Back to Journals » Medical Devices: Evidence and Research » Volume 19
Design and Technical Validation of a Novel O2 Mixed Fitting for Dual Connection in Medical Oxygen Delivery Systems
Authors Quintero Osorio OI ![]() , Basançelebi B
, Basançelebi B ![]() , Santos EDCD
, Santos EDCD ![]() , Prada SI
, Prada SI ![]() , Lemos DA
, Lemos DA ![]() , Domínguez AF, Esquinas AM
, Domínguez AF, Esquinas AM ![]()
Received 17 April 2026
Accepted for publication 10 June 2026
Published 9 July 2026 Volume 2026:19 612748
DOI https://doi.org/10.2147/MDER.S612748
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mohamad Bashir
Video abstract of “O2 Mixed Fitting for Dual Connection in Medical Oxygen Delivery” [612748].
Views: 9
Oscar Ivan Quintero Osorio,1 Berkan Basançelebi,2 Elinaldo da Conceição dos Santos,3 Sergio I Prada,1,4 David Alexander Lemos,1 Andrés Felipe Domínguez,5 Antonio M Esquinas6
1Centro de Investigaciones Clínicas, Fundación Valle del Lili, Cali, Colombia; 2Department of Electroneurophysiology, Vocational School, Istanbul Medipol University, Istanbul, Turkey; 3Department of Biological and Health Sciences, Universidade Federal Do Amapá, Macapá, Brazil; 4Centro PROESA, Universidad Icesi, Cali, Colombia; 5PromPack S.A.S, Cali, Colombia; 6Intensive Care Unit, Hospital Meseguer, NIV-ICM, Instituto Murciano de Investigación Biosanitaria, Murcia, Spain
Correspondence: Oscar Ivan Quintero Osorio, Email [email protected]
Background: Medical oxygen delivery systems require adaptable connection interfaces capable of supporting different clinical configurations during oxygen therapy. Integrating multifunctional connection mechanisms within a single component offers an opportunity to improve system versatility and connection management in respiratory care settings.
Objective: To design and experimentally validate a novel dual-connection fitting for medical oxygen delivery, designated as the O2 Mixed Fitting, that enables simultaneous attachment of both a bubble humidifier and conventional oxygen tubing while remaining installed on the flowmeter.
Methods: A comprehensive state-of-the-art review informed the conceptual development of the device. Iterative design refinement was performed using computer-aided design. The final device was manufactured by injection molding using medical-grade Acrylonitrile Butadiene Styrene. Validation included gas flow analysis, leak and pressure-holding tests, microbiological and physical stability evaluation under controlled climatic conditions, and sustainability assessment using a structured eco-design framework.
Results: The integrated dual-connection mechanism enabled transition between humidified and non-humidified oxygen delivery without detachment from the flowmeter. Gas flow measurements remained within predefined accuracy tolerances, including ± 0.5 L/min at low flows and ± 10% at higher flows. No leakage was detected during pressure testing up to 10 psi. During the 12-month natural stability study, physical and microbiological parameters remained within predefined acceptance criteria under climatic zone IVb conditions. The eco-design assessment demonstrated favorable environmental performance.
Conclusion: The O2 Mixed Fitting represents an innovative dual-connection solution for medical oxygen delivery applications. Laboratory validation confirmed structural integrity, flow stability, pressure resistance, and physical and microbiological stability under the evaluated conditions. The integrated design enhances functional versatility while maintaining full compatibility with existing clinical infrastructure. Further clinical and operational studies are warranted to evaluate its potential impact on patient care and clinical workflow.
Keywords: medical oxygen, oxygen therapy, oxygen connector, bubble humidifier, medical device design, biomedical engineering
Introduction
Medical oxygen connectors are widely used devices in the administration of oxygen therapy. These connectors are known by several names, including oxygen connector, nut adapter, mouse-tail connector, Christmas-tree connector, and Diameter Index Safety System (DISS) oxygen connector, the latter being among the most used terms in clinical practice.1
The design of these connectors has evolved alongside advances in oxygen storage and delivery systems. Although their shape, color, and manufacturing materials may vary among manufacturers, their structural characteristics are regulated by international standards established for medical gas devices.
When attached to the flowmeter, the connector enables the delivery of oxygen to the patient. However, standard clinical practice often requires removal of the connector to attach a bubble humidifier (BH). In routine clinical settings, this repeated manipulation may occasionally lead to connector misplacement or loss, which can contribute to workflow interruptions during oxygen therapy.
Several strategies and devices have been developed to enable dual connectivity between BHs and conventional oxygen tubing (COT), including dual-port flowmeters, modified oxygen tubing with threaded DISS 1240 connectors, and metal or plastic connectors with fixation systems.1 Although these alternatives may facilitate oxygen therapy management, their implementation may be limited by equipment availability, compatibility constraints, higher costs, or additional handling requirements during routine clinical use. Repeated attachment and detachment of conventional oxygen connectors may also contribute to temporary connector loss, additional handling steps, or operational inefficiencies during oxygen therapy administration.
In this context, the present study describes the development of a novel mixed fitting for medical oxygen that allows connection of both a BH and COT without removing the device from the flowmeter, providing an additional alternative for connection management during oxygen therapy.
