol. 2018;6(3):31–39. doi:10.11648/j.jgo.20180603.11
8. Alkire BC, Vincent JR, Burns CT, Metzler IS, Farmer PE, Meara JG. Obstructed labor and caesarean delivery: the cost and benefit of surgical intervention. PLoS One. 2012;7(4):e34595. doi:10.1371/journal.pone.0034595
9. GotFDR E. National Nutrition Programme June 2013-June 2015. Addis Ababa: Government of Federal Democratic Republic of Ethiopia; 2013.
10. Agency CS, Ababa A. Federal democratic Republic of Ethiopia demographic and health survey. 2016.
11. Okube OT, Mirie W, Odhiambo E, Sabina W, Habtu M. Prevalence and factors associated with anaemia among pregnant women attending antenatal clinic in the second and third trimesters at pumwani maternity hospital, Kenya. Open J Obstet Gynecol. 2016;6(01):16. doi:10.4236/ojog.2016.61003
12. Jufar AH, Zewde T. Prevalence of anemia among pregnant women attending antenatal care at Tikur Anbessa Specialized Hospital, Addis Ababa Ethiopia. J Hematol Thromb Dis. 2014;2(125):2.
13. Alem M, Enawgaw B, Gelaw A, Kena T, Seid M, Olkeba Y. Prevalence of anemia and associated risk factors among pregnant women attending antenatal care in Azezo Health Center Gondar town, Northwest Ethiopia. J Interdiscip Histopathol. 2013;1(3):137–144. doi:10.5455/jihp.20130122042052
14. Anlaakuu PE Anaemia in Pregnancy among Antenatal Attendants at the Sunyani Municipal Hospital [Doctoral dissertation]. University of Ghana. 2015.
15. Tadesse SE, Seid O, GMariam Y, et al. Determinants of anemia among pregnant mothers attending antenatal care in Dessie town health facilities, northern central Ethiopia, unmatched case-control study. PLoS One. 2017;12(3):e0173173. doi:10.1371/journal.pone.0173173
16. Mulepati S, Chaudhary TK. Determinants of anemia among pregnant women attending in a tertiary level Hospital, Kathmandu. Med Phoenix. 2017;2(1):24–33. doi:10.3126/medphoenix.v2i1.18382
17. Weldekidan F, Kote M, Girma M, Boti N, Gultie T. Determinants of anemia among pregnant women attending antenatal clinic in public health facilities at Durame town: unmatched Case Control Study. Anemia. 2018;2018:1–8. doi:10.1155/2018/8938307
18. Ebuy Y, Alemayehu M, Mitiku M, Goba GK, Ciccozzi M. Determinants of severe anemia among laboring mothers in Mekelle city public hospitals, Tigray region, Ethiopia. PLoS One. 2017;12(11):e0186724. doi:10.1371/journal.pone.0186724
19. Nurdin MS, Hadju V, Ansariadi AZ, Zulkifli A, Arundhana AI. Determinants of anaemia among pregnant women in Jeneponto Regency. Pak J Med Sci. 2018;12(1):429–434.
20. Nik Rosmawati NH, Mohd Nazri S, Mohd Ismail I. The rate and risk factors for anemia among pregnant mothers in Jerteh Terengganu, Malaysia. J Community Med Health Educ. 2012;2(150):2161–2711.
21. Grum T, Brhane E, Hintsa S, Kahsay G. Magnitude and factors associated with anemia among pregnant women attending antenatal care in public health centers in central zone of Tigray region, northern Ethiopia: a cross sectional study. BMC Pregnancy Childbirth. 2018;18(1):433. doi:10.1186/s12884-018-2063-z
22. Argaw B, Argaw-Denboba A, Taye B, Worku A, Worku A. Major risk factors predicting anemia development during pregnancy: unmatched-case control study. J Community Med Health Educ. 2015;5(353):2161–2711.
23. Karaoglu L, Pehlivan E, Egri M, et al. The prevalence of nutritional anemia in pregnancy in an east Anatolian province, Turkey. BMC Public Health. 2010;10(1):329. doi:10.1186/1471-2458-10-329
24. Baig-Ansari N, Badruddin SH, Karmaliani R, et al. Anemia prevalence and risk factors in pregnant women in an urban area of Pakistan. Food Nutr Bull. 2008;29(2):132–139. doi:10.1177/156482650802900207
25. World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Geneva: WHO; 2011. Contract No.: WHO/NMH/NHD/MNM/11.1. 2018.
26. Nkrumah B, Nguah SB, Sarpong N, et al. Hemoglobin estimation by the HemoCue® portable hemoglobin photometer in a resource poor setting. BMC Clin Pathol. 2011;11(1):5. doi:10.1186/1472-6890-11-5
27. Alemayehu A, Gedefaw L, Yemane T, Asres Y. Prevalence, Severity, and Determinant Factors of Anemia Among Pregnant Women in South Sudanese Refugees, Pugnido, Western Ethiopia. Hindawi Publishing Corporation; 2016. doi:10.1155/2016/9817358
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.