Back to Journals » Psychology Research and Behavior Management » Volume 16
Depressive and Anxious Symptoms Increase with Problematic Technologies Use Among Adults: The Effects of Personal Factors Related to Health Behavior
Authors Méndez-López F ![]() , Oliván-Blázquez B, Domínguez García M, López-Del-Hoyo Y, Tamayo-Morales O
, Oliván-Blázquez B, Domínguez García M, López-Del-Hoyo Y, Tamayo-Morales O ![]() , Magallón-Botaya R
, Magallón-Botaya R
Received 10 March 2023
Accepted for publication 12 May 2023
Published 4 July 2023 Volume 2023:16 Pages 2499—2515
DOI https://doi.org/10.2147/PRBM.S412013
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Fátima Méndez-López,1,2 Bárbara Oliván-Blázquez,1– 3 Marta Domínguez García,1,2,4 Yolanda López-Del-Hoyo,2,3,5 Olaya Tamayo-Morales,2,6 Rosa Magallón-Botaya1,2,7
1Primary Care Research Unit (GAIAP), Health Research Institute of Aragon (IISA), Zaragoza, Spain; 2Network for Research on Chronicity, Primary Care and Health Promotion (RICAPPS), Health Institute Carlos III, Madrid, Spain; 3Department of Psychology and Sociology, University of Zaragoza, Zaragoza, Spain; 4Aragonese Healthcare Service (SALUD), Zaragoza, Spain; 5Mental Health Research in Primary Care Unit, Health Research Institute of Aragon (IISA), Zaragoza, Spain; 6Primary Care Research Unit of Salamanca (APISAL), Institute of Biomedical Research of Salamanca (IBSAL), Salamanca, Spain; 7Department of Medicine, Psychiatry and Dermatology, University of Zaragoza, Zaragoza, Spain
Correspondence: Bárbara Oliván-Blázquez, Primary care research unit, Health Research Institute of Aragon, 13 San Juan Bosco AVE FL 0, Zaragoza, 50009, Spain, Tel +34 976 50 65 78, Email [email protected]
Background: Depression and anxiety disorders are a significant and growing health problem that has a significant impact on psychosocial functioning and quality of life. The onset and severity of mental health problems have been related to various biological, psychosocial, and behavioral variables.
Purpose: The purpose of this study was to explore the association among the severity of depression and anxiety, problematic information and communications technology (ICT) use, and some related personal factors with health behavior among adults. It also analyzes the moderating role of personal factors in the relationship between the problematic use of ICT and anxiety and depression.
Patients and Methods: Descriptive, bivariate, multivariate and moderation analyzes of data from 391 participants of 35– 74 years old in primary health care centers located in Aragón (Spain) were performed between July 2021 and July 2022. The primary outcome was the severity of depressive and anxious symptoms as continuous variable.
Results: Low sense of coherence (β = − 0.058; p = 0.043), low self-esteem (β = − 0.171; p=0.002), and low self-efficacy (β = − 0.122; p= 0.001), are predictors of having more severe depressive symptoms. Furthermore, low self-esteem (β = − 0.120; p= 0.012), low self-efficacy (β = − 0.092; p=0.004), and high problematic use of ICT (β = 0.169; p = 0.001), are predictors of having more severe anxiety symptoms. Moderation analyzes were significant in the effect of self-efficacy (b = − 0.040, p=0.001) and resilience (b = − 0.024, p=0.033) on the relationship between problematic ICT use and anxiety.
Conclusion: The problematic use of ICT and personal factors are related to depressive and anxiety symptoms. The interrelationship between problematic ICT use, personal factors, and depression needs to be further explored.
Keywords: depression, anxiety, problematic information and communication technologies use, technology addiction, personal health factors
Introduction
Affective disorders are a significant and growing health problem with significant morbidity worldwide.1 Currently, affective disorders have a significant impact on the quality of life of 246 million people with major depressive disorders and 374 million people with anxiety disorders worldwide.2 These disorders are more prevalent in women than in men; for instance, depression affects 5.1% of women vs 3.6% of men, and anxiety affects 4.6% of women vs 2.6% of men.3
These syndromes are characterized by a clinically significant alteration in the cognition, emotional regulation, or behavior of an individual.4 Moreover, they are the result of complex interactions between social, psychological, and biological factors and are generally associated with significant distress or impairment in personal, family, social, educational, occupational, or other important areas of functioning.5 The onset and severity of mental health problems such as depression or anxiety have been related to the addiction or problematic use of new technologies.6–8 The advent of information and communications technology (ICT) has led to numerous positive changes in all facets of human life (business, education, and health).9 However, its excessive use may lead to addictive behavior forming a global phenomenon of increasing magnitude.10 Despite being a behavioral addiction, excessive internet use has not been recognized as a disorder by the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) or the International Classification of Diseases (ICD-11).11 However, internet gambling and internet gaming disorders are found in the behavioral addictive disorders of the DSM-5-TR,12 and in the ICD-11.13 Nowadays in Spain, 3.5% of the population between 15–64 years old presents a compulsive use of the Internet, and 2.5% between 35–44 years old.14
According to the World Health Organization people who make excessive use of the Internet have high comorbidity with many mental health disorders (depression, anxiety).10 Current evidence shows a strong correlation between the problematic use of information and communications technology and mental health,15 quality of life,16 and stress level.17 More specifically, a recent study carried out on students from Bangladesh exposes how addiction to smartphones, social networks, depression and anxiety are risk factors for Internet addiction.18 Also, a recent study highlighted the relationship between anxiety and problematic Internet use, reporting seven types of anxiety caused by excessive Internet use (Internet terminology anxiety, Internet time delay anxiety, General Internet failure anxiety, Usage anxiety, Experience anxiety, Environment and attraction anxiety, and Net Search anxiety).19 Depression has been reported to be associated with Internet addiction in a 12-month follow-up cohort in a Chinese student population.20 In this study, baseline IA status significantly predicted probable incident of mild or major depression (CESD ≥16) (aOR = 1.57, 95% CI = 1.18, 2.09) at follow-up.20
Furthermore, some personal factors are connected to the abuse of excessive use of technologies and are related to mental health.21 Some of these factors are resilience,22 self-efficacy,23 sense of coherence,24 self-esteem,25 and personality characteristics.26 First, resilience represents a positive adaptation to circumstances of significant adversity, such as misfortunes and adverse life events.22 Low resilience has been associated with high levels of depression, hopelessness, anxiety, and mortality.27,28 High resilience has been shown to be an effective way to reduce addictive behavior on the Internet.29,30 Second, self-efficacy is represented as a feeling of confidence in one’s abilities to handle certain stressors in life.23 Self-efficacy plays an important role in the quality of life of people with depression. Increased self-efficacy beliefs have also been linked with more effective emotion regulation and psychosocial functioning.31,32 A previous study also found a negative correlation between self-control and internet addiction.33,34 Third, the sense of coherence is defined as values the personal disposition toward the values of vital experiences.24 Some evidence provides a positive relationship of a greater sense of coherence with the decrease in depressive and anxiety symptoms.35 In a study conducted on young people with a lower level of sense of coherence showed the highest intensity of the problematic use of internet, while those with the highest level of the sense of coherence achieved the lowest results in the problematic use of internet.36 Fourth, self-esteem is defined as feelings toward oneself, which can be positive or negative, and is built through an evaluation of one’s own characteristics.25 Adults who have high global self-esteem are more likely to have greater physical, mental, occupational, and social well-being. Low self-esteem is related, for example, to emotional problems, substance abuse, eating disorders, and behavioral addictions such as ICT.37,38 Finally, among the personality characteristics that affect mental health and addictions are introversion, low conscientiousness, neuroticism, low agreeableness, and low openness.26 People who scored much higher in neuroticism and lower in extraversion and conscientiousness had greater anxiety and depression symptoms.39 Addictions to new technologies are related to adults with the personality traits of neuroticism, openness, and low conscientiousness.21,40 These personal factors are framed around Antonovsky’s Salutogenic approach.41 This theory focuses on its objective to improve the capacity of the participants mental health and well-being by increasing their awareness, confidence, and ability to use their personal factors related to health behavior.42
Currently, there is little scientific evidence available that allows us to know patterns of personal factors and problematic use of ICT and how they affect the severity of depression and anxiety among adults. This type of research in the young population has been centralized, being a scarcely investigated issue in adults. We cannot forget that approximately 85% of the European population older than 35 makes daily use of information and communication technologies,43 and thereby their potential risk of excessive and addictive use of them. Knowing the psychosocial and psychobiological risk factors that predispose people to this problematic use of ICTs should be the key to preventive identification and early care measures among people at risk and their families. Considering the previous associations between problematic ICT use and mental health, this study aims to analyze the association among the severity of depression and anxiety, problematic ICT use, and some related personal factors with health behavior (resilience self-efficacy, sense of coherence, self-esteem, personality characteristics). It also aims to analyze the moderating role of personal factors in the relationship between the problematic use of ICT and anxiety and depression. This effect of personal factors has been demonstrated in studies with the adolescent population and young adults, in which they show how self-efficacy and resilience influence the problematic use of smartphones and anxiety in university students.44,45 Therefore, our secondary hypothesis is that the relationship between the problematic use of ICT and anxiety and depression will change according to the value of the different moderators, such as self-efficacy, resilience, personality traits, sense of coherence, and self-esteem.
Materials and Methods
Study Design
This research project was a cross-sectional study conducted between July 2021 and July 2022 in primary health care centers located in Aragón, in northern Spain. This study was registered with the ISRCTN Registry before commencement (ISRCTN12820058).