Materials and Methods
In 2017, after identifying the opportunity to develop a device capable of integrating both oxygen connection mechanisms, the development of the Mixed Fitting for Medical Oxygen (O2 Mixed Fitting) was conceptualized and developed. The following sections provide a detailed description of the state-of-the-art review, design and prototyping stages, manufacturing process, applicable regulations, metrological validation, intellectual property protection, and environmental impact assessment.
State-of-the-Art Review
The development process was informed by a systematic review of the state of the art of connection devices used in medical oxygen systems. The literature review was conducted using major academic databases (Web of Science, Scopus, PubMed, Semantic Scholar, and Google Scholar) and patent databases (Patentscope, Espacenet, EPO, USPTO, Google Patents, and The Lens). In addition, information available on manufacturers and distributors’ websites was reviewed.
Boolean operators (AND, OR, NOT) were applied using combinations of keywords such as fitting, nipple, oxygen adapter, and oxygen connector. Retrieved information was screened to identify designs compatible with the DISS 1240 thread, specifically the 9/16-inch female interface and the coupling port for COT with internal diameters ranging from 5/32 inch (3.97 mm) to 1/4 inch (6.35 mm), consistent with standard connector configurations.
The state-of-the-art review confirmed that BHs are commonly used in the management of patients receiving oxygen therapy. In these devices, gas flow passes through water, generating multiple bubbles that increase air–liquid contact and promote evaporation, allowing humidification of the delivered oxygen.2,3 BHs may be reusable devices, disposable units requiring manual filling, or disposable units prefilled with sterile water.4
Bubble humidifiers typically incorporate a female DISS 1240 thread for connection to the flowmeter and include a pressure-relief valve as a safety mechanism, usually calibrated between 2 and 7 psi depending on the manufacturer.
In conventional clinical practice, when dry oxygen delivery is required during procedures such as drug nebulization, the humidifier is often removed from the flowmeter to allow direct connection of COT through a conventional connector.5,6 Similar situations may occur during bag-valve-mask ventilation or when reservoir masks are used, where humidifier use is not recommended due to condensation and potential interference with proper reservoir bag expansion.7,8 These situations involve repeated manipulation of the connector, which may increase the likelihood of device misplacement.
Strategies Enabling Dual Connection
Several devices and strategies currently incorporate dual connection mechanisms for COT and BHs (Figure 1). Some flowmeter designs integrate both connection ports directly into the device, including a dedicated outlet for COT and a DISS 1240 threaded port for BH attachment. This configuration standardizes a gas-specific thread design, functioning as a physical error-prevention mechanism by using connector size and geometry to reduce the risk of misconnections between different medical gases.
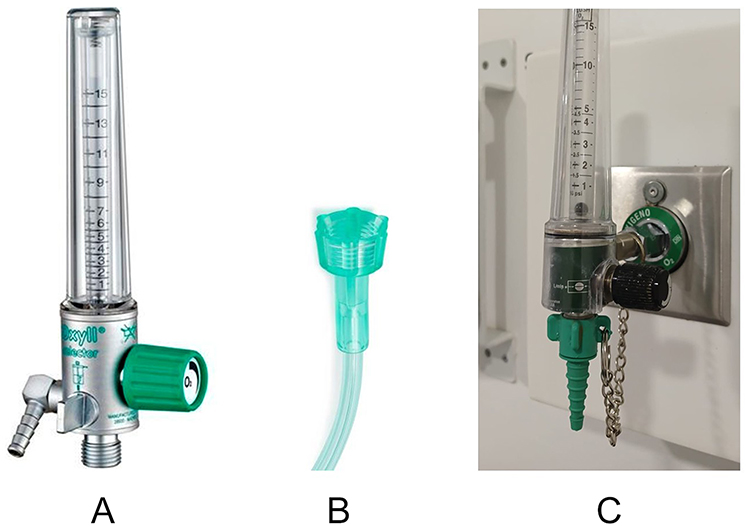 |
Figure 1 Devices and strategies incorporating connection ports for bubble humidifiers and oxygen tubing. (A) Flowmeter with a dedicated port for conventional oxygen tubing and a DISS 1240 threaded connection. (B) Oxygen tubing with an integrated female DISS 1240 thread. (C) Strategy for securing a plastic connector to the flowmeter using a chain. |
An alternative approach involves modifications to the COT itself. In some designs, one end of the tubing incorporates a female DISS 1240 thread that allows direct connection to the flowmeter while simultaneously permitting attachment of a conventional fitting through the central lumen of the tubing.
Metal connectors incorporating chain-fastening systems to secure the connector to the flowmeter are also commercially available. Similar strategies have been replicated in plastic designs using nylon cords, wires, or stainless-steel chains. However, in plastic implementations, these solutions often require additional handling during installation and routine use. As a result, strict cleaning and disinfection protocols between uses are necessary to minimize the risk of cross-contamination and to ensure safe operating conditions.1
Although these devices and strategies can be effective in maintaining dual connectivity, their implementation may vary depending on the clinical setting and the availability of compatible equipment. Limitations include the higher cost of metal connectors and dual-connection flowmeters, the lack of universal availability of DISS 1240 threads across all oxygen tubing designs, and international guidelines recommending single-patient use for disposable medical devices, which restrict reprocessing or reuse across patients.9 Consequently, frequent attachment and detachment of plastic connectors during routine use may introduce additional handling steps for healthcare personnel.
