Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Depression is Associated with the Increase Risk of Multimorbidity Among the General Population in Indonesia
Authors Sinaga IOY, Barliana MI ![]() , Pradipta IS
, Pradipta IS ![]() , Iskandarsyah A
, Iskandarsyah A ![]() , Abdulah R, Alfian SD
, Abdulah R, Alfian SD ![]()
Received 2 June 2022
Accepted for publication 15 August 2022
Published 30 August 2022 Volume 2022:15 Pages 1863—1870
DOI https://doi.org/10.2147/JMDH.S372712
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ivanny OY Sinaga,1 Melisa I Barliana,2,3 Ivan Surya Pradipta,1,3 Aulia Iskandarsyah,4 Rizky Abdulah,1,3 Sofa D Alfian1,3
1Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jatinangor, Indonesia; 2Department of Biological Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jatinangor, Indonesia; 3Centre of Excellence in Higher Education for Pharmaceutical Care Innovation, Universitas Padjadjaran, Jatinangor, Indonesia; 4Department of Clinical Psychology, Faculty of Psychology, Universitas Padjadjaran, Jatinangor, Indonesia
Correspondence: Sofa D Alfian, Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jl. Raya Jatinangor, KM 21, Jatinangor, Sumedang, Indonesia, Tel/Fax +62-022-7796200, Email [email protected]
Purpose: Depression is common among patients with chronic disease. However, little is known about the association between depression and the risk of developing multimorbidity. This study aims to identify the association between depression and the incidence of multimorbidity among the general population in Indonesia.
Patients and Methods: The national cross-sectional population-based survey used publicly available data from the Indonesian Family Life Survey (IFLS-5) for 2014 among respondents aged ≥ 15 years. Depression was assessed using the Center for Epidemiologic Studies-Depression (CES-D) scale. The number of chronic diseases and amount of sociodemographic information were obtained from self-reported data. A logistic regression analysis was used to assess the association between depression and multimorbidity, adjusting for confounders. Odds ratios (ORs) with 95% confidence intervals (CIs) were reported.
Results: The study recruited 2222 respondents; the majority of them were male (68.0%) and aged 55– 64 years (34.7%). Of the total number of respondents, 69.6% have depression and 36.5% have multimorbidity. The prevalence of depression in respondents increases with age. Depressive symptoms were more likely to report multimorbidity (OR 2.05, 95% CI: 1.66– 2.52).
Conclusion: Depression is associated with the increased risk of multimorbidity among the general population in Indonesia. Therefore, screening for and treatment of depression for those at risk of developing multimorbidity are urgently needed.
Keywords: mental health problem, multimorbidity, Indonesian Family Life Survey
Introduction
The prevalence of depression as a mental health problem is one of the highest worldwide, with about 280 million people diagnosed in 2021. In Indonesia, a study from the Institute for Health Metrics and Evaluation showed that, since 1990, depression has the most significant burden among mental health problems.1 In 2018, it was reported that 6.1% of the population in Indonesia experienced it, with the highest prevalence in the Central Sulawesi Province (12.3%) and the lowest in Jambi Province (1.8%). The prevalence of depression in Indonesia also increases with age, the highest being in the age group of 75 years and older (8.9%), followed by 65–74 years (8.0%).1
Depression significantly increases the overall burden of illness in patients with chronic diseases, which is an association that researchers have long been reporting.2 Individuals with depression are at significant risk of developing chronic diseases, such as diabetes, stroke, and heart diseases.3 Furthermore, depression is associated with both poor prognosis and a rapid progression of chronic diseases, including ischemic heart disease4 and diabetes.5 Population-based studies also demonstrate a strong association between depression and mortality resulting from cardiovascular diseases.6 Therefore, depression is linked to a significant burden in terms of the number of chronic diseases.7 Patients with depression and chronic diseases may require additional complicated treatment, thereby leading to adverse drug reactions and higher treatment costs.8 However, little is known about the association between depression and multimorbidity.