Sample Size
The sample size was computed using the formula46 for the population estimation of the most prevalent affective disorders in primary care (anxiety and depression). To calculate the sample size, we used the data obtained in Santomauro et al study.2 We used the prevalence of the most frequent affective disorders and addictions in primary care (anxiety, depression) as the main variable, being 3.1% of major depression and 4.8% of anxiety disorders. Accepting a risk of 0.05 and a margin of error 3% units, the total sample size required was 290, with consideration of having a possible 30% withdrawal rate (Supplementary A).
Recruitment and Participants
The inclusion criteria were participants of 35–74 years old who understood written and spoken Spanish and provided consent to participate in the study voluntarily. Based on national clinical data from primary health care, the decade between 30 and 40 years of age is the most common stage of depression and anxiety. These problems are more common in women than in males at this age (depression: 4.2% vs 2.0%; anxiety: 10% vs 5.7%, respectively).47 Furthermore, at this age, these affective illnesses have a significant impact on people who are often at the age of full job, economic, and family activities.48 The prevalence of these illnesses increases with age, with a minor decrease after the age of 75 years, and the pattern of higher prevalence in women than in males remains (depression: 12.2% vs 4.8%; anxiety: 11.3% vs 5.0%, respectively).47
Exclusion criteria were (A) suffering from a terminal illness (B) being institutionalized at the time of the appointment, (C) difficulty to participate due to cognitive dysfunction, dementia, or any serious disease that may seriously interfere with the patient’s participation in the study. Potential participants were selected by random sampling following stratification criteria from the lists of PHC centers to which they were assigned. In Spain, the entire population is assigned to a health center in the area where they reside, and around 85% of the population opts for public primary health care over private health.49 Potential participants were recruited by stratified selection using age, sex, and proportion of rural/urban with respect to the National Institute of Statistics data from the census of Aragon 2021. This stratification was conducted with the intention of providing the greatest variability to the sample and reaching a maximum representativeness for the population. The study was conducted at PHC centers, in one rural area and in one urban area. The rural center sampled was in towns with a population less than 2000 inhabitants. These potential participants were contacted by letter or telephone, and those interested in participating made an appointment at their usual health center to fill out the questionnaires. At the end of the study, 400 patients from primary health care centers were recruited for the study, comfortably exceeding the sample size requirement. The study adhered to the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines (Supplementary B).
Outcomes and Measures
Sociodemographic data: we collected information on gender (woman, man), age, municipality classification (urban, rural), marital status (without a partner: single, separated, divorced, widower or widow; and with a partner: married or living with a partner), education (none or primary and secondary or tertiary), occupation (working: active and not working: unemployment, homemaker, unpaid work, student, pensioner, sick leave, temporary job disability, permanent job disability, and other situations) through an ad hoc questionnaire.
The primary outcome was the severity of depressive and anxious symptoms as continuous variables.
The severity of depression was measured using the Patient Health Questionnaire-9 (PHQ-9, Spanish version).50 This scale measures the degree of depression in the past two weeks. The severity levels included no depression (0–4), mild depression (5–9), moderate depression (10–14), moderately severe depression (15–19), and severe depression (20–27). The validated Spanish version has a Cronbach’s alpha value (α) of 0.80.51 The internal consistency of PHQ-9 in our sample was 0.83.
Anxious symptoms were measured using the Generalized Anxiety Disorder-7 (GAD-7, Spanish version).52 It consists of seven multiple-choice questions, with each response being graded on a scale ranging from 0 to 3. Each item describes one of the typical symptoms of generalized anxiety disorders over the last two weeks. The severity levels included no anxiety (0–4), mild anxiety (5–9), moderate anxiety (10–14), and severe anxiety (15–21) in the original study. The validated Spanish version has a Cronbach’s alpha value (α) of 0.93.53 GAD-7 had good internal consistency (Cronbach’s alpha = 0.84).
Secondary outcomes were problematic information and communications technologies use, and some related personal factors with health behavior (resilience self-efficacy, sense of coherence, self-esteem, personality characteristics).
Problems related to the use of the Internet, mobile phones, video games, instant messaging, and social networks were measured using the MULTICAGE-ICT Questionnaire.16 Composed of 20 total items distributed in five scales (Internet; Mobile Phone; Video Games; Instant Messaging; Social Networks). In each scale, it addresses item 1, the estimation of excess in temporary dedication; item 2, estimation of significant others; item 3, difficulty not performing the behavior; and item 4, difficulties in voluntarily interrupting the behavior. Higher scores indicate higher use/abuse of information and communications technologies. The validated Spanish version has a Cronbach’s alpha value (α) of 0.93.16 The internal consistency of the in our sample was good (α =0.85).
Self-efficacy was assessed using the General Self-Efficacy Scale-12 (GSES-12, Spanish version).23 This scale evaluates perceived global self-efficacy as a feeling of confidence in one’s abilities to adequately handle certain stressors in life. The final score on the questionnaire was the sum of the responses obtained on each item (range 12–60), and the highest scores indicated the highest level of self-efficacy. The validated Spanish version has a Cronbach’s alpha value (α) of 0.69.54 The internal consistency of the in our sample was acceptable (α =0.75).
Resilience was measured using the Connor-Davidson Resilience Scale (CD-RISC-10, Spanish version).22 This scale evaluates resilience as a positive adaptation to circumstances of significant adversity, such as misfortunes and tragic situations in life. The final score on the questionnaire was the sum of the responses obtained for each item (range 0–40), and the highest scores indicated the highest level of resilience. The validated Spanish version has a Cronbach’s alpha value (α) of 0.85.55 The internal consistency of the in our sample was 0.86.
Personality characteristics were assessed using the Big Five Inventory-10 (BFI-10, Spanish version).56 The questionnaire measures the five factors of personality from the five factors model (each factor entails two items). Extraversion (Extraverts engage actively with others to earn friendship, admiration, power, status, excitement, and romance; Introverts conserve their energy and do not work as hard to earn these social rewards). Agreeableness (High scores have a great deal of empathy and tend to get pleasure out of serving and taking care of others; low scorers are often described as hostile, competitive, and antagonist). Conscientiousness (High scorers are organized and determined; low scorers are impulsive and easily side-tracked). Neuroticism (High scorers are more likely to react to a situation with fear, anger, sadness, and the like. Low scorers are more likely to brush off their misfortune and move on). Openness (High scorers tend to be creative, adventurous, and intellectual; low scorers tend to be practical, conventional, and focused on concrete information). The validated Spanish version has a Cronbach’s alpha value (α) of 0.78.26 The internal consistency of the in our sample was acceptable (α =0.72).
The sense of coherence was measured using the Sense of coherence scale (SOC-13, Spanish version).24 This scale evaluates the sense of coherence as values the personal disposition toward the value of vital experiences. It also measures understandability, manageability and meaning. Higher scores (after flipping the flipped items) (range 13–91) indicate a greater sense of coherence. The validated Spanish version has a Cronbach’s alpha value (α) of 0.83.57 The internal consistency of the in our sample was acceptable (α =0.75).
Self-esteem was measured using the Rosenberg Self-Esteem scale (RSES, Spanish version).25 Self-esteem is defined as feelings toward oneself, which can be positive or negative, and is built through an evaluation of one’s own characteristics. Scores below 25 points are treated as significant low self-esteem issues. The validated Spanish version has a Cronbach’s alpha value (α) of 0.85.58 The internal consistency of the in our sample was acceptable (α = 0.79).
Statistical Analysis
The normal distribution of the results was verified using the Kolmogorov–Smirnov test. A descriptive analysis (frequencies (n) and percentages (%) for categorical variables; mean (M) and standard deviation (SD) for continuous variables) was performed to determine the characteristics of the sample. Second, to analyze the associations between the anxiety score (GAD-7) and depression (PHQ-9) and all variables, correlations were performed using the Pearson correlation coefficient (Pearson’s r for the relationship between two continuous variables and Pearson’s Point-Biserial Correlation rpb for the relationship between a continuous variable and a dichotomous variable).59 Third, multicollinearity (VIF and tolerance values) were tested, and multiple linear regression was performed using a stepwise method to obtain a better fit result to the statistical analysis.60 This stepwise regression simply repeats the multiple regression, each time removing the least correlated variable. All of the covariates (socio-demographic, problematic ICT use, and some related personal factors with health behavior variables) were introduced in the regression models, to control for the influence of the various independent variables.61 The sociodemographic variables were categorized into two categories to be included in the multiple regression.
Finally, several hierarchical multiple regressions analyzes were conducted to test whether depression and anxiety are associated with the problematic use of ICT and personal factors, and more specifically whether personal factors (CD-RISC-10, BFI-10, GSES-12, SOC-13, RSES) moderate the relationship between the problematic use of ICT (MULTICAGE-ICT) and depression (PHQ-9) and anxiety (GAD-7). In the first steps, two variables were included as: problematic use of ICT and one of the personal factors. If they accounted for a significant amount of variance in PHQ-9 or GAD-7, an interaction term between them was created. Next, the interaction term between them was added to the regression model; if it accounted for a significant proportion of PHQ-9 or GAD-7, we examined the interaction plot to establish the direction of the relationship.
Moderation analyzes were performed using Hayes’s PROCESS macro (v. 4.2)62 for the IBM SPSS Statistics software (version 25.0).63 Bootstrap resampling (10.000 samples) was used to estimate 95% confidence intervals. Given that heteroscedasticity is common in cross-sectional data, all analyzes included a correction for heteroscedasticity (HC0).64 The Johnson-Neyman technique was used to compute the range of significance and simple slopes for the interaction analyzes.62 We reported unstandardized regression coefficients; all analyzes were two-tailed and used conventional significance thresholds (α = 0.05). All analyzes were performed using IBM SPSS Statistics software (version 25.0).63 Additionally, to visualize the moderating associations, simple regression slopes at three levels (mean minus one standard deviation, mean, and mean plus one standard deviation) were illustrated as moderator variables (personal factors), with the predictor (problematic ICT use) as the independent variable and depressive and anxious symptoms as dependent variables (Figure 1).