Repeated connector manipulation during transitions between humidified and non-humidified oxygen therapy may also contribute to workflow interruptions and increase the number of handling steps required during routine respiratory support. In high-demand clinical settings, simplifying these transitions may improve operational efficiency and facilitate oxygen delivery management.
Conventional Medical Oxygen Connectors: Design and Materials
Following the review of strategies enabling dual connection, the design specifications of conventional medical oxygen fittings and the standards governing their connection to BHs and oxygen tubing were examined.
Analysis of conventional connector designs identified two main configurations: single-body fittings and two-body fittings consisting of a rotating component for coupling to the flowmeter and a separate component for connection to the oxygen tubing (Figure 2). A feature common to all designs is the presence of the DISS 1240 thread. The COT connection port typically has a conical shape with several stepped rings or barbs that facilitate secure tubing attachment. External elements that facilitate tightening of the fitting onto the flowmeter may include smooth or grooved cylindrical fins, flat faces arranged in a hexagonal configuration, or combinations of these features.
 |
Figure 2 Diversity of designs and manufacturing materials used in conventional medical oxygen connectors. (A) Plastic connectors. (B) Metal connectors. (C) Hybrid connectors combining plastic and metal components. |
Medical oxygen fittings are manufactured from materials selected according to their intended use. Devices designed for single-patient use are typically produced from medical-grade plastics such as acrylonitrile butadiene styrene (ABS), nylon, polyacetal, polypropylene, or polyvinyl chloride (PVC). In contrast, fittings intended for multiple uses are commonly manufactured from metallic materials including stainless steel, bronze, aluminum, or nickel-plated brass. Hybrid designs combining plastic and metal components are also available. Plastic oxygen fittings are mainly produced in shades of green, although translucent, blue, and white versions are also available.
Medical oxygen flowmeters are available in a wide range of designs depending on the flow range they provide. Precision flowmeters typically allow flow control between 0.1 and 1 L/min, conventional flowmeters between 1 and 15 L/min, and high-flow flowmeters between 5 and 75 L/min. Despite these variations, all designs incorporate a male DISS 1240 thread that ensures a secure connection with oxygen delivery equipment.
Mixed Fitting Design for Medical Oxygen
Following the state-of-the-art review, it was determined that a new connector design could be developed integrating both connection mechanisms: a port for the BH and a lower port for COT without requiring removal from the flowmeter. This configuration allows the device to remain installed on the flowmeter, reducing the risk of misplacement and improving its availability during oxygen delivery. This concept led to the development of the O2 Mixed Fitting.
During the initial design phase, multiple prototypes were produced using acetal through computerized numerical control (CNC) milling. These were followed by prototypes manufactured by three-dimensional (3D) printing using castable resin. Metrological evaluations conducted during this stage allowed dimensional refinement, optimization of assembly mechanisms, and assessment of component interaction.
The final design was developed using SOLIDWORKS 2022 (Dassault Systèmes SolidWorks Corp., Waltham, MA, USA). Two main components were defined: a main body and a lower port. Structural analysis was performed using the finite element method (FEM)10 to evaluate stress distribution and deformation under expected operating loads. This analysis enabled geometric optimization to reduce material consumption and determine wall thicknesses required to ensure structural integrity and appropriate safety factors during the device’s service life.
The O2 Mixed Fitting was developed at the Clinical Research Center of Fundación Valle del Lili, a high-complexity hospital in Cali, Colombia, and is manufactured by PromPack S.A.S., Cali, Colombia, under the PromMedic brand, operating under a quality management system compliant with ISO 13485:201611 and ISO 9001:2015.12 The O2 Mixed Fitting was classified as a Class IIa medical device by the Colombian regulatory authority, INVIMA (Instituto Nacional de Vigilancia de Medicamentos y Alimentos), through its Specialized Committee for Medical Devices and in vitro Diagnostic Reagents. Intellectual property protection was obtained through a national innovation funding program administered by the Ministerio de Ciencia, Tecnología e Innovación (Minciencias), resulting in patent No. NC2017/0011410, granted by the Superintendence of Industry and Commerce, Colombia.
Injection Mold Design and Fabrication
The injection mold was designed with four cavities (Class 104), enabling simultaneous molding of all components. An automatic unscrewing mechanism was incorporated to facilitate part ejection, together with interchangeable mold plates intended to reduce maintenance time and improve process efficiency.
The O2 Mixed Fitting is produced in a blue-green color and manufactured by injection molding using ABS as a non-sterile, single-patient-use respiratory accessory, consistent with the intended use and classification of similar oxygen connector devices currently available in clinical practice. This material was selected due to its high mechanical strength and rigidity, allowing compliance with the functional and performance requirements for clinical use. In addition, ABS is free of polyvinyl chloride (PVC) and phthalate plasticizers, including di-(2-ethylhexyl) phthalate (DEHP),13–15 reducing potential risks associated with chemical exposure in healthcare environments.