The Indonesian Family Life Survey (IFLS) is a longitudinal socioeconomic and health survey in Indonesia and covers approximately 83% of the Indonesian population.9 Several studies that utilize data from the fourth and fifth waves of the IFLS (IFLS-4 and IFLS-5) demonstrate the association between depressive symptoms and recurrent aphthous stomatitis,10 food insecurity,11 and labor market outcomes in Indonesia.12 However, the association between depression and multimorbidity among the general population in Indonesia remains unclear.
The primary objective of this study was to evaluate the association between depression and the risk of developing multimorbidity in Indonesia. The secondary objective was to explore the prevalence of depression in different age groups.
Methods
Study Design
This study used national longitudinal and cross-sectional data from the IFLS-5 collected from 2014 to 2015 using a multistage stratified sampling design representing 83% of the Indonesian population and with a response rate of more than 90%.9 Data have been publicly available since 2016.9 The IFLS collected extensive measures of basic sociodemographic and certain economic characteristics of all household members as well as their health status, including self-reported measures of general health, symptoms, pain, and biomarker measurements. The ethical review boards of the Research and Development Corporation and Gadjah Mada University approved the IFLS. Written informed consent was obtained from all respondents before data collection.9 Approval was sought from the research ethics committee of Universitas Padjadjaran, Indonesia, who waived the request because this study uses anonymous data from the IFLS (No. 510/UN6.KEP/EC/2022).
Study Population
The total number of IFLS-5 respondents was 34,464 (aged up to >80 years). Data were obtained from respondents who were at least 15 years of age at the completion of the survey. Respondents with available data on depressive symptoms and the number of chronic diseases were included, whereas respondents with missing values for these variables were excluded.
Depression
Depressive symptoms were measured using the self-reported Center for Epidemiologic Studies-Depression (CES-D) scale.9 The CES-D contains 10 questions to assess the feelings of the respondents with a focus on those that are highly correlated with depressive symptoms.13 Eight questions pertain to negative symptoms (eg, I was bothered by things that usually do not bother me), whereas the two other questions assess positive symptoms of depression (eg, I felt hopeful about the future). The respondents indicate the frequency with which each item applied to them in the past week using a three-point Likert-type scale (0 = rarely or none of the time, 1 = some or little of the time, 2 = moderately or much of the time, and 3 = most or almost all the time). The final score is calculated by adding all items after reversing the positive-mood items. A respondent with a total score equal to or above 10 is considered exhibiting depressive symptoms.14 The CES-D questionnaire was translated into Indonesian (forward translation) and retranslated into English (back translation) by two independent translators.15
Multimorbidity
Multimorbidity was defined as respondents reporting more than one chronic condition listed in IFLS-5.16 The chronic conditions were assessed using a self-report questionnaire with the question “Has a doctor/paramedic/nurse/midwife ever told you that you had the following chronic conditions of disease?”. The response options were hypertension, diabetes, tuberculosis, asthma, chronic lung diseases, heart problems, liver diseases, stroke, cancer/malignant tumors, arthritis/rheumatism, high cholesterol, prostatitis, kidney diseases, digestive disorders, psychological problems, and diseases related to memory.
Sociodemographic Factors
Sociodemographic factors included the age at the completion of the survey, gender (male and female), Body Mass Index (underweight, normal, and overweight), smoking habit (never smoked, active smoker, and ex-smoker), ethnicity (non-Javanese and Javanese), marital status (currently unmarried and currently married), working status (unemployed and employed), education level (unschooled, elementary school, junior high school, senior high school, and higher education), and residence (rural and urban).