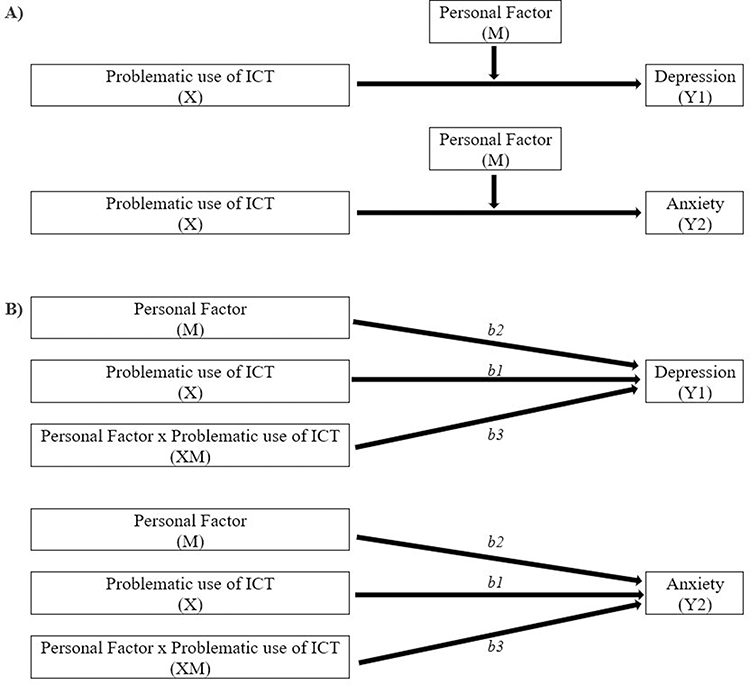 |
Figure 1 Proposed model depicted conceptually (A) and statistically (B). Abbreviations: B, unstandardized regression coefficient; M, moderator variable; X, independent variable; XM, interaction between independent and moderator variable; Y, dependent variable. |
Results
A total of 400 participants were included. Due to the lack of data from the self-administered questionnaires, 9 participants were removed from the final analysis. Of the 391 participants, 228 were females (58.31%) and 163 were males (41.69%), and the mean age of all participants was 54.57±10.72 years (range 35–74). All sociodemographic and personal factors characterization of the sample are described in Table 1.
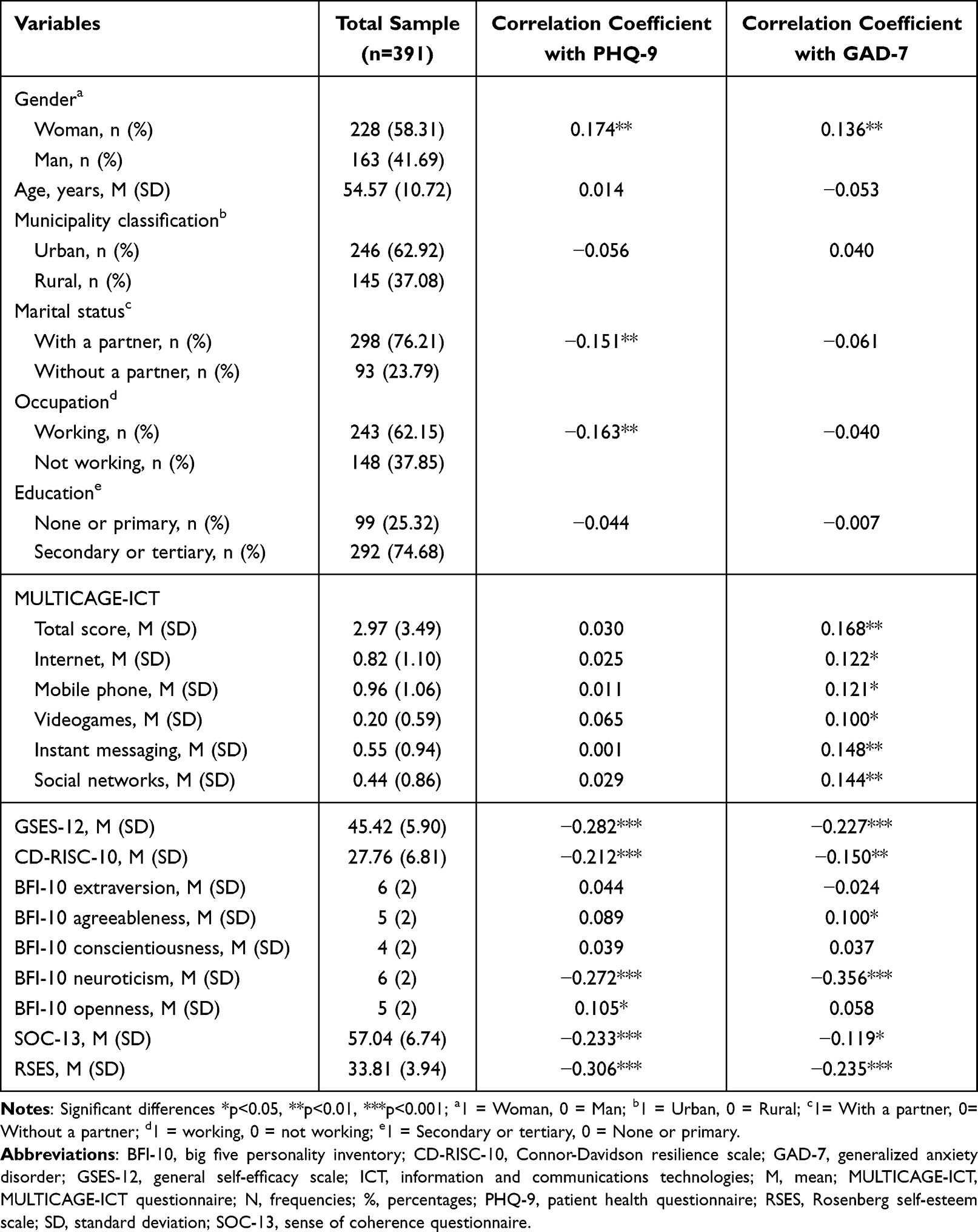 |
Table 1 Descriptive and Bivariate Analysis of Depressive and Anxious Symptoms, Sociodemographic Characteristics, Problematic Use of ICT, and Personal Factors of the Sample |
Bivariate Correlations of Depressive and Anxious Symptoms, Sociodemographic, Problematic Use of ICT, and Personal Factors
Table 1 also shows the results of the bivariate analysis of depressive and anxious symptoms, sociodemographic variables, problematic use of ICT, and personal factors.
Table 1 shows the results of the bivariate analysis of depressive and anxious symptomatology, sociodemographic variables, problematic use of ICT, and personal factors. The relationship between gender and the level of depression (0.174; p=0.001), and anxiety (0.163; p=0.007) was significant. Furthermore, our data revealed a significant relationship between the level of PHQ-9 and marital status (0.151; p=0.003), and occupation (0.163; p=0.001). A negative association between the problematic use of ICT and GAD-7 was found (0.168; p=0.001). No relationship was found between PHQ-9 and MULTICAGE-ICT variables.
The relationship between the level of depression and different personal factors was significant: self-efficacy (−0.282, p < 0.001), resilience (−0.212, p < 0.001), neuroticism (−0.272, p < 0.001), sense of coherence (−0.233, p < 0.001), and self-esteem (−0.306, p < 0.001). Additionally, Table 1 shows a significant relationship between the level of anxiety and personal factors such as self-efficacy (−0.227, p < 0.001), resilience (−0.150, p = 0.003), neuroticism (−0.356, p < 0.001), sense of coherence (−0.119, p < 0.001), self-esteem (−0.235, p < 0.001).
Regression Model of Depressive and Anxious Symptoms, Problematic Use of ICT, and Personal Factors
Multiple regression analysis was conducted to test whether depression and anxiety are associated with the problematic use of ICT and personal factors. Regarding the multivariate analysis, once the stepwise regression eliminated the weakest correlated variables, the remaining variables are shown in Table 2 and Table 3. Excluded variables from the multivariate analysis model of the PHQ-9 and GAD-7 scores can be viewed in the Supplementary C.