Design Description of the O2 Mixed Fitting
The components of the O2 Mixed Fitting are illustrated in (Figure 3). The upper portion of the main body has a quadrant-shaped geometry that facilitates manual gripping during attachment to the flowmeter and, if desired, allows additional tightening with a standard wrench, helping the O2 Mixed Fitting remain installed on the flowmeter. The inventor’s initials (“OIQ”) are engraved in bas-relief on the four lateral faces of the main body (Figure 3A). The device consists of three main components: the main body, the lower port, and a silicone O-ring (Figure 3B). The rotational direction that enables the ascent and descent of the lower port is shown in (Figure 3C).
 |
Figure 3 Injection-molded design and cross-sectional views of the O2 Mixed Fitting. (A) Assembled O2 Mixed Fitting. (B) Disassembled O2 Mixed Fitting showing: 1, main body; 2, lower port; 3, silicone O-ring. (C) Cross-sectional view of the assembled O2 Mixed Fitting with the lower port in the lowered position; arrows indicate the direction of rotation for raising and lowering the lower port. (D) Cross-sectional view of the disassembled O2 Mixed Fitting illustrating: 1, quadrant-shaped gripping surface; 2, upper internal thread; 3, internal cylindrical cavity of the main body; 4, external thread; 5, lower internal thread; 6, silicone O-ring; 7, lower port thread; 8, grip rings; 9, cylindrical cavity of the lower port. |
The individual components and their internal features are shown in (Figure 3D). The upper internal female DISS 1240 thread enables secure coupling to the flowmeter. An internal cylindrical cavity within the main body allows oxygen flow and houses the lower port. The lower internal thread functions as the mechanism for raising and lowering the lower port and works together with the silicone O-ring to provide positional stability and sealing. The lower external male DISS 1240 thread serves as the connection interface for the BH and COT equipped with a DISS threaded connector.
The lower port is designed for connection to COT. It includes an upper threaded section that engages with the lower internal thread of the main body, allowing controlled vertical movement. A circumferential groove accommodates the silicone O-ring. Three external rings facilitate secure attachment of COT, while an internal lumen allows the passage of oxygen.
Instructions for Use of the O2 Mixed Fitting
Connection to the Flowmeter
Manually screw the O2 Mixed Fitting onto the flowmeter until it reaches the mechanical stop, then complete tightening with approximately one-quarter (1/4) turn. Because the O2 Mixed Fitting is designed to remain installed during use, this adjustment improves stability and reduces the risk of misplacement.
Use with a Bubble Humidifier
Without removing the O2 Mixed Fitting from the flowmeter, rotate the lower port upward and connect either oxygen tubing with a DISS 1240 connector or a bubble humidifier to the external DISS 1240 thread of the fitting. Subsequently, connect the COT to the humidifier.
Use with Conventional Oxygen Tubing
When the bubble humidifier is removed from the O2 Mixed Fitting, the lower port partially descends by gravity. Full descent is achieved by rotating the lower port until it reaches the mechanical stop. In this position, compression of the silicone O-ring provides effective sealing that prevents leakage and stabilizes the lower port. Once in this position, the oxygen tubing can be securely connected and removed by pulling downward.
Special Recommendations and Precautions
Although the design of the O2 Mixed Fitting complies with applicable manufacturing standards, its configuration requires specific handling recommendations to ensure proper operation and durability.
- When attaching the bubble humidifier to the O2 Mixed Fitting, ensure proper alignment of the threads to prevent damage to the threaded interfaces.
- When connecting or removing COT from the lower port, apply force in a vertical direction and avoid lateral pulling.
These recommendations reflect general handling principles for plastic devices. Although the O2 Mixed Fitting is manufactured from high-density ABS and designed for safe clinical use, excessive force or improper handling may cause mechanical damage.
Validation of the O2 Mixed Fitting
Selection of Metrological Instruments
Airflow and leak detection tests were performed by an independent metrology laboratory, which selected the measurement instruments and established the evaluation protocols for the O2 Mixed Fitting in both lower port configurations (raised and lowered) (Figure 4). All instruments used in the evaluation were calibrated according to the manufacturers’ specifications and maintained traceability to national or international measurement standards. Metrological measurements were performed on three samples (one sample per batch, selected at random). The same sample was evaluated in each of the leakage and flow scenarios. All measurement points and test conditions were maintained for 5 minutes to evaluate flow and pressure stability, measurement accuracy, and leakage performance. Measurement uncertainty was estimated by the metrology laboratory using expanded uncertainty calculations with a 95% confidence level, considering contributions from the measurement equipment and reference standards. Each O2 Mixed Fitting was manually tightened onto the flowmeter and measuring instrument until the mechanical stop was reached, followed by an additional one-quarter (1/4) turn.
 |
Figure 4 Schematic diagram and metrological setup used to evaluate airflow and leakage in the O2 Mixed Fitting. Flow testing: (A) O2 Mixed Fitting with the lower port lowered and connected to conventional oxygen tubing; (B) lower port raised and connected to oxygen tubing with a plastic DISS 1240 thread; (C) lower port raised and connected to a bubble humidifier. Leakage (pressure-holding) testing: (D) lower port lowered and connected to conventional oxygen tubing; (E) lower port raised and connected to oxygen tubing with a plastic DISS 1240 thread. |
Flow Testing
Flow measurements were performed using a VT PLUS HF Gas Flow Analyzer (Fluke Corporation, Everett, WA, USA). The oxygen source consisted of a compressed oxygen cylinder connected to a Victor® (oxygen pressure regulator, VMG 15LN, 2–15 L/min, CGA 540). For high-flow measurements (5–75 L/min), a Timeter® (high-flow flowmeter, Model TB30, Allied Medical LLC, USA) connected to the wall oxygen supply was used.