Statistical Analysis
Descriptive statistics were used to summarize the characteristics of the respondents. Depressive symptoms were estimated for each age group. We grouped the prevalence of depression by age according to the National Basic Health Research from Indonesia in 2018. A Chi-square test was performed to assess the univariate association between the characteristics of the respondents and outcome. We conducted complete case analyses because the amount of missing data was small. The potential factors associated with the outcome at a significance level of p < 0.25 in the univariate analyses were included in the initial multivariate model. Multivariate binary logistic regression was performed to evaluate the association between depressive symptoms and the risk of multimorbidity, adjusting for age, smoking habits, ethnicity, working status, and education level. The adjusted association was obtained, and an odds ratio (OR) with a 95% confidence interval (95% CI) was reported. All statistical analyses were performed using Statistical Package for the Social Sciences (version 26.0; IBM, Armonk, NY, USA).
Results
Baseline Characteristics
Of the 34,464 respondents in IFLS-5, a total sample of 2222 respondents was included in this study. The majority were male (68.0%) and aged 45–54 years (37.4%). No respondents under 35 years old were included because they did not meet the inclusion criteria. Approximately half the respondents were non-Javanese (55.3%), had graduated from elementary school (51.5%), and resided in urban areas (62.4%) at the time of the IFLS-5 (Table 1). Of the total participants, 69.6% had depressive symptoms, whereas 36.5% experienced multimorbidity. The prevalence pattern of depression increased with age, wherein the highest rate is observed for the oldest age group (Figure 1).