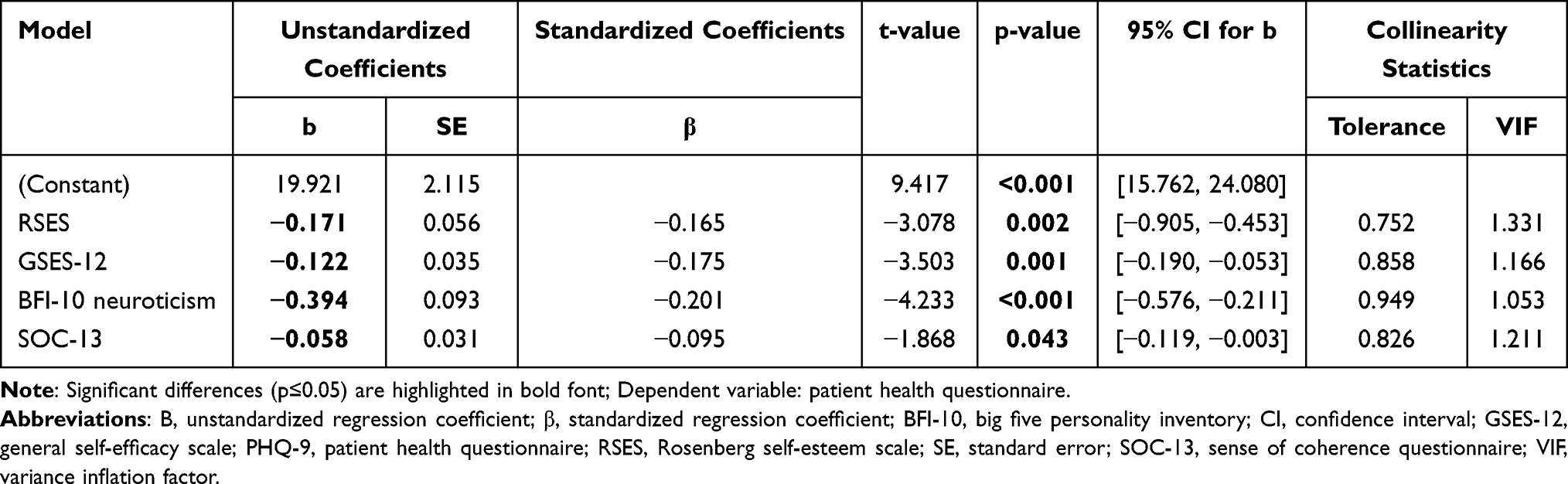 |
Table 2 Regression Model of the PHQ-9 Scores with MULTICAGE-ICT and Personal Factors as Predictors |
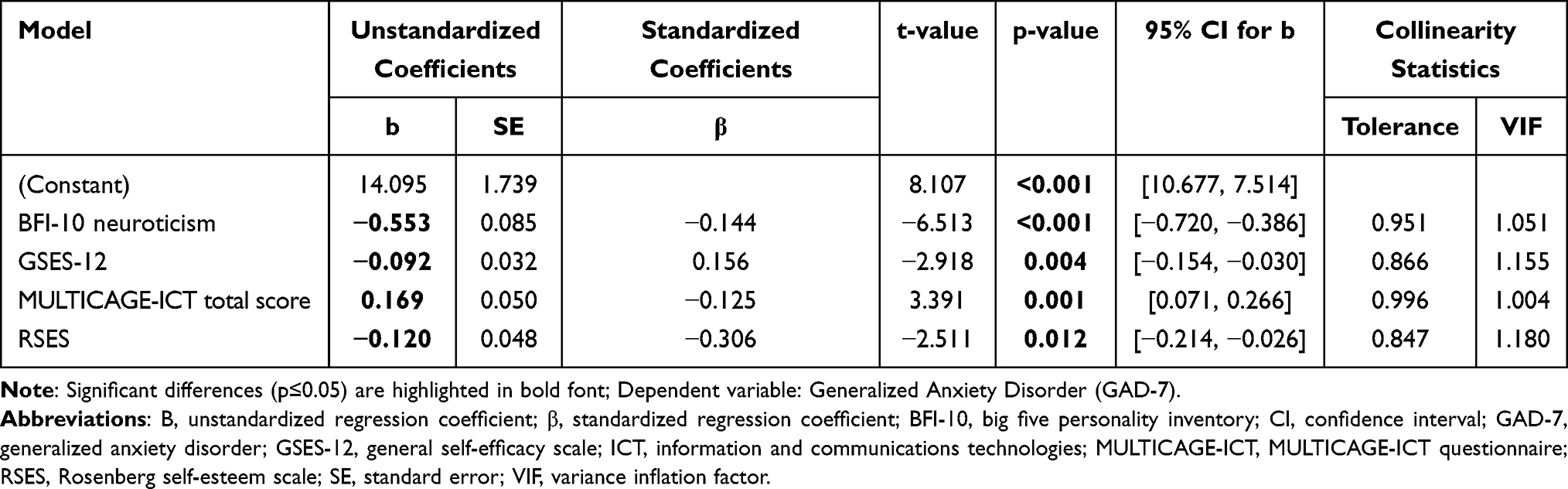 |
Table 3 Regression Model of the GAD-7 Scores with MULTICAGE-ICT and Personal Factors as Predictors |
Low sense of coherence (β = - 0.058; p = 0.043), low self-esteem (β = −0.171; p=0.002), low self-efficacy (β = −0.122; p= 0.001), and low neuroticism (β = −0.394; p< 0.001), are predictors of having more severe depressive symptoms. This model explains 17% of the overall variance [R2 adjusted = 0.169, F (1382) = 20.667, p< 0.001].
Furthermore, low self-esteem (β = −0.120; p= 0.012), low self-efficacy (β = −0.092; p=0.004), low neuroticism (β = −0.553; p< 0.001), and high problematic use of ICT (β = 0.169; p = 0.001), are predictors of having more severe anxious symptoms. This model explains 19% of the overall variance [R2 adjusted = 0.189, F (1383) = 23.586, p< 0.001].
Moderation Roles of Personal Factors Between Problematic Use of ICT and Depression or Anxiety
Several hierarchical multiple regressions analyzes were conducted to test whether personal factors (resilience (CD-RISC-10), personality (BFI-10), self-efficacy (GSES-12), sense of coherence (SOC), self-esteem (RSES)) moderate the relationship between the problematic use of ICT (MULTICAGE-ICT) and depression (PHQ-9) and anxiety (GAD-7). In each model, MULTICAGE-ICT and one of the significant personal factors from the bivariate analysis were included. Next, as all the models were significant, the interaction term between them was created and added to the regression model. Regarding depressive symptomatology, only the interaction between self-efficacy and problematic use of ICT, was significant [ΔR2 = 0.009, ΔF (1, 387) = 3.887, p =0.049], as shown in Table 4. However, the effect only showed a tendency b = -0.022, t (387) = -1.860, p = 0.063.
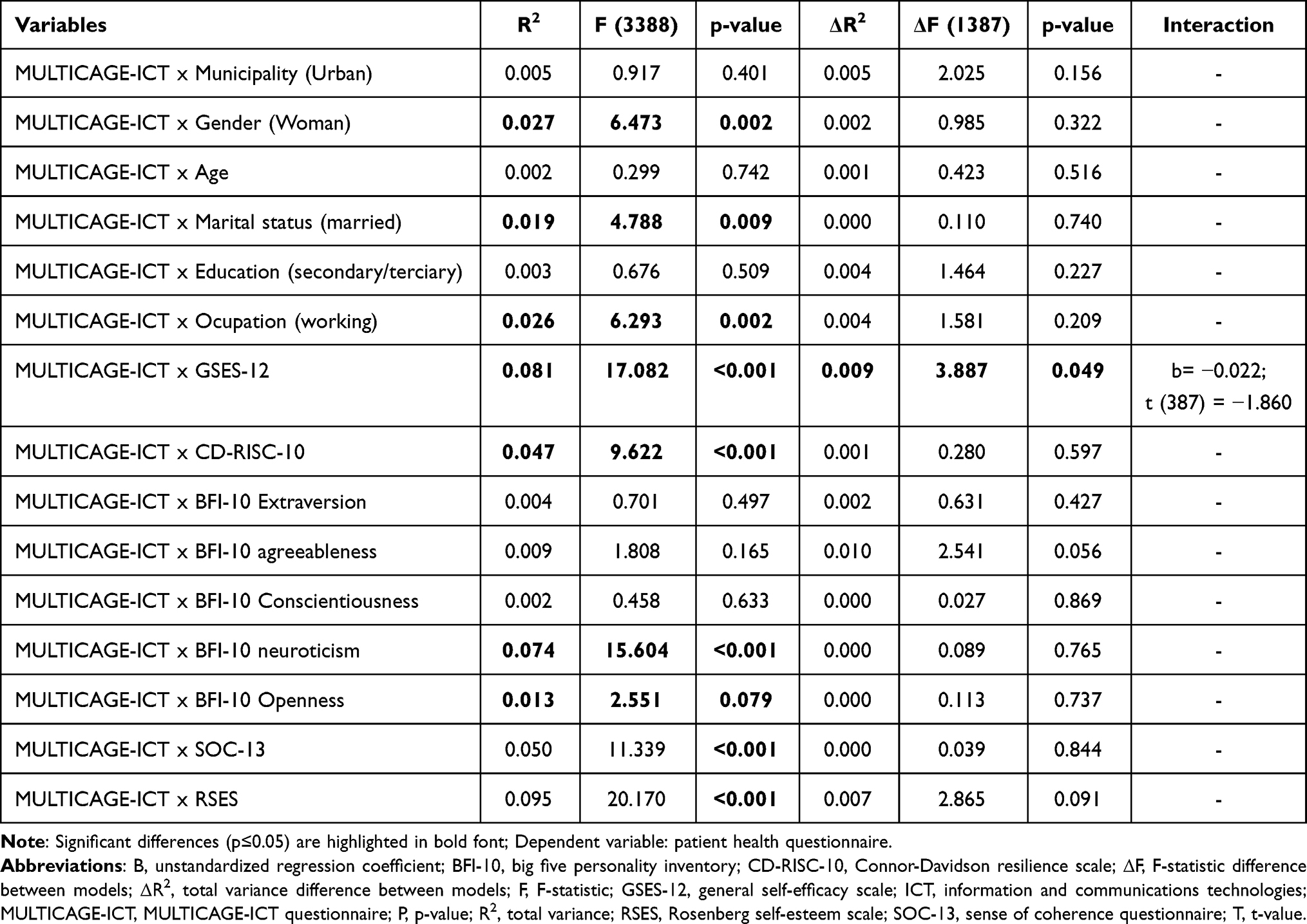 |
Table 4 Linear Regression Analysis of Personal Factors, Problematic Use of ICT, and the Interaction Between Them on Depression (PHQ-9) |
For anxious symptomatology, the interaction between self-efficacy and problematic use of ICT [ΔR2 = 0.034, ΔF (1, 387) = 14.744, p < 0.001], and resilience and problematic use of ICT were significant [ΔR2 = 0.015, ΔF (1, 387) = 6.425, p = 0.012]. The effect of the interaction was significant for both models, (self-efficacy; b = −0.040, p=0.001) and (resilience; b = −0.024, p=0.033) (Table 5).