Measurements were conducted with the O2 Mixed Fitting in the raised lower port configuration under three connection scenarios: (A) connected to COT (Figure 4A); (B) connected to DISS 1240–threaded oxygen tubing (Figure 4B); and (C) connected to a BH filled with water to the maximum level recommended by the manufacturer (Figure 4C).
Leak and Pressure-Holding Test
A pneumatic hand test pump (LPP-40 Air Pressure Gauge Test Pump, WIKA Instrument, Germany) was used to generate controlled pressure during leak testing. Measurements were performed with the O2 Mixed Fitting in both lower port configurations.
For the lowered lower port configuration, the fitting was connected to COT and to the VT PLUS HF analyzer (Figure 4D). For the raised lower port configuration, the fitting was connected to DISS 1240 threaded oxygen tubing and to a high-precision digital pressure gauge (CPG 1500, WIKA Instrument, Germany) (Figure 4E).
Leak testing was performed using pressures exceeding 10 psi, selected to surpass the maximum pressure expected under clinical conditions, considering that BHs typically incorporate pressure-relief valves calibrated up to 7 psi.
The O2 Mixed Fitting was designed, tested, and manufactured in compliance with the following international standards: risk management (ISO 14971:201915), connector non-interchangeability (CGA V-5, DISS 1240 specification), safety in oxygen-enriched environments (ISO 15001:202116), and flow performance evaluation (ISO 15002:202317).
Microbiological and Organoleptic Evaluation
To assess device stability, analyses were performed in an independent laboratory using five samples from each of two production batches of the O2 Mixed Fitting. Natural stability studies were conducted under controlled conditions of 30 °C ± 2 °C and 75% ± 5% relative humidity, consistent with climatic zone IVb environmental conditions for long-term stability studies.18,19 The samples were evaluated over a 12-month period. The same samples were longitudinally evaluated throughout the study period and returned to the climatic chamber after each analysis.
Physical and dimensional measurements were performed at baseline (T0) and at 3 month (T3), 6 month (T6), 9 month (T9), and 12 months (T12), final. Physical evaluations included assessment of internal and external surface homogeneity, threaded profile integrity, presence of cracks or molding defects, and color changes. Dimensional measurements included assembly length, body length, width, and weight. Mean values were calculated from the evaluated samples for longitudinal comparison during the study period.
Microbiological analyses were conducted at T0, T6, and T12 and included total aerobic microbial count, combined yeast and mold count, and detection of Staphylococcus aureus and Pseudomonas aeruginosa.
Eco-Design
Environmental Strategy Evaluation
The environmental performance of the O2 Mixed Fitting was assessed using the Environmental Impact Strategy (Ecodesign Strategy Wheel; VEA, by its Spanish acronym)20 (Table 1 and Figure 5).
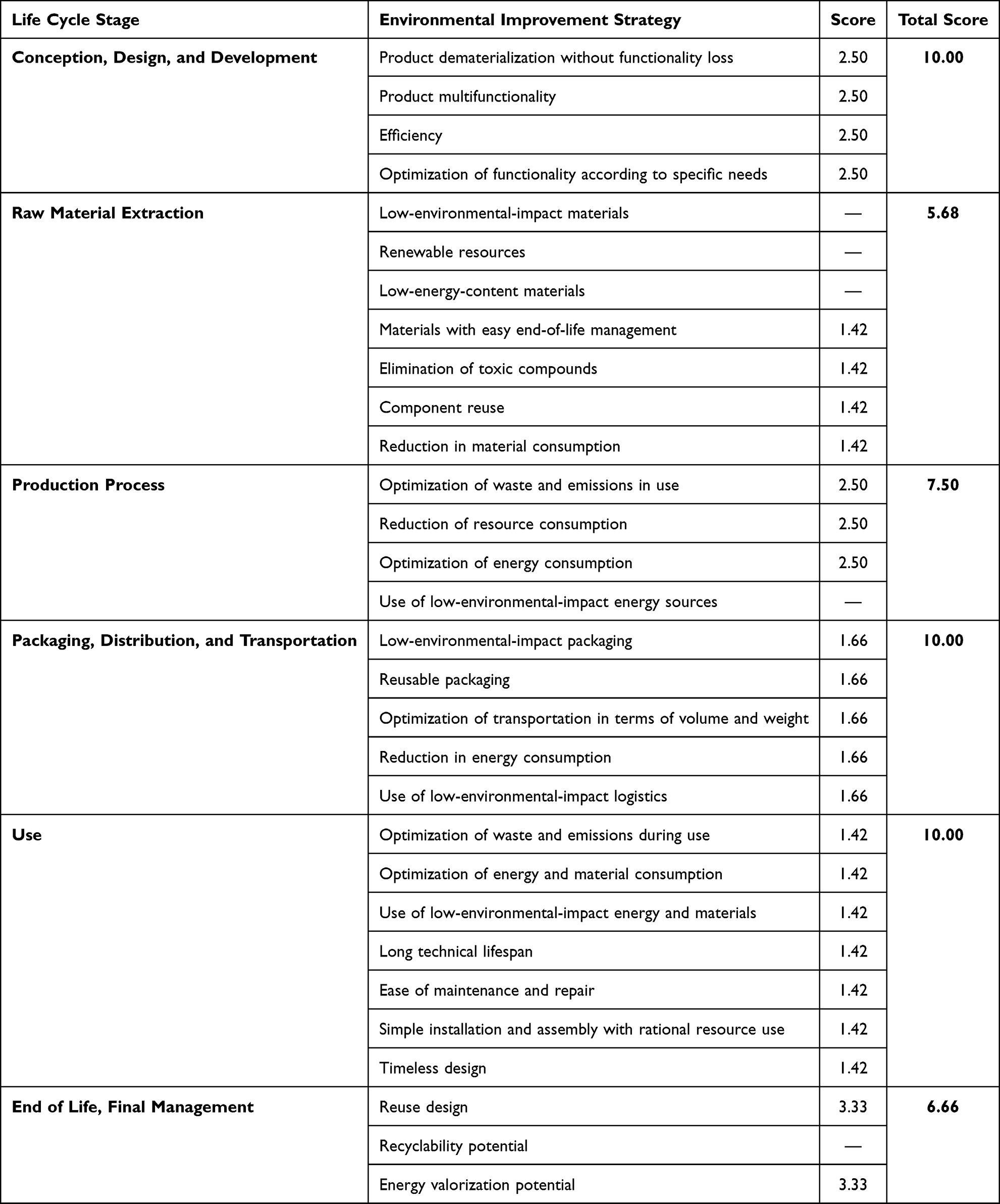 |