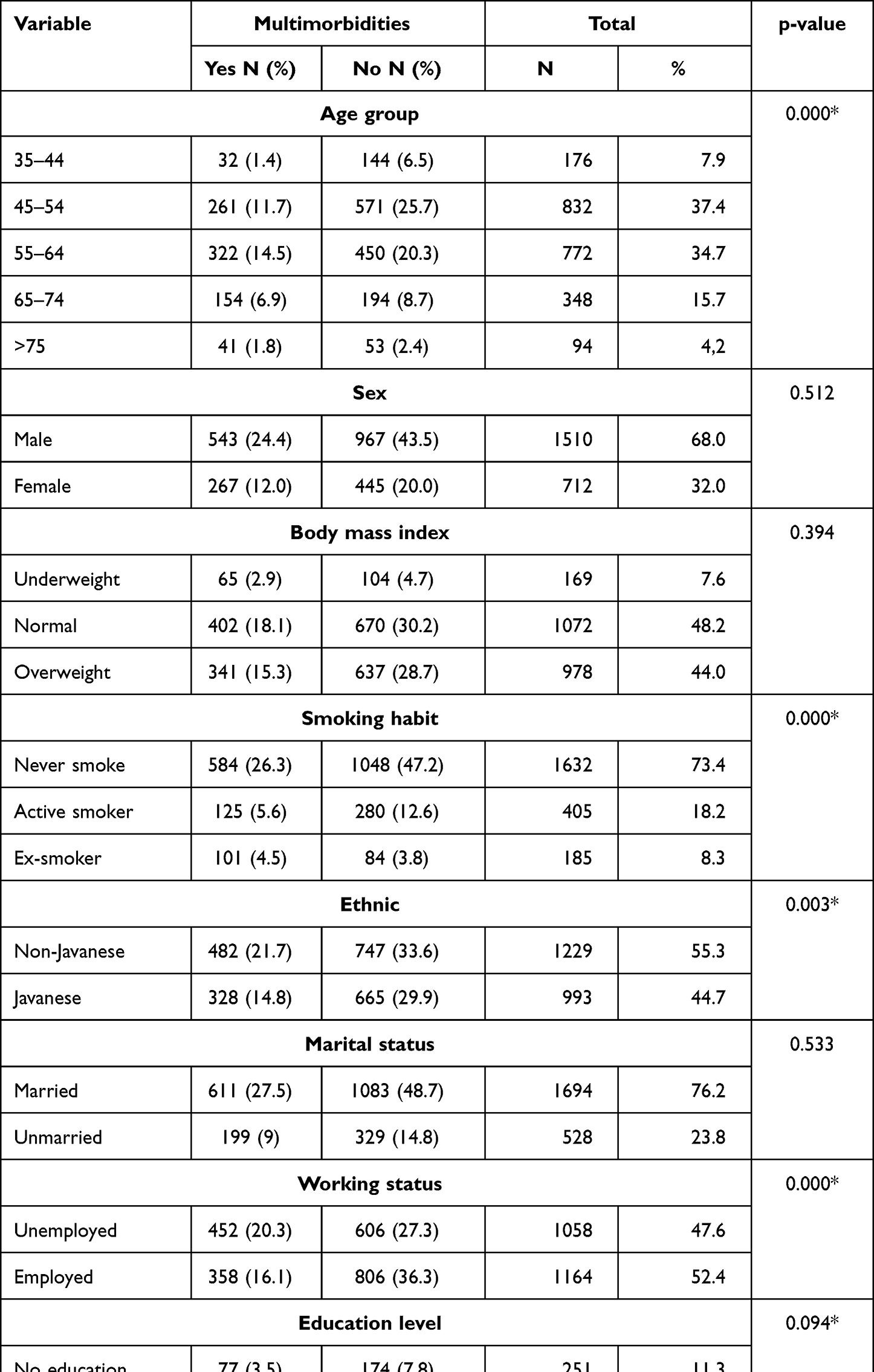 |
Table 1 Characteristics of Respondents (n = 2222) |
 |
Figure 1 Respondents’ depression prevalence pattern. |
Association Between Depression and Multimorbidity
Adjusted analyses were conducted for the age group (p < 0.001), smoking habits (p < 0.001), ethnicity (p = 0.003), working status (p < 0.001), and education level (p = 0.094) variables (Table 1). In the multivariate model, having depressive symptoms is associated with an increased risk of developing multimorbidity (OR: 2.28; 95% CI: 1.86–2.80) (Table 2) compared with those without depressive symptoms.
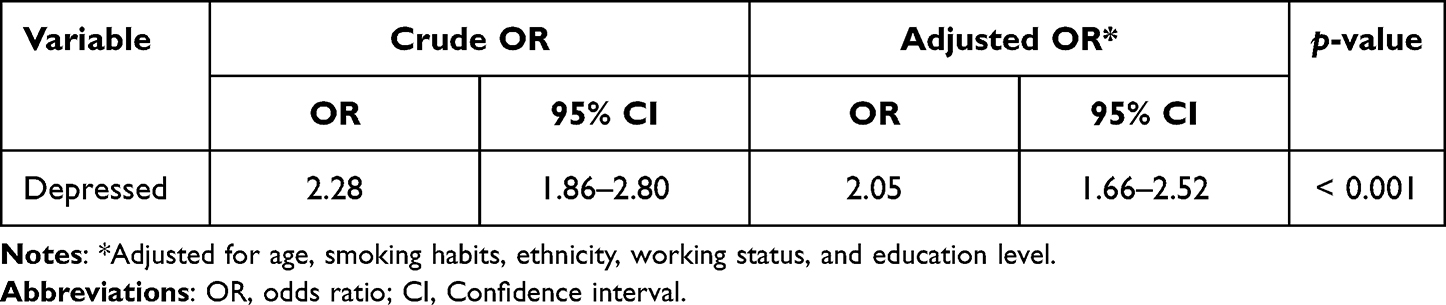 |
Table 2 Multivariate Regression Analysis of Depression Associated with Multimorbidity |
Discussion
Of the 2222 respondents, more than half of them reported having depressive symptoms and more than a quarter of them experienced multimorbidity. Respondents with depressive symptoms were more likely to report multimorbidity. The prevalence pattern of depression increased with age.
We observed that the increased prevalence of depression by age is consistent with previous studies.17,18 One study showed that depressive disorders increase substantially in the highest age groups.18 However, although depression is a common problem associated with age, it is not part of aging.18 This phenomenon may be explained by factors associated with aging, such as a higher proportion of women in the population, more physical disabilities, high levels of cognitive impairment, and lower socioeconomic status.19 Furthermore, the high prevalence of depression observed in this study may be explained by the lack of public awareness about depression and limited availability of screening for depression.