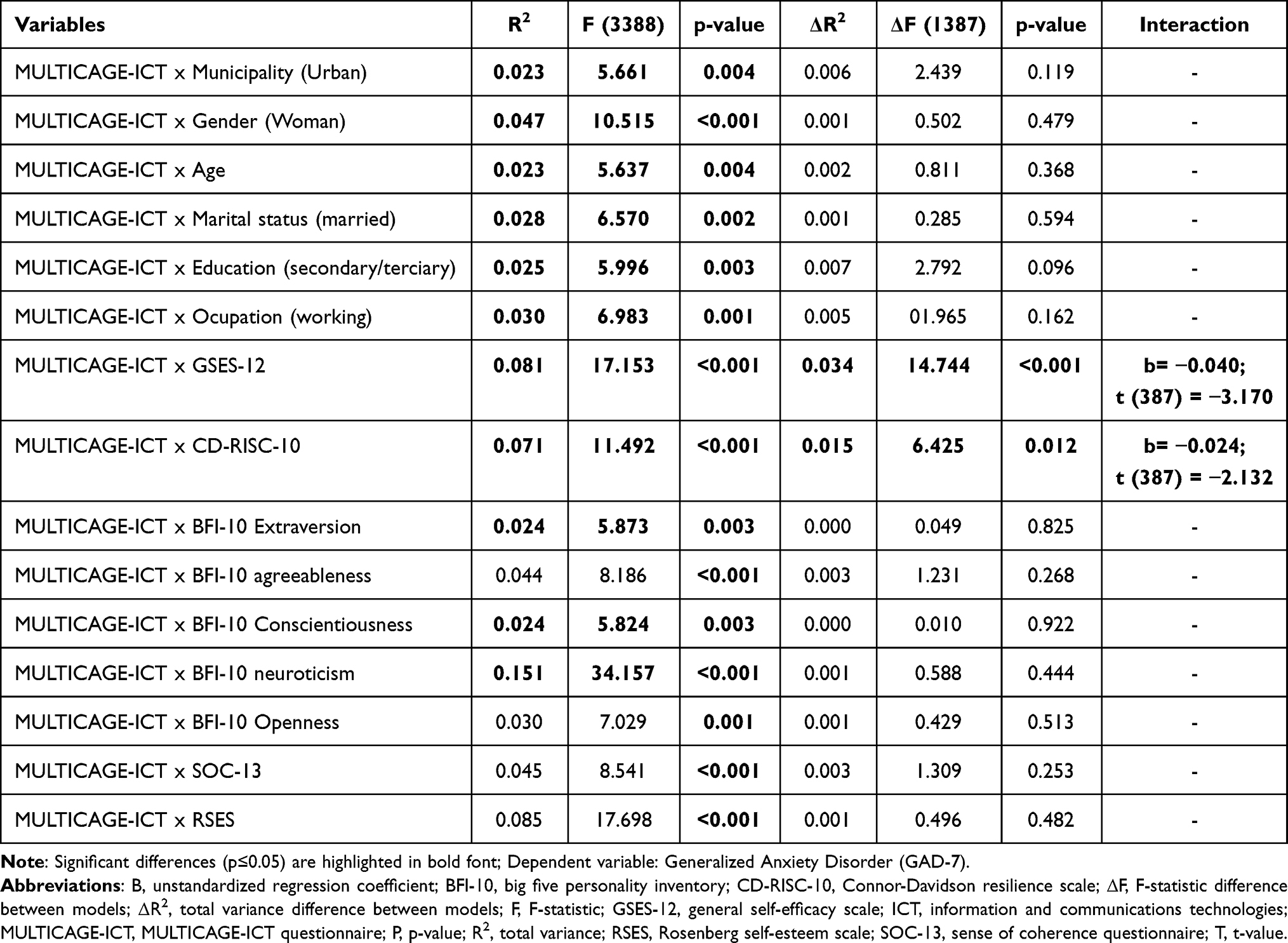 |
Table 5 Linear Regression Analysis of Personal Factors, Problematic Use of ICT, and the Interaction Between Them on Anxiety (GAD-7) |
Additionally, the moderation effects were examined to establish the direction of the different relationships. As shown in Figure 2, the negative relationship between problematic ICT use and higher depression was stronger in participants with lower self-efficacy (b = 0.1805, p=0.080). However, this is not a statistically significant relationship.
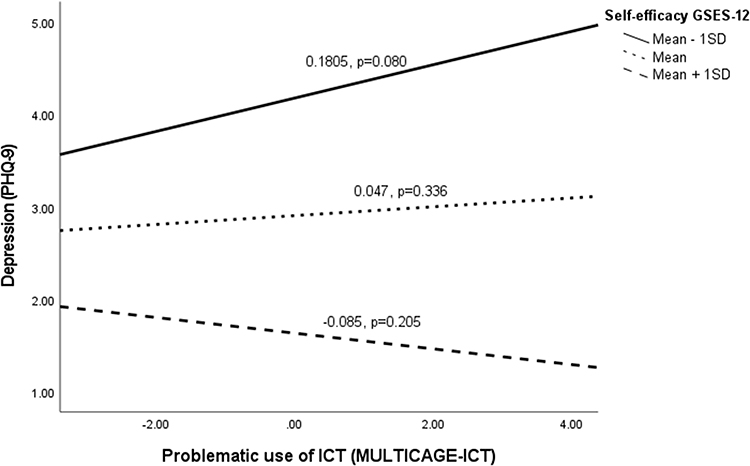 |
Figure 2 The moderating effect of self-efficacy in the relationship between the problematic use of ICT and depression. Abbreviations: GSES-12, general self-efficacy scale ICT, information and communications technologies; P, p-value; PHQ-9, patient health questionnaire; SD, standard deviation. |
The negative relationship between problematic ICT use and higher anxiety was stronger in participants with lower self-efficacy (b = 0.434, p<0.001) (Figure 3). While in Figure 4, it is observed in the same way that the relationship is stronger in participants with less resilience (b = 0.382, p=0.001).
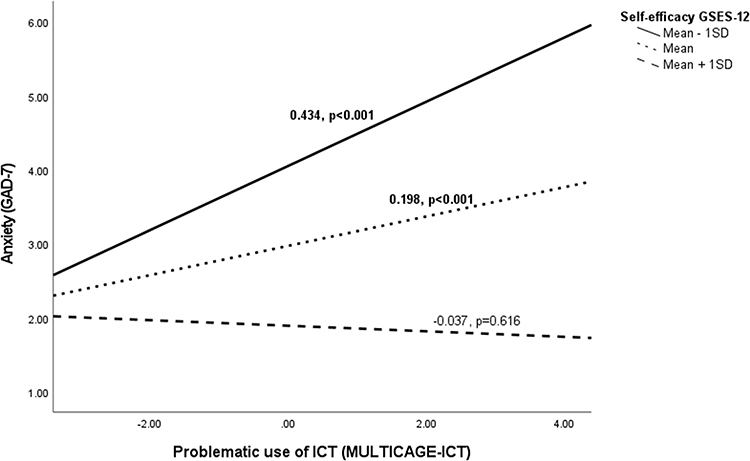 |
Figure 3 The moderating effect of self-efficacy in the relationship between the problematic use of ICT and anxiety. Abbreviations: GAD-7, generalized anxiety disorder; GSES-12, general self-efficacy scale; ICT, information and communications technologies; P, p-value; SD, standard deviation. |
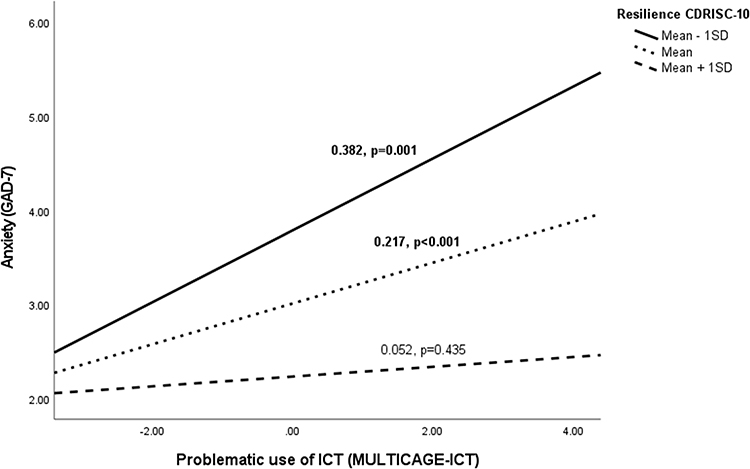 |
Figure 4 The moderating effect of resilience in the relationship between the problematic use of ICT and anxiety. Abbreviations: CD-RISC-10, Connor-Davidson resilience scale; GAD-7, generalized anxiety disorder; ICT, information and communications technologies; P, p-value; SD, standard deviation. |
Discussion
This study analyzed the association among the severity of depression and anxiety, problematic ICT use, and some related personal factors with health behavior (resilience self-efficacy, sense of coherence, self-esteem, personality characteristics). The depressive symptoms were statistically significant in relation to woman gender, marital status without a partner and employment situation without work. Additionally, depression was associated with lower scores in self-efficacy, resilience, sense of coherence, self-esteem, and neuroticism. Individuals with more anxiety symptoms were woman with lower scores in self-efficacy, resilience, sense of coherence, self-esteem, and neuroticism. Furthermore, data from multivariate analysis showed that having a low sense of coherence, low self-esteem, low self-efficacy, and low neuroticism are predictors of having more severe depressive symptoms. However, high problematic use of ICT, low self-esteem, low self-efficacy, and low neuroticism are predictors of having more severe anxiety symptoms. As we obtained in our study, it has been widely demonstrated that the sense of coherence performs a protective function against depressive and anxiety symptoms.65,66 In line with other studies, self-efficacy is associated with better mental health and is negatively correlated with depression. Higher self-efficacy scores allow better functionality and quality of life for people with depressive symptoms, allowing better control of their emotional state.31 Regarding the effect of self-esteem, as is already known from the existing evidence, low self-esteem is a prospective risk factor for depression.67 Finally, currently evidence shows that people who scored much higher in neuroticism had greater anxiety and depression symptoms.39 However, in our study, the neuroticism score was inversely correlated with depression and anxiety. These results may be due to the characteristics of our sample. The relationship between neuroticism with depression and anxiety is well evidenced in the young and adolescent population, and our study works in a different age range.68
Additionally, anxious symptoms were statistically significant related to a higher score on the problematic use of internet, mobile phone, videogames, instant messaging, and social networks. Findings from the systematic review demonstrated that problematic social networking site use was correlated with depression (seven studies), and anxiety (six studies).69 The association between the problematic use of the Internet and anxiety has been found in recent studies with older adults,70 and on problematic use of smartphones in young adults.71 However, people with more depressive symptoms have a higher score for the problematic use of ICT, but the results are not statistically significant. This relationship has been verified in various studies in the young population.72 However, there are also studies at the same age that, like us, have not obtained significant results.73 In the results of a recent investigation of 3600 individuals in the United States,74 it is observed that 75% recognized that they lose track of time when on their smartphone. In this study, it was estimated how this problematic use of smartphones affected depression, anxiety, and stress in individuals. Additionally, Taylor et al 2020,75 through structural equation models verified the relationship between the problematic use of smartphones, the severity of social anxiety symptoms and behaviors and attitudes related to technology.