Table 1 Environmental Strategy Evaluation of the O2 Mixed Fitting Across Its Life Cycle Using the VEA Method |
 |
Figure 5 Environmental impact profile of the O2 Mixed Fitting across the different stages of the product life cycle. Environmental impact scores for the O2 Mixed Fitting at different stages of the product life cycle, assessed using the Ecodesign Strategy Wheel. |
Statistical Analysis
Descriptive statistics were used to summarize flow and pressure measurements. Continuous variables are presented as mean ± standard deviation (SD). Measurement agreement with nominal flow settings was evaluated by calculating absolute deviation and percentage error. Acceptance criteria were predefined according to ISO 15002:202317 using ±0.5 L/min for low-flow ranges and ±10% for high-flow ranges. Analyses were performed using SPSS version 26 (IBM Corp., Armonk, NY, USA).
Results
Over a nine-year period (2017–2026), the development of the O2 Mixed Fitting progressed through sequential stages of design, prototyping, manufacturing, environmental assessment, and metrological validation.
Results of high- and low-flow metrological testing with the lower port lowered and connected to COT are presented in Table 2; the corresponding experimental setup is illustrated in Figure 4A. Results with the lower port raised and connected to DISS 1240–threaded tubing are presented in Table 3; the corresponding setup is shown in Figure 4B. Measurements with the lower port raised and connected to a BH are presented in Table 4; the corresponding setup is shown in Figure 4C. Leak (pressure-holding) test results with the lower port lowered and connected to COT are presented in Table 5; the corresponding setup is shown in Figure 4D. Results with the lower port raised and connected to DISS 1240–threaded tubing are shown in Table 6; the corresponding setup is illustrated in Figure 4E.
 |
Table 2 Flow Test of the O2 Mixed Fitting with the Lower Port Lowered and Connected to Conventional Oxygen Tubing |
 |
Table 3 Flow Test of the O2 Mixed Fitting with the Lower Port Raised and Connected to DISS 1240–Threaded Oxygen Tubing |
 |
Table 4 Flow Test of the O2 Mixed Fitting with the Lower Port Raised and Connected to a Bubble Humidifier |
 |
Table 5 Leak (Pressure-Holding) Test of the O2 Mixed Fitting with the Lower Port Lowered and Connected to Conventional Oxygen Tubing |
 |
Table 6 Leak (Pressure-Holding) Test of the O2 Mixed Fitting with the Lower Port Raised and Connected to DISS 1240–Threaded Oxygen Tubing |
The 12-month natural stability study, conducted between April 2025 and April 2026, showed no significant changes in the evaluated physical or dimensional parameters of the O2 Mixed Fitting. Mean dimensional and weight measurements remained stable throughout the evaluation period. Microbiological analyses performed at T0, T6, and T12 demonstrated total aerobic microbial count and combined yeast and mold count values <1 CFU/g, with no detection of Staphylococcus aureus or Pseudomonas aeruginosa. These findings support the physical and microbiological stability of the device under the evaluated storage conditions.