After adjusting for confounders, we further observed that respondents with depression were more likely to experience multimorbidity. These findings were consistent with previous studies where patients with the major depressive disorders exhibited significantly higher incidences of chronic diseases, such as cardiometabolic diseases (Hazard Ratio (HR) = 1.78, 95% CI = 1.21–2.60), musculoskeletal diseases (HR = 1.74, 95% CI = 1.23–2.47), and digestive diseases (HR = 1.78, 95% CI = 1.20–2.64) compared with patients without major depression.20 Moreover, the findings of the present study were consistent with those from the United States, Denmark, England, and Australia. These studies reported that depressive symptoms are associated with a high incidence rates of multiple conditions of chronic diseases such as arthritis, heart problems, diabetes, cancer, and respiratory problems.15,20–24 Two studies on the Danish population reported that individuals diagnosed with mood disorders have a higher likelihood of acquiring various of medical illnesses.22,23 A study in Australia stated that the odds of a cohort with depression developing multimorbidity prior to the onset of depressive symptoms was 1.81 (95% CI = 1.49–2.20) compared with a cohort without depression. After the onset of depressive symptoms, the OR was 2.38 (95% CI = 2.20–2.57).24 Even in the absence of clinically diagnosed depression, the burden of depression was associated with multiple diseases such as cardiometabolic, respiratory, musculoskeletal and digestive diseases, and with cancer, especially in individuals with mood-related depressive and somatic symptoms.20
Biological or behavioral mechanisms may mediate the interaction between depression and chronic diseases. However, the biological mechanism of depression that results in multimorbidity remains unclear, although several factors, such as inflammation, metabolic burden, and vascular burden, may underlie this association.7,25 Depression may also affect chronic diseases by decreasing both treatment adherence and physical activity and by increasing tobacco and alcohol use.26 Therefore, lifestyle modification can be implemented to reduce the burden of multimorbidity.
Some types of lifestyles tend to play a more significant role in the occurrence of depression when compared with the occurrence of chronic diseases.7 Previous studies illustrate that depression has a two-way relationship with smoking,27–29 which is also associated with several chronic diseases such as diabetes, stroke, and coronary heart disease.30–32 In addition, depression may trigger other behaviors associated with physical inactivity due to the symptoms of major depression, including fatigue and reduced pleasure in activities.33 A study on patients with heart disease also demonstrated that depressive symptoms reduced the exercise capacity pursued.34
An individual with depression requires exceptional management regarding their mental state and physical condition to manage chronic s and even more severe multimorbidity. Indonesia is a low-middle-income country with a high prevalence of multimorbidity.35,36 Therefore, programs for the prevention, early detection, and management of depression among those who experience chronic diseases are urgently needed.
To our knowledge, this is the first study that assesses the association between depression and risk of multimorbidity using a population-based national survey. However, we acknowledge certain limitations related to methodological issues. This study cannot provide conclusions regarding the temporal relationship between depression and multimorbidity due to the cross-sectional design of the IFLS. We used a complete case analysis, which may reduce our study’s statistical power due to the sample size and may lead to selection bias. Furthermore, individual combinations of chronic diseases cannot be described due to the limitations of the data used. However, we do not believe this limitation poses a significant threat to the internal validity of the results.
Conclusion
After adjusting for confounders (age, smoking habits, ethnicity, occupation, and education level), respondents having depressive symptoms were more likely to report multimorbidity. Therefore, it can be concluded that depression or depressive symptoms are associated with the incidence of multiple morbidities. Screening for and treatment of depression for those at risk of developing multimorbidity are urgently needed.
Acknowledgments
We would like to thank Survey Meter and RAND Corporation for allowing us to use the Indonesian Family Life Survey database.