Furthermore, this study also analyzed whether personal factors moderate the relationship between the problematic use of ICT and affective mental health (depression or anxiety). The relationship between problematic ICT use, self-efficacy and depression was significant, but its moderation was not. In other words, in our study we cannot observe that the relationship between the problematic use of ICTs and depression changes in a statistically significant way according to the value of the different personal factors. However, this moderation was significant in the effect of self-efficacy and resilience on the relationship between problematic ICT use and anxiety. This means that in this sample, the relationship between the problematic use of ICTs and anxiety does change according to the value of the different moderators, such as self-efficacy and resilience. This effect of self-efficacy and resilience has been shown in studies with the adolescent population and young adults. Some studies show how self-efficacy influences on the problematic use of smartphones and anxiety in university students.44,45
However, there is not much existing evidence on the moderating effect of resilience and self-efficacy on this relationship in adult population, so our conclusions represent new evidence on this topic. In other studies, it has already been confirmed that other personal factors such as dispositional confidence and self-control moderate the relationship between anxiety and the problematic use of ICT.71,76 Furthermore, some studies have measured the mediator role of different personal factors (procrastination, self-control) in the relationship between smartphone addiction, and depression and anxiety.77
The interrelationship between problematic ICT use, personal factors, and affective mental health (depression or anxiety) needs to be further explored. More studies of this type are needed in larger sample sizes where there may be more power to detect moderation effects by testing other types of analysis (mediation analysis) and/or using longitudinal data. Due to the moderating role of self-efficacy and resilience in our findings, this model should be applied to provide a possible framework for developing health education and health-related inventions. Effective strategies must be taken to reduce psychological dependence on the use of new technologies. Improvement in self-efficacy might help reduce symptoms of anxiety and depression in the population.
Strengths
This type of research, in which various topics on addictions and problematic uses of new technologies and personal factors (self-efficacy, resilience, sense of coherence, self-esteem and personality characteristics) in their association with mental health, are jointly analyzed.
There is little scientific evidence available that allows knowing patterns of personal factors and problematic use of ICT and how they affect the severity of depression and anxiety, particularly in the adult population. It is true that the young population is currently the most prevalent in the use of new technologies. However, we cannot forget that new technologies have appeared in the life of the global population.43 The abusive use of information and communication technologies occurs at all ages and in very different cultural spheres, forming a global phenomenon of increasing magnitude.10,16 Therefore, our study represents a small advance in this new evidence. In addition, the profile of the participants corresponded to the profile in the most common age of depression and anxiety, and in which affective diseases have a significant impact on people who are often of the age of work activities, economic and complete family.48
Limitations
Several limitations must be considered in this study. First, the data were collected at a single point in time, rather than longitudinally, which limited the ability to draw causal inferences or determine the direction of causal relationships. Future prospective studies with a large sample size are warranted to validate our findings.78 Second, the survey was carried out with two types of questionnaires that present different limitations (on the one hand, self-administered and other hetero-administered). On the one hand, self-administered questionnaires give rise to possible biases due to missing or misinterpreting the questions, since they do not have the interviewer to ask questions about the questionnaire itself. On the other hand, hetero-administered questionnaires lose the freedom of response time and objective exposure of the actual use of networks or psychological exposures, since they may feel pressured or observed by the recruiter.79,80 Third, the symptoms of depression and anxiety were measured for this analysis as continuous variables using the PHQ-9 and GAD-7 scores, without considering the different levels of depression in a qualitative way. Additionally, these questionnaires were only measured once, and subsequent changes in the level of these affective problems, cumulative burden of depression and anxiety, or time-varying associations with outcomes were not tracked. Finally, as an observational study, the moderating effect of self-efficacy and resilience in the relationship between anxiety and problematic ICT use needs to be confirmed by randomized controlled trials. Future intervention research needs to be carried out extensively to verify our hypothesized models.
Conclusion
These findings make a significant contribution to the growing literature on problematic ICT use, personal health factors, and anxiety and depression symptoms among adults. Our findings reveal that low self-efficacy, low resilience, low sense of coherence, low self-esteem and highly problematic use of technologies are associated with greater severity of depression and anxiety. Of significance, we also found the moderation effect of self-efficacy and resilience in the relationship between problematic ICT use and anxiety. Adults with low resilience and self-efficacy have a worse severity of depression and anxiety associated with the problematic use of ICTs.
Our findings provide new insight into the role that personal health factors plays in problematic use of ICT and affective mental health, and underline the a new approach to preventive identification and early care measures among people at risk and their families. However, more research is needed on the interrelationship between problematic ICT use and addictions, personal factors, and depression and anxiety. The study findings provided a foundation for future research on the combined role of personal factors and problematic ICT use and how they affect the severity of depression and anxiety.
Abbreviations
B, unstandardized regression coefficient; β, standardized regression coefficient; BFI-10, big five personality inventory; CD-RISC-10, Connor-Davidson resilience scale; CI, confidence interval; DSM-5, diagnostic and statistical manual of mental disorders; ΔF, F-statistic difference between models; ΔR2, total variance difference between models; F, F-statistic; GAD-7, generalized anxiety disorder; GSES-12, general self-efficacy scale; ICT, information and communications technologies; ICD-11, international classification of diseases; M, mean; N, frequencies; %, percentages; P, p-value; PHC, primary health care; PHQ-9, patient health questionnaire; R2, total variance; RSES, Rosenberg self-esteem scale; SE, standard error; SD, standard deviation; SOC-13, sense of coherence questionnaire; STROBE, Strengthening the Reporting of Observational studies in Epidemiology; T, t-value; VIF, variance inflation factor.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Ethics Approval and Informed Consent
The project was approved by the Clinical Research Ethics Committee of Aragon N° PI20/302. The study was developed in accordance with the Declaration of Helsinki. Since the project involves the collection and processing of personal data, including personal information; the collection, treatment, communication, and transfer of personal data of all participating subjects must comply with the provisions of the General Data Protection Regulation (EU) (GDPR 2016/679) and the applicable national legislation, Organic Law 3/2018, of December 5, on the Protection of Personal Data. Informed consent was obtained from all participants. All subjects allowed their data to be anonymized and used only for the purposes and publication of the results of this study.
Acknowledgments
We would like to thank the Aragonese Primary Care Research Group (GAIAP, B21_23R) that is part of the Department of Innovation, Research and University at the Government of Aragón (Spain), the Primary Care Prevention and Health Promotion Network [RedIAPP-Health Institute Carlos III, Spain (RD16/0007/0001)], the Research Network on Chronicity, Primary Care and Health Promotion (RICAPPS, RD21/0016/0005) that is part of the Results-Oriented Cooperative Research Networks in Health (RICORS) (Carlos III Health Institute), and Feder Funds (Another way to make Europe), for their support in the development of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study has been funded by Health Institute Carlos III (ISCIII) through the project grant number PI19/01076, Feder Funds Another way to make Europe. The funders had no role in the study design, data collection and analysis, decision to publish, or manuscript preparation. The trial will be audited once a year by the funding organization.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. World Health Organization. Depression; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/depression.