The environmental strategy assessment indicated that the Conception, Design and Development, and Use stages achieved the maximum score (10). Production Processes scored 7.5, while End of Life, Final Management scored 6.66. The Raw Material Extraction stage showed the lowest performance (5.7), reflecting reliance on non-renewable resources and limited incorporation of low-environmental-impact materials.
Discussion
The development of the O2 Mixed Fitting extended over nearly a decade. The initial concept emerged in 2017, and the licensing agreement with the manufacturer was finalized in the second half of 2023, enabling the stages of design refinement, manufacturing, metrological validation, and regulatory alignment, which were completed in the first half of 2026. These timelines are consistent with typical research and development pathways for medical devices, where the process from concept to market introduction commonly ranges from 3 to 7 years, compared with an average of approximately 12 years for pharmaceutical products.21
The O2 Mixed Fitting enables simultaneous connection of both a BH and COT without removal from the flowmeter (Figure 6), addressing a practical limitation in routine oxygen therapy management. By enabling dual connection without removing the connector from the flowmeter, the device provides an alternative approach to connection management in oxygen therapy systems. The O2 Mixed Fitting is designed to remain installed on the flowmeter during patient management. Its quadrangular upper body allows an additional tightening of approximately one-quarter (1/4) turn, promoting device stability and reducing the risk of loss.
 |
Figure 6 Real-world use scenarios of the O2 Mixed Fitting. (A) connected to a flowmeter and conventional oxygen tubing. (B) connected to a flowmeter and bubble humidifier. (C) connected to DISS 1240–threaded oxygen tubing. |
This adjustment principle is consistent with that used in conventional oxygen fittings, promoting familiarity for healthcare personnel. This configuration also reduces the need for repeated removal and reattachment of the connector during routine oxygen therapy, potentially simplifying device handling in clinical practice.
The mechanism relies on controlled rotation of a lower port that descends by gravity until reaching a mechanical stop, while sealing in the lowered configuration is reinforced by compression of the integrated silicone O-ring. Because connecting the bubble humidifier requires raising the lower port, while connecting conventional oxygen tubing requires lowering it, this mechanism introduces a modification in the routine handling behavior expected of healthcare personnel. Likewise, the fact that the O2 Mixed Fitting remains installed on the flowmeter during use, rather than being removed as in conventional practice, also introduces a modification in routine device handling. Sealing performance was evaluated through metrological leak testing. No detectable leakage was observed under the evaluated conditions, indicating stable pressure retention in both functional configurations of the device.
High- and low-flow metrological testing confirmed that measured flow values remained within ±0.5 L/min at low flows and ±10% at higher flows. Minor differences between nominal set points and measured values can be attributed to the intrinsic tolerances of flowmeters and measurement instrumentation, as well as the normal flow resistance introduced by the tubing and test setup.
The metrological evaluation included one representative sample obtained from each of three independent production batches, allowing assessment of device performance consistency across manufacturing batches. The consistent results observed in both flow and leak tests demonstrated stable functional performance of the device under the evaluated conditions.
In addition, the 12-month natural stability study conducted under climatic zone IVb conditions demonstrated no significant changes in the evaluated physical, dimensional, or microbiological parameters throughout the study period. Mean dimensional and weight measurements remained stable over time, while microbiological analyses remained within acceptable limits at all evaluated intervals, supporting the storage stability of the device under the tested environmental conditions.
The environmental profile of the O2 Mixed Fitting reflects an eco-design approach focused on multifunctionality and operational efficiency, including reduced material mass and lower transportation-related impacts. The main environmental hotspot was the reliance on virgin raw materials, largely driven by safety, validation, traceability, and risk management requirements within medical device regulatory frameworks such as ISO 14971:201915 and ISO 13485:2016. 11 While these standards ensure patient safety and product quality, they also limit circular material use. Nevertheless, emerging initiatives for recovering and reprocessing single-use medical plastics and metals represent early steps toward improving sustainability in the sector.22–24
Limitations
This study has several limitations. First, the evaluation was limited to bench, metrological, and laboratory stability testing conditions and did not include clinical usability or human factors assessment during routine oxygen therapy. Second, long-term repeated-use performance was not evaluated under extended real-world clinical conditions. Third, the study did not include direct comparative testing against commercially available dual-connection systems. Therefore, potential workflow and operational benefits remain theoretical and should be further investigated in future clinical and usability studies.
In conclusion, the O2 Mixed Fitting represents a practical innovation enabling continuous dual connectivity between BH and COT in medical oxygen delivery systems. Its design features, metrological validation, natural stability evaluation, and regulatory alignment support safe functional performance for the intended application while maintaining compatibility with existing clinical equipment. The device demonstrated stable flow performance, leak resistance, and physical and microbiological stability during a 12-month natural stability study conducted under controlled climatic zone IVb conditions. Future studies should further evaluate long-term repeated-use performance, usability among healthcare personnel, and comparative performance against existing dual-connection systems across different clinical care settings.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Oscar Ivan Quintero is the inventor of the O2 Mixed Fitting described in this study and reports a granted patent No. NC2017/0011410, Resolution No. 49169, Colombia. Additional industrial design registrations have been filed in multiple jurisdictions and are currently under examination. Fundación Valle del Lili, the authoring institution, and PromPack S.A.S., the device manufacturer, maintain a commercial relationship related to the development and commercialization of the O2 Mixed Fitting. The authors report no other conflicts of interest in this work.