Funding
This study was funded by Universitas Padjadjaran (No: 1959/UN6.3.1/PT.00/2021).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kemenkes RI. Situasi kesehatan jiwa di Indonesia. [Mentah Health Situation in Indonesia]. InfoDATIN. 2019;3:12.
2. Lotfaliany M, Bowe SJ, Kowal P, Orellana L, Berk M, Mohebbi M. Depression and chronic diseases: co-occurrence and communality of risk factors. J Affect Disord. 2018;241:461–468. doi:10.1016/j.jad.2018.08.011
3. National Institute of Mental Health. Chronic illness and mental health: recognizing and treating depression. 2021. Available from: https://www.nimh.nih.gov/health/publications/chronic-illness-mental-health.
4. Glassman AH, Shapiro PA. Depression and the course of coronary artery disease. Am J Psychiatry. 1998;155(1):4–11. doi:10.1176/AJP.155.1.4
5. De Groot M, Anderson R, Freedland KE, Clouse RE, Lustman PJ. Association of depression and diabetes complications: a meta-analysis. Psychosom Med. 2001;63(4):619–630. doi:10.1097/00006842-200107000-00015
6. Unützer J, Patrick DL, Marmon T, Simon GE, Katon WJ. Depressive symptoms and mortality in a prospective study of 2558 older adults. Am J Geriatr Psychiatry. 2002;10(5):521–530. doi:10.1097/00019442-200209000-00005
7. Birk JL, Kronish IM, Moise N, Falzon L, Yoon S, Davidson KW. Depression and multimorbidity: considering temporal characteristics of the associations between depression and multiple chronic diseases. Health Psychol. 2019;38(9):802–811. doi:10.1037/hea0000737
8. Katon WJ, Lin EHB, Von Korff M, et al. Collaborative care for patients with depression and chronic illnesses. N Engl J Med. 2010;363(27):2611–2620. doi:10.1056/nejmoa1003955
9. Strauss J, Witoelar F, Sikoki B. The Fifth Wave of the Indonesia Family Life Survey: Overview and Field Report: Volume 1. RAND Corporation; 2016. doi:10.7249/wr1143.1
10. Hariyani N, Bramantoro T, Nair R, Singh A, Sengupta K. Depression symptoms and recurrent aphthous stomatitis—Evidence from a population-based study in Indonesia. Oral Dis. 2020;26(5):948–954. doi:10.1111/odi.13303
11. Isaura ER, Chen Y-C, Adi AC, Fan H-Y, Li C-Y, Yang S-H. Association between depressive symptoms and food insecurity among Indonesian adults: results from the 2007–2014 Indonesia Family Life Survey. Nutrients. 2019;11(12):3026. doi:10.3390/nu11123026
12. Sohn K. Depressive symptoms are not related to labor market outcomes in Indonesia. Hitotsubashi J Econ. 2018;59(2):45–60.
13. Vilagut G, Forero CG, Barbaglia G, Alonso J. Screening for depression in the general population with the center for epidemiologic studies depression (ces-d): a systematic review with meta-analysis. PLoS One. 2016;11(5):1–17. doi:10.1371/journal.pone.0155431
14. Björgvinsson T, Kertz SJ, Bigda-Peyton JS, McCoy KL, Aderka IM. Psychometric properties of the CES-D-10 in a psychiatric sample. Assessment. 2013;20(4):429–436. doi:10.1177/1073191113481998
15. Holahan CJ, Pahl SA, Cronkite RC, Holahan CK, North RJ, Moos RH. Depression and vulnerability to incident physical illness across 10 years. J Affect Disord. 2010;123(1):222–229. doi:10.1016/j.jad.2009.10.006
16. Hajat C, Stein E. The global burden of multiple chronic conditions: a narrative review. Prev Med Rep. 2018;12(6):284–293. doi:10.1016/j.pmedr.2018.10.008
17. Kemenkes RI. Hasil Riset kesehatan dasar tahun 2018. [2018 Results of Basic Health Research]. Kementrian Kesehat RI. 2018;53(9):1689–1699.