2. Santomauro DF, Mantilla Herrera AM, Shadid J, et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet. 2021;398(10312):1700–1712. doi:10.1016/S0140-6736(21)02143-7
3. World Health Organization. Depression and other common mental disorders: global health estimates; 2017. Available from: https://apps.who.int/iris/handle/10665/254610.
4. International classification of diseases 11th revision. Mental, behavioural or neurodevelopmental disorders; 2022. Available from: http://id.who.int/icd/entity/334423054.
5. Sekhon S, Gupta V. Mood Disorder. StatPearls; 2022.
6. Elhai JD, Dvorak RD, Levine JC, Hall BJ. Problematic smartphone use: a conceptual overview and systematic review of relations with anxiety and depression psychopathology. J Affect Disord. 2017;207:251–259. doi:10.1016/j.jad.2016.08.030
7. Elhai JD, Levine JC, Hall BJ. The relationship between anxiety symptom severity and problematic smartphone use: a review of the literature and conceptual frameworks. J Anxiety Disord. 2019;62:45–52. doi:10.1016/j.janxdis.2018.11.005
8. Vahedi Z, Saiphoo A. The association between smartphone use, stress, and anxiety: a meta-analytic review. Stress Health. 2018;34(3):347–358. doi:10.1002/smi.2805
9. Cuervo Carabel T, Orviz Martínez N, Arce García S, Fernández Suárez I. Technostress in communication and technology society: scoping literature review from the web of science. Arch Prev Riesgos Labor. 2018;21(1). doi:10.12961/aprl.2018.21.01.4
10. World Health Organization. Public health implications of excessive use of the internet, computers, smartphones and similar electronic devices: meeting report; 2014. Available from: https://apps.who.int/iris/handle/10665/184264.
11. Grant JE, Potenza MN, Weinstein A, Gorelick DA. Introduction to behavioral addictions. Am J Drug Alcohol Abuse. 2010;36(5):233–241. doi:10.3109/00952990.2010.491884
12. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-V-TR).
13. World Health Organization. International Classification of Diseases (ICD-11); 2023. Available from: https://icd.who.int/browse11/l-m/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f1448597234.
14. Spanish Observatory of Drugs and Addictions. Report on behavioral disorders 2022: gambling with money, use of video games and compulsive use of the internet in surveys on drugs and other addictions in Spain EDADES and ESTUDES; 2022.
15. Morrison CM, Gore H. The relationship between excessive internet use and depression: a questionnaire-based study of 1319 young people and adults. Psychopathology. 2010;43(2):121–126. doi:10.1159/000277001
16. Pedrero Pérez EJ, Ruiz Sánchez de León JM, Rojo Mota G, et al. Information and Communication Technologies (ICT): abuse of the Internet, video games, mobile phones, instant messaging and social networks through MULTICAGE-ITC. Adicciones. 2017;30(1):19. doi:10.20882/adicciones.806
17. Younes F, Halawi G, Jabbour H, et al. Internet addiction and relationships with insomnia, anxiety, depression, stress and self-esteem in university students: a cross-sectional designed study. PLoS One. 2016;11(9):e0161126. doi:10.1371/journal.pone.0161126
18. Jahan I, Hosen I, Al Mamun F, Kaggwa MM, Griffiths MD, Mamun MA. How has the COVID-19 pandemic impacted internet use behaviors and facilitated problematic internet use? A Bangladeshi study. Psychol Res Behav Manag. 2021;14:1127–1138. doi:10.2147/PRBM.S323570
19. Kalwar SK, Heikkinen K, Porras J. Conceptual framework for assessing human anxiety on the internet. Procedia Soc Behav Sci. 2012;46:4907–4917. doi:10.1016/j.sbspro.2012.06.358
20. Lau JTF, Walden DL, Wu AMS, Cheng K, Lau MCM, Mo PKH. Bidirectional predictions between Internet addiction and probable depression among Chinese adolescents. J Behav Addict. 2018;7(3):633–643. doi:10.1556/2006.7.2018.87
21. Rachubińska K, Cybulska A, Szkup M, Grochans E. Analysis of the relationship between personality traits and Internet addiction. Eur Rev Med Pharmacol Sci. 2021;25(6):2591–2599. doi:10.26355/eurrev_202103_25422
22. Campbell-Sills L, Stein MB. Psychometric analysis and refinement of the Connor-Davidson resilience scale (CD-RISC): validation of a 10-item measure of resilience. J Trauma Stress. 2007;20(6):1019–1028. doi:10.1002/jts.20271
23. Sherer M, Maddux JE, Mercandante B, Prentice-Dunn S, Jacobs B, Rogers RW. The self-efficacy scale: construction and validation. Psychol Rep. 1982;51(2):663–671. doi:10.2466/pr0.1982.51.2.663
24. Antonovsky A. The structure and properties of the sense of coherence scale. Soc Sci Med. 1993;36(6):725–733. doi:10.1016/0277-9536(93)90033-Z
25. Rosenberg M. Society and the Adolescent Self-Image. Princeton: Princeton University Press; 1965. doi:10.1126/science.148.3671.804
26. Benet-Martínez V, John OP. Los Cinco Grandes across cultures and ethnic groups: multitrait-multimethod analyses of the Big Five in Spanish and English. J Pers Soc Psychol. 1998;75(3):729–750. doi:10.1037/0022-3514.75.3.729
27. Smith JL, Hollinger-Smith L. Savoring, resilience, and psychological well-being in older adults. Aging Ment Health. 2015;19(3):192–200. doi:10.1080/13607863.2014.986647
28. To QG, Vandelanotte C, Cope K, et al. The association of resilience with depression, anxiety, stress and physical activity during the COVID-19 pandemic. BMC Public Health. 2022;22(1):1–8. doi:10.1186/S12889-022-12911-9/TABLES/4
29. Zhou P, Zhang C, Liu J, Wang Z. The relationship between resilience and internet addiction: a multiple mediation model through peer relationship and depression. Cyberpsychol Behav Soc Netw. 2017;20(10):634–639. doi:10.1089/cyber.2017.0319
30. Yilmaz R, Karaoglan Yilmaz FG. Problematic internet use in adults: the role of happiness, psychological resilience, dispositional hope, and self-control and self-management. J Rational. 2022;1–19. doi:10.1007/S10942-022-00482-Y/FIGURES/1
31. Milanovic M, Ayukawa E, Usyatynsky A, Holshausen K, Bowie CR. Self efficacy in depression. J Nervous Ment Dis. 2018;206(5):350–355. doi:10.1097/NMD.0000000000000804
32. Schönfeld P, Preusser F, Margraf J. Costs and benefits of self-efficacy: differences of the stress response and clinical implications. Neurosci Biobehav Rev. 2017;75:40–52. doi:10.1016/J.NEUBIOREV.2017.01.031
33. Mei S, Yau YHC, Chai J, Guo J, Potenza MN. Problematic Internet use, well-being, self-esteem and self-control: data from a high-school survey in China. Addict Behav. 2016;61:74–79. doi:10.1016/j.addbeh.2016.05.009
34. Yang SY. Effects of self-efficacy and self-control on internet addiction in middle school students: a social cognitive theory-driven focus on the mediating influence of social support. Child Health Nurs Res. 2020;26(3):357–365. doi:10.4094/CHNR.2020.26.3.357
35. Giglio RE, Rodriguez-Blazquez C, de Pedro-Cuesta J, Forjaz MJ. Sense of coherence and health of community-dwelling older adults in Spain. Int Psychogeriatr. 2015;27(4):621–628. doi:10.1017/S1041610214002440
36. Skonieczna J, Fronczak A, Kielan A, Brytek-Matera A, Olejniczak D. The impact of the sense of coherence on the problematic internet use among secondary school students. J Health Educ Res Dev. 2018;06:04. doi:10.4172/2380-5439.1000290
37. Orth U, Robins RW, Widaman KF. Life-span development of self-esteem and its effects on important life outcomes. J Pers Soc Psychol. 2012;102(6):1271–1288. doi:10.1037/A0025558
38. Seabra L, Loureiro M, Pereira H, Monteiro S, Afonso RM, Esgalhado G. Relationship between internet addiction and self-esteem: cross-cultural study in Portugal and Brazil. Interact Comput. 2017;29(5):767–778. doi:10.1093/IWC/IWX011
39. Jourdy R, Petot JM. Relationships between personality traits and depression in the light of the “Big Five” and their different facets. L’Évolution Psychiatrique. 2017;82(4):e27–e37. doi:10.1016/j.evopsy.2017.08.002
40. Marciano L, Camerini AL, Schulz PJ. Neuroticism and internet addiction: what is next? A systematic conceptual review. Pers Individ Dif. 2022;185:111260. doi:10.1016/j.paid.2021.111260
41. Antonovsky A. The salutogenic model as a theory to guide health promotion. Health Promot Int. 1996;11(1):11–18. doi:10.1093/heapro/11.1.11
42. Mittelmark MB, Sagy S, Eriksson M, et al. The Handbook of Salutogenesis. Springer International Publishing; 2017. doi:10.1007/978-3-319-04600-6
43. European Union. Eurostat statistics data browser; 2023. Available from: https://ec.europa.eu/eurostat/databrowser/view/ISOC_CI_IFP_FU__custom_5093896/default/table?lang=en.