References
1. Colandrea NA, Cleary ML, Peaper DR, Sullivan LK, Martinello RA, Murray TS. Oxygen nipple and nut (Christmas tree) adaptor contamination rates and decontamination with disinfecting wipes. Infect Control Hosp Epidemiol. 2020;41(4):396–15. doi:10.1017/ice.2020.9
2. Hayes B, Robinson J, Lee C. Bubble humidification of oxygen: evaluation of humidification efficiency during low-flow oxygen therapy. J Clin Eng. 2016;41(4):182–187. doi:10.1097/JCE.0000000000000163
3. Chikata Y, Onodera M, Oto J, Nishimura M. Humidification performance of two humidification devices for oxygen therapy: a bench study. Respir Care. 2017;62(1):24–30. doi:10.4187/respcare.04940
4. Pilkington F. Humidification for oxygen therapy in non-ventilated patients. Br J Nurs. 2004;13(2):111–115. doi:10.12968/bjon.2004.13.2.16981
5. Ari A, Restrepo RD; (AARC) AA for RC. Clinical practice guideline: aerosol delivery device selection for spontaneously breathing patients. Respir Care. 2012;57(4):613–627. doi:10.4187/respcare.01783
6. Poiroux L, Piquilloud L, Seegers V, et al. Effect on comfort of administering bubble-humidified or dry oxygen: the Oxyrea non-inferiority randomized study. Ann Intensive Care. 2018;8(1):126. doi:10.1186/s13613-018-0472-9
7. O’Driscoll BR, Howard LS, Earis J, Mak V. British thoracic society guideline for oxygen use in adults in healthcare and emergency settings. Thorax. 2017;72(Suppl 1):i1–i90. doi:10.1136/thoraxjnl-2016-209729
8. Gehdoo RP, Kakroo AZ. Oxygen therapy devices. In: Understanding Anesthetic Equipment & Procedures: A Practical Approach. Jaypee Brothers Medical Publishers; 2021:238.
9. World Health Organization. Care, cleaning, disinfection and sterilization of oxygen concentrators and related interfaces. World Health Organization; 2024.
10. Zhao M, Tang Z. Finite element simulation of injection mold design integrating different structures of conformal cooling channels. Processes. 2025;13(1):234. doi:10.3390/pr13010234
11. Standardization IO for. ISO 13485:2016 medical devices — quality management systems — requirements for regulatory purposes. ISO; 2016. Available from: https://www.iso.org/standard/59752.html.
12. Standardization IO for. ISO 9001:2015 quality management systems — requirements. ISO; 2015. Available from: https://www.iso.org/standard/62085.html.
13. Tickner JA, Schettler T, Guidotti T, McCally M, Rossi M. Health risks posed by use of di-2-ethylhexyl phthalate (DEHP) in PVC medical devices: a critical review. Am J Ind Med. 2001;39(1):100–111. doi:10.1002/1097-0274(200101)39:1<100::AID-AJIM9>3.0.CO;2-Q
14. Latini G, Ferri M, Chiellini F. Materials degradation in PVC medical devices, DEHP leaching and neonatal outcomes. Curr Med Chem. 2010;17(26):2979–2989. doi:10.2174/092986710792064992
15. Standardization IO for. ISO 14971:2019 medical devices — application of risk management to medical devices. ISO; 2019. Available from: https://www.iso.org/standard/72704.html.
16. Standardization IO for. ISO 15001:2021 anaesthetic and respiratory equipment — compatibility with oxygen. ISO; 2021. Available from: https://www.iso.org/standard/75149.html.
17. Standardization IO for. ISO 15002:2023 flow-metering devices for connection to terminal units of medical gas pipeline systems. ISO; 2023. Available from: https://www.iso.org/standard/84789.html.
18. World Health Organization. Stability testing of active pharmaceutical ingredients and finished pharmaceutical products. World Health Organization; 2018.
19. Harmonisation IC for. ICH Q1A(R2): stability testing of new drug substances and products. ICH; 2003.
20. Standardization IO for. ISO 14040: environmental management — life cycle assessment — principles and framework. ISO; 2006.
21. Van Norman GA. Drugs, devices, and the FDA: part 2: an overview of approval processes: FDA approval of medical devices. JACC Basic Transl Sci. 2016;1(3):277–287. doi:10.1016/j.jacbts.2016.03.009
22. MacNeill AJ, Hopf H, Khanuja A, et al. Transforming the medical device industry: road map to a circular economy. Health Aff. 2020;39(12):2088–2097. doi:10.1377/hlthaff.2020.01118
23. Fathi R, Khajavi SH, Hosseini S, Faludi J, Bakker C. Circular economy for medical devices: barriers, opportunities and best practices from a design perspective. Resour Conserv Recycl. 2024;208:107719. doi:10.1016/j.resconrec.2024.107719
24. Acharya B, Marino M, Brooks AL, Eckelman MJ, Bilec MM. Advancing the circular economy of healthcare plastics: a systematic literature review. Resour Conserv Recycl. 2025;219:108317. doi:10.1016/j.resconrec.2025.108317
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.