18. National Institute of Aging. Depression and older adults. 2021. Available from: https://www.nia.nih.gov/health/depression-and-older-adults.
19. Luppa M, Sikorski C, Luck T, et al. Age- and gender-specific prevalence of depression in latest-life - Systematic review and meta-analysis. J Affect Disord. 2012;136(3):212–221. doi:10.1016/j.jad.2010.11.033
20. Gaspersz R, Lamers F, Beekman ATF, van Hemert AM, Schoevers RA, Penninx BWJH. The impact of depressive disorder symptoms and subtypes on 6-year incidence of somatic diseases. Psychother Psychosom. 2018;87(5):308–310. doi:10.1159/000491933
21. Karakus MC, Patton LC. Depression and the onset of chronic illness in older adults: a 12-year prospective study. J Behav Health Serv Res. 2011;38(3):373–382. doi:10.1007/s11414-011-9234-2
22. Poole L, Steptoe A. Depressive symptoms predict incident chronic disease burden 10 years later: findings from the English Longitudinal Study of Ageing (ELSA). J Psychosom Res. 2018;113:30–36. doi:10.1016/j.jpsychores.2018.07.009
23. Momen NC, Plana-Ripoll O, Agerbo E, et al. Association between mental disorders and subsequent medical conditions. N Engl J Med. 2020;382(18):1721–1731. doi:10.1056/NEJMoa1915784
24. Xu X, Mishra GD, Jones M. Depressive symptoms and the development and progression of physical multimorbidity in a national cohort of Australian women. Health Psychol. 2019;38(9):812–821. doi:10.1037/hea0000738
25. Triolo F, Harber-Aschan L, Belvederi Murri M, et al. The complex interplay between depression and multimorbidity in late life: risks and pathways. Mech Ageing Dev. 2020:192. doi:10.1016/j.mad.2020.111383.
26. DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherence. Arch Intern Med. 2000;160(14):2101–2107. doi:10.1001/ARCHINTE.160.14.2101
27. Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005;352(16):1685–1695. doi:10.1056/NEJMra043430
28. Dantzer R, O’Connor JC, Freund GG, Johnson RW, Kelley KW. From inflammation to sickness and depression: when the immune system subjugates the brain. Nat Rev Neurosci. 2008;9(1):46–56. doi:10.1038/nrn2297
29. Goldring MB, Otero M. Inflammation in osteoarthritis. Curr Opin Rheumatol. 2011;23(5):471–478. doi:10.1097/BOR.0b013e328349c2b1
30. Wolf PA, D’Agostino RB, Kannel WB, Bonita R, Belanger AJ. Cigarette smoking as a risk factor for stroke: the Framingham Study. JAMA. 1988;259(7):1025–1029. doi:10.1001/jama.1988.03720070025028
31. Willi C, Bodenmann P, Ghali WA, Faris PD, Cornuz J. Active smoking and the risk of type 2 diabetes. A systematic review and meta-analysis. JAMA. 2007;298(22):2654–2664. doi:10.1001/jama.298.22.2654
32. Huxley RR, Woodward M. Cigarette smoking as a risk factor for coronary heart disease in women compared with men: a systematic review and meta-analysis of prospective cohort studies. Lancet. 2011;378(9799):1297–1305. doi:10.1016/S0140-6736(11)60781-2
33. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
34. Papasavvas T, Alhashemi M, Micklewright D, Association between depressive symptoms and exercise capacity in patients with heart disease: a meta-analysis. J Cardiopulm Rehabil Prev. 2017;37(4):239–249. doi:10.1097/HCR.0000000000000193
35. World Health Organization. Multimorbidity: A Priority for Global Health Research. Academy of Medical Sciences; 2018.
36. The World Bank. The world bank in Indonesia; 2021. Available from: https://www.worldbank.org/en/country/indonesia/overview#1.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.