44. Li Y, Li GX, Yu ML, Liu CL, Qu YT, Wu H. Association between anxiety symptoms and problematic smartphone use among Chinese university students: the mediating/moderating role of self-efficacy. Front Psychiatry. 2021;12. doi:10.3389/fpsyt.2021.581367
45. Hao Z, Jin L, Huang J, Wu H. Stress, academic burnout, smartphone use types and problematic smartphone use: the moderation effects of resilience. J Psychiatr Res. 2022;150:324–331. doi:10.1016/j.jpsychires.2022.03.019
46. Pita-Fernández S. Determination of the sample size. Cad Aten Primaria. 2001;3:138–214.
47. Spanish Ministry of Health. Mental health in data: prevalence of health problems and consumption of psychotropic drugs and related drugs from primary care clinical records; 2021. Available from: https://www.sanidad.gob.es/estadEstudios/estadisticas/estadisticas/estMinisterio/SIAP/home.htm.
48. World Health Organization. Depressive disorder. 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/depression.
49. Government of Aragon. Aragon transparency: Health and Health Service. Available from: https://transparencia.aragon.es/content/salud-y-sanidad.
50. Kroenke K, Spitzer RL. The PHQ-9: a new depression diagnostic and severity measure. Psychiatr Ann. 2002;32(9):509–515. doi:10.3928/0048-5713-20020901-06
51. Muñoz-Navarro R, Cano-Vindel A, Medrano LA, et al. Utility of the PHQ-9 to identify major depressive disorder in adult patients in Spanish primary care centres. BMC Psychiatry. 2017;17(1):291. doi:10.1186/s12888-017-1450-8
52. Spitzer RL, Kroenke K, Williams JBW, Löwe B, Brief A. Measure for assessing generalized anxiety disorder. Arch Intern Med. 2006;166(10):1092. doi:10.1001/archinte.166.10.1092
53. Garcia-Campayo J, Zamorano E, Ruiz MA, et al. Cultural adaptation into Spanish of the generalized anxiety disorder-7 (GAD-7) scale as a screening tool. Health Qual Life Outcomes. 2010;8(1):8. doi:10.1186/1477-7525-8-8
54. Herrero R, Espinoza M, Molinari G, et al. Psychometric properties of the general self efficacy-12 scale in Spanish: general and clinical population samples. Compr Psychiatry. 2014;55(7):1738–1743. doi:10.1016/j.comppsych.2014.05.015
55. Notario-Pacheco B, Solera-Martínez M, Serrano-Parra MD, Bartolomé-Gutiérrez R, García-Campayo J, Martínez-Vizcaíno V. Reliability and validity of the Spanish version of the 10-item Connor-Davidson Resilience Scale (10-item CD-RISC) in young adults. Health Qual Life Outcomes. 2011;9(1):63. doi:10.1186/1477-7525-9-63
56. John OP, Donahue E, Kentle R The Big Five Inventory--Versions 4a and 54. University of California, Berkeley, Institute of Personality and Social Research; 1991. Available from: https://www.ocf.berkeley.edu/~johnlab/bfi.htm.
57. Moreno B, Alonso M, Álvaréz E. Sense of coherence, resistant, personality, self-esteem and health. J Health Psychol. 1997;9(2):115–137.
58. Martín-Albo J, Núñez JL, Navarro JG, Grijalvo F. The Rosenberg self-esteem scale: translation and validation in university students. Span J Psychol. 2007;10(2):458–467. doi:10.1017/S1138741600006727
59. Sheskin DJ. Handbook of Parametric and Nonparametric Statistical Procedures.
60. Núñez E, Steyerberg EW, Núñez J. Regression modeling strategies. Rev Esp Cardiol. 2011;64(6):501–507. doi:10.1016/j.recesp.2011.01.019
61. Hamilton JD. Time Series Analysis. Princeton University Press; 1994.
62. Hayes A. Introduction to Mediation, Moderation, and Conditional Process Analysis. A Regression-Based Approach.
63. IBM Corp. IBM SPSS statistics for windows, version 25.0; 2017. Available from: https://www.ibm.com/.
64. Hayes AF, Cai L. Using heteroskedasticity-consistent standard error estimators in OLS regression: an introduction and software implementation. Behav Res Methods. 2007;39(4):709–722. doi:10.3758/BF03192961
65. Anyfantakis D, Symvoulakis EK, Linardakis M, Shea S, Panagiotakos D, Lionis C. Effect of religiosity/spirituality and sense of coherence on depression within a rural population in Greece: the Spili III project. BMC Psychiatry. 2015;15(1). doi:10.1186/S12888-015-0561-3
66. López-Martínez C, Frías-Osuna A, del-Pino-Casado R. Sentido de coherencia y sobrecarga subjetiva, ansiedad y depresión en personas cuidadoras de familiares mayores[Sense of coherence and subjective overload, anxiety and depression in caregivers of elderly relatives]. Gac Sanit. 2019;33(2):185–190. Spanish. doi:10.1016/J.GACETA.2017.09.005
67. Orth U, Robins RW, Widaman KF, Conger RD. Is low self-esteem a risk factor for depression? Findings from a longitudinal study of Mexican-origin youth. Dev Psychol. 2014;50(2):622–633. doi:10.1037/a0033817
68. Uliaszek AA, Zinbarg RE, Mineka S, et al. The role of neuroticism and extraversion in the stress–anxiety and stress–depression relationships. Anxiety Stress Coping. 2010;23(4):363–381. doi:10.1080/10615800903377264
69. Hussain Z, Griffiths MD. Problematic social networking site use and comorbid psychiatric disorders: a systematic review of recent large-scale studies. Front Psychiatry. 2018;9:686. doi:10.3389/FPSYT.2018.00686/BIBTEX
70. Rochat L, Wilkosc-Debczynska M, Zajac-Lamparska L, et al. Internet use and problematic use in seniors: a comparative study in Switzerland and Poland. Front Psychiatry. 2021;12. doi:10.3389/fpsyt.2021.609190
71. Annoni AM, Petrocchi S, Camerini AL, Marciano L. The relationship between social anxiety, smartphone use, dispositional trust, and problematic smartphone use: a moderated mediation model. Int J Environ Res Public Health. 2021;18(5):2452. doi:10.3390/ijerph18052452
72. Ha JH, Kim SY, Bae SC, et al. Depression and internet addiction in adolescents. Psychopathology. 2007;40(6):424–430. doi:10.1159/000107426
73. Kim K, Ryu E, Chon MY, et al. Internet addiction in Korean adolescents and its relation to depression and suicidal ideation: a questionnaire survey. Int J Nurs Stud. 2006;43(2):185–192. doi:10.1016/j.ijnurstu.2005.02.005
74. Lazaroiu G, Kovacova M, Siekelova A, Vrbka J. Addictive behavior of problematic smartphone users: the relationship between depression, anxiety, and stress. Rev Contemp Philos. 2020;19:50. doi:10.22381/RCP1920204
75. Taylor P, Kral P, Vrbka J, Gregova E. Problematic smartphone use, social anxiety symptom severity, and technology-related behaviors and attitudes. Analysis Metaphysics. 2020;19:73. doi:10.22381/AM1920208
76. Tao Z, Wu G, Wang Z. The relationship between high residential density in student dormitories and anxiety, binge eating and Internet addiction: a study of Chinese college students. Springerplus. 2016;5(1):1579. doi:10.1186/s40064-016-3246-6
77. Geng Y, Gu J, Wang J, Zhang R. Smartphone addiction and depression, anxiety: the role of bedtime procrastination and self-control. J Affect Disord. 2021;293:415–421. doi:10.1016/j.jad.2021.06.062
78. Álvarez-Hernández G, Delgado-DelaMora J. Design of Epidemiological Studies. I. The Cross-Sectional Study: Taking a Picture of Health and Disease. Bol Clin Hosp Infant Edo Son. 2015;32(1):26–34.
79. Demetriou C, Ozer BU, Essau CA. Self-report questionnaires. In: The Encyclopedia of Clinical Psychology. John Wiley & Sons, Inc.; 2015:1–6. doi:10.1002/9781118625392.wbecp507
80. Choi B, Granero R, Pak A. Catalog of bias in health questionnaires. Rev Costarr Salud Pública. 2010;19(2):106–118.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Subjective Sleep Disruption and Mood Disorders are Associated with the Risk of Chronic Pain in Patients with Obstructive Sleep Apnea
Liu L, Li X, Xue P, Wu M, Zeng S, Dai Y, Zhou J
Nature and Science of Sleep 2022, 14:2023-2032
Published Date: 7 November 2022
Vitamin B12, Folate, Homocysteine, Inflammatory Mediators (Interleukin-6, Tumor Necrosis Factor-α and C-Reactive Protein) Levels in Adolescents with Anxiety or Depressive Symptoms
Tan Y, Zhou L, Huang J, Chen X, Wu Y, Song X, Wang J, Hu H, Yang Q
Neuropsychiatric Disease and Treatment 2023, 19:785-800
Published Date: 7 April 2023
AI Technology panic—is AI Dependence Bad for Mental Health? A Cross-Lagged Panel Model and the Mediating Roles of Motivations for AI Use Among Adolescents
Huang S, Lai X, Ke L, Li Y, Wang H, Zhao X, Dai X, Wang Y
Psychology Research and Behavior Management 2024, 17:1087-1102
Published Date: 12 March 2024
Longitudinal Problematic Social Media Use in Students and Its Association with Negative Mental Health Outcomes
Shannon H, Bush K, Shvetz C, Paquin V, Morency J, Hellemans KGC, Guimond S
Psychology Research and Behavior Management 2024, 17:1551-1560
Published Date: 8 April 2024
Mushrooms, Microdosing, and Mental Illness: The Effect of Psilocybin on Neurotransmitters, Neuroinflammation, and Neuroplasticity
Kinderlehrer DA
Neuropsychiatric Disease and Treatment 2025, 21:141-155
Published Date: 29 January 2025